Back to Journals » Clinical Interventions in Aging » Volume 18
The Predictive Values of White Blood Cell Indices (Lymphocyte and Eosinophilic Granulocyte) for Heart Failure in Acute Coronary Syndrome Patients Following Percutaneous Coronary Intervention: A Prospective Cohort Study
Authors Wen W ![]() , Zhang Z, She J
, Zhang Z, She J ![]() , Bai X
, Bai X ![]() , Wu Y, Gao L, Zhou J, Yuan Z
, Wu Y, Gao L, Zhou J, Yuan Z
Received 31 March 2023
Accepted for publication 8 June 2023
Published 17 June 2023 Volume 2023:18 Pages 951—962
DOI https://doi.org/10.2147/CIA.S413313
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Wen Wen,1 Zhanyi Zhang,2 Jianqing She,2 Xiaofang Bai,3 Yan Wu,2 Li Gao,2 Juan Zhou,2,4,5 Zuyi Yuan2,4,5
1Department of Ultrasound, Clinical Medical College, First Affiliated Hospital of Chengdu Medical College, Chengdu, People’s Republic of China; 2Department of Cardiovascular Medicine, First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China; 3Department of Ultrasound, First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China; 4Key Laboratory of Environment and Genes Related to Diseases, Ministry of Education, Xi’an Jiaotong University, Xi’an, People’s Republic of China; 5Key Laboratory of Molecular Cardiology, Xi’an Jiaotong University, Xi’an, People’s Republic of China
Correspondence: Juan Zhou; Zuyi Yuan, Email [email protected]; [email protected]
Background: White blood cell (WBC) indices are strongly associated with cardiovascular disease, but data on the prognostic values of these parameters in patients with acute coronary syndrome (ACS) following percutaneous coronary intervention (PCI) are sparse. The current study aimed to investigate the relationship between baseline WBC indices levels and the incidence of heart failure (HF) in ACS patients after PCI and explore the predictive values over a 2-year follow-up period.
Methods: A total of 416 consecutive ACS patients treated with PCI were enrolled and received a median of 27.7 months follow-up. Univariate and multivariate Cox regression analyses and the receiver operating characteristic (ROC) curves were performed.
Results: Baseline lymphocyte (LYMPH) count, eosinophil (EO) count and eosinophil percentage (EO %) were higher in patients who experienced HF over a 2-year follow-up. In multivariate Cox proportional hazards analysis, LYMPH count, EO count and EO % were independently associated with the occurrence of HF (hazard ratio [HR] = 12.876, P = 0.025; HR = 16.625, P = 0.004; HR = 1.196, P = 0.031, respectively). The area under the ROC curve of baseline EO count predicting the occurrence of HF in ACS patients following PCI was 0.625 (P = 0.037). For patients aged 60 years and above, who had PCI or history of coronary artery bypass grafting, the higher EO count, the higher the risk of HF.
Conclusion: Elevated baseline LYMPH count, EO count and EO % were independently associated with the incidence of HF in ACS patients following PCI, suggesting that WBC indices might be available, simple, and cost-efficient biomarkers with predictive value, especially for patients aged more than 60 years.
Keywords: heart failure, acute coronary syndrome, lymphocytes, eosinophils, independent predictive factors
Background
Acute coronary syndrome (ACS), such as unstable angina (UA) and acute myocardial infarction (MI) caused by the rupture of the atherosclerotic plaque and subsequent thrombosis, is a serious form of cardiovascular disease with a high mortality risk worldwide.1–3 Multiple studies have proved the influence of immune cells has moved into focus with respect to their involvement in ACS, especially the pathogenesis of atherosclerosis and thrombosis.4,5 Although revascularisation and antithrombotic strategies have achieved great success in decreasing mortality of patients with ACS, the outcomes are considered to be unsatisfactory.6 The occurrence of heart failure (HF) is closely related to long-term survival of patients with ACS. There is a body of evidence suggesting that immune and inflammatory processes are involved in the pathophysiology of HF, and inflammation is currently discussed as a therapeutic target in HF.7
White blood cell (WBC) count is a marker of systemic inflammation. Inflammatory cytokines, which are closely related to the development of HF, are mainly secreted by WBC and, conversely, were also shown to impact WBC levels.8 Large amounts of clinical observations suggest that, besides classical players, WBC count is strongly associated with HF, additionally, associated with the risk factors of HF such as age and smoking.9,10 Several lines of evidence link lymphocytes (LYMPH) and eosinophils (EO) to cardiovascular events,11,12 but data on the association with the incident of HF are sparse, and the prognostic values of these WBC indices in ACS patients are still unclear. The aim of this study was to investigate the association of WBC indices, particularly its individual components such as LYMPH and EO counts, with the occurrence of HF in ACS patients following percutaneous coronary intervention (PCI) over a 2-year follow-up. We assume that WBC indices can be fast and convenient candidate markers to predict the risk of long-term adverse cardiovascular events in ACS patients after PCI.
Materials and Methods
Study Participants, Outcome and Follow-Up
The investigation presented a single-centre, prospective, cohort study as we previously described.13 Briefly, from January 2013 to February 2014, after screening of 2132 consecutive patients diagnosed with CAD at First Affiliated Hospital of Xi’an Jiaotong University, a total of 416 consecutive patients who were diagnosed with ACS and then underwent PCI were eventually enrolled in this study. The detailed inclusion and exclusion criteria are shown in Table 1. HF was defined as end point in the current study. Participants were eligible if they were in New York Heart Association (NYHA) functional class ≥II and were required to have a left ventricular ejection fraction (LVEF) ≤40%, and were pharmacologically treated for HF. Patients with HF also have N-terminal pro-B-type natriuretic peptide (NT-proBNP) concentration ≥600 pg/mL (≥400 pg/mL if hospitalized for HF within the previous 12 months). All participants received follow-up through personal interviews by well-trained physicians until March 31, 2016. Follow-up ended on the date of end point (HF) occurrence. The median follow-up time was 27.7 months.
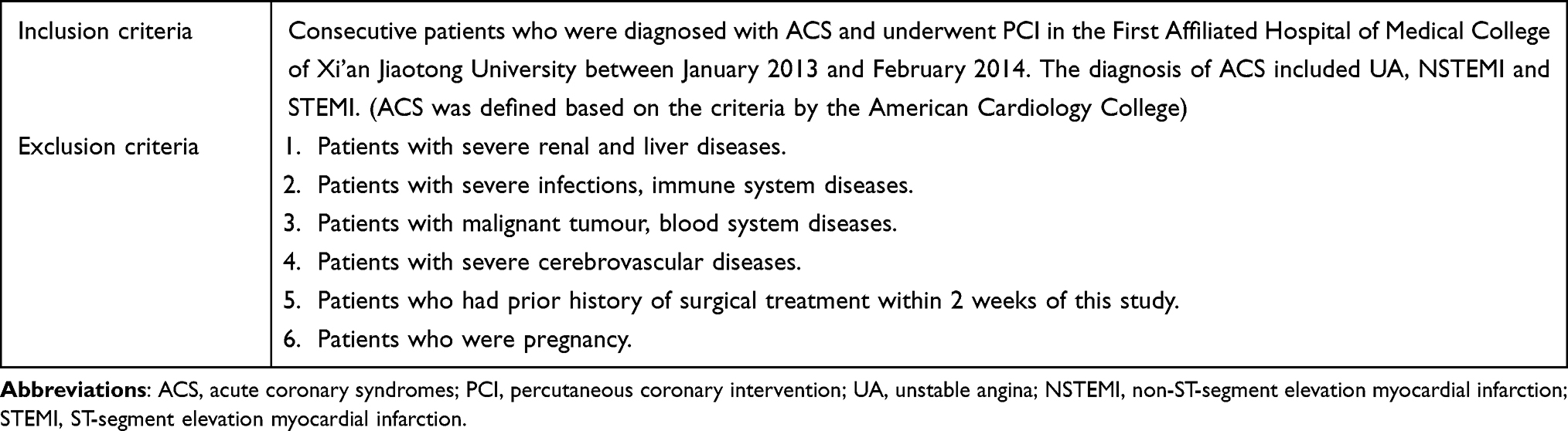 |
Table 1 Inclusion and Exclusion Criteria |
Ethics Statement
Approval of the Ethics Committee of Xi’an Jiaotong University (Ethical approval number: XJTU1AF2012LSK-312) was obtained, and the written informed consents were obtained from all the participants. The study conformed to the Declaration of Helsinki and collected the required data from the clinical records without clinical intervention to protect patients’ privacy.
Data Collection
The baseline information was composed of the demographic characteristics (age, gender, etc.) and partial known cardiovascular risk factors (smoking, family history, diabetes mellitus, hypertension, etc.). Clinical indexes (ejection fraction, systolic pressure, diastolic pressure, ACS type, NYHA classification, etc.) were recorded. After admission, peripheral blood samples of patients were collected from fasting state early in the morning before PCI. Baseline laboratory data containing partial cardiovascular risk factors (blood routine, blood lipids, creatine kinase isoenzymes MB, NT-proBNP, fibrinogen, blood glucose, and D-Dimer) were performed by experts from the biochemistry centre of the First Affiliated Hospital of Xi’an Jiaotong University, using standard biochemical techniques. More specifically, blood samples were harvested and blood routine examination including absolute and percentage counts (eg, blood neutrophil (NEUT) count, LYMPH count, EO count and EO percentage (EO %), etc.) was performed using the whole blood by an automatic hematology analyzer (Sysmex 2100, Japan). Echocardiographic parameters and other biochemical parameters were measured using standard methods.
Statistical Analysis
Statistical analyses were performed by SPSS 18.0 (SPSS Inc, Chicago, IL) and EmpowerStats (http://www.empowerstats.com/). Continuous variables are presented as the mean ± standard deviation if normally distributed or median (lower quartile, upper quartile) otherwise. Categorical variables are presented as numbers (percentages). Variables of interest were compared using Student’s t-test, one-way ANOVA or the Chi squared test as appropriate. For nonnormally distributed continuous variables, the Kruskal–Wallis analysis was used. Cox regression analysis was applied to calculate hazard ratios (HRs) and 95% confidence intervals (CIs) to determine the independent predictors of HF. Multivariate and stratified analysis were used to identify predictors. Kaplan–Meier survival analysis and Log rank tests were performed to compare the adverse event-free survival rate. The area under the receiver operating characteristic (ROC) curves (AUCs) were used to indicate the predictive value of variables for HF. A value of P < 0.05 was considered statistically significant.
Results
Basic Characteristics of Participants
A total of 416 patients who were diagnosed with ACS and underwent the follow-up were enrolled in this investigation, with HF patients accounting for 9.9% (41/416) of the overall cohort. Table 2 displays the baseline characteristics of the whole patients, patients with HF and without HF. There were no significant differences observed in the baseline demographic, clinical parameters and laboratory data except for age, gender, the history of smoking, LYMPH count, EO count and EO % (P < 0.05). Of these, LYMPH count, EO count and EO % in patients with HF were significantly higher than those without HF (1690 (1280–2390) cells/µL vs 1440 (1100–1905) cells/µL, P = 0.029; 150 (40–210) cells/µL vs 80 (40–140) cells/µL, P = 0.008; 1.8 (0.8–3.4) vs 1.2 (0.6–2.2), P = 0.038, respectively). No significant differences were observed in other blood routine parameters (all had P > 0.05).
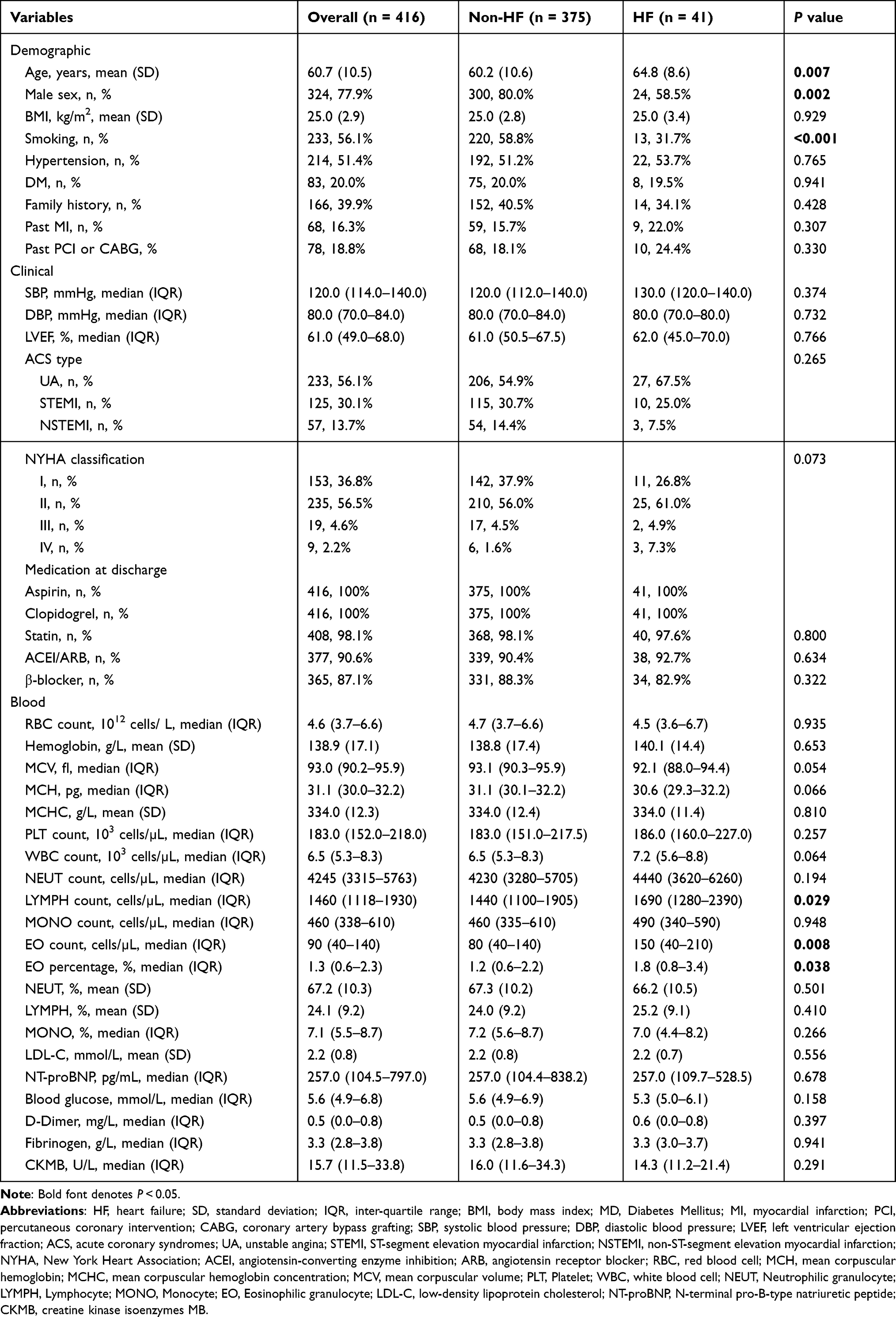 |
Table 2 Basic Characteristics of Patients with HF, without HF and Overall |
Univariate and Multivariate Cox Regression Analysis
To determine the clinical predictive values of baseline demographic, clinical and laboratory parameters we observed for over a median of 27.7 months of follow-up in the patients with ACS after PCI, univariate and multivariate Cox regression analysis were performed. Univariate Cox regression analysis reported that age and gender as well as baseline platelet (PLT) count, LYMPH count, EO count and EO % were positively correlated with the occurrence of HF in ACS patients following PCI, whereas mean corpuscular volume (MCV) and mean corpuscular hemoglobin (MCH) were negatively correlated with HF, over a 2-year follow-up (Table 3). Of note, EO count displayed significantly predictive value of HF in ACS patients after PCI (HR: 9.935, 95% CI: 2.136–46.215, P = 0.003).
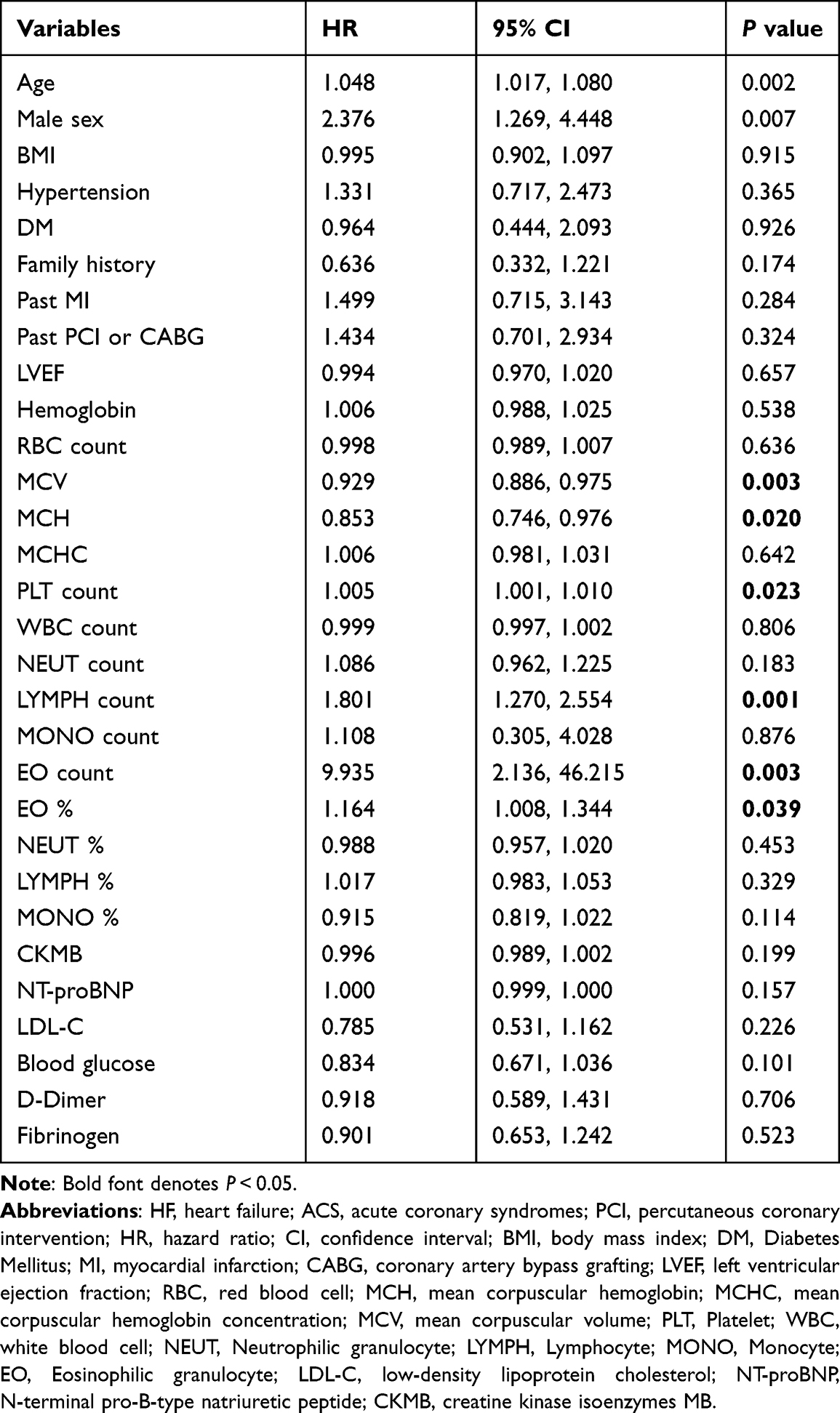 |
Table 3 Partial Univariate Cox Regression Analysis for Predictors of HF in ACS Patients Following PCI Over a 2-Year Follow-Up |
Based on the results of the univariate analysis, we then used multivariate analysis to further explain whether PLT count, LYMPH count, EO count and EO % could independently be in predictive value for HF. We selected the confounders according to variables’ associations with the outcomes of interest or a change in effect estimate of more than 10%. Multivariate analysis showed that PLT count had no value for prediction of HF in the patients with ACS after PCI. However, compared with crude regression analysis, the association between LYMPH count, EO count, EO % and the occurrence of HF were enhanced markedly even after adjusting for age, male sex, BMI, smoking, diabetes mellitus, past PCI or CABG, SBP, DBP and EF (Model 1), and further for red blood cell (RBC) count, MCV, WBC count, NEUT count, LYMPH %, MONO %, NT-proBNP, blood glucose and D-Dimer (Model 2), respectively, in the multivariable regression analysis (Table 4). Especially, the positive association of EO count was the most pronounced (Model 1: HR = 10.695, P = 0.007; Model 2: HR = 12.625, P = 0.004).
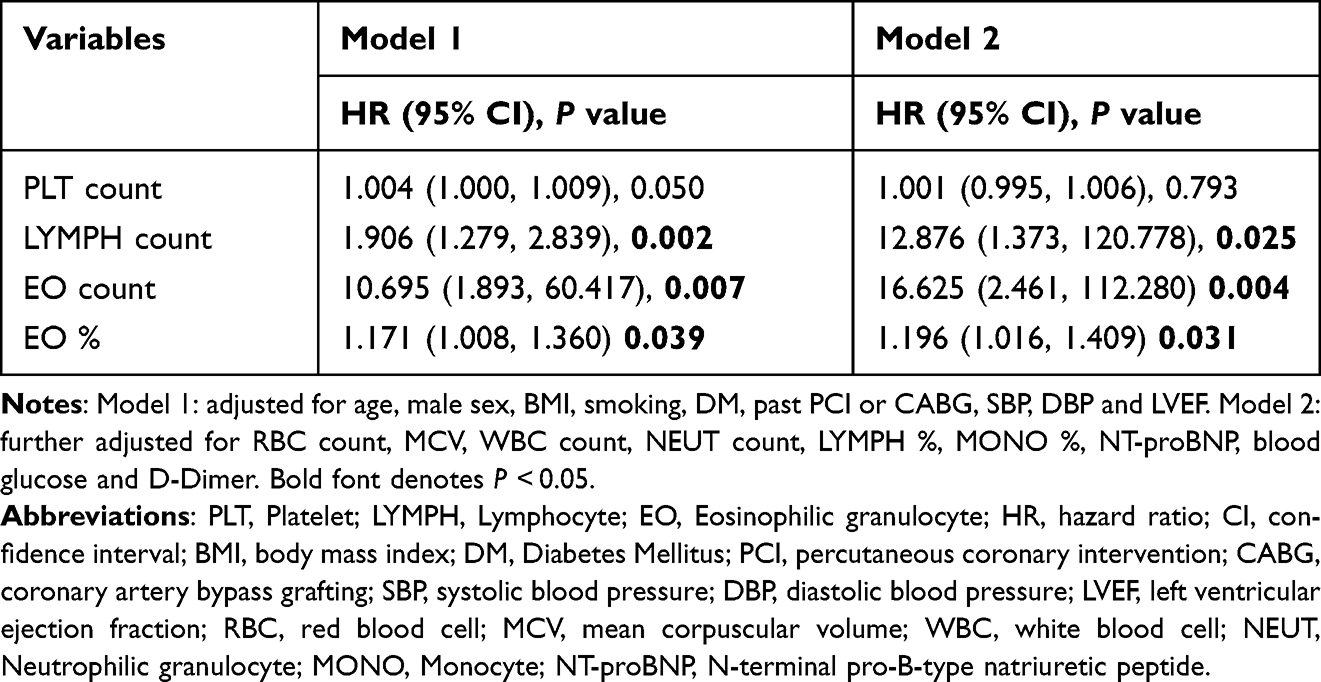 |
Table 4 Multivariate Cox Regression Analysis for PLT Count, LYMPH Count, EO Count and EO % |
Kaplan–Meier Survival Analysis
Next, we explored the respective values for predicting HF in subgroups with different LYMPH count, EO count and EO % levels. Patients were equally divided into two groups (low-level and high-level) based on LYMPH count, EO count and EO % levels. Kaplan–Meier survival analysis was conducted to determine the long-term prognostic value of LYMPH count, EO count and EO % in ACS patients following PCI. With a median follow-up of 27.7 months, our results showed that high-level EO count was significantly associated with increased incidence of HF (Figure 1A, Log rank test: P = 0.008). As can be seen from Supplementary Results, there were no statistically differences between high-level and low level of LYMPH count and EO % (Figure 1B and C), despite a similar trend with the result of Cox regression analysis based on the levels of LYMPH count, EO % (Supplementary Table 1).
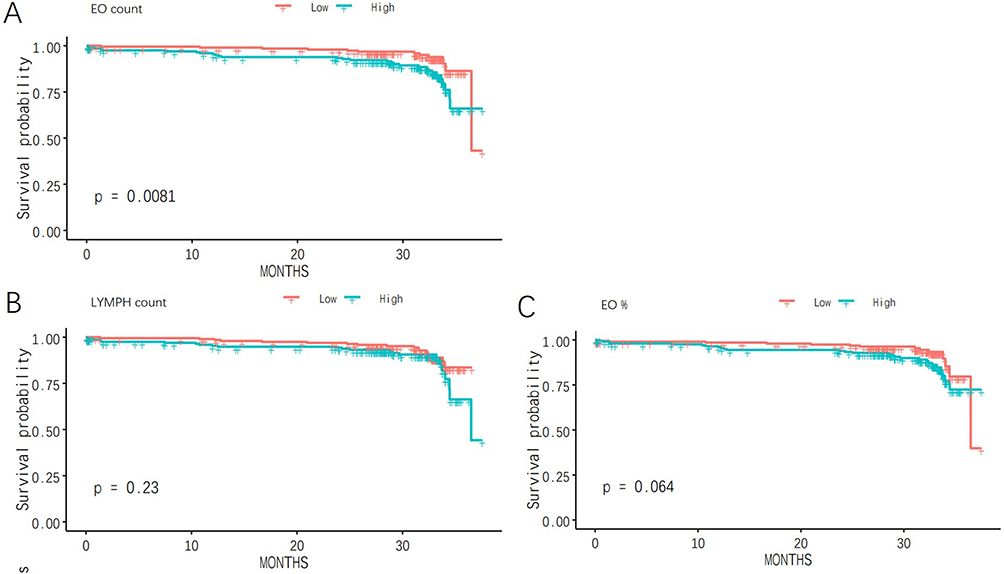 |
Figure 1 Kaplan-Meier survival analysis of the occurrence of HF based on EO count (A), LYMPH count (B), and EO% (C) levels (low-level and high-level) in ACS patients during the 2-year follow-up period. |
Stratified Cox Regression Analysis
Considering that LYMPH count, EO count and EO % levels are closely related to age, gender, history of smoking and hypertension, we conducted stratification analysis further (Table 5). Our results demonstrated that, compared to patients younger than 60 years, both LYMPH and EO counts had greater predictive power for HF in those older than 60 years (HR: 1.588 vs 2.099; 9.242 vs 31.328, respectively). Compared to non-smoker, LYMPH count showed a stronger capacity to predict HF in patients who had a smoking history (HR: 1.650 vs 2.091). Moreover, for patients who had PCI or CABG history, EO count was typically a stronger predictor for HF.
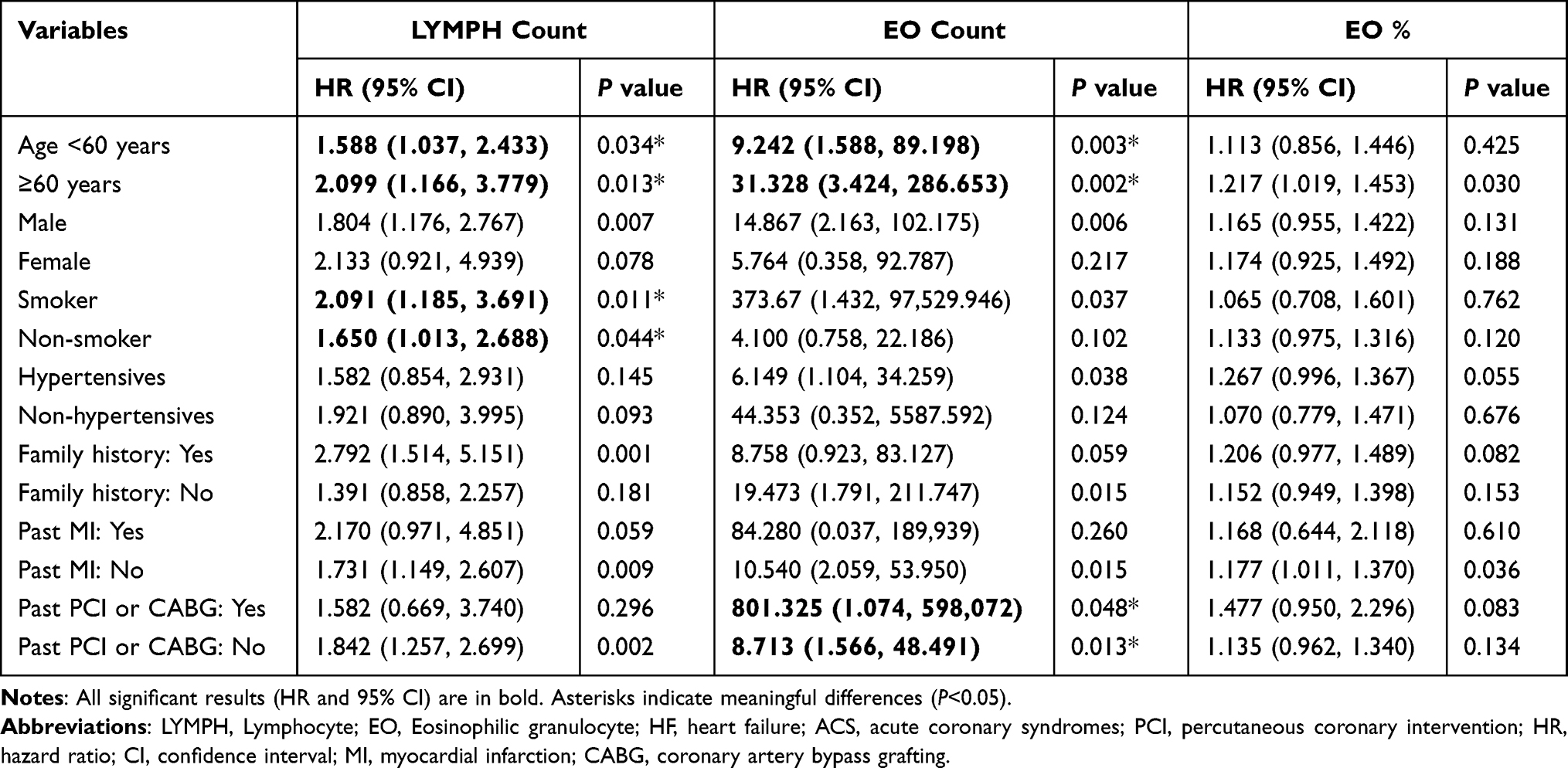 |
Table 5 Stratified Cox Regression Analysis for LYMPH Count, EO Count and EO % in Predicting of HF in ACS Patients Following PCI Over a 2-Year Follow-Up |
Receiver-Operating Characteristic (ROC) Curve Analysis
The AUCs of LYMPH count, EO count and EO % for predicting the occurrence of HF in ACS patients after PCI over a 2-year follow-up are shown in Table 6. The AUC of EO count was 0.625 (P = 0.037), with a sensitivity of 0.705 and a specificity of 0.575. The ROC curves of EO count as a marker to predict HF in ACS patients after PCI are illustrated in Figure 2A.
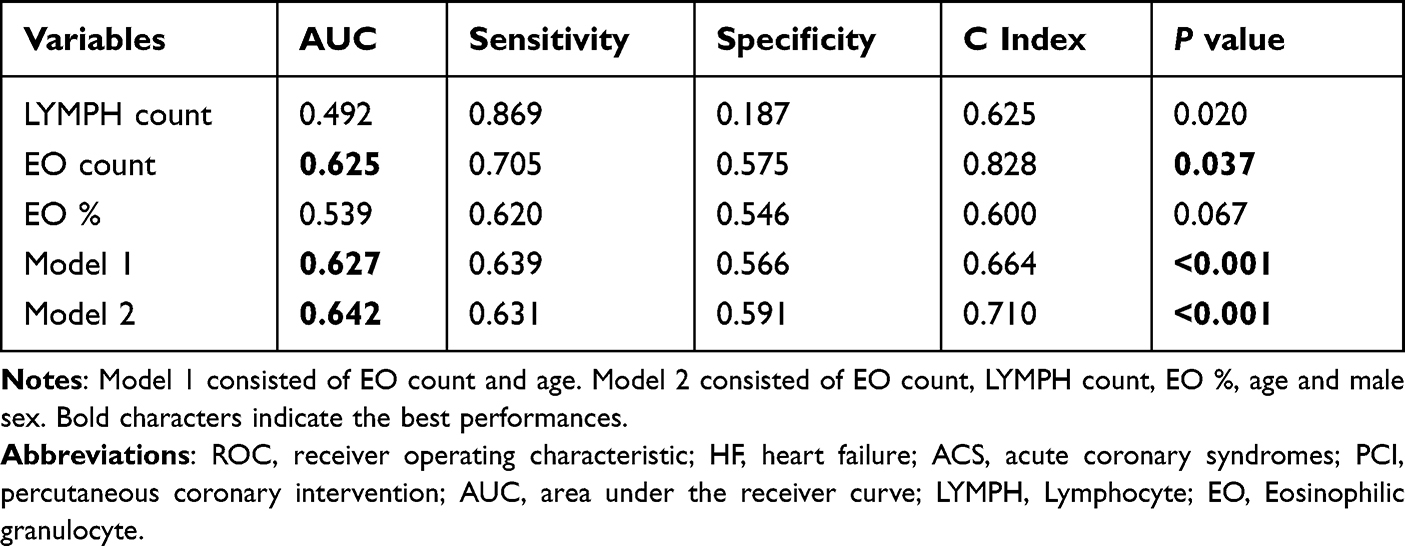 |
Table 6 ROC Analysis for Predicting the Occurrence of HF in ACS Patients Following PCI Over a 2-Year Follow-Up |
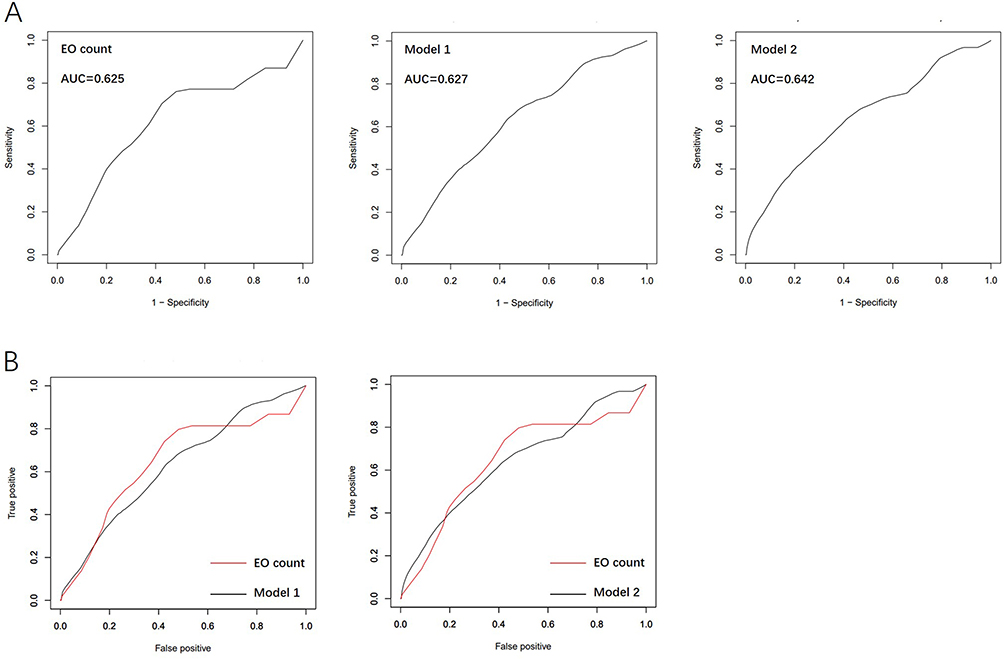 |
Figure 2 Receiver-operating characteristic (ROC) curve analysis. (A) ROC curve analysis of EO count, Model 1 and Model 2 (Model 1: EO count combined with age; Model 2: EO count combined with LYMPH count, EO %, age and gender) in ACS patients following PCI over a 2-year follow-up. (B) Comparisons of the ROC curve of EO count and ROC curves of model 1 or model 2, respectively. |
To find the best predictive index for HF, we next evaluated various combinations of these four blood cell indices with age and gender. The results revealed that only two of these combinations (Model 1 and Model 2) were found to have statistical significance. The AUC of EO count combined with age (Model 1) was 0.627 (P < 0.001), and the AUC of EO count combined with LYMPH count, EO %, age and gender (Model 2) was 0.642 (P < 0.001), which were higher than that of each blood cell index. Regrettably, no difference between ROC curve of EO count and ROC curve of model 1 was observed neither ROC curve of EO count and ROC curve of model 2 (Figure 2B). In a word, the combinations were not more valuable than EO count alone. EO count had a high long-term prognostic value in the parameters observed.
Discussion
We conducted this study, enrolling 416 ACS patients after PCI and making follow-up (the median follow-up time was 27.7 months), to explore the clinical predictive values of WBC indices (LYMPH and EO) for the occurrence of HF. The results indicated that LYMPH count, EO count and EO % were higher in ACS patients who suffered HF. Secondly, LYMPH count, EO count and EO % were independent predictors for HF in patients with ACS undergoing PCI over a 2-year of prospective observation, even after adjustment for potential confounding factors. Of these, for smokers aged 60 years and above, who had PCI or CABG history, the higher EO count, the higher the incidence of HF. Furthermore, EO count had highest long-term prognostic value among all the parameters we observed. To the best of our knowledge, this study is the first time to uncover the relationship between EO count and EO % and 2-year adverse cardiovascular events in ACS patients after PCI in China.
Our data are important as they uncover the causal relationships to provide the supplementation that earlier observational studies have reported, indicating associations between peripheral WBC and HF. In our previous studies,14 we have reported that MCV and MCH, two of the RBC indices included in routine blood examination which is widely used in clinic, related to increased long-term major adverse cardiovascular events (MACEs) in ACS patients. The results combined with our present data, which displayed high value of RBC and WBC indices, help to highlight the potential importance of routine blood examination, the most basic but most easily ignored laboratory examination.
Although an orchestrated and strongly controlled immune response is a novel step for an adequate repair of the infarcted myocardium, a deregulated and excessive activation of the immune response leading to inflammatory cascade has been demonstrated to mediate myocardial damage and in turn associated with worse clinical outcomes in ACS patients.12,15 Traditionally, WBC count determined by blood routine examination has been used as a biomarker to explore the association. Of these, neutrophil, monocyte, lymphocyte and, more recently, eosinophils cell counts have been gradually gained considerable attention.16 As an important effector of immune system, T lymphocyte-mediated immune response has a vital role in the progression of cardiovascular disease.17,18 In congestive HF, autoreactive T helper (Th) cells with specificity for an antigen expressed in cardiomyocytes can promote the progression from hypertrophy to HF in response to pressure overload, and the activation of the immune system leads to increased production and release of proinflammatory cytokines.16 Patients with congestive HF show increased pro-inflammatory CD4+ Th1 and Th17 cells, as well as lower anti-inflammatory T regulatory cells (Treg), and these features are related to disease severity.19 In chronic ischemic cardiomyopathy, systemic expansion of CD4+ and CD8+ T lymphocyte and CD4+ Th1, Th2, Th17, and Treg subsets can be found in the heart, circulation, and lymphoid organs. Moreover, various studies have shown that T lymphocytes play an important role in the progression of cardiac remodeling after MI.16 In addition, CD4/CD28-null T cells are observed to accumulate preferentially in unstable ruptured coronary plaques and have been suggested to promote plaque instability, which predisposes ACS patients to recurrent acute coronary events and indicates a poor prognosis.20 At the same time, we have observed a correlation between lymphocyte count and HF in ACS patients. The results of the current study indicate that baseline lymphocyte count is an independent predictor of HF in patients with ACS undergoing percutaneous coronary intervention (PCI) over a 2-year period of prospective observation, even after adjustment for potential confounding factors. Thus, our findings provide pathophysiological insights into the development of HF, and reducing T lymphocyte infiltration in ACS patients may be a necessary translational target in the treatment of HF, albeit after immediate revascularization and antithrombotic strategies. At the same time, we have observed relations between lymphocyte and HF in ACS patients. The result in the current study indicated that baseline LYMPH count was independent predictors for HF in patients with ACS undergoing PCI over a 2-year of prospective observation, even after adjustment for potential confounding factors. Thus, our findings provide pathophysiological insight into the development of HF, and the reduction of T lymphocyte infiltration in ACS patients may be a necessary translational target in HF although after immediate revascularisation and antithrombotic strategies.
Compared to other inflammatory parameters, eosinophil was seldom discussed, although the routine blood examination is a frequently used measure of immune responses in ACS patients. Cardiovascular manifestations of hyper-eosinophilic syndrome are the main cause of morbidity and mortality in the uncommon disorder, eosinophilic cardiomyopathy.21 The toxic effects of eosinophil cells in the pathophysiology of eosinophilic cardiomyopathy have been demonstrated. Pathological observations of the patients’ hearts with sustained eosinophilia illustrate that both ventricles may be affected by the infiltration of eosinophil cells in the interstitial compartment, which is deleterious to cardiac tissue and associated with thickening of LV wall, fibrosis of the endocardium, thrombus formation, vasculitis, and myocardial necrosis.22,23 In recent years, emerging findings of eosinophils in cardiovascular diseases are focus on its effect on regulating the inflammation progress. Eosinophils act an important role in the initiation, progression, and rupture of thrombus.24 For instance, the infiltration of eosinophils into the infarcted myocardial area is involved in atherosclerotic plaque rupture, a basic inflammatory pathogenesis of ACS. Eosinophils help platelets adhering to the injured vessel wall and secondary releasing cytokines such as interleukin (IL)-4, IL-10, and IL-13 which are suggested to modulate the inflammatory response.25 Similar to our findings, some studies have reported that a higher EO count is associated with a higher risk of cardiac events after MI. For instance, Jiang concluded that circulatory eosinophils reflected the extent of MI.26 Besides, study from Toor et al showed that augmented eosinophil count was associated with a higher death risk at long-term follow-up, and eosinophils were found to be a useful biomarker for risk stratification of CAD patients and predicting mortality.27 However, Shiyovic et al found that increased circulating EO count after admission in ST-elevation myocardial infarction (STEMI) patients had association with a lower risk of death over 1-year follow-up.28 Furthermore, since the single inflammatory cell is unable to not representative of the overall systematic inflammation, new indexes are proposed by combining different subtypes of WBC indices. For instance, eosinophil to leukocyte ratio was reported to be independently associated with MACEs in STEMI patients following PCI.29 The authors urged that study methodology, study period or different cohorts may account for these discrepancies between studies. Our results, obtained in a homogeneous group of ACS patients undergoing PCI, suggesting an association between increased peripheral EO count after admission with high risk of the incidence of HF. The last but not least, stratified Cox regression analysis for EO count indicated that, when compared to ACS patients younger than 60 years, both LYMPH and EO counts had greater predictive power for HF in those older than 60 years, what is more, ROC curve analysis demonstrated that the combinations of EO count with patient’ age had a higher long-term prognostic value for HF. These findings could be incorporated into our daily armamentarium to improve risk stratification of ACS patients.
Overall, WBC count is a new risk factor and biomarker for the development of HF; importantly, in contrast to IL-6, tumor necrosis factor-α, and high-sensitive C-reactive protein, WBC count is established as a routine laboratory parameter in clinical practice. First, our results further support WBC indices as strong independent risk factors for HF in ACS patients, even after PCI, which warrants evaluation as a target for intervention not only in manifest HF but also in prevention. Second, we add evidence suggesting the differences in age and gender in the development of HF, which might have implications for future trials on preventive interventions targeting inflammatory process. Additionally, we suggest high eosinophils count as a novel risk factor of HF which warrants further study in human population and animal model.
Limitation
(1) The current study was a single-center study with a small sample size limited to ACS patients following PCI from China. A larger cohort from more-centre and different populations would be needed to further refine our findings. (2) The duration of follow-up was likely too short that a longer follow-up visit is needed to further clarify the influence of the WBC indices on long-term prognoses. (3) There may be other possible factors which might have impacts on the outcomes but have not been adjusted. (4) Due to missing data of basophil count and percentage, statistical analyses were not performed. Further investigation in terms of basophil count is required to extend our findings.
Conclusion
Elevated baseline LYMPH count, EO count and EO % measured by routine blood examination were independently associated with the risk of heart failure in ACS patients following PCI, suggesting that WBC indices might be available, simple, and cost-efficient biomarkers with predictive values, and be worthy of further exploration of the underlying mechanism. As standard and easily obtained, parameters from routine blood examination could provide the possibility to help clinicians to identify high-risk patients, predict the long-term clinical outcomes, and optimize clinical decisions, especially for patients aged more than 60 years.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author Juan Zhou (Email: [email protected]) on reasonable request.
Ethics Approval and Consent to Participate
Approval of the Ethics Committee of Xi’an Jiaotong University (Ethical approval number: XJTU1AF2012LSK-312) was obtained, and the written informed consents were obtained from all the participants. The study conformed to the Declaration of Helsinki and collected the required data from the clinical records without clinical intervention to protect patients’ privacy.
Acknowledgments
We sincerely thank the participating hospitals, patients, their families and colleagues who have provided valuable suggestions for this study.
Funding
This work was supported by the National Key Research and Development Program of China [2021YFA1301200, 2019YFA0802300], and the National Natural Science Foundation of China [81800446].
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Bergmark BA, Mathenge N, Merlini PA, Lawrence-Wright MB, Giugliano RP. Acute coronary syndromes. Lancet. 2022;399(10332):1347–1358. doi:10.1016/S0140-6736(21)02391-6
2. Benjamin EJ, Virani SS, Callaway CW, et al. Heart disease and stroke statistics-2018 update: a report from the American Heart Association. Circulation. 2018;137(12):e67–e492. doi:10.1161/CIR.0000000000000558
3. Shen C, Ge J. Epidemic of cardiovascular disease in china: current perspective and prospects for the future. Circulation. 2018;138(4):342–344. doi:10.1161/CIRCULATIONAHA.118.033484
4. Libby P, Loscalzo J, Ridker PM, et al. Inflammation, immunity, and infection in atherothrombosis: JACC review topic of the week. J Am Coll Cardiol. 2018;72(17):2071–2081. doi:10.1016/j.jacc.2018.08.1043
5. Engelmann B, Massberg S. Thrombosis as an intravascular effector of innate immunity. Nat Rev Immunol. 2013;13(1):34–45. doi:10.1038/nri3345
6. De Luca G, Verdoia M, Suryapranata H. Benefits from intracoronary as compared to intravenous Abciximab administration for STEMI patients undergoing primary angioplasty: a meta-analysis of 8 randomized trials. Atherosclerosis. 2012;222(2):426–433. doi:10.1016/j.atherosclerosis.2012.02.041
7. Heymans S, Hirsch E, Anker SD, et al. Inflammation as a therapeutic target in heart failure? A scientific statement from the Translational Research Committee of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2009;11(2):119–129. doi:10.1093/eurjhf/hfn043
8. Pfister R, Sharp SJ, Luben R, Wareham NJ, Khaw KT. Differential white blood cell count and incident heart failure in men and women in the EPIC-Norfolk study. Eur Heart J. 2012;33(4):523–530. doi:10.1093/eurheartj/ehr457
9. Bekwelem W, Lutsey PL, Loehr LR, et al. White blood cell count, C-reactive protein, and incident heart failure in the Atherosclerosis Risk in Communities (ARIC) Study. Ann Epidemiol. 2011;21(10):739–748. doi:10.1016/j.annepidem.2011.06.005
10. Rana JS, Boekholdt SM, Ridker PM, et al. Differential leucocyte count and the risk of future coronary artery disease in healthy men and women: the EPIC-Norfolk prospective population study. J Intern Med. 2007;262(6):678–689. doi:10.1111/j.1365-2796.2007.01864.x
11. Forteza MJ, Trapero I, Hervas A, et al. Apoptosis and mobilization of lymphocytes to cardiac tissue is associated with myocardial infarction in a reperfused porcine model and infarct size in post-PCI patients. Oxid Med Cell Longev. 2018;2018:1975167. doi:10.1155/2018/1975167
12. Husser O, Bodi V, Sanchis J, et al. White blood cell subtypes after STEMI: temporal evolution, association with cardiovascular magnetic resonance--derived infarct size and impact on outcome. Inflammation. 2011;34(2):73–84. doi:10.1007/s10753-010-9209-0
13. Zhang L, Xu C, Liu J, et al. Baseline plasma fibrinogen is associated with haemoglobin A1c and 2-year major adverse cardiovascular events following percutaneous coronary intervention in patients with acute coronary syndrome: a single-centre, prospective cohort study. Cardiovasc Diabetol. 2019;18(1):52. doi:10.1186/s12933-019-0858-5
14. Zhang Z, Gao S, Dong M, et al. Relationship between red blood cell indices (MCV, MCH, and MCHC) and major adverse cardiovascular events in anemic and nonanemic patients with acute coronary syndrome. Dis Markers. 2022;2022:2193343. doi:10.1155/2022/2193343
15. Tamhane UU, Aneja S, Montgomery D, Rogers EK, Eagle KA, Gurm HS. Association between admission neutrophil to lymphocyte ratio and outcomes in patients with acute coronary syndrome. Am J Cardiol. 2008;102(6):653–657. doi:10.1016/j.amjcard.2008.05.006
16. Strassheim D, Dempsey EC, Gerasimovskaya E, Stenmark K, Karoor V. Role of inflammatory cell subtypes in heart failure. J Immunol Res. 2019;2019:2164017. doi:10.1155/2019/2164017
17. Kallikourdis M, Martini E, Carullo P, et al. T cell costimulation blockade blunts pressure overload-induced heart failure. Nat Commun. 2017;8:14680. doi:10.1038/ncomms14680
18. Gröschel C, Sasse A, Monecke S, et al. CD8(+)-T cells with specificity for a model antigen in cardiomyocytes can become activated after transverse aortic constriction but do not accelerate progression to heart failure. Front Immunol. 2018;9:2665. doi:10.3389/fimmu.2018.02665
19. Zhao RX, Li WJ, Lu YR, et al. Increased peripheral proinflammatory T helper subsets contribute to cardiovascular complications in diabetic patients. Mediators Inflamm. 2014;2014:596967. doi:10.1155/2014/596967
20. Dumitriu IE. The life (and death) of CD4+ CD28(null) T cells in inflammatory diseases. Immunology. 2015;146(2):185–193. doi:10.1111/imm.12506
21. Ogbogu PU, Rosing DR, Horne MK. Cardiovascular manifestations of hypereosinophilic syndromes. Immunol Allergy Clin North Am. 2007;27(3):457–475. doi:10.1016/j.iac.2007.07.001
22. Diny NL, Baldeviano GC, Talor MV, et al. Eosinophil-derived IL-4 drives progression of myocarditis to inflammatory dilated cardiomyopathy. J Exp Med. 2017;214(4):943–957. doi:10.1084/jem.20161702
23. Cheung CC, Constantine M, Ahmadi A, Shiau C, Chen LYC. Eosinophilic Myocarditis. Am J Med Sci. 2017;354(5):486–492. doi:10.1016/j.amjms.2017.04.002
24. Marx C, Novotny J, Salbeck D, et al. Eosinophil-platelet interactions promote atherosclerosis and stabilize thrombosis with eosinophil extracellular traps. Blood. 2019;134(21):1859–1872. doi:10.1182/blood.2019000518
25. Jacobsen EA, Taranova AG, Lee NA, Lee JJ. Eosinophils: singularly destructive effector cells or purveyors of immunoregulation? J Allergy Clin Immunol. 2007;119(6):1313–1320. doi:10.1016/j.jaci.2007.03.043
26. Jiang P, Wang DZ, Ren YL, Cai JP, Chen BX. Significance of eosinophil accumulation in the thrombus and decrease in peripheral blood in patients with acute coronary syndrome. Coron Artery Dis. 2015;26(2):101–106. doi:10.1097/MCA.0000000000000186
27. Toor IS, Jaumdally R, Lip GY, Millane T, Varma C. Eosinophil count predicts mortality following percutaneous coronary intervention. Thromb Res. 2012;130(4):607–611. doi:10.1016/j.thromres.2012.05.033
28. Shiyovich A, Gilutz H, Plakht Y. White blood cell subtypes are associated with a greater long-term risk of death after acute myocardial infarction. Texas Heart Insti J. 2017;44(3):176–188. doi:10.14503/THIJ-16-5768
29. Konishi T, Funayama N, Yamamoto T, et al. Prognostic value of eosinophil to leukocyte ratio in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. J Atheroscler Thromb. 2017;24(8):827–840. doi:10.5551/jat.37937
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nitroglycerin Use in the Emergency Department: Current Perspectives
Twiner MJ, Hennessy J, Wein R, Levy PD
Open Access Emergency Medicine 2022, 14:327-333
Published Date: 9 July 2022
Evaluation of Health Literacy Levels and Associated Factors Among Patients with Acute Coronary Syndrome and Heart Failure in Qatar
Elbashir M, ElHajj MS, Rainkie D, Kheir N, Hamou F, Abdulrhim S, Mahfouz A, Alyafei S, Awaisu A
Patient Preference and Adherence 2023, 17:89-105
Published Date: 7 January 2023
Acute Cardiovascular Events After COVID-19 in England in 2020: A Self-Controlled Case Series Study

Davidson JA, Banerjee A, Strongman H, Herrett E, Smeeth L, Breuer J, Warren-Gash C
Clinical Epidemiology 2023, 15:911-921
Published Date: 1 September 2023
Predictive Role of White Blood Cell Differential Count for the Development of Acute Exacerbation in Korean Chronic Obstructive Pulmonary Disease
Yoon EC, Koo SM, Park HY, Kim HC, Kim WJ, Kim KU, Jung KS, Yoo KH, Yoon HK, Yoon HY
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:17-31
Published Date: 4 January 2024