Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
The Red Cell Distribution Width-to-Albumin Ratio Predicts 1-Year Mortality in Patients with Chronic Obstructive Pulmonary Disease: Evidence From MIMIC-IV and NHANES
Authors Sheng P ![]() , Lei W, Cheng T, Deng Y, Li Y, Wu Z, Liu B
, Lei W, Cheng T, Deng Y, Li Y, Wu Z, Liu B
Received 30 May 2025
Accepted for publication 12 September 2025
Published 1 October 2025 Volume 2025:20 Pages 3351—3360
DOI https://doi.org/10.2147/COPD.S543479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jill Ohar
Pengcheng Sheng,1 Wanqi Lei,1 Tanyun Cheng,1 Yaoting Deng,2 Yeshan Li,3 Zhaoyan Wu,3 Bangzhu Liu1,3
1Bengbu Medical University, Bengbu, Anhui, People’s Republic of China; 2Gansu University of Chinese Medicine, Lanzhou, Gansu, People’s Republic of China; 3The Second People’s Hospital of Wuhu, Wuhu, Anhui, People’s Republic of China
Correspondence: Bangzhu Liu, The Second People’s Hospital of Wuhu, Wuhu, Anhui, People’s Republic of China, Email [email protected]
Purpose: The red blood cell distribution width-to-albumin ratio (RAR) is an emerging biomarker that reflects systemic inflammation and nutritional status. However, its prognostic value in patients with chronic obstructive pulmonary disease (COPD) remains unclear. This study aimed to evaluate the predictive value of RAR for 1-year all-cause mortality in patients with COPD and to explore its clinical relevance.
Patients and methods: We conducted a retrospective analysis using two independent cohorts: hospitalized COPD patients from the MIMIC-IV database (2008– 2019, n = 2649) and community-dwelling individuals with COPD from the NHANES database (2003– 2018, n = 2415). RAR levels were stratified into quartiles (Q1–Q4). Multivariable logistic regression models were used to examine the association between RAR and 1-year all-cause mortality. Generalized additive models (GAMs) assessed nonlinear relationships. Receiver operating characteristic (ROC) analysis evaluated the predictive performance of RAR compared with other markers such as NLR, PLR, and RDW.
Results: Higher RAR levels were independently associated with an increased risk of 1-year all-cause mortality in patients with COPD. In the MIMIC-IV cohort, the highest quartile (Q4) had an OR of 7.90 (95% CI: 6.05– 10.32; P < 0.001) compared to Q1. In the NHANES cohort, the OR for Q4 was 11.16 (95% CI: 4.42– 28.18; P < 0.001). ROC analysis revealed that RAR achieved a higher area under the curve (AUC) (0.801 in MIMIC-IV and 0.787 in NHANES) than other markers, indicating superior discriminatory ability.
Conclusion: RAR serves as an independent predictor of 1-year all-cause mortality in patients with COPD. By integrating indicators of systemic inflammation and nutritional status, RAR provides a reliable tool for clinical risk stratification.
Keywords: chronic obstructive pulmonary disease, red blood cell distribution width-to-albumin ratio, all-cause mortality
Chronic obstructive pulmonary disease (COPD) is a chronic condition characterized by persistent airway obstruction, with high global prevalence and mortality rates, posing a significant public health challenge. COPD is currently the third leading cause of death worldwide and severely impacts patients’ quality of life and life expectancy.1 Due to its heterogeneous nature, the disease progression and prognosis of COPD vary significantly among individuals. Early identification of high-risk patients is therefore essential for optimizing management strategies and improving outcomes. Despite the availability of several biomarkers, there remains a lack of integrated indicators that simultaneously reflect both systemic inflammation and nutritional status in COPD. Inflammation and nutritional status play critical roles in the development, progression, and prognostic evaluation of COPD.2
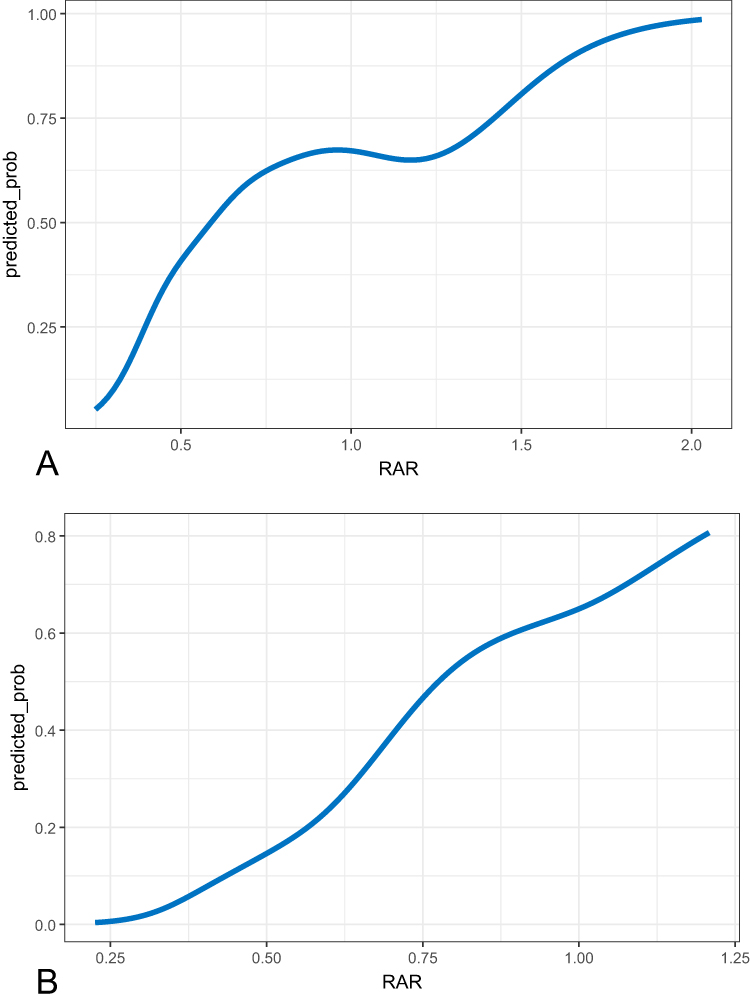 |
Figure 1 Relationship between the RAR value and the 1-year mortality probability in patients with chronic obstructive pulmonary disease (COPD). Panels (A) (MIMIC database) and (B) (NHANES database) depict smoothed curves fitted using generalized additive models (GAMs). The x-axis (RAR) represents the range of RAR values, while the y-axis (predicted probability) indicates the model-estimated 1-year mortality probability. The curve reflects the association between RAR values and mortality risk; a steeper slope suggests a more substantial change in predicted risk. |
In recent years, several inflammatory markers, such as the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR), have been widely used to assess systemic inflammation in COPD patients.3–9 Meanwhile, serum albumin level, as an indicator of nutritional status, has also been associated with disease severity and mortality risk. Red cell distribution width (RDW), a measure of the variability in red blood cell size, has been linked to systemic inflammation and poor prognosis in various chronic diseases. The red cell distribution width-to-albumin ratio (RAR) is a composite index that reflects both inflammatory and nutritional status simultaneously. This index combines RDW, which tends to increase under inflammatory and hypoxic conditions, and albumin, which decreases in malnourished or catabolic states, making RAR a potentially useful prognostic indicator. Previous studies have demonstrated the prognostic value of RAR in a variety of diseases.10–16 However, evidence regarding its predictive value for all-cause mortality in COPD remains limited, and large-scale, multicenter database studies to validate its clinical utility are still lacking.
Therefore, in this study, we utilized two authoritative databases (MIMIC-IV and NHANES) to systematically evaluate the predictive value of RAR for 1-year mortality risk in patients with COPD. We also compared RAR with other established inflammatory and nutritional indicators, aiming to provide a novel and practical tool for the clinical assessment and management of COPD patients.
Materials and Methods
Data Sources and Study Population
The MIMIC-IV database contains data on hospitalized patients from the Beth Israel Deaconess Medical Center between 2008 and 2019. Patients diagnosed with chronic obstructive pulmonary disease (COPD) were identified based on the International Classification of Diseases, Ninth and Tenth Revisions (ICD-9 codes: 49120, 49,121, 49122, and 496; ICD-10 codes: J44, J440, J441, and J449). After excluding individuals with missing data, a total of 2,649 patients were included. Baseline information from the patients’ first hospitalization, including age, sex, and laboratory test results, was extracted to assess 1-year mortality risk.
The NHANES database provides health data from a nationally representative sample of the US population collected between 2003 and 2018. COPD diagnosis was based on a positive response to at least one of the following questions in the NHANES medical condition questionnaire: “Has a doctor ever told you that you had COPD?”, “Has a doctor ever told you that you had chronic bronchitis?”, or “Has a doctor ever told you that you had emphysema?”. This diagnostic method has been validated in several previous studies using NHANES data.17–19 Participants with a COPD diagnosis and available 1-year follow-up data were included, resulting in a total of 2,415 individuals. Demographic characteristics, clinical diagnoses, and laboratory measurements were collected. The primary variable of interest was the red cell distribution width-to-albumin ratio (RAR). Additional markers included the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), systemic immune-inflammation index (SII), and systemic inflammation response index (SIRI).
Methods
To evaluate the association between the red cell distribution width-to-albumin ratio (RAR) and 1-year mortality risk, RAR was categorized into quartiles (Q1–Q4). Logistic regression models were used to assess this association, and odds ratios (ORs) with corresponding 95% confidence intervals (CIs) were reported. A trend test (P for trend) was performed to examine dose–response relationships across quartiles. To explore potential nonlinear associations between RAR and mortality probability, a generalized additive model (GAM) was fitted and visualized.
Receiver operating characteristic (ROC) curves were used to evaluate the predictive performance of RAR, and the area under the curve (AUC), Youden index, sensitivity, and specificity were calculated for both the unadjusted model (Crude model) and the model adjusted for age and sex (Model 1). Comparative analyses were also performed with other inflammatory markers. Continuous variables were summarized as mean ± standard deviation, and categorical variables were expressed as counts and percentages. All statistical analyses were conducted using R software (version 4.4.1), and two-sided P-values < 0.05 were considered statistically significant.
Definitions of Inflammatory Markers
RAR (Red Cell Distribution Width-to-Albumin Ratio): Calculated by dividing the red cell distribution width (RDW) by the serum albumin concentration.
NLR (Neutrophil-to-Lymphocyte Ratio): Calculated as the neutrophil count divided by the lymphocyte count.
PLR (Platelet-to-Lymphocyte Ratio): Calculated as the platelet count divided by the lymphocyte count.
MLR (Monocyte-to-Lymphocyte Ratio): Calculated as the monocyte count divided by the lymphocyte count.
Systemic Immune-Inflammation Index (SII): Defined as the neutrophil count multiplied by the platelet count and divided by the lymphocyte count, ie, (neutrophil count × platelet count) / lymphocyte count.
Systemic Inflammation Response Index (SIRI): Defined as the neutrophil count multiplied by the monocyte count and divided by the lymphocyte count, ie, (neutrophil count × monocyte count) / lymphocyte count.
Results
Baseline Characteristics
In the MIMIC-IV cohort (N = 2,649), the mean age was 69 ± 16 years in the survival group and 74 ± 15 years in the mortality group, with a statistically significant difference (P < 0.001). There was no significant difference in sex distribution between the survival and mortality groups (P = 0.16). Among males, 868 survived and 533 died; among females, 807 survived and 441 died. The red cell distribution width (RDW) was 14.6 ± 2.5 in the survival group and 15.5 ± 3.2 in the mortality group (P < 0.001). Serum albumin (ALB) was 34 ± 9 g/L in the survival group and 30 ± 8 g/L in the mortality group, also showing a significant difference (P < 0.001).
In the NHANES cohort (N = 2,415), the mean age was 63 ± 20 years in the survival group and 73 ± 14 years in the mortality group (P < 0.001). A significant difference in sex distribution was observed between the two groups (P = 0.002). Among males, 1,007 survived and 60 died; among females, 1,307 survived and 41 died. RDW was 13.4 ± 1.6 in the survival group and 14.3 ± 2.2 in the mortality group (P < 0.001). ALB was 41 ± 4 g/L in the survival group and 39 ± 5 g/L in the mortality group (P < 0.001) (Table 1).
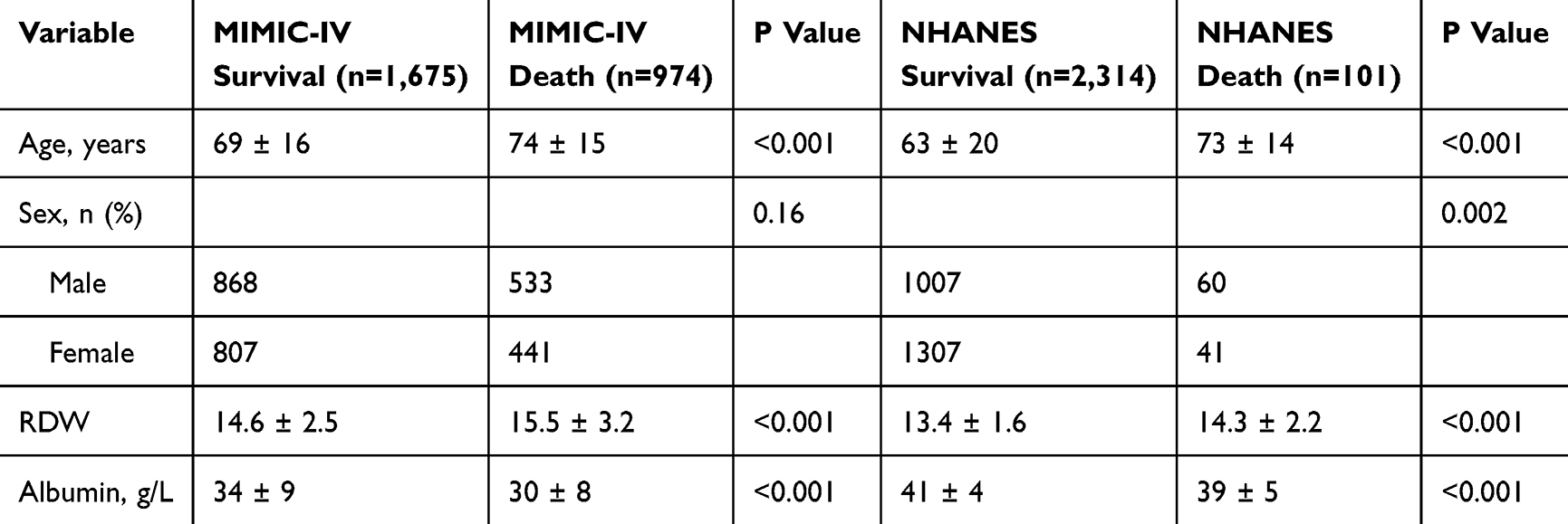 |
Table 1 Baseline Characteristics of Participants in the MIMIC-IV and NHANES Cohorts |
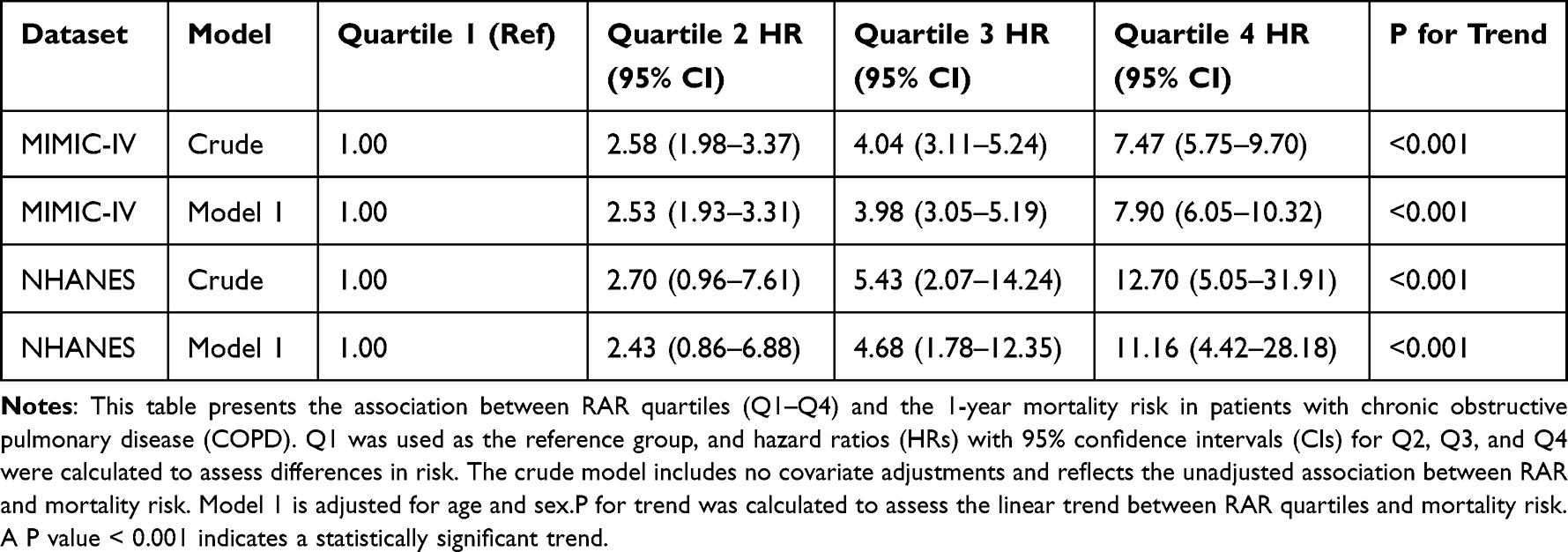 |
Table 2 Association Between RAR Quartiles and 1-Year Mortality in COPD Patients in the MIMIC-IV and NHANES Cohorts |
Association Between RAR and 1-Year Mortality Risk in COPD Patients
In the MIMIC-IV cohort, compared with the lowest RAR quartile (Q1, reference), patients in quartiles Q2, Q3, and Q4 had hazard ratios (HRs) of 2.58 (95% CI: 1.98–3.37), 4.04 (95% CI: 3.11–5.24), and 7.47 (95% CI: 5.75–9.70), respectively, in the unadjusted (crude) model (P for trend < 0.001). After adjusting for age and sex (Model 1), the HRs remained statistically significant at 2.53 (95% CI: 1.93–3.31), 3.98 (95% CI: 3.05–5.19), and 7.90 (95% CI: 6.05–10.32), respectively (P for trend < 0.001).
A similar trend was observed in the NHANES cohort. In the crude model, the HRs for Q2, Q3, and Q4 were 2.70 (95% CI: 0.96–7.61), 5.43 (95% CI: 2.07–14.24), and 12.70 (95% CI: 5.05–31.91), respectively (P for trend < 0.001). After adjusting for age and sex, the HRs remained elevated at 2.43 (95% CI: 0.86–6.88), 4.68 (95% CI: 1.78–12.35), and 11.16 (95% CI: 4.42–28.18), respectively (P for trend < 0.001) (Table 2).
In addition, generalized additive models (GAMs) were applied to further confirm this association. Both cohorts showed a consistent positive association between higher RAR values and increased 1-year mortality risk (Figure 1).
Predictive Performance of RAR for 1-Year Mortality in COPD Patients
Univariate predictive models were applied using both the MIMIC-IV and NHANES datasets to evaluate the ability of various inflammatory markers to predict 1-year mortality in patients with chronic obstructive pulmonary disease (COPD). RAR consistently demonstrated the highest predictive performance in both datasets. In the MIMIC-IV dataset, the area under the receiver operating characteristic curve (AUC) for RAR was 0.697, which was notably higher than that of other markers (NLR: 0.618; MLR: 0.614; PLR: 0.551; SII: 0.569; SIRI: 0.605; RDW: 0.627; ALB: 0.678). Similarly, in the NHANES dataset, the AUC of RAR was 0.733, again exceeding those of other markers (NLR: 0.684; MLR: 0.675; PLR: 0.614; SII: 0.639; SIRI: 0.682; RDW: 0.697; ALB: 0.680).
After adjusting for age and sex, the predictive ability of RAR further improved, with AUCs increasing to 0.724 in the MIMIC-IV dataset and 0.787 in the NHANES dataset, indicating its stability and reliability in predicting mortality risk in COPD (Figure 2). Sensitivity and specificity were also assessed for each univariate model. RAR-containing models consistently demonstrated stronger discriminatory capacity and greater clinical applicability than other biomarkers (Table 3).
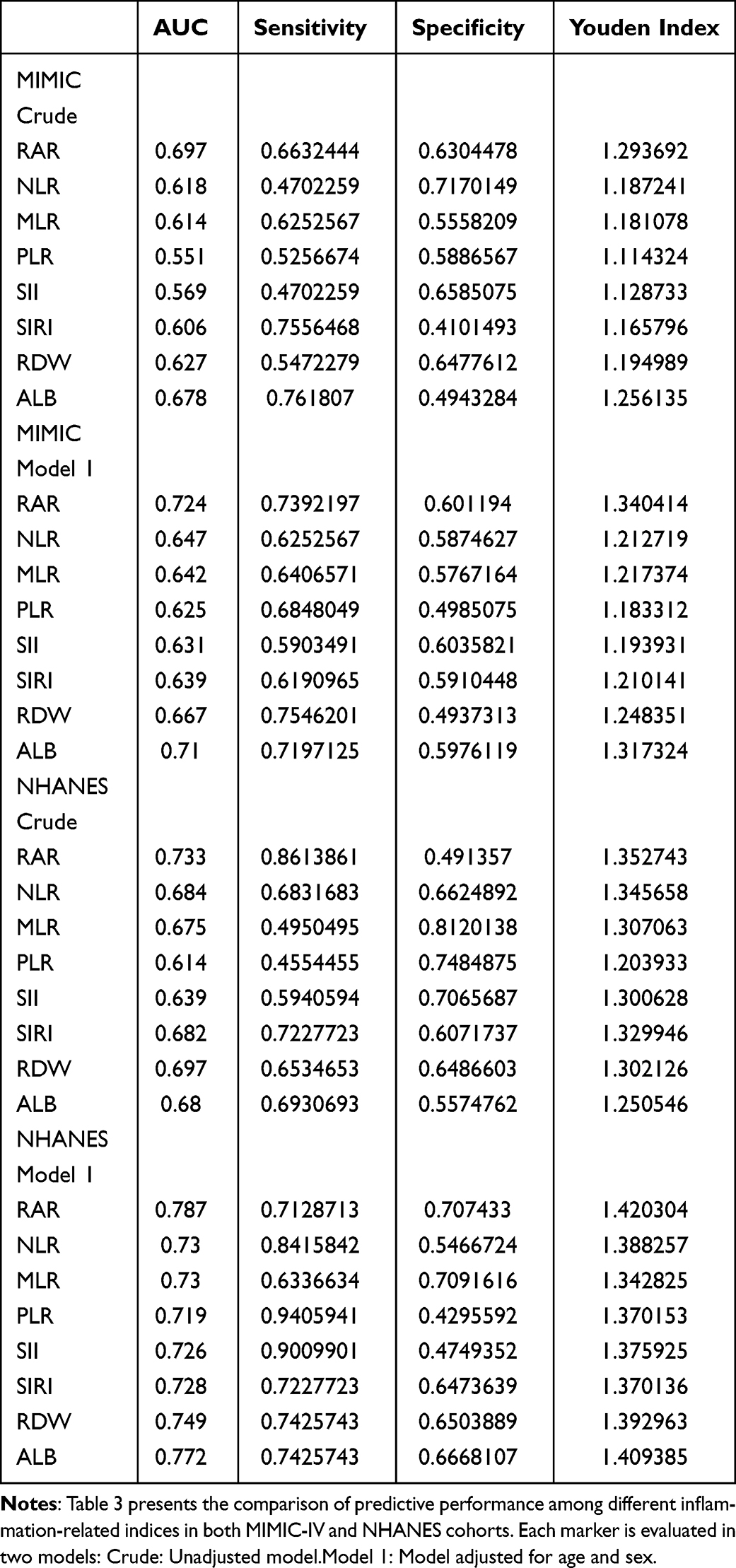 |
Table 3 Comparison of the Youden Index, Sensitivity, and Specificity |
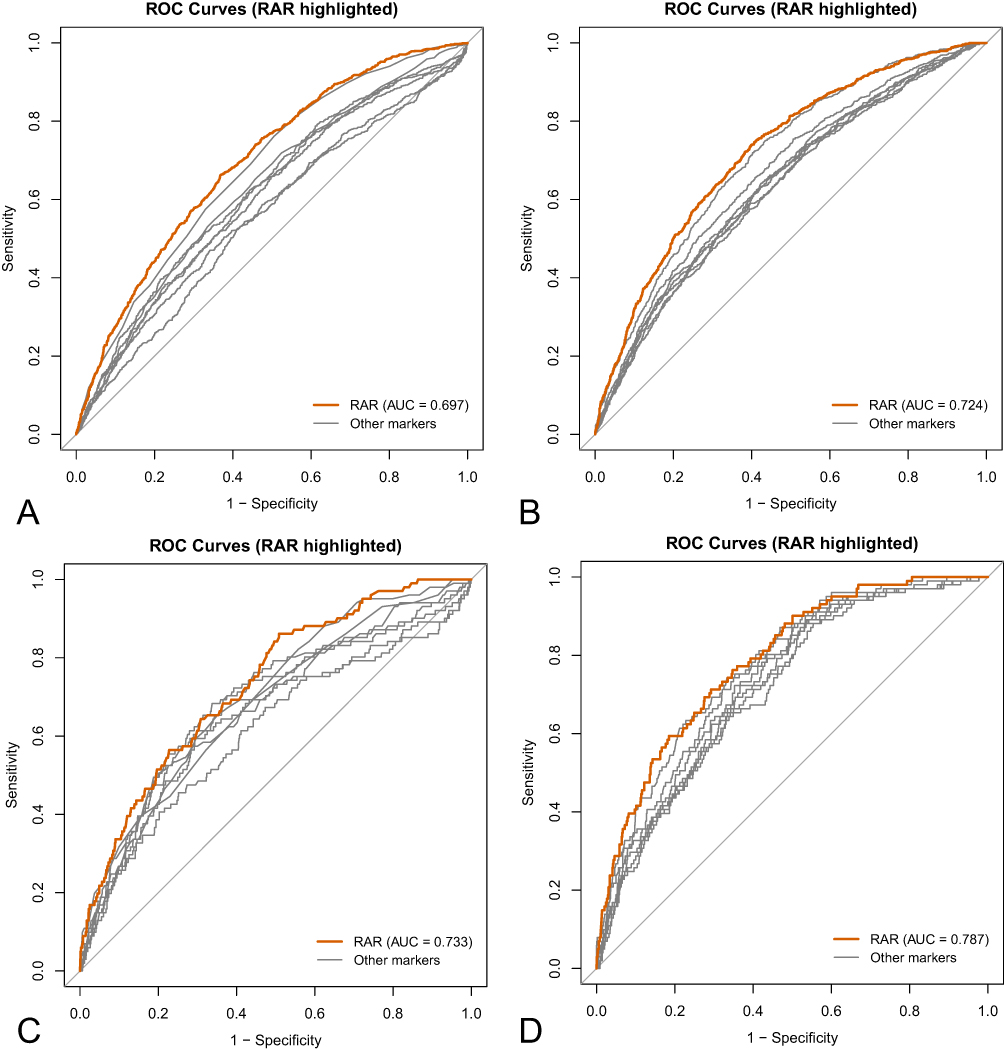 |
Figure 2 Panels (A) and (B) show the receiver operating characteristic (ROC) curves based on the MIMIC database: Panel (A) presents the univariate model, and Panel (B) displays the model adjusted for age and sex. Panels (C) and (D) display the corresponding results derived from the NHANES database. |
Multivariate models with and without RAR were further compared. In the MIMIC-IV dataset, the inclusion of RAR improved the AUC to 0.731, compared with 0.652 for the model without RAR. Similarly, in the NHANES dataset, the model including RAR achieved an AUC of 0.801, outperforming the model without RAR (AUC = 0.737) (Figure 3). These results collectively support the added value of RAR in enhancing predictive accuracy and facilitating more precise risk stratification.
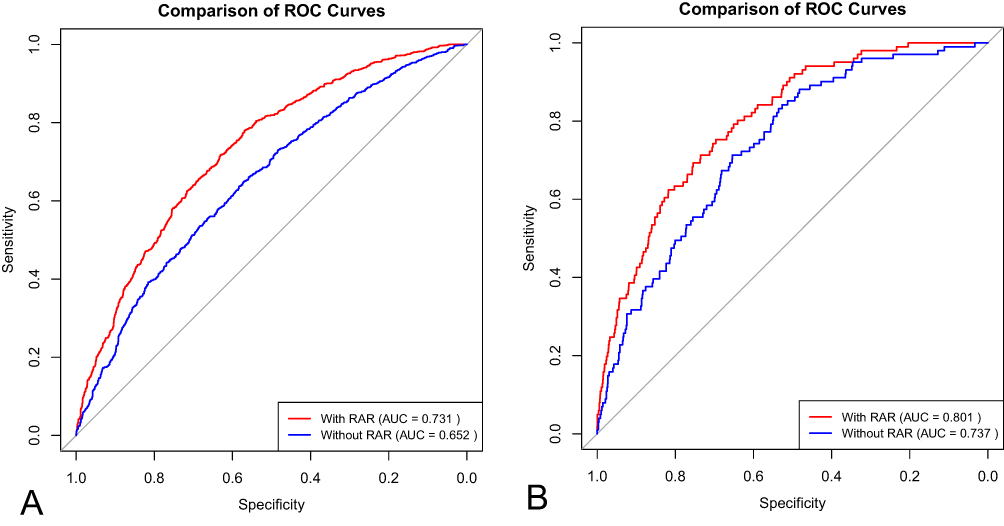 |
Figure 3 Panels (A) (MIMIC database) and (B) (NHANES database) illustrate ROC curves generated from two datasets to compare the contribution of RAR to model predictive performance. The model including RAR consisted of seven variables: age, sex, RAR, neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), platelet-to-lymphocyte ratio (PLR), systemic immune-inflammation index (SII), and systemic inflammation response index (SIRI). The model excluding RAR contained the same covariates except RAR. The x-axis (1 − Specificity) represents the false positive rate, and the y-axis (Sensitivity) indicates the true positive rate. The red curve (With RAR) represents the model that includes the RAR variable, while the blue curve (Without RAR) corresponds to the model without the RAR variable. The area under the curve (AUC) quantifies the model’s discriminatory ability; a larger AUC indicates better predictive performance. |
To evaluate the correlation between inflammatory markers, Spearman correlation heatmaps were generated for both datasets (Figure 4). The results consistently revealed weak correlations between RAR and other markers, indicating low collinearity. This suggests that RAR may reflect a relatively independent inflammatory profile, supporting its potential role as an independent predictor of 1-year mortality in COPD patients.
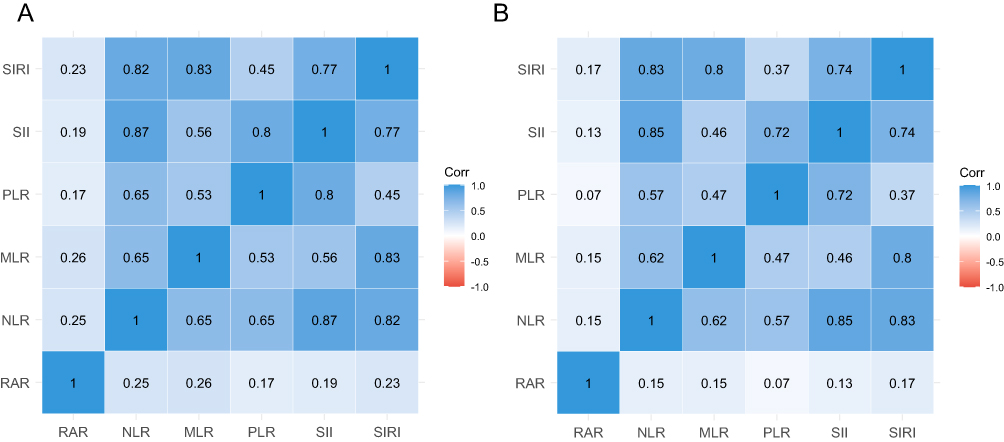 |
Figure 4 Panels (A) and (B) show the Spearman correlation coefficients among variables in the MIMIC and NHANES datasets, respectively. The color intensity indicates the strength of correlation, with blue representing positive correlations and red indicating negative correlations. The color bar represents the range of correlation coefficients, from −1 to 1. |
Discussion
Using data from two large-scale cohorts, MIMIC-IV and NHANES, we systematically evaluated the association between the red cell distribution width-to-albumin ratio (RAR) and 1-year mortality in patients with chronic obstructive pulmonary disease (COPD). The results showed that RAR significantly outperformed other commonly used inflammation-related indices, including the neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), systemic immune-inflammation index (SII), and systemic inflammation response index (SIRI), in predicting mortality risk among COPD patients. These findings provide robust evidence for the prognostic value of RAR across distinct clinical settings.
During the pathophysiological progression of COPD, elevated red cell distribution width (RDW) is often closely associated with chronic inflammation20,21 and hypoxic states.22,23 Previous studies have suggested that malnutrition may also contribute to increased RDW24,25 and decreased albumin levels. Systemic inflammation and chronic hypoxemia stimulate the secretion of erythropoietin (EPO), accelerating erythropoiesis and red blood cell release.26 Under EPO stimulation, the bone marrow may release immature reticulocytes with larger volumes, thereby increasing RDW. Inflammatory cytokines can additionally impair erythrocyte membrane integrity, resulting in greater red blood cell volume heterogeneity.27 At the same time, malnutrition contributes to reduced albumin levels,28 and inflammatory mediators further suppress hepatic albumin synthesis.29,30 The combined effects of chronic hypoxia and inadequate nutritional intake aggravate this imbalance, ultimately leading to elevated RAR levels. Increased RAR may thus reflect a systemic disturbance involving inflammation, oxygenation, and nutrition, which is particularly relevant in COPD.
In both the critically ill population from the MIMIC-IV database and the community-based population from the NHANES database, RAR consistently demonstrated superior predictive performance for 1-year mortality compared to traditional inflammatory markers such as NLR and PLR. This consistent performance across distinct cohorts highlights the added value of combining inflammatory and nutritional information in a single index, and supports RAR’s robustness and generalizability as a prognostic biomarker in COPD.
From a clinical perspective, RAR may complement established prognostic tools such as the GOLD classification and BODE index. Its low cost, ease of measurement, and availability in routine laboratory testing make it an attractive option for early risk stratification and personalized management of COPD patients. Incorporating RAR into existing prognostic models may help clinicians better identify high-risk patients and optimize therapeutic decisions.
Nevertheless, several limitations should be noted. First, the retrospective design precludes causal inference. Second, although multivariable adjustments were applied, the possibility of residual confounding cannot be excluded. Third, both MIMIC-IV (2008–2019) and NHANES (2003–2018) datasets represent relatively old cohorts, and advances in COPD management in recent years may influence generalizability. Future studies should therefore validate these findings in large-scale, prospective, multicenter cohorts with updated data. In addition, mechanistic studies are warranted to further elucidate the role of RAR in inflammatory regulation, nutritional metabolism, and erythropoiesis. Such work may help clarify the pathophysiological basis of RAR and promote its application in early intervention and individualized treatment for COPD. Lastly, in the MIMIC-IV cohort, we could not distinguish whether hospital admissions were due to acute exacerbation of COPD (AECOPD) or other comorbid conditions, such as infection, heart failure, or procedural indications. This heterogeneity may have introduced residual confounding, particularly if certain causes disproportionately affected RDW or albumin levels. Such bias may have amplified the observed association between RAR and mortality. Future studies using datasets with detailed clinical notes or admission diagnoses are needed to confirm our findings in more homogenous COPD subgroups.
Conclusion
In conclusion, our study demonstrates that the red cell distribution width-to-albumin ratio (RAR) is a robust and independent predictor of 1-year mortality in patients with COPD. Given its accessibility and integrative reflection of inflammation and nutritional status, RAR may serve as a valuable tool in clinical risk stratification and decision-making.
Ethics Statement
This study used publicly available and de-identified human data, which contained no information that could identify individual participants. According to Article 32 (Items 1 and 2) of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects issued by the National Health Commission of China on February 18, 2023, such research is exempt from ethical review. Therefore, approval from an ethics committee was not required for this study.
Acknowledgments
This work was funded by the following projects:
- Wuhu Science and Technology Projects (2022jc76).
- Key Project Funding from Wuhu Health Commission (WHWJ2023z014).
- Anhui Provincial Health Commission General Project (AHWJ2023A20165).
The authors acknowledge the use of ChatGPT (version 4.0) for language polishing. No AI tools were used for data analysis, result interpretation, or content generation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Agustí A, Celli BR, Criner GJ, et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Am J Respir Crit Care Med. 2023;207(7):819–837. doi:10.1164/rccm.202301-0106PP
2. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011
3. Leung C, Sin DD. NLR in CBC: a holy grail for biomarker research in COPD? Respirology. 2023;28(12):1095–1097. doi:10.1111/resp.14597
4. Cai C, Zeng W, Wang H, Ren S. Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR) and Monocyte-to-Lymphocyte Ratio (MLR) as Biomarkers in Diagnosis Evaluation of Acute Exacerbation of Chronic Obstructive Pulmonary Disease: a Retrospective, Observational Study. Int J Chron Obstruct Pulmon Dis. 2024;19:933–943. doi:10.2147/copd.S452444
5. Du D, Zhang G, Xu D, et al. Association between systemic inflammatory markers and chronic obstructive pulmonary disease: a population-based study. Heliyon. 2024;10(10):e31524. doi:10.1016/j.heliyon.2024.e31524
6. Gayaf M, Karadeniz G, Güldaval F, Polat G, Türk M. Which one is superior in predicting 30 and 90 days mortality after COPD exacerbation: DECAF, CURB-65, PSI, BAP-65, PLR, NLR. Expert Rev Respir Med. 2021;15(6):845–851. doi:10.1080/17476348.2021.1901584
7. Liao QQ, Mo YJ, Zhu KW, et al. Platelet-to-Lymphocyte Ratio (PLR), Neutrophil-to-Lymphocyte Ratio (NLR), Monocyte-to-Lymphocyte Ratio (MLR), and Eosinophil-to-Lymphocyte Ratio (ELR) as Biomarkers in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD). Int J Chron Obstruct Pulmon Dis. 2024;19:501–518. doi:10.2147/copd.S447519
8. Xu Y, Yan Z, Li K, Liu L. The association between systemic immune-inflammation index and chronic obstructive pulmonary disease in adults aged 40 years and above in the United States: a cross-sectional study based on the NHANES 2013–2020. Front Med Lausanne. 2023;10:1270368. doi:10.3389/fmed.2023.1270368
9. Zinellu A, Zinellu E, Mangoni AA, et al. Clinical significance of the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in acute exacerbations of COPD: present and future. Eur Respir Rev. 2022;31(166):2. doi:10.1183/16000617.0095-2022
10. Hao M, Jiang S, Tang J, et al. Ratio of Red Blood Cell Distribution Width to Albumin Level and Risk of Mortality. JAMA Network Open. 2024;7(5):e2413213. doi:10.1001/jamanetworkopen.2024.13213
11. Li D, Ruan Z, Wu B. Association of Red Blood Cell Distribution Width-Albumin Ratio for Acute Myocardial Infarction Patients with Mortality: a Retrospective Cohort Study. Clin Appl Thromb Hemost. 2022;28:10760296221121286. doi:10.1177/10760296221121286
12. Chen C, Cai J, Song B, et al. Relationship between the Ratio of Red Cell Distribution Width to Albumin and 28-Day Mortality among Chinese Patients over 80 Years with Atrial Fibrillation. Gerontology. 2023;69(12):1471–1481. doi:10.1159/000534259
13. Hong J, Hu X, Liu W, et al. Impact of red cell distribution width and red cell distribution width/albumin ratio on all-cause mortality in patients with type 2 diabetes and foot ulcers: a retrospective cohort study. Cardiovasc Diabetol. 2022;21(1):91. doi:10.1186/s12933-022-01534-4
14. Ni Q, Wang X, Wang J, Chen P. The red blood cell distribution width-albumin ratio: a promising predictor of mortality in heart failure patients - A cohort study. Clin Chim Acta. 2022;527:38–46. doi:10.1016/j.cca.2021.12.027
15. Kimura H, Tanaka K, Saito H, et al. Impact of red blood cell distribution width-albumin ratio on prognosis of patients with CKD. Sci Rep. 2023;13(1):15774. doi:10.1038/s41598-023-42986-2
16. Zhao N, Hu W, Wu Z, et al. The Red Blood Cell Distribution Width-Albumin Ratio: a Promising Predictor of Mortality in Stroke Patients. Int J Gen Med. 2021;14:3737–3747. doi:10.2147/ijgm.S322441
17. Lan CC, Su WL, Yang MC, Chen SY, Wu YK. Predictive role of neutrophil-percentage-to-albumin, neutrophil-to-lymphocyte and eosinophil-to-lymphocyte ratios for mortality in patients with COPD: evidence from NHANES 2011–2018. Respirology. 2023;28(12):1136–1146. doi:10.1111/resp.14589
18. Ran B, Zhang Y, Wu Y, Wen F. Association between depression and COPD: results from the NHANES 2013–2018 and a bidirectional Mendelian randomization analysis. Expert Rev Respir Med. 2023;17(11):1061–1068. doi:10.1080/17476348.2023.2282022
19. Wang X, Wen J, Gu S, Zhang L, Qi X. Frailty in asthma-COPD overlap: a cross-sectional study of association and risk factors in the NHANES database. BMJ Open Respir Res. 2023;10(1):1. doi:10.1136/bmjresp-2023-001713
20. He Y, Liu C, Zeng Z, Ye W, Lin J, Ou Q. Red blood cell distribution width: a potential laboratory parameter for monitoring inflammation in rheumatoid arthritis. Clin Rheumatol. 2018;37(1):161–167. doi:10.1007/s10067-017-3871-7
21. Lan W, Liu E, Sun D, et al. Red cell distribution in critically ill patients with chronic obstructive pulmonary disease. Pulmonology. 2024;30(1):34–42. doi:10.1016/j.pulmoe.2022.04.001
22. Yčas JW, Horrow JC, Horne BD. Persistent increase in red cell size distribution width after acute diseases: a biomarker of hypoxemia? Clin Chim Acta. 2015;448:107–117. doi:10.1016/j.cca.2015.05.021
23. Mattioli AV, Coppi F, Nasi M, Pinti M, Gallina S. Long COVID: a New Challenge for Prevention of Obesity in Women. Am J Lifestyle Med. 2023;17(1):164–168. doi:10.1177/15598276221111054
24. Haenggi E, Kaegi-Braun N, Wunderle C, et al. Red blood cell distribution width (RDW) - A new nutritional biomarker to assess nutritional risk and response to nutritional therapy? Clin Nutr. 2024;43(2):575–585. doi:10.1016/j.clnu.2024.01.001
25. Quintana JM, Esteban C, Unzurrunzaga A, et al. Predictive score for mortality in patients with COPD exacerbations attending hospital emergency departments. BMC Med. 2014;12(1):66. doi:10.1186/1741-7015-12-66
26. Chaudhury A, Miller GD, Eichner D, Higgins JM. Single-cell modeling of routine clinical blood tests reveals transient dynamics of human response to blood loss. Elife. 2019;8:48590. doi:10.7554/eLife.48590
27. Pretorius E, Olumuyiwa-Akeredolu OO, Mbotwe S, Bester J. Erythrocytes and their role as health indicator: using structure in a patient-orientated precision medicine approach. Blood Rev. 2016;30(4):263–274. doi:10.1016/j.blre.2016.01.001
28. Hausman DB, Fischer JG, Johnson MA. Protein, lipid, and hematological biomarkers in centenarians: definitions, interpretation and relationships with health. Maturitas. 2012;71(3):205–212. doi:10.1016/j.maturitas.2011.12.002
29. Eckart A, Struja T, Kutz A, et al. Relationship of Nutritional Status, Inflammation, and Serum Albumin Levels During Acute Illness: a Prospective Study. Am J Med. 2020;133(6):713–722.e7. doi:10.1016/j.amjmed.2019.10.031
30. Sheinenzon A, Shehadeh M, Michelis R, Shaoul E, Ronen O. Serum albumin levels and inflammation. Int J Biol Macromol. 2021;184:857–862. doi:10.1016/j.ijbiomac.2021.06.140
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Prognostic Performance of Lung Diffusing Capacity in Preserved Ratio Impaired Spirometry: An Observational Cohort Study
Ogata H, Sha K, Kotetsu Y, Enokizu-Ogawa A, Katahira K, Ishimatsu A, Taguchi K, Moriwaki A, Yoshida M
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2791-2799
Published Date: 28 October 2022
Association Between Blood Urea Nitrogen to Serum Albumin Ratio and Mortality in Critically Ill Patients With Chronic Obstructive Pulmonary Disease: A Retrospective Study
Li J, Peng J, Cheng C, Zhang J, Li L
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:349-360
Published Date: 17 February 2025
Association Between Lactate-to-Albumin Ratio and 28-Day All-Cause Mortality in Critical Care Patients with COPD: Can Both Arterial and Peripheral Venous Lactate Serve as Predictors?
Zhao K, Zhou L, Ni Y, Tao J, Yu Z, Li X, Wang L
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1419-1434
Published Date: 11 May 2025