")
Back to Journals » Psychology Research and Behavior Management » Volume 15
The Psychological Impact of COVID-19 on Residents of Saudi Arabia
Authors Rafique N , Al Tufaif F, Alhammali W, Alalwan R, Aljaroudi A, AlFaraj F, Latif R , Ibrahim Al-Asoom L , Alsunni AA , Al Ghamdi KS , Salem AM , Yar T
Received 3 February 2022
Accepted for publication 29 April 2022
Published 13 May 2022 Volume 2022:15 Pages 1221—1234
DOI https://doi.org/10.2147/PRBM.S360772
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Nazish Rafique,1 Fatimah Al Tufaif,2 Wala Alhammali,2 Reem Alalwan,2 Alzahraa Aljaroudi,2 Fatimah AlFaraj,2 Rabia Latif,1 Lubna Ibrahim Al-Asoom,1 Ahmed A Alsunni,1 Kholoud S Al Ghamdi,1 Ayad M Salem,1 Talay Yar1
1Department of Physiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Nazish Rafique, Department of Physiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia, Tel +966 5035042329, Fax +966 38578048, Email [email protected]
Purpose: This study aimed to determine the stress levels and identify various factors responsible for causing high-stress scores during the COVID-19 pandemic in the Saudi population.
Patients and Methods: This cross-sectional study was conducted at Imam Abdulrahman Bin Faisal University, Dammam, from June 2020 until December 2020 on 4052 respondents from the Eastern province of Saudi Arabia. An online survey was used to collect information about various stress factors. The psychological impact of COVID-19 was measured by using the COVID-19 impact event scale (COVID-19 IES), whereas general stress levels were assessed by K10 Kessler Psychological Distress Scale (K10).
Results: The psychological impact of the COVID-19 outbreak revealed that 35.4% of participants suffered from moderate or severe psychological impact (score> 33); 19.7% had a mild psychological impact (scores24– 32), whereas 44.9% reported minimal psychological impact (score < 23). The factors significantly associated with higher stress scores and COVID-19 IES included male gender, low monthly income, having a private business, living in apartments/residential complexes, poor general health status, visit hospital/doctor in the past three months, presence of chronic disease, direct/indirect contact with someone diagnosed with/suspected to have COVID-19, contact with surfaces/tools infected with COVID-19, getting screened or quarantined for COVID-19, follow-up of the latest news about COVID-19 and knowledge of a greater number of people infected and died with COVID-19 (p < 0.05). In contrast, being an elementary school student, having 4– 10 children, observing various protective measures, and staying home for 4– 12 hours were associated with lower COVID-19 IES (p < 0.05).
Conclusion: During the initial six months of the COVID-19 outbreak in Saudi Arabia, 35.4% participants suffered from moderate to the severe psychological impact. This study identified various factors responsible for high COVID-19 IES and K10 stress scores. These findings can help formulate psychological interventions for improving the stress scales in vulnerable groups during the COVID-19 pandemic.
Keywords: COVID-19, stress, psychological impact, Saudi Arabia
Introduction
In December 2019, a cluster of pneumonia cases with a new virus emerged in Wuhan, China. 1 The virus started to propagate gradually through other countries and shortly constituted a worldwide health concern. On 11th February 2020, the novel virus was named of COVID-19 by the WHO, and on 13th March 2020 was declared a pandemic. 1 Locally, the novel virus’s first case was announced in Saudi Arabia on the 2nd of March 2020. 2 The number of confirmed cases started to grow exponentially and affect Saudi residents’ daily lives. 3
The Saudi government took several actions to limit the spread of infection by encouraging people to stay at home and following preventative measures.4 On March 8th, the government introduced online teaching to all students to limit direct human-to-human interactions. In addition, numerous activities including meetings, traveling, and gatherings were postponed throughout the country.5–7 On March 23, a curfew was applied to all cities in Saudi Arabia between 7 p.m. to 6 a.m. Moreover, the curfew was extended to 24 hours on April 2nd in five cities and four governorates (the cities of Riyadh, Dammam, Tabuk, Dhahran, and Alhafoof and the governorates of Jeddah, Taif, Qatif, and AlKhobar) and was modified to start at 3 p.m. on the rest of the cities, the curfew was fully lifted on June 21, 2020, while schools and universities continued the online teaching.5–8
The worldwide strict preventative regulations affected the psychological state of citizens of all countries and stress has been reported to be increased. Stress can be defined as the perception of a threat that results in feelings of discomfort, tense emotions, and difficulty in coping.9 A study conducted in Saudi Arabia during the early months of the pandemic demonstrated high levels of stress and anxiety. The majority of respondents stayed at home for 20–24h to avoid getting infected and were concerned about their family members contracting the infection.4 Review articles by Xiong J also concluded a strong relationship between the COVID-19 pandemic and high levels of psychological stress.10 Moreover, a study in the United States demonstrated other factors causing stress, including the news about the severity of how contagious the virus is, the uncertainty of the quarantine period, and changes in the social and personal care routines.11
On the other hand, some studies suggested that the levels of stress during the pandemic were reduced. Personal control using positive coping strategies was adapted. Acceptance, humor, and planning strategies were used.12 In addition, quarantine allowed people to get enormous support from their families and friends by sharing the same concerns. People had more time to rest and relax to preserve their mental health.13 Moreover, studies have shown that living with parents in urban areas with a stable income was a protective factor against anxiety, depression, and stress.14
Despite the available data on COVID-19, certain aspects of this global pandemic got more attention than others. With the emergence of a new infection, more attention is directed towards uncovering the pathogenesis of this organism, mode of transmission, and possible treatment modalities rather than studying the mental health ramifications.15,16 However, studies have been conducted on the mental health and psychological impact of COVID-19, but most of them have small sample sizes compared to ours.17,18
To conclude, the effect of the pandemic on the psychological state is not yet apparent, and information about the Saudi residents is insufficient. The existing Saudi studies had a small sample size and were conducted on the general population ignoring certain group-to-group variations.4 So, this study was designed to determine the relationship between COVID-19, psychological stress, and various factors, focusing on multiple groups and targeting a considerable sample size.
To our knowledge, to date, this study recruited the “largest sample size” to identify stress factors and COVID-19 IES in the Saudi population.
Patients and Methods
Settings and subjects: This cross-sectional study was conducted at Imam Abdulrahman Bin Faisal University (IAU), Dammam, KSA, from June 2020 until December 2020. The study was ethically approved by DSR, IAU, ethical approval number IRB-UGS-2020-01-320. The study complies with the Declaration of Helsinki. The calculated sample size was 4000. The sample size was calculated using open-source epidemiologic statistics for public health tools software. This calculation was based on the estimated prevalence of psychological stress during COVID-19 pandemic and a target adult population of 1160 in a Saudi survey with: Proportion (psychological stress during pandemic) 28%; Precision (d) 5%; Confidence level 95%.19
The snowball sampling technique was used to recruit the participants. The Saudi government recommended that people isolate themselves at home and minimize their social interaction, the study respondents were invited electronically to respond to the survey. This online survey was translated into Arabic and was distributed to the students of IAU and the general Saudi population. Inclusion criteria were the Saudi nationals who can read, understand and fill the questionnaire, whereas the subjects under the age of 10 years were excluded from the study. Data collection was done in one month (1st September–1st October 2020), and willing participants filled this survey based on their experiences in the last 6 months (from March 2020 –to September 2020, which included the period of curfew, lockdowns, work from home and online line teaching for students). The online survey also included a portion for the informed consent of the participants, which all the study participants signed. For the children (aged 10–16 years), informed consent was taken from their parents/guardians and the questionnaire was filled out under the guidance of the parents/guardians.
Survey Development
The three main tools used in the survey were:
1. K10 Kessler Psychological Distress Scale (K10).
2. “Covid-19 impact event scale” (Covid-19 IES).
3. Structured self-administered questionnaire (SSAQ).
Structured self-administered questionnaire (SSAQ).
SSAQ was developed by the authors, based on three previous surveys on the “psychological impacts of COVID-19 Pandemic on the general population.”4,10,12 These surveys were reviewed and updated by adding and removing some questions. The questionnaire was validated by three experts in medical education, and tested by pilot-testing and reliability analysis. The reliability and validity of the questionnaire (excluding the demographic section) were tested by Cronbach’s alpha and were found to be 0.811.
The SSAQ included various questions that covered six major areas including (1) demographic details and general characteristics of study participants (2) general health status (3) Physical symptoms and contact history related to the COVID-19 pandemic (4) fears/concerns related to covid-19 (5) knowledge about COVID-19 (6) precautionary measures against COVID-19.(Appendix 1)
The psychological impact of COVID-19 was measured by using the COVID-19 impact event scale (COVID-19IES), whereas general stress level was assessed by K10 Kessler Psychological Distress Scale (K10).
K10 Kessler Psychological Distress Scale (K10)
It is a 10-item questionnaire intended to find a global measure of distress based on anxiety and depressive symptoms that a person has experienced in the last month.20 Numbers are assigned to 10 response items, which are added to compile a total score. The score range is from 0 to 50. The subjects are then categorized as having mild, moderate, and severe stress, as below:
<10 =no stress
11–18= mild stress
19–26 = moderate stress
≥27= severe stress
“COVID-19 Impact Event Scale” (COVID-19 IES)
This psychological impact specific to COVID −19 was measured by the “COVID-19 impact event scale” (COVID-19 IES).21 It is a self-administered questionnaire that has been validated in the Chinese population to find out the psychological impact of exposure to the COVID-19 pandemic. This 22-item questionnaire comprises three subscales that aim to measure the mean avoidance, intrusion, and hyperarousal. The subscores are added to compile a total score, based on which the subjects are categorized as having a mild, moderate, and severe psychological impact, as below:
0–23= normal
24–32= mild psychological impact
33–36= moderate psychological impact
>37 = severe psychological impact
(Higher the score, greater the psychological impact).
Statistical Analysis
SPSS version 20 (IBM Corp, Armonk, USA) was used for statistical analysis. Frequencies of all variables were calculated. The linear regression method was used to find univariate associations of sociodemographic variables, general health status, contact history, fear against covid-19, knowledge, and precautions of Covid 19, with the K-10 scores as well as the Covid-19 impact event scale. K-10 scores and covid-19 scores were considered dependent variables, whereas all remaining variables were considered independent variables. For all tests, p less than 0.05 was considered significant.
Results
The response rate was 65%, as 4052 out of 7000 participants completed the questionnaire. The psychological impact of the COVID-19 outbreak, using the IES-R scale, revealed a sample mean score of 25.73 ± 15.30 (Mean±SD). Of all respondents, 1819 (44.9%) reported minimal psychological impact (score<23), 799 (19.7%) had mild psychological impact (scores24–32) whereas 1434 (35.4%) reported moderate or severe psychological impact (score > 33).
The sample mean scores for the K10 scale were 19.44 ± 15.25 (Mean±SD). For the stress subscale (k-10 scores), 1483 of the participants (36.6%) were considered to have a normal score (score: 0–10), 710 (17.5%) suffered from mild stress (score: 11–18), 608 (15%) suffered from moderate stress (score: 19–26) whereas 1251 (30.9%) were considered to be suffering from severe and extremely severe stress (score: 27–42).
Table 1 shows the association between demographic variables and (the COVID-19) impact of the event as well as stress during the epidemic. Male gender, low monthly income, and having a private business were associated with high-stress scores. All age groups were significantly associated with higher K10 and Covid-19 impact scores. Being a student was associated with low-stress levels. The students of elementary school reported the lowest stress levels. 46% of the students mentioned that they enjoy online teaching and 80% enjoyed their home isolation period with their families. Having 1–3 children was associated with significantly higher COVID-19 impact and having 4–10 children with lower impact. Living in villas was also associated with lower covid-19 scores compared to living in apartments and residential complexes.
 |
Table 1 Association Between Demographic Variables and (COVID-19) Impact of Event as Well as Stress During the Epidemic |
Table 2 highlights the association between general health status and (COVID-19) impact of the event as well as stress during the epidemic. The majority of study participants reported their physical health status as “Very good” (42.7%) and were free from chronic illness (86.5%). “Poor general health status” and “visit to hospital/doctor in past three months” were associated with significantly higher scores on the K10 and COVID-19 impact scales. “Presence” of chronic disease” was also related to higher scores in COVID-19 impact.
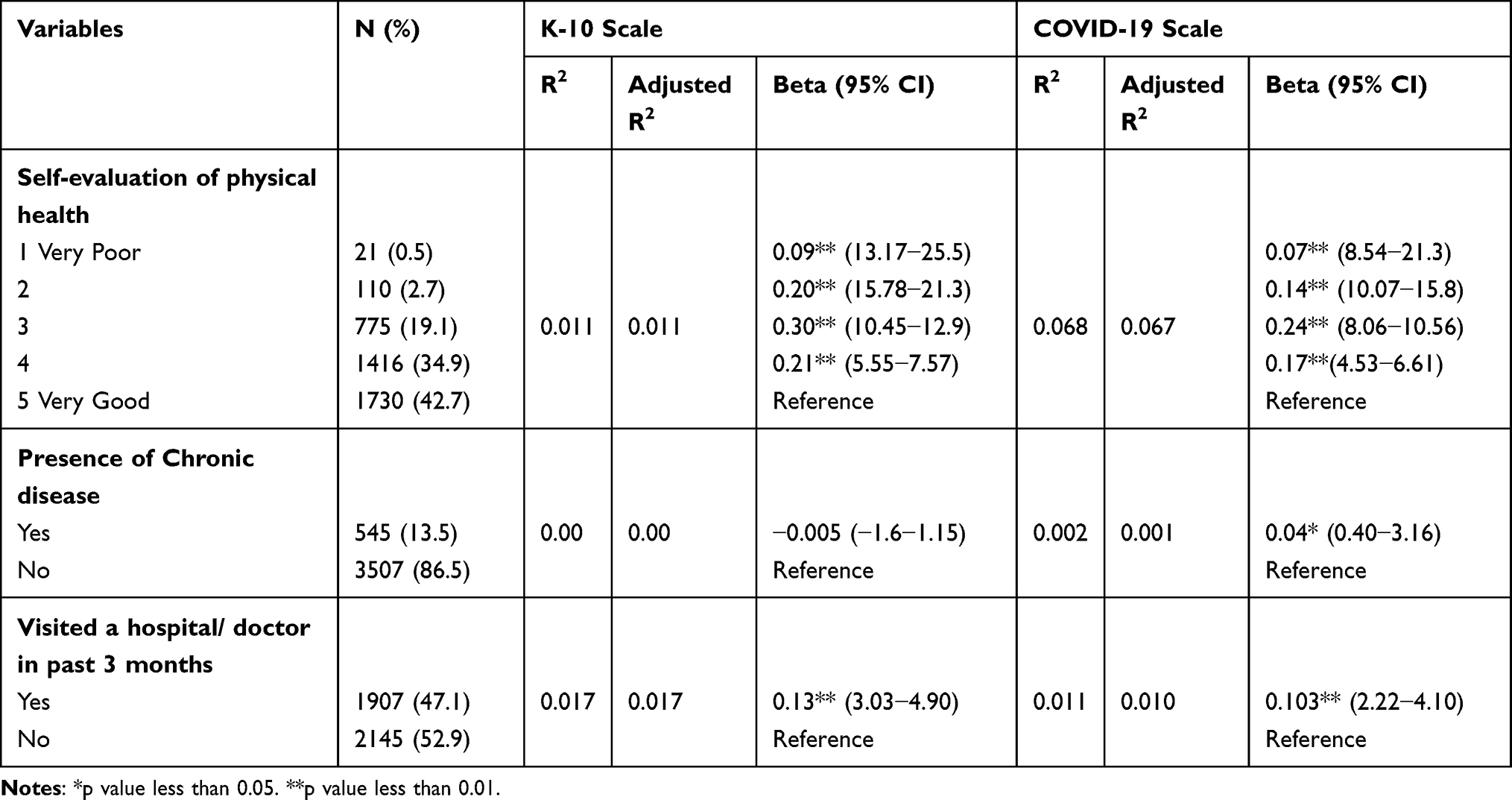 |
Table 2 Association Between General Health Status and (COVID-19) Impact of Event as Well as Stress During the Epidemic. (Already Completed) |
The majority of study participants had no history of direct/indirect contact with COVID-19 (52.1%) or quarantine (81.5%) Table 3. 17.3% of participants had relatives diagnosed with COVID-19, and 45% of the study participants got screened for covid-19. Direct/indirect contact with someone diagnosed with/suspected of having COVID-19 raised stress levels. Moreover, contact with surfaces/tools infected with COVID-19 was also associated with higher k10 scores only. Getting screened for COVID-19, and visiting a hospital in the last six months were also associated with high-stress scores. 18% of our study participants had to do quarantine, either being screened positive or due to a positive contact history also had high-stress scores and COVID-19 impact scales.
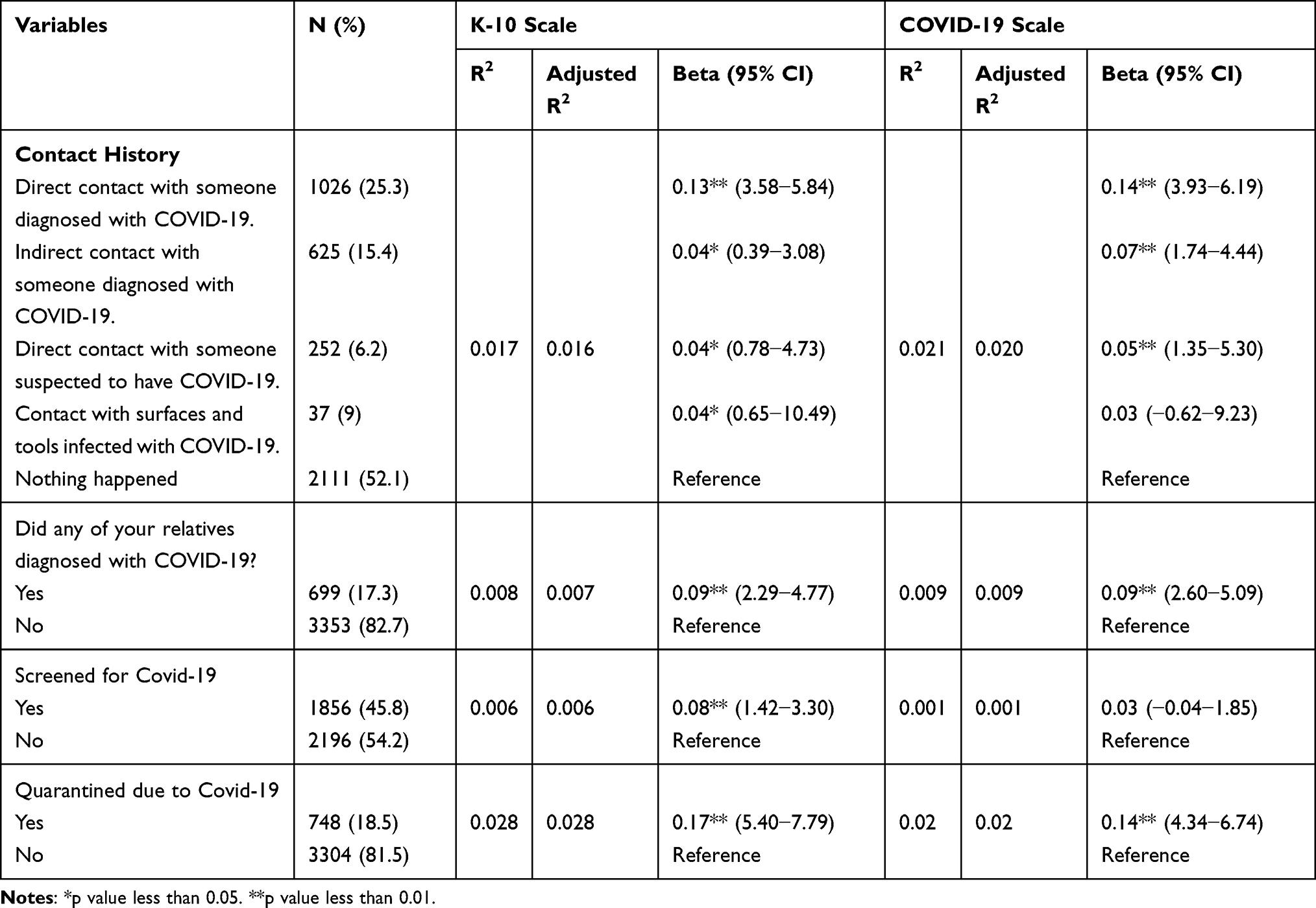 |
Table 3 Association Between Physical Symptoms/Contact History in Past 3 Months and (COVID-19) Impact of Event as Well as Stress During the Epidemic |
Table 4, explores the association between fears against COVID-19 and stress during the pandemic. Regarding Corona, the biggest fear of most of the participants was that Covid-19 can affect their parents.
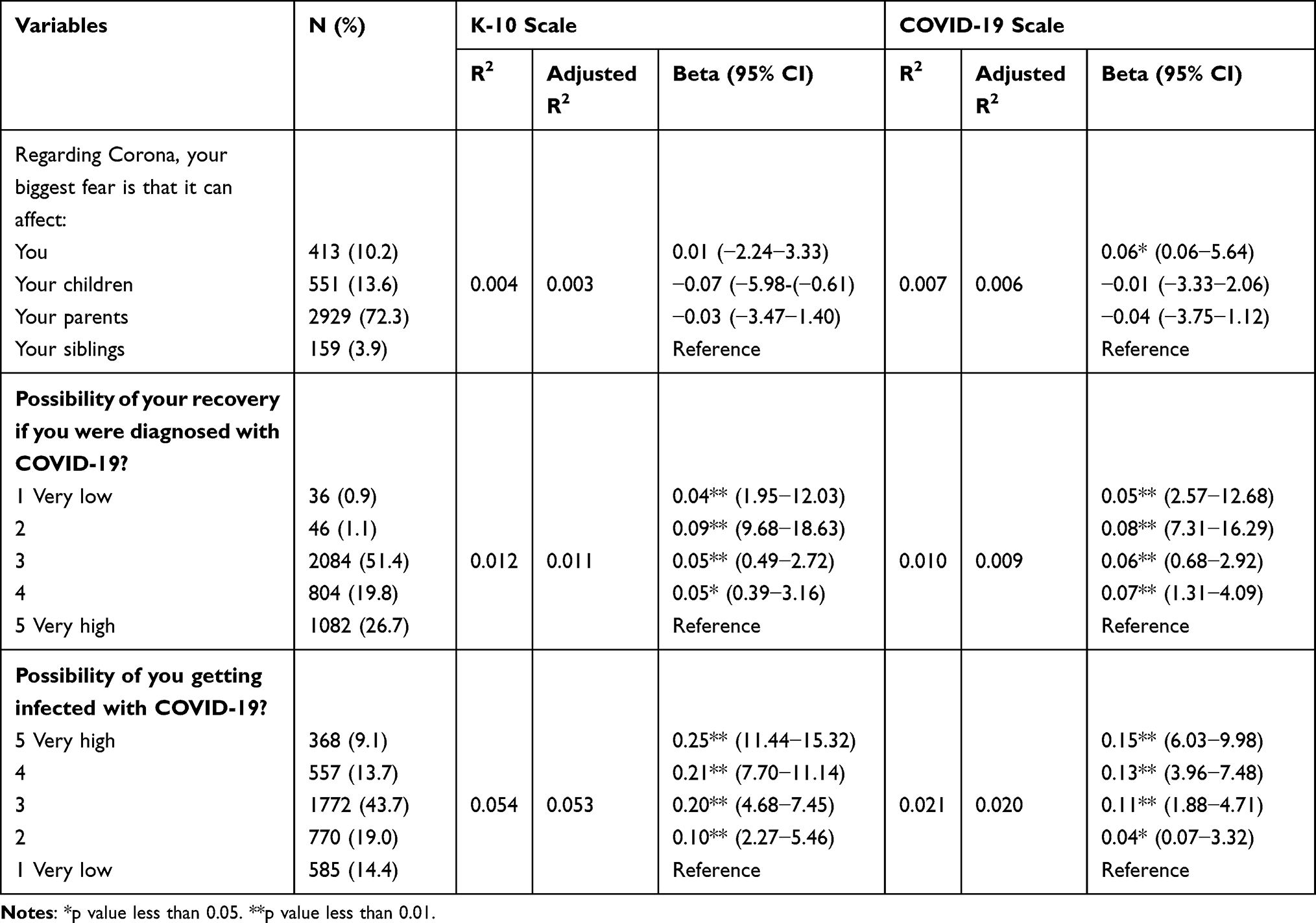 |
Table 4 Association Between Fears Against COVID-19 and (COVID-19) Impact of Event as Well as Stress During the Epidemic |
Table 5, shows the association between Knowledge of COVID-19 and (the COVID-19) impact of the event as well as stress during the epidemic. 90.8% of study participants knew the correct route of transmission of COVID-19. Having less confidence in diagnostic methods of covid-19 and the amount of information available about COVID-19 was associated with higher stress scores. Knowledge of the greater number of people infected with COVID-19 and a greater number of deaths was associated with higher K10 and Covid impact scores. Follow-up of the latest news about Covid vaccines and medication was associated with a higher impact.
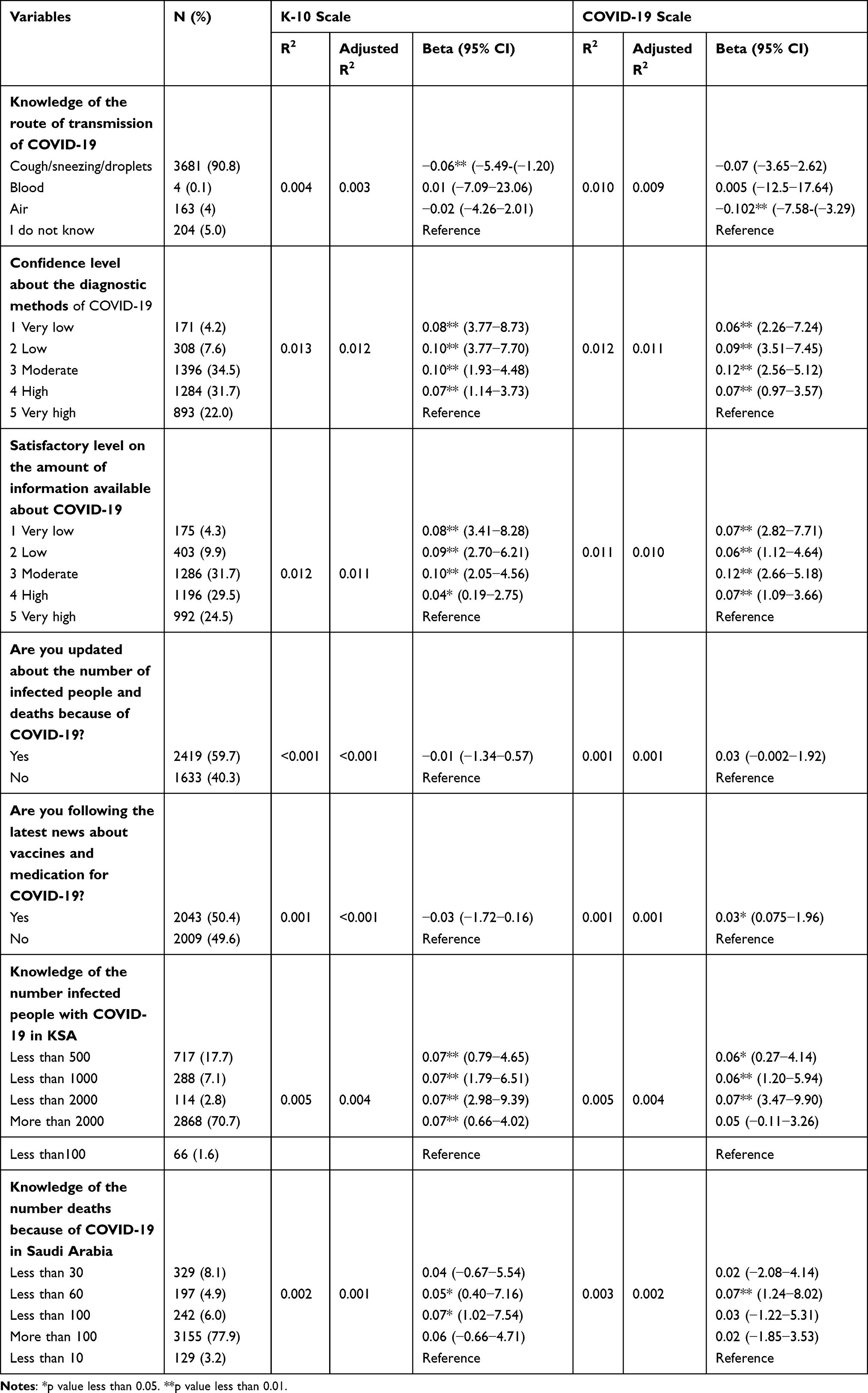 |
Table 5 Association Between Knowledge of COVID-19 and (COVID-19) Impact of Event as Well as Stress During the Epidemic |
The association between precautionary measures against COVID-19 and (COVID-19) Impact on events and stress is shown in Table 6. Observing various protective measures such as home isolation was associated with low impact. Those who stayed home for 4–12 hours had low-stress scores. Failure to follow any of the precautionary measures against COVID-19 was associated with higher K-10 scores. The belief that necessary precautionary measures were associated with lower K-10 and COVID-19 impact scores.
 |
Table 6 Association Between Precautionary Measures Against COVID-19 and (COVID-19) Impact of Event as Well as Stress During the Epidemic |
Discussion
This study aimed to investigate the psychological impact of the COVID-19 outbreak on the general population in Saudi Arabia and its association with multiple factors. In our study, 35.4% of participants suffered from moderate or severe psychological impact (IES >33). Whereas data from other parts of the world showed comparatively high-stress levels in their populations. Passavanti et al examined the psychological impact of Covid −19 in seven different countries and showed that 55.3% of their respondents suffered from moderate to severe stress.22 In addition, another Mexican study revealed moderate and severe impact scores of 50.3% of their study population.23 Comparatively low psychological impact on the Saudi population can be attributed to various factors, including less mortality rate and being confident regarding the governmental actions towards the pandemic.24 For example, shifting schools and universities to virtual learning, travel suspension, holding-up gatherings, and implementation of digital health applications.5,6
Although the psychological impact of COVID-19 was found to be low in the kingdom compared to other countries4,21,22 the levels are still high compared to the pre-pandemic state.25 Therefore, we aimed to identify various factors causing elevated stress scores during the COVID-19 pandemic in the Saudi population.
Male sex was associated with high COVID-19 IES. This opposed other studies, where females had a higher impact on the COVID-19 pandemic.24 The difference might be caused by the financial burden, which males in Saudi society mostly handle.25,26
Regarding the employment status, our results showed that being employed or retired was associated with less COVID-19 IES compared to private business employees. As the private sector has been affected the most since the pandemic started. Some private businesses have been affected significantly, such as tourism, airline transportation, and outpatient services.27 However, those who are retired are already getting pensions, and as per Saudi governmental initiative, most of the employed individuals are being given their regular salary even during the pandemic.28
This study revealed that elementary school students had lower stress levels. The government withheld campus education since March 2020, and the classes are being held online for all school and university students. By our findings, a study examining the perception of students toward online education found that 73% of the participants had enjoyed the e-learning method, mainly due to the ability to stay at home longer and spend time with their families (69%), ability to access the online materials at any desired time (69%) and the feasibility to learn at their own pace (64%).29 On the contrary, another study conducted in Saudi Arabia at the beginning of the pandemic found that students had significantly higher scores of stress, anxiety, and depression 4 Similarly, a study conducted in Serbia found an increase in depression and stress levels in students during the pandemic.30 This may be explained by the disturbance and uncertainty caused by the pandemic on the flow of training and education. Students also reported the two significant disadvantages of social isolation and the technical issues faced during the e-learning process.31
Another interesting finding of this study was that the individuals with one–three children showed high COVID-19 IES compared to those with more than four children. These findings are in consistence with other international studies where families with fewer children had more psychological distress. This may be due to parents’ concerns towards their children during the pandemic, such as their chance of being infected by the novel virus or the responsibility of combining both working from home and taking care of the quarantined child.4,32,33
We also explored the association between “residential type” and stress. The data indicated that living in villas was associated with lower COVID-19 IES than living in apartments. Some studies found that countries and areas where residents tend to live in large, clustered families (ie, co-residence) or tall buildings generally have more deaths due to COVID-19 infections. In addition, it was found that overcrowding was a major risk factor for increasing COVID-19 infection rates.34,35.
This study also inquired about the general health status and its association with Covid −19 IES. The participants who rated their physical health status below “very good”, those who visited a hospital in the past three months, or those with a chronic disease had significantly higher scores of K10 and COVID-19 IES than others. Our data is compatible with other studies conducted in China and Saudi Arabia.4,36,37
Regarding the contact history, contact with diagnosed or suspected COVID-19 individuals either directly or indirectly was associated with high-stress levels. However, maintaining precautionary measures, including hand hygiene, wearing masks, and social distancing, brought protective effects against the virus and psychological stress.4,38
Roughly 18.5% of our study participants had to do quarantine in the past 6 months due to positive tests. It is reported that quarantine raised the stress level in participants, and this was consistent with the reports from various other studies.39–41 Therefore, these groups should be supported by expanding telepsychiatry, focusing on behavioral therapy and relaxation exercises to lower their stress levels.4
Approximately 90.8% of our sample knew the correct mode of transmission of COVID-19, which can be attributed to the availability of information over the internet. A study in the Philippines demonstrated that 98.6% of their sample knew that the transmission is via droplets, and 96.7% believed it can be transmitted through contaminated surfaces.42,43 In addition, 4.2% of our respondents felt less confident in the available diagnostic methods and this group showed higher levels of stress. Other studies also demonstrated higher DASS scores in individuals who think their doctor could not diagnose COVID-19.22,44 Similar to our study population, people vigilantly following the news and internet reported higher stress levels. Moreover, a study in Pakistan showed that 72% of the sample think they will feel less stressed if they do not follow the news. It, therefore, suggested spending no more than 3 hours per day checking the news to avoid excessive stress.44
Knowledge about the number of infected cases daily was associated with increased stress levels among participants. However, it is crucial to keep people updated regarding the number of local cases of infection and recovery. According to a study, people who do not know of the recoveries have higher anxiety levels.43 It perhaps can aid in adherence to health precautions. Furthermore, getting information from a trusted, authorized source is thought to benefit the psychological state of individuals. In a study, 90% of people thought that news from untrusted sources sparks a panic.44 Ministry of health has taken Twitter account to release a daily report of infections, recoveries, and mortalities. They have also dedicated a whole section of their website to this matter. In addition, virtual clinics are now established with an option for mental health support.6,28
Our findings showed that precautionary measures, especially home isolation have protective psychological effects. Consistent with our findings, the individuals who focused on the benefits of staying at home, seeing it as responsible behavior and a requirement for feeling secure, had less severe psychological issues.45 In contrast, some studies indicated home isolation may impact on people’s social lives by limiting contact with others, leading to an increase in feelings of loneliness and social isolation.4
The biggest strength of this study is the large sample size focusing on the general population, thereby ignoring certain group-to-group variations. As with any empirical results, the initial findings from the present study are subject to several limitations. First, data collected from self-reported online surveys cannot directly measure the full psychological impact of the participants compared to professional medical mental health assessments. The second limitation concerns the inability to generalize the study to the whole population, especially among non-social media users and the illiterate.
Conclusion
During the first few months of the COVID-19 pandemic, the psychological impact of the Covid-19 outbreak revealed that 35.4% of participants suffered from moderate or severe psychological impact (score > 33); 19.7% rated mild psychological impact (scores24–32); whereas 44.9% reported minimal psychological impact (score <23).
This study also identified various stress factors responsible for high COVID-19 IES. These findings can help formulate psychological interventions for improving the stress scales in vulnerable groups during this COVID-19 pandemic.
Data Sharing Statement
Data can be obtained from the corresponding author on request.
Ethics Approval
The study was ethically approved by Deanship of scientific research, IAU, ethical approval number IRB-UGS-2020-01-320.
Consent for Publication
The authors give consent to publish the whole content of the article.
Author Contributions
All the authors have made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas. All the authors have contributed significantly in the drafting or writing, or substantially revising or critically reviewing the article. All the authors have agreed on the journal to which the article was submitted. All the authors have reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. All authors gave final approval of the version to be published. All the authors agree to take responsibility and be accountable for the contents of the article.
Funding
This was non funded research.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. World Health Organization.int. Listings of WHO’s response to COVID-19. cited 23 September 2020]; 2020. Available from: https://www.who.int/news-room/detail/29-06-2020-covidtimeline.
2. Moh.gov.sa. MOH News - MOH reports first case of coronavirus infection; 2020 Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-03-02-002.aspx.
3. Covid19.moh.gov.sa. COVID 19 dashboard: Saudi Arabia. [cited 23 September 2020]; 2020. Available from: https://covid19.moh.gov.sa.
4. Alkhamees A, Alrashed S. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr Psychiatry. 2020;102:152–159. doi:10.1016/j.comppsych.2020.152192
5. Algaissi A, Alharbi N, Hassanain M, Hashem A. Preparedness and response to COVID-19 in Saudi Arabia: building on MERS experience. J Infect Public Health. 2020;13(6):834–838. doi:10.1016/j.jiph.2020.04.016
6. Alshammari T, Altebainawi A, Alenzi K. Importance of early precautionary actions in avoiding the spread of COVID-19: Saudi Arabia as an Example. Saudi Pharm J. 2020;28:898–902. doi:10.1016/j.jsps.2020.05.005
7. Yezli S, Khan A. COVID-19 social distancing in the Kingdom of Saudi Arabia: bold measures in the face of political, economic, social and religious challenges. Travel Med Infect Dis. 2020;10:169–172.
8. Spa.gov.sa. An approval issued to fully lift the curfew from 06 am on Sunday, Ban on Umrah, Visit, Int’l flights to continue the official Saudi Press Agency. [cited 29 March 2021]; 2020. Available from: https://www.spa.gov.sa/viewfullstory.php?lang=en&newsid=2100088.
9. Fink G. Stress: Concepts, Cognition, Emotion, and Behavior. Academic Press; 2016.
10. Xiong J, Lipsitz O, Nasri F, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. 2020;277:55–64. doi:10.1016/j.jad.2020.08.001
11. Park C, Russell B, Fendrich M. Americans’ COVID-19 stress, coping, and adherence to CDC guidelines. J Gen Intern Med. 2020;35:2296–2303. doi:10.1007/s11606-020-05898-9
12. Skapinakis P, Bellos S, Oikonomou A. Depression and its relationship with coping strategies and illness perceptions during the COVID-19 lockdown in Greece: a cross-sectional survey of the population. Depress Res Treat. 2020;2020:1–11. doi:10.1155/2020/3158954
13. Zhang Y, Ma Z. Impact of the COVID-19 pandemic on mental health and quality of life among local residents in Liaoning Province, China: a Cross-Sectional Study; 2020. Available from: https://pubmed.ncbi.nlm.nih.gov/32244498.
14. Cao W, Fang Z, Hou G. The psychological impact of the covid-19 epidemic on college students in China. Psychiatry Res. 2020;22:112–119.
15. Sun J, Zhuang Z, Zheng J, Li K. Generation of a broadly useful model for COVID-19 pathogenesis, vaccination, and treatment. Cell. 2020;182(3):734–739. doi:10.1016/j.cell.2020.06.010
16. Attia Y, El-Saadony M, Swelum A. COVID-19 pathogenesis, advances in treatment and vaccine development and environmental impact—an updated review. Environ Sci Pollut Res. 2021;25:236–246.
17. Shah I, Prajapati J. COVID −19 pandemic: immediate psycological impact during the 3TD stage of lockdown among general population of selected areas of Vadodara City. Indian J Forensic Med Toxicol. 2020;11:136–141.
18. Temsah M, Al-Sohime F, Alamro N, et al. The psychological impact of COVID-19 pandemic on health care workers in a MERS-CoV endemic country. J Infect Public Health. 2020;13(6):877–882. doi:10.1016/j.jiph.2020.05.021
19. EPITOOLS. Sample size to estimate a proportion or apparent prevalence with specified precision. Available from: http://epitools.ausvet.com.au/content.php?page=1Proportion&Proportion.
20. Kessler RC, Andrews G, Colpe LJ. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002;32(6):959–976. doi:10.1017/S0033291702006074
21. Horowitz M, Wilner N, Alvarez W. Impact of event scale: a measure of subjective stress. Psychosomatic Med. 1979;41(3):209–218. doi:10.1097/00006842-197905000-00004
22. Passavanti M, Argentieri A, Barbieri DM, et al. The psychological impact of COVID-19 and restrictive measures in the world. J Affect Disord. 2021;283:36–51. doi:10.1016/j.jad.2021.01.020
23. Cortés NY, Lamas R, Vuelvas CR. Psychological effects and associated factors of COVID-19 in a Mexican sample. Disaster Med Public Health Prep. 2020;14(3):413–424. doi:10.1017/dmp.2020.215
24. AlHumaid J, Ali S, Farooq I. The psychological effects of the COVID-19 pandemic and coping with them in Saudi Arabia. Psychol Trauma. 2020;12(5):505–525. doi:10.1037/tra0000623
25. Alhabib K, Batais M, Almigbal T, et al. Demographic, behavioral, and cardiovascular disease risk factors in the Saudi population: results from the Prospective Urban Rural Epidemiology study (PURE-Saudi). BMC Public Health. 2020;20(1):111–121. doi:10.1186/s12889-020-09298-w
26. Almosaed N. Money and power in Saudi family. J King Abdulaziz Univ Arts Humanit. 2008;16(2):61–87. doi:10.4197/art.16-2.3
27. Beirne K, Oorley D, Regan K. The potential costs and distributional effect of covid-19 related unemployment in Ireland; 2020. Available from https://www.esri.ie/system/files/publications/BP202101%20%281%29.pdf.
28. Ministry of investment Initiatives and services introduced by Saudi Arabian government authorities to support businesses during the emerging COVID-19 pandemic; 2021. Available from: https://www.misa.gov.sa/en/covid-19-gov-initiatives.
29. Bączek M, Zagańczyk-Bączek M, Szpringer M. Students’ perception of online learning during the COVID-19 pandemic. Medicine. 2021;100:248–253. doi:10.1097/MD.0000000000024821
30. Vujcic I, Safiye T, Milikic B, et al. Coronavirus disease 2019 (COVID-19) epidemic and mental health status in the general adult population of Serbia: a Cross-Sectional Study. Int J Environ Res Public Health. 2019;18:195–197.
31. Msherghi A, Alsuyihili A, Alsoufi A, et al. Mental health consequences of lockdown during the COVID-19 pandemic: a cross-sectional study. Front Psychol. 2021;12:111–119. doi:10.3389/fpsyg.2021.605279
32. Taylor M, Agho K, Stevens G, Raphael B. Factors influencing psychological distress during a disease epidemic: data from Australia’s first outbreak of equine influenza. BMC Public Health. 2008;8:245–248. doi:10.1186/1471-2458-8-347
33. Mazza C, Ricci E, Biondi S, et al. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: immediate psychological responses and associated factors. Int J Environ Res Public Health. 2020;17:31–65. doi:10.3390/ijerph17093165
34. Aparicio Fenoll A, Grossbard S. Intergenerational residence patterns and Covid-19 fatalities in the EU and the US. Econ Hum Biol. 2021;39:100–134.
35. Meyerowitz E, Richterman A, Gandhi R, Sax P. Transmission of SARS-CoV-2: a Review of Viral, Host, and Environmental Factors. Ann Intern Med. 2021;174(1):69–79. doi:10.7326/M20-5008
36. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069. doi:10.1001/jama.2020.1585
37. Alghamdi S, Alqahtani J, Aldhahir A. Current status of telehealth in Saudi Arabia during COVID-19. J Family Community Med. 2020;27(3):208–211. doi:10.4103/jfcm.JFCM_295_20
38. Lotfi M, Hamblin MR, Rezaei N. COVID-19: transmission, prevention, and potential therapeutic opportunities. Clinica chimica acta. 2020;508:254–266. doi:10.1016/j.cca.2020.05.044
39. Public Health Authority. Guideline for (quarantine - medical isolation) - public health authority; 2021. Available from: https://covid19.cdc.gov.sa/professionals-health-workers/guideline-for-quarantine-medical-isolation-en/.
40. Nkire N, Mrklas K, Hrabok M, et al. COVID-19 pandemic: demographic predictors of self-isolation or self-quarantine and impact of isolation and quarantine on perceived stress, anxiety, and depression. Front Psychiatry. 2021;12:553–560. doi:10.3389/fpsyt.2021.553468
41. Wang P, Wang R, Tian M. The pathways from type A personality to physical and mental health amid COVID-19: a multiple-group path model of frontline anti-epidemic medical staff and ordinary people. Int J Environ Res Public Health. 2021;18:187–194.
42. Rahman HS, Aziz MS, Hussein RH. The transmission modes and sources of COVID-19: a systematic review. Int J Surg Open. 2020;26:125–136. doi:10.1016/j.ijso.2020.08.017
43. Tee ML, Tee CA, Anlacan A. Psychological impact of COVID-19 pandemic in the Philippines. J Affect Disord. 2020;277:379–391. doi:10.1016/j.jad.2020.08.043
44. Khan AA, Lodhi FS, Rabbani U, Ahmed Z, Abrar S, Arshad S. Impact of coronavirus disease (COVID-19) pandemic on psychological well-being of the Pakistani general population. Front Psychiatry. 2021;11:564–569. doi:10.3389/fpsyt.2020.564364
45. Bozdağ F. The psychological effects of staying home due to the COVID-19 pandemic. J Gen Psychol. 2021;18:1–23.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.