")
Back to Journals » International Journal of General Medicine » Volume 16
The Prevalence of Symptomatic Dry Eye Disease Among Coal Workers in Huainan Region of China
Received 18 November 2022
Accepted for publication 5 January 2023
Published 19 January 2023 Volume 2023:16 Pages 203—209
DOI https://doi.org/10.2147/IJGM.S396670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Cui Qiu,1– 3 Yan Fang1– 3
1First Affiliated Hospital of Anhui University of Science and Technology (Huainan First People’s Hospital) Tianjia ‘an District, Huainan City, People’s Republic of China; 2Anhui University of Science and Technology Medical College Tianjia ‘an District, Huainan City, People’s Republic of China; 3Institute of Ophthalmology, Anhui University of Science and Technology Tianjia ‘an District, Huainan City, People’s Republic of China
Correspondence: Yan Fang, Tel +8613721126292, Fax +8605543320706, Email [email protected]
Purpose: To investigate the prevalence and influencing factors of symptomatic dry eye disease (DED) in Chinese coal workers.
Methods: The prevalence of symptomatic DED in coal workers was investigated by using the questionnaire of Ocular Surface Disease Index (OSDI) and the influencing factors were explored.
Results: The prevalence of symptomatic DED was 50.7% in coal workers. Of the influencing factors of symptomatic DED, the level of dust exposure had an odds ratio (OR) of 1.26, the time of dust exposure had an OR of 1.02, and the age had an OR of 1.03.
Conclusion: There was a high morbidity of symptomatic DED among coal workers and the level and the time of dust exposure and the age of coal workers had important effects.
Keywords: symptomatic DED, prevalence, influencing factors, coal workers
Introduction
DED has become an important eye health issue of public concern. It is a multifactorial disease of the ocular surface, in which inflammation and injury of the ocular surface play an etiological role, and it is mainly characterized by discomfort symptoms such as blurred vision and eye pain, affecting the quality of life related to vision and physical and mental health, reducing work productivity, and causing economic losses to individuals and the society as well.1–4 It has been shown that DED is about 70% attributable to environmental factors and particulate matter(PM)2.5 and PM10 in the air contribute to the incidence of DED, and that the risk of DED is relatively high in construction workers exposed to a high-dust working environment.5–7 Coal, the main pillar of China’s energy sources, is mainly mined in deep underground.8 Coal workers work in a high-dust environment that the dust concentration at the working face can be as high as 3000 mg/m3,while respiratory dust has shown to induce pneumoconiosis.9,10 Meanwhile, goggles are not commonly used in underground mines, and the miner’s eyes are directly exposed to high concentrations of dust.11 Dust in large amounts is often found in the eyelid margin of coal workers during eye examinations in the ophthalmology clinics. There have been few reports of whether dust can cause ocular surface damage and DED in coal workers.12,13 Therefore, we conducted an epidemiological survey of DED in coal workers and discussed related risk factors.
Methods
Study Population
This was a cross-sectional survey, which was in line with the ethical principles of the Declaration of Helsinki. The study protocol was reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Anhui University of Science and Technology (Approval No. KJ2020A0339), and the questionnaire can be completed only after the informed consent was obtained from the respondent. In March, 2022, three coal mines of different depths in Huainan region of China were selected and surveys were carried out using DED questionnaire in coal workers working on the ground, those performing auxiliary underground work and those mining coal, respectively. Because underground coal workers are mostly males, the selected respondents were all males.
Groups
There are three groups with different levels of dust exposure:13
A group: Ground workers who were barely exposed to dust.
B group: Workers who did auxiliary underground work and were exposed to small amounts of dust.
C group: Coal miners and digger who were heavily exposed to rock and coal dust.
The depths of the three mines are −650 m, −750 m, −850 m and deeper, respectively.
Surveys Conducted Using the Internationally Recognized OSDI Questionnaire
OSDI questionnaire measures the presence and severity of symptomatic DED, including 12 questions about the frequency of eye symptoms, vision-related functions, and environmentally induced symptoms in the past week, with 0 for no and 4 for very frequent. Total OSDI score equals to [(score of all questions answered) x 100]/[(total number of questions answered) x 4] and ranges from 0–100.14 Total OSDI score ≥ 13 suggests the presence of symptomatic DED. The higher the score, the more severe the symptoms; total OSDI score ≥ 33 suggests severe symptomatic DED.15
The questionnaire was administered online via the website http://www.wjx.cn. After the coal workers had filled out and submitted the questionnaires, the survey results can be viewed on the website.
Primary Observations
The prevalence of symptomatic DED, the prevalence of severe DED, and the associated risk factors among coal workers: level of dust exposure, time of dust exposure, age and mine depth.
Statistical Methods
Statistical analysis was performed using SPSS 25.0 software. The reliability of the collected questionnaires was analyzed. Measurement data of normal distribution are expressed as mean ± standard deviation, and group differences were analyzed by t-test and variance analysis. Measurement data of skewed distribution are expressed as median and 25% and 75% quartiles, and group differences were analyzed by nonparametric rank sum test. Categorical data were analyzed by Chi-square test and multivariate Logistic regression. P<0.05 was considered statistically significant.
Results
Reliability Analysis
3749 respondents were surveyed and 3683 questionnaires received, with a recovery rate of 98.2%. We used the Cronbach coefficient method to analyse the reliability of the OSDI questionnaire. Reliability analysis of all questionnaires showed α=0.939, and the results were reliable.
Overall Population Characteristics (Table 1)
1) In the population of coal workers, the prevalence of symptomatic DED was 50.7% (n=1868/3683) and that of severe symptomatic DED was 22.8% (n= 883/3683).
 |
Table 1 Overall Characteristics of Coal Workers |
2) The 3683 coal workers were 41.87±7.64 years of age (95% CI 41.63–42.1), and 16.69±7.61 working years (95% CI 16.65–16.9), with a total OSDI score of 14.58 (4.17, 30.21). The prevalence of symptomatic DED was 50.7%, and that of severe symptomatic DED was 22.8%. Coal workers working underground accounted for 84.5%, and the prevalence of symptomatic DED was 51.4%, and that of severe symptomatic DED was 24.1% in them.
Effect of the Mine Depth on the Prevalence of Symptomatic DED (Table 2)
There was no statistical difference in the prevalence of symptomatic and severe symptomatic DED among underground workers working at different depths.
 |
Table 2 Dry Eye Status of Coal Workers Working at Different Depths |
Effect of the Level of Dust Exposure on the Prevalence of Symptomatic DED (Table 3)
1) The total OSDI score increased with increasing levels of dust exposure, and the difference was statistically significant (H=48.81, P<0.001). Group comparisons showed no statistical difference in the total OSDI score between the mild dust exposure group and the moderate dust exposure group (H=−97.4, P=0.173) (Figure 1).
 |
Table 3 Comparison of Coal Workers with Different Levels of Dust Exposure |
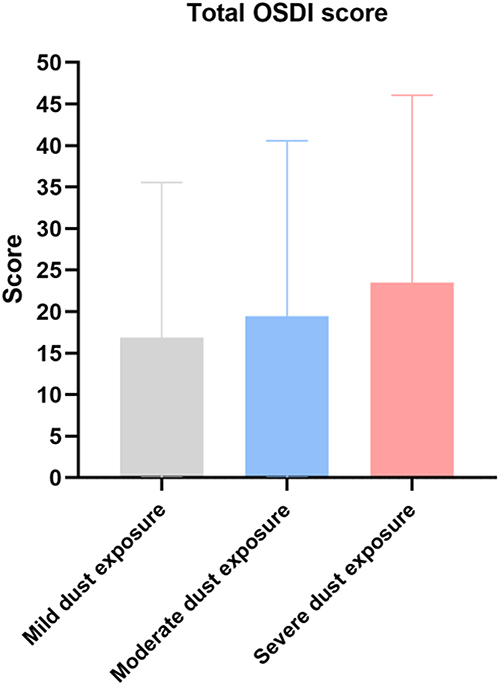 |
Figure 1 OSDI score increases with increasing levels of dust exposure. |
2) The prevalence of DED was significantly higher in the severe dust exposure group than in the mild and the moderate dust exposure groups (56.5% vs 47.1% vs 47.0%, χ²=31.26, P<0.001). There was no statistical difference in the prevalence of symptomatic DED between the mild and the moderate dust exposure groups (χ²=0.001, P=0.971).
3) The prevalence of severe symptomatic DED increased with increasing level of dust exposure. The prevalence of severe symptomatic DED was higher in the severe dust exposure group than in the moderate dust exposure group (27.5% v 21.1%), and higher in the moderate dust exposure group than in the mild dust exposure group (21.1% vs 15.6%). The difference was statistically significant (χ²= 37.67, P<0.001), and group comparisons also indicated a statistical difference (P<0.05) (Figure 2).
 |
Figure 2 The prevalence of severe symptomatic DED increases with increasing levels of dust exposure. |
4) There were significant differences in age and working years between the severe dust exposure group and the other two groups (P<0.001). The age difference was statistically significant (P<0.001), but the difference in working years was not between the mild and the moderate dust exposure groups (P=0.53).
Multivariate Logistic Regression Analysis of Age, Working Years and Level of Dust Exposure (Table 4)
The results showed that the level of dust exposure exhibited statistically significant effect on the prevalence of symptomatic DED (OR=1.26, 95% CI 1.14–1.3%, P<0.001), so did the time of dust exposure, ie, working years (OR=1.02, 95% CI 1.01–1.0%, P<0.001) and age (OR=1.03, 95% CI 1.01–1.0%, P<0.001).
 |
Table 4 Effect of Age, Working Years and Level of Dust Exposure on Symptomatic DED |
Discussion
DED causes visual impairment, such as blurred vision, glare and decreased visual contrast sensitivity, not only affecting the quality of life associated with vision, but also threatening life safety.2 Hence, it is undoubtedly a major safety risk for coal workers who perform heavy physical labor in a harsh environment with low visibility.16,17 DED reduces work productivity, but increases medical expenses, thus bringing financial burdens to individuals and the society as well.18,19 Surveys showed that the costs of DED treatment per patient per year ranged from US$270 to 1100 in Europe over 2003–2004 and the losses due to DED were worth US$11,302 per patient on average due to DED caused work productivity losses in the United States in 2008.20 Huainan, an energy city in north-central Anhui Province, China, has an abundance of coal workers; however, the eye health status of coal workers in this city is yet to be investigated.
This study was a cross-sectional survey of DED status of male coal workers by professional ophthalmologists using the internationally recognized OSDI questionnaire and the aim was to investigate the prevalence and influencing factors of symptomatic DED in male coal workers. This study found that about one out of two male coal workers had symptomatic DED, and that age and the level and time of dust exposure had an impact on the incidence of symptomatic DED in coal workers. Specifically, the older the age, the longer the time of dust exposure, the higher the level of dust exposure, the higher the prevalence of symptomatic DED, and the more severe the symptoms. At the same time, it was found that the depth of mine had little effect on the incidence of symptomatic DED.
The dust concentration ranges from 1750–2680 mg/m3 in the mining area of a deep mine, and the dust particles are 0.25–16 μm in size. In the non-mining area, the dust concentration is lower than 660 mg/m3, and the dust particles below 10 μm account for about 60%.9 Despite the measures such as ventilation, slurry and water sprays used to reduce the dust concentration of the working face, the dust concentration is still far higher than the total dust concentration specified in the Coal Mine Safety Law of China.6 PM2.5, PM10 and heavy metals in the dust have been proved to induce pneumoconiosis, while PM2.5 and PM10 in the air pollutants to cause symptomatic DED.21 Therefore, we speculate that the high concentrations of dust in the mining face may lead to the incidence of symptomatic DED in male coal workers, and symptomatic DED worsens with the dust concentration increasing. Our survey confirmed that the total OSDI score increased with the increasing level of dust exposure. The prevalence of symptomatic DED was the highest in the severe dust exposure group (56.7%). The severity of symptomatic DED increases with the increasing level of dust exposure. A 0.26-fold increase in the risk of symptomatic DED was observed by an elevated level of dust exposure when other influencing factors remained unchanged.
The dust exposure time was measured by the working years in this study, namely, the longer the working years, the longer the dust exposure time. Pneumoconiosis caused by long-term dust exposure is generally developed among miners who have worked for more than 25 years.22 There has not been relevant literature on the exact time of coal dust exposure that causes symptomatic DED. Our survey found that the longer the exposure to coal dust, the higher the risk of symptomatic DED in coal workers, and the odds ratio was 1.02 (1.01–1.04), that is, the risk of symptomatic DED increased by 0.02-fold for every working year. The longer you work, the older you may be. Age is an important factor in the incidence of symptomatic DED, and people >60 years of age are susceptible to symptomatic DED. In this study, the age of the population was 41.87±7.64 years, and the majority were young and middle-aged ones.23 However, the incidence of symptomatic DED in coal workers was still affected by the age, and the odds ratio was 1.03 (1.01–1.04), which is consistent with the linear correlation between the prevalence of DED and the age as reported previously.5
Interestingly, our survey found that the mine depth was not associated with the incidence of symptomatic DED, and that the incidence rate of symptomatic DED was comparable between coal workers who work on ground with mild dust exposure and underground coal workers with moderate dust exposure. As the mining depth increases, the surrounding rock temperature and the ground temperature of the working face increase in a nonlinear manner. When the ground temperature at 0 m is 16°C, it is about 26°C at −500 m and over 38°C at −1000 where the relative humidity is 96–100%.24 The relative humidity in the environment is negatively correlated with the incidence of symptomatic DED. The higher the humidity, the less the water loss in the tear film.25 The higher the ocular surface temperature in the high-temperature working environment, the faster the lipid flow of Meibomian glands, thus preventing obstruction of the glands, increasing the thickness of the lipid layer in the pre-corneal tear film and the stability of the tear film, and reducing the prevalence of symptomatic DED.26 This may be an important reason why the prevalence of symptomatic DED is not higher in coal workers with moderate dust exposure in deep mines than in those working on ground.
The limitation of the study is that the study is a questionnaire-based cross-sectional survey without carrying out physical examination of DED, which bears certain subjectivity. Further studies are to be conducted on the relationship between symptomatic DED and physical signs and possible factors that may influence the incidence of DED in coal workers, so as to make the survey results more accurate and credible.
Conclusion
A lack of eye protection awareness and long-term exposure to a high-dust working environment result in a high prevalence of symptomatic DED in coal workers. The incidence of symptomatic DED is associated with the level and time of dust exposure and the age of coal workers, but not with the depth of the mine. As DED not only reduces the quality of life of coal workers, but also affects production safety, thus causing huge economic losses to individuals and the enterprises, coal workers should enhance their awareness of personal protection, and enterprises should consider symptomatic DED as a public health issue and even an occupational disease and pay special attention to the eye health of coal workers.
Acknowledgments
The authors would like to thank the Occupational Disease Prevention and Control Institute of Huaihe Energy Group for supporting the implementation of this survey.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
2. Morthen MK, Magno MS, Utheim TP, et al. The vision-related burden of dry eye. Ocul Surf. 2022;23:207–215. doi:10.1016/j.jtos.2021.10.007
3. Vehof J, Kozareva D, Hysi PG, et al. Relationship between dry eye symptoms and pain sensitivity. JAMA Ophthalmol. 2013;131(10):1304–1308. doi:10.1001/jamaophthalmol.2013.4399
4. Greco G, Pistilli M, Asbell PA, et al. Association of severity of dry eye disease with work productivity and activity impairment in the dry eye assessment and management study. Ophthalmology. 2021;128(6):850–856. doi:10.1016/j.ophtha.2020.10.015
5. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II epidemiology report. Ocul Surf. 2017;15(3):334–365. doi:10.1016/j.jtos.2017.05.003
6. Kim Y, Choi Y-H, Kim MK, et al. Different adverse effects of air pollutants on dry eye disease: ozone, PM2.5, and PM10. Environ Pollut. 2020;265(Pt B):115039. doi:10.1016/j.envpol.2020.115039
7. Bazeer S, Jansonius N, Snieder H, et al. The relationship between occupation and dry eye. Ocul Surf. 2019;17(3):484–490. doi:10.1016/j.jtos.2019.04.004
8. Wang YX, Fu G, Lyu Q, et al. Reform and development of coal mine safety in China: an analysis from government supervision, technical equipment, and miner education. Resour Policy. 2022;77:102777. doi:10.1016/j.resourpol.2022.102777
9. Zhang LC, Zhou G, Ma Y, et al. Numerical analysis on spatial distribution for concentration and particle size of particulate pollutants in dust environment at fully mechanized coal mining face. Powd Technol. 2021;383:143–158. doi:10.1016/j.powtec.2021.01.039
10. Balkhyour MA, Ahmad I, Rehan M. Assessment of personal protective equipment use and occupational exposures in small industries in Jeddah: health implications for workers. Saudi J Biol Sci. 2019;26(4):653–659. doi:10.1016/j.sjbs.2018.06.011
11. Dain SJ, Hoskin AK, Winder C, et al. Assessment of fogging resistance of anti-fog personal eye protection. Ophthalmic Physiol Opt. 1999;19(4):357–361. doi:10.1046/j.1475-1313.1999.00418.x
12. Chen H, Feng Q, Long RY, et al. Focusing on coal miners’ occupational disease issues: a comparative analysis between China and the United States. Saf Sci. 2013;51:217–222. doi:10.1016/j.ssci.2012.06.025
13. Tonga RP, Cheng MZ, Yang XY, et al. Exposure levels and health damage assessment of dust in a coal mine of Shanxi Province, China. Process Saf Environ Prot. 2019;128:184–192. doi:10.1016/j.psep.2019.05.022
14. Schiffman RM, Christianson MD, Jacobsen G, et al. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. 2000;118(5):615–621. doi:10.1001/archopht.118.5.615
15. Sullivan DA, Rocha EM, Aragona P, et al. TFOS DEWS II sex, gender, and hormones report. Ocul Surf. 2017;15(3):284–333. doi:10.1016/j.jtos.2017.04.001
16. Gao JQ, Li YL, Wu X. Revision and validation of the Connor-Davidson resilience scale of coal miners in China. Int J Ind Ergon. 2021;85:103191. doi:10.1016/j.ergon.2021.103191
17. Cai P, Nie W, Chen DW, et al. Effect of air flowrate on pollutant dispersion pattern of coal dust particles at fully mechanized mining face based on numerical simulation. Fuel. 2019;239:623–635. doi:10.1016/j.fuel.2018.11.030
18. Binyousef FH, Alruwaili SA, Altammami AF, et al. Impact of Dry Eye Disease on Work Productivity Among Saudi Workers in Saudi Arabia. Clin Ophthalmol. 2021;15:2675–2681. doi:10.2147/OPTH.S313158
19. Dana R, Meunier J, Markowitz JT, et al. Patient-reported burden of dry eye disease in the United States: results of an online cross-sectional survey. Am J Ophthalmol. 2020;216:7–17. doi:10.1016/j.ajo.2020.03.044
20. McDonald M, Patel DA, Keith MS, et al. Economic and humanistic burden of dry eye disease in Europe, north america, and Asia: a systematic literature review. Ocul Surf. 2016;14(2):144–167. doi:10.1016/j.jtos.2015.11.002
21. Moreno T, Trechera P, Querol X, et al. Trace element fractionation between PM10 and PM2.5 in coal mine dust: implications for occupational respiratory health. Int J Coal Geol. 2019;203:52–59. doi:10.1016/j.coal.2019.01.006
22. Harris DA, Willis J, Tomann M. A new era of coal workers’ pneumoconiosis: decades in mines may not be required. Lancet. 2020;395(10234):e82. doi:10.1016/S0140-6736(20)30731-5
23. Tellefsen NS, Badian RA, Utheim TP, et al. Sex and age differences in symptoms and signs of dry eye disease in a Norwegian cohort of patients. Ocul Surf. 2021;19:68–73. doi:10.1016/j.jtos.2020.11.009
24. Wang KP, Li QM, Wang J, et al. Thermodynamic characteristics of deep space: hot hazard control case study in 1010-m-deep mine. Case Stud Therm Eng. 2021;28:101656. doi:10.1016/j.csite.2021.101656
25. Mo Z, Fu Q, Lyu D, et al. Impacts of air pollution on dry eye disease among residents in Hangzhou, China: a case-crossover study. Environ Pollut. 2019;246:183–189. doi:10.1016/j.envpol.2018.11.109
26. Huang SZ, Jiao XW, Lu DL, et al. Light cycle phase advance as a model for jet lag reprograms the circadian rhythms of murine extraorbital lacrimal glands. Ocul Surf. 2021;20:95–114. doi:10.1016/j.jtos.2021.02.001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.