")
Back to Journals » Cancer Management and Research » Volume 11
The prognostic value of serum albumin–globulin ratio in early-stage non-small cell lung cancer: a retrospective study
Authors Wang Y , Li S, Hu X, Wang Y, Wu Y, Li P, Che G
Received 18 October 2018
Accepted for publication 6 March 2019
Published 24 April 2019 Volume 2019:11 Pages 3545—3554
DOI https://doi.org/10.2147/CMAR.S191288
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmet Emre Eşkazan
Yan Wang,1,* Shuangjiang Li,1,* Xu Hu,2,* Yanwen Wang,2 Yanming Wu,1 Pengfei Li,1 Guowei Che1
1Department of Thoracic Surgery, West China Hospital, Sichuan University, Chengdu 610041, People’s Republic of China; 2West China School of Medicine, Sichuan University, Chengdu 610041, People’s Republic of China
*These authors contributed equally to this work
Background: Previous studies demonstrated a significant association between the albumin–globulin ratio (AGR) and various types of cancers. The aim of this study was to evaluate the prognostic value of preoperative AGR in patients with early-stage non-small cell lung cancer (NSCLC).
Methods: Patients diagnosed as NSCLC in a single center between January 1, 2014 and February 29, 2016 were retrospectively reviewed. AGR was defined as the ratio between the serum albumin level and the serum globulin level. Receiver operating characteristics analysis was performed to determine optimal cutoff values. Overall survival (OS) and disease-free survival (DFS) were clinical outcomes of our study. Univariate and multivariate Cox regression analyses were used to identify independent prognostic factors, and the Kaplan–Meier method was used to estimate survival curves.
Results: A total of 279 early stage NSCLC patients were enrolled in our study with the median follow-up of 39 months (range 1–56 months). The statistical analyses manifested that the age (hazard ratio (HR)=1.045, 95% confidence interval (95% CI): 1.010–1.081, P=0.011) and AGR P=0.002) were independent prognostic factors for OS; larger tumor (HR=1.211, 95% CI: 1.011–1.450, P=0.038) and AGR P=0.036) were significantly associated with decreased DFS.
Conclusion: The current research reported that the preoperative AGR was an independent prognostic factor for both OS and DFS in early NSCLC, and patients with AGR <1.51 were more likely to have a poor prognosis.
Keywords: albumin-globulin ratio, early non-small cell lung cancer, overall survival; disease-free survival
Introduction
Lung cancer remains the leading cause of cancer-related death in the world and non-small cell lung cancer (NSCLC) accounts for 85% of lung cancer.1 In 2015, there were approximately 221,200 newly diagnosed lung cancer cases and 158,400 died of this malignancy in the United States.2 With the advances in the diagnostic methods of NSCLC, early-stage patients are far more than before, and there are already more patients in the early stage than in the advanced stage in our center.
Previous studies revealed that many clinical and laboratory factors were significantly associated with clinical outcomes of lung cancer such as gender, age, smoking history, body mass index (BMI), baseline serum CEA value and abnormally elevated lactate dehydrogenase,3–7 and increased evidence demonstrated that both the body nutritional status and chronic inflammation played an important role in the prognosis of several kinds of cancers including NSCLC.8–13
Albumins and globulins are the main components of serum proteins. Albumins reflect the nutritional status of the human body, and some investigators have proved that hypoalbuminemia is an independent risk factor of survival in several cancers including gastric, colorectal, breast and lung cancers.8–10 Globulin family consists of alpha, beta, and gamma globulins and globulin plays a crucial role in immunity and chronic inflammation.10,11 A number of studies manifested that high inflammatory parameters such as alpha and gamma globulins were associated with significantly poor overall survival (OS) in cancer patient.14–18 Low albumin and high globulin are both independent prognostic factors of various cancers including NSCL.14–20 However, the albumin and globulin levels can be interfered by many factors such as illness, dehydration and fluid retention, which limit their application and credibility in clinic.21,22
The albumin–globulin ratio (AGR = albumin/total protein-albumin) combines the two strong prognostic factors, nutrition status and systemic inflammation response; so, we hypothesized that this ratio may also have a high prognostic value. In the current study, for the first time, we aimed to evaluate the prognostic value of serum AGR in early NSCLC.
Material and methods
Study design
This is a retrospective study from a single center.
Patients
Patients diagnosed as early-stage NSCLC in the same medical group of the Department of Thoracic Surgery, West China Hospital, between January 1, 2014 and February 29, 2016 were assessed. The diagnoses of NSCLC were confirmed pathologically by bronchoscopic biopsies, CT-guided needle specimens or surgically resected specimens. The inclusion criteria were as follows: 1) patients were histologically diagnosed as NSCLC; 2) patients were in tumor-node-metastasis (TNM) stage I or II based on the 7th TNM classification of lung cancer by the Union for International Cancer Control (UICC); 3) patients received thoracoscopic radical lung resection; 4) patients received the biochemistry test within 1 week before the surgery; 5) patients had normal liver function. The exclusion criteria were as follows: 1) patients received neoadjuvant therapy; 2) patients received another surgery within 3 months preoperatively; 3) patients with detectable hematology diseases, liver diseases, inflammatory or infectious diseases; 4) transfusion of albumin or globulin preoperatively; 5) recurrent tumors; 6) combined with other tumors; 7) data incomplete or could not be obtained.
Data collection
We extracted clinicopathologic data of all patients from the medical records, including the gender, age, smoking history, BMI, preoperative comorbidity, preoperative lung function representing by forced expiratory volume in one second (FEV1), forced vital capacity (FVC) and FEV1/FVC, tumor location, size, histology, resection type, TNM stage and laboratory data.
Definition of the preoperative AGR and endpoint events
The AGR was defined as the ratio between the preoperative serum albumin level and globulin level. OS and disease-free survival (DFS) were end points of our study. OS was defined as the interval from the date of surgery to the date of death caused by any causes or the date of the last follow-up. DFS was defined as the interval from the date of surgery to the date of recurrence, metastasis or last follow-up. We obtained the follow-up information from out-patients clinic records or telephone contacts.
Statistical analysis
The Microsoft Office Excel 2007 (Microsoft Corporation, Redmond, WA, USA) was used for data collection, and the IBM SPSS Statistics for Windows, version 22.0 (IBM Corp, USA) was used for statistical analyses. The optimal cutoff values were obtained by receiver operating characteristics (ROC) curves, as the values at the largest Youden Index. Continuous and categorical variables were presented as the mean±standard deviation (SD) and frequencies, respectively. Student’s t-test or one-way analysis of variance were used for comparison of continuous variables, and χ2 test or Fisher’s exact test were used for comparison of categorical variables separately. Prognostic factors for OS and DFS were identified via the Cox regression model. Univariate regression analyses were used to identify potential risk factors associated with a poor prognosis, and variables with a P-value<0.05 were enrolled in multivariate regression analyses. Survival curves were estimated via Kaplan–Meier analysis, and the survival differences between groups were assessed via the log-rank test.
All statistical tests were two-sided and P-values<0.05 were considered statistically significant.
Results
Basic patient characteristics
We included a total of 279 early-stage NSCLC patients in accordance with the inclusion criteria and exclusion criteria, with a median follow-up of 39 months (1–56 months). Detailed patient selection process is shown in Figure 1.
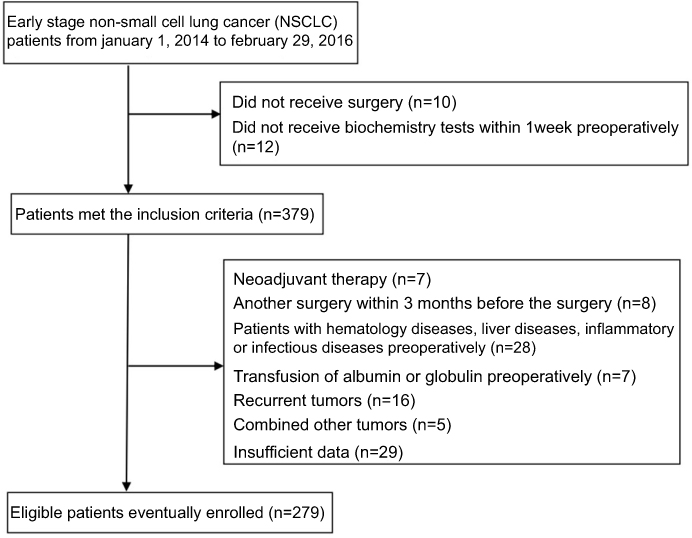 | Figure 1 Patient selection process. |
Basic patient characteristics are presented in Table 1. Among the 279 early-stage NSCLC patients, 145 patients were male, the mean age of all patients was 62.16 years and 124 patients were current or ex-smokers. A total of 128 patients had at least one kind of preoperative comorbidities including hypertension, diabetes mellitus, chronic obstructive pulmonary disease (COPD), coronary heart disease and emphysema. One hundred and one cases were located at the left and 194 cases were adenocarcinomas which accounted for the majority. One hundred and ninety patients received lobectomy, and the number of patients in TNM stage I and II were 246 and 33, respectively.
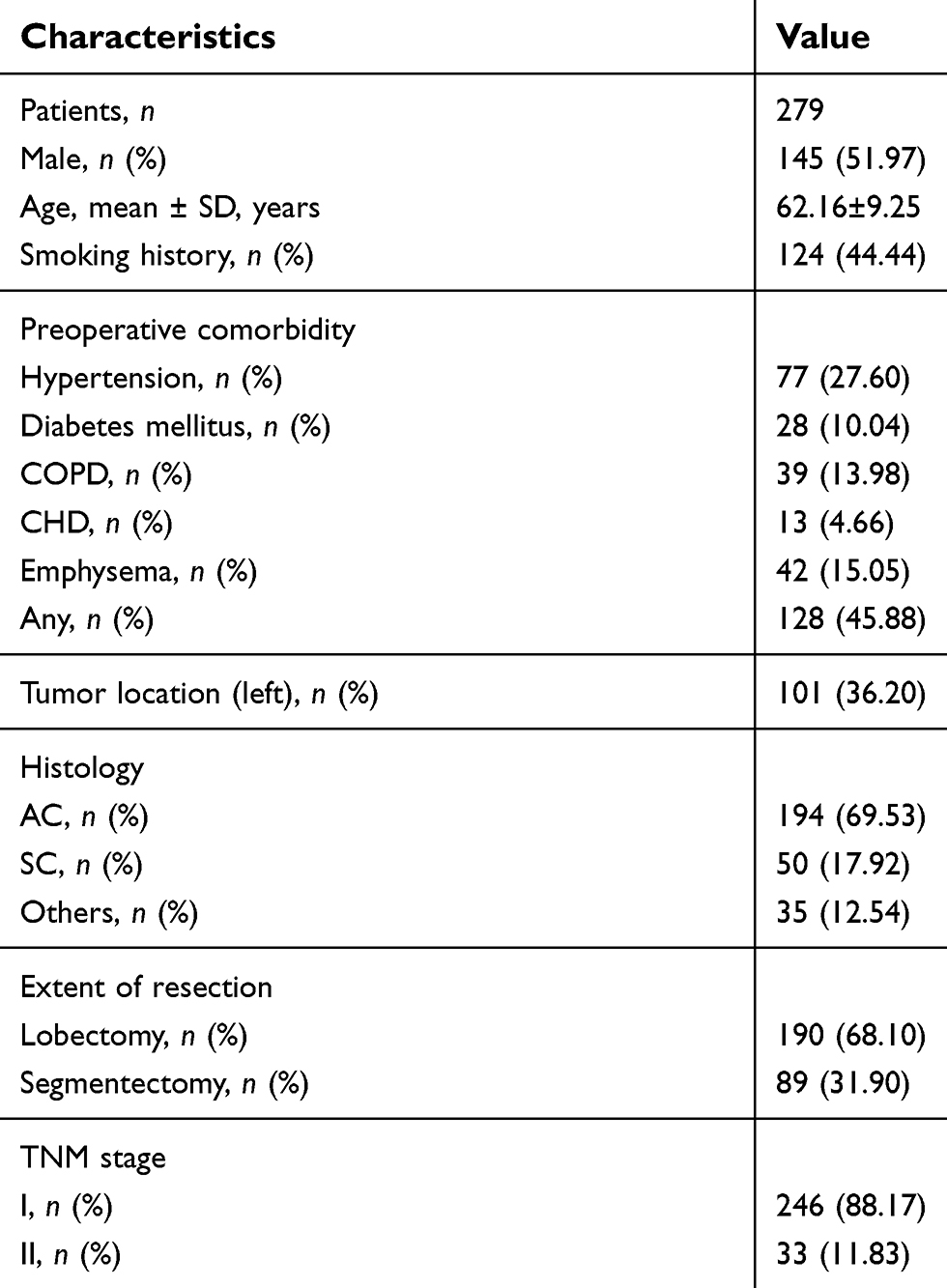 | Table 1 Baseline clinicopathologic characteristics |
The optimal cutoff values according to ROC curves
The cutoff value of the AGR for predicting OS was 1.51 (sensitivity of 69.1% and specificity of 67.0%, area under the curve (AUC) =0.698) (Figure 2A). The cutoff value of the AGR for predicting DFS was also 1.51 (sensitivity of 57.1% and specificity of 64.1%, AUC =0.589) (Figure 2B).
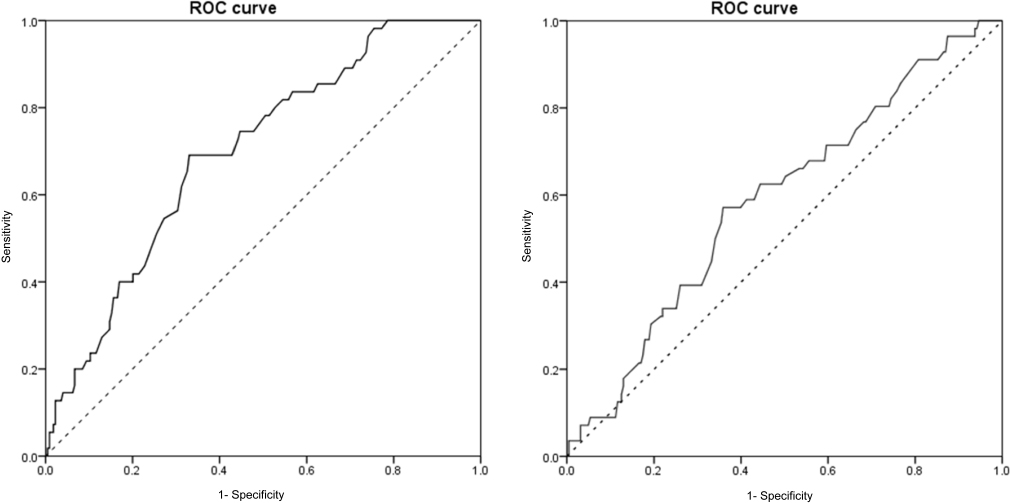 | Figure 2 (A) ROC curve of the AGR for predicting OS. (B) ROC curve of the AGR for predicting DFS. Abbreviations: ROC, receiver operating characteristic; AGR, albumin-globulin ratio; OS, overall survival; DFS, disease-free survival. |
Associations between the AGR and clinicopathologic characteristics
According to the optimal cutoff value of AGR, we divided 112 patients with AGR <1.51 into the low AGR group and 167 patients with AGR ≥1.51 into the high AGR group and then we compared differences of clinicopathological characteristics between the two groups (Table 2). The preoperative AGR significantly correlated with the FEV1 (P=0.038), FVC (P=0.026), tumor size (P<0.001), TNM stage (P=0.011), albumin level (P<0.001) and globulin level (P<0.001). However, there was no significant association between the AGR and histological type (P=0.238).
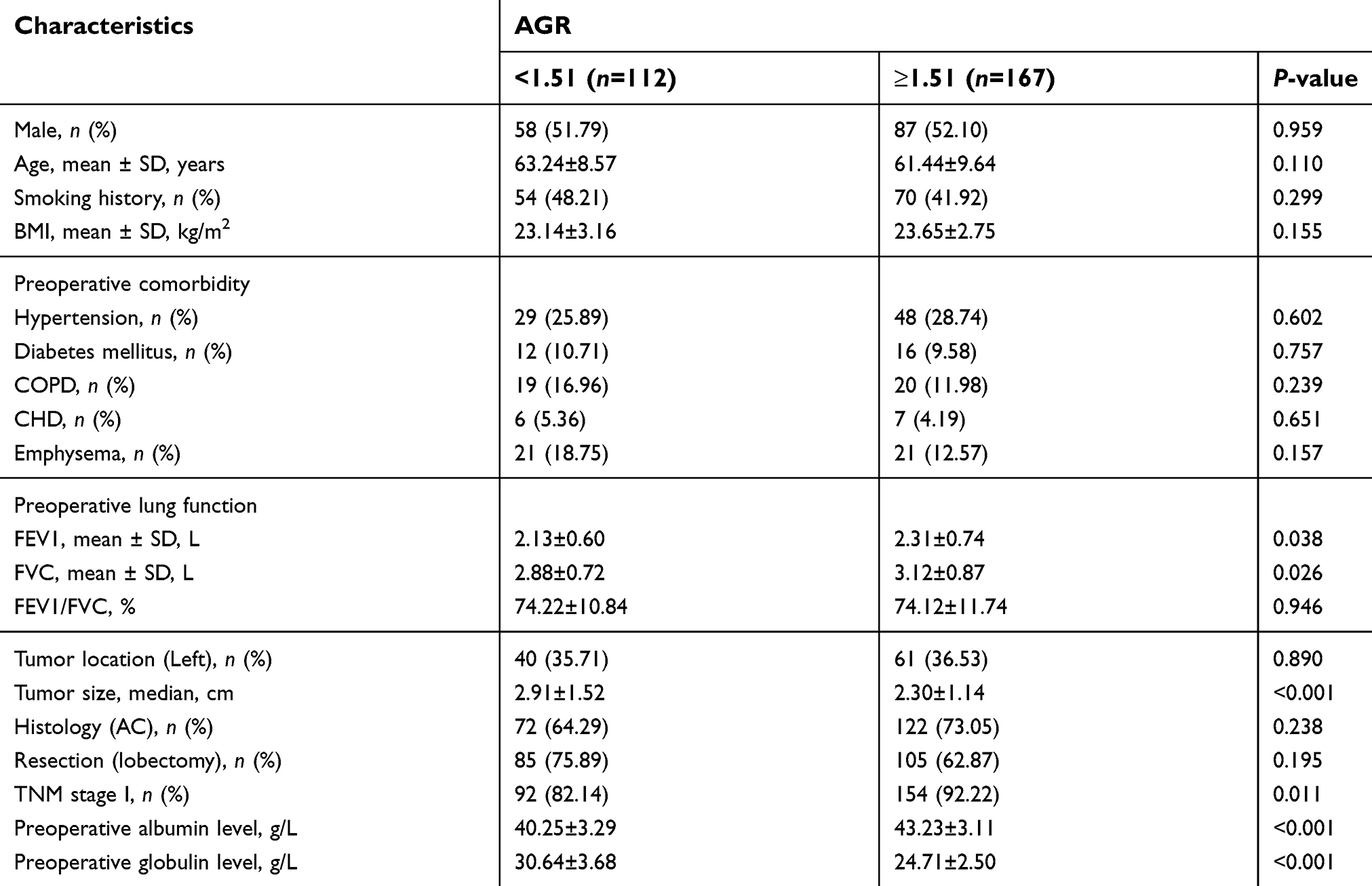 | Table 2 Associations between the AGR and clinicopathologic characteristics |
Univariate and multivariate Cox regression analyses for OS
Univariate analyses demonstrated that the age (P=0.002), history of smoking (P=0.039), history of emphysema (P=0.040), tumor size (P=0.043), low albumin level (P=0.001), high globulin level (P<0.001) and AGR <1.51 (P<0.001) were potential risk factors for a worse OS. Multivariate analyses indicated that only the age (hazard ratio (HR)=1.045, 95% confidence interval (95% CI): 1.010–1.081, P=0.011) and AGR <1.51 (HR=3.424, 95% CI: 1.600–7.331, P=0.002) significantly correlated with poor OS. Detailed information is shown in Table 3.
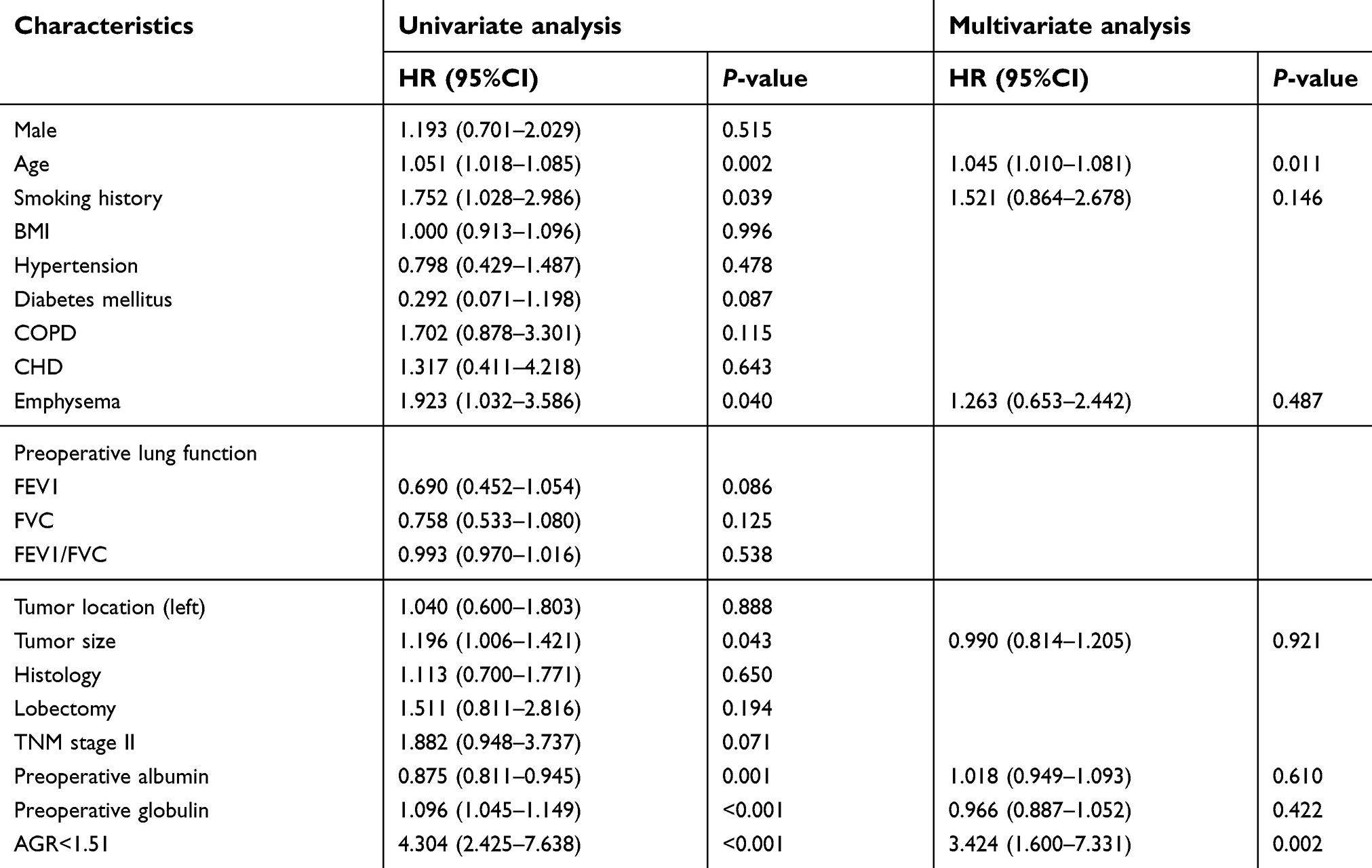 | Table 3 Univariate and multivariate Cox regression analyses to assess the prognostic factors of OS |
Univariate and multivariate Cox regression analyses for DFS
Univariate analyses manifested that the history of COPD (P=0.022), history of emphysema (P=0.015), tumor size (P<0.001), lobectomy (P=0.013), high globulin level (P=0.043) and AGR <1.51 (P=0.001) were potential risk factors for a worse DFS. On multivariate analysis, larger tumor (HR=1.211, 95% CI: 1.011–1.450, P=0.038) and AGR <1.51 (HR=2.177, 95% CI: 1.052–4.508, P=0.036) were independently associated with poor DFS. Detailed data is presented in Table 4.
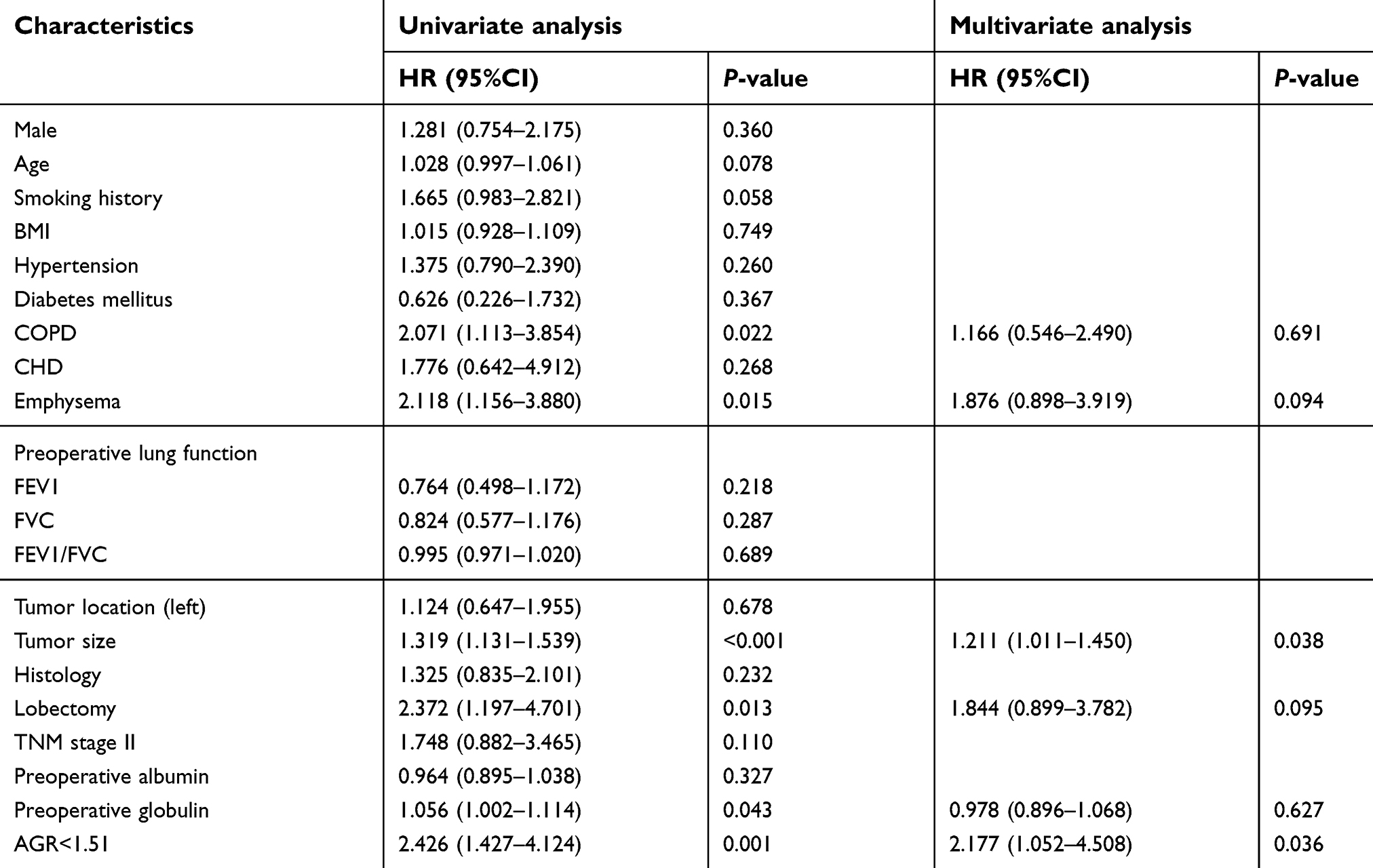 | Table 4 Univariate and multivariate Cox regression analyses to assess the prognostic factors of DFS |
Postoperative OS based on the AGR
Patients with AGR <1.51 (P<0.001; Figure 3A) were significantly associated with a poorer OS rate. Median OS in low AGR group was 37 months (mean ± SD, 36.99±12.22) compared with 45 months (mean ± SD, 43.37±8.57) in high AGR group (P<0.001).
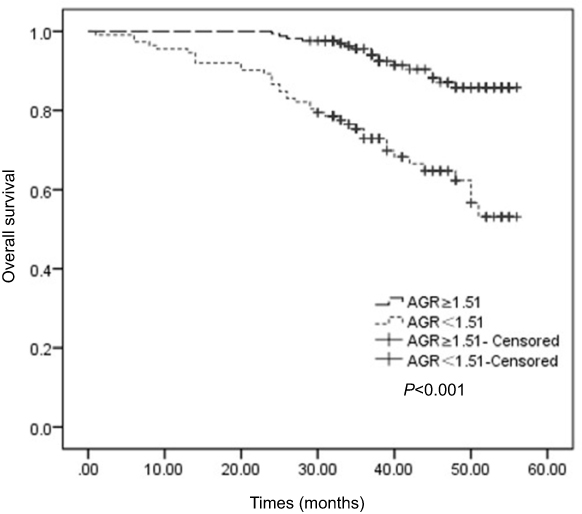 | Figure 3 Kaplan–Meier survival curves showing the relationship between the AGR and OS. Abbreviations: AGR, albumin-globulin ratio; OS, overall survival. |
Postoperative DFS based on the AGR
Patients with AGR ≥1.51 (P=0.001; Figure 4) were associated with a significantly improved DFS rate. Median DFS in patients with AGR ≥1.51 was 39 months (mean ± SD, 41.38±10.43) compared with 35 months (mean ± SD, 34.14±13.31) in patients with AGR <1.51 (P<0.001).
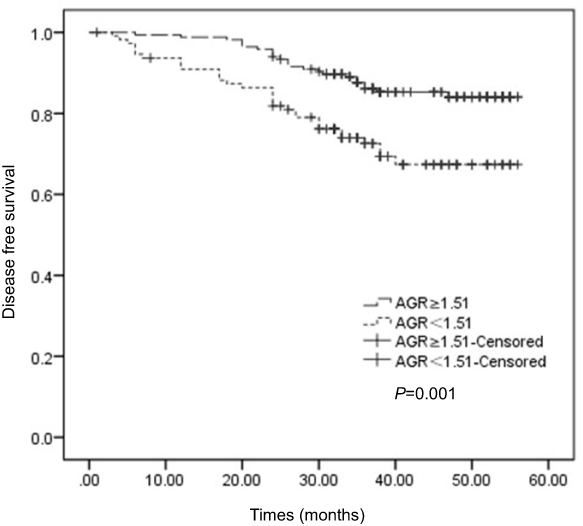 | Figure 4 Kaplan–Meier survival curves showing the relationship between the AGR and DFS. Abbreviations: AGR, albumin-globulin ratio; DFS, disease-free survival. |
Discussion
In the current study, we testified the prognostic value of preoperative AGR in early NSCLC for the first time. Patients with AGR <1.51 had worse OS and DFS. The results of multivariate analysis showed that AGR was an independent factor associated with OS and DFS. Besides AGR, age and tumor size were demonstrated to be independent prognostic factors for OS and DFS, respectively.
Serum albumins account for the largest proportion of serum proteins and play an important role of the human body by maintaining the colloid osmotic pressure of blood, acting like transporters and binding fatty acids, hormones, pharmaceuticals and cations.20,22 It is produced by the liver and one of the indicators of liver function evaluation (Child–Pugh).23 Previous research showed that lower albumin levels indicated worse nutrition status and clinical outcomes of several types of cancers.24–27 Besides, albumin plays a crucial role in the drug delivery in chemotherapy which is one of the mechanisms that albumin affects the prognosis of cancer patients.28,29 However, the albumin level can be interfered by many factors such as illness, hepatic insufficiency, stress and changes of body fluid volume; so, it failed to be widely applied to predict prognosis of cancer patients in the clinic.
Globulins are calculated by the formula (total serum protein-albumin) and have been proven to be related with immunity and chronic inflammation.22 They contain a large amount of immunity-related proteins such as C-reactive proteins (CRP), immunoglobulins, interleukins, complements, etc.20 The prognostic value of these inflammatory proteins has been verified in some research. Higher CRP level indicated worse survival in lung cancer and colorectal cancers, and C3 and C4 were proven to be negative predictors for survival in lung cancer.30–32 Furthermore, a high level of immunoglobulins was an independent risk factor for poor prognosis of lung cancer patients.32 Numerous studies manifested that the chronic inflammation played a vital role in tumor proliferation, metastasis and immune evasion involving all types of serum globulins such as the CRP, tumor necrosis factors, etc.20,29–32 These serum globulins secreted by tumor-associated cells can promote tumor development, metastasis, angiogenesis and immunosuppres-sion.20,29–32 Unfortunately, the level of globulin can also be interfered by various conditions, which limits its utility in predicting the prognosis of cancer patients.
Instead of the absolute concentration of albumin and globulin, AGR is a ratio which combines the two indexes. We supposed that the AGR could demonstrate the prognostic effect in lung cancer mainly for the following two reasons. First, the low AGR is a combination of two significant predictive factors for adverse outcomes, low albumin and high globulin. Second, as we mentioned above, the levels of albumin and globulin can be affected by some conditions such as fluid retention and dehydration, but AGR would not be affected by these conditions. Therefore, we believed AGR was capable of evaluating outcomes of lung cancer patients.
A few studies have examined the prognostic value of AGR in lung cancer.21,22,30 Yao et al manifested a significant connection between pretreatment AGR and advanced NSCLC.21 In the study of Duran et al, low AGR was proved to be a valuable predictor of long-term mortality in lung adenocarcinoma.22 Zhou et al reported that the AGR <1.29 was an independent risk factor of worse OS in small-cell lung cancer patients.30 However, none of them focused on early-stage NSCLC. Therefore, we designed the present research to explore the correlation between the AGR and prognosis in early NSCLC, and we reported that the AGR <1.51 was associated with significantly worse OS and DFS in early-stage NSCLC patients.
The most important clinical significance of our study is that the preoperative AGR may not only assess the risk of early-stage NSCLC patients but also assist the decision-making for therapeutic schedules. In detail, compared with limited stage NSCLC patients with high pretreatment AGR, patients with low preoperative AGR should be treated more actively and the neoadjuvant or postoperative adjuvant therapy may be more beneficial and adaptable for these patients under the same conditions. Meanwhile, preoperative therapies for the inflammation response and nutritional status may improve outcomes of early-stage NSCLC patients. However, these recommendations or opinions still need to be further evaluated.
There were several limitations in our research. First, this is a retrospective study from a single center, so large-scale prospective studies are still needed to verify our findings. Second, we determined 1.51 as the optimal cutoff value of AGR and the critical values in previous studies ranged from 0.90 to 1.93,33 which meant 1.51 may not be the most suitable cutoff value to predict prognosis of early NSCLC. Third, the follow-up period in our study was a bit short, and so we failed to calculate the five-year survival rate among the study population. Fourth, due to the lack of external data, we were unable to design a validation group to verify our findings.
In conclusion, our study first reported the correlation between the preoperative AGR and prognosis of early NSCLC. Preoperative AGR was significantly associated with OS and DFS of early-stage NSCLC patients and superior to the albumin and globulin in predicting prognosis. The role of AGR in the estimation of clinical outcomes still needs to be verified with more large-scale prospective research.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Ethics Committee of West China Hospital, Sichuan University and national research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Because of the nature of retrospective design, the Ethics Committee of West China Hospital approved the current study and also determined that the informed consent was not required.
Informed consent
Written informed consent for the information to be stored and used in the hospital database was obtained from each patient.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30. doi:10.3322/caac.21166
2. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29. doi:10.3322/caac.21294
3. Tas F, Ciftci R, Kilic L, Karabulut S. Age is a prognostic factor affecting survival in lung cancer patients. Oncol Lett. 2013;6:1507–1513. doi:10.3892/ol.2013.1566
4. Wainer Z, Wright GM, Gough K, et al. Impact of sex on prognostic host factors in surgical patients with lung cancer. ANZ J Surg. 2017;87:1015–1020. doi:10.1111/ans.13728
5. Yoshino I, Maehara Y. Impact of smoking status on the biological behavior of lung cancer. Surg Today. 2007;37:725–734. doi:10.1007/s00595-007-3516-6
6. Inomata M, Hayashi R, Tokui K, et al. Lactate dehydrogenase and body mass index are prognostic factors in patients with recurrent small cell lung cancer receiving amrubicin. Tumori. 2016;102:606–609. doi:10.5301/tj.5000435
7. Fizazi K, Cojean I, Pignon J-P, et al. Normal serum neuron specific enolase (NSE) value after the first cycle of chemotherapy: an early predictor of complete response and survival in patients with small cell lung carcinoma. Cancer. 1998;82:1049–1055. doi:10.1002/(ISSN)1097-0142
8. Oñate-Ocaña LF, Aiello-Crocifoglio V, Gallardo-Rincón D, et al. Serum albumin as a significant prognostic factor for patients with gastric carcinoma. Ann Surg Oncol. 2007;14:381–389. doi:10.1245/s10434-006-9093-x
9. Gupta D, Lis CG. Pretreatment serum albumin as a predictor of cancer survival: a systematic review of the epidemiological literature. Nutr J. 2010;9:69. doi:10.1186/1475-2891-9-69
10. Azab B, Kedia S, Shah N, et al. The value of the pretreatment albumin/globulin ratio in predicting the long-term survival in colorectal cancer. Int J Colorectal Dis. 2013;28:1629–1636. doi:10.1007/s00384-013-1748-z
11. Azab BN, Bhatt VR, Vonfrolio S, et al. Value of the pretreatment albumin to globulin ratio in predicting long-term mortality in breast cancer patients. Am J Surg. 2013;206:764–770. doi:10.1016/j.amjsurg.2013.03.007
12. Yin Y, Wang J, Wang X, et al. Prognostic value of the neutrophil to lymphocyte ratio in lung cancer: a meta-analysis. Clinics (Sao Paulo). 2015;70:524–530. doi:10.6061/clinics/2015(07)10
13. Yuan C, Li N, Mao X, et al. Elevated pretreatment neutrophil/white blood cell ratio and monocyte/lymphocyte ratio predict poor survival in patients with curatively resected non-small cell lung cancer: results from a large cohort. Thorac Cancer. 2017;8:350–358. doi:10.1111/1759-7714.12454
14. Canna K, McArdle PA, McMillan DC, et al. The relationship between tumour T-lymphocyte infiltration, the systemic inflammatory response and survival in patients undergoing curative resection for colorectal cancer. Br J Cancer. 2005;92:651–654. doi:10.1038/sj.bjc.6602419
15. Dai J, Tang K, Xiao W, et al. Prognostic significance of C-reactive protein in urological cancers: a systematic review and meta-analysis. Asian Pac J Cancer Prev. 2014;15:3369–3375.
16. Kaya V, Yildirim M, Demirpence O, et al. Prognostic significance of basic laboratory methods in non-small-cell-lung cancer. Asian Pac J Cancer Prev. 2013;14:5473–5476.
17. Shimada H, Nabeya Y, Okazumi S, et al. Elevation of preoperative serum C-reactive protein level is related to poor prognosis in esophageal squamous cell carcinoma. J Surg Oncol. 2003;83:248–252. doi:10.1002/jso.10275
18. Soliman NA, Keshk WA, Shoheib ZS, et al. Inflammation, oxidative stress and L-fucose as indispensable participants in schistosomiasis-associated colonic dysplasia. Asian Pac J Cancer Prev. 2014;15:1125–1131.
19. Jin Y, Zhao L, Peng F. Prognostic impact of serum albumin levels on the recurrence of stage I non-small cell lung cancer. Clinics (Sao Paulo). 2013;68:686–693. doi:10.6061/clinics/2013(05)17
20. He J, Pan H, Liang W, et al. Prognostic effect of albumin-to-globulin ratio in patients with solid tumors: a systematic review and meta-analysis. J Cancer. 2017;8:4002–4010. doi:10.7150/jca.21141
21. Yao Y, Zhao M, Yuan D, et al. Elevated pretreatment serum globulin albumin ratio predicts poor prognosis for advanced non-small cell lung cancer patients. J Thorac Dis. 2014;6:1261–1270. doi:10.3978/j.issn.2072-1439.2014.07.13
22. Duran AO, Inanc M, Karaca H, et al. Albumin-globulin ratio for prediction of long-term mortality in lung adenocarcinoma patients. Asian Pac J Cancer Prev. 2014;15:6449–6453.
23. Cholongitas E, Papatheodoridis GV, Vangeli M, et al. Systematic review: the model for end-stage liver disease–should it replace Child-Pugh’s classification for assessing prognosis in cirrhosis? Aliment Pharmacol Ther. 2005;22:1079–1089. doi:10.1111/j.1365-2036.2005.02691.x
24. Ataseven B, du Bois A, Reinthaller A, et al. Pre-operative serum albumin is associated with post-operative complication rate and overall survival in patients with epithelial ovarian cancer undergoing cytoreductive surgery. Gynecol Oncol. 2015;138:560–565. doi:10.1016/j.ygyno.2015.07.005
25. Chiang JM, Chang CJ, Jiang SF, et al. Pre-operative serum albumin level substantially predicts post-operative morbidity and mortality among patients with colorectal cancer who undergo elective colectomy. Eur J Cancer Care (Engl). 2017;26:e12403. doi:10.1111/ecc.12403
26. Ishizuka M, Nagata H, Takagi K, Iwasaki Y, Shibuya N, Kubota K. Clinical significance of the C-reactive protein to albumin ratio for survival after surgery for colorectal cancer. Ann Surg Oncol. 2016;23:900–907. doi:10.1245/s10434-015-4948-7
27. Jiang H, Li H, Li A, et al. Preoperative combined hemoglobin, albumin, lymphocyte and platelet levels predict survival in patients with locally advanced colorectal cancer. Oncotarget. 2016;7:72076–72083. doi:10.18632/oncotarget.12271
28. Matsumoto I, Tanaka M, Shirakawa S, et al. Postoperative serum albumin level is a marker of incomplete adjuvant chemotherapy in patients with pancreatic ductal adenocarcinom. Ann Surg Oncol. 2015;22:2408–2415. doi:10.1245/s10434-014-4280-7
29. Arrieta O, Michel Ortega RM, Villanueva-Rodriguez G, et al. Association of nutritional status and serum albumin levels with development of toxicity in patients with advanced non-small cell lung cancer treated with paclitaxel-cisplatin chemotherapy: a prospective study. BMC Cancer. 2010;10:50. doi:10.1186/1471-2407-10-663
30. Zhou T, Zhan J, Hong S, et al. Ratio of C-reactive protein/albumin is an inflammatory prognostic score for predicting overall survival of patients with small-cell lung cancer. Sci Rep. 2015;5:10481. doi:10.1038/srep10481
31. Oner F, Savas I, Numanoglu N. Immunoglobulins and complement components in patients with lung cancer. Tuberk Toraks. 2004;52:19–23.
32. Cohen MH, Makuch R, Johnston-Early A, et al. Laboratory parameters as an alternative to performance status in prognostic stratification of patients with small cell lung cancer. Cancer Treat Rep. 1981;65:187–195.
33. Lv G-Y, An L, Sun X-D, Hu Y-L, Sun D-W. Pretreatment albumin to globulin ratio can serve as a prognostic marker in human cancers: a meta-analysis. Clin Chim Acta. 2018;476:81–91. doi:10.1016/j.cca.2017.11.019
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.