Back to Journals » International Journal of General Medicine » Volume 15
The Relationship Between Prognosis and Red Cell Distribution Width (RDW) and RDW-Albumin Ratio (RAR) in Patients with Severe COVID-19 Disease
Received 7 October 2022
Accepted for publication 30 November 2022
Published 16 December 2022 Volume 2022:15 Pages 8637—8645
DOI https://doi.org/10.2147/IJGM.S392453
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Birsen Ertekin, Tarık Acar
Department of Emergency, University of Health Sciences, Beyhekim Training and Research Hospital, Konya, Turkey
Correspondence: Birsen Ertekin, Tel +903322243524 – 3145, Email [email protected]
Purpose: The present study aimed to investigate the relationship between prognosis and the red cell distribution width (RDW) and the RDW-albumin ratio (RAR) in patients with coronavirus diseases 2019 (COVID-19), since serum albumin and RDW levels may reflect inflammatory conditions.
Patients and Methods: A total of 289 patients who had been diagnosed with severe COVID-19 in the emergency department were retrospectively analyzed. The RAR levels were calculated by dividing RDW-CV by albumin. Patient groups (survivors, dying patients, those who received mechanical ventilation (MV) support or not, and those who needed vasopressors or not) were compared with regard to RDW-SD, RDW-CV and the RAR levels.
Results: RDW-SD, RDW-CV and the RAR levels were found to be statistically significantly higher in patients who died, and who received MV and vasopressor support, compared to those who survived and did not receive support (p< 0.001 for all). In addition, while the cut-off value of RAR was > 5.43, the sensitivity was 91.6%, the specificity was 93.7%, NPV was 93.1% and the AUC was 0.965 in predicting mortality (p< 0.001). Logistic regression analysis showed that RDW-SD and RAR were independent risk factors for mortality in patients with severe COVID-19.
Conclusion: Elevated RDW and RAR levels at the time of admission may independently predict mortality and the need for vasopressor or MV support.
Keywords: RDW–albumin ratio, Covid-19, prognosis, mortality
The Plain Language Summary
Currently, hematological and biochemical parameters are markers that can support diagnosis or predict severe disease in COVID−19. In this study, it was investigated whether RDW and RAR were associated with the prognosis of severe COVID-19 patients.
RDW-SD, RDW-CV and the RAR levels were found to be statistically significantly higher in patients who died, and who received MV and vasopressor support, compared to those who survived and did not receive support. Logistic regression analysis showed that RDW-SD and RAR were independent risk factors for mortality in patients with severe COVID-19.
Elevated RDW and RAR levels at the time of admission may independently predict mortality and prognosis.
Introduction
The determination of laboratory markers that predict clinical impairment and prognosis during the coronavirus disease 2019 (COVID-19) pandemic is of vital importance. Severe COVID-19 is often characterized by the need for mechanical ventilation (MV) and intensive care unit (ICU), and the mortality rate has been reported to be around 40%.1 Due to being inexpensive, widespread and easily available, hematological parameters have become the first choice for the early diagnosis and prognosis prediction in COVID-19.2,3 Red cell distribution width (RDW) which may easily and routinely be measured in venous blood seems to be a marker with a high potential in providing risk classification and in predicting poor outcomes in patients with severe pneumonia.4,5 Today, many studies have indicated that RDW is a significant and potent prognostic marker for COVID-19 patients.6,7
Albumin is a protein that has an important role in the nutrition and preservation of plasma osmolarity.8 It was particularly shown that there was a close relationship between disease severity and the albumin level in elderly pneumonia patients and low albumin levels are a prognostic marker in these patients.9 In many studies, hypoalbuminemia at the time of admission was stated to be related to mortality in COVID-19 patients.10,11
RAR, which is defined as the proportion of RDW to albumin, is a novel and simple inflammatory marker. A strong inflammatory response may lead to a significant increase in RAR.12 Recent studies have suggested that RAR alone may yield better results for the prediction of prognosis than evaluating RDW and albumin separately.13,14 Zhao et al have reported that RAR has a better predictive value than RDW and albumin in the prediction of mortality in stroke patients. The authors have also stated that RAR could be used for risk classification particularly in emergency rooms as it is not influenced by parameters such as blood pressure and heart rate and could easily be obtained.15 Two recent studies have indicated that the RAR is an independent marker for mortality in critically ill patients.4,16 Yoo et al, associated RAR with mortality in patients with acute respiratory distress syndrome (ARDS).17 Although RAR has been investigated in various inflammatory disorders, to the best of our knowledge, there are no studies available in the literature investigating the relationship between RAR and COVID-19. Since serum albumin and RDW levels could reflect inflammatory conditions,13,18 the present study has investigated the relationship between RDW and RAR, and the prognosis of patients with severe COVID-19.
Materials and Methods
Patients and Study Design
A total of 289 consecutive patients who had been hospitalized due to confirmed diagnosis of severe COVID-19 at the emergency department of a pandemic hospital between February 01, 2022, and April 01, 2022, and who fulfilled the inclusion criteria were included in the study. Patients who were above 18 years of age, those whose real-time reverse transcriptase polymerase chain reaction (RT-PCR) test results were positive, those whose clinical and laboratory data could be reached through the hospital data management system, and those whose diagnoses of severe/critical COVID-19 had been confirmed based on the current guidelines, were included in the study.19,20 Patients who were under 18 years of age, those who were pregnant, those who had a history of acute/chronic hematological disorders, hepatic or renal failure, chronic alcohol or substance addiction, those who had been diagnosed with cancer, bacterial pneumonia/sepsis, autoimmune and immunosuppressive disorders, those who had been subjected to trauma and those whose data could not be accessed through the hospital data management system were excluded from the study. RAR (%/g/dL) was obtained by dividing RDW-CV (%) that was obtained from the routine whole blood analysis by albumin (g/dL). All parameters, mainly RDW-SD (standard deviation), RDW-CV (coefficient of variation) and RAR were compared between the two groups (patients who survived and died). RDW-SD, RDW-CV and RAR levels were also compared among patients who needed MV support and vasopressors or not. The study was approved by the Local Ethics Committee of Necmettin Erbakan University [date: March 18, 2022, and number: 2022/3695 (8563.R1)].
Data Collection
The data regarding age, gender, medical history, vital signs at the time of admission (fever, pulse rate, systolic blood pressure, oxygen saturation, respiratory rate), Glasgow Coma Scale (GCS), CURB-65 score, arterial blood gas, routine blood analysis results [white blood cell (WBC) count, neutrophil, lymphocyte, platelet (PLT) count, RDW-SD, RDW‐CV, MCV (mean corpuscular volume), hemoglobin (Hb), MPV (mean platelet volume), platelet distribution width (PDW)], AST (aspartate transaminase), ALT (alanine transaminase), troponin-I, D-dimer, CRP, procalcitonin (PCT), lactate and albumin values], PCR result, report of spiral computed tomography (CT) of the thorax, the need for MV (non-invasive/ invasive/ high-flow nasal cannula oxygen) or vasopressor support, the duration of hospital stays and the outcomes (discharge/ in-hospital mortality) were retrospectively obtained from epicrisis reports of the patients. Patients who required MV and/or vasopressor support during their admission to the emergency room and also during hospitalization were included in the study. For prediction of prognosis, further analyses were carried out for RDW-SD, RDW-CV, RAR, albumin, lactate, PCT, CRP, neutrophil and lymphocyte values. Only the variables that fulfilled the Box-Tidwell assumption were included in the logistic regression model. Complete blood count (CBC) was measured using the Mindray auto hematology analyzer BC-6800 device (Shenzhen, China). Biochemical parameters were measured using the Mindray chemistry analyzer BS-2000M device (Jiangsu, China). PaO2, PaCO2, and lactate levels were tested using the Siemens Healthcare diagnostic Rapidpoint 500 blood gas device (Dublin, Ireland). The Coronex COVID-19 QPCR (DS BIO and NANO Tech. Ltd, Ankara, Turkey) kit was used for the RT-PCR test.
Statistical Analysis
Descriptive analyses were carried out. The categorical data were given as rates and numbers. The categorical data were compared with the Chi-square test. The distribution of the numerical data was analyzed using the visual (histogram and likelihood plots) and analytical methods (Kolmogorov–Smirnov/Shapiro–Wilk tests). The normally distributed data were given as mean ± standard deviation and the non-normally distributed data were given as median and interquartile range (IQR). The normally distributed groups were compared using the Student’s t-test and the non-normally distributed groups were compared using the Mann–Whitney U-test. For estimation of mortality, Binary logistic regression analysis was carried out for determining the independent variables. The likelihood of mortality prediction of the RDW-SD, RDW-CV, RAR, Albumin, Lactate, PCT, CRP, Neutrophil, Lymphocyte values and the diagnostic predictive value of RDW-SD, RDW-CV, RAR for prediction of mechanical ventilator and vasopressor need was analyzed with the receiver operating characteristics (ROC) curve analysis. In the assessment of the area under the curve (AUC), the diagnostic value of the test was interpreted to be statistically significant when the type 1 error level was below 5%. The AUC values of ROC analyses were compared with the DeLong method using the MedCalc program. Cut-off values were calculated with the Youden index. The sensitivity, specificity and negative predictive values (NPV) of the cut-off values were calculated. A p level of < 0.05 was accepted to be statistically significant in all tests. Statistical analyses were performed using the IBM SPSS version 22 and MedCalc version 20 programs.
Results
While 158 out of 289 patients survived, 131 patients died. Of all patients, 162 (56.1%) were male and the mean age was 66.09±15.9 years. The comparison of the surviving and the dying patient groups with regard to demographic, clinical and laboratory findings have been presented in Table 1. When the surviving and the dying patients were compared with regard to age and gender, while the mean age of dying patients was statistically significantly higher (p<0.001), no difference was found with regard to gender (p=0.185). Fever, pulse rate, respiratory rate, CURB-65, RDW-SD, RDW-CV, RAR, WBC, neutrophil count, MPV, PDW, AST, ALT, troponin I, D-dimer, CRP, PCT, lactate levels and the rate of the patients who needed vasopressor medications were found to be significantly higher in the dying patient group (p<0.001 for all). Similarly, oxygen saturation, systolic blood pressure, PaO2, lymphocyte count, Hb, PLT, albumin values, GCS scores and the rate of the patients who needed MV were lower (for all p<0.001) and the duration of hospital stay was shorter (p=0.209) in the dying patient group.
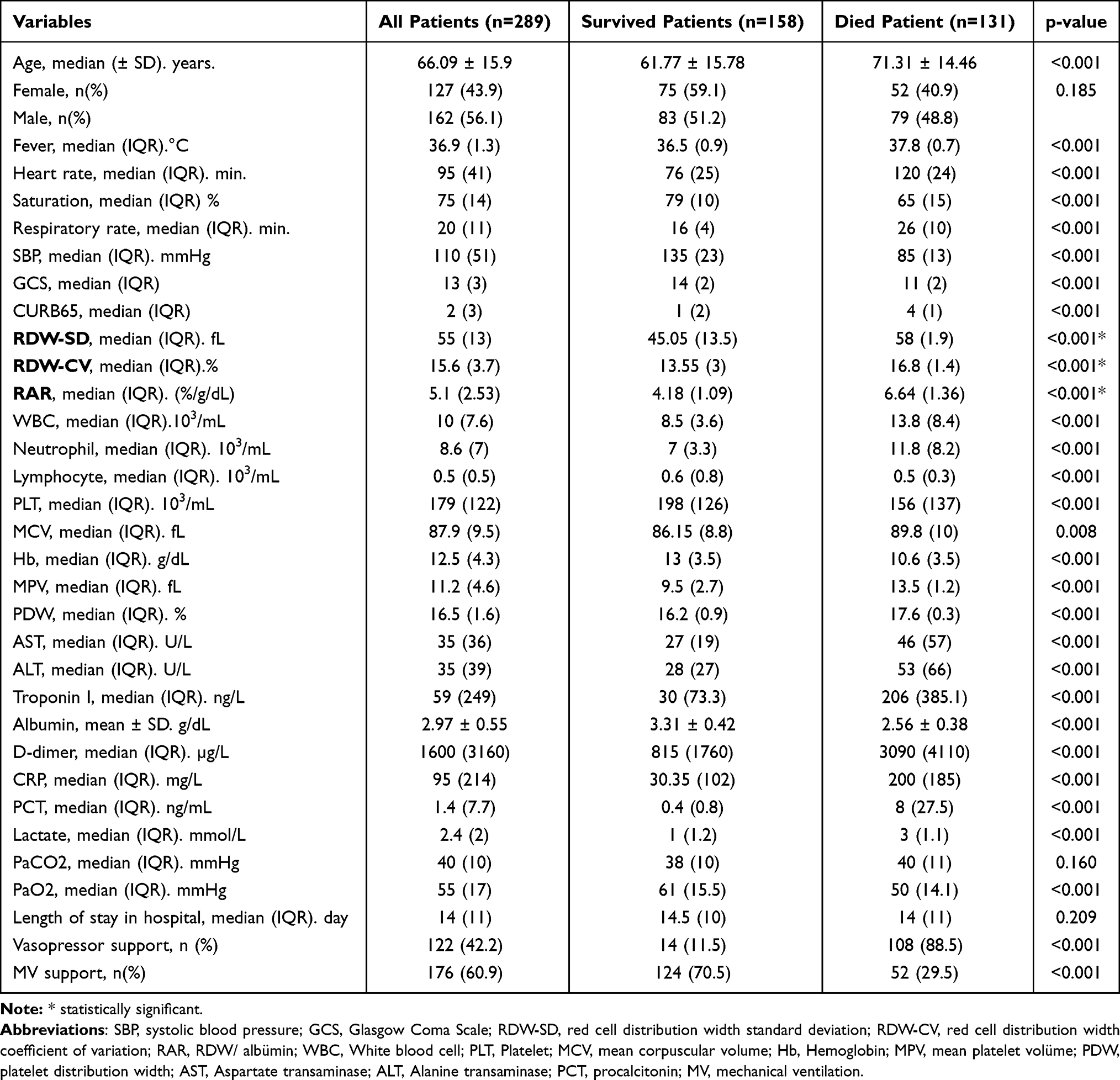 |
Table 1 Comparison of Demographic, Clinical and Laboratory Findings of Survived and Died Patients |
When the patients who received MV and vasopressor support and who did not receive were compared with regard to RDW-SD, RDW-CV and RAR, the RDW-SD, RDW-CV and RAR values were determined to be statistically significantly higher among those who received MV and vasopressor support (p<0.001 for all) (Table 2).
 |
Table 2 Relationship with Patient Groups of RDW-SD. RDW-CV and RAR Parameters |
The ROC analysis of RDW-SD, RAR, RDW-CV, albumin, lactate, PCT, CRP, neutrophil, and lymphocyte levels for mortality estimation has been demonstrated in Table 3. According to this, RDW-SD had the highest AUC value, and the lymphocyte count had the lowest AUC value (0.976, 0.965, 0.944, 0.914, 0.913, 0.900, 0.813, 0.790, 0.685, respectively) (p<0.001 for all). In addition, among all parameters, the RDW-SD cut-off value was >55.32, it reached the maximum values with 98.5% sensitivity, 96.2% specificity and 98.7% NPV. The logistic regression analysis showed that RDW-SD and RAR were independent risk factors for COVID-19-related mortality (Tables 4 and 5).
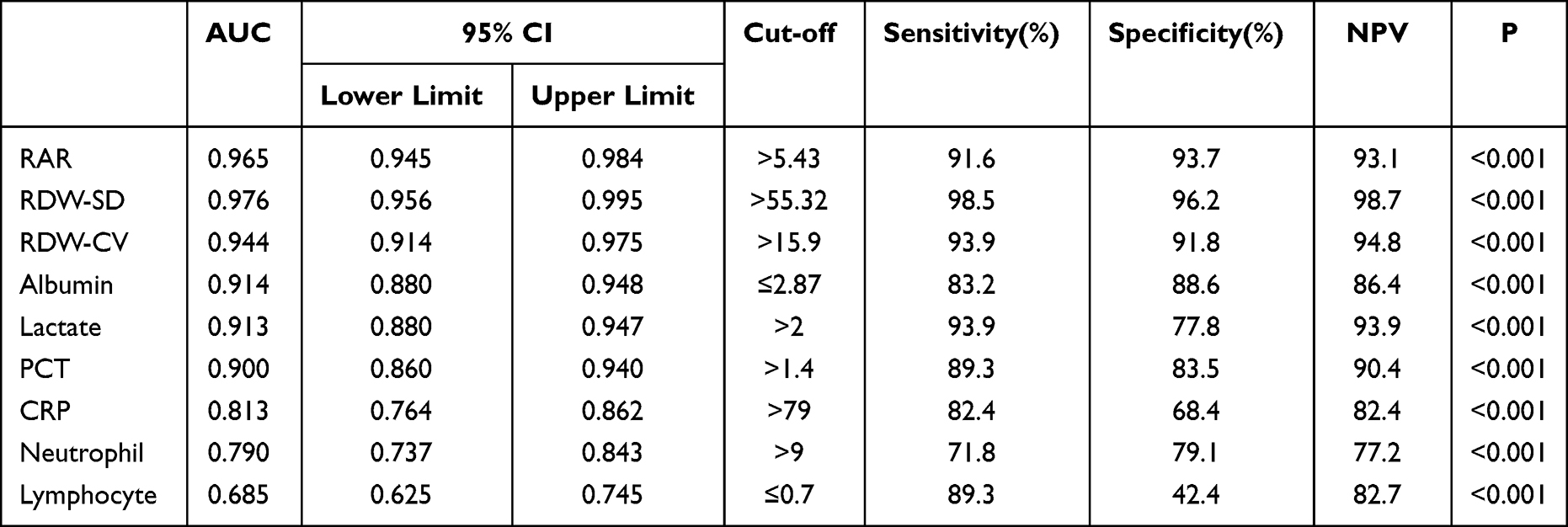 |
Table 3 The ROC Analysis of Parameters in the Prediction of Mortality |
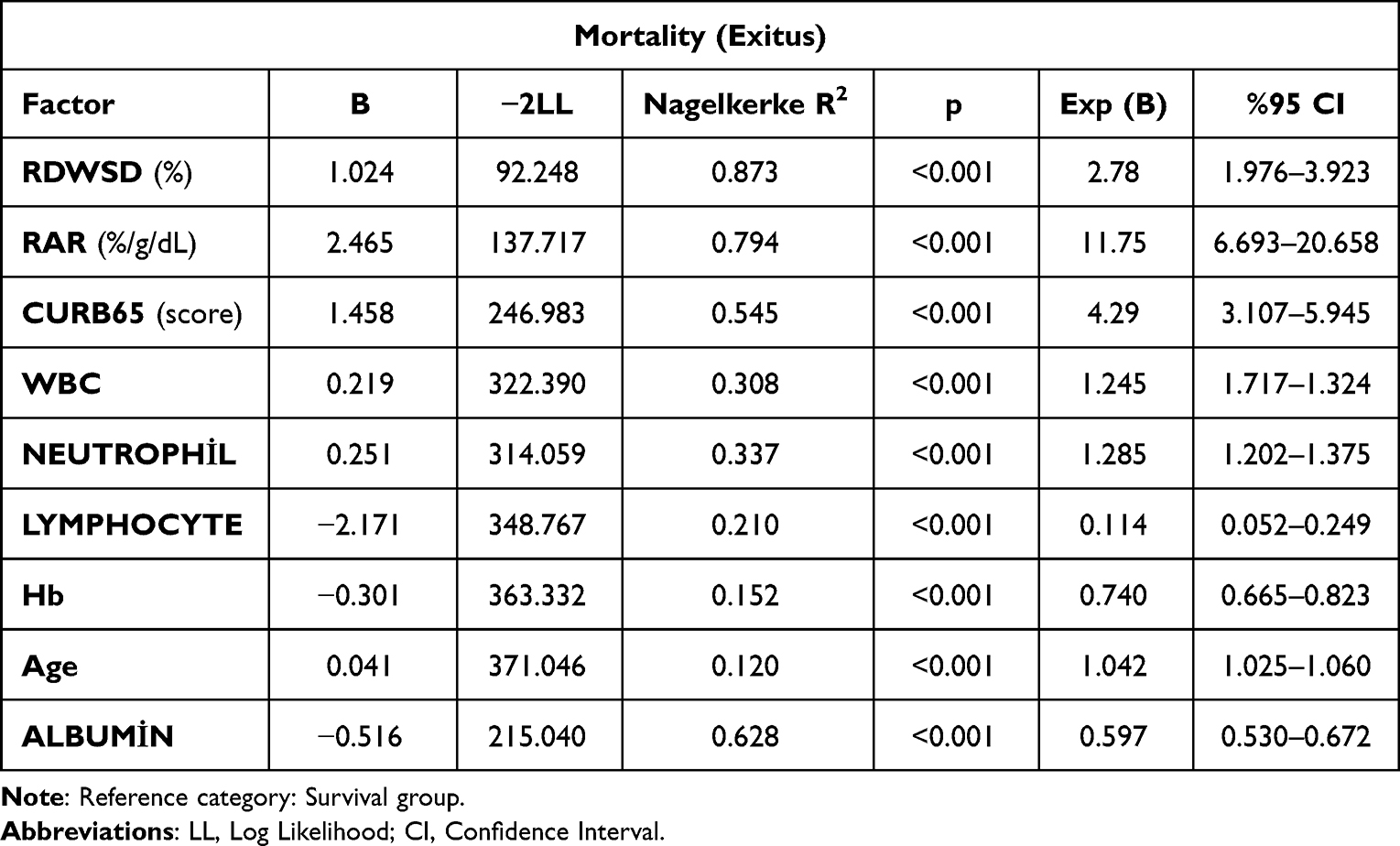 |
Table 4 Logistic Regression Analysis of Parameters According to Mortality Separately |
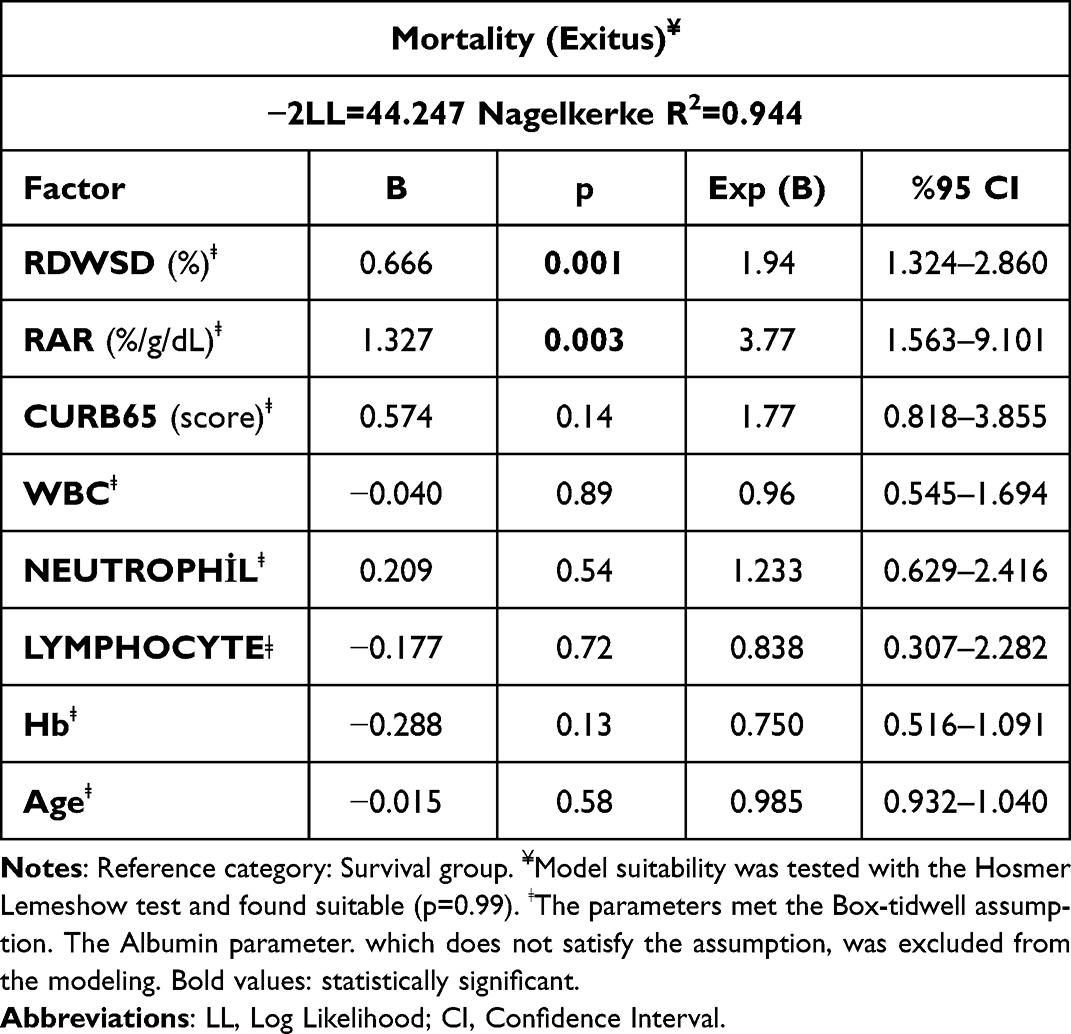 |
Table 5 Logistic Regression Model According to Mortality When Parameters Used Together |
Discussion
The rates of hospitalization, admission to ICU and death are high among patients with severe COVID-19. Hence, early detection of high-risk patients and early triage may help facilitate intervention and proper use of hospital resources.21 Hematological tests are economic, rapid, and they are early accessible prognostic markers with proven usefulness for evaluating the disease severity in COVID-19. Elevated RDW levels on admission or gradually increasing RDW levels during hospitalization have been associated with higher morbidity and mortality in patients with COVID-19.22
Conditions such as oxidative stress, tissue hypoxia, neuro-humoral over-activity, endothelial dysfunction and inflammation that play important roles in COVID-19 infection affect the RDW levels.23 RDW demonstrates anisocytosis among red blood cells (RBC). Anisocytosis is mostly due to inflammation.18 An elevated RDW means increased RBC destruction, ineffective erythropoiesis, and/or shortened RBC life.24 In previous studies, elevated RDW values were found to be related to prognosis in patients with community-acquired pneumonia (CAP), ARDS and COVID-19.25–27 In a meta-analysis, RDW values were found to be significantly higher in dying COVID-19 patients compared to survivors (95% CI=0.63–1.23; I2=85.58%). In addition, elevated RDW values were reported to be associated with the disease severity (30-day mortality, duration of hospital stays and the need for vasopressor support) (95% CI=0.47–0.97; I2=89.51%).28 In our study, as in the study of Wang et al,3 both RDW-SD and RDW-CV values were found to be significantly higher in dying patients compared to survivors (p<0.001). Furthermore, these two markers were also higher in patients who received MV and vasopressor support compared to those who did not (p<0.001). Therefore, according to the results of our study, an elevated RDW value on admission may be used as a marker that is related to disease severity and negative outcomes in patients with severe COVID-19.
Up to date, researchers have emphasized that the cut-off value of RDW-CV could vary between 12.85% and 14.35% in studies on COVID-19.3,22,27 Wang et al, reported that RDW could predict critical COVID-19 cases early when the cut-off value was >11.5%.23 Kilercik et al, demonstrated that when the cut-off value of RDW was 13.7, it showed 75.7% sensitivity and 81.6% specificity with an AUC of 0.787, and that it was the most valuable blood parameter for estimation of disease severity.24 Wang et al, determined that sensitivity, specificity and the AUC values were 73.1%, 80.2%, and 0.870, respectively when the cut-off value of RDW-SD was 42.15.3 In another study, RDW was shown to be a more valuable parameter for mortality estimation compared to CRP and PDW with a cut-off value of 15% (AUC:0.708, 92% sensitivity and 95% NPV).29 In our study, when compared to the other hematological markers, RDW-SD reached the maximum mortality estimation power with 98.5% sensitivity, 96.2% specificity, 98.7% NPV and 0.976 AUC, when the cut-off value was >55.32. Hence, this strong relationship between RDW levels and mortality could be suggested to result from inflammation, hypoxia and oxidative stress that are responsible for the pathophysiology of severe COVID-19.
Serum albumin is a laboratory marker that can be routinely measured in blood; it is an acute phase reactant, a protein that plays a role in the control of oncotic pressure and one that has antioxidant properties.4 In addition, albumin has been shown to be an inflammation marker.13,30 In the studies of Chen and Takegawa et al, the albumin levels were emphasized to be a prognostic factor in patients with pneumonia or sepsis.16,31 In many recent studies, low albumin levels on admission were proposed to be associated with all the other negative outcomes in addition to mortality in patients with severe COVID-19.10,11,32 Similar to the studies in the literature, in our study, too, low albumin levels were found to be closely associated with mortality (cut-off ≤2.87, 83.2% sensitivity, 88.6% specificity, AUC: 0.914, p<0.001).
RAR, which is defined as the ratio of RDW to albumin, is a new inflammatory marker.15 Elevated RAR, representing high RDW and decreased albumin levels, can predict severe inflammation.33 Therefore, RAR alone can reflect inflammatory states more accurately than either marker.13,15,30 In the study of Yoo et al, conducted with patients with ARDS, the RAR levels were associated with 60-day mortality (hazard ratio 1.134, p = 0.003). The authors also reported that the calculated AUC value for RAR was higher than that for RDW alone (0.681, 0.576, respectively, p= 0.002).17 In another study comprising patients with critical pneumonia who received MV support, it was shown that the mean RAR value in deceased patients was significantly higher than that in survivors (5.8 vs 4.8, p < 0.001, respectively). In addition, the authors reported that the 28-day mortality rate was significantly higher in patients with a RAR cut-off value of >5.73 than in patients with a RAR cut-off value of <5.73 (52.3% sensitivity, 79.2% specificity, and AUC: 0.688).4 In our study, the RAR levels were found to be higher in patients who died and in those who received MV and vasopressor support than in those who survived and did not receive support (for all p< 0.001). Furthermore, when the RAR cut-off value is >5.43, it seems to be as powerful a parameter as RDW in estimating mortality with 91.6% sensitivity, 93.7% specificity, 93.1% NPV and 0.965 AUC values. Consistent with the literature, the results of our study support that RAR, an inflammation marker, is a stronger parameter to predict the prognosis and disease severity in COVID-19 than RDW and albumin, even if it is used alone.12,15 Furthermore, RAR may contribute to risk classification and early triage in emergency rooms in case of intensive conditions such as the COVID-19 pandemic due to being a rapid and economic parameter that is easily calculated from routine blood analysis.34 Although the important roles of RDW or albumin have been reported in many studies on patients with COVID-19,10,24 we could not find a study on the prognostic value of RAR. Therefore, we hope that our study will be supported by other studies on this issue.
Strengths and Limitation
The strength of our study is its evaluating RDW, albumin and RAR values on admission, and also comparing all three parameters in severe COVID-19 patients. Hence, it may be accepted as a pioneer for the prediction of mortality and disease severity. However, there are some limitations in this study; First, selection bias cannot be excluded, since our study was a single-center, retrospective study with a small number of patients. Therefore, our results should be supported by larger, multicenter and prospective studies. Second, our patients could not be followed-up after discharge. Therefore, in our study, we have only presented the short-term mortality rates of RDW and RAR and cannot evaluate the effect on long-term mortality. Third, since we only used RDW and albumin values at the time of admission to the emergency department in our study, we cannot comment on whether the temporal changes in RDW and RAR may affect the outcome. Fourth, since our study was limited to a hospitalized group, the results cannot be generalized to all non-hospitalized individuals with COVID-19. Despite these limitations, we suggest that our study can contribute to the literature.
Conclusion
The results of our study indicate that elevated RDW and RAR levels at the time of admission could independently predict mortality, vasopressor support or the mechanical ventilation need in patients with severe COVID-19.
Ethical Approval
The study was approved by the Necmettin Erbakan University Faculty of Medicine Local Ethics Committee [date: 18/03/2022 and number: 2022/3695(8563.R1)]. The study was conducted in according to the principles of the Helsinki Declaration. Patients were informed about the study and written consents were obtained. The identity information of the patients was kept confidential.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
Not source of funding and support.
Disclosure
No authors declared any potential conflict of interest.
References
1. Henry BM, Benoit JL, Benoit S, et al. Red Blood Cell Distribution Width (RDW) predicts COVID-19 severity: a prospective, observational study from the cincinnati SARS-CoV-2 emergency department cohort. Diagnostics. 2020;10(9):618. doi:10.3390/diagnostics10090618
2. Şan İ, Gemcioğlu E, Davutoğlu M, et al. Which hematological markers have predictive value as early indicators of severe COVID-19 cases in the emergency department. Turk J Med Sci. 2021;51(6):2810–2821. doi:10.3906/sag-2008-6
3. Wang C, Zhang H, Cao X, et al. Red cell distribution width (RDW): a prognostic indicator of severe COVID-19. Ann Transl Med. 2020;8(19):1230. doi:10.21037/atm-20-6090
4. Jeong JH, Heo M, Lee SJ, Jeong YY, Lee JD, Yoo JW. Clinical usefulness of red cell distribution width/albumin ratio to discriminate 28-day mortality in critically ill patients with pneumonia receiving invasive mechanical ventilation, compared with lacate/albumin ratio: a retrospective cohort study. Diagnostics. 2021;11(12):2344. doi:10.3390/diagnostics11122344
5. Ren Q, Liu H, Wang Y, et al. The role of red blood cell distribution width in the severity and prognosis of community-acquired pneumonia. Can Respir J. 2021;2021:8024024. doi:10.1155/2021/8024024
6. Foy BH, Carlson JCT, Reinertsen E, et al. Association of red blood cell distribution width with mortality risk in hospitalized adults with SARS-CoV-2 infection. JAMA Netw Open. 2020;3(9):e2022058. doi:10.1001/jamanetworkopen.2020.22058
7. Lippi G, Henry BM, Sanchis-Gomar F. Red blood cell distribution is a significant predictor of severe illness in coronavirus disease 2019. Acta Haematol. 2021;144(4):360–364. doi:10.1159/000510914
8. Bernardi M, Angeli P, Claria J, et al. Albumin in decompensated cirrhosis: new concepts and perspectives. Gut. 2020;69:1127–1138. doi:10.1136/gutjnl-2019-3188430
9. Chen B, Liu W, Chen Y, et al. Effect of poor nutritional status and comorbidities on the occurrence and outcome of pneumonia in elderly adults. Front Med. 2021;8:719530. doi:10.3389/fmed.2021.719530
10. Akman C, Bakırdöğen S. The role of serum inflammatory markers, albumin, and hemoglobin in predicting the diagnosis in patients admitted to the emergency department with a pre-diagnosis of COVID-19. Rev Assoc Med Bras. 2021;67Suppl 1(Suppl1):91–96. doi:10.1590/1806-9282.67
11. Violi F, Cangemi R, Romiti GF, et al. Is albumin predictor of mortality in COVID-19? Antioxid Redox Signal. 2021;35(2):139–142. doi:10.1089/ars.2020.8142
12. Xu W, Huo J, Chen G, et al. Association between red blood cell distribution width to albumin ratio and prognosis of patients with sepsis: a retrospective cohort study. Front Nutr. 2022;9:1019502. doi:10.3389/fnut.2022.1019502
13. Long J, Xie X, Xu D, et al. Association between red blood cell distribution width-to-albumin ratio and prognosis of patients with aortic aneurysms. Int J Gen Med. 2021;14:6287–6294. doi:10.2147/IJGM.S328035
14. Donmez M, Ayata O. Prognostic significance of the red cell distribution width/albumin ratio in the prediction of the severity of acute biliary pancreatitis: a preliminary report. Cureus. 2022;14(10):e30183. doi:10.7759/cureus.30183
15. Zhao N, Hu W, Wu Z, et al. The red blood cell distribution width-albumin ratio: a promising predictor of mortality in stroke patients. Int J Gen Med. 2021;14:3737–3747. doi:10.2147/IJGM.S322441
16. Chen L, Lu XY, Zhu CQ. Prognostic value of albumin-red cell distribution width score in patients with severe community acquired pneumonia. Ann Palliat Med. 2020;9(3):759–765. doi:10.21037/apm.2020.04.22
17. Yoo JW, Ju S, Lee SJ, Cho YJ, Lee JD, Kim HC. Red cell distribution width/albumin ratio is associated with 60-day mortality in patients with acute respiratory distress syndrome. Infect Dis. 2020;52(4):266–270. doi:10.1080/23744235.2020.1717599
18. Jandaghian S, Vaezi A, Manteghinejad A, Nasirian M, Vaseghi G, Haghjooy Javanmard S. Red Blood Cell Distribution Width (RDW) as a predictor of in-hospital mortality in COVID-19 patients; a cross sectional study. Arch Acad Emerg Med. 2021;9(1):e67. doi:10.22037/aaem.v9i1.1325
19. Ministry of Health, Republic of Turkey. Guidance to COVID-19(SARSCov2infection). Available from: https://hsgm.saglik.gov.tr/depo/birimler/gocsagligi/covid19/rehber/COVID-19Rehberi20200414engv400214.05.2020.pdf.
20. WHO. Clinical management of severe acute respiratory infection when Novel coronavirus (nCoV) infection is suspected: interim guidance. Available from: https://www.who.int/internal-publications-detail/clinical-managementof-severe-acute-respiratory-infection-when-novel-Coronavirus-(ncov)-infection-is-suspected.
21. Lagadinou M, Gkentzi D, Marangos MN, Paliogianni F, Solomou EE. Red blood cell distribution width: another prognostic factor for COVID-19? Clin Hematol Int. 2021;3(2):69–71. doi:10.2991/chi.k.210404.001
22. Banon T, Wortsman J, Ben Moshe S, et al. Evaluating red blood cell distribution width from community blood tests as a predictor of hospitalization and mortality in adults with SARS-CoV-2: a cohort study. Ann Med. 2021;53(1):1410–1418. doi:10.1080/07853890.2021.1968484
23. Wang ZH, Fu BQ, Lin YW, et al. Red blood cell distribution width: a severity indicator in patients with COVID-19. J Med Virol. 2022;94(5):2133–2138. doi:10.1002/jmv.27602
24. Kilercik M, Demirelce Ö, Serdar MA, Mikailova P, Serteser M. A new haematocytometric index: predicting severity and mortality risk value in COVID-19 patients. PLoS One. 2021;16(8):e0254073. doi:10.1371/journal.pone.0254073
25. Lee JH, Chung HJ, Kim K, et al. Red cell distribution width as a prognostic marker in patients with community-acquired pneumonia. Am J Emerg Med. 2013;31:72–79. doi:10.1016/j.ajem.2012.06.004
26. Cai N, Jiang M, Wu C, He F. Red cell distribution width at admission predicts the frequency of acute kidney injury and 28-day mortality in patients with acute respiratory distress syndrome. Shock. 2022;57(3):370–377. doi:10.1097/SHK.0000000000001840
27. Sarkar S, Kannan S, Khanna P, Singh AK. Role of red blood cell distribution width, as a prognostic indicator in COVID-19: a systematic review and meta- analysis. Rev Med Virol. 2022;32(2):e2264. doi:10.1002/rmv.2264
28. Lee JJ, Montazerin SM, Jamil A, et al. Association between red blood cell distribution width and mortality and severity among patients. with COVID-19: a systematic review and meta-analysis. J Med Virol. 2021;93(4):2513–2522. doi:10.1002/jmv.26797
29. Bommenahalli Gowda S, Gosavi S, Ananda Rao A, et al. Prognosis of COVID-19: red cell distribution width, platelet distribution width, and C reactive protein. Cureus. 2021;13(2):e13078. doi:10.7759/cureus.13078
30. Zhao F, Liu M, Kong L. Association between red blood cell distribution width-to-albumin ratio and diabetic retinopathy. J Clin Lab Anal. 2022;36(4):e24351. doi:10.1002/jcla.24351
31. Takegawa R, Kabata D, Shimizu K, et al. Serum albumin as a risk factor for death in patients with prolonged sepsis: an observational study. J Crit Care. 2019;51:139–144. doi:10.1016/j.jcrc.2019.02.004
32. Acharya R, Poudel D, Bowers R, et al. Low serum albumin predicts severe outcomes in COVID-19 infection: a single-center retrospective case-control study. J Clin Med Res. 2021;13(5):258–267. doi:10.14740/jocmr4507
33. Zhou D, Wang J, Li X. The red blood cell distribution width–albumin ratio was a potential prognostic biomarker for diabetic ketoacidosis. Int J Gen Med. 2021;14:5375–5380. doi:10.2147/IJGM.S327733
34. Lu C, Long J, Liu H, et al. Red blood cell distribution width-to-albumin ratio is associated with all-cause mortality in cancer patients. J Clin Lab Anal. 2022;36(5):e24423. doi:10.1002/jcla.24423
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Red Cell Distribution Width and Mortality in Patients with Klebsiella pneumoniae Bloodstream Infection: A Cohort Study
Huang Y, Ao T, Hu M, Zhen P
Infection and Drug Resistance 2025, 18:5961-5971
Published Date: 14 November 2025