Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
The Relationship Between Communicative Health Literacy and Patient Loyalty in China: A Chain Mediation Study Based on Social Exchange Theory
Authors Chen Y, He Y, Zhao S, Wu S, Zhou J, Hu L, Lu R ![]()
Received 29 September 2025
Accepted for publication 20 December 2025
Published 14 January 2026 Volume 2026:19 557014
DOI https://doi.org/10.2147/JMDH.S557014
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jacqueline Dunbar-Jacob
Yang Chen,1,* Yijia He,1,* Shenyu Zhao,2 Siyuan Wu,3 Jing Zhou,1 Lingmin Hu,1 Renjie Lu2,4
1Changzhou Maternal and Child Health Care Hospital, Changzhou Medical Center, Nanjing Medical University, Changzhou, Jiangsu, 213000, People’s Republic of China; 2The Affiliated Changzhou Hospital of Xuzhou Medical University, Changzhou Third People’s Hospital, Changzhou, Jiangsu, 213000, People’s Republic of China; 3Tianjin University of Traditional Chinese Medicine, Tianjin, 301617, People’s Republic of China; 4Changzhou Institute for Advanced Study of Public Health, Nanjing Medical University, Changzhou, Jiangsu, 213000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Renjie Lu, The Affiliated Changzhou Hospital of Xuzhou Medical University, Changzhou Third People’s Hospital, Changzhou, Jiangsu, 213000, People’s Republic of China, Email [email protected] Lingmin Hu, Changzhou Maternal and Child Health Care Hospital, Changzhou Medical Center, Nanjing Medical University, Changzhou, Jiangsu, 213000, People’s Republic of China, Email [email protected]
Objective: In the Chinese medical context, there is a large variation in patient health literacy levels and an imbalance of power between doctors and patients. The mechanism by which communicative health literacy (CHL) influences patient loyalty (PL) remains unclear. This study aims to explore how CHL in the medical context improves PL by promoting enhancement of perceived health literacy (EPHL) and strengthening decision-making involvement satisfaction (DMIS) based on the Social Exchange Theory (SET).
Methods: This study employs a questionnaire survey to collect data from five representative cities in China (Beijing, Shanghai, Guangzhou, Wuhan, and Chengdu), with a total of 4018 questionnaires collected, yielding 3264 valid questionnaires after quality control (valid rate: 81.23%). A structural equation model is used to examine the relationships between CHL, EPHL, DMIS, and PL, and to test the relevant hypotheses. Additionally, data from three cities in Jiangsu Province, China, are collected, with 2393 questionnaires collected and 1942 valid questionnaires obtained (valid rate: 81.15%), to conduct a robustness test of the model.
Results: CHL was significantly positively correlated with EPHL (β=0.516), DMIS (β=0.329), and PL (β=0.192). EPHL was also significantly positively correlated with DMIS (β=0.301) and PL (β=0.355). DMIS was significantly positively correlated with PL (β=0.316). EPHL partially mediated the relationship between CHL and DMIS (32.02%), and between CHL and PL (48.80%). DMIS partially mediated the relationship between CHL and PL (35.02%). EPHL and DMIS played a chain-mediated role between CHL and PL (20.33%). DMIS partially mediated the relationship between EPHL and PL (21.11%).
Conclusion: This study extends the application of SET to the realm of doctor-patient communication, and is the first to confirm the sequential process of “cognitive reserve - capability construction - emotional identification - relational return” within a Chinese context. It provides a new perspective for understanding the formation mechanism of PL and offers theoretical support for the construction of health literacy–oriented medical institutions. Future research could expand the sample scope to cover different cultural backgrounds and various types of medical institutions, thereby enhancing the model’s generalizability and further exploring its mechanisms of action.
Keywords: communicative health literacy, enhancement of perceived health literacy, decision-making involvement satisfaction, patient loyalty, social exchange theory
Introduction
Background
In the field of medical services, patient loyalty (PL) has become a core indicator for measuring the quality of medical care and the competitiveness of medical institutions.1–3 The mechanism by which the quality of doctor-patient interactions affects loyalty has gradually become a focus of both academia and practice.4–7 However, the doctor-patient relationship in China exhibits unique complexity. The tiered diagnosis and treatment system is accelerating, yet the service capacity of primary-level medical institutions remains limited;8–10 high-quality medical resources are concentrated in high-level hospitals, creating a pronounced “siphon effect” that increases the difficulty of building long-term trust relationships.11,12
In mature healthcare systems, long-term doctor-patient relationships and patient-centered decision-making models are widely recognized. As early as the 1960s-1970s, the US healthcare system has generally emphasized the construction of family physician and general practitioner systems, stressing continuous care and long-term doctor-patient relationships to promote trust accumulation and improve healthcare quality.13 In Germany, surveys of general practice, multiple sclerosis, and dental patients also indicate that patients generally prefer to co-decide treatment plans with their doctors.14 In English-speaking countries such as Canada, the United States, the United Kingdom, and Australia, patient-centered medical models have become mainstream, advocating patient autonomy, active participation, and shared decision-making, forming a communication model centered on shared care.15 In contrast, under China’s collectivist cultural background, patients are often placed in a subordinate position, and doctor-patient communication is more hierarchical and paternalistic.15–17 Research shows that some doctors in China still underestimate the importance of patient consultation and shared decision-making, believing that patients lack rational judgment and that participation in treatment plans may not improve outcomes. For example, a survey in Shandong, China, found that over 20% of doctors hold this view.17 Furthermore, China’s medical service structure characterized by “short doctor-patient contact, high pressure, and high mobility” further limits the depth and quality of doctor-patient communication.18 This phenomenon of power imbalance between doctors and patients poses numerous challenges to trust-building and communication quality. Overall, the long-established communication culture in Western countries centered on patient autonomy and continuous care differs significantly from the doctor-patient relationship in China’s collectivist and high-load medical environment. It is precisely this cultural and structural contrast that provides a unique contextual perspective for this study and highlights the theoretical innovation space for exploring communication mechanisms within China’s medical system.
PL typically denotes patients’ continuous choice intention and recommendation behavior toward a medical institution or physician.7 It not only reflects their sustained preference and willingness to recommend the same provider, but also embodies affective identification and psychological commitment, constituting a vital foundation for long-term value creation in medical service relationships. Research demonstrates that PL is significantly associated with medical service quality and serves as a key indicator for evaluating institutional competitiveness and improving health outcomes.19 Further empirical evidence reveals that patient trust mediates the relationship between satisfaction and loyalty, indicating that loyalty is rooted not merely in behavioral intention, but also in cognitive understanding and emotional connection.20 Existing measurement tools for PL have predominantly emphasized outcome-level constructs such as care-seeking intention and recommendation behavior, often examining linkages among service quality,21 satisfaction,22 doctor-patient relationship,7 and loyalty. The present study, by contrast, focuses on the formation process of loyalty, expands its theoretical scope and measurement dimensions, and offers a novel analytical framework for elucidating the generative mechanisms of loyalty within doctor-patient relationships.
Health literacy is commonly described as a prerequisite for good health decisions, healthy behaviors, and overall health.23 As the ability of individuals to obtain and understand health information, health literacy is crucial for promoting health and reducing disparities. Traditional research often views health literacy as a static individual trait, neglecting its interactive relationship with communication behavior. In recent years, the concept of Communicative Health Literacy (CHL) has provided a new perspective to address this issue. Unlike traditional communication evaluation, CHL emphasizes patients’ ability to actively express themselves, interact effectively, and process information in medical contexts.24 Existing research has primarily focused on the development and validation of CHL measurement tools, lacking systematic analysis of theoretical connotation and mechanism. In Ishikawa et al’s health literacy scale, CHL items focus on individuals’ ability to process general health information, not covering doctor-patient interaction capabilities.25 Chinn et al’s All Aspects of Health Literacy Scale (AAHLS) contains only three CHL items, limiting its independent application.26 Some empirical studies use communication quality as the independent variable without directly verifying CHL’s role.7 In the Chinese medical context, heterogeneous patient health literacy27 and doctor-patient power asymmetry28 make revealing CHL’s internal logic of influencing loyalty through multi-stage resource exchange more theoretically valuable and practically significant. Moreover, no previous study has applied this CHL measurement tool in Chinese populations. CHL can facilitate effective communication and interaction between patients and doctors. Higher levels of health literacy imply the capability to make good health decisions. When patients possess good CHL, they are able to participate more effectively in medical decision-making, enhance their perceived health literacy, and improve decision-making involvement satisfaction (DMIS). This satisfaction is an important resource that patients obtain through doctor-patient interactions. When the resources they gain outweigh their investments, it strengthens their trust in and loyalty to medical services. Based on the Social Exchange Theory (SET), this study integrates the aforementioned stages to fully present the resource exchange process of SET: patients start with CHL (cognitive reserve) → transform into enhancement of perceived health literacy (EPHL) (capability construction) through interaction → EPHL facilitates DMIS (emotional identification) → ultimately driving loyalty (relational return). This chain path directly corresponds to the path logic of SET.
In this context, the mechanism through which CHL affects PL remains unclear. Existing research has shown that patients’ health literacy level is significantly correlated with the quality of doctor-patient information exchange. For instance, Ishikawa et al found that diabetic patients with higher CHL experienced more sufficient information exchange during their visits.29 Other studies have indicated that the quality of doctor-patient communication is significantly positively correlated with PL.7 Additionally, a questionnaire survey of patients in Chinese public hospitals revealed that although patient satisfaction did not directly affect loyalty, it significantly enhanced loyalty through the mediating variable of patient trust.20 Based on this evidence, while related pathways have been partially verified, two major gaps persist in current research: first, few studies have analyzed how CHL forms a loyalty-driving chain through cognitive transformation and emotional identification; second, there is a lack of contextualized interpretation of resource exchange mechanisms within China’s doctor-patient power asymmetry context.
Furthermore, recent studies have indicated that patients with lower socioeconomic status often face greater barriers in health information acquisition, communication initiative, and doctor-patient trust.30,31 The proliferation of digital health tools may either amplify or narrow this gap across different demographic groups.32,33 This suggests that socioeconomic background and disparities in digital health literacy may serve as important potential confounders influencing doctor-patient communication and PL. Therefore, this study incorporates variables such as registration category, hospital type, age, gender, marital status, and education level as control factors in the analysis to mitigate potential confounding effects and enhance the robustness of the findings.
In summary, under the dual constraints of uneven patient health literacy and doctor-patient power asymmetry, this study will, based on SET, explore how CHL promotes PL through perceived fairness and trust in the Chinese context, constructing a chain mediation model of “cognitive reserve - capability construction - emotional identification - relational return”. It is worth noting that the CHL, EPHL, DMIS, and PL involved in this study originate from multiple disciplinary fields, possessing interdisciplinary attributes in public health, humanistic communication, clinical decision-making, and psychological behavior, which endows the model with a naturally multidisciplinary perspective-an important innovation of this study. Through this model, this study aims to reveal the important role of CHL in the medical context and its influence mechanism on PL, and to provide new strategies for medical institutions and physicians on how to enhance PL in practice.
Theoretical Framework
The theoretical framework of this study is constructed based on SET. SET emphasizes that individuals contribute their time, energy, and skills to obtain various rewards, including salary, benefits, and job security.34 The resources involved in the exchange encompass two dimensions: economic resources (tangible) and socio-emotional resources (symbolic).35 In doctor-patient relationships, information and emotions are the most common resources exchanged, while satisfaction and loyalty are also important outcomes of the exchange. When patients perceive that the resources they obtain from doctor-patient interactions (such as informational support, emotional care, trust, and satisfaction) outweigh the costs they have invested, they are more likely to maintain this relationship and exhibit higher loyalty.
Nutbeam’s model categorizes health literacy into three sequential levels: Functional health literacy, Interactive health literacy, and Critical health literacy. Among them, both Interactive health literacy and Critical health literacy are more advanced cognitive skills.36 CHL has been further developed based on Nutbeam’s model. It reflects the patient’s ability to clearly express their own needs, effectively obtain and understand health information, and actively participate in medical decision-making during the communication process with doctors.24 Therefore, CHL represents a comprehensive ability that patients possess, covering aspects such as cognition, communication, social interaction, information processing, and decision-making. These abilities help patients to better exchange information, preferences, emotions, and trust with doctors during their interactions.
In the Integrated model of health literacy proposed by Kristine Sørensen et al, the “application” dimension in the “Health care” domain means that patients can use health information to make informed decisions about medical issues.37 Danielle M Muscat et al were the first to explore the expansion of health literacy into the shared decision-making model, and they proposed that health literacy skills should be developed for shared decision-making.38 Enhanced health literacy and satisfactory decision-making involvement can be regarded as valuable exchange outcomes between patients and healthcare providers, which helps to establish long-term trusting relationships.
In the theoretical framework of this study, CHL is regarded as the starting point and resource foundation of social exchange, representing patients’ ability to express needs, understand information, and share personal experiences and emotions in doctor-patient communication. EPHL reflects the “resource gains” that patients perceive in the interaction, that is, the sense of control, autonomy, and trust obtained through effective communication, and is the intermediate product of resource transformation in the social exchange process. DMIS embodies socio-emotional returns, reflecting the emotional feedback of respect, being heard, and value realization that patients experience in shared decision-making. Finally, PL is regarded as the long-term outcome of the social exchange relationship, typically manifested as patients’ trust in medical institutions, continuous choice, and positive recommendation behavior.
In summary, based on SET, this study proposes the chain mediation path “CHL → EPHL → DMIS → PL” to explore how CHL drives the formation of PL through resource acquisition, emotional identification, and social returns. This path helps further expand the applicability of SET in the medical service field and provides a potential reference for deepening the understanding of resource exchange mechanisms in doctor-patient interactions: that is, when patients possess high CHL, they can achieve dual cognitive-emotional returns in the interaction, perceive higher empowerment and satisfaction, and thus form stable trust and loyalty. This framework provides ideas for exploring the potential links of EPHL and DMIS between CHL and PL, and also offers a new theoretical perspective for explaining the possible mechanism of action of CHL in long-term doctor-patient relationships and organizational performance. The hypothesized model is shown in Figure 1.
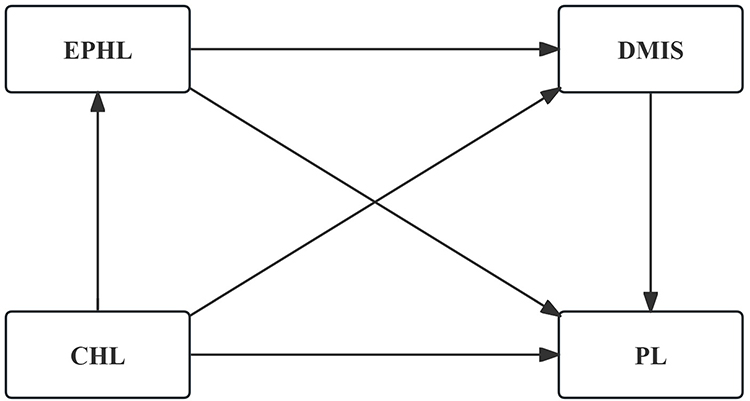 |
Figure 1 Hypothesized Model. Abbreviations: CHL, Communicative Health Literacy; EPHL, Enhancement of Perceived Health Literacy; DMIS, Decision-making Involvement Satisfaction; PL, Patient Loyalty. |
Research Hypotheses
CHL refers to the patient’s ability to clearly express their needs, obtain and understand information, and participate in decision-making during interactions with doctors.24 Patients with high levels of health literacy tend to have a greater awareness of their own health conditions.39 In contrast, individuals with limited health literacy are more likely to misunderstand health information.40 Conversely, individuals possessing adequate health literacy tend to communicate their needs more effectively, acquire and comprehend information more efficiently during interactions with healthcare professionals, thereby enhancing their health literacy further. CHL serves as patients’ cognitive/communication resource input (Resource Input); high CHL helps improve patients’ ability to acquire and process information, thereby being transformed in interaction into perceived health literacy empowerment- that is, the cognitive reserve → capability construction pathway.24 Therefore, this study proposes the following hypotheses.
H1: CHL is positively correlated with EPHL.
Decision-making involvement satisfaction (DMIS) is an individual’s subjective evaluation of the medical decision-making process and outcome, reflecting the respect they feel during the decision-making process.41 According to the theoretical conception of “incorporating health literacy into the shared decision-making model” proposed by Danielle M. Muscat et al,38 and the “application” dimension in the Integrated model of health literacy proposed by Kristine Sørensen et al, which represents the patient’s ability to use health information to make informed decisions about medical issues,37 this study boldly infers that satisfaction with the “application” of health literacy is equivalent to satisfaction with shared decision-making. CHL serves as an input resource that helps enhance patients’ ability to express themselves and participate in interactions, thereby increasing emotional returns (feeling respected, being heard) in the shared decision-making process, ie, improving DMIS (cognitive reserve → emotional identification pathway).38 Therefore, this study proposes the following hypothesis.
H2: CHL is positively correlated with DMIS.
Loyalty to medical services refers to the tendency of an individual to choose the same medical institution again to meet their future medical needs, based on their satisfaction with past medical experiences and trust in medical service providers and medical professionals.7 The better the feedback patients have on their experiences, the more likely they are to feel valued by medical service providers and to have high loyalty to the hospital.42 Patients possessing a high level of CHL are capable of articulating their symptoms and requirements with clarity, and they demonstrate a superior understanding of medical advice and treatment protocols. This results in a favorable experience, which in turn strengthens their satisfaction and loyalty towards healthcare services. CHL, as a stable input resource, promotes patients’ long-term relationship maintenance behaviors when it generates sustained positive returns (information, respect, trust) through interaction, thereby reflecting the cognitive reserve → relational return pathway.19 Therefore, this study proposes the following hypothesis.
H3: CHL is positively correlated with PL.
Under normal circumstances, health literacy is the foundation for patients to participate in medical decision-making.43–45 Improvements in health literacy enable individuals to better understand medical information, thereby allowing them to more confidently express their opinions and choices during the decision-making process. This enhanced ability can increase individuals’ sense of participation and satisfaction in the decision-making process. Moreover, patients with different levels of health literacy significantly differ in the topics they discuss during communication.46 Enhancing patients’ health literacy can also help them better evaluate the risks and benefits of medical plans, further increasing their satisfaction with decision-making participation. EPHL represents the capability conversion (Resource Conversion) that patients acquire through exchange. This capability enhancement increases patients’ sense of control and feeling valued in decision-making interactions, thereby promoting shared decision-making (capability construction → emotional identification).36 Therefore, this study proposes the following hypothesis.
H4: EPHL is positively correlated with DMIS.
EPHL not only helps individuals better manage their own health but also strengthens their trust in medical service providers.47,48 Higher levels of health literacy enable individuals to more accurately understand medical information, thereby allowing them to more accurately assess the professional competence and service quality of medical service providers. The determinants of PL include satisfaction, service quality, and a sense of trust.19 When patients have a high evaluation of the professionalism and service quality of medical service providers, they are more likely to develop trust and satisfaction with the medical service providers. EPHL, as a resource gain obtained through interaction, is often accompanied by higher levels of trust and satisfaction, and these positive experiences may contribute to the sustained development of the relationship—that is, capability construction → relational return.49 Therefore, this study proposes the following hypothesis.
H5: EPHL is positively correlated with PL.
Shared decision-making is a patient-centered approach to medical care.50 Patients with high DMIS often feel respected and valued in the medical process through a “patient-centered” approach. This positive emotional experience may enhance their satisfaction with medical service providers. Patient satisfaction with medical services is one of the key factors influencing their loyalty.4,22,51 Higher levels of satisfaction can motivate patients to more willingly choose the same medical service provider for subsequent medical services. DMIS may be conceptualized as socio-emotional returns within the exchange process. Higher levels of DMIS are typically associated with positive emotional experiences such as feeling respected and being heard, and such emotional returns may underpin the formation and maintenance of loyalty relationships (emotional return → relationship maintenance).20 Therefore, this study proposes the following hypothesis.
H6: DMIS is positively correlated with PL.
Among the three levels of health literacy, CHL is similar to interactive health literacy, both of which are considered advanced cognitive skills.36 Many patients, due to their lack of medical knowledge, often struggle to communicate effectively with medical staff.52,53 However, individuals with higher levels of CHL are able to communicate more effectively with doctors. Research has shown that effective communication is an important prerequisite for improving patients’ health literacy.23,54,55 At the same time, when patients have higher levels of health literacy, they are usually more proactive in participating in shared decision-making.56 During the shared decision-making process, patients are more likely to effectively express their needs, understand doctors’ recommendations, and be satisfied with the decision outcomes. CHL contributes to enhancing patients’ capacity to acquire, understand, and apply health information, enabling the gradual transformation of information into perceivable interactive capability, and potentially augmenting their sense of involvement and emotional feedback in medical interactions.57 This hypothesis corresponds to the mediating chain of “cognitive reserve → capability construction → emotional identification” in SET. Therefore, this study proposes the following hypothesis.
H7: EPHL mediates the relationship between CHL and DMIS.
In modern medical practice, the paternalistic care model of physicians is gradually shifting towards a model that shares power, information, and decision-making with patients.58 This patient-centered approach to medical care emphasizes patient participation and autonomy. Individuals with higher levels of CHL are able to more clearly express their preferences and values, and engage in more effective interactions with doctors during the medical decision-making process. This positive communication may enhance individuals’ sense of control and satisfaction in the decision-making process. Communication quality and satisfaction are key drivers of PL.4 If CHL investment can generate emotional returns during the decision-making process, this emotional return will be transformed into relationship maintenance behaviors, reflecting the exchange path of “cognitive reserve → emotional identification → relational return”.59 Therefore, this study proposes the following hypothesis.
H8: DMIS mediates the relationship between CHL and PL.
Patients with higher levels of CHL may more easily enhance their health literacy further during the communication process. An increase in EPHL means that patients are better able to recognize the value of cognitive resources. Research has shown that perceived value has a positive impact on PL.60 Additionally, studies have indicated that the higher the level of health literacy, the greater the trust patients have in doctors and the healthcare system.61 In summary, CHL may indirectly promote patients’ loyalty to medical service providers by enhancing perceived value. EPHL, as a capability gain, may enable patients to more readily acquire trust and satisfaction in subsequent interactions, thereby fostering loyalty; this hypothesis corresponds to the indirect path of “cognitive reserve → capability construction → relational identification” in SET.49,62 Therefore, this study proposes the following hypothesis.
H9: EPHL mediates the relationship between CHL and PL.
Health literacy is commonly described as a prerequisite for good health decisions, healthy behaviors, and overall health.43 CHL can facilitate effective communication and interaction between patients and doctors.24 Higher levels of health literacy imply the capability to make good health decisions.43 When patients possess good CHL, they are able to participate more effectively in medical decision-making, enhance their health literacy, and improve DMIS. This satisfaction is an important resource that patients obtain through doctor-patient interactions. When the resources they gain outweigh their investments, it strengthens their trust in and loyalty to medical services. Based on SET, this study integrates the aforementioned stages to fully present the resource exchange process of SET: patients start with CHL (cognitive reserve) → transform into EPHL (capability construction) through interaction → EPHL facilitates DMIS (emotional identification) → ultimately driving loyalty (relational return). This chain path directly corresponds to the path logic of SET.
H10: EPHL and DMIS play a chain mediating role between CHL and PL.
Objects and Methods
Research Subjects
This study employed a convenience sampling survey method. A pilot survey was conducted from February 13 to February 16, 2024, and the questionnaire was optimized based on the results of the pilot survey to form the final survey questionnaire. The questionnaire consists of two parts: demographic characteristics and scales. All scales used in this study were selected from validated and well-established instruments. After translation into Chinese, these scales were appropriately adjusted to ensure that their original meanings were retained while making them more suitable for the reading and comprehension habits of the Chinese population. This study was approved by the ethics committee, and an electronic informed consent form was placed on the first page of the questionnaire. Participants were required to actively click the “Agree” button before filling out the questionnaire to indicate their voluntary participation in the study; those who did not click “Agree” could not access the formal question pages. The survey was distributed through Questionnaire Star (https://www.wjx.cn) in five representative large cities across China: Shanghai (eastern region), Chengdu (western region), Guangzhou (southern region), Beijing (northern region), and Wuhan (central region). Additionally, to further validate the model, the survey was also distributed in three representative cities within Jiangsu Province (the province where the research team is based): Suzhou (southern region), Nanjing (central region), and Xuzhou (northern region). The survey targeted patients who had visited a hospital within the past six months. To better facilitate respondents’ recall of their medical visits, the study included situational prefixes such as “During this medical visit.” or “Through this medical visit.” before each item. Modifications to some scales were also attuned to Chinese respondents’ cognitive and linguistic conventions. The questionnaire for this study was distributed through an online platform, with all items set as mandatory. Participants were required to complete all entries before submission, resulting in no missing values in the obtained data and eliminating the need for missing data processing. Additionally, to ensure data quality, this study implemented a dual-person independent verification procedure, guaranteeing the accuracy and reliability of the data.
The formal survey was conducted from February 17 to March 4, 2024. Using the convenience sampling method, a total of 4018 questionnaires were collected from the five representative large cities. According to the quality control criteria, the system of Questionnaire Star automatically excluded 750 invalid questionnaires (668 questionnaires with insufficient completion time; 1 questionnaire with an ineligible survey respondent; 81 questionnaires with incorrect answers to common knowledge questions). Additionally, 4 duplicate questionnaires were manually identified and removed, resulting in a total of 754 invalid questionnaires. Consequently, 3,264 valid questionnaires remained, yielding an effective response rate of 81.23%. In Jiangsu Province, a total of 2,393 questionnaires were collected. Using the VIP features of Questionnaire Star to set rules for screening, 447 invalid questionnaires were automatically excluded (364 questionnaires with completion time < 200 seconds; 2 questionnaires with ineligible participants; 81 questionnaires with incorrect answers to common knowledge questions). Moreover, 4 duplicate questionnaires were manually identified and removed, resulting in a total of 451 invalid questionnaires. Thus, 1,942 valid questionnaires remained, with an effective response rate of 81.15%.
Research Instruments
Communicative Health Literacy Scale
The HLS19 instrument used in this research was developed within the “European Health Literacy Population Survey 2019–2021 (HLS19)” conducted by M-POHL. It is a novel measurement tool designed to assess CHL in individuals’ interactions with physicians.24 Individual health literacy is conditional and situational.63,64 The six-item short version of the HLS19 scale demonstrates a good unidimensional structure.
Enhancement of Perceived Health Literacy Scale
This scale was adapted from some widely validated health literacy measurement instruments in existing literature. The wording of the items has been appropriately adjusted to fit the comprehension of Chinese respondents. In this study, this variable is redefined as perceived health literacy improvement. The response options were presented on a 5-point Likert scale, ranging from Strongly Disagree to Strongly Agree.
Decision-Making Involvement Satisfaction Scale
The Clinical Decision-making Involvement and Satisfaction (CDIS) patient version was developed by Slade et al.65 The satisfaction subscale of the patient version of the CDIS provided a reference for the development of DMIS in this study. Based on the Chinese adaptation of CDIS by Chongmei Huang et al, the wording of the items has been appropriately adjusted to fit the comprehension of Chinese respondents.41 The response options were presented on a 5-point Likert scale, ranging from Strongly Disagree to Strongly Agree.
Patient Loyalty Scale
This scale was adapted from the patient loyalty scale developed by Huang et al.66 The scale primarily measures the intention to choose the same doctor again in the future and to recommend this doctor to others. The wording of the items has been appropriately adjusted to fit the comprehension of Chinese respondents. The response options were presented on a 5-point Likert scale, ranging from Strongly Disagree to Strongly Agree.
Statistical Methods
This study used SPSS 26.0 and AMOS 26.0 software for data processing and statistical analysis. First, the normality assumption of continuous variables was tested using P-P plots, histograms, and other methods to ensure that the data met the prerequisites for subsequent analyses. Before formal analysis, given that scale items were contextually adapted and rephrased, this study randomly divided the sample into two subsamples (each n ≈ 50% of the total sample size) for exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) respectively, to systematically examine the appropriateness and structural validity of the measurement instrument in the context of this study. Specifically, SPSS 26.0 was first used for EFA, followed by AMOS 26.0 for CFA through a multi-model comparison strategy (eg, single-factor model, multi-factor competing models) to select the best-fitting measurement model. Subsequently, Cronbach’s α coefficient and composite reliability (CR) were used to assess scale reliability, and Harman’s single-factor test was employed to diagnose common method bias.
Second, descriptive statistical analysis was used to present the basic information of respondents and the means, standard deviations, and distribution characteristics of the research variables. For variables that met the normal distribution, Pearson correlation analysis was used to assess their linear associations; otherwise, Spearman rank correlation test was used to provide preliminary evidence for hypothesis testing.
Finally, based on the measurement model established by CFA, AMOS 26.0 was used to construct a structural equation model (SEM) to test the research hypotheses, and model fit was evaluated using indices such as χ2/df, RMSEA, CFI, and TLI. To ensure the robustness of the statistical results, bootstrap resampling technique (5000 iterations) was used to estimate the standard errors and confidence intervals of the parameters. All statistical tests used a two-tailed P < 0.05 as the significance level.
Results
Descriptive Statistics
Among the samples collected from the five representative large cities, the average age of respondents was 36.01 ± 9.11 years. Regarding registration categories, the highest proportion of patients chose general registration (47.1%), followed by specialist registration (44.3%). The types of hospitals visited were primarily county-level public hospitals (32.5%) and township health centers or community health service centers (24.8%). In terms of gender composition, there were slightly more female patients than male patients (52.9% vs 47.1%). The majority of respondents were married (71.5%). In terms of educational level, 46.9% had an associate degree or lower, 46.9% had a bachelor’s degree, and 6.2% had a master’s degree or higher (Table 1).
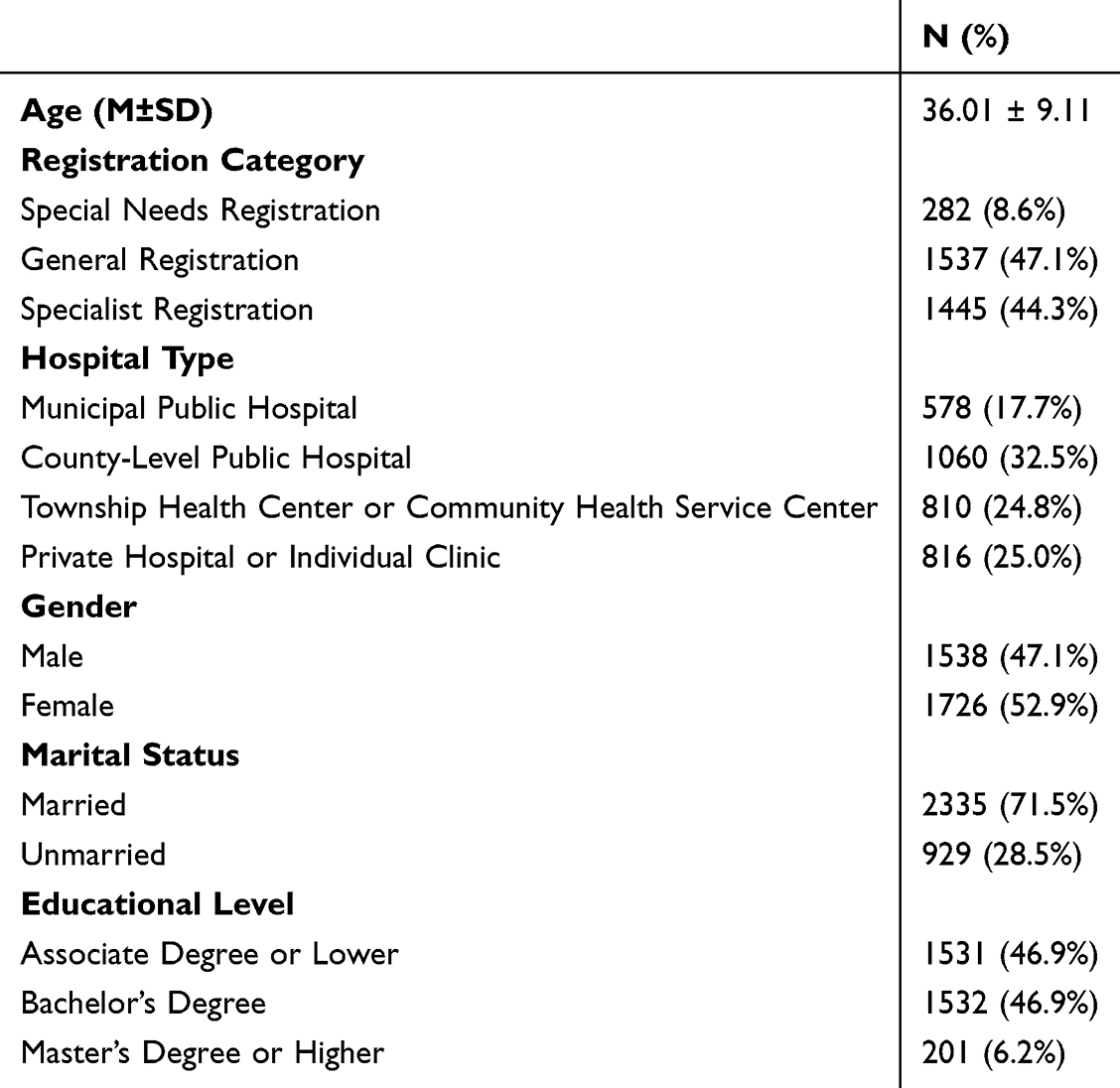 |
Table 1 Basic Demographic Information of Participants |
Validity Analysis
Structural Validity Analysis
Exploratory factor analysis was conducted on each scale in this study. The Kaiser-Meyer-Olkin (KMO) values for all scales were greater than 0.6, indicating that factor analysis was appropriate. The cumulative variance explained by the first factor of each scale ranged from 68.485% to 82.347%. The structure of each scale was rational and adequately explained the underlying factors (Table 2).
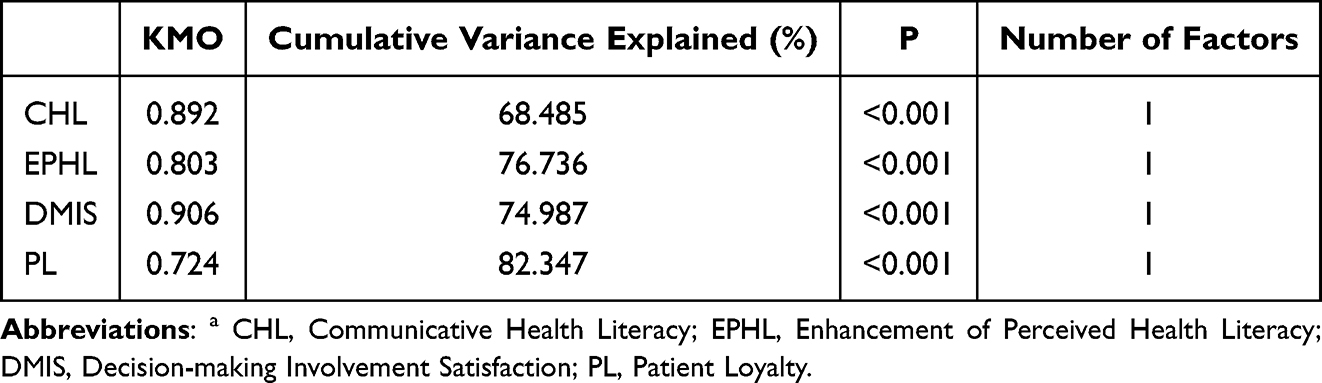 |
Table 2 Exploratory Factor Analysis of Each Scalea |
Convergent Validity Analysis
Convergent validity analysis was conducted using AMOS. The results showed that the standardized factor loadings for all scales were greater than 0.4, the Average Variance Extracted (AVE) values were greater than 0.5, and the Composite Reliability (CR) values were greater than 0.6, indicating that all scales had good convergent validity (Table 3).
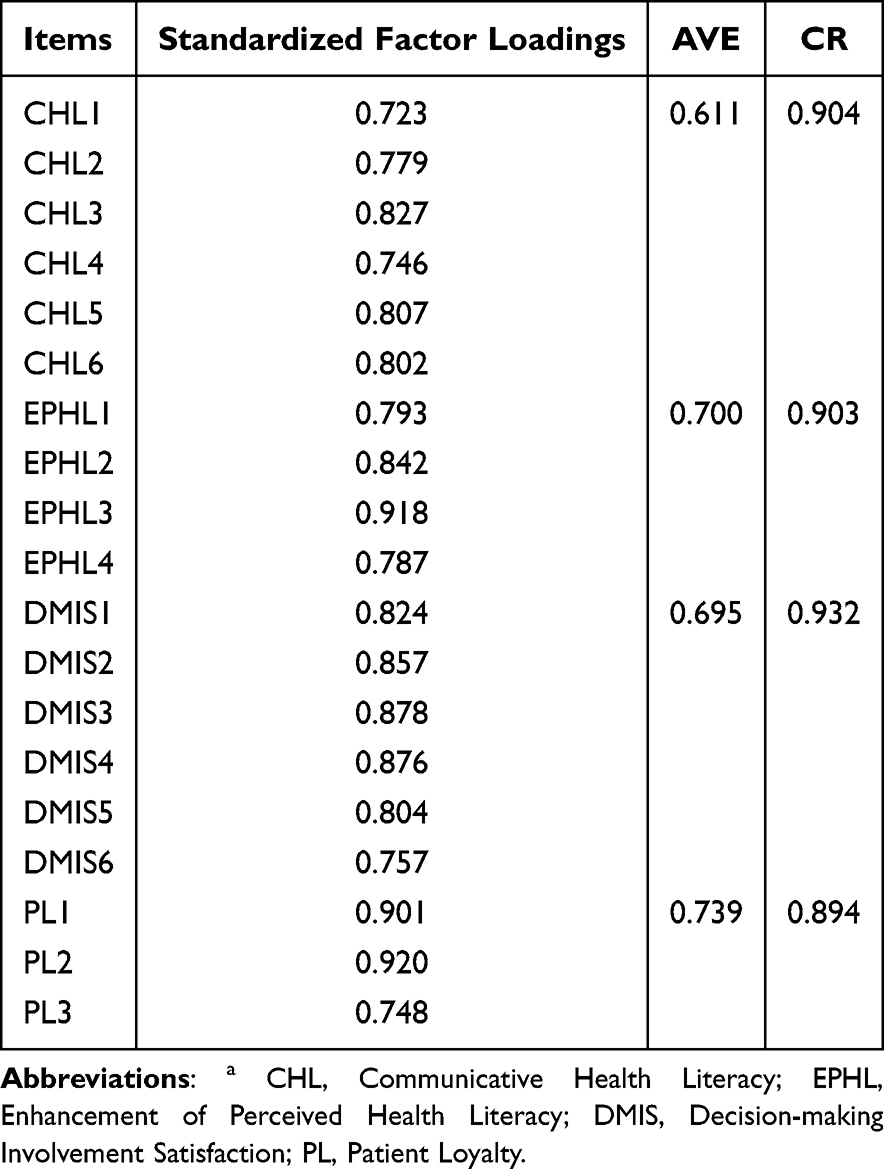 |
Table 3 Convergent Validity Analysis of Each Scalea |
Confirmatory Factor Analysis of Multi-Factor Model
As the model evolved from a single-factor model to a combined model of all factors, the χ2/df ratio gradually increased, while the GFI, CFI, and NFI values gradually decreased. Conversely, the RMSEA and SRMR values increased. Therefore, the model with separate factors exhibited the best fit (Table 4).
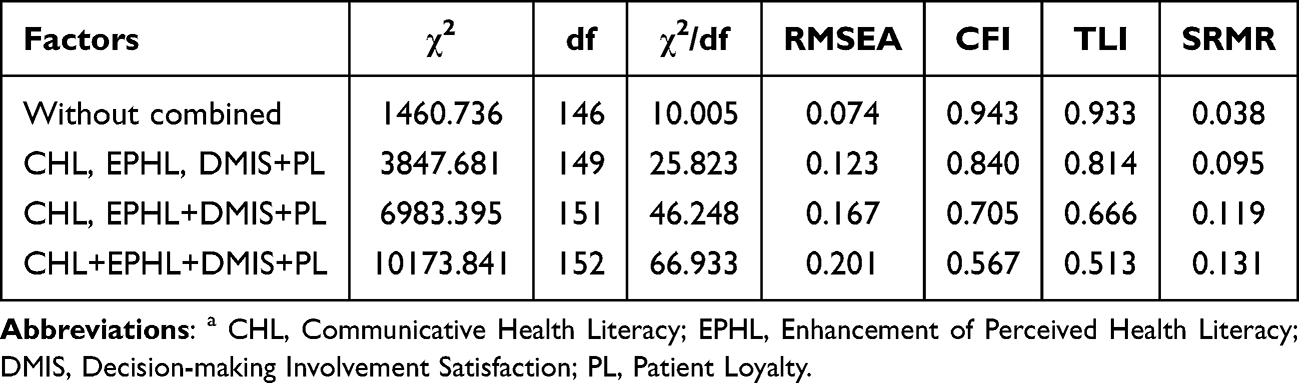 |
Table 4 Confirmatory Factor Analysis of the Multi-Factor Model a |
Reliability Analysis
The Cronbach’s α coefficients for all scales ranged from 0.891 to 0.930, all of which were greater than 0.7, indicating good internal consistency of the scales. After the removal of any item, the changes in Cronbach’s α remained within acceptable ranges. The Corrected Item-Total Correlation (CITC) for each scale was greater than 0.4. In summary, all scales demonstrated good reliability (Table 5).
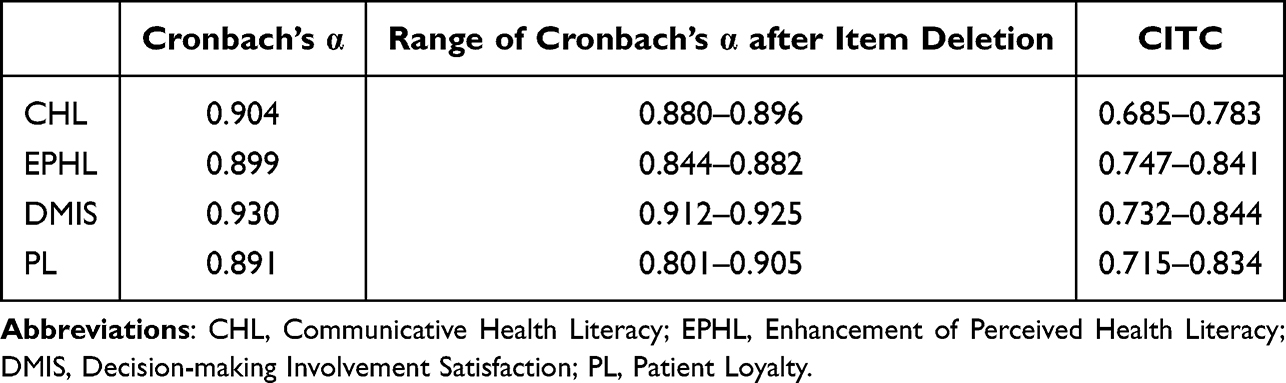 |
Table 5 Reliability Analysis of Each Scale a |
Common Method Bias Analysis
During the questionnaire design and survey implementation phases, this study adopted a series of procedural control measures to address common method bias. However, since the questionnaire responses were self-reported by participants, the possibility of common method bias could not be completely ruled out. Therefore, this study utilized Harman’s single-factor test to assess the severity of common method bias. The results showed that the first common factor explained 46.219% of the variance, which is below the critical threshold of 50%. Consequently, no significant common method bias was detected in the data collected for this study.
Correlation Analysis
Pearson correlation analysis was employed in this study. Significant positive correlations were found among all variables, with all correlation coefficients were statistically significant (p < 0.001). The range of correlation coefficients was 0.440 to 0.574 (Table 6).
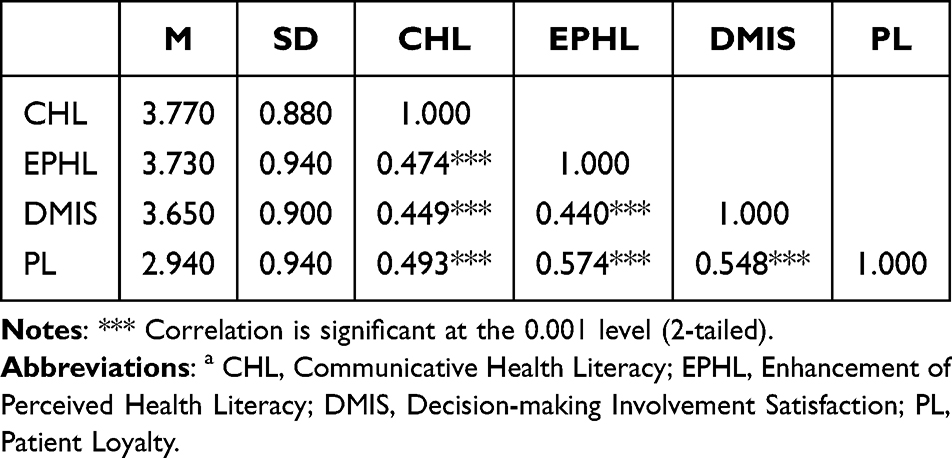 |
Table 6 Correlation Analysis of Each Scalea |
Model Construction
The initial structural equation model (SEM) was constructed using AMOS 26.0. In the initial model (M0), the standardized root mean square residual (SRMR) was 0.037, and the root mean square error of approximation (RMSEA) was 0.075, both of which are below the threshold of 0.08. The goodness of fit index (GFI) was 0.911, and the non-normed fit index (NNFI or TLI) was 0.933, both of which exceed the threshold of 0.9. The adjusted goodness of fit index (AGFI) was 0.884, which is close to the recommended threshold of 0.9 (Tables 7, 8). Therefore, the model fit was considered to be acceptable. After controlling for demographic characteristics, the model remained significant (Appendix 1).
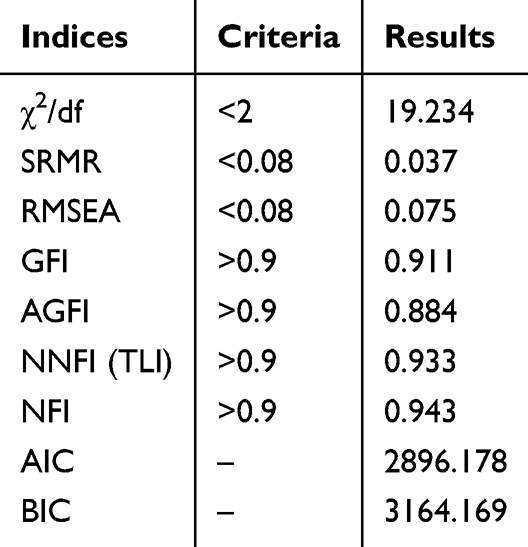 |
Table 7 Model Fit Results for Model (M0) |
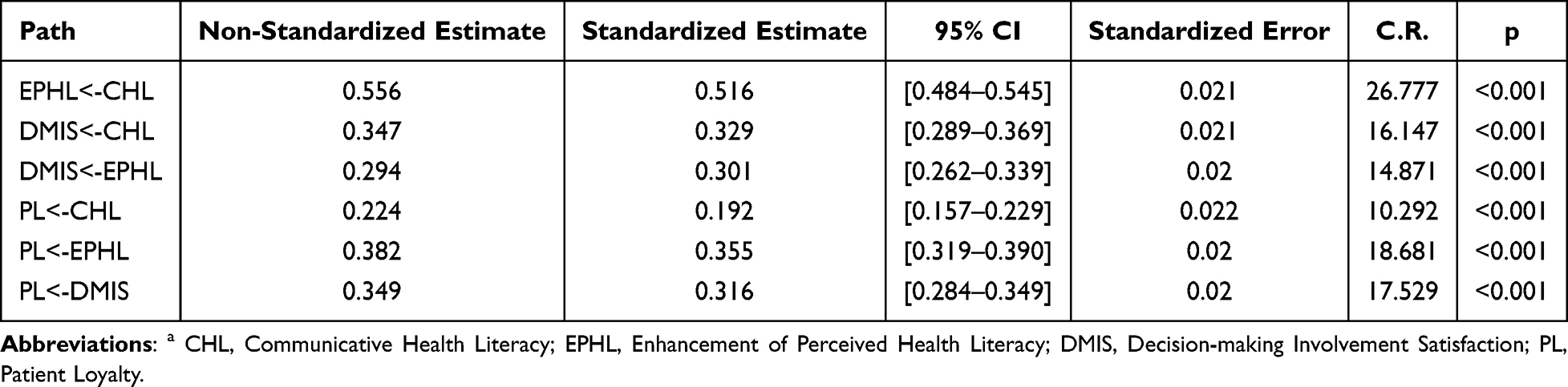 |
Table 8 Standardized Coefficients for Model (M0)a |
Testing and Decomposition of Mediation Effects
EPHL mediates the relationship between CHL and DMIS, accounting for 32.02% of the total effect (0.155/0.484). DMIS mediates the relationship between EPHL and PL, accounting for 21.11% of the total effect (0.095/0.450). EPHL mediates the relationship between CHL and PL, accounting for 48.80% of the total effect (0.183/0.375). DMIS mediates the relationship between CHL and PL, accounting for 35.02% of the total effect (0.104/0.297). The chain mediating effect of EPHL and DMIS between CHL and PL accounts for 20.33% of the total effect (0.049/0.241) (Table 9).
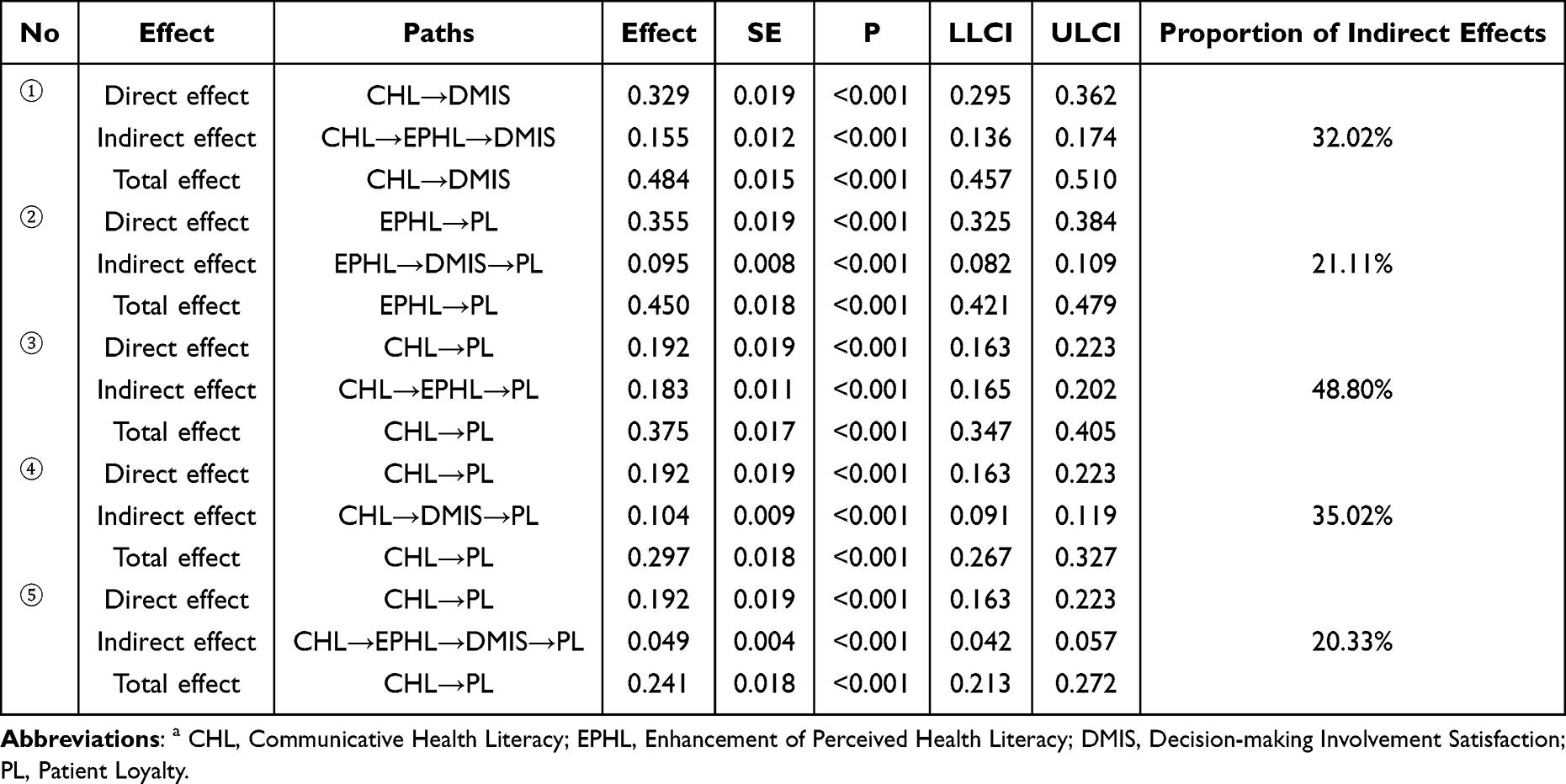 |
Table 9 Testing and Decomposition of Mediation Effectsa |
Small Sample Model Validation
This study employed data from Jiangsu Province in China to validate the generalizability of model M0. The results showed that the model fit was relatively ideal, with the χ2/df ratio decreasing to 11.721, which also explains the impact of sample size on the χ2/df ratio mentioned earlier in the text (Table 10). Additionally, the standardized coefficients for each path were 0.483, 0.261, 0.299, 0.181, 0.354, and 0.305, respectively (p < 0.001 overall). These results are similar to those obtained from the national data model fitting, further confirming the good generalizability of model M0 (Table 11 and Figure 2).
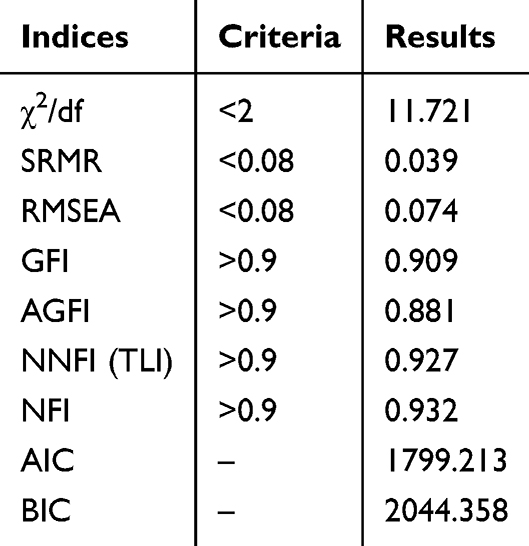 |
Table 10 Model Fit Results for Model (M1) |
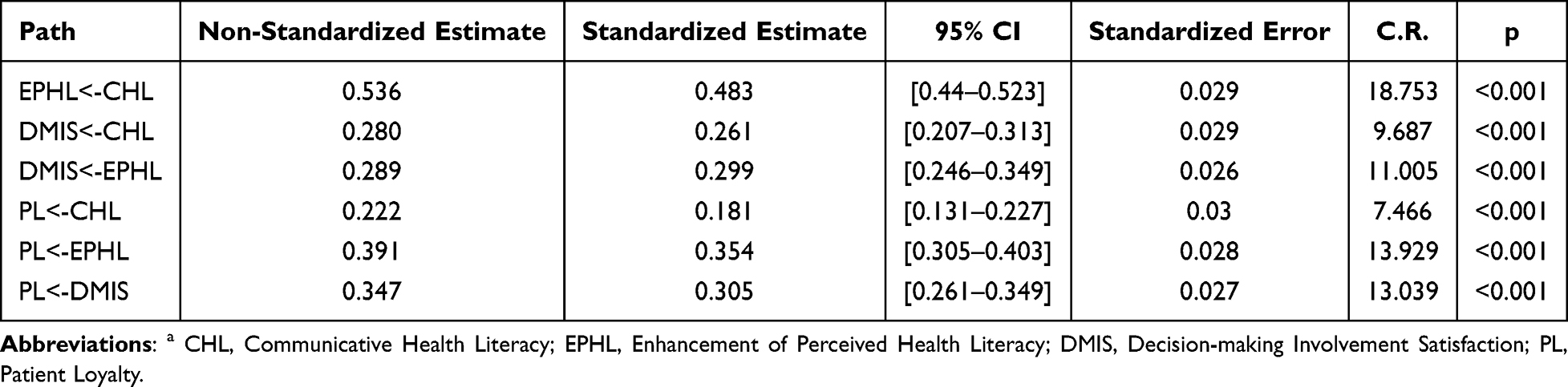 |
Table 11 Standardized Coefficients for Model (M1)a |
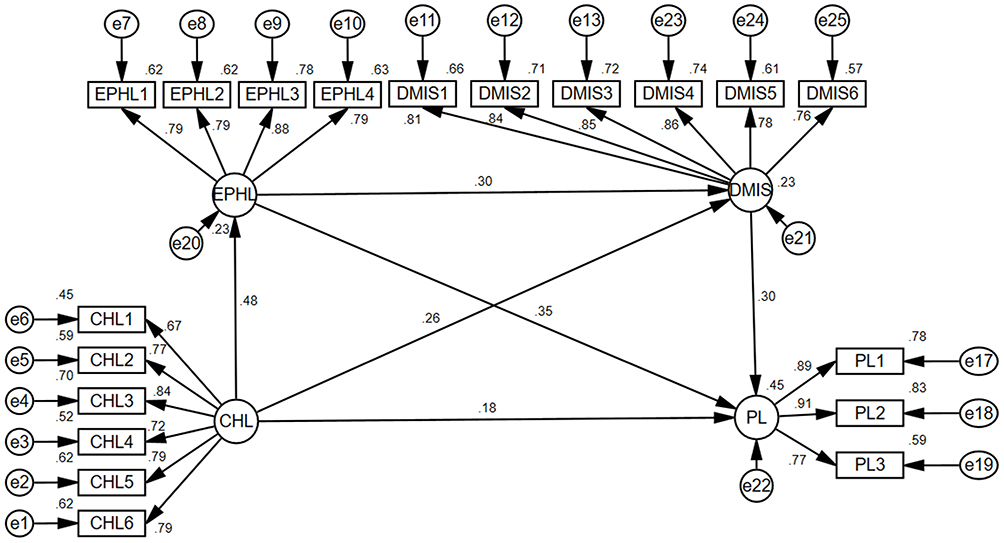 |
Figure 2 Structural Equation Model Path Diagram (M1). Abbreviations: CHL, Communicative Health Literacy; EPHL, Enhancement of Perceived Health Literacy; DMIS, Decision-making Involvement Satisfaction; PL, Patient Loyalty. |
Discussion
Based on SET, this study explored the direct effects of CHL on EPHL, DMIS, and PL, as well as the mediating effects of EPHL and DMIS. The results supported all hypotheses, revealing the complete chain of effects through which doctor-patient communication impacts loyalty via multi-stage resource exchange. Additionally, the variables involved in the model span public health, humanistic communication, clinical decision-making, and psychobehavioral domains, reflecting its conceptual multidisciplinary nature. This provides a new theoretical framework for understanding the comprehensive mechanisms of health literacy, shared decision-making, and loyalty formation in doctor-patient interactions, and establishes a foundation for future multidisciplinary team research.
CHL is positively correlated with EPHL (β=0.516, P<0.001), DMIS (β=0.329, P<0.001), and PL (β=0.192, P<0.001), which confirms the reciprocity principle of resource exchange in SET. CHL reflects the confidence and ease with which patients communicate with doctors.24 Patients with higher levels of CHL are better able to communicate with doctors during medical visits, thereby obtaining more health-promoting information and enhancing their health literacy. In short, individuals with higher CHL are more likely to further improve their health literacy levels. Secondly, when patients have higher levels of CHL, they are more likely to ask questions, express their opinions and needs.24 This active participation in treatment decision-making may lead to greater satisfaction with the decision outcomes. Moreover, good communication between doctors and patients positively impacts PL.7 When patients can communicate smoothly with doctors, they have better experiences with medical services, which in turn increases their loyalty to doctors. In summary, patients exchange good CHL for the supply of health information and a sense of control in decision-making from doctors, which may result in positive feedback evaluations of medical services.
EPHL is positively correlated with DMIS (β=0.301, P<0.001) and PL (β=0.355, P<0.001), reflecting the transformation of cognitive resources into emotional commitment and relationship maintenance. In the comprehensive model of health literacy, “application” is the fourth dimension of health literacy, and making informed decisions is a concrete manifestation of this dimension.37 Higher levels of health literacy imply that individuals have the capacity to make good health decisions.43 The enhancement of health literacy empowers patients to comprehend medical information more effectively, leading to greater confidence in their involvement during decision-making and increased satisfaction with the results. This finding also confirms the theoretical conception of “incorporating health literacy into the shared decision-making model” proposed by Danielle M. Muscat et al.38 Additionally, the improvement of patients’ health literacy helps them better manage their own health.47 Patients who maintain a positive attitude and behavior towards health are also more likely to recognize and appreciate medical services. Moreover, there is a positive correlation between DMIS and PL (β=0.316, P<0.001), supporting the reinforcing effect of equal interaction on relationship maintenance. Patient satisfaction with medical services usually directly affects their loyalty.4,22,51 As an evaluation index of the decision-making process and its outcomes, DMIS may directly drive repeat selection behavior.
In terms of mediating effects, EPHL partially mediates the relationship between CHL and DMIS (indirect effect = 0.155, P<0.001), and also partially mediates the relationship between CHL and PL (indirect effect = 0.183,P<0.001). This reveals the hierarchical transmission logic of “cognitive reserve - capability construction - emotional identification - relational return.” Individuals with higher levels of CHL are more likely to establish good communication with doctors. Effective communication helps individuals obtain, understand health information, and make informed decisions, thereby reinforcing its key role in enhancing health literacy.23 At the same time, communication aimed at improving health literacy can be regarded as a dynamic and interactive outcome between patients and medical service providers.55 This positive outcome may make patients feel more supported and respected in the medical process, thereby enhancing their loyalty to medical services. Therefore, CHL can directly or indirectly enhance patient DMIS and loyalty by promoting improvements in health literacy.
DMIS partially mediates the relationship between CHL and PL (indirect effect = 0.104, P<0.001), revealing the hierarchical transmission logic of “cognitive reserve - emotional identification - relational return.” Compared with individuals with sufficient health literacy, those with limited health literacy have lower awareness of shared decision-making rights, more negative attitudes, and ask fewer questions.67 Shared decision-making is key to promoting a shift in healthcare from a paternalistic care model to patient-centered care.50 Patient satisfaction with shared decision-making implies that patient-centered care has been effectively implemented. In this process, patients are able to effectively communicate their health-related knowledge and articulate their personal desires and values. They also experience a sense of respect and validation during their interactions with healthcare professionals. Therefore, CHL can directly or indirectly influence PL by enhancing DMIS.
EPHL and DMIS play a chain mediating role between CHL and PL (total indirect effect = 0.049, P< 0.001), revealing the cumulative effect of multi-stage resource exchange. The transformation of continuous positive experiences into long-term loyalty creates a hierarchical transmission logic of “cognitive reserve - capability upgrade - emotional identification - relationship return.” Although this model appears to involve the exchange and interaction of resources between patients and doctors, from a higher level, the key to driving this transmission logic lies in the construction of health literacy-oriented medical institutions. Medical institutions with stronger health literacy responsiveness are more likely to bring benefits to patients with lower levels of health literacy.68 Existing studies have also shown that health-promoting hospitals have a positive impact on PL.60 Therefore, this result suggests a deeper solution strategy, that is, the construction of health literacy-promoting medical institutions brings benefits to patients, doctors, and hospitals at three levels simultaneously.
Furthermore, with the rapid development of Artificial Intelligence (AI) and mobile health (mHealth) technologies, digital tools are profoundly transforming models of health literacy cultivation and dissemination. AI-driven health management systems, intelligent consultation platforms, and personalized health notification technologies can effectively enhance individuals’ information acquisition and comprehension abilities, promoting active learning and application of health knowledge.62 In the domain of oral health, Chau, Thu, Hsung, McGrath and Lam69 developed an AI-powered smart selfie monitoring system for oral health self-management, demonstrating that AI technology can augment individuals’ self-monitoring and health decision-making capabilities. Additionally, Deniz-Garcia, Fabelo, Rodriguez-Almeida, Zamora-Zamorano, Castro-Fernandez, Alberiche Ruano, Solvoll, Granja, Schopf, Callico, Soguero-Ruiz and Wägner70 noted that integrating AI into mHealth applications not only enhances information availability and interactivity but also improves patients’ health behavior change and adherence. These studies suggest that AI technology, as a novel “resource exchange” medium, can reinforce the “cognitive reserve - capability construction - emotional identification - relational return” pathway within the SET framework, offering a new digitally-supported direction for future efforts to enhance CHL and promote PL.
Theoretical Implications
This study is the first to apply CHL as a measurement tool in the Chinese population. Based on SET, this research provides a new perspective for understanding the role of individual CHL in medical contexts. In medical settings, patients exchange their CHL for health information and decision-making respect from doctors. This bidirectional exchange model enriches the theoretical connotations. Meanwhile, this research goes beyond the traditional view of health literacy as a fixed personal characteristic, confirming its role as a dynamic process in building capabilities. The spiral growth of communication and health literacy among patients sets the stage for their future involvement in decision-making and loyal actions. Additionally, this study enriches the research on the relationship between health literacy and loyalty. Previous studies have mostly focused on the impact of health literacy on health behaviors and outcomes. In contrast, this study links health literacy with PL, revealing the significant role of constructing health literacy-promoting medical institutions.
Policy Implications
Patient Level
Healthcare systems urgently need to develop and implement strategies differentiated by patients’ age, language, and cultural background to meet their specific health literacy needs.71 Systematic health literacy interventions and contextualized communication training should be employed to help patients become active participants in health decision-making. Medical practitioners can employ structured communication, guided questioning, feedback confirmation, and other techniques to facilitate patients’ expression of needs, comprehension of information, and application of knowledge to self-health management, thereby achieving a spiral interaction of “information understanding-capacity building-trust reciprocity.” This process not only enhances patients’ decision-making confidence and compliance but also contributes to the construction of long-term, mutually trusting doctor-patient relationships.
Institutional Level
Medical institutions should integrate health literacy responsiveness into the core domain of service quality management. Specifically, CHL indicators can be incorporated into patient experience and service quality evaluation systems, interdisciplinary health literacy communication training mechanisms can be established, and follow-up and feedback systems can be improved to continuously monitor patients’ communication experiences and satisfaction. Concurrently, enhancing healthcare professionals’ health literacy capabilities is equally crucial for optimizing doctor-patient communication.72,73 This capability is multidimensional in nature, encompassing functional skills (eg, clear expression), communication skills (eg, shared decision-making), and critical skills (eg, facilitating patient empowerment).72 Tailoring communication strategies according to patients’ health literacy levels can motivate them to play an active role as “co-producers” and make more information-based health decisions.24 Furthermore, developing assessment and improvement tools to support medical institutions in enhancing health literacy responsiveness74,75 can help institutionalize health literacy-oriented services, enhancing PL and institutional reputation within a positive cycle of “equity-trust-loyalty.”
Policy Level
Policymakers should promote the construction of a health literacy-friendly environment at the macro level, integrating health literacy and communication competencies into medical institution performance assessment and accreditation standards. Policy guidance can be used to encourage collaboration between hospitals and communities to establish a stratified and tiered health education system, forming a literacy support network covering the entire continuum of prevention, treatment, and rehabilitation. Simultaneously, requirements for communication equity and information accessibility should be strengthened in healthcare policies to promote the enhancement of health decision-making capabilities among diverse cultural and age groups and foster the development of a trust-centered medical service ecosystem.
Practical Implications
The healthcare system urgently needs to develop and implement strategies that are differentiated based on patients’ age, language, and cultural backgrounds in order to meet their specific health literacy needs.71 Developing tools that support medical institutions in enhancing their health literacy responsiveness holds significant practical importance.74,75 Additionally, improving doctors’ health literacy capabilities is equally important for promoting doctor-patient communication.72,73 These capabilities are multidimensional, encompassing functional skills (eg, clear communication), communication skills (eg, shared decision-making), and critical skills (eg, patient empowerment).72 Tailoring communication to patients’ health literacy levels may enable them to play an active role as co-producers and make informed health decisions.24 Moreover, this study highlights the crucial role of DMIS in the formation of PL. Customizing decision aids according to the needs of patients with low health literacy can ensure shared decision-making while reducing patients’ cognitive burden.76
Limitations
Despite the achievements of this study, there are still some limitations. First, in terms of sample selection, the samples of this study are limited to medical institutions in specific regions of China. Future studies can expand the scope of samples to cover more different cultural regions and different types of medical institutions to enhance the cultural adaptability and representativeness of the research results. Second, the data collected in this study were obtained through a questionnaire survey, which may be subject to subjective bias and recall bias. Future studies can combine multiple research methods, such as interviews and observation, to obtain more comprehensive and objective data. Third, this study mainly focuses on the direct and mediating effects of CHL. Future research can further explore other potential influencing factors and moderating variables, such as the accessibility of medical services, medical costs, and patients’ social support, to gain a deeper understanding of the complex relationships between these variables. Fourth, this study is a cross-sectional design, and therefore the causal association between variables cannot be fully verified. Future studies could further test and strengthen the causal inference of these hypothesized paths through longitudinal or experimental studies.
Conclusion
Based on SET, this study constructed an integrated model in which CHL affects loyalty through multi-stage resource exchange in the Chinese medical context, and explored the hierarchical transmission logic of “cognitive reserve - capability construction - emotional identification - relational return.” Specifically, EPHL and DMIS demonstrated a chain-related trend between CHL and PL. This finding not only provides a new perspective for understanding the possible formation mechanism of PL but also offers important theoretical support for the construction of health literacy-promoting medical institutions. Future research could test the robustness of this model in cross-cultural samples and explore how to translate it into operational policies and institutional management strategies to promote patient-centered high-quality medical services globally.
Abbreviations
CHL, communicative health literacy; PL, patient loyalty; SET, social exchange theory; EPHL, enhancement of perceived health literacy; DMIS, decision-making involvement satisfaction; CDIS, clinical decision-making involvement and satisfaction; SEM, structural equation modeling; AVE, average variance extracted; CR, composite reliability; GFI, goodness of fit index; CFI, comparative fit index; NFI, normed fit index; RMSEA, root mean square error of approximation; SRMR, standardized root mean square residual; NNFI, non-normed fit index; AGFI, adjusted goodness of fit index.
Data Sharing Statement
Due to privacy restrictions, the datasets used and/or analyzed in this study are available from the corresponding author Renjie Lu (e-mail: [email protected]) upon reasonable request.
Ethical Approval and Consent to Participate
The study was approved by the ethics committee of Changzhou Third People’s Hospital (02A-A2023030). All participants provided informed consent online before the survey, in accordance with the principles of the Helsinki Declaration.
Acknowledgement
The HLS19 instrument used in this research was developed within “The European Health Literacy Population Survey 2019-2021(HLS19)” of M-POHL. Further information regarding the HLS19 instrument can be accessed at: https://m-pohl.net/HLS19Instruments. We also acknowledge the CDIS scale developed by Slade et al65 for providing the theoretical and measurement foundation for this research, and express sincere appreciation for the original authors’ scholarly contributions.
Author Contributions
Yang Chen: Article Submission, Questionnaire Survey, Article Writing, Translation & Proofreading. Yijia He: Data Curation, Formal Analysis, Validation, Conceptualization, Supervision. Shenyu Zhao: Literature Review, Visualization, Writing-Review & Editing. Siyuan Wu: Response to Reviewers, Validation, Writing-Review & Editing. Jing Zhou: Investigation, Writing-Review & Editing. Lingmin Hu: Conceptualization, Methodology, Funding Acquisition & Supervision. Renjie Lu: Research Ideas, Determine Revisions, Review & Funding Acquisition. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Open Research Fund Program of Changzhou Institute for Advanced Study of Public Health, Nanjing Medical University [CPHS202303], and the 2024 Medical Quality (Evidence-Based) Management Research Project of the National Institute of Hospital Administration, National Health Commission of the People’s Republic of China [YLZLXZ24G031], and the Hospital Management Innovation Research Project of Jiangsu Hospital Association in 2023 [JSYGY-3-2023-247], and the Research Project on Policy of Traditional Chinese Medicine for Deepening Reform of Healthcare System in 2024 of the Monitoring and Statistical Research Center of the National Administration of Traditional Chinese Medicine [YGZXKT2024124], and Jiangsu Province Hospital Association Special Research Project on Hospital Pharmaceutical Administration in 2024 [JSYGY-2-2024-YS41], and Jiangsu Pharmaceutical Association - Aosaikang Hospital Pharmacy Research Fund Project in 2024 [A202426], and the 2024 Hospital-level Research Project of Changzhou Third People’s Hospital [SY202433], and Changzhou Soft Science Research Project in 2024 [CR20241102], and Nanjing Medical University Science and Technology Development Fund Project in 2024 [NMUB20240045], and Changzhou Hospital Association Practical Research Project on “Improving Medical Experience and Enhancing Patient Experience” in 2025.
Disclosure
Yang Chen and Yijia He are co-first authors for this study. The authors declare that they have no competing interests in this work.
References
1. Arab M, Tabatabaei SG, Rashidian A, Forushani AR, Zarei E. The Effect of Service Quality on Patient loyalty: a Study of Private Hospitals in Tehran, Iran. Iran J Public Health. 2012;41(9):71–21.
2. Goetz K, Jossen M, Rosemann T, Hess S, Brodowski M, Bezzola P. Is patient loyalty associated with quality of care? Results of a patient survey over primary care in Switzerland. Int J Qual Health Care. 2019;31(3):199–204. doi:10.1093/intqhc/mzy142
3. Hajikhani S, Tabibi SJ, Riahi L. The Relationship Between the Customer Relationship Management and Patients’ Loyalty to Hospitals. Glob J Health Sci. 2015;8(3):65–71. doi:10.5539/gjhs.v8n3p65
4. Alodhialah AM, Almutairi AA, Almutairi M. Key Predictors of Patient Satisfaction and Loyalty in Saudi Healthcare Facilities: a Cross-Sectional Analysis. Healthcare. 2024;12(20):2050. doi:10.3390/healthcare12202050
5. Patrícia Antunes L, Gomes JJ, Cavaco AM. How pharmacist-patient communication determines pharmacy loyalty? Modeling relevant factors. Res Social Adm Pharm. 2015;11(4):560–570. doi:10.1016/j.sapharm.2014.11.003
6. Szabó RM, Buzás N, Braunitzer G, Shedlin MG, Antal M. Factors Influencing Patient Satisfaction and Loyalty as Perceived by Dentists and Their Patients. Dent J. 2023;11(9):203. doi:10.3390/dj11090203
7. Unal O, Akbolat M, Amarat M. The influence of patient-physician communication on physician loyalty and hospital loyalty of the patient. Pak J Med Sci. 2018;34(4):999–1003. doi:10.12669/pjms.344.15136
8. Gao Y, Yang Y, Wang S, Zhang W, Lu J. Has China’s hierarchical medical system improved doctor-patient relationships? Health Econ Rev. 2024;14(1):54. doi:10.1186/s13561-024-00520-8
9. Li X, Xu H, Du F, et al. Does increasing physician volume in primary healthcare facilities under the hierarchical medical system help reduce hospital service utilisation in China? A fixed-effects analysis using province-level panel data. BMJ Open. 2023;13(2):e066375. doi:10.1136/bmjopen-2022-066375
10. Zhang Q, Chen Y. Research on the Present Situation and Countermeasures of Health Human Resources Development at Grass-roots Level in China. BCP Business Management. 2022;25:176–183. doi:10.54691/bcpbm.v25i.1753
11. Chen Y, Wang L, Cui X, et al. COVID-19 as an opportunity to reveal the impact of large hospital expansion on the healthcare delivery system: evidence from Shanghai, China. Ann Transl Med. 2021;9(16):1297. doi:10.21037/atm-21-2793
12. Yang G, Zhang X, Xu Z, Zhang L. Social Medical Insurances, Choices of Medical Institutions and the ‘Siphon Effect’ in the Health Service Market: evidence from 2021 Yangtze River Delta Region of China. Risk Manag Healthc Policy. 2024;17:1287–1299. doi:10.2147/rmhp.S458178
13. Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Q. 2005;83(3):457–502. doi:10.1111/j.1468-0009.2005.00409.x
14. Benecke M, Kasper J, Heesen C, Schäffler N, Reissmann DR. Patient autonomy in dentistry: demonstrating the role for shared decision making. BMC Med Inf Decis Making. 2020;20(1):318. doi:10.1186/s12911-020-01317-5
15. Pun JKH, Chan EA, Wang S, Slade D. Health professional-patient communication practices in East Asia: an integrative review of an emerging field of research and practice in Hong Kong, South Korea, Japan, Taiwan, and Mainland China. Patient Educ Couns. 2018;101(7):1193–1206. doi:10.1016/j.pec.2018.01.018
16. Chung VCH, Lau CH, Wong EMC, Yeoh EK, Griffiths SM. Perceived quality of communication amongst outpatients in western and traditional Chinese medicine clinics in a Chinese population. Health Policy. 2009;90(1):66–72. doi:10.1016/j.healthpol.2008.09.005
17. Liang Z, Xu M, Liu G, Zhou Y, Howard P. Patient-centred care and patient autonomy: doctors’ views in Chinese hospitals. BMC Med Ethics. 2022;23(1):38. doi:10.1186/s12910-022-00777-w
18. Tu J, Kang G, Zhong J, Cheng Y. Outpatient communication patterns in a cancer hospital in China: a qualitative study of doctor-patient encounters. Health Expect. 2019;22(3):594–603. doi:10.1111/hex.12890
19. Zhou W-J, Wan -Q-Q, Liu C-Y, Feng X-L, Shang S-M. Determinants of patient loyalty to healthcare providers: an integrative review. Int J Qual Health Care. 2017;29(4):442–449. doi:10.1093/intqhc/mzx058
20. Liu S, Li G, Liu N, Hongwei W. The Impact of Patient Satisfaction on Patient Loyalty with the Mediating Effect of Patient Trust. Inquiry. 2021;58:469580211007221. doi:10.1177/00469580211007221
21. Yu Y, Chen Z, Zhao Y, Wang Y, Zhang R, Zhou X. Medical service quality, psychological contract, and patient loyalty: an empirical study among patients in China. Medicine. 2020;99(48):e21079. doi:10.1097/md.0000000000021079
22. Rostami M, Ahmadian L, Jahani Y, Niknafs A. The effect of patient satisfaction with academic hospitals on their loyalty. Int J Health Plann Manag. 2019;34(1):e726–e735. doi:10.1002/hpm.2685
23. Caeiros P, Ferreira PP, Chen-Xu J, Francisco R, de Arriaga MT. From Health Communication to Health Literacy: a Comprehensive Analysis of Relevance and Strategies. Port J Public Health. 2024;42(2):159–164. doi:10.1159/000537870
24. Finbråten HS, Nowak P, Griebler R, et al. The HLS(19)-COM-P, a New Instrument for Measuring Communicative Health Literacy in Interaction with Physicians: development and Validation in Nine European Countries. Int J Environ Res Public Health. 2022;19(18):11592. doi:10.3390/ijerph191811592
25. Ishikawa H, Takeuchi T, Yano E. Measuring Functional, Communicative, and Critical Health Literacy Among Diabetic Patients. Diabetes Care. 2008;31(5):874–879. doi:10.2337/dc07-1932
26. Chinn D, McCarthy C. All Aspects of Health Literacy Scale (AAHLS): developing a tool to measure functional, communicative and critical health literacy in primary healthcare settings. Patient Educ Couns. 2013;90(2):247–253. doi:10.1016/j.pec.2012.10.019
27. Li Y, Lv X, Liang J, Dong H, Chen C. The development and progress of health literacy in China. Front Public Health. 2022;10:1034907. doi:10.3389/fpubh.2022.1034907
28. Wu Q, Jin Z, Wang P. The Relationship Between the Physician-Patient Relationship, Physician Empathy, and Patient Trust. J Gen Intern Med. 2022;37(6):1388–1393. doi:10.1007/s11606-021-07008-9
29. Ishikawa H, Yano E, Fujimori S, et al. Patient health literacy and patient–physician information exchange during a visit. Family Practice. 2009;26(6):517–523. doi:10.1093/fampra/cmp060
30. Estrela M, Semedo G, Roque F, Ferreira PL, Herdeiro MT. Sociodemographic determinants of digital health literacy: a systematic review and meta-analysis. Int J Med Inform. 2023;177:105124. doi:10.1016/j.ijmedinf.2023.105124
31. Nejati B, Lin -C-C, Aaronson NK, et al. Determinants of satisfactory patient communication and shared decision making in patients with multiple myeloma. Psycho-Oncology. 2019;28(7):1490–1497. doi:10.1002/pon.5105
32. Xu RH, Zhou LM, Wong EL, Wang D. The Association Between Patients’ eHealth Literacy and Satisfaction With Shared Decision-making and Well-being: multicenter Cross-sectional Study. J Med Internet Res. 2021;23(9):e26721. doi:10.2196/26721
33. Sieck CJ, Sheon A, Ancker JS, Castek J, Callahan B, Siefer A. Digital inclusion as a social determinant of health. Npj Digital Med. 2021;4(1):52. doi:10.1038/s41746-021-00413-8
34. Ahmad R, Nawaz MR, Ishaq MI, Khan MM, Ashraf HA. Social exchange theory: systematic review and future directions. Front Psychol. 2022;13:1015921. doi:10.3389/fpsyg.2022.1015921
35. Foa EB, Foa UG. Resource theory: interpersonal behavior as exchange. In: Social Exchange: Advances in Theory and Research. Springer; 1980:77–94.
36. Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promotion Int. 2000;15(3):259–267. doi:10.1093/heapro/15.3.259
37. Sørensen K, Van den Broucke S, Fullam J, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12(1):80. doi:10.1186/1471-2458-12-80
38. Muscat DM, Shepherd HL, Nutbeam D, Trevena L, McCaffery KJ. Health Literacy and Shared Decision-making: exploring the Relationship to Enable Meaningful Patient Engagement in Healthcare. J Gen Intern Med. 2021;36(2):521–524. doi:10.1007/s11606-020-05912-0
39. Ilardo ML, Speciale A. The Community Pharmacist: perceived Barriers and Patient-Centered Care Communication. Int J Environ Res Public Health. 2020;17(2):536. doi:10.3390/ijerph17020536
40. Friedman DB, Hoffman-Goetz L, Arocha JF. Health literacy and the World Wide Web: comparing the readability of leading incident cancers on the Internet. Med Inform Internet Med. 2006;31(1):67–87. doi:10.1080/14639230600628427
41. Huang C, Plummer V, Lam L, Cross W. Translation and psychometric testing of a decision-making scale. J Psychiatr Ment Health Nurs. 2020;27(5):533–542. doi:10.1111/jpm.12601
42. Chen X, Zhao W, Yuan J, Qin W, Zhang Y, Zhang Y. The Relationships Between Patient Experience with Nursing Care, Patient Satisfaction and Patient Loyalty: a Structural Equation Modeling. Patient Prefer Adherence. 2022;16:3173–3183. doi:10.2147/ppa.S386294
43. Rüegg R. Decision-Making Ability: a Missing Link Between Health Literacy, Contextual Factors, and Health. Health Lit Res Pract. 2022;6(3):e213–e223. doi:10.3928/24748307-20220718-01
44. Wang KY, Chu NF, Lin SH, Chiang IC, Perng WC, Lai HR. Examining the causal model linking health literacy to health outcomes of asthma patients. J Clin Nurs. 2014;23(13–14):2031–2042. doi:10.1111/jocn.12434
45. Xiao L, Miao J, Peng M, et al. The effect of health literacy on patient’s perceived shared decision-making among Chinese cancer patients. Psychooncology. 2022;31(1):70–77. doi:10.1002/pon.5777
46. van Driel AG, Maghroudi E, van der Klis A, et al. Considering health literacy in communication about medications between nurses and patients with heart failure: a cross sectional observational study. Patient Educ Couns. 2025;135:108709. doi:10.1016/j.pec.2025.108709
47. Dinh TTH, Bonner A. Exploring the relationships between health literacy, social support, self-efficacy and self-management in adults with multiple chronic diseases. BMC Health Serv Res. 2023;23(1):923. doi:10.1186/s12913-023-09907-5
48. Shan Y, Ji M, Xing Z, Dong Z. Factors Associated With Limited Cancer Health Literacy Among Chinese People: cross-sectional Survey Study. JMIR Form Res. 2023;7:e42666. doi:10.2196/42666
49. Chen D, Zhou Q, Pratt CB, Su Z, Gu Z. Investigating the Relationships Between Public Health Literacy and Public Trust in Physicians in China’s Control of COVID-19: a Cross-Sectional Study. Front Public Health. 2021;9:758529. doi:10.3389/fpubh.2021.758529
50. Tulinayo FP, Ortega-Gil A, González N, et al. Understanding Complexities in Collaborative Management of Knowledge on Advance Care Planning for Multi-morbid Patients Within Personalized Integrated Care. J Healthc Inform Res. 2025;9(2):220–245. doi:10.1007/s41666-025-00185-w
51. Li L, Zhang Q, Zhu L, et al. Patients’ loyalty to primary care institutions and associated factors in China: a cross-sectional study. BMC Health Serv Res. 2025;25(1):162. doi:10.1186/s12913-025-12244-4
52. Schillinger D, McNamara D, Crossley S, et al. The Next Frontier in Communication and the ECLIPPSE Study: bridging the Linguistic Divide in Secure Messaging. J Diabetes Res. 2017;2017:1348242. doi:10.1155/2017/1348242
53. Williams MV, Davis T, Parker RM, Weiss BD. The role of health literacy in patient-physician communication. Fam Med. 2002;34(5):383–389.
54. Al-Adhami M, Durbeej N, Daryani A, Wångdahl J, Larsson EC, Salari R. Can extended health communication improve newly settled refugees’ health literacy? A quasi-experimental study from Sweden. Health Promot Int. 2024;39(2):15. doi:10.1093/heapro/daae015
55. Cesar FCR, Oliveira L, Galvão MC, Lacerda ALA. How Do Healthcare Professionals Develop the Communication Process to Promote Patients’ Health Literacy? Int J Environ Res Public Health. 2024;21(5):536. doi:10.3390/ijerph21050536
56. Pel-Littel RE, Buurman BM, Minkman MM, Scholte op Reimer WJM, Twisk JWR, van Weert JCM. The influence of health literacy, anxiety and education on shared decision making and decisional conflict in older adults, and the mediating role of patient participation: a video observational study. Patient Educ Couns. 2024;124:108274. doi:10.1016/j.pec.2024.108274
57. Edwards M, Wood F, Davies M, Edwards A. The development of health literacy in patients with a long-term health condition: the health literacy pathway model. BMC Public Health. 2012;12(1):130. doi:10.1186/1471-2458-12-130
58. Britten N, Ekman I, Naldemirci Ö, Javinger M, Hedman H, Wolf A. Learning from Gothenburg model of person centred healthcare. BMJ. 2020;370:m2738. doi:10.1136/bmj.m2738
59. Fatima T, Malik SA, Shabbir A. Hospital healthcare service quality, patient satisfaction and loyalty: an investigation in context of private healthcare systems. Int J Qual Reliab Manage. 2018;35(6):1195–1214. doi:10.1108/IJQRM-02-2017-0031
60. Wartiningsih M, Supriyanto S, Widati S, Ernawaty E, Lestari R. Health promoting hospital: a practical strategy to improve patient loyalty in public sector. J Public Health Res. 2020;9(2):1832. doi:10.4081/jphr.2020.1832
61. Tsai TI, Yu WR, Lee SD. Is health literacy associated with greater medical care trust? Int J Qual Health Care. 2018;30(7):514–519. doi:10.1093/intqhc/mzy043
62. Liang CY, Wang KY, Hwang SJ, Lin KC, Pan HH. Factors affecting the physician-patient relationship of older veterans with inadequate health literacy: an observational study. Br J Gen Pract. 2013;63(610):e354–60. doi:10.3399/bjgp13X667222
63. Baker DW. The meaning and the measure of health literacy. J Gen Intern Med. 2006;21(8):878–883. doi:10.1111/j.1525-1497.2006.00540.x
64. Nutbeam D. The evolving concept of health literacy. Soc sci med. 2008;67(12):2072–2078. doi:10.1016/j.socscimed.2008.09.050
65. Slade M, Jordan H, Clarke E, et al. The development and evaluation of a five-language multi-perspective standardised measure: clinical decision-making involvement and satisfaction (CDIS). BMC Health Serv Res. 2014;14(1):1–15. doi:10.1186/1472-6963-14-323
66. Huang IC, Du PL, Lin LS, Liu TY, Lin TF, Huang WC. The Effect of Perceived Value, Trust, and Commitment on Patient Loyalty in Taiwan. Inquiry. 2021;58:469580211007217. doi:10.1177/00469580211007217
67. Muscat DM, Cvejic E, Smith J, et al. Equity in Choosing Wisely and beyond: the effect of health literacy on healthcare decision-making and methods to support conversations about overuse. BMJ Qual Saf. 2025;34(4):213–222. doi:10.1136/bmjqs-2024-017411
68. Vidnes TK, Wahl AK, Larsen MH, Meyer KB, Hermansen Å, Andersen MH. Two-Year Follow-Up of a Communication Intervention on Medication Adherence and Health Literacy in Kidney Transplanted Recipients-A Randomised Controlled Study. J Ren Care. 2025;51(1):e70010. doi:10.1111/jorc.70010
69. Chau RC, Thu KM, Hsung RT, McGrath C, Lam WY. Self-monitoring of Oral Health Using Smartphone Selfie Powered by Artificial Intelligence: implications for Preventive Dentistry. Oral Health Prev Dent. 2024;22:327–340. doi:10.3290/j.ohpd.b5758200
70. Deniz-Garcia A, Fabelo H, Rodriguez-Almeida AJ, et al. Quality, Usability, and Effectiveness of mHealth Apps and the Role of Artificial Intelligence: current Scenario and Challenges. J Med Internet Res. 2023;25:e44030. doi:10.2196/44030
71. Smith G, Lui SF, Kalantar-Zadeh K, Bonner A. The Shift from Individual to Organizational Health Literacy: implications for Kidney Healthcare Leaders and Clinicians. Nephron. 2024;148(5):349–356. doi:10.1159/000534073
72. Chang CC, Tseng PL, Liu CC, Ming JL, Fan SH, Tung CY. Development and validation of the Physician’s Health Literacy Competence Scale: a step towards effective doctor-patient communication. Medicine. 2025;104(9):e41643. doi:10.1097/md.0000000000041643
73. Liu C, Chen Z, Qin H, et al. Health Knowledge Acquisition and Health Communication Ability of Nurses: a Chain Mediating Model of Health Literacy and Health Education Competence. J Adv Nurs. 2025;81(9):5903–5913. doi:10.1111/jan.16728
74. Elisabeth Stømer U, Klopstad Wahl A, Gunnar Gøransson L, Hjorthaug Urstad K. Health Literacy in Kidney Disease: associations with Quality of Life and Adherence. J Ren Care. 2020;46(2):85–94. doi:10.1111/jorc.12314
75. Trezona A, Dodson S, Osborne RH. Development of the Organisational Health Literacy Responsiveness (Org-HLR) self-assessment tool and process. BMC Health Serv Res. 2018;18(1):694. doi:10.1186/s12913-018-3499-6
76. Richter R, Jansen J, van der Kraan J, et al. How Inclusive Are Patient Decision Aids for People with Limited Health Literacy? An Analysis of Understandability Criteria and the Communication about Options and Probabilities. Med Decis Making. 2025;45(2):143–155. doi:10.1177/0272989x241302288
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.