Back to Journals » Advances in Medical Education and Practice » Volume 14
The Pros and Cons of Use of Handheld Electronic Devices During Ward Rounds and the Impact of the COVID-19 Pandemic
Authors Suliman S ![]() , Akbar R, Yousaf Z
, Akbar R, Yousaf Z ![]() , Ghazouani H, Al-Mohanadi D, Al-Mohammed A
, Ghazouani H, Al-Mohanadi D, Al-Mohammed A ![]() , Alkhal A
, Alkhal A ![]()
Received 30 October 2022
Accepted for publication 10 March 2023
Published 16 March 2023 Volume 2023:14 Pages 245—255
DOI https://doi.org/10.2147/AMEP.S395501
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Shireen Suliman,1– 3 Raza Akbar,1,2 Zohaib Yousaf,4 Hafedh Ghazouani,1 Dabia Al-Mohanadi,1,5 Ahmed Al-Mohammed,1,2 Abdullatif Alkhal1– 3,5
1Department of Medicine, Hamad Medical Corporation, Doha, Qatar; 2Department of Clinical Medicine, Weill Cornell Medical College, Doha, Qatar; 3College of Medicine, Qatar University, Doha, Qatar; 4Internal Medicine, Tower Health, West Reading, PA, USA; 5Medical Education Department, Hamad Medical Corporation, Doha, Qatar
Correspondence: Shireen Suliman, Hamad General Hospital, Medicine Department, Hamad Medical Corporation, Doha, 3050, Qatar, Email [email protected]
Purpose: The exponential use of handheld electronic devices (HEDs) among healthcare providers has shown the potential to enhance clinical workflows and improve patient care. However, the challenges and risks of carrying these devices during ward rounds and their impact on postgraduate trainees’ (PGTs’) training in general and more specifically during the COVID-19 pandemic need to be explored.
Methods: A cross-sectional mixed-methods online survey was conducted to evaluate the perceptions of trainees and faculty at Accreditation Council for Graduate Medical Education International accredited residency and fellowships programs in Qatar on the use of HEDs on clinical workflow, trainees’ education, and the impact of the COVID-19 pandemic. One hundred and fifty-eight participants were enrolled in the study (87 postgraduate trainees and 71 faculty). Exploratory data analysis and descriptive statistics were performed using STATA version 12 and thematic analysis of 301 qualitative responses to the survey open-ended questions using Atlas. ti qualitative software, version 9.4.0.
Results: Almost all PGTs, 83 (95.4%), and faculty 43 (62.3%) use HEDs during ward rounds. Accessibility of patient information by PGTs 73 (94.8%) and faculty 46 (84.4%) and work efficiency were the main perceived benefits. Hindering communication between team members, disruption of interaction with patients, increased risk of infection and breach of patient confidentiality were among the challenges associated with their use. Carrying devices reduced the frequency of hand hygiene practices and physical examinations of patients by trainees. The COVID-19 pandemic led to a decrease in the use of HEDs by both faculty [38(64%)] and PGTs [42(60%)].
Conclusion: HEDs’ use is valued by both faculty and PGTs in enhancing workflow, trainees’ education, patient experience, and patient care during the COVID-19 pandemic. Graduate medical education leaders should adopt measures to monitor their use during ward rounds as they can negatively impact trainees’ education, reduce interaction with patients, increase the risk of infection, and breach patient confidentiality.
Keywords: COVID-19, handheld electronic devices, ward rounds, postgraduate medical education, Accreditation Council for Graduate Medical Education International, ACGME-I
Introduction
The use of hand-held electronic devices (HEDs) by healthcare providers has been increasing over the last decade for accessing patient information and reference medical information.1 The HEDs include many devices such as smartphones, laptops, tablets, and personal digital assistant devices. The use of computers is one of the predominant activities for residents in inpatient clinical settings.2,3 Having the advantages of being generally small, lightweight, and portable, along with seamless connectivity to wireless networks, HEDs improve access to information during structured rounds and can save time during checking medical data.3 Moreover, HEDs were found to perform better than the non-radiology graded screens for dermatologic photographs, ECG images, chest x-ray, and echocardiographic images.4–6 This coincided with a reported patient’s positive attitude towards HEDs with evident value in patient education and self-management.7–9 Similarly positive benefits have been reported by healthcare providers on patient communications, patient education, and patient perceptions of the provider.10 There is limited evidence on the perceived effect of HEDs on postgraduate medical training necessitating the need for evidence that better understands and optimizes the use of HEDs,7 especially in ward rounds.
Increased use of these HEDs is not without its share of issues, including infection control measures. HEDs have the potential to cause healthcare-associated infections with a reportedly high rate of colonization of mobile devices carried by healthcare workers.11 Due to a lack of clear disinfection policies for personal devices like mobile phones and tablets, the use of these devices increased the risk of contamination between the hands and face, as mobile phones are not regularly disinfected after handling.12 For instance, microbiological sampling of the portable electronic devices used by house officers and attending physicians revealed at least one positive culture from the screen or cover due to low cleaning practices of the devices.13 In addition, mobility and flexibility are the new norms in the COVID-19 pandemic era where the use of personalized HEDs for patient care becomes even more critical when compared to shared workstations. Their use during the pandemic facilitated the clinical work of staff working in isolation settings where they could be shielded to participate in virtual ward rounds to prevent cross-infection.14,15 However, the effect of using of HEDs on the workflow during the COVID-19 pandemic has not been fully studied.
In summary, many studies reported on different dimensions of HEDs, yet, the majority have reported use amongst medical trainees with little mention of the use by faculty.3,16 Moreover, no study has assessed these questions during the Covid-19 pandemic. Therefore, there is a need for a robust study which has not been undertaken to answer many of these questions together – like the overall impact of HEDs on clinical rounds, education, and training of trainees, especially assessing these aspects for both medical trainees and faculty that highlights the paucity of high-quality evidence reported in this domain which further necessitates and justifies our current study.17 At a practical level, healthcare staff working on the frontline during and after the era of the Covid-19 pandemic is going through some major challenges at workplaces. It is crucial to understand the pros and cons of the use and adoption of technology in healthcare delivery systems, including patient care, workflows, and patient electronic medical records. On day-to-day bases, the use of HEDs by medical trainees and faculty is crucial for patient data capturing and retrieval, documentation, medication, and ordering of investigations during clinical rounds. Hence the use of any suitable and appropriate medical devices which can be handheld and portable can have significant impacts on the delivery of such goals, especially in the post-Covid-19 era. This has not been addressed in medical literature, hence the need for our study.
Our study aims to determine the perspectives of both postgraduate trainees (PGTs) and the teaching faculty on the use of electronic devices in the workplace, especially during ward rounds. More specifically, we evaluated the perceived benefits, disadvantages, and challenges with their use in the clinical workflow and PGTs education during inpatient ward rounds. In addition, we also studied the impacts of the COVID-19 pandemic on the use of HEDs.
Materials and Methods
Study Design
A cross-sectional study was conducted at Hamad Medical Corporation (HMC), Doha, Qatar between April 2021 and August 2021. All trainees and faculty from the Accreditation Council for Graduate Medical Education International accredited residency and fellowship programs at HMC were invited to participate in the study. Trainees at the undergraduate level and under internship were excluded from the study. Of the approximately 560 PGTs, 87 responded and were included in the current analysis. Among faculty, the survey was sent to 578 members and 71 total faculty responses were included in the current analysis.
Survey Design
Two surveys (S File), a faculty and a trainee survey were designed to determine the perception of HEDs use during inpatient ward rounds. The unique nature of the question and the dearth of available literature led the authors to generate a questionnaire with the help of the population that is affected by it (ie, trainees and faculty). The survey format included binary, multiple-choice, and Likert scale-type questions with some open-ended questions. It explored the following main parts: (i) the general demographics of the participants, (ii) the impact of HEDs on workflow and patients, (iii) the impact of HEDs on PGTs’ education, and (iv) the impact of the COVID-19 pandemic on the use of HEDs.
Six experts in medical education evaluated the surveys for content and construct validity before their distribution. Changes were made to the questionnaire based on the expert recommendations The calculated Item-content validity index (I-CVI) across all items was 0.90 for both faculty and PGTs surveys. The surveys were distributed using Qualtrics software to all participants via work email by the graduate medical education coordinator. Informed consent was obtained from all study participants with detailed information about the use of the data and its confidentiality, anonymity, and publication of anonymized responses. Responses were recorded once a read receipt for the email was received. Participants were excluded from the response rate calculation if a read receipt was not received. Additionally, to enhance the response, anonymized text messages with links to the surveys were sent to the faculty and PGTs who had not opened the initial survey request by email. These responses were not added to calculate the response rate. Handheld electronic devices (HEDs) were defined as smartphones, iPads, other tablets, laptops, or other portable electronic devices capable of being carried around by an individual during ward rounds.
Ethical Consideration
Ethical approval was obtained by the Medical Research Centre at Hamad Medical Corporation Ethical review board HMC-MRC-01-21-012. All methods were carried out in accordance with the ethical review guidelines and regulations. Informed consent was obtained from all subjects. The survey included the research information sheet that explained the aim of the study and the autonomy participation, confidentiality, and anonymized data analysis.
Data Analysis
Descriptive statistics organized and summarized our sample data, which are presented as the median and interquartile range (IQR) for the numerical variables and frequencies and proportions used for categorical variables. Differences between groups were evaluated using Pearson’s Chi-Squared Test or Fisher’s Exact Test as appropriate. We used the Spearman correlation coefficient to evaluate the Correlation between variables when appropriate. The level of statistical significance was set as p < 0.05. To evaluate if perceptions regarding the HEDs use during ward rounds and the impact of the COVID-19 pandemic differ between PGTs and faculty, all quantitative exploratory data analysis and descriptive statistics were performed using STATA version 12, College Station, TX, USA). This integrated statistical software was utilized because it is convenient, swift, and meticulous. Moreover, it delivers a range of data science functions such as data visualization, manipulation, automated reporting, advanced programming, and broad statistical features. Every effort (including regular checks of data completeness and quality) was undertaken during the data collection phase to avoid missing or spurious data. At the time of statistical analysis, missing data due to incomplete responses were handled primarily by complete case analysis. As a secondary analysis, missing data were imputed using multiple imputations.
We conducted a thematic analysis of 301 qualitative responses to the open-ended questions in the survey using Atlas. ti, version 9.4.0, a qualitative data analysis software that is widely used in academic and social sciences research. It directs the researcher, allowing the use of different types of codes, and enhancing the formulation of categories and themes, thus reducing the time used to analyze data manually. SS conducted open and axial coding18 and generated a preliminary coding scheme including emerging codes and categories. The coding scheme was reviewed by RA and ZY, using constant comparison, and discussed iteratively.19,20
Results
Characteristics of Participants
Of the approximately 560 PGTs, 64 opened the survey, and 49 (77%) responded. Thirty-seven additional PGTs to the survey once the survey link was made available via text message. Hence, 87 total PGTs responses were included in the current analysis. Among faculty, the survey was sent to 578 members via email. Sixty-seven opened the survey, and 50 (75%) responses were received. Twenty-one additional faculty members responded to the survey once the survey link was sent via text message. Hence, 71 total faculty responses were included in the current analysis. The gender distribution in faculty and PGTs was comparable: 57 (65.5%) of the PGTs were men, and 30 (34.5%) were women. In comparison, 44 (62%) of the faculty were men, and 27 (38%) were women. Trainees were younger, with a median age of 28 (26–34) and 47 (39–55) for faculty. Out of the PGTs, 67 (77.9%) of the respondents were residents, and 19 (22.1%) were clinical fellows. The demographics are displayed in Table 1.
 |
Table 1 The Demographic Variables of Participants |
Use of HEDs During Clinical Work
Almost all of the PGTs, 83 (95.4%), and more than half of the faculty, 43 (62.3%), use electronic devices during ward rounds. Handheld Electronic Devices particularly laptops 64 (77.1%) were the most used by PGTs. Trainees use them during 76 (88.4%) after the ward rounds 69 (80.2%) with more preference 60 (69.8%) during the busy post-call rounds and to less extent 26 (30.2%) in the clinics. The primary use for HEDs was for accessing patient information, ordering investigations and medications, and to less extent, patient documentation. Table 2 describes the use of electronic devices in the workplace by both faculty and trainees.
 |
Table 2 The Use of Handheld Electronic Devices in the Workplace |
Impact of the Use of HEDs During Inpatient/Ward Rounds
Table 3 demonstrates faculty and PGTs’ perceived impact of HEDs use in inpatient/ward rounds. Accessibility of patient information was the main benefit of the use of HEDs by PGTs followed by efficiency in ordering investigations and medications and overall better time management as agreed by both faculty and PGTs. Although over 80% (62) of PGTs found that HEDs helped them document patient notes on time, only 33 (53.2%) of the faculty agreed with this with a p-value of 0.0005. PGTs strongly agree with the role HEDs play in providing effective patient education and experience and their overall good perception by patients. A vast majority of PGTs [63(84%)] and faculty [41(69.5%] reported the value of HEDs use in enhancing PGTs learning during rounds by allowing them to access educational information.
 |
Table 3 The Impact of Use HEDs During Inpatient/Ward Rounds |
Among the challenges identified with the HEDs use during inpatient/ward rounds by faculty and PGTs were: hindering communication between team members during inpatient/ward rounds and increased risk of infection. Of all the PGTs, 73 (100%), were aware of their responsibilities to protect the patient’s sensitive information and confidentiality while using HEDs during ward rounds. Yet, one-third of the faculty believe that the use of HEDs carries the risk of breaching patient confidentiality. Trainees highlighted some technical issues with carrying the HEDs such as their weight and the need for connection and charging. Overall, HEDs use was recommended by both the faculty and PGTs, 44 (73%) and 57 (85%), respectively.
Impact of COVID-19 Pandemic on HEDs Use During Workflow
Despite the reduced use of HEDs during the COVID-19 pandemic by faculty [38(64%)] and PGTs [42(60%)], almost two-thirds [46 (65.7%)] of PGTs reported that HEDs facilitated patient care during the COVID-19 pandemic. Forty-five (64%) of PGTs became stricter in following infection control precautions. Almost all of the PGTs [71(98.6%)] found it vital to have an infection control policy for using electronic devices at the workplace, and 65 (89%) stated that it is vital to receive orientation on infection control measures related to electronic device usage at the workplace.
Qualitative Analysis of the Trainees and Faculty Surveys
Four themes emerged from the qualitative analysis of the survey: (1) We value the use of HEDs during ward rounds, (2) We are aware of the risks of use of HEDs during ward rounds, (3) The COVID-19 impacted our use of HEDs during ward rounds, and (4) Suggestions to use HEDs during ward rounds wisely. PGTs are identified with (R) and faculty with (F) in the supporting quotes. This is shown in Table 4.
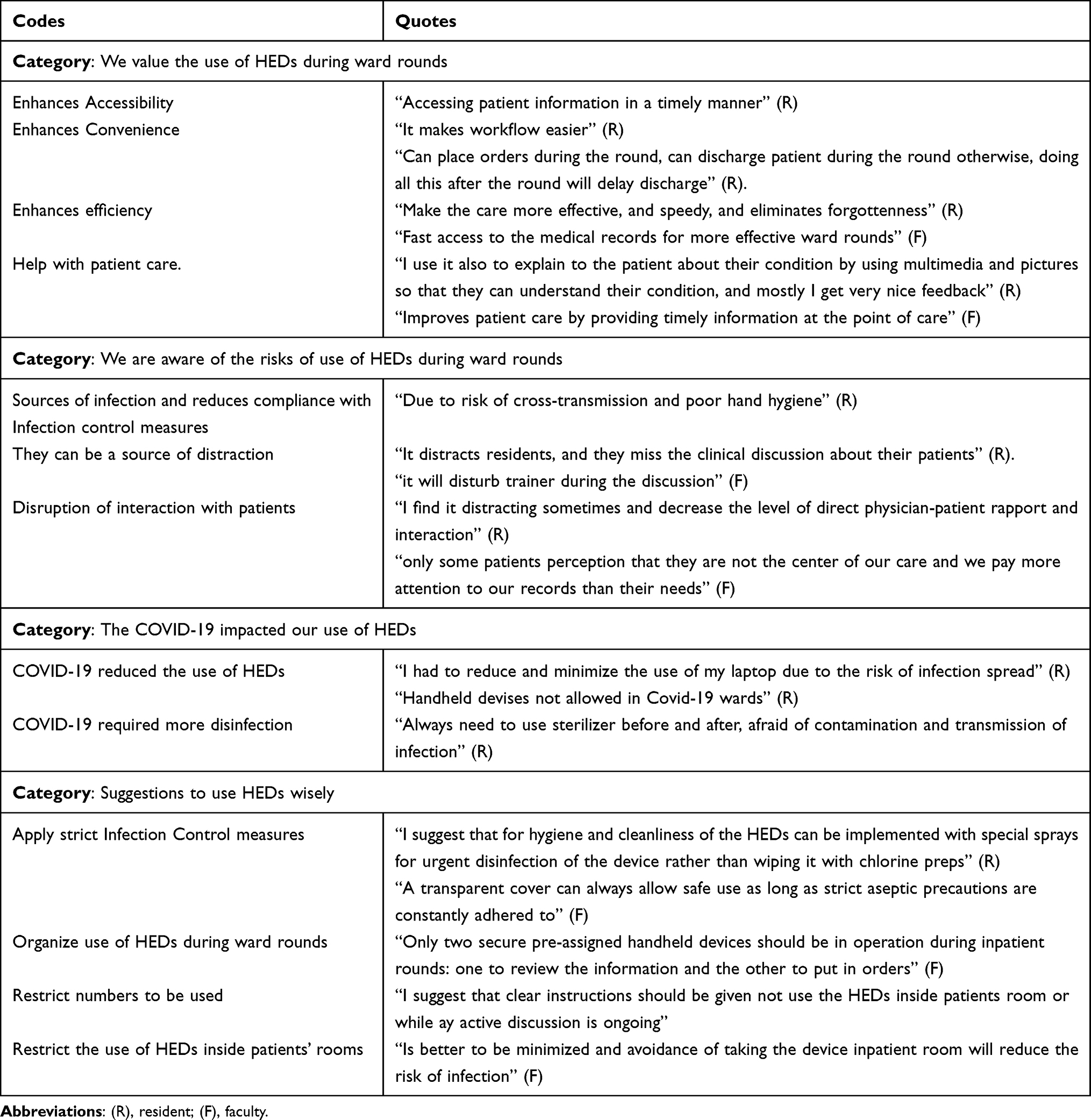 |
Table 4 The Four Themes with Codes and Exemplar Quotations |
The survey respondents valued the use of HED devices and their impact on the workflow during ward rounds. HEDs during ward rounds allowed access to information, were convenient with ease of ordering, and were efficient and faster. Participants also identified several disadvantages of the use of HEDs during ward rounds: (1) a source of distraction that disrupts interaction with patients and communication between team members, (2) a potential source of infection due to reduced compliance with hand hygiene and device cleaning practices, and (3) a risk of breaching security and patient confidentiality. Besides finding them occupying both hands and heavy to carry during the rounds, PGTs strongly believe that
If handheld devices are banned, the quality of patient care will be seriously damaged (R)
This is because PGTs can be enormously busy with the work demand and load of clinical work, and the limited number of computers due to the increase in the numbers of several undergraduates and PGTs, coupled with low speed of Wi-Fi, makes it
Impractical to wait for a desktop to carry out the necessary orders as it will cause a massive delay in patient care (R)
The majority of respondents perceived the COVID-19 pandemic had affected the use of HEDs during ward rounds. PGTs reduced their use in the patient’s wards and increased the frequency of disinfection due to the perceived risks of infection.
Finally, Table 5. provides a summary of faculty/trainee perceived barriers to HED use and suggestions for improvement.
 |
Table 5 A Summary of Faculty/Trainee Perceived Barriers to HED Use and Suggestions for Improvement |
Discussion
Our study investigated the HEDs use in the workplace from both PGTs and faculty’s perspectives. Two surveys were distributed among the faculty and the PGTs exploring the HEDs use at the workplace with perceived benefits on the workflow and PGTs training, the challenges with their use, and the impact of the COVID-19 pandemic on their use.
The findings confirmed the broad utilization of the HEDs by the faculty and PGTs during the workflow and particularly during ward rounds. PGTs favored the use of laptops during ward rounds as they allowed for timely accessing patient information, enhancing work efficiency in ordering investigations, medications, and documentation of patients’ encounters leading to better time management and patient flow. This is in line with previous research which demonstrated that the use of HEDs such as iPads or Tablets during ward rounds may contribute to increased clinical efficiency, reduced hours spent on administrative tasks, enhanced educational opportunities for residents, and promoted workflow.3,16,21 Handheld computers provided easy access to clinical decision support systems and patient management systems, which improved decision-making for patient care. This ties in with a previous study that showed access to information regarding patient investigation status and the patient condition are crucial for decision-making during morning activities, including ward rounds.22 HEDs saved time and gave easier and quick access to new information that enhanced work patterns and efficiency.
Regarding their impact on patient care, most PGTs and faculty found HEDs use in ward rounds useful in providing patients’ education and enhancing the overall patient experience and satisfaction. In addition, the provision of timely information at the point of care is translated to better patient care which was established in previous work.23 Studies showed that HEDs improved patient communications and inpatient education and engagement in discharge planning and the whole process of care when used in combination with health information resources.24,25 Nevertheless, our findings highlighted the distracting nature of HEDs that might compromise direct physician-patient rapport and interaction during ward rounds. Mobile phones were also seen as promoting a nonprofessional image and appearing rude or impersonal when used in front of patients.9,10
Besides patient care and experience, bedside teaching and PGTs education are crucial during ward rounds and have been shown to improve certain clinical diagnostic skills amongst medical students and residents.17 Our study showed mixed findings on the impact of HEDs use on PGTs training during ward rounds. Similar to previous studies, the use of HEDs improved efficiency, accessibility, and quality of communication with the use of mobile devices with a positive impact on interprofessional interactions and involvement of senior decision-makers in clinical care.26 Yet, HEDs were considered distractors to interpersonal communication and clinical discussions between team members. In addition, the practice of conducting physical examinations on patients by the trainees during ward rounds is challenged by the carrying of these devices.
Concerns about the potential harm of HEDs use in the workplace that needs to be addressed, were highlighted in this study. Firstly, accessing patient information might compromise patient confidentiality and our study added to the previous literature about both faculty and PGTs’ concerns about the security and confidentiality of patient information with the use of personal devices.27 Thus, it is advised to seek permission from patients before integrating smartphones into the provider-patient relationship and thus respecting patient autonomy.28 Secondly, holding these devices makes it challenging for the PGTs to comply with hand hygiene and infection control practices, potentially leading to a reduction in infection control measures. A previous study identified a potential risk with mobile devices and recommended that the routine disinfection of these devices should be incorporated into infection control standards which can significantly reduce the incidence of nosocomial infections presently reported in medical facilities.13,29–31 Thirdly, the use of those devices during the COVID-19 pandemic was even more challenging. There was an exponential increase in the use of electronic devices during the COVID-19 pandemic due to its accessibility of patient information for staff in isolation facilities, allowing them to participate in virtual ward rounds and support front-line staff with clinical advice and administrative support and their use in telehealth services.14,15 However, our study showed reduced use of HEDs in ward rounds during the COVID-19 pandemic because of the risks of infection. Their use in the COVID-19 wards was even prohibited to reduce the risks of transmission of the virus. Despite all this, participants found their use to be very productive as PGTs felt that they facilitated patient care and that it was safer to use them rather than the computers with multiple users at the stations - yet their overall use was still reduced during the COVID-19 pandemic. Policies and restrictions around the use of HEDs were suggested by the faculty: (i) reducing the total number of devices simultaneously used by the team members, (ii) restricting their use inside patients’ rooms, and (iii) if required at all for patient education, then strict infection control measures should be applied.
Study Limitations and Future Directions
A limitation of our study is the low response rate to surveys in both trainees (87/560, 15.5%) and faculty (74/578, 12.8%). This low response might be due to the survey being conducted in the middle of the pandemic when the health staff was overworked. Also, this may be related to the development of survey fatigue during a pandemic.32 The majority of people did not even open the email containing the link to the survey. However, considering the number of people who opened the email, the response rate was good (76.4% in faculty and 77% in trainees). Although we included both faculty and trainees’ perspectives, another limitation of the study is that the findings were drawn from a sample of participants, all of whom belonged to a single institution that may not be completely transferable to other institutions. Despite the rich information obtained during the pandemic, another limitation is the cross-sectional methodology that makes it worthwhile to conduct a multi-institutional study that incorporates qualitative methodology in attaining rich data about the use of HEDs with the inclusion of the perspectives of other healthcare providers involved during ward rounds such as nurses, clinical pharmacists, and patients.
Conclusion
HEDs use is the new reality during inpatient ward rounds. The results add to the previous literature both the perspectives of faculty and postgraduate trainees. It suggests the added value of their use in enhancing the workflow, trainees’ education, and patient experience. Despite their reduced use during the COVID-19 pandemic, and is prohibited in COVID wards, the use of HEDs facilitated patient care. However, their use can be a source of distraction, reduce interaction with patients, increase the risk of breaching patient confidentiality, and can negatively impact trainees’ education as being source of distraction during discussion during ward rounds and reduce the physical examination practices by trainees. This study signifies the value of HEDs devices and addressed their risks, especially during pandemic situations. The results of this study provide a basis for future research on measures to be adopted by graduate medical education leaders in monitoring their use during ward rounds to ensure their effectiveness in trainees’ education, compliance with patient data confidentiality, and infection control measures. The latter is of paramount importance, especially during pandemic situations.
Acknowledgments
The authors would like to thank the faculty and the postgraduate trainees who participated in the study. Open access funding is is provided by the Qatar National Library.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dexheimer JW, Borycki EM. Use of mobile devices in the emergency department: a scoping review. Health Informatics J. 2015;21(4):306–315. doi:10.1177/1460458214530137
2. Oxentenko AS, Manohar CU, McCoy CP, et al. Internal medicine residents’ computer use in the inpatient setting. J Grad Med Educ. 2012;4(4):529–532. doi:10.4300/JGME-D-12-00026.1
3. Fleischmann R, Duhm J, Hupperts H, Brandt SA. Tablet computers with mobile electronic medical records enhance clinical routine and promote bedside time: a controlled prospective crossover study. J Neurol. 2015;262(3):532–540. doi:10.1007/s00415-014-7581-7
4. Caffery L, Armfield N, Smith A. Radiological interpretation of images displayed on tablet computers: a systematic review. Br J Radiol. 2015;88(1050):20150191. doi:10.1259/bjr.20150191
5. Choi BG, Mukherjee M, Dala P, et al. Interpretation of remotely downloaded pocket-size cardiac ultrasound images on a web-enabled smartphone: validation against workstation evaluation. J Am Soc Echocardiogr. 2011;24(12):1325–1330. doi:10.1016/j.echo.2011.08.007
6. Toomey RJ, Rainford LA, Leong DL, et al. Is the iPad suitable for image display at American board of radiology examinations? Am J Roentgenol. 2014;203(5):1028–1033. doi:10.2214/AJR.13.12274
7. Archer N, Fevrier-Thomas U, Lokker C, McKibbon KA, Straus SE. Personal health records: a scoping review. J Am Med Inform Assoc. 2011;18(4):515–522. doi:10.1136/amiajnl-2011-000105
8. Mackert M, Love B, Whitten P. Patient education on mobile devices: an e-health intervention for low health literate audiences. J Inf Sci. 2009;35(1):82–93. doi:10.1177/0165551508092258
9. Scholl J, Groth K. Of organization, device and context: interruptions from mobile communication in highly specialized care. Interact Comput. 2012;24(5):358–373. doi:10.1016/j.intcom.2012.06.002
10. Wyber R, Khashram M, Donnell A, Meyer-Rochow GY. The Gr8est good: use of text messages between doctors in a tertiary hospital. J Commun Healthc. 2013;6(1):29–34. doi:10.1179/1753807612Y.0000000019
11. Heyba M, Ismaiel M, Alotaibi A, et al. Microbiological contamination of mobile phones of clinicians in intensive care units and neonatal care units in public hospitals in Kuwait. BMC Infect Dis. 2015;15(1):1–9. doi:10.1186/s12879-015-1172-9
12. Foong YC, Green M, Zargari A, et al. Mobile phones as a potential vehicle of infection in a hospital setting. J Occup Environ Hyg. 2015;12(10):D232–D235. doi:10.1080/15459624.2015.1060330
13. Khan A, Rao A, Reyes-Sacin C, et al. Use of portable electronic devices in a hospital setting and their potential for bacterial colonization. Am J Infect Control. 2015;43(3):286–288. doi:10.1016/j.ajic.2014.11.013
14. Doraiswamy S, Abraham A, Mamtani R, Cheema S. Use of telehealth during the COVID-19 pandemic: scoping review. J Med Internet Res. 2020;22(12):e24087. doi:10.2196/24087
15. Raza A, Mukherjee S, Patel V, Kamal N, Lichtarowicz-Krynska E. Smartphone use in virtual student teaching and virtual ward rounds during and after the COVID-19 pandemic? BMJ Innov. 2021;7:4.
16. Lobo MJ, Crandley EF, Rumph JS, et al. Pilot study of iPad incorporation into graduate medical education. J Grad Med Educ. 2013;5(1):142–144. doi:10.4300/JGME-D-12-00007.1
17. Peters M, Ten Cate O. Bedside teaching in medical education: a literature review. Perspect Med Educ. 2014;3(2):76–88. doi:10.1007/S40037-013-0083-Y
18. Watling CJ, Lingard L. Grounded theory in medical education research: AMEE Guide No. 70. Med Teach. 2012;34(10):850–861. doi:10.3109/0142159X.2012.704439
19. Corbin J, Strauss A. Basics of Qualitative Research.
20. Glaser B, Strauss A. The Discovery of Grounded Theory: Strategies for Qualitative Research. Aldine Publishing Company; 1967. doi:10.1097/00006199-196807000-00014
21. Duhm J, Fleischmann R, Schmidt S, Hupperts H, Brandt SA. Mobile electronic medical records promote workflow: physicians’ perspective from a survey. JMIR Mhealth Uhealth. 2016;4(2):e5464. doi:10.2196/mhealth.5464
22. Kim J, Lee Y, Lim S, Kim JH, Lee B, Lee J-H. What clinical information is valuable to doctors using mobile electronic medical records and when? J Med Internet Res. 2017;19(10):e8128. doi:10.2196/jmir.8128
23. Walker KE, Migneault D, Lindsay HC, Abu-Laban RB. Use of personal mobile devices to record patient data by Canadian emergency physicians and residents. Can J Emerg Med. 2019;21(4):455–459. doi:10.1017/cem.2019.29
24. Greysen SR, Khanna RR, Jacolbia R, Lee HM, Auerbach AD. Tablet computers for hospitalized patients: a pilot study to improve inpatient engagement. J Hosp Med. 2014;9(6):396–399. doi:10.1002/jhm.2169
25. Schooley B, Walczak S, Hikmet N, Patel N. Impacts of mobile tablet computing on provider productivity, communications, and the process of care. Int J Med Inform. 2016;88:62–70. doi:10.1016/j.ijmedinf.2016.01.010
26. Martin G, Khajuria A, Arora S, King D, Ashrafian H, Darzi A. The impact of mobile technology on teamwork and communication in hospitals: a systematic review. J Am Med Inform Assoc. 2019;26(4):339–355. doi:10.1093/jamia/ocy175
27. Prochaska MT, Bird A-N, Chadaga A, Arora VM. Resident use of text messaging for patient care: ease of use or breach of privacy? JMIR Med Inform. 2015;3(4):e4797. doi:10.2196/medinform.4797
28. Hitti E, Hadid D, Melki J, Kaddoura R, Alameddine M. Mobile device use among emergency department healthcare professionals: prevalence, utilization and attitudes. Sci Rep. 2021;11(1):1–8. doi:10.1038/s41598-021-81278-5
29. Cremers-Pijpers S, van Rossum C, Dautzenberg M, Wertheim H, Tostmann A, Hopman J. Disinfecting handheld electronic devices with UV-C in a healthcare setting. Infect Prev Pract. 2021;3(2):100133. doi:10.1016/j.infpip.2021.100133
30. Otter JA, Yezli S, Salkeld JA, French GL. Evidence that contaminated surfaces contribute to the transmission of hospital pathogens and an overview of strategies to address contaminated surfaces in hospital settings. Am J Infect Control. 2013;41(5):S6–S11. doi:10.1016/j.ajic.2012.12.004
31. Wagoner M, Snyder S, McCarty M, et al. Routine disinfection of mobile communication devices in the postanesthesia care unit. J Perianesth Nurs. 2019;34(6):1176–1180. doi:10.1016/j.jopan.2019.03.011
32. De Koning R, Egiz A, Kotecha J, et al. Survey fatigue during the COVID-19 pandemic: an analysis of neurosurgery survey response rates. Front Surg. 2021;8:690680. doi:10.3389/fsurg.2021.690680
 © 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.