Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
The Relationship Between Level of Education, Cognitive Function and Medication Adherence in Patients with Schizophrenia
Authors Zhu X, Wen M, He Y, Feng J, Xu X, Liu J
Received 6 June 2023
Accepted for publication 21 September 2023
Published 15 November 2023 Volume 2023:19 Pages 2439—2450
DOI https://doi.org/10.2147/NDT.S424694
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Richard J Porter
Xiaodan Zhu,1 Min Wen,1 Ying He,1 Jing Feng,2 Xuebing Xu,2 Juan Liu3
1School of Nursing, Ningxia Medical University, Yinchuan, Ningxia, People’s Republic of China; 2Inpatient Department, Ningxia Mental Health Center, Ningxia Ning-An Hospital, Yinchuan, Ningxia, People’s Republic of China; 3General Hospital of Ningxia Medical University, Yinchuan, Ningxia, People’s Republic of China
Correspondence: Juan Liu, General Hospital of Ningxia Medical University, Shengli Road #804, Yinchuan, Ningxia, 750004, People’s Republic of China, Tel/Fax +86 09516744007, Email [email protected] Xuebing Xu, Ningxia Mental Health Center, Ningxia Ning-An hospital, Jingbo Road #236, Yinchuan, Ningxia, 750011, People’s Republic of China, Tel/Fax +86 09512160739, Email [email protected]
Purpose: Several studies have explored the relationship between level of education and medication adherence, as well as the relationship between level of education and cognitive function. However, there have been few studies on the relationships between level of education, cognitive function, and medication adherence. This study aimed to explore whether cognitive function has a mediating effect between level of education and medication adherence in patients with schizophrenia.
Patients and Methods: A total of 329 participants were included in this study. Cognitive function was assessed using the Brief Assessment of Cognition in Schizophrenia, and medication adherence using the Medication Adherence Questionnaire. The relationships between the clinical factors and cognitive function that contributed to medication adherence were tested through multivariable linear regression analysis. The mediating effect of medication adherence was tested using the bootstrapping approach with the PROCESS macro.
Results: Family history, insight and executive function were associated with medication adherence in individuals with schizophrenia, and executive function had a mediating effect between level of education and medication adherence.
Conclusion: Adopting specific education programs that promote cognitive development as well as actively intervening in executive function might be conducive to improve medication adherence in patients with schizophrenia.
Keywords: antipsychotic adherence, mediating effect, neurocognition, executive function, severe mental disorders
Introduction
Most individuals with schizophrenia receive long-term treatment with antipsychotic medication. However, approximately half of these individuals experience a relapse and have to be hospitalized due to poor medication adherence.1 These incidents are associated with poor functional outcomes and increased costs of care for those with schizophrenia.2 Therefore, clarifying the factors that affect medication adherence is crucial for formulating intervention programs and improving adherence. Insight, medication beliefs, knowledge gaps, types of antipsychotics, medication side effects, and psychiatric symptoms were identified as the key influencing factors of medication adherence.3,4 Although the aspects associated with medication adherence in patients with schizophrenia have been extensively studied, there is still very little known in respect of the relationship between the level of education, cognitive function and medication adherence.
Cognitive impairment is a key feature of schizophrenia, especially when we consider working memory, attention, executive function, verbal memory, processing speed, and verbal fluency.5 Medication adherence is defined as the extent to which the doses a patient takes, the methods of taking the medication and the intervening time periods between the taking of doses are consistent with the agreed recommendations of the prescribing medical practitioner.6 Currently, there have only been a few studies conducted that have assessed the relationship between cognitive function and medication adherence. The five studies we were able to locate used different measures, putative predictors of adherence and study designs, and obtained conflicting results. El-Missiry et al assessed 109 patients with schizophrenia using the Wechsler Adult Intelligence Scale (WAIS), Wechsler Memory Scale-Revised (WMS-R) and Wisconsin Card Sorting Test (WCST).7 Six months later the same patients were assessed using the Brief Adherence Rating Scale (BARS). The results indicated that the total performance intelligence quotient (IQ), verbal memory and executive function were associated with non-adherence to medication regimen. Robinson et al found that patients with first-episode schizophrenia who had poorer premorbid cognitive function were more likely to stop taking their antipsychotic medication and that better executive function decreased the likelihood that patients would discontinue maintenance medication after a first relapse.8 Jeste et al assessed 110 middle-aged and elderly patients with schizophrenia using the Medication Management Ability Assessment (MMAA) and Mattis’ Dementia Rating Scale (DRS), and found that global cognitive function, conceptualization and memory, were related to an individual’s capacity to comply with medication regimens.9 Jónsdóttir et al evaluated 166 outpatients with schizophrenia using a comprehensive neuropsychological test battery as well as blood samples and reported that there was no association between neurocognition and adherence behaviour.10 Brain et al evaluated 112 outpatients with schizophrenia and schizophrenia-like psychosis using a comprehensive neuropsychological test battery and a Medication Event Monitoring System for a period of 12 months and reported that there was no association between global cognitive function and non-adherence.11 Given the inconsistency of published data on the relationship between cognitive function and medication adherence, we submit that it is necessary to address this gap in the research in this area of study.
The level of education plays an important role in an individual’s life and is closely related to cognitive function and medication adherence. The neuroplasticity theory posits that the brain still has the capacity in adulthood to grow, evolve and undergo structural and functional changes in response to environmental stimulation and behaviour training.12 The number of years of formal education completed by an individual is positively correlated to their cognitive function throughout adulthood.13 The educational experience provides students with opportunities to develop “cognitive control” or the skills necessary for inhibiting inappropriate thoughts and actions in favour of those more appropriate to the task at hand.14,15 Training with cognitive tasks during educational attainment may lead to plasticity in prefrontal regions.16 However, individuals who have schizophrenia experience cognitive impairment at the onset of the disease and so most individuals with schizophrenia show poorer academic achievement and are less likely to enter higher education than their normal peers.17 Some studies have found that a patient’s level of education is associated with their medication adherence.18–20 Patients who exhibit poor medication adherence generally have higher incidence of relapse and readmissions, which may limit the patients’ opportunities to study further and obtain a higher level of education.21 A low education level is also a disadvantage as it may hinder understanding of the features of a certain medication and the treatment framework, and may even inhibit the establishment of a positive attitude toward medications, which may further affect a patient’s medication adherence.22
Cognitive development theory posits that human cognitive development is not only demonstrated by an increase in knowledge, but also in the growth and enhancement of the cognitive structure, and learning is associated with the improvement and development of this cognitive structure.23 This cognitive structure is formed in the earlier learning stages, and then transferred to the next stage for improvement and development. Therefore, we propose the theoretical framework that a higher level of education enhances an individual’s ability to respond to medication information stimulation by improving their cognitive function, and in turn this will increase medication adherence (See Figure 1). Based on this theoretical framework, this study proposes the hypothesis that a higher level of education enhances medication adherence by improving the cognitive functioning of schizophrenia patients. We propose that the ability of patients with schizophrenia to adhere to medication regimens depends on their cognitive ability to sort out, summarize and understand information relating to their medication, and learning is associated with the improvement and development of cognitive functioning.
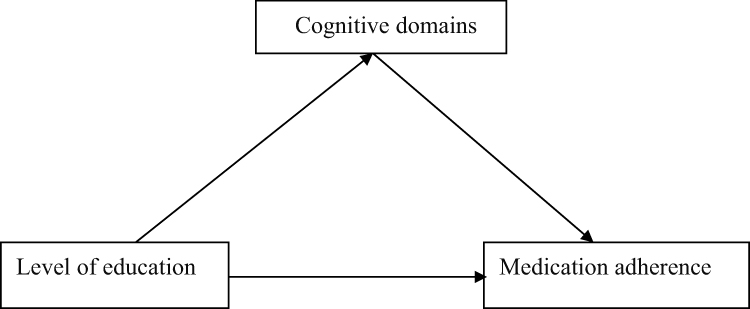 |
Figure 1 Theorized model of the relationship between level of education and medication adherence as mediated by cognitive domains. |
Although much research has been conducted on the relationship between level of education and medication adherence, as well as on the relationship between level of education and cognitive function, there have been few studies that have focused on the relationship between the three factors. This study aims to explore two major questions. First, we explored which cognitive domains affected medication adherence in patients with schizophrenia. Second, we investigated the mediating effect of the cognitive domains on level of education and medication adherence.
Materials and Methods
Participants
The possible participants of our study were 412 inpatients with schizophrenia at the Ningxia Mental Health Centre in Ningxia, China. The inclusion criteria were as follows: Participants 1) had to be between the ages of 18 and 60 years; 2) had to have a confirmed diagnosis of schizophrenia that has been rendered on the basis of a structured clinical interview in accordance with the International Classification of Diseases and Related Health Problems, 10th revision (ICD-10);24 3) had to be capable of completing the assessments, as measured by the Positive and Negative Syndrome Scale (PANSS), the degree of thinking disorder is less than severe (the scores of items P2, P3, P5 and G9 <6 points); 4) had to have received antipsychotic medication for at least six months prior to participation in the study. The exclusion criteria were as follows: 1) any mental retardation, organic central nervous system disorders, severe somatic disorders; 2) received modified electroconvulsive therapy (MECT) within 3 months prior to assessment in the study; 3) pregnant or lactating; 4) substance-related disorders.
Approximately 83 patients were excluded because they did not meet the inclusion criteria or they met the criteria for exclusion. Of these 30 patients did not meet the inclusion criteria (age: n=6; the scores of items P2, P3, P5 and G9 >6 points: n=16; antipsychotic medication for at less six months: n=8) and 18 patients met the exclusion criteria (severe somatic disorders: n=4; organic central nervous system disorders: n=3; substance-related disorders: n=4; received MECT within 3 months: n=5; pregnant or lactating: n=2). In addition, 35 patients who met the inclusion criteria refused to participate (see Figure 2). Finally, a total of 329 participants signed the informed consent form and agreed to take part in our study.
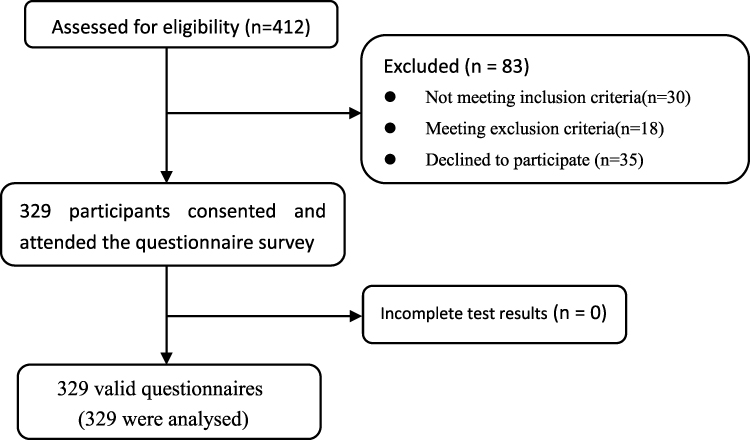 |
Figure 2 Sample flowchart. |
Measures
The Chinese version of the Brief Assessment of Cognition in Schizophrenia (BACS) was used to assess the participants’ cognitive function due to its high test-retest reliability, high internal consistency, acceptable concurrent validity, and good discriminant validity.25,26 The domains of cognition which were assessed included working memory, attention, executive function, verbal memory, motor speed, and verbal fluency. The following assessment tools were used: Digital Sequencing (DS) Test, Symbol Coding (SC), Tower of London (TL), Learning (LL) Test, Token Motor (TM) task, Category Instances, and Controlled Oral Word Association (COWA) test. Higher scores reflected better cognitive functioning in the corresponding dimensions.
The Medication Adherence Questionnaire (MAQ) was used to assess the participants’ medication adherence.27 The MAQ is a structured, self-reported medication adherence measure containing four items. The items are as follows: Item 1: Did you ever forget to take your medication? Item 2: Were you careless sometimes about taking your medicine? Item 3: Did you sometimes stop taking your medication when you felt better? Item 4: Did you sometimes stop taking your medication when you felt worse? The response for each item is scored as 1=yes or 2=no. Higher scores reflect better medication adherence.
The Positive and Negative Syndrome Scale (PANSS) was used to measure the participants’ symptom severity. It was utilized to evaluate positive symptoms, negative symptoms and general symptoms of schizophrenia.28 Both the positive and negative symptoms scales consist of seven items. The score for each item ranges from 1 to 7 points. Higher scores indicate that the participant is experiencing more severe symptoms.
The Insight and Treatment Attitudes Questionnaire (ITAQ) was used to assess the insight of individuals with schizophrenia.29 This assessment tool was developed to measure a patient’s awareness of their illness and attitude towards treatment. The ITAQ consists of 11 items which are rated on a scale ranging from 0 to 2. Higher scores reflect greater insight.
Data pertaining to the sociodemographic characteristics of the participants (such as age, gender, occupation and level of education), the onset and progression of the disease, family history of schizophrenia, dose of antipsychotic medication, types of antipsychotics, as well as history of tobacco smoking were obtained from the participants’ medical records. The participants’ level of education was calculated by adding the number of years they spent receiving a formal education. Limited by the national medical insurance policy, all the participants in this study were from the same administrative region, which adopts the same education system.
According to the records of medication side effects in the participants’ medical records, the occurrence of serious effects on function of body or serious complications more than once a week was defined as key medication side effects (See Supplementary Table 1). According to the World Health Organization Framework Convention on Tobacco Control (WHO FCTC),30 we defined smokers as those individuals who smoked more than four cigarettes per week continuously or cumulatively for more than six months.
Procedures
The participants were inpatients who were recently admitted to the hospital. To minimize the impact of in-hospital treatment and symptoms during the acute phase on our assessments, the patients were evaluated by a psychiatrist and two psychologists during the second week after their admission.
Patients’ assessments were conducted in a quiet room following a fixed sequence of events. First, individuals were identified as potential participants by a psychiatrist, and they signed the informed consent form before completing the questionnaire survey. Then, the participants’ psychiatric symptoms and insight were assessed by a psychiatrist by way of face-to-face interviews. Finally, the participants completed the MAQ, and their cognitive function was assessed by two psychologists based paper-pencil. The Pearson correlation coefficient was used to measure the inter-rater reliability (r=0.92).
The psychiatrist received training on inclusion and exclusion criteria, evaluation order, and assessment methods for PANSS and ITAQ prior to the start of the study. Two psychologists received training on evaluation order as well as assessment methods for MAQ and BACS prior to the start of the study.
Statistical Analyses
We performed descriptive statistical analysis to describe the sample characteristics of the participants, categorical variables were described as percentages and quantitative variables as mean ± standard deviation (SD). Multivariable linear regression analysis was used to analyse possible correlations among the sociodemographic characteristics, clinical factors, cognitive function and medication adherence. Based on the previous studies on the influencing factors of medication adherence in patients with schizophrenia and the theoretical framework of this study,3,4,31 the following variables: age, sex, family history, duration of disease, level of education, tobacco smoking, dose of antipsychotic medication, types of antipsychotics, medication side effects, PANSS scores, occupation, insight and each domain in BACS were set as the independent variables after discussion by a group of experts. Medication adherence was set as the dependent variable. The independent variable sex was assigned as “male =0”, “female =1”; family history was assigned as “no =0”, “yes =1”; medication side effects was assigned as “no =0”, “yes =1”; the dummy variable of type of antipsychotics was assigned as first generation antipsychotics+second generation antipsychotics (FGA+SGA): “SGA=0”, “FGA+SGA=1”, “SGA+SGA=0” and second generation antipsychotics+second generation antipsychotics (SGA+SGA): “SGA=0”, “FGA+SGA=0”, “SGA+SGA=1”; tobacco smoking was assigned as “no =0”, “yes =1”; occupation was assigned as blue-collar work: “unemployed=0”, “blue-collar work=1”, “white-collar work=0” and white-collar work: “unemployed=0”, “blue-collar work=0”, “white-collar work=1”.
The results of collinearity diagnostics showed that the variance inflation factor (VIF) for all independent variables was between 1 and 2. As the multiple linear regression analysis indicated a significant correlation between executive function and medication adherence, the mediating role of executive function was explored further. Spearman correlation analysis was used to analyse the relationships between level of education, executive function and medication adherence. These two steps were performed using SPSS.32
A bootstrapping approach with the PROCESS macro for SPSS was used to analyse the mediating effect of executive function on level of education and medication adherence in individuals with schizophrenia.33 A bootstrap sampling procedure was used to determine the significance of indirect effects.34 The bootstrapping procedure used generated 5000 samplings from the original data set (N = 329) by random sampling that made it possible to obtain 95% bias-corrected confidence intervals (BcCI), which indicate the existence of a significant indirect effect in the case of not containing the zero. Level of education was set as the independent variable, medication adherence was set as the outcome variable, and executive function was set as the mediation variable. Based on the results of multivariable linear regression analysis and previous studies,3,4,31 age, family history, insight, dosage of antipsychotics, types of antipsychotics, medication side effects, psychiatric symptoms were also included as covariates in the analysis of mediation effect. In our analyses, we used a 95% confidence interval (CI).
Results
Sample Characteristics
In our study we analysed data collected from 329 adults with schizophrenia; 160 participants were male (48.6%) and 169 were female (51.4%). The average age was 33.42 years old (SD = 9.36), the average course of disease was 9.76 years (SD = 7.25), the average level of education was 11.55 years (SD = 3.12), and medication adherence was medium, with an average score of 5.91 (SD = 1.34). The descriptive statistics of the cognitive function and clinical variables of the participants are presented in Table 1.
 |
Table 1 Demographic and Assessment Results of Patients with Schizophrenia (N = 329) |
Potential Covariates
The results of the regression analysis detected correlations among age, family history, insight and medication adherence. However, there were no significant correlations among sex, duration of disease, dosage of antipsychotics, types of antipsychotics, medication side effects, psychiatric symptoms, tobacco smoking, occupation, level of education, verbal memory, working memory, attention, motor speed, verbal fluency, and medication adherence (See Table 2). Thus, age, family history and insight were also included as covariates in the analysis of mediation effect.
 |
Table 2 Multiple Regression Analysis of the Cognitive Function with Medication Adherence in Patients with Schizophrenia |
The Correlation Between Cognitive Function and Medication Adherence
The results of the regression analysis detected correlations between executive function and medication adherence. However, there were no significant correlations among verbal memory, working memory, attention, motor speed, verbal fluency, and medication adherence (see Table 2).
The Correlation Between Level of Education, Medication Adherence and Executive Function
As indicated in Table 3, our results showed that level of education (r = 0.286, p < 0.01) was positively associated with executive function, and medication adherence (r = 0.183, p < 0.01). Executive function was also positively associated with medication adherence (r = 0.270, p < 0.01).
 |
Table 3 Correlation Analysis of Level of Education, Medication Adherence and Executive Function |
The Mediating Effect of Executive Function on the Relationship Between Level of Education and Medication Adherence
Table 4 and Figure 3 present the bootstrap results of the mediating effect of executive function on the relationship between level of education and adherence to medication regimen. As shown in Table 4 and Figure 3a, the level of education was associated with medication adherence (β = 0.069, 95% [0.022, 0.116]). As shown in Table 4 and Figure 3b, the indirect effect (β = 0.021, 95% [0.009, 0.042]) was significant, accounting for 30.43% of the total effect. The level of education - executive function path (β = 0.353, 95% [0.204, 0.502]) and the executive function - medication adherence path (β = 0.062, 95% [0.029, 0.094]) were significant. When introducing executive function as a mediator, the direct effect for level of education - medication adherence path (β =0.048, 95% [0.001, 0.095]) was also significant, accounting for 69.57% of the total effect, indicating partial mediation of executive function on level of education and medication adherence.
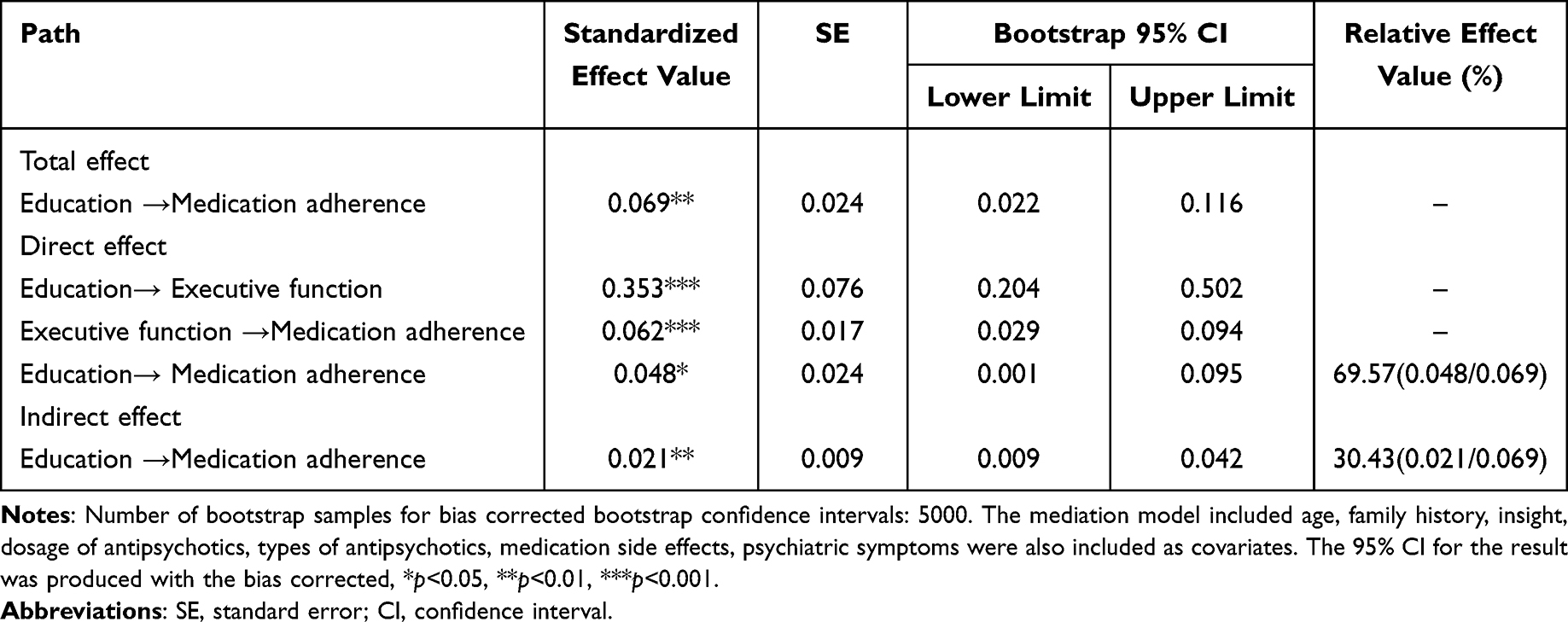 |
Table 4 Mediation Effect of Executive Function on the Relationship Between Level of Education and Medication Adherence (N=329) |
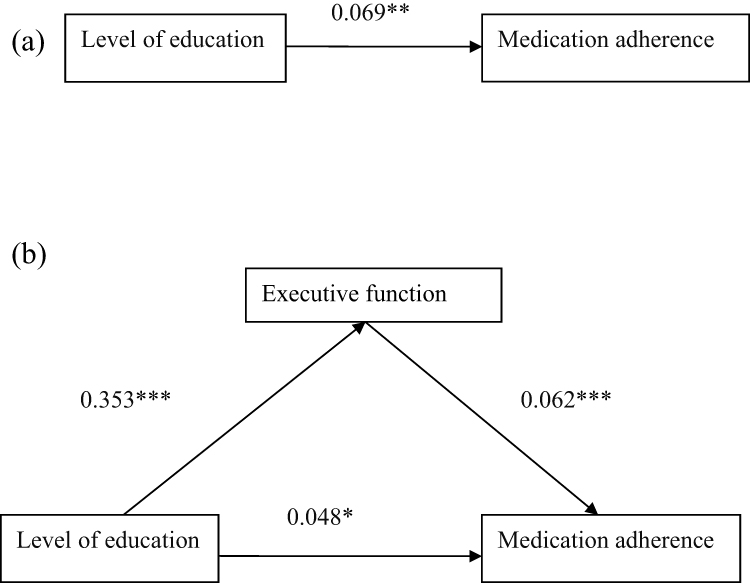 |
Figure 3 A mediation model of the role of executive function in the relationship between level of education and medication adherence in patients with schizophrenia. Notes: (a) The total effect (level of education predicting medication adherence). (b) The indirect effect (with executive function as mediator), effect value=0.021**. The mediation model included age, family history, insight, dosage of antipsychotics, types of antipsychotics, medication side effects, psychiatric symptoms were also included as covariates. *p<0.05, **p<0.01, ***p<0.001. |
Discussion
Most of the studies already published on this topic only explored the influence of cognitive function on medication adherence in individuals with schizophrenia.7,35 Some studies have suggested that higher cognitive function may be required to maintain adherence to treatment plans and medication schedules.36,37 However, few studies have investigated the relationship between level of education, cognitive function and medication adherence in patients with schizophrenia. Our results contribute to the reasoning that executive functioning and level of education may play an essential role in the medication adherence. More importantly, our findings filled a gap in the existing literature in terms of the mediating effect of executive function, which might be crucial to improving medication adherence and determining intervention targets.
Our results indicate that executive function is positively associated with medication adherence, which is consistent with the findings in previous studies.38,39 Executive functioning is a set of cognitive processes, including attentional control, cognitive inhibition, and cognitive flexibility, which are necessary for selecting and successfully monitoring behaviours to achieve chosen goals.40 Previous studies have indicated that executive function plays an important role in patients’ ability to manage complex medication regimens and was an important factor in individual motivations for medication adherence.8 However, no cognitive domains, such as memory or attention, other than executive function were associated with medication adherence. This inconsistency may be due to the heterogeneity in the participants, the methods used to measure medication adherence and cognitive function, or the study design.9,41
The results also showed that level of education was positively related to executive function.42,43 The development of individual intelligence is the result of the combined effect of innate and acquired factors according to the cognitive development theory.44 Although subtle cognitive deficits in childhood and adolescence of individuals with schizophrenia prior to the onset of psychosis may lead to lower academic achievements,45 the organisational structure of cognition can still be gradually formed during children’s acquired learning activities.46 Training in attentional control, verbal learning and memory, as well as cognitive flexibility and problem solving during the education process may contribute to an improvement in executive functioning for individuals with schizophrenia, and patients with better executive functioning may have access to higher levels of education.
We submit that our findings that level of education was not related to medication adherence in multivariable regression analyses, whereas it was related to medication adherence in the correlation analyses was quite peculiar. A possible reason for this contradictory outcome is that level of education is not the only factor associated with medication adherence; there are other factors linked to medication adherence, such as executive function, family history and insight. These findings are consistent with the results of previous studies.4,38 It is possible that patients with good insight may be more likely to be compliant with their mental healthcare practitioner’s plan and to adhere to their medication treatment as prescribed.47 The complex interactions among these factors influences medication adherence in patients with schizophrenia. As we have proposed in this study, the cognitive domains may have a mediating effect of level of education and medication adherence. Based on these findings and previous studies,3,4 age, family history, insight, dosage of antipsychotics, types of antipsychotics, medication side effects, and psychiatric symptoms were included as covariates in the mediation model.
The analysis of the mediating effect indicated that the participants’ executive functioning played a partial mediating role on the relationship between level of education and medication adherence. Considering the three variables are intercorrelated, we further tested a mediation model with executive functioning as an independent variable and level of education as a mediation variable. We found that the indirect effect with level of education as mediation variable was significant (See Supplementary Table 2), indicating the mediation model with level of education as a mediation variable may be valid.
Partial mediation of this model revealed that level of education was not only directly related to medication adherence, but also indirectly affected medication adherence through the mediating effect of executive function. It has been found that patients with a low level of education often have a worse understanding of the treatment framework and have less access to health care knowledge, which is not conducive to the improvement of medication adherence for these patients.48 In addition, patients with a low education level often earn less, have less access to health care resources, have worse living conditions, and face more stressful life events. None of these factors are conducive to improving access to medical resources, motivation to adhere to treatment, and treatment attitude for patients with low education level.49 Poor executive functioning can lead to worse formal thought disorder and worse daily functioning capability, which are not conducive to improving the medication adherence.50,51 This study suggested that the individualization of comprehensive interventions should be adopted to improve medication adherence among patients with schizophrenia. Such interventions include cognitive remediation therapy to improve neurocognitive abilities and specific education programmers.52,53
This study is not without limitations. First, as a cross-sectional study, it was impossible to imply any causal relationship. Second, as we used self-administered questionnaires, there might be bias in the participants’ reporting. However, to minimize recall bias and reporting bias, we compared MAQ results with the information relating to the participants’ medication in their medical records. When the MAQ results were inconsistent with the medical records, the participant’s attending psychiatrist communicated this with his or her guardian and obtained the correct information. Third, readmitted participants tended to demonstrate worse medication adherence than other participants, which may induce bias. However, we submit that our relatively large sample size would have reduced this bias to some extent as participants would have had various reasons for being readmitted, not only medication non-adherence. Finally, cognitive function was assessed during the acute phase. Some longitudinal studies showed that cognitive functioning, including executive functioning, can be altered with the change of symptoms in patients with schizophrenia over time.54–57 However, studies that attempted to separate cognitive impairment present during active periods versus the persistent cognitive deficits in symptomatic remission have remained scarce. The available evidence is indicative of severe attentional impairments during active periods and during symptomatic remission, but show decreasing demands on attentional effort during active periods.58 While attention, working memory, and executive function imply separable systems, executive control is realized through an integration of selective attention and working memory in the service of behavioural goals.59,60 Thus, psychosis or illness severity is a confounder for executive function and medication adherence and these were included as covariates in the mediational analyses. To address these limitations, we suggest that future research should adopt a longitudinal research design and multi-method data acquisition strategies to decrease the possibility of bias.
Conclusions
We found positive correlations between level of education, executive function, and adherence to medication regimen, while executive function was found to partially mediate the relationship between level of education and medication adherence. We submit that the goal of improving medication adherence may be achieved through cognitive remediation therapy as well as specific education programmers that promote cognitive development in patients with schizophrenia.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of the Ningxia Medical University (No: 2021-N0011). All procedures were performed in accordance with the latest version of the Declaration of Helsinki. All participants and their guardians provided written informed consent prior to enrolment in the study.
Author Statement
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by the Natural Science Foundation Projects of Ningxia (grant number 2022AAC03164), the Key R & D Projects of Ningxia (grant number 2019BFG02023).
Disclosure
The authors declare that they have no competing interests.
References
1. Kikkert MJ, Dekker J. Medication Adherence Decisions in Patients With Schizophrenia. Primary Care Companion CNS Disorders. 2017;19(6). doi:10.4088/PCC.17n02182
2. Predmore ZS, Mattke S, Horvitz-Lennon M. Improving antipsychotic adherence among patients with schizophrenia: savings for states. Psychiatr Serv. 2015;66(4):343–345.
3. Tham XC, Xie HT, Chng CML, Seah XY, Lopez V, Klainin-Yobas P. Factors Affecting Medication Adherence Among Adults with Schizophrenia: a Literature Review. Arch Psychiatr Nurs. 2016;30(6):797–809.
4. Higashi K, Medic G, Littlewood KJ, Diez T, Granström O, De Hert M. Medication adherence in schizophrenia: factors influencing adherence and consequences of nonadherence, a systematic literature review. Adv Psychopharmacol. 2013;3(4):200–218.
5. McCleery A, Green MF, Hellemann GS, et al. Latent structure of cognition in schizophrenia: a confirmatory factor analysis of the MATRICS Consensus Cognitive Battery (MCCB). Psychol Med. 2015;45(12):2657–2666.
6. World Health Organization. Adherence to long term therapies: evidence for action. World Health Organization; 2003.
7. El-Missiry A, Elbatrawy A, El Missiry M, Moneim DA, Ali R, Essawy H. Comparing cognitive functions in medication adherent and non-adherent patients with schizophrenia. J Psychiatr Res. 2015;70:106–112.
8. Robinson DG, Woerner MG, Alvir J, Bilder RM, Hinrichsen GA, Lieberman JA. Predictors of medication discontinuation by patients with first-episode schizophrenia and schizoaffective disorder. Schizophr Res. 2002;57(2–3):209–219.
9. Jeste SD, Patterson TL, Palmer BW, Dolder CR, Goldman S, Jeste DV. Cognitive predictors of medication adherence among middle-aged and older outpatients with schizophrenia. Schizophr Res. 2003;63(1–2):49–58.
10. Jónsdóttir H, Opjordsmoen S, Birkenaes AB, et al. Predictors of medication adherence in patients with schizophrenia and bipolar disorder. Acta Psychiatr Scand. 2013;127(1):23–33. doi:10.1111/j.1600-0447.2012.01911.x
11. Brain C, Allerby K, Sameby B, et al. Drug attitude and other predictors of medication adherence in schizophrenia: 12 months of electronic monitoring (MEMS (R)) in the Swedish COAST-study. Eur Neuropsychopharmacol. 2013;23(12):1754–1762.
12. Sur M, Leamey CA. Development and plasticity of cortical areas and networks. Nat Rev Neurosci. 2001;2(4):251–262.
13. Lvdén M, Fratiglioni L, Glymour MM, Lindenberger U, Tucker-Drob EM. Education and cognitive functioning across the life span. Psychol Sci Public Interest. 2020;21(1):6–41.
14. Van der Elst W, Van Boxtel MPJ, Van Breukelen GJP, Jolles J. The Stroop color-word test: influence of age, sex, and education; and normative data for a large sample across the adult age range. Assessment. 2006;13(1):62–79.
15. Liston C, Cohen MM, Teslovich T, Levenson D, Casey BJ. Atypical prefrontal connectivity in attention-deficit/hyperactivity disorder: pathway to disease or pathological end point? Biol Psychiatry. 2011;69(12):1168–1177.
16. Springer MV, McIntosh AR, Winocur G, Grady CL. The relation between brain activity during memory tasks and years of education in young and older adults. Neuropsychology. 2005;19(2):181–192.
17. Dickson H, Hedges EP, Ma SY, et al. Academic achievement and schizophrenia: a systematic meta-analysis. Psychol Med. 2020;50(12):1949–1965.
18. Hudson TJ, Owen RR, Thrush CR, et al. A pilot study of barriers to medication adherence in schizophrenia. J Clin Psychiatry. 2004;65(2):211–216.
19. Acosta FJ, Bosch E, Sarmiento G, Juanes N, Caballero-Hidalgo A, Mayans T. Evaluation of noncompliance in schizophrenia patients using electronic monitoring (MEMS) and its relationship to sociodemographic, clinical and psychopathological variables. Schizophr Res. 2009;107(2–3):213–217.
20. Aldebot S, de Mamani AGW. Denial and acceptance coping styles and medication adherence in schizophrenia. J Nerv Men Dis. 2009;197(8):580–584.
21. Novick D, Haro JM, Suarez D, Perez V, Dittmann RW, Haddad PM. Predictors and clinical consequences of non-adherence with antipsychotic medication in the outpatient treatment of schizophrenia. PSYCHIAT RES. 2009;176(2–3):109–113.
22. Lemay J, Waheedi M, Al-Sharqawi S, Bayoud T. Medication adherence in chronic illness: do beliefs about medications play a role? Patient Prefer Adherence. 2018;12:1687–1698.
23. Neisser U, Boodoo G, Bouchard TJ, et al. Intelligence: knowns and unknowns. Am Psychol. 1996;51:77–101.
24. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59:S22–S33.
25. Wang LJ, Lin PY. Validation of the Chinese version of Brief Assessment of Cognition in Schizophrenia. Neuropsychiatr Dis Treat. 2016;12:2819–2826.
26. Keefe RSE, Goldberg TE, Harvey PD, Gold JM, Poe MP. The Brief Assessment of Cognition in Schizophrenia: reliability, sensitivity, and comparison with a standard neurocognitive battery. Schizophr Res. 2004;68(2–3):283–297.
27. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67–74.
28. Khan A, Yavorsky C, Liechti S, et al. A rasch model to test the cross-cultural validity in the positive and negative syndrome scale (PANSS) across six geo-cultural groups. BMC Psychol. 2013;1(1):5.
29. McEvoy JP, Freter S, Everett G, et al. Insight and the clinical outcome of schizophrenic patients. J Nerv Ment Dis. 1989;177(1):48–51.
30. Xiao D, Bai CX, Chen ZM, Wang C. Implementation of the World Health Organization Framework Convention on Tobacco Control in China: an arduous and long-term task. Cancer. 2015;121:S3061–S3068.
31. Zhao JP, Shi SX. Guidelines for Prevention and Treatment of Schizophrenia. Beijing: Chinese Medical Multimedia Press; 2015.
32. IBM Corporation. IBM SPSS Statistics for Windows. Version 20.0. New York: Armonk; 2011.
33. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. New York: Guilford Press; 2013.
34. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40(3):879–891.
35. Maeda K, Kasai K, Watanabe A, Henomatsu K, Rogers MA, Kato N. Effect of subjective reasoning and neurocognition on medication adherence for persons with schizophrenia. Psychiatr Serv. 2006;57(8):1203–1205.
36. Raskin SA, Maye J, Rogers A, Correll D, Zamroziewicz M, Kurtz M. Prospective memory in schizophrenia: relationship to medication management skills, neurocognition, and symptoms in individuals with schizophrenia. Neuropsychology. 2014;28(3):359–365.
37. Bowie CR, Harvey PD. Cognitive deficits and functional outcome in schizophrenia. Neuropsychiatr Dis Treat. 2006;2(4):531–536.
38. Na E, Yim SJ, Lee JN, et al. Relationships among medication adherence, insight, and neurocognition in chronic schizophrenia. Psychiatry Clin Neurosci. 2015;69(5):298–304.
39. Nuechterlein KH, Ventura J, Subotnik KL, Bartzokis G. The early longitudinal course of cognitive deficits in schizophrenia. J Clin Psychiatry. 2014;75:S25–S29.
40. Diamond A. Executive functions. Annu Rev Psychol. 2013;64:135–168.
41. Settem VVJ, Karanadi H, Praharaj SK. Cognitive deficits, depressive symptoms, insight, and medication adherence in remitted patients with schizophrenia. Indian J Psychiatry. 2019;61(4):335–341.
42. Huizinga M, Baeyens D, Burack JA. Editorial: executive Function and Education. Front Psychol. 2018;9:1357.
43. Shanmugan S, Satterthwaite TD. Neural markers of the development of executive function: relevance for education. Curr Opin Behav Sci. 2016;10:7–13.
44. Papalia DE, Olds SW, Fieldman RD. Human Development. Jakarta: Salemba Humanika; 2008.
45. Mollon J, Reichenberg A. Cognitive development prior to onset of psychosis. Psychol Med. 2018;48(3):392–403.
46. Zacharopoulos G, Sella F, Kadosh RC. The impact of a lack of mathematical education on brain development and future attainment. Proce National Acad Sci. 2021;118(24):e2013155118.
47. Deng MJ, Zhai SY, Ouyang X, Liu ZN, Ross B. Factors influencing medication adherence among patients with severe mental disorders from the perspective of mental health professionals. BMC Psychiatry. 2022;22:22.
48. Dharmapuri S, Best D, Kind T, Silber TJ, Simpson P, D’Angelo L. Health Literacy and Medication Adherence in Adolescents. J Pediatrics. 2015;166(2):378–382.
49. Lacro JP, Dunn LB, Dolder CR, Leckband SG, Jeste DV. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. 2002;63(10):892–909.
50. Xu JQ, Hui CLM, Longenecker J, et al. Executive function as predictors of persistent thought disorder in first-episode schizophrenia: a one-year follow-up study. Schizophr Res. 2014;159(2–3):465–470.
51. Iampietro M, Giovannetti T, Drabick DAG, Kessler RK. Empirically defined patterns of executive function deficits in schizophrenia and their relation to everyday functioning: a person-centered approach. Clin Neuropsychol. 2012;26(7):1166–1185.
52. Penadés R, Catalán R, Salamero M, et al. Cognitive Remediation Therapy for outpatients with chronic schizophrenia: a controlled and randomized study. Schizophr Res. 2006;87(1–3):323–331.
53. Nuechterlein KH, Subotnik KL, Turner LR, Ventura J, Becker DR, Drake RE. Individual placement and support for individuals with recent-onset schizophrenia: integrating supported education and supported employment. Psychiatr Rehabil J. 2008;31(4):340–349.
54. Gold S, Arndt S, Nopoulos P, O’Leary DS, Andreasen NC. Longitudinal Study of Cognitive Function in First-Episode and Recent-Onset Schizophrenia. Am J Psychiatry. 1999;156(9):1342–1348.
55. Harvey PD, Green MF, Bowie C, Loebel A. The dimensions of clinical and cognitive change in schizophrenia: evidence for Independence of improvements. Psychopharmacology. 2006;187(3):356–363.
56. Hughes C, Kumari V, Soni W, et al. Longitudinal study of symptoms and cognitive function in chronic schizophrenia. Schizophr Res. 2003;59(2–3):137–146.
57. Fett AKJ, Velthorst E, Reichenberg A, et al. Long-term Changes in Cognitive Functioning in Individuals With Psychotic Disorders: findings From the Suffolk County Mental Health Project. JAMA Psychiatry. 2020;77(4):387–396.
58. Sarter M, Martinez V, Kozak R. A neurocognitive animal model dissociating between acute illness and remission periods of schizophrenia. Psychopharmacology. 2009;202(1–3):237–258.
59. Gold JM, Robinson B, Leonard CJ, et al. Selective Attention, Working Memory, and Executive Function as Potential Independent Sources of Cognitive Dysfunction in Schizophrenia. Schizophr Bull. 2018;44(6):1227–1234.
60. Lesh TA, Niendam TA, Minzenberg MJ, Carter CS. Cognitive control deficits in schizophrenia: mechanisms and meaning. Neuropsychopharmacology. 2011;36(1):316–338.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.