Back to Journals » Psychology Research and Behavior Management » Volume 16
The Relationship Between Perceived Vulnerability to Disease and Anxiety During the COVID-19 Pandemic: Serial Mediation by Fear of COVID-19 and Trust in the Government
Authors Yang Y ![]() , Wei W, Wang T
, Wei W, Wang T
Received 21 November 2022
Accepted for publication 14 March 2023
Published 25 March 2023 Volume 2023:16 Pages 989—996
DOI https://doi.org/10.2147/PRBM.S398555
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Yong Yang, Wenwen Wei, Ting Wang
School of Educational Science, Xinyang Normal University, Xinyang, Henan, People’s Republic of China
Correspondence: Yong Yang, School of Educational Science, Xinyang Normal University, Room 517, Xinyang, Henan, 464000, People’s Republic of China, Email [email protected]
Purpose: The continuing global spread of COVID-19 has seriously jeopardized human mental health. How to reduce the damage of COVID-19 pandemic to people’s mental health is a current research hotspot. The purpose of this study was to explore the influence mechanism of perceived vulnerability to disease on anxiety level during the COVID-19 pandemic.
Methods: A total of 1085 Chinese subjects were investigated by using the Fear of COVID-19 Scale, Perceived Vulnerability to Disease Scale, Trust in the Government Measure Scale and Anxiety Scale, which was conducted by an online survey using snowball sampling technique. Hayes PROCESS macro for SPSS was used to test the hypothesized mediating effects of fear of COVID-19 and rust in the government measure in the relationship between perceived vulnerability to disease (PVD) and anxiety.
Results: (1) the PVD significantly positively predicts anxiety level (0.001); (2) Fear of COVID-19 (p< 0.001) and trust in the government (p< 0.001) mediated the relationship between PVD and anxiety level respectively; (3) PVD could also indirectly predict anxiety level through the chain-mediated role of the fear of COVID-19 and the trust in the government measure (p< 0.001).
Conclusion: Our findings shed light on a correlation between perceived vulnerability to disease and anxiety. This study emphasizes the value of trust in the government in facing public stress events. Moreover, this study provides some implications for how to prevent or reduce public anxiety in an epidemic setting.
Keywords: COVID-19 pandemic, fear of COVID-19, perceived vulnerability to disease, anxiety, trust in the government measure
Introduction
The coronavirus disease 2019 (COVID-19) not only attacked our bodies, but also seriously affected the mental health and well-being of the whole society.1 The COVID-19 has led to an increase on anxiety level in many countries. Anxiety not only affects the individual’s life satisfaction,2 persistent anxiety may also lead to despair and depression, which in turn increases the risk of self-injury and suicide.3,4 Therefore, it is of great practical significance to study the psychological mechanism of anxiety under the background of COVID-19 to prevent or reduce the anxiety level.
High infectivity and high mortality rates make COVID-19 become a “very high-risk” epidemic. Based on the risk perception model of SARS epidemic situation, it is believed that individuals would show higher risk perception and worry about their own health and safety, and then induce anxiety level in this high-risk epidemic.5 However, for individuals, different perceived vulnerability to disease (PVD) may lead to different levels of perceived risk for the COVID-19. PVD means individual’s belief that they are susceptible to infectious diseases.6 Specifically speaking, individuals who perceive themselves as more vulnerable to the disease may feel higher risk in the outbreak, and then may experience higher anxiety levels; individuals who believe they are not susceptible to the disease, on the other hand, may feel lower risk in the outbreak; and then reduces anxiety levels.
When individuals face death threats, they induce strong fears. In the context of the COVID-19 outbreak, this death threat stems from individuals’ fear that they will be infected with the COVID-19. The terror management theory insists that receiving information related to death falls into a state of panic or anxiety.7,8 For individuals with lower PVD, they perceive themselves to have a lower probability of contracting the epidemic and therefore show a lower level of risk perception with fear. In contrast, for those individuals who perceive a higher vulnerability to the disease, they perceive themselves to have a high probability of contracting the COVID-19 and therefore perceive a higher risk and fear. Thus, PVD may positively influence an individual’s fear of COVID-19.9
Based on the fact that there is no specific drug for the COVID-19, the coronavirus epidemic is considered to coexist with humans for a long time, which means that humans may be in a dangerous situation for the COVID-19 for a long time. People have a strong fear of infection and death when an individual is in a dangerous situation for a long time or is unable to change the current situation.10,11 This may further lead to long-lasting anxiety and even negative emotions such as depression.12–14
Government management plays an important role in responding to public health safety incidents. At a time when the COVID-19 is ravaging the world, governments have successively taken a series of measures to curb the spread of the epidemic.15 Tough government management measures, such as home isolation, maintaining social distance, wearing masks and the like can minimize the infection rate of the public. These effective management measures will not only win the public trust in government, but also make the public feel safe to a large extent, and then reduce anxiety.
In the context of the epidemic, individuals with different degrees of PVD also showed significant differences in the risk perception of the COVID-19. It has been shown that higher risk perception can make individuals more dependent on the application of government measures.16 When individuals underestimate their probability of contracting the pandemic, they may believe that the government exaggerates the degree of risk, and thus feel dissatisfied with the government and its countermeasures; conversely, when the public feels higher risk and is consciously unable to change the current status, they will prefer to believe in the government and be willing to take the countermeasures proposed by the government to protect themselves.16
Studies have shown that information about outbreaks is an important factor in individuals’ perceived risk.17 For example, the public is more concerned about the government’s response in the epidemic, and when the government takes tough and effective defense measures, it will allow individuals to perceive a reduced risk, which in turn reduces individuals’ fear of the new crown virus. In contrast, when individuals show a higher fear of the coronavirus, it means that individuals still have a higher risk perception of the coronavirus, that is to say, individuals believe that the government response measures do not effectively control the spread of the coronavirus, and then reduce individuals’ trust in the government.
Since the outbreak of the COVID-19, the Chinese government has taken decisive and strict measures to control the spread of the epidemic. In this context, it is of great significance to study the effect of government management and fear of COVID-19 on individual mental health in group stress events from macro and micro perspectives. We proposed the research hypotheses based on the literature review:
Hypothesis: PVD is able to positively predict anxiety levels. Hypothesis: PVD could increase anxiety levels through the mediating effect of the fear of COVID-19. Hypothesis: PVD could decrease anxiety levels through the mediating effect of government management trust.
Hypothesis: Fear of COVID-19 and trust in the government play a chain mediation effect between the PVD and the anxiety level.
Methods
Participants
This cross-sectional study was conducted at Xinyang Normal University, Xinyang, China, from 19rd January to 15rd March 2021. The data and the informed consent were obtained via a web-based questionnaire. These questionnaires were published on the WJX web, a free online platform for collecting data (https://www.wjx.cn/). The researchers sent the questionnaire link to the subjects through email or WeChat and other chat tools, and encouraged the subjects to forward the link to other people. The person who received the questionnaire link can voluntarily choose whether to participate in this study. After completing the survey, each subject can participate in the lottery and get a reward of 2–10 RMB. The study complies with the Declaration of Helsinki. The research was approved by the human research ethics committee for non-clinical faculties of School of Educational Science, Xinyang Normal University (Approval Number: XYEC-2021-002). A total of 1085 subjects (160 males) were recruited to participate the present study. Their ages ranged from 18 to 65 years, with a mean of 20.24 years (SD = 3.97), which indicated that this study is representative of young adults only. The sample size was chosen based on the experience of previous similar studies.18,19 Inclusion criteria were the Chinese national who can read, understand and fill the questionnaire,20 whereas the subjects who failed the polygraph test were excluded from the study. The polygraph test is set up as a common sense test with a standard answer, ie the sun rises in the east and sets in the west, which can identify subjects who choose an answer without understanding the question. All subjects passed the polygraph test, so no subjects were excluded from the study.
Instruments
Fear of COVID-19 Scale (FCV-19)
It is a 7-item questionnaire intended to measure individual levels of fear of COVID-19, which was developed by Ahorsu et al.11 The items were rated on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). The higher score represents the higher fear level. Chi et al have confirmed that the Chinese version of FCV-19 has good psychometric properties in the Chinese communities.21 The Cronbach’s α was 0.89 in the present study.
Perceived Vulnerability to Disease Scale (PVD)
The PVD was consisted of 15 items, developed by Duncan et al.22 One of subscale is used to assess beliefs about one’s own susceptibility to infectious diseases (Perceived Infectability [PVD-PI] with 7 items). Such as “I am more susceptible to infectious diseases than the people around me”, and “I am less likely to get a cold, flu, or other illness, even if it’s ‘spreading around’ (reverse score).” Since the content measured in this subscale is more appropriate to the connotation of perceived disease susceptibility, this dimension is mainly used as the measurement tool of perceived vulnerability to disease. In addition, for brevity, the similar items in this dimension are removed, leaving five items. The items were rated on a 7-point Likert scale (1= “strongly disagree”, 7= “strongly agree”), the higher the score represents the individual feels susceptible to the disease. Yu et al have confirmed that the Chinese version of PVD has good psychometric properties in the Chinese communities.23 The Cronbach’s α was 0.82 in the present study.
Trust in the Government Scale (TGS)
This study adopts Trust in the Government Subscale of the Self-Efficacy and Trust in the Government Scale, which was compiled by Johnson et al.24 Trust in the Government was measured by “Politicians never tell us what they really think” (reverse coded), and “I don’t think public officials care much about what people like me think” (reverse coded). The items were rated on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). The Cronbach’s α was 0.72 in the present study.
Anxiety Scale
This study adopts the anxiety subscale of Depression-Anxiety-Stress Scale, which was translated into Chinese version by Gong et al and have been confirmed it’s good psychometric properties in the Chinese communities.25 This scale comprises 7 items, which were rated on a 4-point Likert scale (0=completely out of line, 3 = fully compliance). A mean score of all the items was computed as an index of overall feelings of anxiety and higher scores indicate higher levels of anxiety. The Cronbach’s α was 0.86 in the present study.
Statistical Analysis
Harman univariate test was conducted and showed that there was no serious common method bias in this study.26 Descriptive statistics and the correlation analysis were first conducted. PROCESS Models 6 macros for SPSS was used to test the serial mediation models with 5000 random sample bootstrapping confidence intervals (CIs).27 PVD, fear of COVID-19, trust in the government and anxiety were study variables, and the gender, age, education background and economic situation were used as the control variables. All variables were standardized prior to being analyzed.
Results
Descriptive Statistics and the Correlation Analysis
Table 1 shows the means, standard deviations, and correlations of the variables. PVD was found to be positively correlated with fear of COVID-19 (r = 0.15, p < 0.001), trust in the government (r = 0.11, p < 0.001) and anxiety (r = 0.09, p < 0.01); Fear of COVID-19 was positively correlated with anxiety (r = 0.30, p < 0.001) and negatively correlated with trust in the government (r = −0.19, p < 0.001); Anxiety negatively correlated with trust in the government (r = −0.23, p < 0.001).
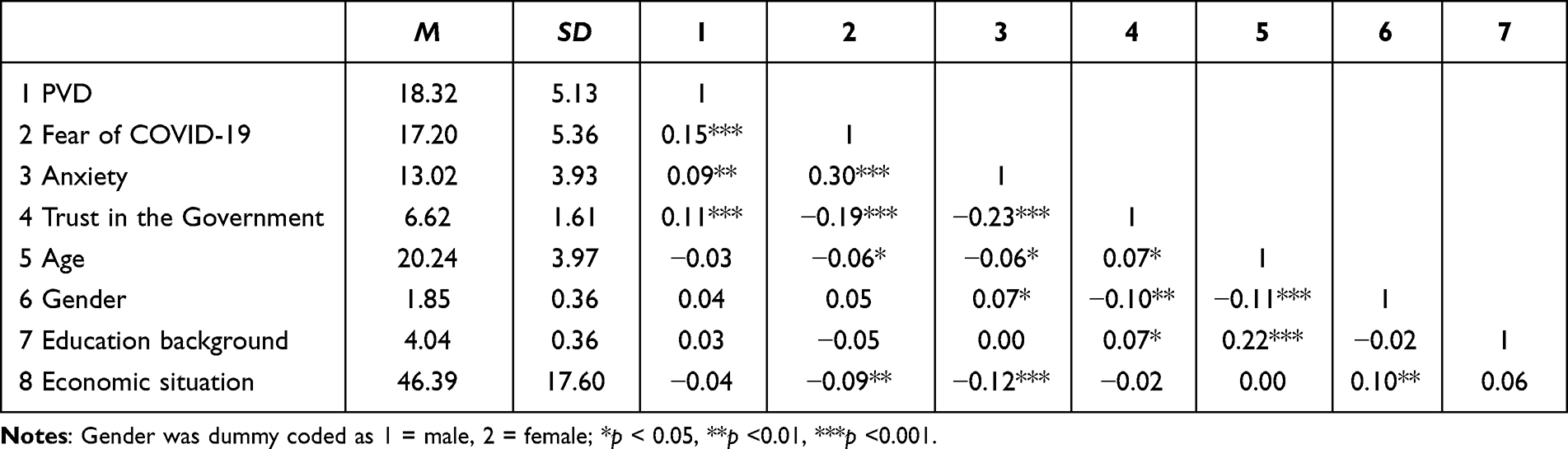 |
Table 1 Correlations Among the Variables (n = 1085) |
Testing for Mediation Effect
To test the serial mediating effect of fear of COVID-19 and trust in the government, 3 linear regression models were run by Model 6 of the PROCESS macro.27 To see if there are differences between gender, age, education background and economic situation, we used them as the control variables (see Figure 1).
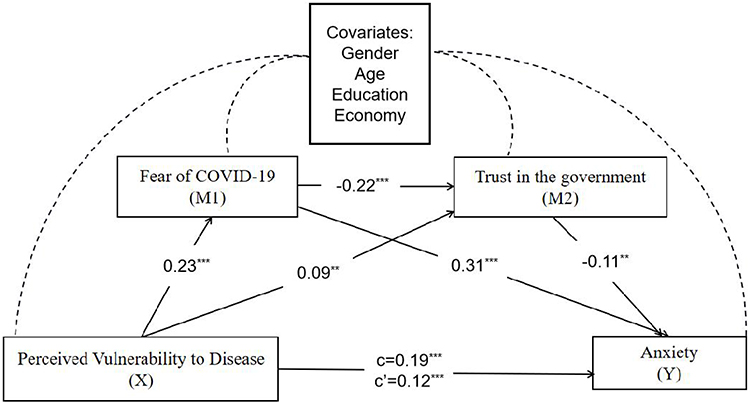 |
Figure 1 The serial mediation model. Notes: Genders, age, education background and economic situation were used as the control variables in the model. Gender was dummy coded as 1 = male, 2 = female; **p <0.01, ***p <0.001. |
As Table 2 shows, PVD significantly positively predicts fear of COVID-19 and trust in the government. Fear of COVID-19 significantly negatively predicted trust in the government; fear of COVID-19 significantly positively predicted anxiety; trust in the government significantly negatively predict anxiety. In addition, we found that females tended to show lower level of trust in the government compared to males, and more educated individuals show more trust in government. Individuals with better family economic conditions and older age tend to have lower levels of anxiety, while females seem to show higher levels of anxiety compared to males. After the addition of fear of COVID-19 and trust in the government as mediators, the predictive effect of PVD on anxiety remains significant. Accordingly, fear of COVID-19 and trust in the government could be in a partial intermediary role between PVD and anxiety. Further analysis reveals that this mediation effect contains three indirect effects: Indirect Effect 1, PVD→fear of COVID-19→anxiety (indirect effect = 0.07, SE = 0.01, 95% CI = [0.05, 0.10]); Indirect Effect 2, PVD→trust in the government→anxiety (indirect effect = −0.01, SE = 0.00, 95% CI = [−0.02, −0.00]); Indirect Effect 3, PVD→fear of COVID-19→trust in the government→anxiety (indirect effect = 0.01, SE = 0.00, 95% CI = [0.00, 0.01]). These results supported our given Hypotheses I–IV.
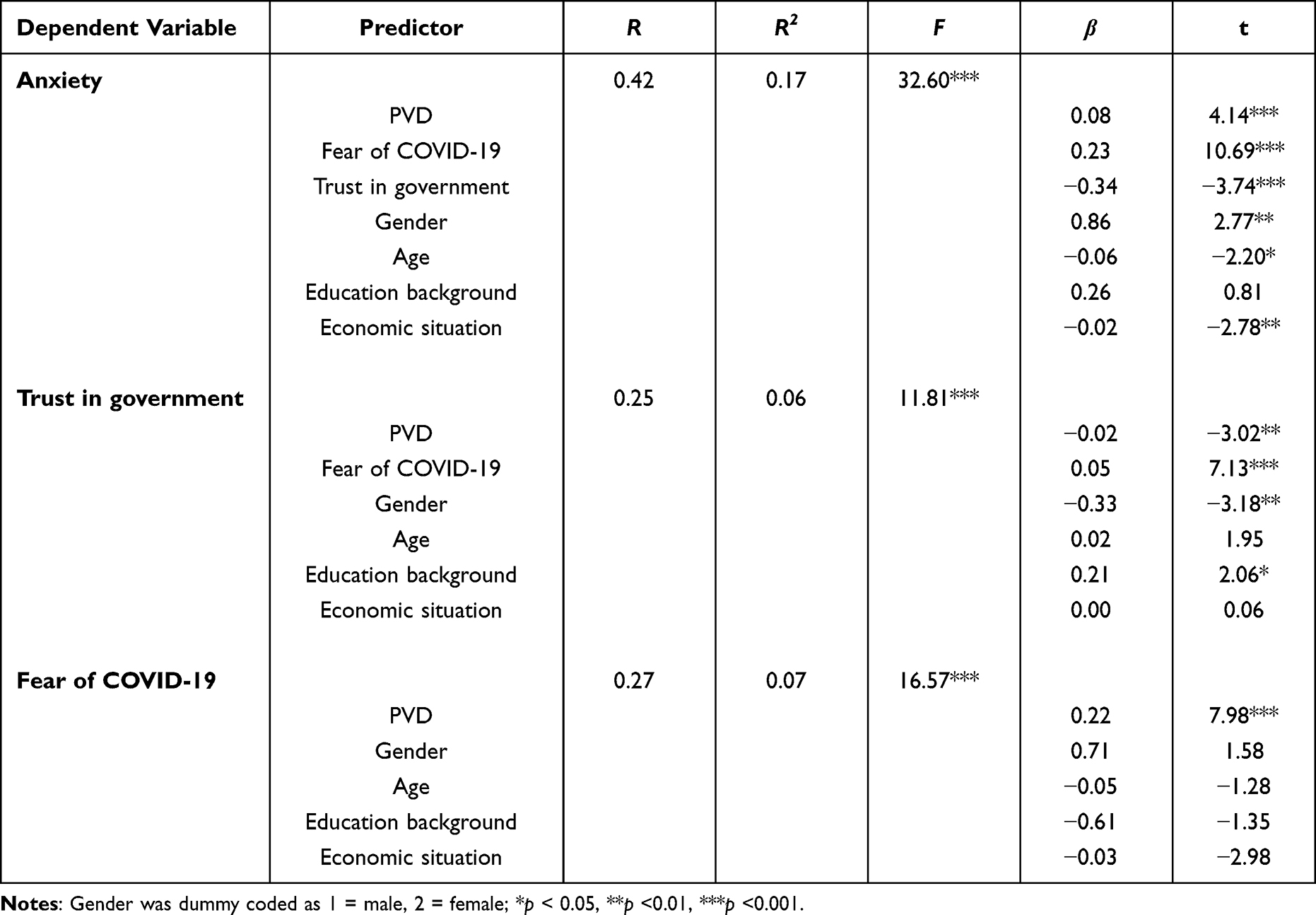 |
Table 2 Regression Analyses of Variables in Chain Mediation Model |
Discussion
This study aimed to explore the psychological mechanism by which perceived vulnerability to disease (PVD) affects anxiety levels in the context of COVID-19. The results showed that PVD can predict anxiety level through the mediating effect of fear of COVID-19 and trust in the government, and can also affect anxiety level through the chain mediation effect of fear of COVID-19 and trust in the government.
This study found that PVD can positively predict anxiety level, which is consistent with previous research results.28 Studies have shown that individual cognitive differences lead to differences in perceived disease risk.14 As a cognitive factor, PVD may change emotional states by influencing individual social cognition and corresponding behavioral responses.22 In the context of COVID-19, individuals with higher PVD may perceive COVID-19 as a stressful event with higher risk and thus experience higher levels of anxiety.29 Therefore, in the COVID-19 situation, we can try to reduce the anxiety level of the public by changing the individual’s cognitive level, such as the susceptibility to disease. We can also strengthen physical exercise and professional guidance to shape individuals’ awareness of their disease susceptibility before the COVID-19, so as to prevent serious anxiety when the COVID-19 comes.
In addition, fear of COVID-19 was found to mediate between PVD and anxiety in this study, suggesting that fear is an important factor in understanding PVD-induced anxiety. The possible explanation is that, according to the terror management theory, individuals will experience fear and anxiety when facing death threats.7,8 On the other hand, PVD may enhance individuals’ fear of COVID-19 by increasing the confirmed and uncontrollable information that COVID-19 is of “high risk” to them,30 thereby increasing the level of anxiety. On the other hand, PVD may induce anxiety by increasing the uncertainty of an individual’s infection, such as whether he or she can be cured.
Interestingly, this study found that trust in the government also played a mediating role between PVD and anxiety. This means that in the context of COVID-19, individuals with higher PVD are more likely to trust in the government. This may be because those individuals with higher PVD need to take measures to reduce their risk of infection, but cannot achieve this through their own strength and efforts, so they will rely more on and trust in the management measures of government. In contrast, for those individuals with low PVD, their perceived risk is low enough that no additional measures need to be taken and therefore do not increase their reliance on government regulation. This prediction is consistent with previous studies, which found that individuals who believe they are more susceptible to disease may pay more attention to COVID-19-related information, adhere more strictly to public safety measures, and rely more on the government.31 According to the social support theory, effective government management enables individuals to feel strong support and protection, which helps to improve their resilience to catastrophic events and plays a buffer role in alleviating psychological pain.32 The results suggest that timely release of effective response measures by the government can protect people’s mental health to a certain extent.
By the way, we found that females tended to show lower trust in the government and higher anxiety compared to males, which may be related to women having a higher susceptibility to anxiety.33,34 Meanwhile, we found that more educated individuals show more trust in government and whose with better family economic conditions and older age tend to have lower levels of anxiety. This may be because more educated individuals are more rational when faced with public stress events, and more willing to trust governments. At the same time, individuals with better family economic conditions can buffer the anxiety caused by the uncertainty of public stress events. An older age means they may have more experience, making their thinking more mature and rational, thus showing more confidence and courage when facing public stress events. These incidental findings suggest that females may have higher mental health risks in public stress events, and that increased educational level, improved family economic conditions, and increased life experience may reduce the mental health risks to some extent.
Although this study has some significant findings, there are still some limitations. First, the scales used in this study were developed by foreign researchers, among which the Fear of COVID-19 Scale, Trust in the Government Scale, and Perceived Vulnerability to Disease Scale have not yet been translated into Chinese versions. The current study is the first attempt to translate these scales into Chinese. Therefore, it is necessary to explore more suitable research tools in the future. Second, there was a serious gender imbalance in the sample of this study. Although gender was taken as a control variable in the analysis, it is necessary to explore whether there are gender differences in some psychological mechanisms in coping with COVID-19 in the future. Third, the study used the cross-sectional and self-reported measure to collect data. Cross-sectional research can obtain a large amount of data in a short period of time, but the research time span is so short that researcher cannot in-depth analyses other factors causing individual anxiety. Meanwhile, although self-reported measure has the advantages of strong operability, objective, comprehensive and self-diagnosis, the report stability is poor as individual anxiety levels changing over time. Hence the depth of our investigation will be limited to a certain extent. In the future research, we should employ various methods based on the cross-sequential design to comprehensively explore the relationship between perceived vulnerability to disease and anxiety level.
Conclusions
The study concludes that perceived vulnerability to disease could directly and indirectly predict anxiety level through the chain-mediated role of the fear of COVID-19 and the trust in the government measure. Specifically, the PVD, as a critical risk factor, was significantly and positively associated with fear of COVID-19 as well as negatively associated with trust in the government, which could predict the increased level of anxiety during the COVID-19 pandemic.
This study also analyzed and discussed the role of gender, age, education background and economic situation in the relationship between the PVD and anxiety during the COVID-19 pandemic. These findings are of great significance for formulating effective intervention programs to reduce people’s mental health risks in response to public stress events in the future, such as improving people’s education level, improving family economic conditions, and especially giving more attention and help to individual women.
Ethical Considerations
The study has received ethics approval from the Ethics Committee of Xinyang Normal University (Project no: XYEC-2021-002).
Funding
This work was supported by a grant from the National Natural Science Foundation of China (32200902), funding scheme for young core teachers of Xinyang Normal University (XYNU), Nanhu Scholars Program for Young Scholars of XYNU.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Brief P. COVID-19 and the Need for Action on Mental Health. World Health Organization; 2020.
2. Duong CD. The impact of fear and anxiety of Covid-19 on life satisfaction: psychological distress and sleep disturbance as mediators. Pers Individ Dif. 2021;178:110869. doi:10.1016/j.paid.2021.110869
3. Carr MJ, Steeg S, Webb RT, et al. Effects of the COVID-19 pandemic on primary care-recorded mental illness and self-harm episodes in the UK: a population-based cohort study. Lancet Public Health. 2021;6(2):e124–e135. doi:10.1016/S2468-2667(20)30288-7
4. Fountoulakis KN, Apostolidou MK, Atsiova MB, et al. Self-reported changes in anxiety, depression and suicidality during the COVID-19 lockdown in Greece. J Affect Disord. 2021;279:624–629. doi:10.1016/j.jad.2020.10.061
5. Wei-Peng HU. Comparative study on risk perception and coping behavior of Beijing residents during sars period. Chin J Clin Psychol. 2004;12(3):293–295.
6. Magallares A, Jauregui-Lobera I, Carbonero-Carreño R, Ruiz-Prieto I, Bolaños-Ríos P, Cano-Escoriaza A. Perceive vulnerability to disease and antifat attitudes in a sample of children and teenagers. Eat Weight Disord. 2015;20(4):483–489. doi:10.1007/s40519-015-0220-1
7. Pyszczynski T, Greenberg J, Solomon S. Why do we need what we need? A terror management perspective on the roots of human social motivation. Psychol Inq. 1997;8(1):1–20. doi:10.1207/s15327965pli0801_1
8. Weng ZG, Zhang RT, Song LZ. Terror management account of consumption behavior and group affiliation of people after catastrophe. China Soft Sci. 2011;01:181–192.
9. Schweda A. Phenotyping mental health: age, community size, and depression differently modulate covid-19-related fear and generalized anxiety. Compr Psychiatry. 2020;104:422–430.
10. Rossi A, Panzeri A, Pietrabissa G, Manzoni GM, Castelnuovo G, Mannarini S. The anxiety-buffer hypothesis in the time of COVID-19: when self-esteem protects from the impact of loneliness and fear on anxiety and depression. Front Psychol. 2020;11:2177. doi:10.3389/fpsyg.2020.02177
11. Ahorsu DK, Lin CY, Imani V, Saffari M, Griffiths MD, Pakpour AH. The fear of COVID-19 scale: development and initial validation. Int J Ment Health Addict. 2020;1:1–9.
12. Sakib N, Bhuiyan AI, Hossain S, et al. Psychometric validation of the bangla fear of COVID-19 scale: confirmatory factor analysis and rasch analysis. Int J Ment Health Addict. 2020;11:1–2.
13. Soraci P, Ferrari A, Abbiati FA, et al. Validation and psychometric evaluation of the Italian version of the fear of COVID-19 scale. Int J Ment Health Addict. 2020;4:1–10.
14. Silva WAD, de Sampaio Brito TR, Pereira CR. Anxiety associated with COVID-19 and concerns about death: impacts on psychological well-being. Pers Individ Dif. 2021;176:110772. doi:10.1016/j.paid.2021.110772
15. Hale T, Webster S, Petherick A, Phillips T, Kira B. Oxford COVID-19 government response tracker (OxCGRT). Last Updated. 2020;8:30.
16. Fragkaki I, Maciejewski DF, Weijman EL, Feltes J, Cima M. Human responses to Covid-19: the role of optimism bias, perceived severity, and anxiety. Pers Individ Dif. 2021;176:110781. doi:10.1016/j.paid.2021.110781
17. Faour-Klingbeil D, Osaili TM, Al-Nabulsi AA, Jemni M, Todd EC. The public perception of food and non-food related risks of infection and trust in the risk communication during COVID-19 crisis: a study on selected countries from the Arab region. Food Control. 2021;121:107617. doi:10.1016/j.foodcont.2020.107617
18. Li. X, Liu F, Li H. The impact of subjective socioeconomic status on well-being in early adulthood: a serial mediation model. Chin J Clin Psychol. 2022;30(04):802–807. doi:10.16128/j.cnki.1005-3611.2022.04.010
19. Yang L, Yang Z, Xia Y. Relationship between negative coping style and fear of COVID-19 among Wuhan college students during the post-pandemic period: a moderated chain mediation model. Front Psychiatry. 2022;13:994685. doi:10.3389/fpsyt.2022.994685
20. Rafique N, Al Tufaif F, Alhammali W, et al. The psychological impact of COVID-19 on residents of Saudi Arabia. Psychol Res Behav Manag. 2022;15:1221–1234. doi:10.2147/PRBM.S360772
21. Chi X, Chen S, Chen Y, et al. Psychometric evaluation of the fear of COVID-19 scale among Chinese population. Int J Ment Health Addict. 2022;20(2):1273–1288. doi:10.1007/s11469-020-00441-7
22. Duncan LA, Schaller M, Park JH. Perceived vulnerability to disease: development and validation of a 15-item self-report instrument. Pers Individ Dif. 2009;47(6):541–546. doi:10.1016/j.paid.2009.05.001
23. Yu X, Zhang Y, Zheng X. The influence and mechanism of optimism on college student’s health. J Guangxi Norm Univ. 2019;55(06):83–90. doi:10.16088/j.issn.1001-6597.2019.06.009
24. Johnson TJ, Kaye BK. In blog we trust? Deciphering credibility of components of the internet among politically interested internet users. Comput Human Behav. 2009;25(1):175–182. doi:10.1016/j.chb.2008.08.004
25. Gong X, Xie X, Xu R, Yuejia L. Psychometric properties of the Chinese versions of dass-21 in Chinese college students. Chin J Clin Psychol. 2010;18(4):443–446.
26. Hayes A. Introduction to mediation, moderation, and conditional process analysis. J Educ Meas. 2013;51(3):335–337.
27. Hao Z, Long L. Statistical remedies for common method biases. Adv Psychol Sci. 2004;12(6):942–950.
28. Campbell R, Walker J, Makhanova A, Vargas I. 655 the role of insomnia symptoms in the relation between perceived vulnerability to disease and COVID-19 anxiety. Sleep. 2021;44(Suppl 2):A256. doi:10.1093/sleep/zsab072.653
29. Shiina A, Niitsu T, Kobori O, et al. Perception of and anxiety about COVID-19 infection and risk behaviors for spreading infection: an international comparison. Ann Gen Psychiatry. 2021;20(1):1–11. doi:10.1186/s12991-021-00334-6
30. Karataş Z, Tagay Z. The relationships between resilience of the adults affected by the covid pandemic in Turkey and covid-19 fear, meaning in life, life satisfaction, intolerance of uncertainty and hope. Pers Individ Dif. 2021;172(3):110592. doi:10.1016/j.paid.2020.110592
31. De Coninck D, d’Haenens L, Matthijs K. Perceived vulnerability to disease and attitudes towards public health measures: COVID-19 in Flanders, Belgium. Pers Individ Differ. 2020;166:110220. doi:10.1016/j.paid.2020.110220
32. Cheung E. An outbreak of fear, rumours and stigma: psychosocial support for the ebola virus disease outbreak in West Africa. Intervention. 2015;13(1):70–76. doi:10.1097/WTF.0000000000000079
33. Yang Y, Zhao Y, Wang T, Zheng X Gender differences in sensitivity to different types of threat information. Chin J Clin Psychol. 2023;1:45–51+57.
34. Yang Y, Li J, Chen W, et al. Gender differences in fear memory acquisition and extinction and its neural mechanism. Psychol Sci. 2020;43(01):224–231. doi:10.16719/j.cnki.1671-6981.20200131
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Anxiety and Depression Among HIV-Positive and HIV-Negative Pregnant Women During COVID-19 Pandemic in Ekiti State, Southwest Nigeria
Ade-Ojo IP, Dada MU, Adeyanju TB
International Journal of General Medicine 2022, 15:4123-4130
Published Date: 16 April 2022
Spiritual Well-Being, Depression, Anxiety, and Stress in Indonesian Muslim Communities During COVID-19
Hamka, Suen MW, Ramadhan YA, Yusuf M, Wang JH
Psychology Research and Behavior Management 2022, 15:3013-3025
Published Date: 17 October 2022
Fear of COVID-19 and Anxiety: Serial Mediation by Trust in the Government and Hope
Yang Y, Wang H
Psychology Research and Behavior Management 2023, 16:963-970
Published Date: 24 March 2023
Psychological Resilience, Anxiety, and Well-Being of Health Care Providers During the COVID-19 Pandemic
AlQarni AM, Elfaki A, Abdel Wahab MM, Aljehani Y, ALKhunaizi AA, Othman SA, AlShamlan RA
Journal of Multidisciplinary Healthcare 2023, 16:1327-1335
Published Date: 12 May 2023
Digital Therapy: Alleviating Anxiety and Depression in Adolescent Students During COVID-19 Online Learning - A Scoping Review
Yosep I, Suryani S, Mediani HS, Mardhiyah A, Maulana I
Journal of Multidisciplinary Healthcare 2023, 16:1705-1719
Published Date: 21 June 2023