")
Back to Journals » International Journal of Women's Health » Volume 14
The Prescription of Chinese Herbal Medicine and Risk of Endometriosis in Women with Rheumatoid Arthritis: A Population-Based Cohort Study
Authors Chen CJ, Livneh H , Chen WJ , Wang YH, Lu MC, Yeh CC , Yen CT, Tsai TY
Received 13 August 2022
Accepted for publication 13 October 2022
Published 15 November 2022 Volume 2022:14 Pages 1603—1612
DOI https://doi.org/10.2147/IJWH.S386134
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Chia-Jung Chen,1 Hanoch Livneh,2 Wei-Jen Chen,1,3– 5 Yu-Han Wang,5 Ming-Chi Lu,6,7 Chia-Chou Yeh,1,4 Chieh-Tsung Yen,8 Tzung-Yi Tsai9– 11
1Department of Chinese Medicine, Dalin Tzu Chi Hospital, The Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan; 2Rehabilitation Counseling Program, Portland State University, Portland, OR, USA; 3Graduate Institute of Sports Science, National Taiwan Sport University, Taoyuan, Taiwan; 4School of Post-Baccalaureate Chinese Medicine, Tzu Chi University, Hualien, Taiwan; 5Center of Sports Medicine, Dalin Tzu Chi Hospital, The Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan; 6Division of Allergy, Immunology and Rheumatology, Dalin Tzu Chi Hospital, The Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan; 7School of Medicine, Tzu Chi University, Hualien, Taiwan; 8Department of Neurology, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan; 9Department of Nursing, Tzu Chi University of Science and Technology, Hualien, Taiwan; 10Department of Medical Research, Dalin Tzu Chi Hospital, The Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan; 11Department of Environmental and Occupational Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan
Correspondence: Chieh-Tsung Yen; Tzung-Yi Tsai, Tel +886-5-2648000-5003 ; +886-5-2648000-3209, Fax +886-5-2648006, Email [email protected]; [email protected]
Purpose: The systemic inflammation is believed to provide an outline of the association between rheumatoid arthritis (RA) and endometriosis. This retrospective cohort study aimed to explore the association of Chinese herbal medicine (CHM) use with the prevention of endometriosis onset in women diagnosed with RA.
Methods: We utilized the claims data from the National Health Insurance of Taiwan from 2000 to 2009 and excluded individuals diagnosed with endometriosis before being diagnosed with RA, using age at clinical diagnosis. After selection and propensity-score matching, a total of 5992 females aged ≧20 years old and with newly diagnosed RA but without endometriosis at baseline were included, which contained 2996 CHM users and 2996 non-CHM users. All of them were followed until the end of 2013 to measure the incidence of endometriosis.
Results: During the study period, we noticed that CHM users had a substantially lower incidence of endometriosis compared to non-CHM users (2.54 vs 5.19 per 1000 person-years). Use of CHM correlated significantly with a lower endometriosis likelihood even after adjusting for potential covariates, with the adjusted hazard ratio of 0.47 (95% confidence interval, 0.35– 0.65). A longer duration of CHM use was associated with a reduction in endometriosis risk, especially in those using CHM for more than 730 days. Uses of several herbal products may be associated with a lower risk of endometriosis, like Ge-Gen, Da-Huang, Huang-Qin, Ye-Jiao-Teng, Chuan-Niu-Xi, Shu-Jing-Huo-Xue-Tang, Du-Huo-Ji-Sheng-Tang, Ge-Gen-Tang, Shao-Yao-Gan-Cao-Tang, Ping-Wei-San, Gan-Lu-Yin, and Dang-Gui-Nian-Tong-Tang.
Conclusion: Taken together, adding CHM to conventional therapy may reduce the incidence of endometriosis in women with RA. The therapeutic mechanisms and safety of these natural products may be a direction for future clinical studies.
Keywords: endometriosis, rheumatoid arthritis, Chinese herbal medicines, propensity score match
Key Messages
- RA and endometriosis are closely linked physiologically since the two conditions may share underlying physiologic mechanism, namely systemic inflammation.
- This is the first report to identify the therapeutic efficacy of CHM on the prevention of sequent risk of endometriosis among females with RA.
- Our study found that the number of days of CHM use was inversely associated with the likelihood of having endometriosis in a dose-dependent manner.
- Utilization of a nationwide administrative database allowed for detailed CHM prescription records and prevented recall bias.
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory joint disease that leads to pain and inflammation of the tendons in one or more joints. Several studies have linked RA to immune system dysregulation and persistent inflammation.1,2 Nearly up to one-third of RA patients become permanently disabled from work in the first 2 to 3 years of the disease,3 causing enormous socioeconomic burden. A recent study in the United States took a nationally representative sample of RA patients and estimated annual costs of $20,919 per patient, or nearly three times than those without RA ($7197).4
In addition to the enormous economic burden, the systemic inflammation caused by RA has been associated with a wide array of comorbidities, including malignancy, cardiovascular disorders, and respiratory diseases.5 Notably, the link between RA and endometriosis has attracted considerable attention,6 and is especially important because of the higher incidence of RA among females. A recent, large prospective NHS cohort study found that women with RA were at a 40% greater risk of developing endometriosis compared to those without RA.7 While the precise etiology of RA remains elusive, in typical physiological conditions, the dysregulated expression of different types of cytokines from the Helper T (Th) cells is believed to play an important role in the pathogenesis of RA.1,8 In this context, a growing body of evidence has indicated that the upregulation of chronic inflammatory markers, containing interleukin-1(IL-1), interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α), may induce proliferation of endometriosis cells, thus provoking the onset of endometriosis.9 Additionally, recent research efforts have focused on another signaling pathway, namely gut-to-uterus, which suggested that intestinal microbiome dysfunction may cause the activation of immune cells and the production of cytokines in the gut as well, thus driving the risk of endometriosis.10,11 Altogether, these intrinsic inflammatory pathways are presumed to serve as a link between endometriosis and RA. Faced with the increasing burdens caused by these two diseases, the implementation of novel disease management program, with anti-inflammatory agents, may be a more useful addition in early disease stages than in later stages where irreversible tissue damage has already occurred.
Traditional Chinese Herbal Medicine (CHM) has been recognized as a safe and effective method for the treatment of various diseases. Several studies have shown that the active ingredients in CHM may play a role in reducing RA disease activity and have protective effects on joint deformities.12 In addition, CHM has some advantages over Western medicine in lowering the likelihood of endometriosis by regulating inflammation, immunity and angiogenesis.13 However, there is a scarcity of research regarding use of CHM in modulating the subsequent risk of endometriosis among women with RA. To clearly assess effect of CHM on the development of endometriosis among females with RA, we carried out this cohort study using a random sample from a nationwide claims database in Taiwan. By using a larger cohort, we expected to clearly uncover the effect of integrating CHM into conventional therapy for RA patients, which in turn provides the insights into novel disease management strategies.
Methods
Data Source and Identification of Patients with RA
Taiwan’s National Health Insurance Administration Ministry of Health and Welfare (NHI) program, launched in 1995, is a single-payer government-operated compulsory health insurance program. Currently, up to 99% of Taiwanese have been enrolled in the NHI program. The Longitudinal Health Insurance Database (LHID), the database for the NHI program, is made up of one million randomly selected beneficiaries under the NHI and contains the corresponding registration profiles that cover both inpatient and outpatient demographics, primary and secondary diagnoses, procedures, prescriptions, and medical expenditures.14 In the present study, we used the 2000–2009 ambulatory and inpatient data in the LHID to identify subjects with RA and without endometriosis at baseline. RA patients were identified using the International Classification of Diseases-Ninth Revision-Clinical Modification (ICD-9-CM) code for RA (ICD-9-CM 714.0). To avoid potential misclassification, subjects were classified as having RA and included in the analysis if they had at least one hospital admission with a diagnostic code of RA or three or more outpatient visits with a RA diagnostic code within 365 calendar days. Further, to avoid any potential misclassifications, all the records were linked to the catastrophic illness registry to ensure the validity of diagnosis. In Taiwan, the insured citizens with major diseases, such as schizophrenia, mood disorders, autoimmune disorders and cancer, are eligible to apply for a catastrophic illness certificate to obtain a subsidy from the government, which can result in the waiving of outpatient and inpatient co-payments.15 The date of approval for catastrophic illness registration was considered the index date. Overall, we enrolled 7406 females with new-onset RA. The Ministry of Health and Welfare manages the claim data and assigns random identification numbers to beneficiaries to protect their privacy. Accordingly, the Institutional Review Board and Ethics Committee of Buddhist Dalin Tzu Chi Hospital approved this study and waived informed consent for the entire study cohort (Approval Number: B10803015-1).
Outcome of Interest
The primary outcome measure was the development of endometriosis. The diagnosis of endometriosis required that patients were treated with ≥3 outpatient treatment claims or ≥1 hospitalization due to endometriosis (ICD-9-CM code of 617).16 To establish a temporal link between RA and endometrioses, we excluded patients who had a diagnosis of endometrioses before the first RA diagnosis (n = 257), as well as those being followed for less than one year after the cohort entry or with missing data (n = 39). The final cohort comprised 7110 new-onset RA patients (Figure 1).
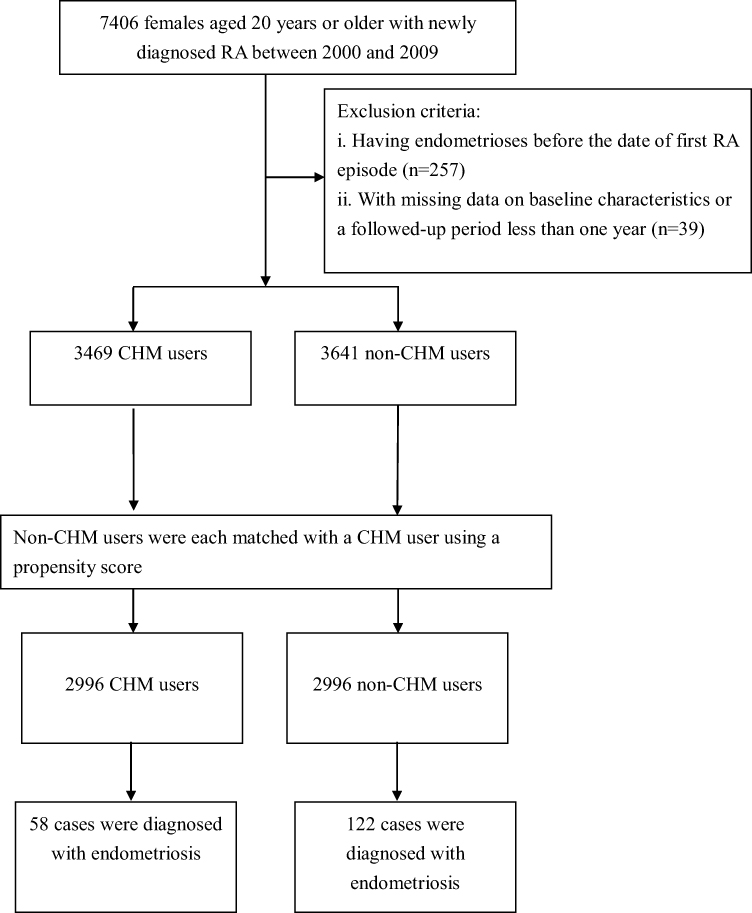 |
Figure 1 Flowchart showing the method of selecting and following study subjects. |
Exposure of CHM Use
Under the NHI program in Taiwan, only certified Chinese medicine physicians are allowed to provide CHM treatment. Based on formerly established methods,17 CHM users were identified if they were ever treated for RA with CHM for more than 30 days (n = 3469). Those treated for ≤30 days were considered to be non-CHM users. Because participation and non-participation in CHM were not randomized in this observational study, we employed the propensity score matching method, in a 1:1 ratio, to improve consistency in the baseline characteristics between both groups. The propensity score value and the predicted probability of CHM exposure were calculated using logistic regression from the patient demographic data (Table 1). We calculated person-years (PYs) of CHM use based on time from initiation of CHM to correct for survival bias in patients who received CHM. The index date of the follow-up period for non-CHM users was assigned as the date of the first RA diagnosis, whereas for CHM users, the date was the start of a CHM prescription.18 All subjects were followed until the end of 2013 to measure the incidence of endometriosis. The duration of observation for each person was calculated until endometriosis diagnosed or censored. Censoring occurred when the patients died, transferred out the insurance system or reached the end of study period, whichever came first.
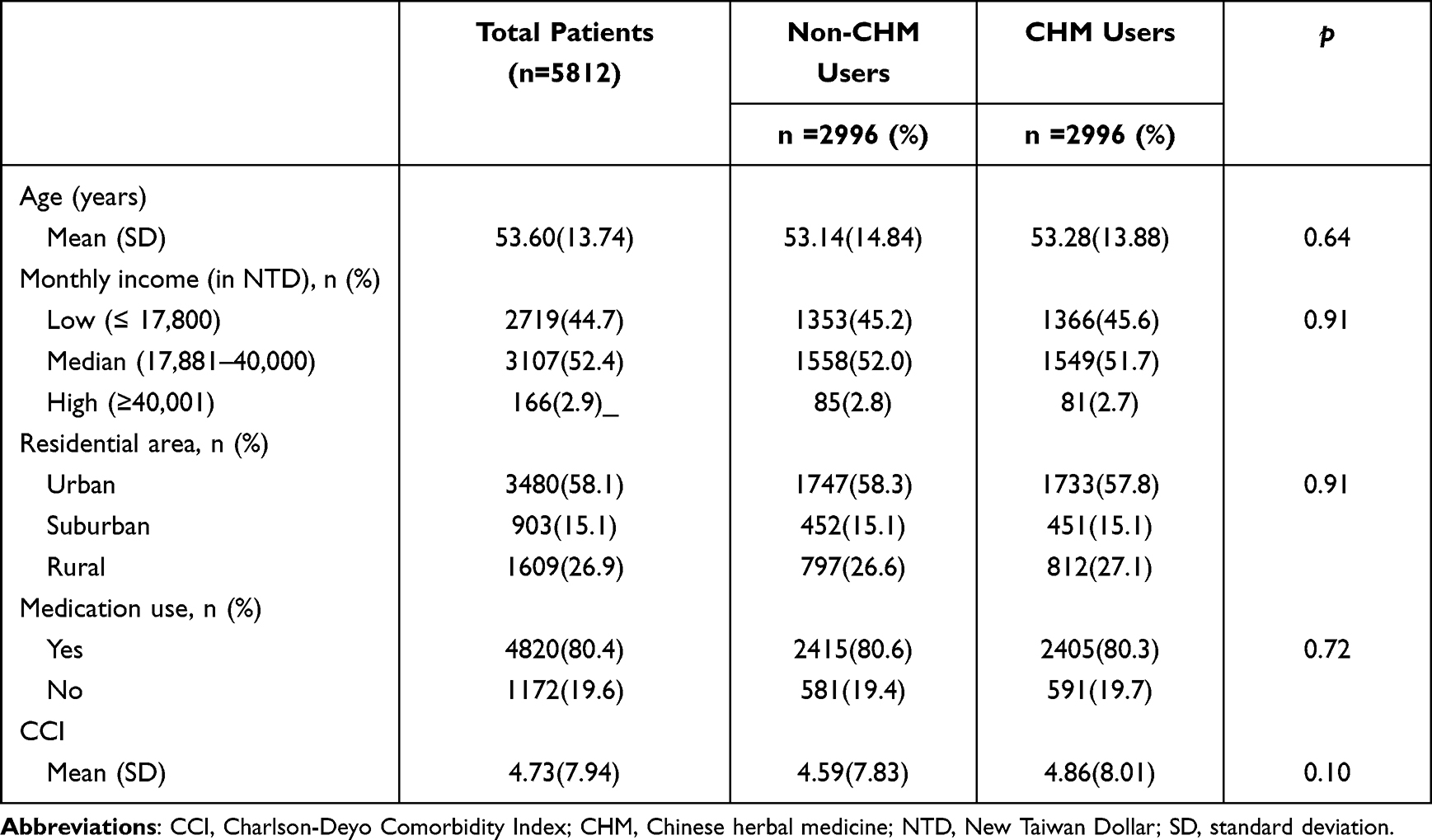 |
Table 1 Characteristics of RA Females According to Use of CHM |
Covariates
Regression model covariates included age, sex, insured amount, urbanization level of the enrollee’s residential area, former comorbidities, and medication use. The insured amount was calculated from the patient’s average monthly income and then served as an economic index, with 17,880 New Taiwanese Dollar (NTD) being the lowest income-related insurance amount (approximately 623 $US) at that time. Additionally, the participant’s postal address closet to the index date was considered to determine the level of urbanization according to the categorization scheme developed in a previous study,19 which included population density, proportion of persons with a college-level education or higher, proportion of elderly residents, proportion of agricultural workers, and number of physicians per 100,000 population. The Charlson-Deyo Comorbidity Index (CCI), a validated indicator of a patient’s relative burden of disease, was determined from individual medical records in the year preceding cohort entry.20 This index contained 17 chronic diseases, and each assigned a score of 1–6 points, with a higher score indicating a higher burden. Medication use was stratified in both cohorts into two categories based on whether or not the subject has ever used disease-modifying anti-rheumatic drugs (methotrexate, sulfasalazine, ciclosporin, hydroxychloroquine, penicillamine, or leflunomide) for more than 6 months after the index date.
Statistical Analysis
All analyses were performed using the SAS statistical package (Version 9.3; SAS Institute Inc., Cary, NC, USA) with a two-tailed significance level of 0.05. Incident rates were calculated by dividing the case number from endometriosis by the number of PYs of follow-up. Differences in baseline characteristics between RA patients who received CHM treatment and those who did not receive CHM treatment were assessed using a two-sided t-test or the Pearson’s chi-square test. The Cox proportional hazard regression models adjusting for all potential confounders were used to estimate the relative magnitude of risk in relation to the use of CHM. To further verify the robustness of the relationship between CHM use and endometriosis risk, the enrollees were divided into four groups based on CHM exposure categories: nonusers, CHM users for 31–365 days, CHM users for 366–730 days, and CHM users for more than 730 days. We also treated it as a continues variable to calculate the P value of the linear trend. Hazard ratio (HR) and their 95% confidence interval (CI) were calculated using patients with no exposure as reference. The Kaplan–Meier method and Log rank test were used to estimate the event-free survival rate and to examine differences in the risk of endometriosis across all four groups. We checked the assumptions of proportional hazards by plotting a log (-log[survival]) versus log of survival time plot.
Results
Of the whole study cohort, the CHM user and non-CHM user groups contributed data on 2996 patients each. The mean age of patients was 53.60 ± 13.74 years, and most of the patients had a monthly income of NTD 17,881–43,900 (52.4%) and lived in urban areas (58.1%) (Table 1). There were no differences between the CHM user and non-CHM user groups in the baseline distributions that reached statistical significance after matching (Table 1).
We identified 180 cases of endometriosis, 122 in non-CHM users and 58 in CHM users, during follow-up periods of 23,508.31 and 22,870.99 PYs, respectively. The incidence of endometriosis was indeed lower in the CHM users than in non-CHM users (2.54 vs 5.19 per 1000 PYs) (adjusted HR = 0.47; 95% CI: 0.35–0.65) (Table 2). Notably, subgroups with a longer duration of CHM use had lower risks of endometriosis, with a dose-dependent relationship identified between days of CHM usage and endometriosis risk (Table 2). Results of Kaplan–Meier survival analysis and the Log rank test also showed differences in the endometriosis-free survival rate across the four groups during the follow-up period (p < 0.001) (Figure 2).
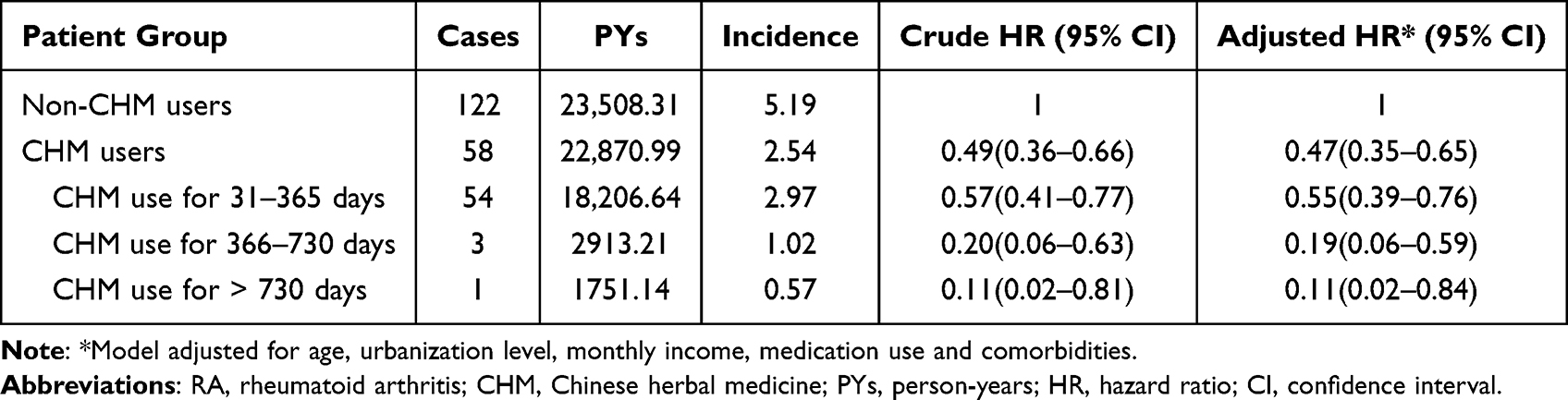 |
Table 2 Cox Model with HR and 95% CI of Endometriosis Associated with CHM Use |
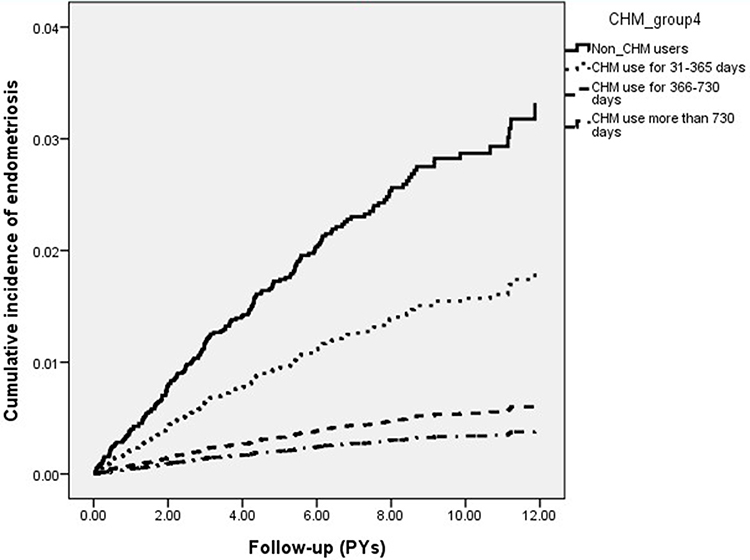 |
Figure 2 Kaplan–Meier curves plotting cumulative incidence of endometriosis across four groups (Log rank test, p<0.001). |
In addition, among the commonly prescribed CHM therapies for RA, twelve herbal products were noted to be associated with a lower risk of endometriosis, like Ge-Gen, Da-Huang, Huang-Qin, Ye-Jiao-Teng, Chuan-Niu-Xi, Shu-Jing-Huo-Xue-Tang (SJHXT), Du-Huo-Ji-Sheng-Tang (DHJST), Ge-Gen-Tang (GGT), Shao-Yao-Gan-Cao-Tang (SYGCT), Ping-Wei-San (PWS), Gan-Lu-Yin (GLY), and Dang-Gui-Nian-Tong-Tang (DGNTT) (Figure 3).
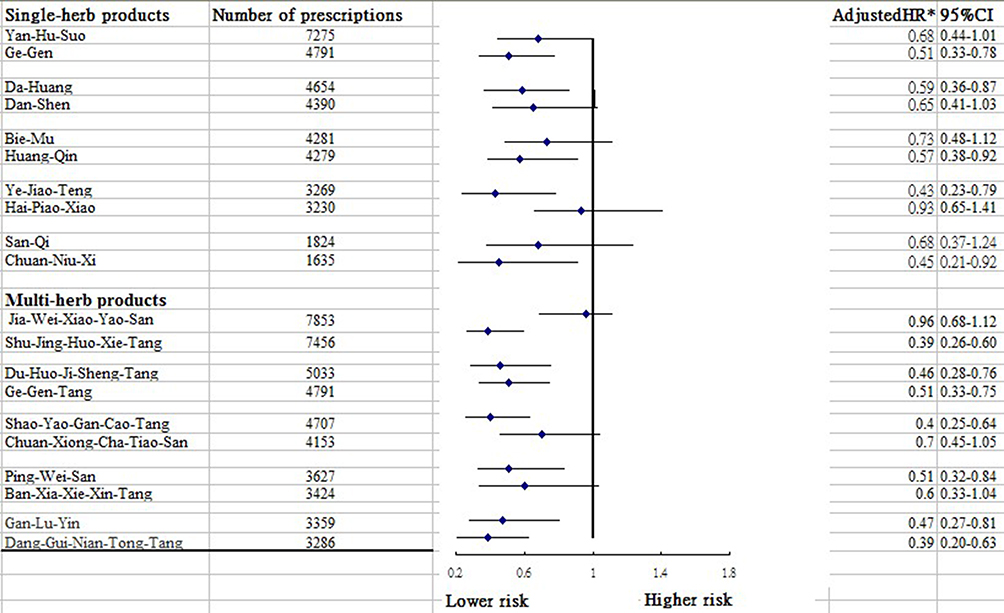 |
Figure 3 Risk of endometriosis in relation to the 10 most-used single-herb and multi-herb CHM products among subjects. |
Discussion
The onset of RA often arises within the ages of 30–50 years, which may pose a major health burden and affect many women of reproductive age. It is well known that the pathophysiology of RA involves chronic inflammation of the synovial membrane, such as the expressions of TNF-α and several of interleukins containing IL-1, IL-6 as well as IL-7, all of which gradually destroy articular cartilage and juxta-articular bone1,8 The production of various pro-inflammatory mediators is also shown to affect tissue destruction and this further leads to the induction of endometriosis.7,9 Thus, early detection and treatment to prevent endometriosis following a diagnosis of RA seems an important clinical goal. Findings of this study showed that, compared with those without receiving CHM, those treated with CHM in addition to routine care experienced a 53% lower risk of developing endometriosis. Those receiving CHM treatments for more than two years had a nearly 90% lower risk of endometriosis than the non-CHM users. Even though there is a lack of comparable literature, these positive effects of CHM on the reduction of endometriosis chance could add to a growing body of literature on the clinical efficacy of CHM.21,22 A variety of natural products from traditional Chinese medicines have been shown to safely regulate proinflammatory pathways and control inflammation-associated diseases,13 which may account for the positive impacts of CHM observed in this study.
For example, the current study showed that several herb products may have potential for preventing endometriosis, like SYGCT, GLY and PWS. All of these remedies have been shown to regulate cellular responses to inflammation, which in turn decrease the risk of endometriosis after RA onset. Regarding SYGCT, it is traditionally used to treat muscle spasms and pain throughout the body by acting as a muscle relaxant. A previous in vivo study demonstrated that paeoniflorin, the main component of SYGCT, dose-dependently decreases the secretion of pro-inflammatory mediators by inhibiting the activation of nuclear factor kappa light chain enhancer in B cells p65 (NF-κB/p65).23 As to the prescription of GLY, a mechanistic study in a rat model revealed that the anti-inflammatory activity of GLY may be tied to the inhibition of pro-inflammatory cytokines such as IL-1β, IL-6, TNF-α, and PGE2.24 One former study using an animal experimental model also found that an extract of Magnolia officinalis, a major ingredient purified from PWS, could substantially regulate the production of inflammatory mediators by abating the NF-κB pathway.25 All of these may point to the possible mechanisms for these herbs.
We also noted that other commonly prescribed CHM therapies targeting RA, such as SJHXT and DHJST, were significantly linked to a lower risk of endometriosis. In practice, these two herbal products are commonly used for pain and muscle soreness relief. In addition to regulating immunity, SJHXT possesses anti-inflammatory properties. One earlier rodent experiment suggested that SJHXT might exert anti-inflammatory and analgesic effects by modulating the activity of the α-2 adrenoceptor.26 A review article reported that dysregulation of the α2- adrenoceptor pathway may contribute to aberrant cytokine gene expression.27 Additionally, gentianine, a major compound of DHJST, was found to exhibit powerful anti-inflammatory effects via the downregulation of cytokines, including IL-6 and TNF-α,28 all of which are implicated in the pathogenesis of endometriosis.1,2
The positive therapeutic impacts of DGNTT and GGT in reducing the likelihood of endometriosis were also identified. The prescription of DGNTT was found to have anti-inflammatory and immune regulatory effects in murine macrophages by regulating the activation of p38 mitogen-activated protein kinase (MAPK) pathway.29 In addition, we observed positive effects of GGT when taken together with Ge-Gen in preventing endometriosis. An earlier report showed that, compared to untreated controls, mice fed with GGT had remarkably lower inflammatory-induced cytokine levels through the down-regulation of NF-κB/p65 activation and the inhibition of NF-kB activity.30 The anti-inflammatory effects of these polyherbal formulations may explain the reduction in the endometriosis risk among females with RA.
Among the other single-herb products used to treat those with RA, uses of Da-Huang and Huang-Qin were effective in reducing the risk of endometriosis. We speculate that the positive impacts may be related to the corresponding compounds, such as the baicalin in Huang-Qin and emodin in Da-Huang, respectively. Both of these compounds can mediate brain-derived neurotrophic factor (BDNF) expression.31,32 In addition to their positive effects on cognitive function and long-term memory, serum BDNF level has been implicated not only in neuroinflammation but also in inflammatory processes in visceral organs, especially in RA.33 Meanwhile, BDNF, together with its high-affinity tyrosine kinase type B (TrKB) receptor, has been linked to the onset of severe female reproductive disorders, including endometriosis.34
Further, the present investigation pointed out the positive effects of Ye-Jiao-Teng and Chuan-Niu-Xi in preventing the onset of endometriosis. A murine model showed that an extract of Ye-Jiao-Teng could downregulate nitric oxide (NO) and pro-inflammatory cytokines, such as TNF-α and IL-1β, which are key mediators of inflammation.35 One recent review article mentioned that oxidative stress was associated with the inflammatory response, and excess reactive oxygen species may play an essential role in endometriosis onset.9 For Chuan-Niu-Xi, this remedy has demonstrated various beneficial pharmacological activities both in vivo and in vitro, including analgesic, immunostimulant, antitumor, and anti-inflammatory effects.36 Cao et al compared a group of mice injected an extract of Chuan-Niu-Xi to a control group of mice that had not been injected, and they found this CHM product can significantly reduce levels of IL‑6, TNF-α and cyclooxygenase-2 (COX-2) in the plasma,37 all of which have been implicated in the pathogenesis of endometriosis.9
This investigation is strengthened by the use of a population-based design, a large and nationally representative sample, and a long follow-up time, especially given the relatively low incidence of RA in the population. Furthermore, this study applied the medical records from a primary care database, and thus results are less likely to be affected by confirmation bias. The third strength was the use of propensity score matching to select subjects without CHM use, which could reduce the possibility of confounding. Yet, this study has several limitations that should be taken into account. First, certain important information regarding family history, lifestyle, and laboratory parameters were not recorded in the LHID. Thus, the residual confounding might occur in the observed association because participants were not initially randomly assigned into users and non-users. A randomized controlled trial to validate the present findings is warranted. Second, our findings were based on a retrospective cohort design that utilized the ICD-9-CM diagnostic codes. Thus, bias due to miscoding and misclassification may occur. To diminish the possible misdiagnosis, we selected only participants with at least two consistent ICD-9-CM diagnosis, plus at least one inpatient hospitalization claim during the study period. It should be acknowledged that the NHI of Taiwan makes efforts to prevent misdiagnoses by performing quarterly expert reviews on diagnosis and imposing severe penalties on misdiagnosis. Additionally, the probability of individuals being misclassified is equal across groups, so any misclassification in this study was prone to be randomized, thereby reducing the overall HR observed towards the null value and thus providing a conservative estimation of risk. Third, data regarding RA severity are unavailable in the database, and failure to deal with this might bias the conclusion. To address this point, we used a proxy indicator to confirm RA severity, namely a history of biologic agents that include adalimumab, etanercept, infliximab, rituximab and tocilizumab. After considering this surrogate variable in the multivariate analysis, the re-analysis indicated that, as compared to RA patients who did not receive CHM therapy, the selected group of RA who did receive CHM still had a lower risk for endometriosis (adjusted HR, 0.49; 95% CI, 0.36–0.66).
Conclusions
After utilizing a larger, nationally representative medical records database with up to over 10 years of follow-up, we found that RA patients receiving CHM, in addition to conventional treatment, had a 53% lower risk of developing endometriosis. As a consequence, heightened attention for preventing and managing symptoms of RA may be warranted, especially endometriosis. Future prospective randomized trials that overcome the limitations herein are needed to provide more robust evidence to support and guide the use of CHM in clinical practice for patients with RA.
Acknowledgments
This study used data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by the National Health Research Institutes, Taiwan. The interpretation and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health, or the National Health Research Institutes. We also thank for the suggestions from Dr. Hsin-Hua Li. CJC, HL, WJC and YHW equally contributed to this work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflict of interests.
References
1. Aletaha D, Smolen JS. Diagnosis and management of rheumatoid arthritis: a review. JAMA. 2018;320(13):1360–1372. doi:10.1001/jama.2018.13103
2. Lin YJ, Anzaghe M, Schülke S. Update on the pathomechanism, diagnosis, and treatment options for rheumatoid arthritis. Cells. 2020;9:880. doi:10.3390/cells9040880
3. Sokka T. Work disability in early rheumatoid arthritis. Clin Exp Rheumatol. 2003;21:S71–S74.
4. Chen CI, Wang L, Wei W, et al. Burden of rheumatoid arthritis among US medicare population: co-morbidities, health-care resource utilization and costs. Rheumatol Adv Pract. 2018;2:I1–I9.
5. Gabriel S, Michaud K. Epidemiological studies in incidence, prevalence, mortality, and comorbidity of the rheumatic diseases. Arthritis Res Ther. 2009;11:229. doi:10.1186/ar2669
6. Shigesi N, Kvaskoff M, Kirtley S, et al. The association between endometriosis and autoimmune diseases: a systematic review and meta-analysis. Hum Reprod Update. 2019;25:486–503. doi:10.1093/humupd/dmz014
7. Harris HR, Costenbader KH, Mu F, et al. Endometriosis and the risks of systemic lupus erythematosus and rheumatoid arthritis in the Nurses’ Health Study II. Ann Rheum Dis. 2016;75:1279–1284. doi:10.1136/annrheumdis-2015-207704
8. Kotake S, Yago T, Kobashigawa T, et al. The plasticity of Th17 cells in the pathogenesis of rheumatoid arthritis. J Clin Med. 2017;6:67. doi:10.3390/jcm6070067
9. Zhang T, De Carolis C, Man GCW, et al. The link between immunity, autoimmunity and endometriosis: a literature update. Autoimmun Rev. 2018;17:945–955. doi:10.1016/j.autrev.2018.03.017
10. D’Alterio MN, Giuliani C, Scicchitano F, et al. Possible role of microbiome in the pathogenesis of endometriosis. Minerva Obstet Gynecol. 2021;73:193–214. doi:10.23736/S2724-606X.21.04788-2
11. Viganó D, Zara F, Pinto S, et al. How is small bowel permeability in endometriosis patients? A case control pilot study. Gynecol Endocrinol. 2020;36:1010–1014. doi:10.1080/09513590.2020.1766440
12. Zhang Z, Cao H, Shen P, et al. Ping weisan alleviates chronic colitis in mice by regulating intestinal microbiota composition. J Ethnopharmacol. 2020;255:112715. doi:10.1016/j.jep.2020.112715
13. Zheng W, Wu J, Gu J, et al. Modular characteristics and mechanism of action of herbs for endometriosis treatment in Chinese medicine: a data mining and network pharmacology-based identification. Front Pharmacol. 2020;11:147. doi:10.3389/fphar.2020.00147
14. Center for Biomedical Resources of NHRI. National health insurance research database. Taiwan. LHID; 2000. Available from: https://nhird.nhri.org.tw/en/Data_Subsets.html.
15. Patients with catastrophic illnesses or rare disease. National health insurance administration, ministry of health and welfare, Taiwan. Available from: https://www.nhi.gov.tw/English/Content_List.aspx?n=F5B8E49CB4548C60&topn=1D1ECC54F86E9050.
16. Tai FW, Chang CY, Chiang JH, et al. Association of pelvic inflammatory disease with risk of endometriosis: a nationwide cohort study involving 141,460 individuals. J Clin Med. 2018;7:379. doi:10.3390/jcm7110379
17. Chang ZP, Deng GF, Shao YY, et al. Shaoyao-gancao decoction ameliorates the inflammation state in polycystic ovary syndrome rats via remodeling gut microbiota and suppressing the TLR4/NF-κB pathway. Front Pharmacol. 2021;12:670054. doi:10.3389/fphar.2021.670054
18. Zhou Z, Rahme E, Abrahamowicz M, Pilote L. Survival bias associated with time-to treatment initiation in drug effectiveness evaluation: a comparison of methods. Am J Epidemiol. 2005;162(10):1016–1023. doi:10.1093/aje/kwi307
19. Liu CY, Hung YT, Chuang YL, et al. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J Health Manag. 2006;4:1–22.
20. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45:613–619. doi:10.1016/0895-4356(92)90133-8
21. Lee WY, Chen HY, Chen KC, et al. Treatment of rheumatoid arthritis with traditional Chinese medicine. Biomed Res Int. 2014;2014:11.
22. Pan HD, Xiao Y, Wang WY, et al. Traditional Chinese medicine as a treatment for rheumatoid arthritis: from empirical practice to evidence-based therapy. Engineering. 2019;5:895–906. doi:10.1016/j.eng.2019.01.018
23. Lai X, Wei J, Ding X. Paeoniflorin antagonizes TNF-α-induced L929 fibroblastoma cells apoptosis by inhibiting NF-κBp65 activation. Dose Response. 2018;16:1559325818774977. doi:10.1177/1559325818774977
24. Chen YH, Luo R, Lei SS, et al. Anti-inflammatory effect of Ganluyin, a Chinese classic prescription, in chronic pharyngitis rat model. BMC Complement Med Ther. 2020;20:265. doi:10.1186/s12906-020-03057-5
25. Zhang Z, Shen P, Xie W, et al. Pingwei San ameliorates dextran sulfate sodium-induced chronic colitis in mice. J Ethnopharmacol. 2019;236:91–99. doi:10.1016/j.jep.2019.01.043
26. Shu H, Arita H, Hayashida M, et al. Anti-hypersensitivity effects of Shu-jing-huo-xue-tang, a Chinese herbal medicine, in CCI-neuropathic rats. J Ethnopharmacol. 2010;131:464–470. doi:10.1016/j.jep.2010.07.004
27. Scanzano A, Cosentino M. Adrenergic regulation of innate immunity: a review. Front Pharmacol. 2015;6:171. doi:10.3389/fphar.2015.00171
28. Wenjin C, Jianwei W. Protective effect of gentianine, a compound from Du Huo Ji Sheng Tang, against freund’s complete adjuvant-induced arthritis in rats. Inflammation. 2017;40:1401–1408.
29. Kim SB, Kang OH, Keum JH, et al. Anti-inflammatory effects of Danggui Liuhuang decoction in RAW 264.7 cells. Chin J Integr Med. 2012. doi:10.1007/s11655-012-1237-1
30. Yang X, Zhang H, Wang J, et al. Puerarin decreases bone loss and collagen destruction in rats with ligature-induced periodontitis. J Periodontal Res. 2015;50:748–757. doi:10.1111/jre.12261
31. Yu HY, Yin ZJ, Yang SJ, et al. Baicalin reverse AMPA receptor expression and neuron apoptosis in chronic unpredictable mild stress rats. Biochem Biophys Res Commun. 2014;451:467–472. doi:10.1016/j.bbrc.2014.07.041
32. Gao LL, Wang ZH, Mu YH, et al. Emodin promotes autophagy and prevents apoptosis in sepsis-associated encephalopathy through activating BDNF/TrkB signaling. Pathobiology. 2022;89:135–145. doi:10.1159/000520281
33. Lai NS, Yu HC, Huang Tseng HY, et al. Increased serum levels of brain-derived neurotrophic factor contribute to inflammatory responses in patients with rheumatoid arthritis. Int J Mol Sci. 2021;22:1841. doi:10.3390/ijms22041841
34. Wang S, Duan H, Li B, et al. BDNF and TrKB expression levels in patients with endometriosis and their associations with dysmenorrhoea. J Ovarian Res. 2022;15:35. doi:10.1186/s13048-022-00963-9
35. Cha DS, Jeon H. Anti-inflammatory effect of MeOH extracts of the stem of Polygonum multiflorum in LPS-stimulated mouse peritoneal macrophages. Nat Prod Sci. 2009;15:83–89.
36. Huang Y, Wang S, Liu L, et al. Review of traditional uses, botany, chemistry, pharmacology, pharmacokinetics, and toxicology of Radix Cyathulae. Chin Med. 2019;14:17. doi:10.1186/s13020-019-0237-x
37. Cao Y, Gu C, Zhao F, et al. Therapeutic effects of cyathula officinalis kuan and its active fraction on acute blood stasis rat model and identification constituents by HPLC-QTOF/MS/MS. Pharmacogn Mag. 2017;13:693–701. doi:10.4103/pm.pm_560_16
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.