")
Back to Journals » Infection and Drug Resistance » Volume 16
The Prognosis of Patients Tested Positive for Stenotrophomonas maltophilia from Different Sources
Authors Ma R , Chen Q , Huang Y, Cheng Z, Wang X, Xia L, Hu L
Received 3 May 2023
Accepted for publication 12 July 2023
Published 24 July 2023 Volume 2023:16 Pages 4779—4787
DOI https://doi.org/10.2147/IDR.S417151
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Ru Ma,1,* Qiang Chen,1,* Ying Huang,2 Zhongle Cheng,2 Xiaowei Wang,2 Lingling Xia,1 Lifen Hu1
1Department of Infectious Diseases, the First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China; 2Department of Clinical Laboratory, First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lifen Hu; Lingling Xia, Department of Infectious Diseases, the First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, 230031, People’s Republic of China, Tel +86-551-62922258 ; +86-551-62922383, Fax +86-551-62922281, Email [email protected]; [email protected]
Purpose: The purpose of this study was to analyze the prognosis of patients tested positive for Stenotrophomonas maltophilia (SMA) from different sources.
Methods: A retrospective study was conducted among 651 patients tested positive for SMA from January 2020 to October 2022 in the First Affiliated Hospital of Anhui Medical University. The patients were divided into seven groups by the source of SMA. Univariate and multivariate analyses were used to identify risk factors for mortality in patients tested positive for SMA from different sources.
Results: A total of 651 SMA isolates were collected from various sources, including sputum (348 isolates, 53%), bronchoalveolar lavage fluid (52, 8%), abdominal drainage fluid (76, 12%), wound secretion (66, 10%), blood (62, 10%), urine (41, 6%) and cerebrospinal fluid (6, 1%). Compared with other groups, the mortality of the patients in the bronchoalveolar lavage fluid culture group, blood culture group, and abdominal drainage fluid culture group was higher, at 40.38%, 32.26%, and 26.32%, respectively. Multivariate analysis showed that continuous renal replacement therapy was an independent risk factor for mortality in patients with SMA bloodstream infection (P=0.020, OR=6.86), and effective antimicrobial therapy after being positive for S. maltophilia isolates (P=0.002, OR=0.10) was negatively correlated with the death of patients with SMA bloodstream infection. Age ≥ 65 years (P= 0.043, OR=4.96), kidney disease (P=0.045, OR=4.62) and antifungal agent exposure (P=0.036, OR=5.13) were independent risk factors for mortality in patients with SMA intra-abdominal infection. Antifungal agent exposure (P=0.024, OR=0.51) and glycopeptide exposure (P=0.045, OR=0.53) were independent risk factors for mortality in patients in the sputum culture group.
Conclusion: SMA has a high rate of antimicrobial resistance and can cause multisite infection. Pulmonary infections, bloodstream infections and abdominal infections caused by SMA have high mortality, and timely standardized treatment can reduce mortality.
Keywords: Stenotrophomonas maltophilia, prognosis, antimicrobial susceptibility, treatment
Introduction
Stenotrophomonas maltophilia (SMA) is a nonfermentative, gram-negative, conditionally pathogenic bacterium that is widespread in sewage, tap water, soil, animals, plants and human bodies. It can be isolated from tracheal cannulas, various catheters, sputum aspirators, artificial ventilators and hand sanitizers of medical staff in the hospital.1 Currently, S. maltophilia has emerged as an important pathogen of nosocomial infection.2
According to the 2021 China Antimicrobial Surveillance Network(CHINET) report,3 S. maltophilia in China is the third most prevalent bacterial pathogen following Pseudomonas aeruginosa and Acinetobacter baumannii among nonfermentable bacteria, and the isolation rate of S. maltophilia in clinical specimens has been increasing yearly. It mainly induces respiratory tract infection but can also cause multisite infections, such as bloodstream infections, urinary tract infections, skin and soft tissue infections, bone and joint infections, biliary tract infections, ocular, endocarditis, meningitis and oral infections.4,5 S. maltophilia mainly causes infections in vulnerable groups, including patients in the intensive care unit (ICU), neonates, lung transplant recipients, patients with organ failure, patients with cystic fibrosis (CF), and patients with chronic obstructive pulmonary disease (COPD) or bronchiectasis.6–12 In addition, due to its complex resistance mechanisms, including the production of β-lactamase, biofilm and drug efflux pumps, reduction of the outer membrane permeability, and integron-mediated resistance genes, S. maltophilia shows inherent resistance to multi-antimicrobial agents, and the empiric treatment to S. maltophilia should be highlighted accordingly.13–17 Although S. maltophilia is reported to be increasingly resistant to TMP-SMX, it remains effective as a first-line antibiotic.18–20 However, it is controversial whether patients with positive S. maltophilia isolates require treatment, because it is difficult to clearly distinguish infection or colonization with positive S. maltophilia isolates. Colonization is a component of pathogen persistence and damage to susceptible hosts. It has been demonstrated that persisting multidrug-resistant gram-negative bacilli increase mortality and promote bloodstream infection progression in adult patients.21 Recently, there has been no systematic study about the treatment and prognosis of S. maltophilia infection from different sources.
The purpose of this study was to explore risk factors for mortality in patients positive for S. maltophilia isolates from different sources to control S. maltophilia infection.
Materials and Methods
Study Design
A retrospective study was conducted among 651 patients who were positive for S. maltophilia isolates from January 2020 to October 2022 in the First Affiliated Hospital of Anhui Medical University. To avoid duplication, only patients with the first episode of being colonized and infected S. maltophilia were included in this study. The patients’ clinical information was obtained from medical records. The enrolled patients were divided into a blood culture group, urine culture group, sputum culture group, bronchoalveolar lavage fluid culture group, abdominal drainage fluid culture group, wound secretion culture group and cerebrospinal fluid culture group according to the source of S. maltophilia specimens. The patients with positive S. maltophilia isolates from different sources were analyzed using both univariate and multivariate analyses to identify risk factors for mortality.
According to whether patients received antimicrobial therapy, the patients were divided into antimicrobial therapy groups and non-antimicrobial therapy groups. The following antibiotics were used for S. maltophilia infections: TMP-SMX, minocycline, tigecycline, levofloxacin, or cefoperazone-sulbactam, in accordance with the antimicrobial sensitivity testing.
Bacterial cultures were performed using blood agar plate, chocolate agar plate medium and MacConkey agar medium, for 24 hours at 37 °C. The isolates were confirmed using the VITEK GNI system (bioMerieux Vitek Inc, Hazelwood, MO, USA) and Clin-ToF-II.
Data Retrieval
The patients’ electronic medical records were reviewed. Demographic and clinical variables were obtained, including general information (sex, age, length of hospital stay, ICU admission), comorbidities (pulmonary disease, diabetes, kidney disease, hypoalbuminemia, malignancy, cardiovascular, cerebrovascular, rheumatic disease, liver dysfunction), invasive procedures (surgery, mechanical ventilator, tracheotomy, gastric tube insertion, urinary catheterization and central venous catheter), special treatments (corticosteroids, immunosuppressants, chemotherapy, CRRT), antimicrobial exposure (carbapenems, β-lactamase inhibitor, cephalosporins, fluoroquinolone, aminoglycoside, glycopeptides, antifungal agents), and antibiotic treatment data.
Ethics
This study was approved by the Biomedical Ethics Committee of Anhui Medical University (approval No. 20200865). Given that this was a retrospective study, the requirement for informed consent was waived by the ethics committee. Patient data were obtained from the medical record system and analyzed anonymously to protect patient privacy. We declare that this study is in accordance with the Helsinki Declaration and the relevant national laws and policies, and never disclose the information of all patients.
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing was determined using the microdilution method, according to the Clinical and Laboratory Standards Institute Performance Standards for Antimicrobial Susceptibility Testing, 33rd informational supplement.22 The following antimicrobial agents were tested against S. maltophilia strains: trimethoprim/sulfamethoxazole (TMP-SMX), minocycline (MIN), levofloxacin (LVX), cefoperazone/sulbactam, tigecycline (TGC). All antibiotics are from Sigma-Aldrich China, Inc. All experiments were repeated three times. The breakpoint of tigecycline for S. maltophilia was based on the standard of the US Food and Drug Administration. S. maltophilia 17666, Pseudomonas aeruginosa ATCC 27853, and Escherichia coli ATCC 25922 were used as controls for antimicrobial susceptibility testing.
Statistical Analysis
IBM SPSS Statistics V26.0 statistical software package was used for analysis. Categorical variables were expressed as the number of cases (n) or percentage (%). For the univariate analyses, chi-squared or Fisher’s exact tests were used for categorical variables. We considered a P value <0.05 to be statistically significant. A multivariate logistic regression was conducted based on the significant variables from a univariate analysis (P<0.05). The results were reported as odds ratios (ORs) with 95% confidence intervals (CIs) and P values. P values <0.05 were considered statistically significant.
Results
Distribution of S. maltophilia Isolates
A total of 651 S. maltophilia isolates were collected from various sources, including the respiratory tract [sputum (348 isolates, 53%), alveolar lavage fluid (52, 8%)], abdominal drainage fluid (76, 12%), wound secretions (66, 10%), blood (62, 10%), urine (41, 6%) and cerebrospinal fluid (6, 1%). S. maltophilia isolates in the blood culture group, bronchoalveolar lavage fluid culture group in the sputum culture group and cerebrospinal fluid culture group were mainly distributed in the ICU, accounting for 77.4% (48/62), 88% (46/52), 44% (153/348) and 67% (4/6), respectively.
Antimicrobial Sensitivity Testing and Therapy
The antimicrobial susceptibility rates of 651 S. maltophilia isolates to tigecycline, minocycline, cefoperazone-sulbactam, levofloxacin and TMP-SMX were 98.8%, 97.4%, 90.3%, 89.4% and 75.0%, respectively. Among patients who were treated with antimicrobial therapy, 20(46.51%), 38(77.55%), 141(62.95%), 23(54.76%), and 25(55.56%) patients were treated with TMP-SMX, minocycline, tigecycline, levofloxacin, or cefoperazone-sulbactam alone in the blood culture group, abdominal drainage fluid group, sputum culture group, alveolar lavage fluid group, and wound secretion group, respectively, whereas 23(53.49%), 11(22.45%), 83(37.05%), 19(45.24%), and 20(44.44%) patients were treated in combination therapy with cefoperazone-sulbactam. Patients in the urine culture group who received antimicrobial therapy included 16(59.26%) who were treated monotherapy with minocycline, levofloxacin, or cefoperazone-sulbactam, and 11(40.74%) who were treated in combination with levofloxacin.
Prognosis of Patients with Positive S. maltophilia Isolates
As shown in Figure 1, compared with other groups, the mortality of the patients in the bronchoalveolar lavage fluid culture group, blood culture group, and abdominal drainage fluid culture group were higher, which were 40.38%, 32.26%, and 26.32%, respectively.
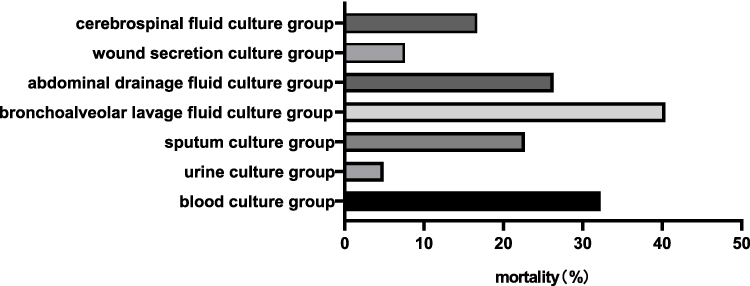 |
Figure 1 The mortality of patients with positive S. maltophilia isolates at different sites. |
As shown in Table 1, timely effective antimicrobial therapy after positive S. maltophilia isolates significantly reduced the mortality of patients with S. maltophilia bloodstream (P=0.001) or intra-abdominal infection (P=0.034) and was not correlated with mortality in the urine culture group, alveolar lavage fluid culture group, sputum culture group or wound secretion culture group.
 |
Table 1 Analysis of Mortality of Patients with Positive S. maltophilia Isolates Between Antimicrobial Therapy Group and Non-Antimicrobial Therapy Group at Different Sites [Cases, Rate (%)] |
Risk Factors for Mortality in Patients Positive for S. maltophilia Isolates
The univariate analysis showed that surgery and timely effective antimicrobial therapy after positive S. maltophilia isolates were negatively correlated with the mortality of the patients with S. maltophilia bloodstream infection (P<0.05), and the patients with S. maltophilia bloodstream infection in the death group received more CRRT (P<0.05) (Table 2). Age ≥65 years, kidney disease, carbapenem exposure and antifungal drug exposure were associated with mortality in the drainage fluid culture group (P<0.05), and antimicrobial therapy after positive S. maltophilia isolates can reduce mortality (P<0.05) (Table 3). ICU admission, kidney disease, urinary catheterization, central venous catheter, CRRT and antibiotic exposure (carbapenem, glycopeptide, antifungal agent) were associated with mortality in the sputum culture group (P<0.05) (Table 4). Age ≥65 and diabetes mellitus were associated with mortality in the alveolar lavage fluid culture group (P<0.05) (Table 5).
 |
Table 2 Analysis of Risk Factors for Mortality in 62 Patients with Positive S. maltophilia in the Blood Culture Group [Cases, Rate (%)] |
 |
Table 3 Analysis of Risk Factors for Mortality of Patients with Positive S. maltophilia in Abdominal Drainage Fluid Culture Group[Cases, Rate (%)] |
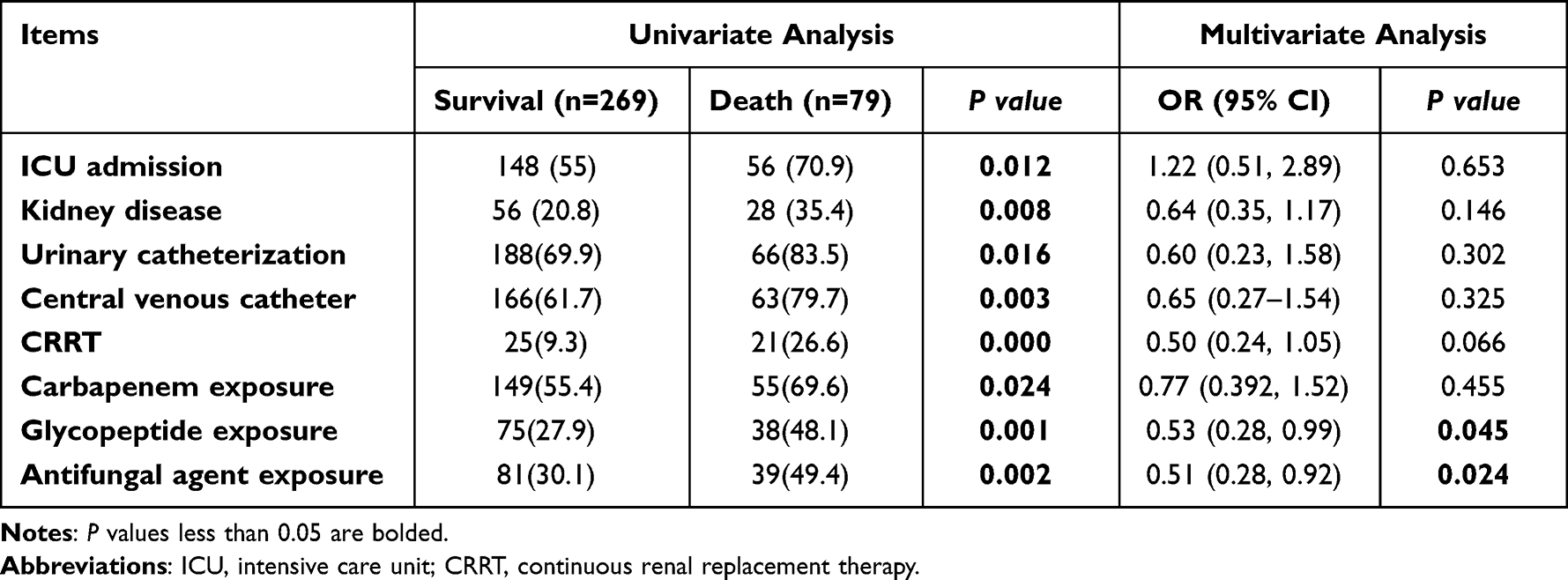 |
Table 4 Analysis of Risk Factors for Mortality of Patients with Positive S. maltophilia in Sputum Culture Group[Cases, Rate (%)] |
 |
Table 5 Analysis of Risk Factors for Death of Patients with Positive S. maltophilia in the Alveolar Lavage Fluid Culture Group[Cases, Rate (%)] |
The multivariate analysis suggested that CRRT was an independent risk factor for the mortality of patients with S. maltophilia bloodstream infection (P=0.020, OR=6.86), and timely effective antimicrobial therapy after being positive for S. maltophilia isolates was negatively correlated with the death of patients with S. maltophilia bloodstream infection (P=0.002, OR=0.10) (Table 2). Age ≥65 years (P=0.043, OR=4.960), kidney disease (P=0.045, OR=4.620) and antifungal agent exposure (P=0.036, OR=5.13) were independent risk factors for mortality in S. maltophilia patients with intra-abdominal infection (Table 3). Antifungal agent exposure (P=0.024, OR=0.51) and glycopeptide exposure (P=0.045, OR=0.53) were independent risk factors for the mortality of patients in the sputum culture group (Table 4).
Discussion
S. maltophilia is an emerging opportunistic pathogen in hospital and community settings, as well as the most common carbapenem-resistant gram-negative bacteria in bloodstream infections, and its morbidity is increasing worldwide.24 S. maltophilia is intrinsically resistant to most antibiotic treatments, which greatly limits its treatment.13 With the progress of the aging society, the threat of S. maltophilia to public health safety has become increasingly serious.
Similar to previous reports, S. maltophilia in this study was mainly isolated from the respiratory tract, accounting for 61% (400/651) of the total isolates, which might be related to its ability to form biofilms and colonize the respiratory tract of hospitalized patients.25,26 In this study, the patients in the bronchoalveolar lavage fluid culture group had significantly higher mortality than those in the sputum culture group (40.38% vs 22.7%), revealing that patients with positive S. maltophilia isolates from bronchoalveolar lavage should be considered for S. maltophilia infection, requiring antimicrobial therapy. According to reported studies, S. maltophilia bloodstream infection (BSI) is often preceded by colonization, and isolation of the organism from respiratory and/or gastrointestinal mucosa may signal a later infection.27 Clinicians should be vigilant for the possibility of future S. maltophilia infection.
Compared with the other groups, the mortality of patients in the bronchoalveolar lavage fluid culture group, blood culture group, and abdominal drainage fluid culture group were higher, at 40.38%, 32.26%, and 26.32%, respectively, suggesting that patients with S. maltophilia pulmonary infection, bloodstream infection and abdominal infection had a higher risk of death. The increasing use of antibiotics and invasive surgery during long hospital stays pose a high risk of screening S. maltophilia out later in the disease process in critically ill patients.28
In this study, more than 50% of the patients in the blood culture group, abdominal drainage fluid culture group, sputum culture group and alveolar lavage fluid culture group had carbapenem exposure, which has been repeatedly identified as a risk factor for S. maltophilia infection.11,29,30 Indiscriminate use of carbapenems may disrupt the normal flora and facilitate the dominant growth of S. maltophilia into pathogenic bacteria, thus causing nosocomial infection.13,31,32 Therefore, it is necessary to be alert to the possibility of S. maltophilia infection when using carbapenems in clinical practice. Our study also showed that carbapenem exposure was associated with mortality in patients in the abdominal drainage fluid group and sputum culture group (P<0.05), and previous studies have shown that dismal outcomes of S. maltophilia infection appeared to be more likely among patients with prior carbapenem exposure.33–35 Clinicians should pay attention to the rational use of carbapenems in the process of diagnosis and treatment. Our study also found that antifungal agent therapy was a risk factor for higher mortality among patients in the abdominal drainage fluid culture group, sputum culture group, and wound secretion culture group (P<0.05). Our study is similar to those reported recently in a retrospective study in China. In that study, antifungal agent therapy was associated with death among patients with S. maltophilia bloodstream infection (P=0.033).18
According to our study, CRRT was associated with higher mortality among patients in the blood culture group, wound secretion culture group, and sputum culture group (P<0.05). According to Jiang’s study, patients who require CRRT have low immunity and multiple organ failure (kidneys, livers, and hearts), resulting in further worsening of the condition, prolonged hospital stays, or even life-threatening effects caused by sepsis or septic shock.36 The long-term prognosis is poor. CRRT often involves central venous catheterization, which easily damages the body’s natural barrier, leading to internal and external communication that destroys the patient’s own barrier and circulatory pathway. As a result, immunity will be reduced, and the risk of bacterial colonization or infection will increase. A study by Yokota PK37 showed that central venous catheters are significant risk factors for bloodstream infection (BSI), which are directly associated with increased morbidity of S. maltophilia. It can be seen that shortening the hospital stay, reducing invasive operations and taking effective disinfection and isolation measures are important to avoid cross infection and prevent the epidemic of S. maltophilia infection. Timely removal of lesions is an important measure affecting the clinical efficacy and prognosis of S. maltophilia infection.38
Currently, it is controversial whether patients who are positive for S. maltophilia isolates require aggressive treatment because a clear distinction cannot be made between colonization and infection of S. maltophilia. According to the guidance document,23 in the present study, patients with mild infections were treated with TMP-SMX, minocycline, tigecycline, levofloxacin, or cefoperazone-sulbactam monotherapy, with TMP-SMX and cefoperazone-sulbactam being preferred treatments. The addition of a second therapeutic agent, such as minocycline, tigecycline, or levofloxacin, was considered if TMP-SMX or cefoperazone-sulbactam alone did not result in clinical improvement. Our study revealed that S. maltophilia isolates were more susceptible to tigecycline, minocycline, and cefoperazone-sulbactam than levofloxacin and TMP-SMX. The susceptibility to TMP-SMX, was 75% in our study, which is lower than that in previous studies.22 Our study found that antimicrobial therapy was significantly associated with lower mortality among patients with S. maltophilia bloodstream infections or abdominal infections (P<0.05). Therefore, when S. maltophilia is isolated from the patient’s blood or abdominal drainage fluid, corresponding antimicrobial therapy should be carried out according to antimicrobial susceptibility testing results. The choice of antimicrobial therapy for patients with positive S. maltophilia isolates from other sites should be based on the specific condition.
This study had some limitations. The sample size of our study was small, especially in the wound secretion group, urine culture group, and cerebrospinal fluid culture group. Besides, the design of our study was retrospective, and there are inherent limitations to this design.
Conclusion
S.maltophilia has a high rate of antimicrobial resistance and multiple susceptibility factors in the clinical setting and can cause infection at different sites. Clinicians need to be alert to the possibility of S. maltophilia infection. S. maltophilia pulmonary infection, bloodstream infections and abdominal infections have high morbidity and mortality rates, and timely standardized treatment can reduce morbidity and mortality. This study suggests that the clinical treatment of S. maltophilia needs further standardized management.
Acknowledgments
We thank all the authors and people who helped us to accomplish this work. This study was supported by the Program for Outstanding Young Talents in Universities (No. gxyq2021172) and Scientific Research Fund for Academic and Scientific Leaders in Anhui Province (No. 2018H194).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tong ZW, Li XF, Qiu J, et al. Stenotrophomonas maltophilia clinical distribution and drug resistance analysis (in Chinese). Chin J Microecol. 2012;24(8):741–743.
2. Lin Y, Wang B, Zhang N, et al. Metagenomic Analysis Identified Stenotrophomonas maltophilia Pneumonia in an Infant Suffering From Unexplained Very Severe Pneumonia. Front Pediatr. 2019;7:380.
3. Hu FP, Guo Y, Zhu DM, et al. CHINET surveillance of bacterial resistance across China: report of the results in 2021(in Chinese). Chin J of Infect Chemother. 2022;22(05):521–530.
4. Prates M, Fernandes F, Proenca F, et al. Oral infection caused by Stenotrophomonas maltophilia: a rare presentation of an emerging opportunistic pathogen. Case Rep Infect Dis. 2020;2020:6346120.
5. Inviati A, Pellegrino DM, Schifano D. Severe hepatic abscess: conservative treatment of multi-organ infection by Stenotrophomonas maltophilia. A case report. Ann Med Surg. 2018;34:62–65.
6. Brooke JS. Stenotrophomonas maltophilia: an emerging global opportunistic pathogen. Clin Microbiol Rev. 2012;25(1):2–41.
7. Chang YT, Lin CY, Chen YH, Hsueh PR. Update on infections caused by Stenotrophomonas maltophilia with particular attention to resistance mechanisms and therapeutic options. Front Microbiol. 2015;6:893.
8. Abda EM, Krysciak D, Krohn-Molt I, et al. Phenotypic heterogeneity affects Stenotrophomonas maltophilia K279a colony morphotypes and beta-Lactamase expression. Front Microbiol. 2015;6:1373.
9. Blanchard AC, Waters VJ. Opportunistic pathogens in cystic fibrosis: epidemiology and pathogenesis of lung infection. J Pediatric Infect Dis Soc. 2022;11(Supplement_2):S3–S12.
10. Olubunmi O, Adeolu O, Oreoluwa O, et al. Stenotrophomonas maltophilia infection in a patient with acute exacerbation of chronic obstructive pulmonary disease (COPD): a colonizer or true Infection? Am J Case Rep. 2020;21:e924577.
11. Nagaia C, Selene B, Felice V, et al. In vitro synergism of colistin and n-acetylcysteine against Stenotrophomonas maltophilia. Antibiotics. 2019;8(3):101.
12. Baidya A, Kodan P, Fazal F, et al. Stenotrophomonas maltophilia: more than just a colonizer! Indian j Critical Care Med. 2019;23(9):434–436.
13. Hu LF, Gao LP, Ye Y, et al. Susceptibility of Stenotrophomonas maltophilia clinical strains in China to antimicrobial combinations. J Chemother. 2014;26(5):282–286.
14. Abbott IJ, Slavin MA, Turnidge JD, et al. Stenotrophomonas maltophilia: emerging disease patterns and challenges for treatment. Expert Rev Anti Infect Ther. 2011;9(4):471–488.
15. Oyardi O, Savage PB, Erturan Z, et al. In vitro assessment of CSA-131 and CSA-131 poloxamer form for the treatment of Stenotrophomonas maltophilia infections in cystic fibrosis. J Antimicrob Chemother. 2021;76(2):443–450.
16. Li-Fen H, Xiao C, Ying Y, et al. Stenotrophomonas maltophilia resistance to trimethoprim/sulfamethoxazole mediated by acquisition of sul and dfrA genes in a plasmid-mediated class 1 integron. Int J Antimicrob Agents. 2011;37(3):230–234.
17. Cruz-Córdova A, Mancilla-Rojano J, Luna-Pineda VM, et al. Molecular epidemiology, antibiotic resistance, and virulence traits of Stenotrophomonas maltophilia strains associated with an outbreak in a Mexican tertiary care hospital. Front Cell Infect Microbiol. 2020;10:50.
18. Jian J, Xie Z, Chen L. Risk factors for mortality in hospitalized patients with Stenotrophomonas maltophilia bacteremia. Infect Drug Resist. 2022;15:3881–3886.
19. Hafiz TA, Aldawood E, Albloshi A, et al. Stenotrophomonas maltophilia Epidemiology, Resistance Characteristics, and Clinical Outcomes: understanding of the Recent Three Years’ Trends. Microorganisms. 2022;10(12):2506.
20. Sarzynski SH, Warner S, Sun J, et al. Trimethoprim-Sulfamethoxazole Versus Levofloxacin for Stenotrophomonas maltophilia Infections: a Retrospective Comparative Effectiveness Study of Electronic Health Records from 154 US Hospitals. Open Forum Infect Di. 2022;9(2):ofab644.
21. Mizusawa M, Konuma T, Kato S, et al. Clinical outcomes of persistent colonization with multidrug-resistant Gram-negative rods in adult patients undergoing single cord blood transplantation. Int J Hematol. 2020;111(6):858–868.
22. Clinical and laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. Twenty-Third Informational Supplement, M100-S33. Wayne, PA: Clinical and Laboratory Standards Institute; 2023.
23. Zhou H, Li GH, Zhuo C, et al. Diagnosis, treatment, prevention and control of Stenotrophomonas Maltophilia infection in China: expert Consensus. National Med J China. 2013;16:1203–1213.
24. Cai B, Tillotson G, Benjumea D, et al. The burden of bloodstream infections due to Stenotrophomonas Maltophilia in the United States: a Large, retrospective database study. Open Forum Infect Dis. 2020;7(5):a141.
25. Elpis H, Annalisa O, Pavel D, et al. Changing epidemiology of the respiratory bacteriology of patients with cystic fibrosis–data from the European cystic fibrosis society patient registry. J Cyst Fibros. 2020;19(3):376–383.
26. Guerci P, Bellut H, Mokhtari M, et al. Outcomes of Stenotrophomonas maltophilia hospital-acquired pneumonia in intensive care unit: a nationwide retrospective study. Crit Care. 2019;23(1):371.
27. Zöllner SK, Kampmeier S, Froböse NJ, et al. Stenotrophomonas maltophilia Infections in Pediatric Patients - Experience at a European Center for Pediatric Hematology and Oncology. Front Oncol. 2021;11:752037.
28. Márió G, Edit U. Epidemiological trends and resistance associated with Stenotrophomonas maltophilia bacteremia: a 10-year retrospective cohort study in a tertiary-care hospital in Hungary. Diseases. 2019;7(2):41.
29. Shi L, Wu AH, Cao L, et al. Risk factors for healthcare-associated infection of Stenotrophomonas maltophilia in intensive care unit(in Chinese). Chin J Infect Control. 2019;18(05):403–409.
30. Wang YL, Scipione MR, Dubrovskaya Y, et al. Monotherapy with fluoroquinolone or trimethoprim-sulfamethoxazole for treatment of Stenotrophomonas maltophilia infections. Antimicrob Agents Chemother. 2014;58(1):176–182.
31. Kanchanasuwan S, Rongmuang J, Siripaitoon P, et al. Clinical characteristics, outcomes, and risk factors for mortality in patients with Stenotrophomonas maltophilia bacteremia. J Clin Med. 2022;11(11):65.
32. Yue C, Shen W, Hu L, et al. Effects of tigecycline combined with azithromycin against biofilms of multidrug-resistant Stenotrophomonas maltophilia isolates from a patient in China. Infect Drug Resist. 2021;14:775–786.
33. Bilen NM, Sahbudak BZ, Guner OG, et al. Risk Factors for Infection and Mortality Associated With Stenotrophomonas maltophilia Bloodstream Infections in Children; Comparison With Pseudomonas aeruginosa Bloodstream Infections. Pediatr Infect Dis J. 2023;42(5):374–380.
34. Gayretli AZ, Tanir G, Bayhan GI, et al. Risk Factors of Stenotrophomonas maltophilia Blood Stream Infections: comparison With Other Gram-Negative Blood Stream Infections in Children. Pediatr Infect Dis J. 2020;39(12):e406–e409.
35. Furuichi M, Ito K, Miyairi I. Characteristics of Stenotrophomonas maltophilia bacteremia in children. Pediatr Int. 2016;58(2):113–118.
36. Stewardson AJ, Marimuthu K, Sengupta S, et al. Effect of carbapenem resistance on outcomes of bloodstream infection caused by Enterobacteriaceae in low-income and middle-income countries (PANORAMA): a multinational prospective cohort study. Lancet Infect Dis. 2019;19(6):601–610.
37. Yokota PK, Marra AR, Belucci TR, et al. Outcomes and Predictive Factors Associated with Adequacy of Antimicrobial Therapy in Patients with Central Line-Associated Bloodstream Infection. Front Public Health. 2016;4:284.
38. Adegoke AA, Stenström TA, Okoh AI. Stenotrophomonas maltophilia as an Emerging Ubiquitous Pathogen: looking Beyond Contemporary Antibiotic Therapy. Front Microbiol. 2017;8:2276.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.