")
Back to Journals » International Journal of General Medicine » Volume 17
The Prevalence and Associated Factors of Occupational Stress in Healthcare Providers in Saudi Arabia
Authors Almutairi AF , Hamdan NA, Altheyabi S, Alsaeed EA, Alammari FS, BaniMustafa A
Received 5 November 2023
Accepted for publication 31 January 2024
Published 5 March 2024 Volume 2024:17 Pages 809—816
DOI https://doi.org/10.2147/IJGM.S446410
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mihajlo Jakovljevic
Adel F Almutairi,1 Nasser Ali Hamdan,2 Saud Altheyabi,1 Emtinan Abdulrahman Alsaeed,3 Faisal S Alammari,4 Ala’a BaniMustafa1
1King Abdullah International Medical Research Center, King Saud bin Abdulaziz University for Health Sciences, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia; 2Dental Intern, King Khalid University, Abha, Saudi Arabia; 3College of Dentistry, Majmaah University, Al Majma’ah, Saudi Arabia; 4College of Dentistry, King Abdullah International Medical Research Center, King Saud bin Abdulaziz University for Health Sciences, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia
Correspondence: Ala’a BaniMustafa, Tel +966596460219, Email [email protected]
Background: Occupational stress is a negative physical and emotional response to job requirements, which might be caused by various factors that can harm the emotional and physical well-being of the employee. We aimed to investigate the factors and conditions associated with occupational stress.
Study Design: The study was cross-sectional, conducted with the Perceived Stress Scale ten item version.
Results: The majority of the participants reported moderate stress 223 (71%) and a small proportion (n=38, 12.2%) a high stress level. Several factors associated with higher risk of stress level for example being single were associated with higher risk of stress level in 135 (74.6%), moderate and high stress level was also reported in the group without enough income, 96 (75%) and 20 (15.6%), respectively.
Conclusion: A group of sociodemographic factors were consistently associated with occupational stress, including gender, income, comorbidity and marital status. However, some factors remained complex and multifaceted.
Recommendation: It is important to focus on reducing stress levels for all employees, regardless of their work experience or income. To prevent losing control of the healthcare worker’s stress and to prevent an escalation to anxiety or depression, stress-management programs are necessary, specifically for those who are experiencing high stress levels.
Keywords: occupational stress, healthcare provider, mental health, emotional response
Background
Mental health and well-being are as important as physical health, and one of the main reasons is that it has an impact on people’s work life. This is matching with WHO definition of health: “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”1 Occupational stress is a negative physical and emotional response when the requirements of the job do not meet the responsibilities, resources, and the work demands.2 Stress is a reaction to stimuli and can have either a positive or negative response.3,4
Nowadays, expectations of employees are more than ever, as they are expected to do more intense work, be more successful, and deliver more, which can affect their quality of life. Occupational stress may be caused by various factors that can harm the emotional and physical well-being by influencing their efficiency and impact negatively on their performance.5 Though some can withstand the stress, other professions are inherently more stressful, specifically professions that require rapid decision-making skills and serious consequences.6 A multi-country study concluded that factors such as time pressure, poor working conditions, deadlines, heavy workload, prolonged working hours, and different beliefs are among the top workplace stress factors.7 The sources of stress can actively accumulate leading to behavioral, psychological, and biological reactions.7
Compared with other occupations, healthcare workers are susceptible to significant psychological stress.8 Healthcare providers are more likely to experience stress due to their work conditions with more intense and stressful situations in caring for those in need. Some of the situations include human suffering and death, fears for personal safety, high workload (particularly for those treating infected patients) and limited support may contribute to fatigue, burnout, and stress.9 A study conducted in Riyadh with healthcare workers showed that 15.8% suffered from high-stress levels and 77.2% from moderate stress levels.10
The history of humanity has been marked by the impact of many fearsome pandemics of infectious diseases such as SARS, MERS, and COVID-19, resulting in more stress in the HCW. Additionally, studies from previous epidemics indicated that the sudden onset of an unknown disease with a high mortality rate affect the mental health of HCWs.11–15 HCW may also experience psychological effects because of the working environment. This includes lacking personal protective equipment, reorganizing units and services with the addition of new teams, fear of contracting an infection or spreading it to loved ones or patients and having to make morally challenging decisions, feeling helpless, longer working hours and others.8,16–20
A cross-sectional study conducted in Egypt and Saudi Arabia with HCWs showed that 69% of the participants were depressed (39.4% mild to moderate and 29.6% severe to very severe).21 A person with depression typically presents with a depressed mood, decreased interest or pleasure, reduced energy, low self-worth, sleep deprivation or decreased appetite, and lack of concentration.22 Depression can cause a significant and long-lasting deficit in a person’s ability to handle daily tasks, and at its worst, it can even result in suicide. The WHO (2012) estimates that suicide claims over 1 million lives each year, or 3000 people per day. The effects of depression on doctors’ health and wellbeing may extend to how it affects their patients. Physicians who are depressed struggle to complete professional and personal obligations take more sick days and are more likely to exhibit subpar performance at work.23–25 According to a study of pediatric residents, depressive people are six times more likely to make prescription mistakes than those who are not depressed, which poses a risk to patient safety.23
Research indicated that there was a bidirectional association between severe medical errors and self-perceived exhaustion, depressive symptoms, and a decline in quality of life. The study aimed to investigate the prevalence of, and factors associated with, occupational stress in Saudi healthcare providers. The significance of this study is based on the fact that people have been affected by a number of pandemics and epidemics in the last two years, as well as the associated precautionary measures, the burden of the situation, media exposure and complications with infected patients. To our knowledge, limited literature is available related to the prevalence of occupational stress and the associating factors in HCWs in Riyadh. The findings of this study are likely to reinforce the necessity for mental health programs tailored to HCWs. Such initiatives will be especially beneficial in preventing and fighting work stress, which will result in better healthcare.
Methodology
A cross-sectional study, using a self-administered questionnaire, was conducted with healthcare workers to investigate the prevalence of, and factors associated with occupational stress in Saudi healthcare providers.
Study Population and Sampling Technique
A convenience sampling technique was used to recruit the participants in the study. Targeting Saudi healthcare workers, a sample of 311 participants was achieved. The data was collected using a web-based electronic survey using Google Forms. The questionnaire was developed after referring to a pre-validated questionnaire and distributed through social media platforms such as Twitter, Telegram, and WhatsApp, though providing a link to the questioner, which was accessible for three months, from July 2022 to September 2022. The English language was used in both the text messages and the questionnaire. The participants were informed about the aim of the study, as well as the voluntary nature and anonymity of participation in the questionnaire survey.
The sample size was determined using a sample size calculation formula and based on the following parameters: 16% of healthcare practitioners suffer from high levels of stress (as reported in prior research in Saudi Arabia), a 95% confidence interval, and a 5% margin of error. However, the research team added 50% more to compensate for incomplete surveys or non-response, resulting in a required sample of 311.
Data Collection and Study Instrument
The data was collected using standardized validated tools, following an extensive literature review. The tool consisted of two sections. The first focused on sociodemographic data (gender, age, occupation, marital status and having a child, years of working, working with COVID-19 patients, being COVID-19 positive, any comorbidity, and the BMI index). The second section contained the Perceived Stress Scale, which is a pre-validated self-report tool used to measure perceived stress over the previous 4 weeks.26 We used the short version with a 10-item questionnaire (four positively related and 6 negatively related). Each item has a 5-point Likert scale ranging from 0 (never) to 4 (very often). The score range is from 0 to 40. Higher scores indicate higher levels of perceived stress; all scores were categorized into three levels: low, moderate and high. Scores of (0–13) was classified as low stress level, Scores of (14–26) classified as moderate stress level and Scores of (27–40) classified as high stress level. In terms of job satisfaction, one independent question was used to evaluate the participant satisfaction with their job using 5-point Likert scale then all values were converted to yes and no answers. Additionally, demographic characteristics were all categorical variables except for age of participants it was continuous variable.
Data Management and Analysis Plan
Data were analyzed using the SPSS version 29. The sample characteristics were analyzed using descriptive statistics, including mean, standard deviation, frequency, and percentage. The mean variation in the outcome scores, depending on the sample characteristics, was evaluated using bivariate analysis. To investigate the association between the demographic characteristics and potential relationships with stress levels, t-test was used to explore the relationship between age and different categories of stress, and chi-square to explain the correlation and significant differences between the categorical variables. The significant level is considered at p-value <0.05.
Study Result
Participant Demographic Information
The sample was realized as 311, 52.9% male. The mean ±SD of age was 31.5 ± 8.93 years. The majority (n=181, 58.0%) were single. The participants had different occupations, the majority were physicians (n=87, 27.9%), 63 were residents (20.2%), and 46 (14.7%) were dentists. Most of participants (n=194, 62.2%) had 5 years of experience, and 31 (9.9%) had 10 to 20 years of working experience. The majority (n=234, 75.0%) worked with COVID-19 patients, and 191(61.2%) were previously COVID-19 positive. A small proportion (n=40, 12.8%) had comorbidities, and 16 (5.2%) were obese and the same proportion, underweight according to the BMI index. Just more than half were satisfied with their work (n=165, 52.9%). The participants who reported enough income and the group who was able to save were 131 (42.0%) and 53 (17.0%), respectively. Table 1 provides more details of the participants’ profile.
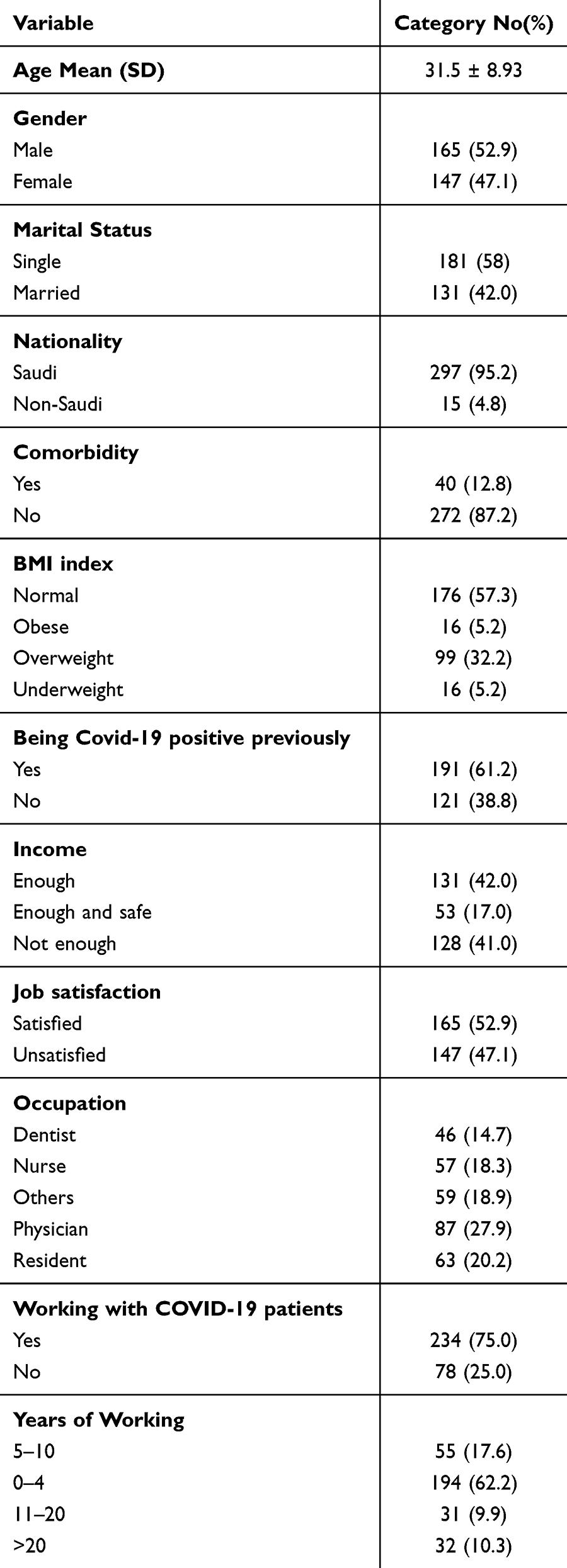 |
Table 1 Participant Profile |
Stress Levels
This study outlined the variables affecting the stress level and how it can vary from participant to participant. The majority of participants (n=223, 71%) reported moderate stress, and 38 (12.2%) had a high level of stress. The mean age of the group who reported moderate and high stress was 30.6 ± 7.3 and 31.6 ± 9.0 years respectively, which was significantly different (p-value = 0.001). The majority of the males (n=113, 68.5%) and females (n=110, 74.8%) reported moderate stress. For the female group 23 (15.6%) reported high stress, comparing to the males (n=15, 9.1%), a significant difference (p-value = 0.004).
This study highlighted that severe stress levels can vary within the financial category. In the group without enough income, 96 (75%) and 20 (15.6%) had moderate and high stress level respectively, compared to 31 (58.5%) and 8 (15.1%) in the group with enough income and the ability to save, a significant difference (p-value = 0.011). In addition, the group with comorbidities had high stress levels (n=10, 25%), compared to the group with none, a significant difference (p-value = 0.029). Being single was associated with an increased risk of a moderate or high stress level in 135 (74.6%), and 25 (13.8%), and in married individuals, 88 (67.2%) and 13 (9.9%), respectively, a significant difference of (p-value = 0.023). Additionally, among those who were satisfied with their job, high stress level reported the less 5 (3%) comparing to those who were unsatisfied 33(22.4%) with significant difference of p <0.001. Table 2 displays the different factors associated with different stress levels.
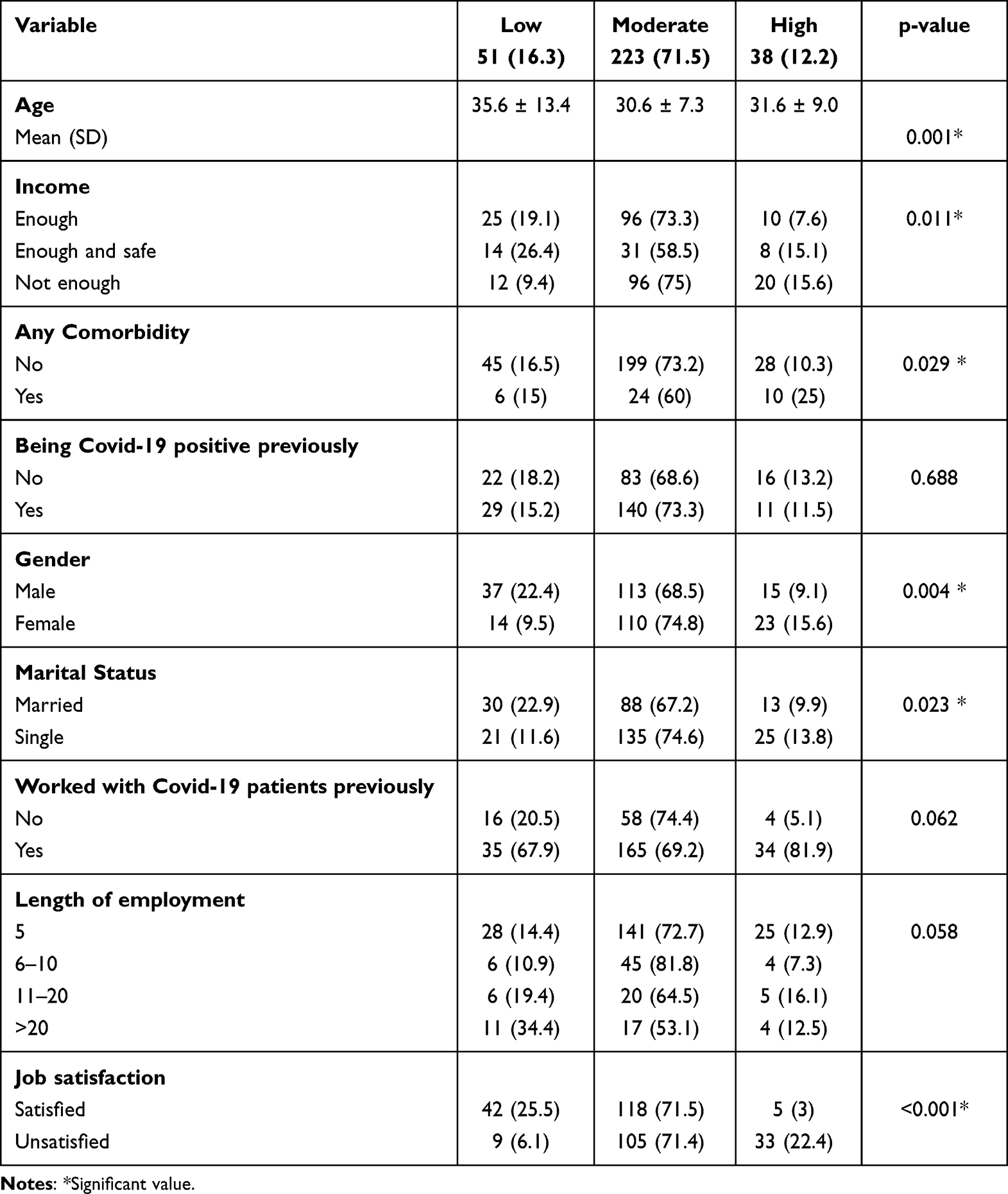 |
Table 2 Factors Associated with Stress Level |
Discussion
Literature reports that the prevalence of work-related stress in HCWs was estimated at 70% and of this group, 30% reported a high level of stress.27–29 Our study reported a slightly higher stress level (73.7%) and 38 (12.2%) with high stress level which could be explained by the presence of expatriate HCWs who might have additional stress due to language barriers and being home-sick. Our study reveals that being single was associated with a higher chance of moderate and high stress levels. This result was compatible with previous studies reporting that marital status was significantly associated with stress.30 In addition, more females reported higher moderate to high levels of stress than males; these findings are parallel with many previous studies reporting the same outcomes.31,32 It could be explained by the biological difference between the genders, for example, releasing hormones such as cortisol has an impact on the response to stress. Another sociodemographic factor associated with stress was income, the group with enough income reported less high levels of stress, but the group with enough income and the ability to save, and the counterpart, reported almost the same stress level; this similarity is interesting. It may be that there is a threshold income level above which additional income does not lead to a significant reduction in stress levels. It is also possible that other factors, such as job security and work-life balance, are more important than income in determining stress levels. It could be justified also by the small sample size, which represent less variation and included only the participants who are physicians with the same socioeconomic status. More research is required to better understand the relationship between income and occupational stress. The current study suggests that income is a significant factor and that individuals with lower incomes are more likely to experience high levels of stress. This finding is important because it highlights the need for employers to focus on reducing stress levels for all employees, regardless of their income level. There are a number of strategies that employers can implement to reduce stress levels, such as providing employees with more control over their work, offering flexible work arrangements, and providing access to employee assistance programs.
Stress was associated with the comorbidity variable. In the current study, we found that the group with comorbidities were less stressed in terms of moderate stress but reported a higher percentage of high stress levels, both interesting and complex. It is possible that individuals with comorbidities are more likely to experience high levels of stress due to the physical and emotional challenges of their condition(s). On the other hand, it is also possible that individuals with comorbidities are more likely to be aware of their stress levels and to seek help when required. It is also important to consider the type of stress that was measured in the study. It is possible that individuals with comorbidities were more likely to experience high levels of stress related to their health, but less likely to experience high levels of stress related to their work or relationships. Thus, the finding that the group with comorbidities were less stressed in terms of moderate stress but reported a higher percentage of high stress levels suggests that the relationship between stress and comorbidity is complex and multifaceted. More research is required to fully understand this relationship.
Our finding regarding to the relationship between working experience and occupational stress was not significant, which is not consistent with previous research reporting that employees with more years of experience reported lower levels of occupational stress.33 It is possible that the study did not have enough participants to detect a statistically significant difference between the two groups. Despite the limitations of our study, our findings are important because it highlights the need for employers to focus on reducing stress levels for all employees, regardless of their work experience or income.
Limitation
The design of this study was a cross-sectional, which might support the assessment of stress levels, but not causality. In addition, our results cannot be generalized to all healthcare communities due to the small sample size.
Conclusion
Our analysis indicated that a quarter of the participants reported high levels of stress and that approximately two-thirds had moderate levels. To be able to investigate the causes of high levels of stress and determine the contributing elements, particularly the connection to the workplace, a sizable nationwide research of healthcare professionals is required. To prevent losing control of the healthcare worker’s stress and the possible escalation to anxiety and/or depression, stress-management programs are necessary, specifically for the group with high stress levels.
Ethical Consideration
Ethical approval was obtained from the Institutional Review Board of King Abdullah International Medical Research Center (RSSR/22R/008/07) prior to data collection. The study protocol was approved ensuring compliance with the Declaration of Helsinki. Patient confidentiality was maintained, as no Personal Identifiable Information (PII) was included.
The purpose of the study was briefly explained in the data collection form, and participants are notified that their participation is entirely voluntary. Those who agreed can proceed with the electronic questionnaire as no formal consent was requested.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Centers for Disease Control and Prevention. Healthcare workers: work stress and mental health. Centers for Disease Control and Prevention; 2016. Available from: https://www.cdc.gov/niosh/topics/healthcare/workstress.html0.
2. Centers for Disease Control and Prevention. Exposure to stress: occupational hazards in hospitals. Centers for Disease Control and Prevention; 2014. Available from: https://www.cdc.gov/niosh/docs/2008-136/default.html.
3. Ismail A, Yao A, Yeo E, et al. Occupational stress features, emotional intelligence and job satisfaction an empirical study in private institutions of higher learning. Rev Cient Electrón Ciencias Gerenciales. 2010;16:5–33.
4. Shinde M, Patel S. Co-relation between problematic internet use and mental health in professional education students. Int J Sci Res. 2014;3(2):194–202.
5. Koinis A, Giannou V, Drantaki V, Angelaina S, Stratou E, Saridi M. The impact of healthcare workers job environment on their mental-emotional health. coping strategies: the case of a local General Hospital:. Health Psychol Res. 2015;3(1):1.
6. Cooper C, Cooper R, Eaker LH. Living with stress. Harmonsworth: Pengium; 1988. Available from: http://www.sciepub.com/reference/351961.
7. Cooper CL, Rachel D. Living with stress (Penguin health library); n.d. Available from: https://www.amazon.com/Living-Stress-Penguin-Health-Library/dp/0140098666.
8. Pfefferbaum B, North CS. Mental health and the Covid-19 pandemic. N Engl J Med. 2020;383(6):510–512. doi:10.1056/NEJMp2008017
9. Giannis D, Geropoulos G, Matenoglou E, Moris D. Impact of coronavirus disease 2019 on healthcare workers: beyond the risk of exposure. Postgrad Med J. 2021;97(1147):326. doi:10.1136/postgradmedj-2020-137988
10. Alwaqdani N, Amer HA, Alwaqdani R, et al. Psychological impact of covid-19 pandemic on healthcare workers in Riyadh, Saudi Arabia: perceived stress scale measures. J Epidemiol Glob Health. 2021;11(4):377–388. doi:10.1007/s44197-021-00014-4
11. Liu X, Kakade M, Fuller CJ, et al. Depression after exposure to stressful events: lessons learned from the severe acute respiratory syndrome epidemic. Comprehensive Psychiatry. 2012;53(1):15–23.
12. Lung F-W, Lu Y-C, Chang -Y-Y, Shu B-C. Mental symptoms in different health professionals during the SARS attack: a follow-up study. Psychiatr Q. 2009;80:107–116.
13. Maunder R, Hunter J, Vincent L. The immediate psychological and occupational impact of the 2003 SARS outbreak in a teaching hospital. CMAJ. 2003;168(10):1245–1251.
14. Wu P, Fang Y, Guan Z, et al. The psychological impact of the SARS epidemic on hospital employees in China: exposure, risk perception, and altruistic acceptance of risk. Can J Psychiatry. 2009;54(5):302–311.
15. Marvaldi M, Mallet J, Dubertret C, Moro MR, Guessoum SB. Anxiety, depression, trauma-related, and sleep disorders among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2021;126:252–264.
16. Sun Y, Song H, Liu H, et al. Occupational stress, mental health, and self-efficacy among community mental health workers: a cross-sectional study during COVID-19 pandemic. Int J Soc Psychiatry. 2021;67(6):737–746.
17. Thomaier L, Teoh D, Jewett P, et al. Emotional health concerns of oncology physicians in the United States: fallout during the COVID-19 pandemic. PLoS One. 2020;15(11):e0242767.
18. Khusid JA, Weinstein CS, Becerra AZ, et al. Well-being and education of urology residents during the covid-19 pandemic: results of an American National Survey. Int J Clin Pract. 2020;74(9):e13559.
19. Shaukat N, Ali DM, Razzak J. Physical and mental health impacts of covid-19 on Healthcare Workers: a scoping review. Int J Emerg Med. 2020;13:1–8.
20. Mokhtari R, Moayedi S, Golitaleb M. Covid-19 pandemic and health anxiety among nurses of intensive care units. Int J Ment Health Nurs. 2020;29(6):1275.
21. Arafa A, Mohammed Z, Mahmoud M, et al. Depressed, anxious, and stressed: what have healthcare workers on the frontlines in Egypt and Saudi Arabia experienced during the covid-19 pandemic? J Affective Disorders. 2021;278:365–371.
22. World Health Organization. Depression. World Health Organization. Available from: https://www.who.int/news-room/fact-sheets/detail/depression.
23. Fahrenkopf AM, Sectish TC, Barger LK, et al. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336(7642):488–491.
24. Druss BG, Rosenheck RA, Sledge WH. Health and disability costs of depressive illness in a major U.S. corporation. Am J Psychiatry. 2000;157(8):1274–1278.
25. Baldisseri MR. Impaired healthcare professional. Crit Care Med. 2007;35(2):S106–S116.
26. Linzer M, Stillman M, Brown R, et al. American medical association–Hennepin healthcare system coping with COVID investigators. Preliminary report: US physician stress during the early days of the COVID-19 pandemic. Mayo Clin Proc Innov Qual Outcomes. 2021;5(1):127–136. PMID: 33718790; PMCID: PMC7930845. doi:10.1016/j.mayocpiqo.2021.01.005
27. Rink LC, Oyesanya TO, Adair KC, Humphreys JC, Silva SG, Sexton JB. Stressors among healthcare workers: a summative content analysis. Glob Qual Nurs Res. 2023;10:23333936231161127. doi:10.1177/23333936231161127
28. American Nurses Foundation. COVID-19 Impact Assessment survey—The Second Year. American Nurses Association Enterprise; 2022.
29. Ta VP, Gesselman AN, Perry BL, Fisher HE, Garcia JR. Stress of singlehood: marital status, domain-specific stress, and anxiety in a national US sample. J Soc Clin Psychol. 2017;36(6):461–485. doi:10.1521/jscp.2017.36.6.461
30. Calvarese M. The effect of gender on stress factors: an exploratory study among university students. Soc Sci. 2015;4(4):1177–1184. doi:10.3390/socsci4041177
31. Matud MP. Gender differences in stress and coping styles. Pers Individ Dif. 2004;37(7):1401–1415. doi:10.1016/j.paid.2004.01.010
32. Mahmood A, Zamir S, Zahoor F. Impact of age and level of experience on occupational stress of academic managers at higher educational level. Mediterr J Soc Sci. 2013;4(1):535–541.
33. Ali AM, Hendawy AO, Ahmad O, Al SH, Smail L;Kunugi H. The Arabic version of the Cohen Perceived Stress Scale: factorial validity and measurement invariance. Brain Sci. 2021;11(4):419.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.