")
Back to Journals » Psychology Research and Behavior Management » Volume 16
The Psychological Network of Loneliness Symptoms Among Chinese Residents During the COVID-19 Outbreak
Authors Zhong BL , Yuan MD, Li F, Sun P
Received 6 June 2023
Accepted for publication 23 August 2023
Published 8 September 2023 Volume 2023:16 Pages 3767—3776
DOI https://doi.org/10.2147/PRBM.S424565
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Bao-Liang Zhong,1,2 Meng-Di Yuan,2 Fang Li,3 Peng Sun3
1Department of Psychiatry, Wuhan Mental Health Center, Wuhan, Hubei Province, People’s Republic of China; 2Research Center for Psychological and Health Sciences, China University of Geosciences (Wuhan), Wuhan, Hubei Province, People’s Republic of China; 3Department of Psychiatry, Huangpu District Mental Health Center, Shanghai, People’s Republic of China
Correspondence: Peng Sun, Department of Psychiatry, Huangpu District Mental Health Center, Shanghai, People’s Republic of China, Email [email protected]
Purpose: Social distancing measures implemented during the COVID-19 pandemic have contributed to increased levels of loneliness, but the specific interactions between loneliness symptoms in the context of the pandemic remain unknown. This study characterized the psychological network of loneliness symptoms in residents during the initial wave of COVID-19 outbreak in China.
Patients and Methods: The study recruited 8472 Chinese residents (61.5% women, aged 33.0± 10.6 years) through online snowball sampling. The Six-item De Jong Gierveld Loneliness Scale (DJGLS) was used to measure loneliness symptoms. Central symptoms of and bridge symptoms between emotional and social loneliness subscales were identified based on centrality and bridge centrality indices, respectively. Network stability was examined using the case-dropping procedures.
Results: The nodes in the loneliness network were separated into two groups, corresponding to the social and emotional loneliness domains of the DJGLS. The strongest direction association was between “no reliable people” and “no trustworthy people” (edge weight=0.546). “No trustworthy people” has the highest node strength (1.047) in the loneliness network, followed by “emptiness sense” (0.767) and “no reliable people” (0.749). “Feeling of rejection” (1.672) and “no close people” (0.403) showed the first and second highest bridge strengths, respectively. Both the stability and accuracy tests supported robustness of the whole network.
Conclusion: Interventions targeting central symptoms “no trustworthy people” and “emptiness sense” and central bridge symptom “feeling of rejection” may be effective for alleviating the overall level of loneliness in pandemic-affected Chinese residents.
Keywords: loneliness symptoms, psychological network, residents, COVID-19, China
Introduction
During the COVID-19 pandemic over the last three years, various public health measures have been implemented to control the spread of SARS-CoV-2, particularly during the initial outbreak phase with the enforcement of strict restriction measures.1–6 While these measures are necessary, they have also inevitably increased the risk of loneliness among people globally.4,7–13 The implementation of social distancing, quarantine, lockdown, and the closure of community gathering places, such as restaurants, theaters, and religious centers, has disrupted daily routines and limited opportunities for social interaction among individuals.14–16 As a result, people may experience elevated levels of social isolation and feelings of loneliness.
Loneliness is a subjective feeling of distress that results from a lack of meaningful social connections, including both a smaller number of relationships than an individual desires and a lack of the desired intimacy in those relationships.17,18 Accordingly, social and emotional loneliness has been distinguished as two basic components of loneliness.19 Loneliness is typically measured by conceptualizing an unobserved latent variable, which is then reflected by several related symptoms, such as feeling left out, disconnected from a group, or isolated from others.20,21 However, empirical data continue to present unstable findings regarding whether commonly used loneliness scales, such as the University of California Los Angeles Loneliness Scale and the De Jong Gierveld Loneliness Scale (DJGLS), exhibit a unidimensional or multidimensional structure, as well as sets of items belonging to the same domain.22 As a result, the traditional latent variable theory is limited to account for the variations in the observed symptoms of loneliness.
The psychological network model provides an alternative to the latent variable model by conceptualizing a mental health problem as a complex system of interacting symptoms.23 Accurately describing and visualizing these interactions is crucial for understanding the potential psychopathological mechanisms and developing effective, targeted intervention strategies.24 In network analysis terminology, each symptom represents a node, and the association between two nodes is an edge.25 Calculating centrality and bridge centrality indices through this symptom-oriented approach may aid in identifying target symptoms for preventing mental health problems and reducing the risk of comorbidities between them.26,27 As far as we know, there have not been any studies exploring the network structure of loneliness scales in the literature.
Loneliness can be caused by various factors, including social isolation, a lack of social support, changes in life circumstances, and mental health problems.21,28–30 The COVID-19 pandemic significantly exacerbated loneliness due to unprecedented restrictions on in-person social interactions. Examining the psychological network in times of COVID-19 is crucial and has public health implications, given the high prevalence of loneliness. Therefore, the goal of this study was to employ network analysis to investigate the psychological network of loneliness symptoms assessed by the Six-item DJGLS in Chinese residents during the COVID-19 outbreak.
Considering the distinct yet interrelated relationships between social and emotional loneliness, we hypothesized that the loneliness symptoms could be categorized into two groups, aligning with the theoretical construct of social and emotional loneliness. According to the theoretical framework of loneliness, various negative feelings converge to form the experience of loneliness. Core symptoms encompass self-alienation such as emptiness, absence of intimacy, lack of closeness to others, social and emotional isolation, rejection by close individuals, self-imposed social detachment, and emotional turmoil.31 In our examination of the Six-item DJGLS, we hypothesized that two symptoms, namely no trustworthy people and emptiness, would hold the most influential roles within the network of loneliness symptoms. This is because the perception of lacking trustworthy individuals in one’s social circle is likely connected to various symptoms, such as absence of intimacy, social isolation, and feelings of rejection. Emptiness is often intertwined with the absence of intimacy, lack of closeness to others, social and emotional isolation, and self-alienation.32–35 As our study is primarily exploratory, we did not establish specific hypotheses regarding the bridge symptoms that link social and emotional loneliness.
Materials and Methods
Study Participants and Sampling
This study was a nationwide online survey among Chinese residents, which was conducted between January 27 and March 13, 2020, a period coincided with the first wave of COVID-19 outbreak in China. To minimize the risk of COVID-19 transmission, the survey was conducted online, and participants were recruited through snowball sampling. In brief, we utilized social media platforms such as Weibo and Wechat, as well as popular media outlet websites in Hubei province, to recruit potential participants by sharing a concise one-page electronic invitation poster. This poster contained essential survey information, emphasized the voluntary nature of participation, assured anonymity and confidentiality, and included a QR code for accessing the survey questionnaire. Furthermore, participants were encouraged to share and repost the invitation poster on their own social media platforms. Further information on the sampling and survey procedures can be found elsewhere.2,7,36 For participation in this study, individuals must have Chinese nationality, be at least 16 years old, have no known or suspected SARS-CoV-2 infection, comprehend the recruitment poster, and be willing to take part.
The Ethics Committee of Wuhan Mental Health Center approved the survey protocol and all participants provided electronic written informed consent before the questionnaire administration commenced. The study protocol, along with the employed methods, followed the principles outlined in the Declaration of Helsinki and complied with the ethical guidelines and regulations applicable in China.
Measures
The validated Chinese Six-item DJGLS was used to assess loneliness symptoms.37–39 The Chinese DJGLS employs a five-point Likert scale for rating all its items, with one indicating “strongly disagree”, two indicating “disagree”, three indicating “neither agree nor disagree”, four indicating “agree”, and five indicating “strongly agree”. The total score is calculated by adding up six items, three of which are positively worded and reversed before scoring. A higher score indicates more loneliness. The Six-item DJGLS can be used either as a single-dimensional scale to assess overall loneliness or as two subscales consisting of three items each, which can investigate social loneliness and emotional loneliness separately.40
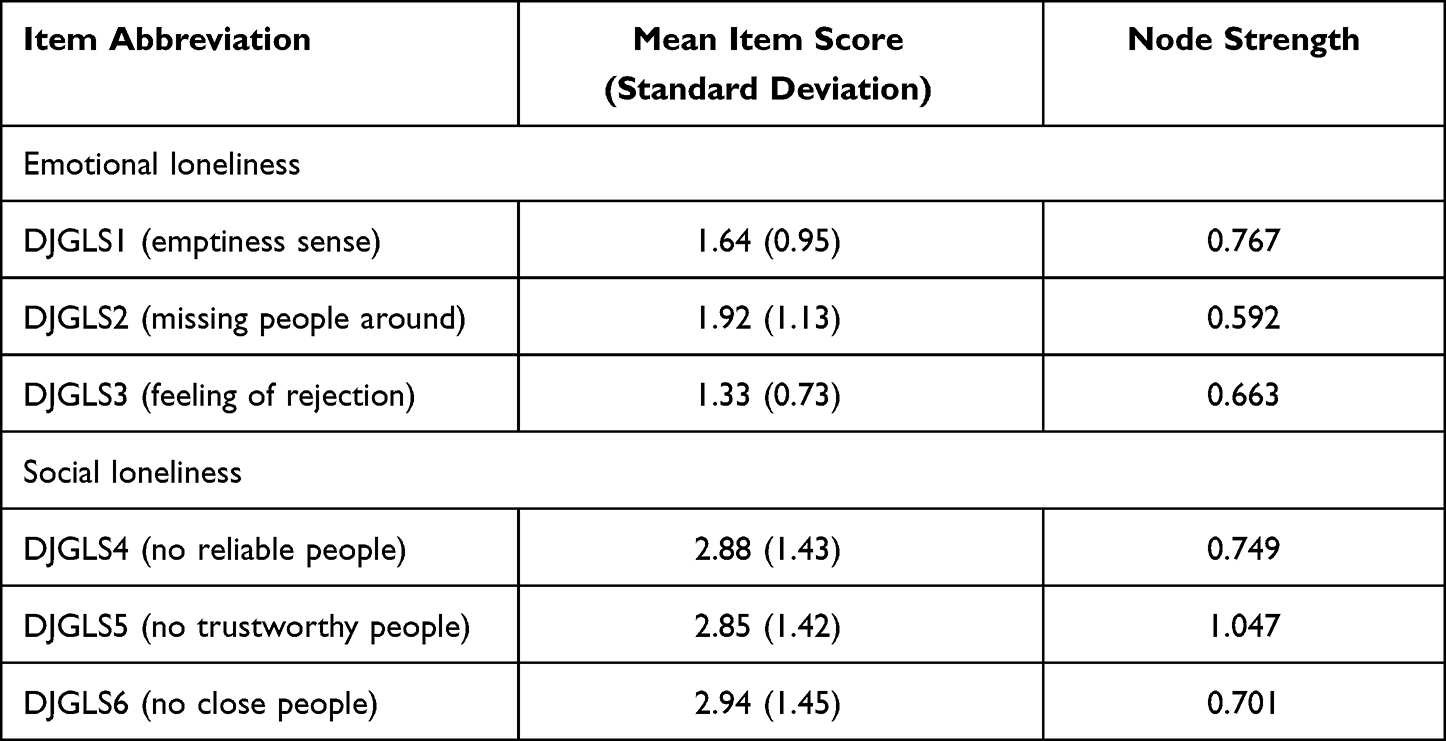 |
Table 1 Descriptive Statistics of the Six-Item De Jong Gierveld Loneliness Scale (n=8472) |
Demographic information, such as sex, age, and current place of residence (Hubei versus other provinces in China), was also collected.
Data Analysis
The R program version 4.2.3 was utilized to perform network analysis, which included procedures for network estimation, network stability, and network comparisons.27,41
Network estimation. The psychological network comprises of nodes (symptoms) and edges (connections) representing the associations between them. Edge thickness indicates the strength of the association, while green and red edges represent positive and negative associations. Nonparanormal transformation was applied to calculate nonparametric correlations since item scores were non-normally distributed. Partial correlation analysis adjusted for potential confounding effects of other nodes. The EBICglasso (Extended Bayesian Information Criterion Graphical Least Absolute Shrinkage and Selection Operator) algorithm was utilized to select the optimal regularization parameter. Loneliness network was estimated and visualized using R packages bootnet version 1.5 and qgraph version 1.6.9, respectively.
To quantify the importance of nodes in the network, we used the centrality plot function of R package qgraph version 1.6.9 to compute centrality indices. While centrality indices such as strength, betweenness, and closeness are often used, we only considered strength as the other indices are not reliable in network analysis of psychopathology.42 To evaluate the importance of a node connecting emotional and social loneliness, we used the bridge function of R package networktools version 1.2.3 to calculate the bridge centrality index of bridge strength.
Network stability. We used the case-dropping bootstrap procedure to analyze the stability of node and bridge strengths. The degree of stability was determined using the correlation stability coefficient (CSC), which indicates the maximum portion of cases that can be removed from the initial sample while maintaining 70% of the centrality indices obtained from the subsamples relative to those from the original sample. Typically, the CSC should have a minimum value of 0.25 but ideally, it should be above 0.50. We assessed the stability of edge weights using a nonparametric bootstrap method to generate their 95% confidence intervals (95% CIs). The accuracy of edges was evaluated by examining the 95% CIs, with narrower CIs indicated more reliable networks. Differences between two edges or node strengths were determined based on bootstrapped tests that generated 95% CIs. Statistical significance was considered present if the 95% CIs did not encompass zero. These stability tests were conducted using R package bootnet version 1.5.
Network comparison. We used the R package NetworkComparisonTest version 2.2.1 to investigate the invariance in structure, edge, and global strength between two networks. Considering the sex-, age-, and epicenter/non-epicenter-residence- differences in the prevalence rates of loneliness,7,21,29,43–45 a permutation test (n=1000) was performed to test the network invariance between subgroups based on the three factors. Statistical significance was set at a two-sided P-value of less than 0.05.
Results
Sample Characteristics
A total of 8472 participants completed the online questionnaire, with a mean age of 33.0 years (standard deviation [SD]: 10.6, range: 16–90). Of these, 5208 (61.5%) were women and 3612 (42.6%) were residents of Hubei province, the epicenter of the COVID-19 outbreak in China. The mean scores (SDs) of the overall, emotional, and social loneliness were 13.6 (4.7), 4.9 (2.3), and 8.7 (3.8), respectively. The correlation coefficient between emotional and social loneliness scores was 0.135 (P<0.001). The mean item scores of the Six-item DJGLS ranged from 1.33 to 2.94 (Table 1).
Network Structure
The network of loneliness symptoms is shown in Figure 1. The nodes are organized into two communities based on social and emotional loneliness. Nodes within the same community exhibit strong connections, whereas connections between nodes in the two communities are weak. The edge “no reliable people” and “no trustworthy people” (0.546) shows the strongest association, followed by edges “no trustworthy people” and “no close people” (0.452) and “missing people around” and “emptiness sense” (0.382). In Table 1 and Figure 1, “no trustworthy people” has the highest node strength (1.047) in the loneliness network, followed by “emptiness sense” (0.767) and “no reliable people” (0.749). In terms of bridge symptoms, “feeling of rejection” (1.672) and “no close people” (0.403) showed the first and second highest bridge strengths, respectively (Figure 2).
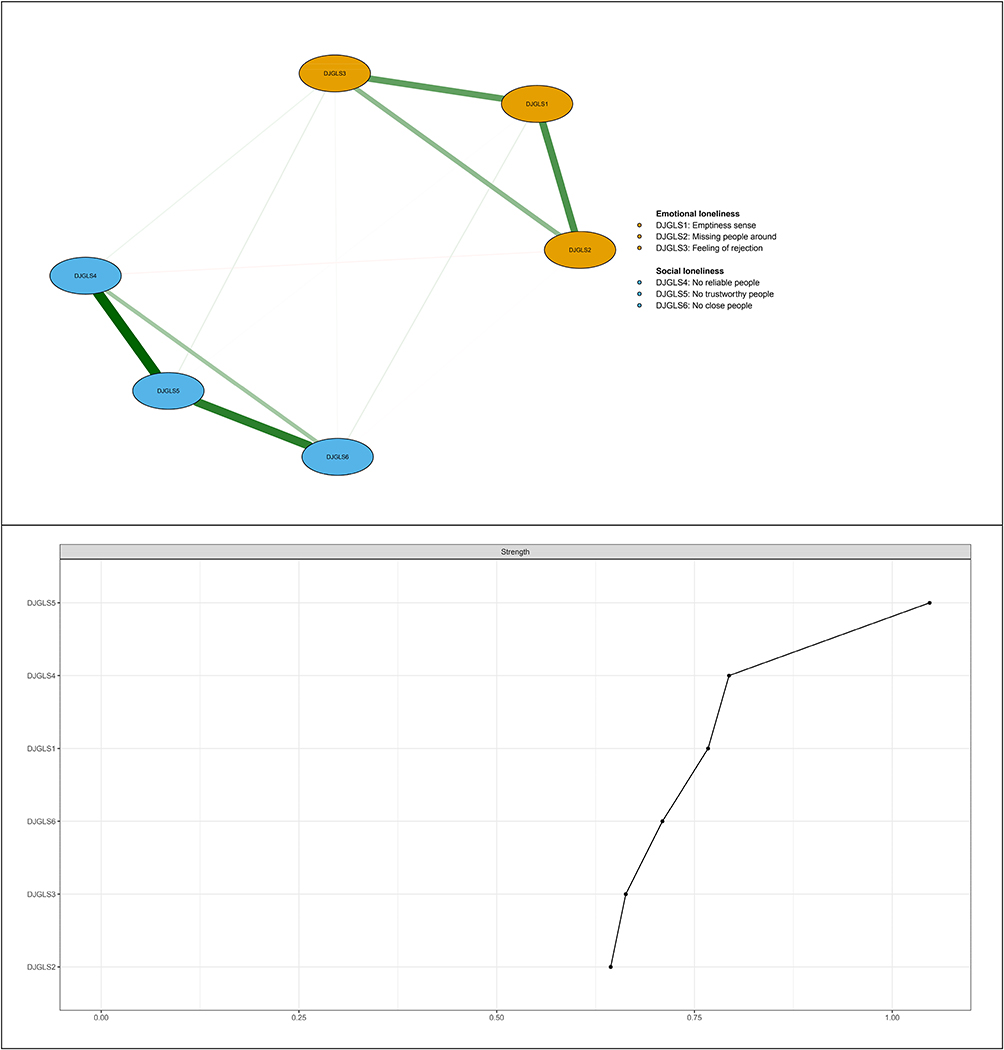 |
Figure 1 Network structure of loneliness symptoms in Chinese residents. The upper panel provides a visualization of the network structure, while the lower panel displays the values of strength in order. In the upper panel, edge thickness indicates the strength of the association, while green and red edges represent positive and negative associations. Light blue nodes and golden yellow nodes represent social and emotional loneliness communities, respectively. |
 |
Figure 2 Network structure of social and emotional loneliness symptoms showing bridge symptoms in Chinese residents. The upper panel presents a visualization of the network structure depicting the bridging symptoms, while the lower panel displays the corresponding bridge strength values in order. In the upper panel, edge thickness indicates the strength of the association, while green and red edges represent positive and negative associations. Light blue nodes and red nodes represent social and emotional loneliness communities, respectively. |
Network Stability
In Figure S1, the CSCs of node strength and bridge node strength in the case-dropping procedure were 0.75 and 0.517, respectively. Most comparisons among edge weights and node strengths were statistically significant in the nonparametric bootstrap procedure (Figures S2 and S3). In addition, bootstrapped 95% CIs were narrow (Figure S4).
Network Comparisons
As shown in Figure S5, there were significant differences in network global strengths between men and women (P=0.007) and in network structure between epicenter and non-epicenter residents (P=0.042). There were no significant differences between two networks in terms of other invariance measures in the three subgroup comparisons (P=0.088–1.00).
Discussion
To the best of our knowledge, this study represents the first investigation of the psychological network of loneliness symptoms in the general population during the initial COVID-19 outbreak in 2020 in China, as well as the first in the world to examine this network. It provides empirical data on the network of loneliness symptoms under the unique context of strict outbreak containment measures, including the unprecedented lockdown of Hubei province, stay-at-home orders, social distancing measures, and public mask mandates.2 The strengths of this study include the very large sample size and the application of psychological network analysis to visualize patterns of loneliness symptoms among Chinese residents impacted by the outbreak, yielding consistently stable results.
Main Findings
The main findings of this study were: first, the nodes in the loneliness network were separated into two groups, corresponding to the social and emotional loneliness domains of the Six-item DJGLS; second, “no trustworthy people”, “emptiness sense”, and “no reliable people” were identified as the central symptoms in the social and emotional loneliness communities; third, “feeling of rejection” and “no close people” were the two most influential bridge symptoms that linked the social and emotional loneliness communities, respectively; fourth, significant differences were observed between men and women in network global strengths and between epicenter and non-epicenter residents in network structure.
Network Structure
Social loneliness refers to the feeling of not having enough social connections, whereas emotional loneliness refers to the absence of close, meaningful, and intimate relationships.19 Persons may experience emotional loneliness even if they are socially connected, whereas someone may feel socially lonely despite having close emotional relationships. Although social and emotional loneliness are correlated, they are distinct domains. Previous studies have reported a moderate correlation between social and emotional loneliness, as measured by the DJGLS.19,39,40 However, in the current network analysis, the two communities of loneliness symptoms appear to be less closely related, with a much lower correlation coefficient (r=0.135). This may be due to the pandemic and its containment measures, which have substantially interrupted social connections between people but has had limited impact on intimate relationships.
During the COVID-19 outbreak, fear of infection and uncertainty about the future may have caused people to become less willing to invest in building social relationships.46 Social distancing measures have limited face-to-face interactions and restricted normal social connectedness, potentially decreasing the chances of building and maintaining strong social connections. Moreover, some people who traveled from Hubei province to other provinces of China during the outbreak period were required to undergo compulsory medical observation and quarantine, causing them to be isolated from their friends and families.36 Additionally, they may be stigmatized and discriminated due to being labeled as “potential carriers of SARS-CoV-2” in their destination sites.36 These factors likely contributed to the feeling among Chinese residents that there are no people they can rely on or trust completely. The disruption of normal routines and decreased opportunities to engage in meaningful activities outside the home may cause many people to experience boredom and a sense of emptiness.47,48 Therefore, “no trustworthy people”, “emptiness sense”, and “no reliable people” were central symptoms in the loneliness network. The strong association between “no reliable people” and “no trustworthy people” is likely due to their shared outbreak-related causes.
“Feeling of rejection” is a key component of the emotional experience of loneliness, which is the subjective perception of being excluded, unwanted, or unwelcome by others.21 Given the widespread use of social distancing measures and the fear of contracting the elusive SARS-CoV-2 from both acquaintances and strangers, socially lonely individuals may be more likely to feel rejected by others. This may explain why the “feeling of rejection” plays a bridging role in linking social loneliness. The bridging role of “having no close people” in linking emotional loneliness is expected, which may be attributed to the fact that individuals without close friends or companions are more likely to experience emotional loneliness.49
Network Comparisons
This study found that men had a significantly higher global strength than women in the network comparison, suggesting strong interconnections among individual symptoms in the male model. Additionally, the network structure differed significantly between residents living in the epicenter versus those living outside of it, indicating differences in the strength and presence of connections between nodes in the two networks. These two findings have not been previously reported in relevant studies using network analysis. We hypothesize that the former finding may be related to the higher risk of loneliness among men compared to women during the pandemic,7 while the latter may be due to more stringent COVID-19 control measures, such as the lockdown of Hubei province, which were strictly implemented in the epicenter region.
Limitations
When interpreting the findings, it is important to consider several limitations. Firstly, the network of loneliness symptoms was constructed from cross-sectional data obtained from a convenience sample of Chinese residents. Therefore, causality between individual symptoms cannot be inferred. Additionally, it is necessary to use representative samples to further validate the accuracy of the current findings. Secondly, due to logistical reasons, loneliness data was not collected before the outbreak. Therefore, it is impossible to evaluate the impact of the outbreak on loneliness. Thirdly, since we did not use the original 11-item version of the DJGLS, it is unknown how unmeasured loneliness symptoms correlate with each other, and further examination of this matter is necessary.
Conclusion
Although the COVID-19 pandemic is no longer a Public Health Emergency of International Concern and seems to be approaching its end, the potential for a resurgence remains. It’s crucial to acknowledge that infectious diseases will always be present in human history, and pandemics are likely to reoccur. Thus, the findings and lessons from this study hold ongoing public health implications for people in future medical pandemics. These insights can aid in better preparation and response strategies for upcoming pandemics.
In conclusion, central symptoms (“no trustworthy people”, “emptiness sense”, and “no reliable people”) and bridge symptoms (“feeling of rejection” and “no close people”) were identified in the psychological network of loneliness symptoms in Chinese residents during the COVID-19 outbreak. Systematic reviews have shown that interventions like mindfulness, social cognitive training, animal therapy, and social support can prevent or reduce loneliness.50–54 During the pandemic, some studies have yielded preliminary evidence supporting the effectiveness of remote interventions, video calls, and assistive technology in reducing social isolation and loneliness.55–58 Based on the results of this network analysis, the development of psychosocial interventions to alleviate loneliness must take into account the central and bridge symptoms identified. Public health and social work service guidelines should include measures that assist individuals in staying connected with their loved ones through various communication means such as phone calls, video chats, social media, or online forums. Additionally, timely access to online professional help from psychotherapists or psychological counselors should be provided to those experiencing severe feelings of loneliness.
Acknowledgments
The authors thank all the participants involved in this study for their cooperation and support.
Funding
This work was supported by National Natural Science Foundation of China (grant number: 71774060), 2015 Irma and Paul Milstein Program for Senior Health Awards from the Milstein Medical Asian American Partnership Foundation, the Young Top Talent Programme in Public Health from Health Commission of Hubei Province (PI: Zhong BL), and Wuhan Health and Family Planning Commission (grant number: WX18C12; WX17Q30; WG16A02; WG14C24). The funding source listed had no role in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cenat JM, Farahi S, Dalexis RD, et al. The global evolution of mental health problems during the COVID-19 pandemic: a systematic review and meta-analysis of longitudinal studies. J Affect Disord. 2022;315:70–95. doi:10.1016/j.jad.2022.07.011
2. Zhong BL, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
3. Lazaroiu G, Adams C. Viral panic and contagious fear in scary times: the proliferation of COVID-19 misinformation and fake news. Anal Metaphys. 2020;19:80–86. doi:10.22381/AM1920209
4. Su Y, Rao W, Li M, Caron G, D’Arcy C, Meng X. Prevalence of loneliness and social isolation among older adults during the COVID-19 pandemic: a systematic review and meta-analysis. Int Psychogeriatr. 2023;35(5):229–241. doi:10.1017/S1041610222000199
5. Hughes TF, Ran X, Fang F, et al. Psychosocial implications of early COVID-19 restrictions on older adults in a small-town region in Southwestern, Pennsylvania (USA). Int Psychogeriatr. 2022:1–10. doi:10.1017/S1041610222000977
6. Ahmed F, Sifat RI. The impact of the COVID-19 pandemic on the mental health of the rickshaw-puller in Bangladesh. J Loss Trauma. 2021;26(8):782–789. doi:10.1080/15325024.2020.1852823
7. Bao L, Li WT, Zhong BL. Feelings of loneliness and mental health needs and services utilization among Chinese residents during the COVID-19 epidemic. Global Health. 2021;17(1):51. doi:10.1186/s12992-021-00704-5
8. Farrell AH, Vitoroulis I, Eriksson M, Vaillancourt T. Loneliness and well-being in children and adolescents during the COVID-19 pandemic: a systematic review. Children. 2023;10(2):279. doi:10.3390/children10020279
9. Ernst M, Niederer D, Werner AM, et al. Loneliness before and during the COVID-19 pandemic: a systematic review with meta-analysis. Am Psychol. 2022;77(5):660–677. doi:10.1037/amp0001005
10. Lăzăroiu G, Horak J, Valaskova K. Scaring ourselves to death in the time of COVID-19: pandemic awareness, virus anxiety, and contagious fear. Linguist Philos Investig. 2020;19:114–120. doi:10.22381/LPI1920208
11. Bratu S. The fake news sociology of COVID-19 pandemic fear: dangerously inaccurate beliefs, emotional contagion, and conspiracy ideation. Linguist Philos Investig. 2020;19:128–134. doi:10.22381/LPI19202010
12. Ruan J, Xu YM, Zhong BL. Loneliness in older Chinese adults amid the COVID-19 pandemic: prevalence and associated factors. Asia Pac Psychiatry. 2023;e12543. doi:10.1111/appy.12543
13. Sifat RI, Ahmed F, Miah MRA, Khisa M. Effects of COVID-19 on livelihood, health, and psychology of hijra population: insights from Dhaka, Bangladesh. J Homosex. 2023;70(10):2096–2112. doi:10.1080/00918369.2022.2048162
14. Chen WC, Chen SJ, Zhong BL. Sense of alienation and its associations with depressive symptoms and poor sleep quality in older adults who experienced the lockdown in Wuhan, China, during the COVID-19 pandemic. J Geriatr Psychiatry Neurol. 2022;35(2):215–222. doi:10.1177/08919887221078564
15. Zhong BL, Xiang YT. Challenges to and recent research on the mental health of older adults in china during the COVID-19 pandemic. J Geriatr Psychiatry Neurol. 2022;35(2):179–181. doi:10.1177/08919887221078558
16. Ahmed F, Sifat RI. Strategic assessment of mental health and suicide amid COVID-19 pandemic in Bangladesh. Int J Health Plann Manage. 2021;36(3):980–985. doi:10.1002/hpm.3121
17. van Tilburg TG, Meeks S. Social, emotional, and existential loneliness: a test of the multidimensional concept. Gerontologist. 2021;61(7):e335–e344. doi:10.1093/geront/gnaa082
18. Zhong BL, Chen SL, Tu X, Conwell Y. Loneliness and cognitive function in older adults: findings from the Chinese Longitudinal Healthy Longevity Survey. J Gerontol B Psychol Sci Soc Sci. 2017;72(1):120–128. doi:10.1093/geronb/gbw037
19. De Jong Gierveld J, Van Tilburg T. The De Jong Gierveld short scales for emotional and social loneliness: tested on data from 7 countries in the UN generations and gender surveys. Eur J Ageing. 2010;7(2):121–130. doi:10.1007/s10433-010-0144-6
20. Cheung SL, Hobbelen H, van der Schans CP, Krijnen WP, Meeks S. Cross-cultural equivalence of De Jong Gierveld Loneliness Scale among Older Native and Diasporic Chinese Adults. Gerontologist. 2022;62(2):e62–e72. doi:10.1093/geront/gnaa151
21. De Jong Gierveld J. A review of loneliness: concept and definitions, determinants and consequences. Rev Clin Gerontol. 1998;8(1):73–80. doi:10.1017/S0959259898008090
22. Maes M, Qualter P, Lodder GMA, Mund M. How (Not) to measure loneliness: a review of the eight most commonly used scales. Int J Environ Res Public Health. 2022;19(17):10816. doi:10.3390/ijerph191710816
23. Zhao YJ, Bai W, Cai H, et al. The backbone symptoms of depression: a network analysis after the initial wave of the COVID-19 pandemic in Macao. PeerJ. 2022;10:e13840. doi:10.7717/peerj.13840
24. Wang Y, Hu Z, Feng Y, Wilson A, Chen R. Changes in network centrality of psychopathology symptoms between the COVID-19 outbreak and after peak. Mol Psychiatry. 2020;25(12):3140–3149. doi:10.1038/s41380-020-00881-6
25. Hevey D. Network analysis: a brief overview and tutorial. Health Psychol Behav Med. 2018;6(1):301–328. doi:10.1080/21642850.2018.1521283
26. Broda MD, Granger K, Chow J, Ross E. Using social network analysis in applied psychological research: a tutorial. Psychol Methods. 2021;28(4):791–805. doi:10.1037/met0000451
27. Bai W, Cai H, Liu S, et al. Anxiety and depressive symptoms in college students during the late stage of the COVID-19 outbreak: a network approach. Transl Psychiatry. 2021;11(1):638. doi:10.1038/s41398-021-01738-4
28. Pinquart M, Sorensen S. Influences on loneliness in older adults: a meta-analysis. Basic Appl Soc Psych. 2001;23(4):245–266. doi:10.1207/S15324834BASP2304_2
29. Zhong BL, Chen SL, Conwell Y. Effects of transient versus chronic loneliness on cognitive function in older adults: findings from the Chinese Longitudinal Healthy Longevity Survey. Am J Geriatr Psychiatry. 2016;24(5):389–398. doi:10.1016/j.jagp.2015.12.009
30. Zhang HG, Fan F, Zhong BL, Chiu HF. Relationship between left-behind status and cognitive function in older Chinese adults: a prospective 3-year cohort study. Gen Psychiatr. 2023;36(3):e101054. doi:10.1136/gpsych-2023-101054
31. Bekhet AK, Zauszniewski JA, Nakhla WE. Loneliness: a concept analysis. Nurs Forum. 2008;43(4):207–213. doi:10.1111/j.1744-6198.2008.00114.x
32. Lieberz J, Shamay-Tsoory SG, Saporta N, et al. Loneliness and the social brain: how perceived social isolation impairs human interactions. Adv Sci. 2021;8(21):e2102076. doi:10.1002/advs.202102076
33. Miller CE, Townsend ML, Day NJS, Grenyer BFS, Doering S. Measuring the shadows: a systematic review of chronic emptiness in borderline personality disorder. PLoS One. 2020;15(7):e0233970. doi:10.1371/journal.pone.0233970
34. D’Agostino A, Pepi R, Monti MR, Starcevic V. The feeling of emptiness: a review of a complex subjective experience. Harv Rev Psychiatry. 2020;28(5):287–295. doi:10.1097/HRP.0000000000000269
35. Rapolienė G, Aartsen M. Lonely societies: low trust societies? Further explanations for national variations in loneliness among older Europeans. Eur J Ageing. 2021;19(3):485–494. doi:10.1007/s10433-021-00649-z
36. Zhong BL, Zhou DY, He MF, et al. Mental health problems, needs, and service use among people living within and outside Wuhan during the COVID-19 epidemic in China. Ann Transl Med. 2020;8(21):1392. doi:10.21037/atm-20-4145
37. Wang, XD, Wang, XL, Ma, H. Handbook of Mental Health Rating Scales
38. Yang B, Guo L. Reliability and validity of the Chinese Version of the De Jong Gierveld Loneliness Scale. Chin Gen Prac. 2019;22(33):4110–4115.
39. Leung GT, de Jong Gierveld J, Lam LC. Validation of the Chinese translation of the 6-item De Jong Gierveld Loneliness Scale in elderly Chinese. Int Psychogeriatr. 2008;20(6):1262–1272. doi:10.1017/S1041610208007552
40. Gierveld JDJ, Tilburg TV. A 6-item scale for overall, emotional, and social loneliness: confirmatory tests on survey data. Res Aging. 2006;28(5):582–598. doi:10.1177/0164027506289723
41. Epskamp S, Maris G, Waldorp L, Borsboom D. Network Psychometrics. Universiteit van Amsterdam; 2016.
42. Bringmann LF, Elmer T, Epskamp S, et al. What do centrality measures measure in psychological networks? J Abnorm Psychol. 2019;128(8):892–903. doi:10.1037/abn0000446
43. Victor CR, Scambler SJ, Marston L, Bond J, Bowling A. Older people’s experiences of loneliness in the UK: does gender matter? Soc Policy Soc. 2006;5(1):27–38. doi:10.1017/S1474746405002733
44. de Jong Gierveld J, Keating N, Fast JE. Determinants of loneliness among Older Adults in Canada. Can J Aging. 2015;34(2):125–136. doi:10.1017/S0714980815000070
45. Zhong BL, Liu XJ, Chen WC, Chiu HF, Conwell Y. Loneliness in Chinese older adults in primary care: prevalence and correlates. Psychogeriatrics. 2018;18(5):334–342. doi:10.1111/psyg.12325
46. Xu YM, Li C, Zhu R, Zhong BL. Prevalence and correlates of insomnia symptoms in older Chinese adults during the COVID-19 outbreak: a classification tree analysis. J Geriatr Psychiatry Neurol. 2022;35(2):223–228. doi:10.1177/08919887221078561
47. Boylan J, Seli P, Scholer AA, Danckert J. Boredom in the COVID-19 pandemic: trait boredom proneness, the desire to act, and rule-breaking. Pers Individ Dif. 2021;171:110387. doi:10.1016/j.paid.2020.110387
48. Hughes E. Meaninglessness and monotony in pandemic boredom. Phenomenol Cogn Sci. 2023;1–15. doi:10.1007/s11097-023-09888-0
49. Perlman D, Peplau L. Toward a social psychology of loneliness. In: Gilmour R, Duck S, editors. Personal Relationships in Disorder. Vol. 3. Academic Press; 1981.
50. Grillich L, Titscher V, Klingenstein P, et al. The effectiveness of interventions to prevent loneliness and social isolation in the community-dwelling and old population: an overview of systematic reviews and meta-analysis. Eur J Public Health. 2023;33(2):235–241. doi:10.1093/eurpub/ckad006
51. Fischer R, Hartle L. Effective interventions to reduce loneliness in big cities. Curr Opin Psychiatry. 2023;36(3):206–212. doi:10.1097/YCO.0000000000000844
52. Hoang P, King JA, Moore S, et al. Interventions associated with reduced loneliness and social isolation in older adults: a systematic review and meta-analysis. JAMA Netw Open. 2022;5(10):e2236676. doi:10.1001/jamanetworkopen.2022.36676
53. Cacioppo S, Grippo AJ, London S, Goossens L, Cacioppo JT. Loneliness: clinical import and interventions. Perspect Psychol Sci. 2015;10(2):238–249. doi:10.1177/1745691615570616
54. Veronese N, Galvano D, D’Antiga F, et al. Interventions for reducing loneliness: an umbrella review of intervention studies. Health Soc Care Community. 2021;29(5):e89–e96. doi:10.1111/hsc.13248
55. Noone C, McSharry J, Smalle M, et al. Video calls for reducing social isolation and loneliness in older people: a rapid review. Cochrane Database Syst Rev. 2020;5(5):CD013632. doi:10.1002/14651858.CD013632
56. Jutai JW, Tuazon JR. The role of assistive technology in addressing social isolation, loneliness and health inequities among older adults during the COVID-19 pandemic. Disabil Rehabil Assist Technol. 2022;17(3):248–259. doi:10.1080/17483107.2021.2021305
57. Williams CYK, Townson AT, Kapur M, et al. Interventions to reduce social isolation and loneliness during COVID-19 physical distancing measures: a rapid systematic review. PLoS One. 2021;16(2):e0247139. doi:10.1371/journal.pone.0247139
58. Fu Z, Yan M, Meng C. The effectiveness of remote delivered intervention for loneliness reduction in older adults: a systematic review and meta-analysis. Front Psychol. 2022;13:935544. doi:10.3389/fpsyg.2022.935544
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.