Back to Journals » Journal of Inflammation Research » Volume 19
The Predictive Value of Nomogram Model Based on Neutrophil-to-Lymphocyte Ratio (NLR) and Prothrombin Time-International Normalized Ratio (PT-INR)-to-Albumin Ratio (PTAR) for Early Bacterial Intra-Abdominal Infection After Orthotopic Liver Transplantation
Authors Peng HB ![]() , Liu Y
, Liu Y ![]() , Hou F, Zhao S
, Hou F, Zhao S ![]() , Zhang YZ
, Zhang YZ ![]() , He ZY, Cui TT, Liu JY, Xiong HF
, He ZY, Cui TT, Liu JY, Xiong HF ![]() , Sun LY
, Sun LY
Received 7 October 2025
Accepted for publication 10 December 2025
Published 9 January 2026 Volume 2026:19 571498
DOI https://doi.org/10.2147/JIR.S571498
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Fatih Türker
Hua-Bin Peng,1 Ying Liu,1 Fei Hou,1 Shuang Zhao,1 Yi-Zhi Zhang,1 Zhi-Ying He,1 Ting-Ting Cui,1 Jing-Yi Liu,1 Hao-Feng Xiong,1 Li-Ying Sun1– 5
1Department of Critical Liver Diseases, National Clinical Research Center for Digestive Diseases, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Liver Transplantation Center, National Clinical Research Center for Digestive Diseases, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 3Beijing Key Laboratory of Organ Cultivation and Organ Protection in Transplantation, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 4State Key Laboratory of Digestive Health, Beijing, People’s Republic of China; 5Laboratory for Clinical Medicine, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Li-Ying Sun, Department of Critical Liver Diseases, Beijing Friendship Hospital, Capital Medical University, Number 101, Luyuan East Road, Tongzhou District, Beijing, 101100, People’s Republic of China, Email [email protected] Hao-Feng Xiong, Department of Critical Liver Diseases, Beijing Friendship Hospital, Capital Medical University, Number 101, Luyuan East Road, Tongzhou District, Beijing, 101100, People’s Republic of China, Email [email protected]
Purpose: To identify risk factors for bacterial intra-abdominal infections (IAIs) after orthotopic liver transplantation (OLT) and establish a nomogram prediction model based on preoperative neutrophil-to-lymphocyte ratio (NLR) and preoperative prothrombin time-international normalized ratio (PT-INR)-to-albumin ratio (PTAR).
Patients and Methods: We retrospectively analyzed 261 patients who received OLT between January 2020 and April 2024 in Beijing Friendship Hospital. Independent risk factors for bacterial IAIs within 30 days postoperatively were identified by logical regression analysis. The area under the receiver operating characteristic (ROC) curve (AUC) was calculated to evaluate the predictive performance of NLR and PTAR as well as the nomogram model based on them. Hepatic function was evaluated using the Child–Turcotte–Pugh (CTP) score and the Model for End-Stage Liver Disease (MELD) score.
Results: Fifty patients (19.2%, 50/261) developed postoperative bacterial IAIs. The majority of the 66 isolated strains were gram-negative (63.6%). Most infections (74.0%, 37/50) occurred within two weeks postoperatively. Multivariate logistic regression analysis identified preoperative NLR, preoperative PTAR, acute physiology and chronic health evaluation II (APACHE II) score, and biliary leakage as independent risk factors. A nomogram-based prediction model was constructed utilizing the identified independent risk factors. Internal validation was conducted through the bootstrap method. The Hosmer–Lemeshow test indicated no significant deviation from the goodness-of-fit (χ2 = 7.349, P = 0.499 > 0.05). The calibration curve indicated excellent concordance between predicted and observed outcomes. The nomogram exhibited strong discriminative capability, evidenced by a C-index of 0.900 (95% CI: 0.828– 0.972) and an AUC of 0.912 (95% CI: 0.864– 0.960) for predicting abdominal infection, with an optimal diagnostic threshold of 0.221 (95% CI: 0.125– 0.265). Decision curve analysis revealed a positive net benefit across a wide range of threshold probabilities (0.03– 1.0), indicating the model’s substantial clinical utility.
Conclusion: Both the preoperative NLR and the preoperative PTAR are independent risk factors for IAIs within 30 days after OLT. The nomogram model based on NLR and PTAR can effectively predict the occurrence of IAIs after OLT.
Keywords: orthotopic liver transplantation, intra-abdominal infection, neutrophil-to-lymphocyte ratio, international normalized ratio-to-albumin ratio, nomogram model
Corrigendum for this paper has been published.
Introduction
Orthotopic liver transplantation (OLT) is the primary and most efficacious therapeutic modality for individuals with end-stage liver diseases.1 In recent years, significant improvements in both short-term and long-term prognoses for transplant recipients and their grafts have been observed, attributable to advancements in organ transplantation technology, the introduction of novel immunosuppressive agents, and continuous refinement of perioperative management.2 Nevertheless, the incidence of early postoperative infections (≤1 month) remains as high as 23.3%-71.4%,3–5 significantly affecting patient prognosis.6 Bacterial intra-abdominal infections (IAIs) are the most prevalent infectious complication during the initial month after liver transplantation, and represent a significant factor contributing to patient mortality.7 Simultaneously, as a result of immunosuppressive therapy, transplant recipients face an elevated risk of contracting multidrug-resistant bacterial infections.3 In the event that such infections occur, mortality rates can rise to as high as 40%,8 posing a significant challenge to clinical management. The risk factors associated with infections after liver transplantation are multifaceted. Empirical studies have indicated that the activation of the inflammatory system, coupled with dysregulation of immune responses, plays a significant role in the onset and progression of infectious complications post-transplantation.9,10 The neutrophil-to-lymphocyte ratio (NLR) is a common inflammatory indicator in clinical practice,11 playing an important role in the immune response.12 In recent years, NLR has gained recognition as a potential predictor of a variety of infections.13–15 Within the domain of liver transplantation, three studies16–18 have consistently indicated that an elevated NLR is significantly correlated with the incidence of postoperative infections. Wiegand18 illustrated that NLR was markedly elevated at the onset of infection. In contrast, Umman16 and Yu17 observed that the NLR in the infected group was already significantly higher compared to the non-infected group prior to the onset of infection. Overall, research on the NLR as a prognostic indicator for early postoperative infection after liver transplantation is currently insufficient. To substantiate the reliability of existing results and to assess its potential synergistic application with other biomarkers for improved clinical utility, further comprehensive studies are necessary.
The prothrombin time-international normalized ratio (PT-INR)-to-albumin ratio (PTAR) is a marker of hepatic synthetic function, systemic nutritional status, and overall immune resistance.19 Empirical research shows that raised PTAR correlates with an elevated risk of adverse outcomes in individuals undergoing hepatectomy for hepatic carcinoma.19 Furthermore, patients with end-stage liver disease who are candidates for liver transplantation frequently present with hepatic insufficiency and diminished hepatic reserve, a condition substantiated by numerous studies to increase vulnerability to infections.20–22 Abnormalities in albumin (ALB) and INR have been extensively documented in patients experiencing infections after liver transplantation.6,23,24 Based on these observations, we hypothesize that PTAR is a valuable predictor for the occurrence of infections post-liver transplantation. Nevertheless, to date, no studies have specifically investigated the predictive value of PTAR for post-liver transplantation infections.
In this study, we analyzed the clinical data of 261patients who underwent OLT to assess the predictive value of preoperative NLR and preoperative PTAR for early postoperative bacterial IAIs. Utilizing preoperative NLR and preoperative PTAR alongside other clinically relevant indicators identified through multivariate analysis, a nomogram-based prediction model was developed. This model aims to facilitate the early identification of infections, enhancing patient outcomes and survival rates.
Materials and Methods
Study Population
This study retrospectively examined a cohort of 261 patients admitted to the Liver Transplantation Center in Beijing Friendship Hospital between January 2020 and April 2024, who experienced bacterial IAIs within 30 days post-liver transplantation. The decision to adopt a retrospective study design was driven by the research objective of identifying multiple risk factors associated with postoperative IAIs and exploring the relationship between preoperative NLR, preoperative PTAR, and the occurrence of postoperative IAIs.The inclusion criteria were as follows: (1) age ≥ 18 years; (2) both anesthesia and surgical procedures were conducted by the same medical team; and (3) postoperative immunosuppressive therapy was administered. The exclusion criteria were as follows: (1) preoperative concurrent infections; (2) donor-derived infections; (3) multiple organ transplantation; (4) postoperative fungal intra-abdominal infections; (5) Infusion of blood, albumin, plasma, fibrinogen or cryoprecipitate within 1 week before liver transplantation; (6) competing deaths within 30 days after the surgery; (7) incomplete follow-ups; (8) patient withdrawals and/or (9) incomplete clinical data. The patient selection flowchart is shown in Figure 1.
 |
Figure 1 Patient Selection Flowchart. |
Preoperative Infection Screening in Recipients
All patients were subjected to comprehensive preoperative infection screening to detect both overt and covert infections. The diagnostic process employs an integrative approach that synthesizes clinical symptoms, physical examination findings, and imaging results, augmented by pathogen-specific detection techniques such as molecular diagnostics, microbial culture, and metagenomic next-generation sequencing (mNGS).
To enhance the detection of occult infections, we systematically monitor the recipient’s inflammatory markers, conduct comprehensive whole-body imaging, and routinely perform PCR testing for respiratory viruses. Additionally, we carry out antibody detection for Epstein-Barr virus (EBV) and cytomegalovirus (CMV) in blood, alongside microbiological cultures of samples including anal swabs, sputum, ascites, and bile,etc. After a thorough screening process, 24 patients who showed evidence of infection were excluded from the study (Figure 1).
Formulation of the Immunosuppressive Regimen
All patients received or did not receive basiliximab for immune induction based on their individual clinical conditions. All patients received postoperative immunosuppressive therapy. The postoperative immunosuppressive regimen predominantly included the following drugs: (1) Tacrolimus (FK506), initiated at a dosage of 0.05–0.1 mg/kg/day, with subsequent adjustments based on target blood concentrations at designated intervals, or Cyclosporine A (CsA), initiated at a dosage of 6–8 mg/kg/day, with subsequent adjustments based on target blood concentrations at designated intervals; (2) Glucocorticoids(GCs), initially administered intravenously at 2–3 mg/kg/day, followed by a gradual tapering and transition to oral administration by postoperative day 7, maintaining a dosage of 5–10 mg/day; (3) Mycophenolic Acid (MPA), including Mycophenolate sodium(MPS), initiated at a dosage of 360–720mg per dose, with subsequent adjustments based on the patient’s clinical condition and (4) Mycophenolate mofetil(MMF), administration typically commences on the seventh day following surgery, with a standard dosage of 0.5–0.75 g per dose, twice daily.
Post-Operative Empirical Anti-Infective Regimen
As previously reported,3 all patients were administered standard prophylactic anti-infective therapy postsurgery. For the 184 recipients who received grafts from donation after brain death (DBD) or donation after circulatory death (DCD), the regimen generally consisted of a combination of meropenem/imipenem, vancomycin, and micafungin. For the 77 recipients who underwent living donor liver transplantation (LDLT), postoperative prophylaxis was achieved using third-generation cephalosporin antibiotics or carbapenem antibiotics.
Diagnostic Criteria for Bacterial IAI
Currently, there is no universally accepted gold standard for diagnosing bacterial IAIs within the context of liver transplantation. Drawing upon established guidelines25,26 and the clinical practice experience of our center, we propose the following diagnostic criteria for bacterial IAIs: 1. Postoperative clinical manifestations characterized by the acute onset of abdominal pain, in conjunction with both localized and systemic inflammatory indicators such as abdominal muscle rigidity, tenderness, rebound tenderness, fever, elevated white blood cell count, and abnormal increases in inflammatory markers, including C-reactive protein and procalcitonin, as well as tachycardia and/or tachypnea; 2. Positive microbial isolation and identification from intra-abdominal drainage fluid; 3. Imaging modalities, such as ultrasound or computed tomography (CT), revealing the presence of peritoneal effusion or intra-abdominal infectious foci.
Microbial Isolation and Identification Methods
The isolation and identification of microorganisms are typically performed using conventional culture methods. Prior to the procedure, the drainage tubes and orifices were disinfected. Under aseptic conditions, drainage fluid samples, with volumes ranging from 10 to 20 mL, were collected into 25 mL aerobic/anaerobic culture bottles. These samples were promptly transported to the microbiology laboratory for bacterial culture analysis. Bacterial cultures were incubated at 37°C using the BACTEC FT5790 fully automated blood culture system (Becton Dickinson, USA) along with its specific reagents. Subsequently, the BD Phoenix™ M50 microbial identification and antimicrobial susceptibility testing system (Becton Dickinson, USA) and its associated reagents were employed for analysis, isolation, identification, and evaluation of bacterial strains and their drug resistance.
Nonetheless, owing to the constraints inherent in conventional culture methods, certain patients with negative ascite cultures continue to present with distinct clinical manifestations or imaging features strongly indicative of IAIs. In these instances, mNGS is commonly utilized to ascertain the causative microorganisms. Prior to the procedure, the drainage tubes and orifices were disinfected. Under aseptic conditions, drainage fluid samples, with volumes ranging from 2 to 3 mL, were then sent to Jieyi Biotechnology (Hangzhou, China) for mNGS detection. Library preparation, metagenomic sequencing and mNGS reporting criteria were as described previously.3
In differentiating between microbial colonization and infection, our clinical experience suggests that pathogens isolated from sterile sites are typically indicative of infection. However, in patients who present with positive cultures but lack clinical signs of infection or do not exhibit positive findings on imaging, bacterial colonization is highly suspected. In these instances, we usually conduct repeated examinations of the drainage fluid, including routine ascite analysis and microbial culture, or to utilize mNGS to assist in distinguishing colonization from infection.
Data Collection and Analysis
The electronic medical record system of Beijing Friendship Hospital, Capital Medical University, was accessed to retrieve relevant clinical data. Preoperative clinical data for the following parameters were collected: gender, age, body mass index (BMI); underlying diseases; primary diseases; preoperative comorbidities; number of liver transplantations (initial transplantation versus retransplantation); severity of ascites prior to surgery; preoperative Model for End-Stage Liver Disease (MELD) score; and preoperative Child–Turcotte–Pugh (CTP) score.
The baseline laboratory indicators (24 hours prior to surgery) were as follows: white blood count (WBC), neutrophil count (NEU), lymphocyte count (LYM), platelet count (PLT), C-reactive protein (CRP), prothrombin time (PT), activated partial thromboplastin time (APTT), prothrombin activity (PTA), INR, alanine transaminase (ALT), aspartate transaminase (AST), gamma-glutamyl transpeptidase (GGT), alkaline phosphatase (AKP), total bilirubin (TBIL), albumin (ALB), blood ammonia (Amon), creatinine (Cr), serum sodium (Na), serum potassium (K), lactic acid (LA), glucose (GLU), triglyceride (TG), and total cholesterol (TC). All collected blood samples were transported to the laboratory by designated personnel within 30 minutes, adhering to the center’s standard operating procedures. Consistent analytical instrumentation was employed for the measurement of the index.
The following intraoperative clinical data were collected: the source of the donor liver, the surgical method, the biliary anastomosis method, the duration of the operative time and anhepatic phase, the graft-to-recipient weight ratio (GRWR), the volume of blood loss, the volumes of transfused red blood cell (RBC), plasma, and albumin, as well as the administration of immunomodulatory and vasoactive drugs during the surgical procedure.
The following postoperative clinical data were collected: immunosuppressive regimen,average levels of FK506 and CsA within 30 days, the administration of reduction or suspension of the immunosuppressants, the intensive care unit (ICU) stay duration, the APACHE II score assessed within the initial 24 hours following ICU admission, the abdominal drainage tube retention duration; and events occurring before the onset of IAI, including laparotomy, abdominal incision debridement and suture, and the administration of continuous renal replacement therapy (CRRT). Additionally, the dataset includes information on surgical complications occurring before the onset of IAI, such as intra-abdominal hemorrhage, bile leakage, colonic leakage, and biliary stricture. Furthermore, it provides detailed documentation of the incidence and timing of bacterial IAIs occurring within 30 days postsurgery, alongside the distribution of pathogens.
Univariate and multivariate logistic regression analyses were conducted to identify independent risk factors for bacterial IAIs occurring within 30 days postoperatively. We also explored the predictive value of NLR and PTAR for early bacterial IAIs after OLT and established a nomogram prediction model based on NLR and PTAR.
NLR and PTAR are indices derived from baseline laboratory indicators (24 hours prior to surgery) measurement. Specifically, NLR was determined by calculating the ratio of the neutrophil count to the lymphocyte count.11 In contrast, PTAR was defined as the prothrombin time-international normalized ratio (PT-INR) divided by the albumin concentration expressed in grams per deciliter (g/dL).19 The calculation formulas for CTP score, MLED score and APACHE II score were derived from relevant previous works.27–29 The term “retransplantation” denotes a subsequent liver transplantation procedure necessitated by functional failure of the initially transplanted liver.30
Statistical Methods
Statistical analysis was conducted using SPSS 27.0; GraphPad Prism 10 software was utilized for data visualization. The measurement data underwent a normality assessment. Data adhering to a normal distribution were presented as mean [SD], and comparisons between groups were conducted using the independent sample t-test. Data not conforming to a normal distribution were represented as median [interquartile range, IQR] with the Mann–Whitney U-test employed for intergroup comparisons. Categorical data were expressed as frequencies and percentages, and the χ2-test was utilized for group comparisons. Spearman correlation analysis was applied to evaluate the correlations between NLR, PTAR, MELD, and CTP scores. The predictive abilities of the NLR, PTAR, CTP score, MELD score, and APACHE II score to predict IAIs were assessed using the area under the ROC curve (AUC). The optimal cut-off values were identified employing the Youden index method. A multivariate logistic regression analysis was performed to ascertain the risk factors associated with the onset of IAIs within 30 days after OLT and a risk prediction nomogram for IAIs was constructed based on that. The nomogram’s calibration was evaluated using a calibration curve and the Hosmer-Lemeshow goodness-of-fit test. Bootstrap resampling was employed to determine the confidence interval and concordance index (C-index) at the optimal cut-off value, utilizing 1000 iterations. The model’s discriminative capacity was assessed using the AUC, while its clinical applicability was evaluated through decision curve analysis (DCA). A two-tailed p-value <0.05 was considered to indicate significant differences.
Results
Incidence and Pathogen Distribution of Bacterial IAIs Within 30 Days Postorthotopic Liver Transplantation
In a cohort of 261 patients who underwent OLT, 50 individuals (19.2%, 50/261) developed IAIs within 30 days postoperatively. A total of 66 bacterial strains were isolated from the IAI group. Gram-negative bacterial infections were the most prevalent, comprising 63.6% (42/66) of the isolates. Klebsiella pneumoniae (15.2%, 10/66), Acinetobacter baumannii (13.6%, 9/66), and Pseudomonas aeruginosa (7.6%, 5/66) were the most common gram-negative bacterial pathogens; Enterococcus faecium (15.2%, 10/66), Staphylococcus epidermidis (7.6%, 5/66), and Enterococcus faecalis (6.1%, 4/66) were the leading gram-positive bacterial pathogens (Table 1).
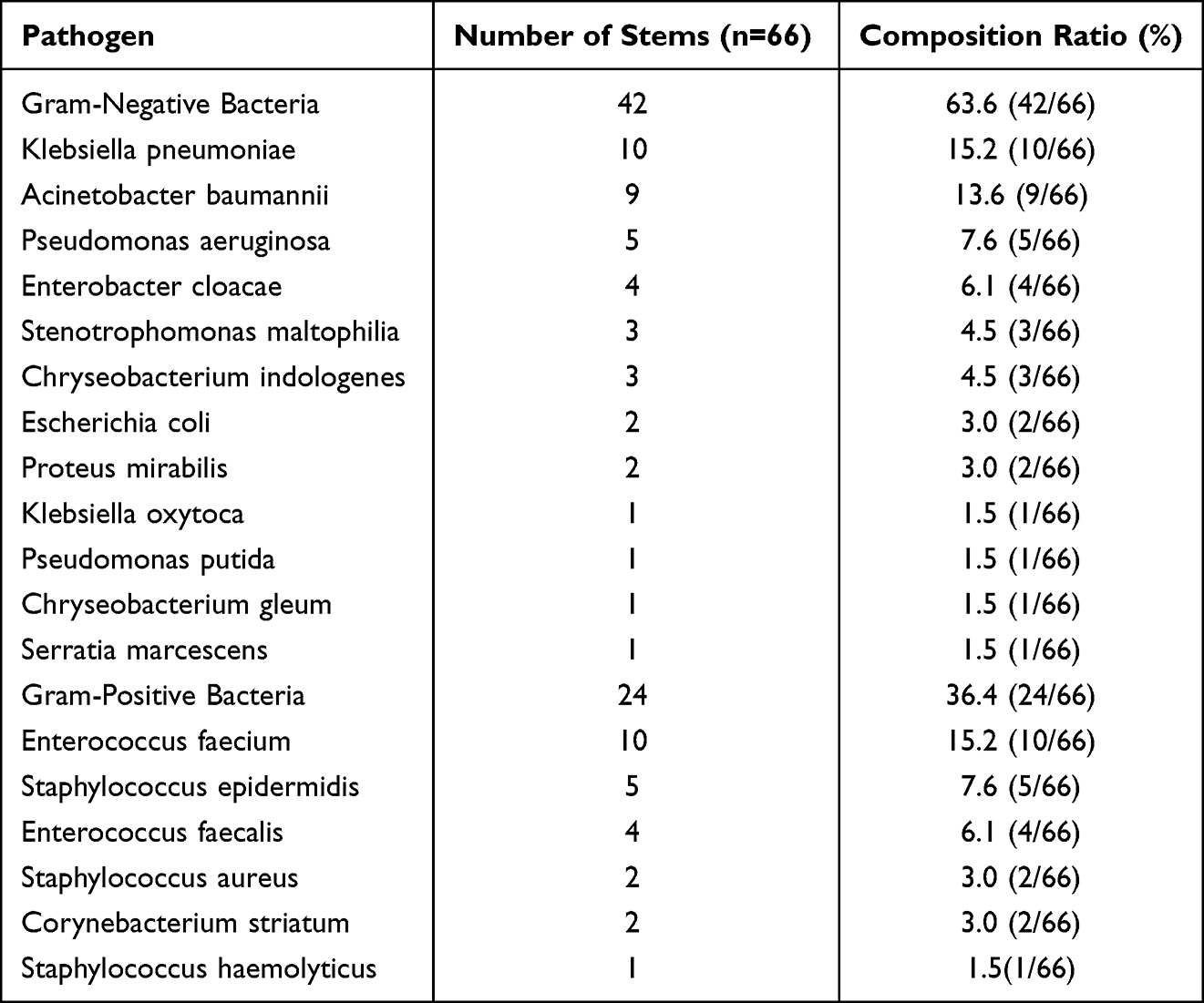 |
Table 1 Distribution of Pathogens Among Patients with Bacterial IAIs |
Temporal Distribution of Bacterial IAIs Postorthotopic Liver Transplantation
Among the cohort of 50 patients who experienced bacterial IAIs within 30 days after OLT, 22 patients (44.0%, 22/50) experienced infection onset within the first 1–7 days postoperation. 15 patients (30.0%, 15/50) experienced infections during the 8–14 day period postoperation. 9 patients (18.0%, 9/50) exhibited infection onset between 15–21 days postoperation, while the remaining 4 patients (8.0%, 4/50) experienced infection onset between 22–30 days postoperation. Statistical analysis indicates that the majority of infections, accounting for 74.0% (37/50) of all cases, occurred within the first two weeks after transplantation (Figure 2).
 |
Figure 2 Temporal Distribution of Bacterial IAIs. |
A Comparative Analysis of Preoperative, Intraoperative and Postoperative Indicators Between Patients with and without Bacterial IAIs
In comparison with the noninfection group, the IAI group exhibited significantly higher rates of retransplantation as well as increased incidences of preoperative moderate-to-severe ascites (all P < 0.05). No statistically significant differences were found between the two groups regarding gender; age; preoperative BMI; underlying diseases; primary disease types; preoperative complications (all P > 0.05) (Table 2).
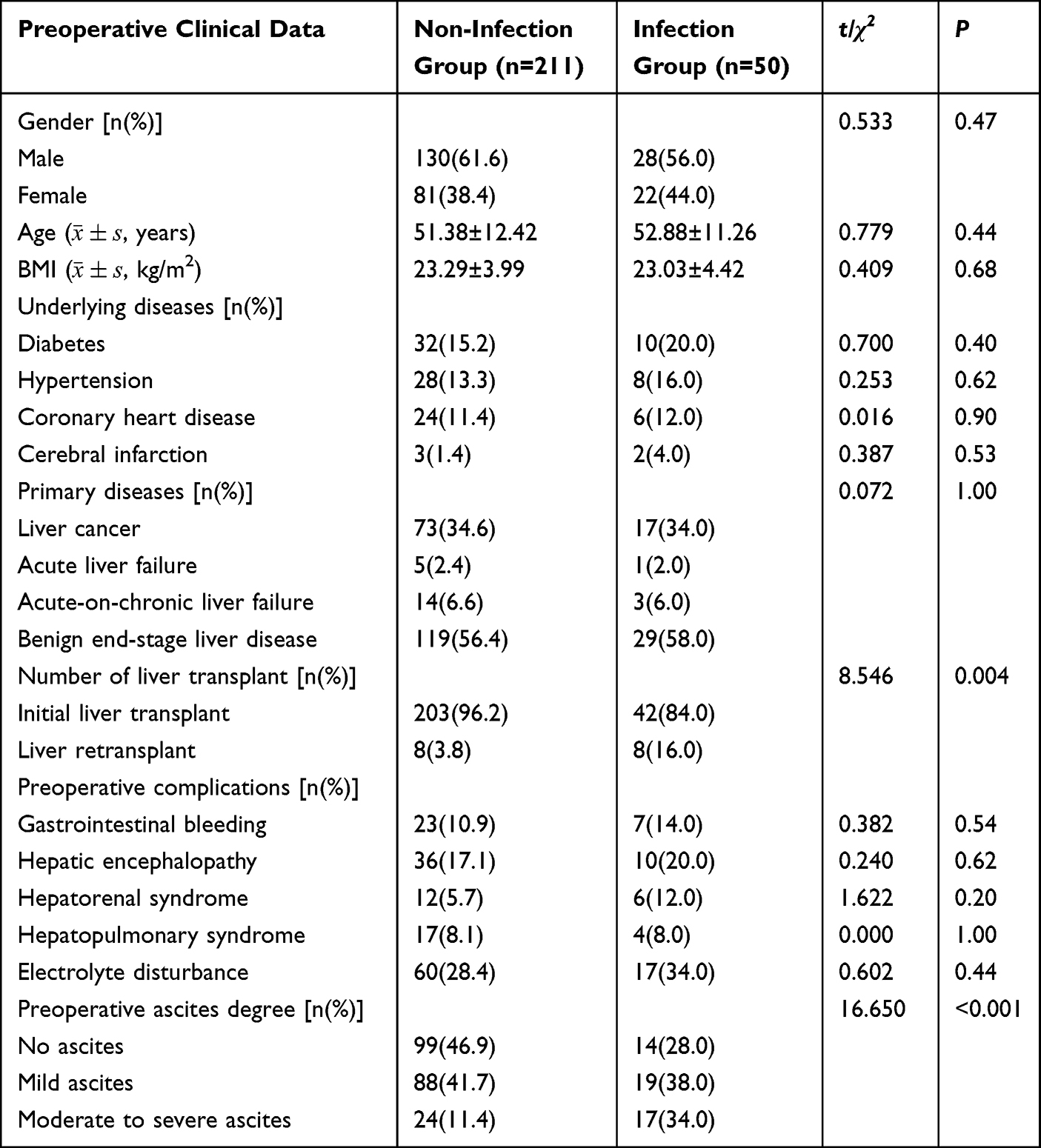 |
Table 2 Preoperative Clinical Data of Patients with or Without Bacterial IAIs |
In comparison with the noninfection group, the IAI group exhibited significantly elevated preoperative levels of NEU, PT, INR, TBIL, NLR, PTAR, CTP score, and MELD score. Conversely, the IAI group showed significantly reduced preoperative levels of LYM, PTA, and ALB. All these differences were statistically significant (all P < 0.05). No statistically significant differences were found between the two groups regarding preoperative levels of WBC, PLT, CRP, APTT, ALT, AST, GGT, AKP, Amon, Cr, serum Na, serum K, LA, GLU, TC, or TG (all P > 0.05) (Table 3).
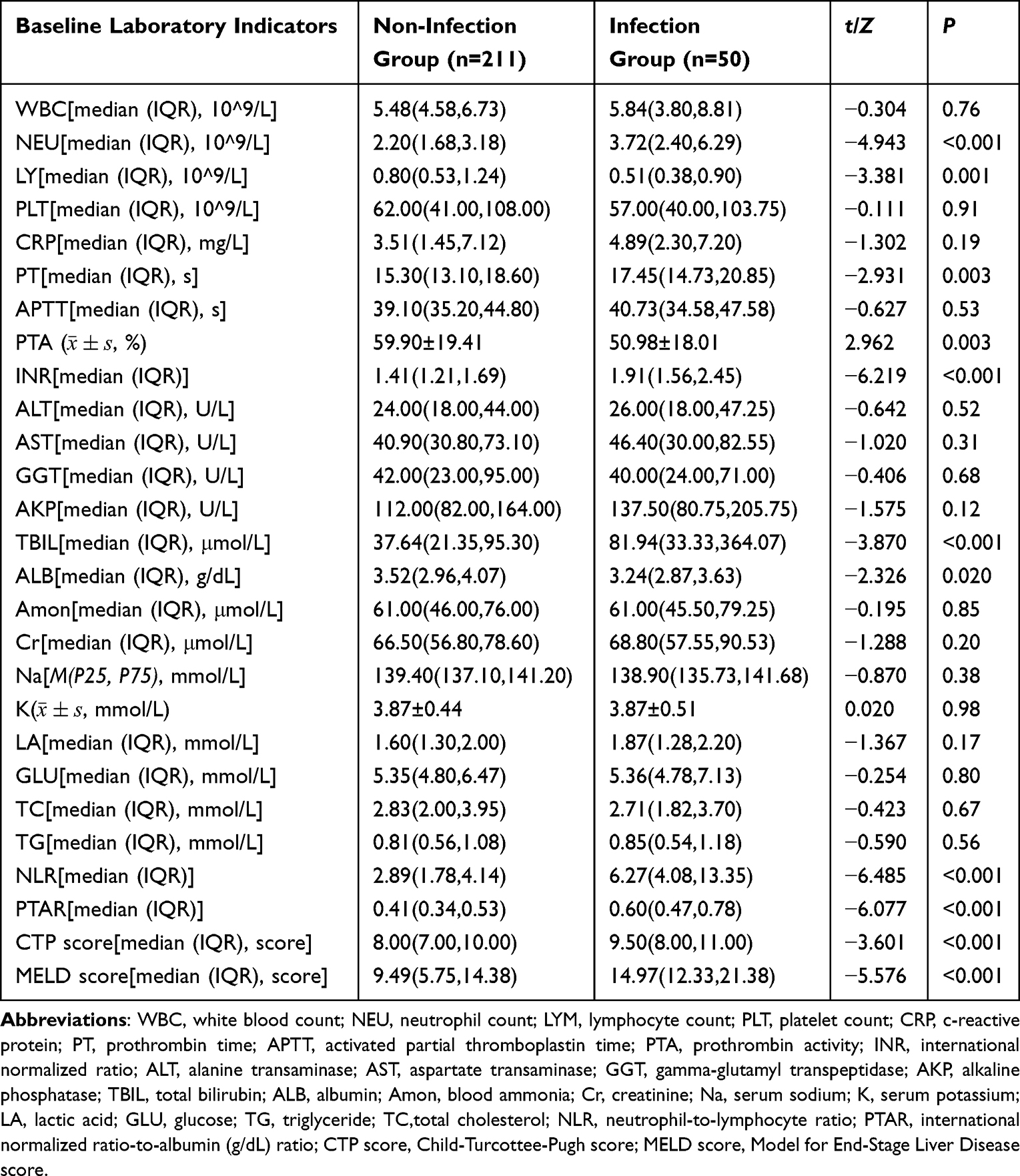 |
Table 3 Baseline Laboratory Indicators (24 Hours Prior to Surgery) of Patients with or Without Bacterial IAIs |
In comparison to the noninfection group, the IAI group demonstrated a significantly greater volume of intraoperative blood loss (P < 0.05). However, there were no statistically significant differences between the two groups regarding donor liver sources; surgical methods; biliary anastomosis methods employed during surgery; operation time; anhepatic phase duration; GRWR (all P > 0.05). All patients received intraoperative blood transfusion or at least one type of blood product—including plasma, albumin, or platelets—during surgery. Given the universal exposure to blood products in this cohort, we individually categorized each product type and quantified the volume administered to enable a more precise assessment of their potential association with postoperative infection. However, there were no statistically significant differences between the two groups regarding intraoperative transfusion volumes of RBC, plasma, and albumin; administration of basiliximab intraoperatively; or the use of vasoactive drugs during surgery (all P > 0.05) (Table 4).
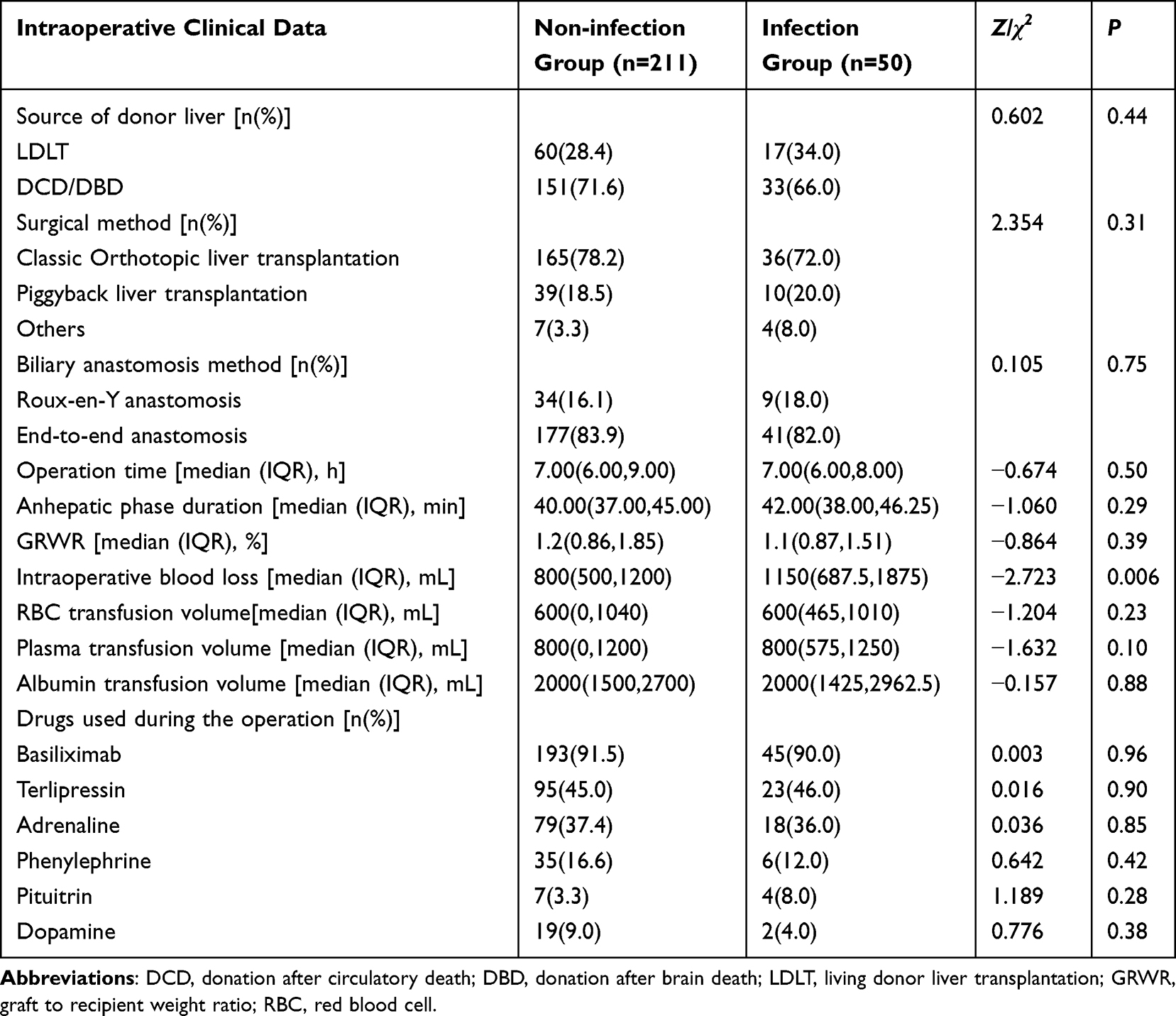 |
Table 4 Intraoperative Clinical Data of Patients with or Without Bacterial IAIs |
The IAI group had a significantly longer ICU stay, higher APACHE II score within the initial 24 hours following ICU admission, extended abdominal drainage tube retention, and a higher incidence of postoperative bile leakage compared to the non-infection group (all P < 0.05). However, there were no significant differences between the groups in the average levels of FK506 and CsA within 30 days after OLT and the rates of different immunosuppressive regimen, administration of reduction or suspension of the immunosuppressants, laparotomy, postoperative abdominal incision debridement and suture, CRRT, postoperative Intra-abdominal hemorrhage, biliary stricture, or colonic leakage (all P > 0.05)(Table 5).
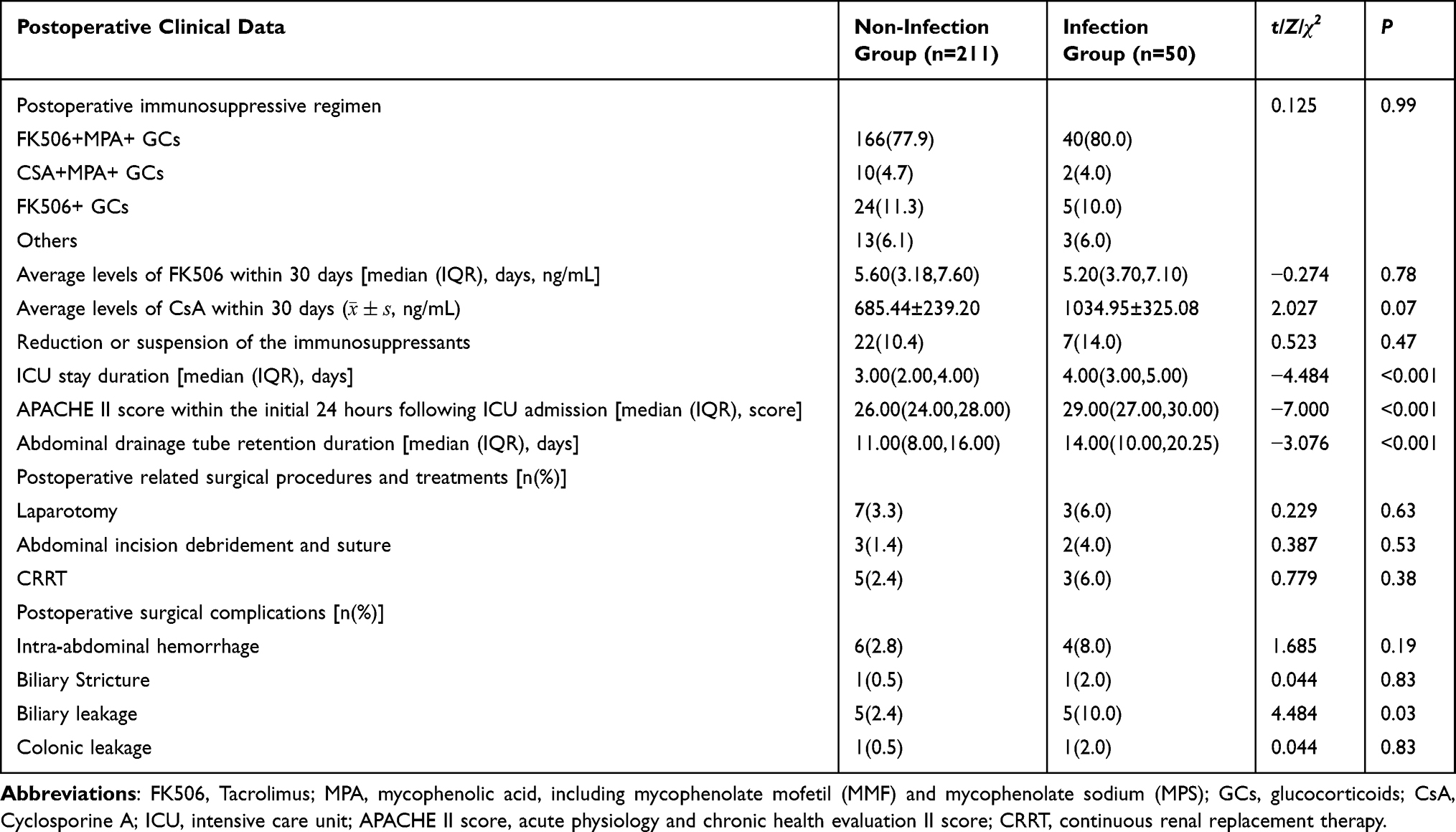 |
Table 5 Postoperative Clinical Data of Patients with or Without Bacterial IAIs |
Correlation Analysis of NLR and PTAR with CTP and MELD Scores
Spearman correlation analysis demonstrated that NLR and PTAR were positively correlated with CTP and MELD scores (all r > 0, P < 0.05). PTAR demonstrated a moderate positive correlation with both CTP and MLED scores (all r > 0.3, P < 0.05). In contrast, NLR displayed a weak positive correlation with both CTP and MLED scores (all 0 < r < 0.3, P < 0.05). (Table 6 and Figure 3).
 |
Table 6 Correlation Analysis of NLR and PTAR with CTP and MELD Scores |
 |
Figure 3 Correlation Analysis of NLR and PTAR with CTP and MELD Score. Abbreviations: NLR, neutrophil-to-lymphocyte ratio; PTAR, international normalized ratio-to albumin (g/dL) ratio; CTP score, Child-Turcottee-Pugh score; MELD score, Model for End-Stage Liver Disease score. |
ROC Curve Analysis of Preoperative NLR, Preoperative PTAR, Preoperative CTP Score, Preoperative MELD Score, and APACHE II Score Within the Initial 24 Hours Following ICU Admission for Predicting Bacterial IAI Within 30 days after OLT
The analysis of the ROC curves indicated that the AUCs for predicting bacterial IAIs were 0.795 for preoperative NLR, 0.776 for preoperative PTAR, 0.662 for preoperative CTP score, 0.754 for preoperative MELD score, and 0.815 for APACHE II score within the initial 24 hours following ICU admission. The P-values associated with all these indicators were less than 0.05, signifying statistically significant predictive value for IAIs. Importantly, the AUC of APACHE II score was the hightest above all. Meanwhile, both the AUC for NLR and PTAR was higher than that for the CTP score and MELD score in predicting bacterial IAIs (Table 7 and Figure 4).
 |
Table 7 ROC Analysis Results of NLR, PTAR, CTP Score, MELD Score and APACHE II Score |
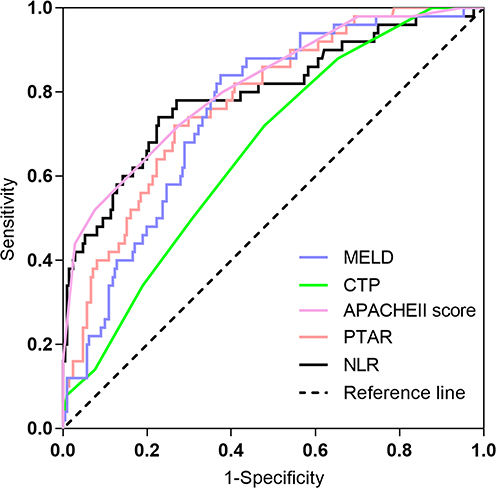 |
Figure 4 ROC curves of NLR, PTAR, CTP score, MELD score, and APACHE II score. Abbreviations: NLR, neutrophil-to-lymphocyte ratio; PTAR, international normalized ratio-to albumin (g/dL) ratio; CTP score, Child-Turcottee-Pugh score; MELD score, Model for End-Stage Liver Disease score, APACHE II score, acute physiology and chronic health evaluation II score. |
Logistic Regression Analysis of Factors Influencing Bacterial IAIs Occurrence Within 30 Days After OLT
A binary logistic regression model was developed utilizing the entry method, with infection status (intra-abdominal infection = 1, noninfection = 0) as the dependent variable. The independent variables included the degree of ascites, number of transplantations, intraoperative blood loss, APACHE II score within the initial 24 hours following ICU admission, duration of postoperative abdominal drainage tube retention, occurrence of postoperative bile leakage, preoperative TBIL, preoperative NLR, and preoperative PTAR. Owing to the presence of collinearity among NEU, LYM, and NLR, as well as among PT, PTA, INR, ALB, CTP score, MELD score, and PTAR, and taking into account that an extended duration of ICU stay may clinically result from an infection,the variables NEU, LYM, PT, PTA, INR, ALB, CTP score, MELD score and ICU stay duration were excluded from the multivariate regression analysis.The analysis revealed that preoperative NLR, preoperative PTAR, APACHE II score within the initial 24 hours following ICU admission, and postoperative bile leakage were statistically significant predictors of IAI occurrence (all P < 0.05), with each serving as a risk factor (odds ratio [OR] > 1). Specifically, elevated preoperative NLR and preoperative PTAR levels, along with a higher APACHE II score within the initial 24 hours following ICU admission, as well as the occurrence of postoperative bile leakage, were all correlated with an increased risk of IAI. (Table 8).
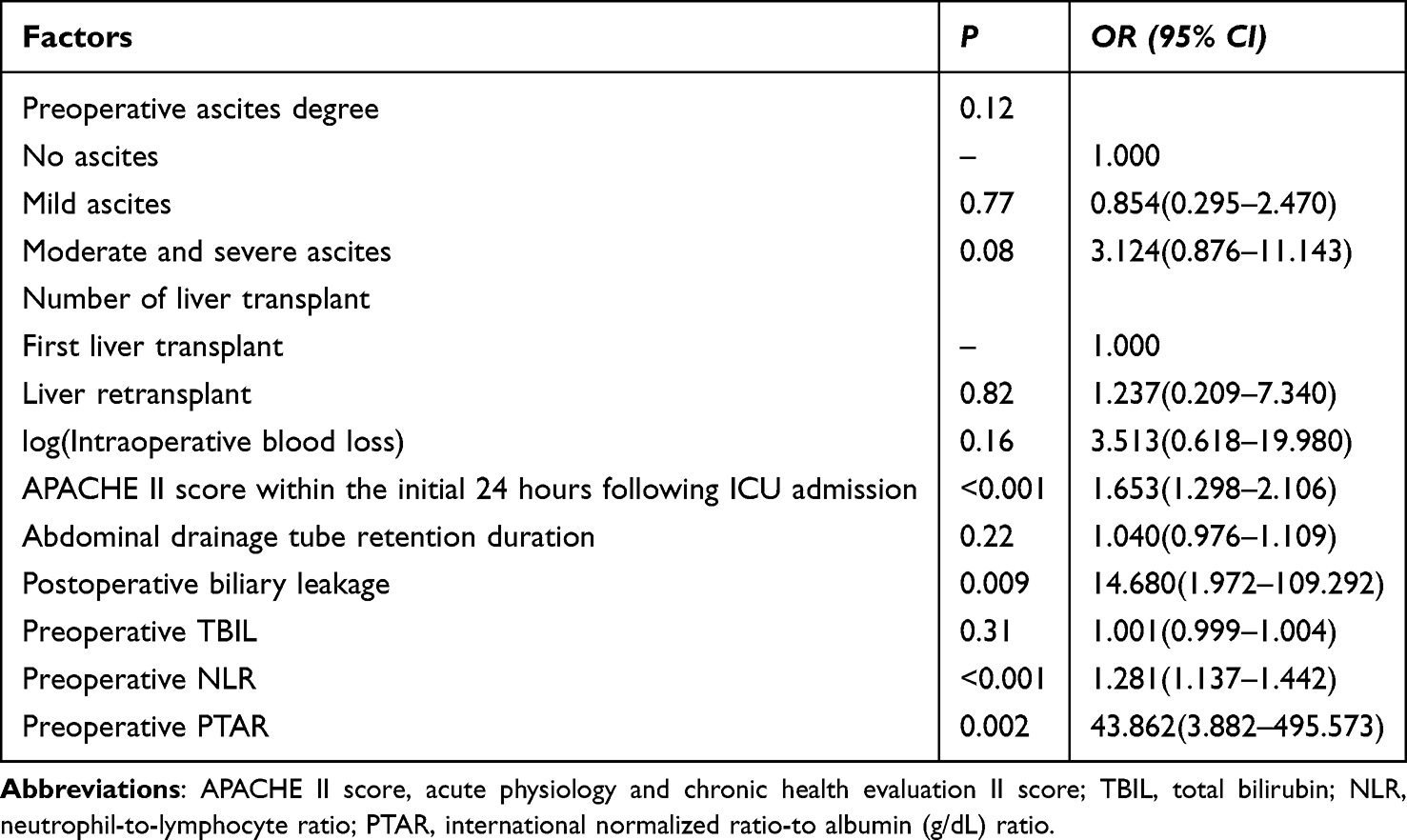 |
Table 8 Results of Logistic Regression Analysis for Factors Influencing the Occurrence of Bacterial IAIs Within 30 Days After OLT |
Construction and Validation of a Nomogram Model for Predicting the Occurrence of Bacterial IAIs Within 30 Days After OLT
Four statistically significant predictors—namely, preoperative NLR, preoperative PTAR, APACHE II score within the initial 24 hours following ICU admission, and occurrence of postoperative bile leakage—were identified through multivariate analysis and utilized as independent variables to construct a combined prediction model employing a coefficient-based approach. The coefficients were derived from the individual logistic regression models fitted separately for each of the four indicators. The specific calculation formula was as follows: ln (P/(1−P)) = 0.488 ×APACHE II score + 2.686 × bile leakage (no = 0, yes = 1) + 0.247 × NLR + 3.781 × PTAR – 23.512. Subsequently, a nomogram was developed based on this model (Figure 5).
 |
Figure 5 Nomogram Model for Predicting Bacterial IAIs within 30 Days After OLT. Abbreviations: NLR, neutrophil-to-lymphocyte ratio; PTAR, international normalized ratio-to albumin (g/dL) ratio; APACHE II score, acute physiology and chronic health evaluation II score. |
The Bootstrap method was employed 1000 times to evaluate the model’s goodness-of-fit. The Hosmer-Lemeshow test for assessing model fit resulted in a χ2 value of 7.349 with a P-value of 0.499, which exceeds the 0.05 threshold. This suggests that the model’s predicted values align well with the observed data (Figure 6).
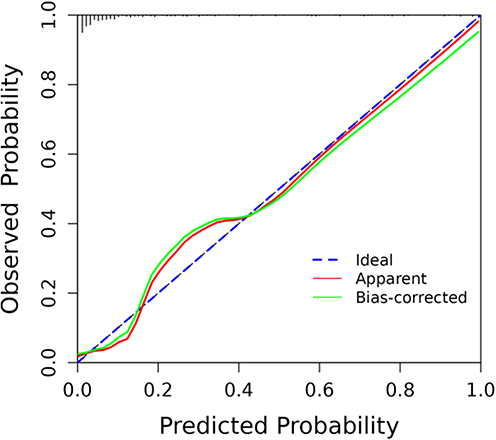 |
Figure 6 Calibration Curve of the Nomogram Model. |
Utilizing the established logistic regression model, the joint probability was computed, and the corresponding ROC curve was subsequently plotted.The AUC was calculated to be 0.912, with a 95% confidence interval (CI) ranging from 0.864 to 0.960. Utilizing the Youden index method, the optimal diagnostic threshold was identified as 0.221 (95% CI: 0.125–0.265). The model exhibited a sensitivity of 86.0% and a specificity of 88.6%, alongside a model-adjusted C-index of 0.900 (95% CI: 0.828–0.972). These metrics collectively suggest that the model possesses strong predictive capability for identifying IAIs within 30 days post-liver transplantation (Figure 7).
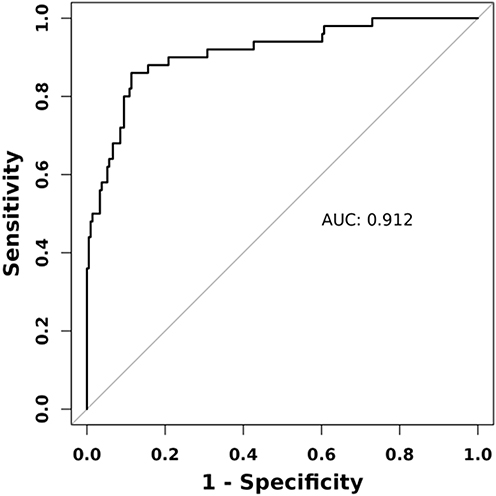 |
Figure 7 ROC Curve of the Nomogram Model. |
In the decision curve analysis (DCA), the y-axis represents the net benefit, the primary x-axis indicates the threshold probability, and the secondary x-axis illustrates the benefit-to-harm ratio. The “None” strategy is depicted by a horizontal line at zero net benefit, signifying that no patients are treated. Conversely, the “All” strategy is represented by a diagonal line with a negative slope, implying that all patients are presumed positive, leading to a diminishing net benefit as the threshold probability increases. The DCA curve of primary interest is derived from our predictive model. In the training dataset, this curve consistently lies above both the “None” and “All” reference lines across the threshold probability range of 0.03 to 1.0, thereby indicating that the model offers enhanced clinical utility within this interval (Figure 8).
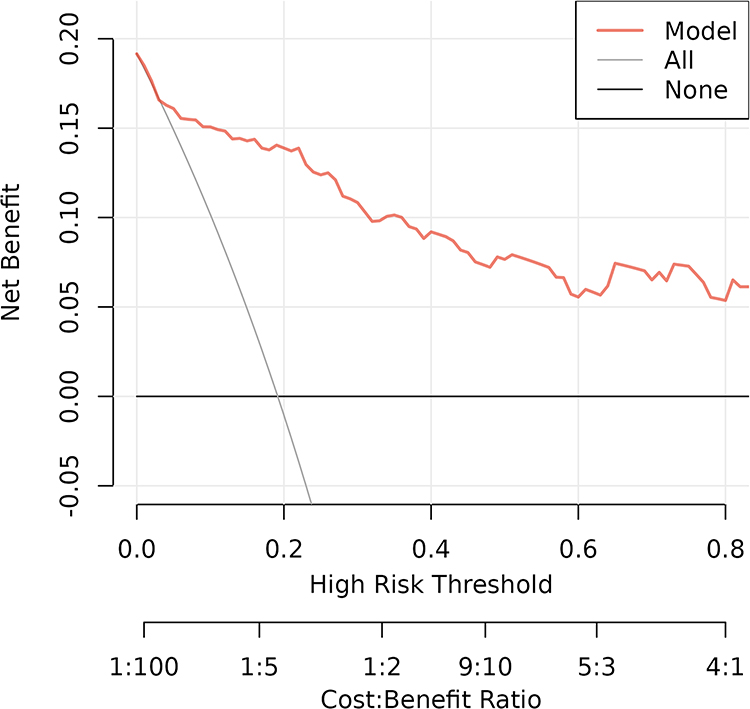 |
Figure 8 DCA Curve of the Nomogram Model. |
Discussion
With the rapid advancement of surgical techniques and perioperative management, the survival rate of liver transplant recipients has significantly improved, with the current 5-year survival rate exceeding 70%.31 Despite these advancements, a considerable proportion of liver transplant recipients continue to experience infections during the early postoperative period.4 Bacterial IAIs are most prevalent within the first month after liver transplantation and have a substantial impact on both recipient and graft survival rates.7,32 In this study, the overall incidence of bacterial IAIs within 30 days after OLT was 19.2% (50/261), a figure consistent with those reported in previous research.7,33 Analysis of the pathogen composition and temporal distribution of infections revealed that E. faecium (15.2%, 10/66) and K. pneumoniae (15.2%, 10/66) were the most frequent cause of IAIs, and among patients with IAIs, 44.0% (22/50) developed infections within one week postoperatively, aligning with findings from previous studies.7,34–36 The mortality rate associated with early infections can reach 10 to 30%,36 significantly affecting patient prognosis. However, the clinical use of immunosuppressants often results in atypical infection symptoms in many patients, and the inherent limitations of conventional culture methods can delay timely diagnosis and treatment to some extent.3 Moreover, early postoperative infections are frequently caused by multidrug-resistant bacteria acquired nosocomially, thereby further complicating treatment management.3 Consequently, early and accurate identification of infection, along with prompt intervention, is critical for reducing mortality and improving patient outcomes.
The NLR is calculated by dividing the number of neutrophils by the number of lymphocytes. The neutrophil count is indicative of the inflammatory status during disease progression,37 whereas the lymphocyte count reflects the regulated immune system.38 NLR serves as a marker for the equilibrium between the host’s inflammatory and immune responses, thereby reflecting immune system homeostasis and effectively predicting both the occurrence and severity of infections.38 Patients with end-stage liver disease awaiting liver transplantation frequently exhibit immune dysfunction and a chronic inflammatory response, resulting in elevated NLR compared to healthy individuals. The extent of NLR elevation serves as an indicator of the inflammatory burden and immune status, and is closely associated with an increased risk of infection.38–40 Umman16 found that patients who developed postoperative infections after liver transplantation exhibited significantly elevated NLR levels 1 week after surgery, prior to the onset of infection. These levels were markedly different from those observed in the non-infection group (P < 0.05). Yu’s study17 indicated that preoperative NLR were significantly elevated in patients experiencing infection compared to those without infection during the early postoperative period following liver transplantation (P < 0.05).Wiegand18 conducted a study to evaluate the efficacy of the NLR as a biomarker for detecting bacterial and fungal infections after liver or lung transplantation. The findings demonstrated that NLR levels significantly elevated in patients experiencing infections. Furthermore, the efficacy of NLR in detecting bacterial and fungal infections surpassed that of interleukin-6 (IL-6), CRP, and WBC. Given that the immune response elicited by fungal infections differs from that elicited by bacterial infections,18 and considering that only 5 patients with fungal infections were included in this study, we excluded these patients to more accurately assess NLR as a biomarker for bacterial infections post-transplantation. Our study revealed that the preoperative NLR was significantly elevated in the bacterial infection group compared to the non-infection group. Since IL-6 was not routinely tested preoperatively, our analysis was limited to preoperative CRP and preoperative WBC, two conventional markers of infection, which did not show a significant difference between the groups. These findings suggest that NLR is a more effective predictor of bacterial infection than traditional inflammatory markers. Multivariate analysis further identified preoperative NLR as an independent risk factor for early bacterial IAIs after OLT. Moreover, preoperative NLR demonstrated satisfactory predictive performance in the infection group, achieving a higher diagnostic accuracy (AUC:0.795 vs 0.754) than the conventional MELD score. This metric shows potential for assisting clinicians in identifying high-risk populations for postoperative infections. Nevertheless, comprehensive studies examining the correlation between NLR and posttransplant infectious complications are relatively scarce, highlighting the necessity for prospective research to further substantiate its reliability.
The PT-INR to albumin ratio PTAR, a novel indicator introduced by Haruki19 in 2018, was initially developed to assess liver function status. Subsequent studies41,42 have further validated its utility, demonstrating its robust predictive capability in evaluating the prognosis of patients with severe cirrhosis. PTAR is calculated using INR and ALB. Elevated INR levels often suggest impaired liver synthetic function and coagulation dysfunction.42 Considering the liver’s critical role in immune defense, this impairment may further compromise the immune function of liver transplant recipients undergoing immunosuppressive therapy, thereby increasing their susceptibility to infections.43 Moreover, an elevated INR may suggest an intensified inflammatory response,44 thereby increasing susceptibility to infection. Empirical studies6,23 have shown that an elevated INR prior to liver transplantation significantly heightened the risk of postoperative infection. ALB, a plasma protein synthesized by the liver, is closely associated with nutritional status and inflammatory response.45,46 Low levels of this protein have been widely recognized as an independent risk factor for infection following solid organ transplantation.24,47,48 From a pathophysiological standpoint, hypoproteinemia is commonly associated with malnutrition, which adversely impacts the activity and function of immune cells, compromising the body’s ability to combat infections and exacerbating the risk of infection in the context of immunosuppression.49 Furthermore, albumin possesses anti-inflammatory properties and plays a role in modulating the release of inflammatory mediators. Consequently, hypoalbuminemia may precipitate dysregulated inflammatory responses, leading to systemic inflammatory response syndrome characterized by the release of substantial quantities of inflammatory mediators and cytokines into the bloodstream, ultimately culminating in various inflammatory complications.50 These observations further elucidate the potential link between liver dysfunction and infection. In our study, we considered that the administration of coagulation substances and albumin could potentially destabilize PTAR parameters. Consequently, we excluded patients who received such treatments within 1 week prior to surgery based on our experience to enhance the reliability of our conclusions. Our study indicates that elevated preoperative PTAR serve as an independent risk factor for early bacterial IAIs after OLT. Moreover, preoperative PTAR demonstrated a higher diagnostic accuracy (AUC:0.776 vs 0.754) than the conventional MELD score. These findings corroborate our hypothesis that PTAR can be a marker for the body’s inflammatory state, with higher PTAR correlating with an increased risk of infection.
The Child–Turcotte–Pugh (CTP) score is currently the most widely utilized method for classifying liver function. It is instrumental in evaluating liver reserve capacity, surgical risks, and prognosis in patients with end-stage liver disease. A high CTP score has been identified as an independent risk factor for posttransplant infections.27,51 The MELD score, a well-established model for assessing the prognosis of patients with various liver diseases, is extensively employed in clinical practice, with higher scores correlating with poorer patient outcomes. Research indicates that liver transplant recipients with low MELD scores tend to exhibit better postoperative liver function preservation and reduced infection risks.52,53 Nonetheless, the MELD score shows limited reliability in predicting posttransplant infection risks in patients with end-stage liver disease. This limitation is attributed to the scoring system’s exclusion of indicators related to inflammatory responses or immune status, which are crucial to the infection development process following liver transplantation.9 Addressing this gap, this study incorporated inflammatory and immune-related markers to evaluate the predictive utility of NLR and PTAR for early bacterial IAIs after OLT. ROC curve analysis demonstrated that both the AUC for postoperative NLR and postoperative PTAR was higher than that for the postoperative CTP scores and postoperative MELD scores, suggesting superior predictive performance of postoperative NLR and postoperative PTAR. Correlation analysis further revealed positive associations of NLR and PTAR with CTP and MELD scores, indicating their potential to reflect liver function status and disease severity, thereby influencing postoperative prognosis.
The APACHE II scoring system, introduced by Knaus29 in 1985, consists of three components: the acute physiology score, the chronic health status score, and the age score, culminating in a total score ranging from 0 to 71. Higher scores correlate with an increased risk of mortality, establishing it as one of the most extensively utilized tools for assessing severity of illness in ICU. Numerous studies54–57 have demonstrated that the APACHE II score not only objectively reflects disease severity but also facilitates early prediction of various infections, with its accuracy being widely acknowledged by clinicians. In this study, we obtained the most adverse values for each parameter within the initial 24 hours following ICU admission and subsequently calculated the APACHE II score for each patient. Importantly, no patient exhibited signs of IAI within the initial 24-hour period, thus eliminating the likelihood that elevated APACHE II scores were attributable to such infections. Multivariate analysis identified the APACHE II score as an independent risk factor for postoperative IAI. Furthermore, the AUC for the APACHE II score in predicting IAI was superior to those of NLR and PTAR, demonstrating enhanced predictive performance. This superior predictive capability may be ascribed to the APACHE II system’s incorporation of a more comprehensive array of physiological and clinical parameters, facilitating a more precise evaluation of postoperative IAI risk.
Through multivariate analysis, it was determined that, along with preoperative NLR, preoperative PTAR, and APACHE II score within the initial 24 hours following ICU admission, the incidence of bile leakage emerged as independent risk factors for the development of bacterial IAIs within 30 days posttransplantation. The result aligns with findings from previous research.58–60 In our study, we systematically documented instances of bile leakage that transpired before the onset of infection. This temporal restriction was applied to maximize the likelihood that these variables are potential predisposing factors rather than consequences of infection. Drawing on the identified independent risk factors, we constructed a nomogram prediction model, which underwent internal validation through the Bootstrap method. The model’s calibration was deemed satisfactory, as evidenced by the Hosmer-Lemeshow goodness-of-fit test. ROC curve analysis demonstrated that the model possessed strong discriminative capability, while DCA affirmed its favorable clinical applicability. This study effectively translates a complex regression equation into a visually interpretable graph. By integrating individual risk parameters from the nomogram, the model enables quantitative prediction and personalized assessment of the risk of bacterial IAIs after OLT, thereby offering substantial clinical value in the prevention of postoperative abdominal infectious complications.
This study has several limitations. As a single-center retrospective analysis, it was restricted to internal validation of the nomogram model. Variability in postoperative anti-infection and immunosuppressive regimens across different transplant centers may introduce potential confounding effects on patient prognosis. Consequently, future multi-center, large-sample prospective studies are necessary to further establish the model’s reliability. Furthermore, this study exclusively utilized clinical-related variables. As detection technologies continue to advance, incorporating novel biomarkers for the early identification of infection in liver transplant recipients could enhance the predictive accuracy of the model in future applications.
Conclusion
In this study, preoperative NLR, preoperative PTAR, APACHE II score assessed within the initial 24 hours following ICU admission, and postoperative bile leakage have been identified as independent risk factors for bacterial IAIs occurring within 30 days after OLT. The nomogram model developed from these variables exhibits significant predictive value for such infections after OLT. This model is clinically significant as it aids in identifying patients at high risk and informs the development of targeted preventive and therapeutic strategies. Importantly, NLR and PTAR are routine, non-invasive laboratory parameters that are easily accessible in clinical practice. Their straightforward calculation methods facilitate monitoring, underscoring their potential for widespread clinical application.
Data Sharing Statement
The data used and analyzed during this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of Beijing Friendship Hospital (Ethical Approval Number: 2025-P2-095-01). Given the retrospective nature of this study and all patients’ information has been anonymized, the ethics committee waived the requirement for written informed consent. Since that patient contact information can be obtained from the electronic medical record system, the ethics committee approved the acquisition of informed consent via telephone communication, with recorded conversations serving as documentation of consent prior to the collection of all research-related data. All methods were carried out in accordance with relevant guidelines and regulations. This study was conducted in accordance with the RECORD reporting guidelines.61 The RECORD checklist requirements are detailed in the online Supplementary Table S1.
Acknowledgments
We thank the study staff of Beijing Friendship Hospital affiliated with Capital Medical University, Department of Critical Liver Diseases and Liver Transplantation Center, who contributed to the study.
Author Contributions
Hua-Bin Peng; Conceptualization, Methodology, Data curation, Formal analysis and Writing-original draft. Ying Liu; Conceptualization and Writing-review & editing. Fei Hou; Conceptualization and Writing-review & editing. Shuang Zhao; Conceptualization and Writing-review & editing. Yi-Zhi Zhang; Conceptualization and Writing-review & editing. Zhi-Ying He; Formal analysis and Writing-review & editing. Ting-Ting Cui; Formal analysis and Writing-review & editing. Jing-Yi Liu; Formal analysis and Writing-review & editing. Hao-Feng Xiong; Conception, Data curation, Formal analysis, Project administration and Writing-review & editing. Li-Ying Sun; Conceptualization, Supervision, Funding acquisition and Writing-review & editing. Each author assumed responsibility for their respective tasks, and all authors reviewed and gave final approval of the version to be published; agreed to submit this paper to Journal of Inflammation Research, and agree to be accountable for the content of this paper.
Funding
This study was funded by the Tongzhou District Science and Technology Innovation Talent Support Project (CXTD2024007).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Raskov H, Orhan A, Christensen JP, et al. Cytotoxic CD8(+) T cells in cancer and cancer immunotherapy. Br J Cancer. 2021;124(2):359–20. doi:10.1038/s41416-020-01048-4
2. Shetty A, Kodali S. Long-term management of the successful adult liver transplant: a patient-friendly summary of the 2012 AASLD and AST Practice Guideline. Clin Liver Dis. 2022;19(3):83–88. doi:10.1002/cld.1179
3. Peng HB, Liu Y, Hou F, et al. Clinical application of metagenomic next-generation sequencing (mNGS) in patients with early pulmonary infection after liver transplantation. Infect Drug Resist. 2024;17:5685–5698. doi:10.2147/IDR.S483684
4. Wu X, Wu L, Wan Q. Pathogen distribution and risk factors of bacterial and fungal infections after liver transplantation. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022;47(8):1120–1128. doi:10.11817/j.issn.1672-7347.2022.220054
5. Ayvazoglu Soy EH, Akdur A, Yildirim S, et al. Early postoperative infections after liver transplant. Exp Clin Transplant. 2018;16(Suppl 1):145–148. doi:10.6002/ect.TOND-TDTD2017.P36
6. Chen C, Guan Q, Li D, et al. Clinical characteristics and risk factor analysis of recipients with multidrug-resistant bacterial bloodstream infections after liver transplantation: a single-centre retrospective study. J Pharm Policy Pract. 2024;17(1):2390072. doi:10.1080/20523211.2024.2390072
7. Taddei R, Riccardi N, Tiseo G, et al. Early intra-abdominal bacterial infections after orthotopic liver transplantation: a narrative review for clinicians. Antibiotics. 2023;12(8). doi:10.3390/antibiotics12081316
8. Dolci G, Burastero GJ, Paglia F, et al. Epidemiology and prevention of early infections by multi-drug-resistant organisms in adults undergoing liver transplant: a narrative review. Microorganisms. 2023;11(6):1606. doi:10.3390/microorganisms11061606
9. Chen G, Hu X, Huang Y, et al. Role of the immune system in liver transplantation and its implications for therapeutic interventions. MedComm. 2023;4(6):e444. doi:10.1002/mco2.444
10. Liu Y, Lei Z, Chai H, et al. Thrombomodulin-mediated inhibition of neutrophil extracellular trap formation alleviates hepatic ischemia-reperfusion injury by blocking TLR4 in rats subjected to liver transplantation. Transplantation. 2022;106(2):e126–e40. doi:10.1097/TP.0000000000003954
11. Regolo M, Vaccaro M, Sorce A, et al. Neutrophil-to-lymphocyte ratio (NLR) is a promising predictor of mortality and admission to intensive care unit of COVID-19 patients. J Clin Med. 2022;11(8).
12. Liu S, Wang X, She F, et al. Effects of neutrophil-to-lymphocyte ratio combined with interleukin-6 in predicting 28-day mortality in patients with sepsis. Front Immunol. 2021;12:639735. doi:10.3389/fimmu.2021.639735
13. Zhang G, Wang T, An L, et al. The neutrophil-to-lymphocyte ratio levels over time correlate to all-cause hospital mortality in sepsis. Heliyon. 2024;10(16):e36195. doi:10.1016/j.heliyon.2024.e36195
14. Liu F, Chen L, Wang MY, et al. Exploring high-risk factors for the prediction of severe mycoplasma pneumonia in children. Transl Pediatr. 2024;13(11):2003–2011. doi:10.21037/tp-24-293
15. Erfanipour M, Dooki ME, Nikbakht HA, et al. Diagnostic value of neutrophil to lymphocyte ratio in identifying gastritis in children with chronic abdominal pain in northern Iran. BMC Res Notes. 2025;18(1):68. doi:10.1186/s13104-025-07148-9
16. Umman V, Gumus T, Kivratma HG, et al. Predictive value of red blood cell distribution width, platelet count to lymphocyte count ratio, and neutrophil count to lymphocyte count ratio values for the detection of postoperative infection in patients undergoing liver transplantation. Transplant Proc. 2023;55(5):1257–1261. doi:10.1016/j.transproceed.2023.05.002
17. Yu J, Jiang J, Fan C, et al. A nomogram for predicting early bacterial infection after liver transplantation: a retrospective study. Front Med Lausanne. 2025;12:1563235. doi:10.3389/fmed.2025.1563235
18. Wiegand SB, Paal M, Jung J, et al. Importance of the neutrophil-to-lymphocyte ratio as a marker for microbiological specimens in critically ill patients after liver or lung transplantation. Infection. 2025;53(2):573–582. doi:10.1007/s15010-024-02398-4
19. Haruki K, Shiba H, Saito N, et al. Risk stratification using a novel liver functional reserve score of combination prothrombin time-international normalized ratio to albumin ratio and albumin in patients with hepatocellular carcinoma. Surgery. 2018;164(3):404–410. doi:10.1016/j.surg.2018.02.022
20. Jensen JS, Peters L, Itenov TS, et al. Biomarker-assisted identification of sepsis-related acute liver impairment: a frequent and deadly condition in critically ill patients. Clin Chem Lab Med. 2019;57(9):1422–1431. doi:10.1515/cclm-2018-1350
21. Ren HQ, Zhong S, Lei Y, et al. Analysis of risk factors for decompensated cirrhosis complicated with sepsis. Zhonghua Gan Zang Bing Za Zhi. 2022;30(11):1163–1169. doi:10.3760/cma.j.cn501113-20210913-00469
22. Kramer L, Jordan B, Druml W, et al. Incidence and prognosis of early hepatic dysfunction in critically ill patients--a prospective multicenter study. Crit Care Med. 2007;35(4):1099–1104. doi:10.1097/01.CCM.0000259462.97164.A0
23. Tezcan H, Altunsoy A, Turan Gökçe D, et al. Multidrug-resistant infections after liver transplantation, etiology and risk factors: a single-center experience. Exp Clin Transplant. 2023;21(12):952–960. doi:10.6002/ect.2023.0081
24. Liu M, Li C, Liu J, et al. Risk factors of early bacterial infection and analysis of bacterial composition, distribution and drug susceptibility after cadaveric liver transplantation. Ann Clin Microbiol Antimicrob. 2023;22(1):63. doi:10.1186/s12941-023-00616-9
25. Sartelli M, Coccolini F, Kluger Y, et al. WSES/GAIS/SIS-E/WSIS/AAST global clinical pathways for patients with intra-abdominal infections. World J Emerg Surg. 2021;16(1):49. doi:10.1186/s13017-021-00387-8
26. Chinese Society of Surgery of Chinese Medical Association, Infectious Diseases Society for Evidence-based and Translational Medicine of Chinese Research Hospital Association, Editorial Board of Chinese Journal of Surgery. 外科常见腹腔感染多学科诊治专家共识 [Expert consensus on multidisciplinary management of intra-abdominal infections]. Zhonghua Wai Ke Za Zhi. 2021;59(3):161–178. Chinese. doi:10.3760/cma.j.cn112139-20201223-00874
27. Zhang J, He Q, Du L, et al. Risk factor for lung infection in recipients after liver transplantation: a meta-analysis. Artif Organs. 2021;45(3):289–296. doi:10.1111/aor.13826
28. Kim -H-H, Youn Y-N. Predictive scoring systems for mortality in heart transplant patients with liver cirrhosis. Sci Rep. 2025;15(1):12663. doi:10.1038/s41598-025-87675-4
29. Knaus WA, Draper EA, Wagner DP, et al. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829. doi:10.1097/00003246-198510000-00009
30. Yoon PD, Patel MS, Murillo Perez CF, et al. Outcomes of adult liver retransplantation: a Canadian National Database analysis. Can J Gastroenterol Hepatol. 2022;2022:9932631. doi:10.1155/2022/9932631
31. Adam R, Karam V, Cailliez V, et al. 2018 annual report of the European Liver Transplant Registry (ELTR) - 50-year evolution of liver transplantation. Transpl Int. 2018;31(12):1293–1317. doi:10.1111/tri.13358
32. Shinde AS, Kapoor D. Infections after liver transplant -timeline, management and prevention. J Clin Exp Hepatol. 2024;14(3):101316. doi:10.1016/j.jceh.2023.101316
33. Nie K, Ran R, Tan W, et al. Risk factors of intra-abdominal bacterial infection after liver transplantation in patients with hepatocellular carcinoma. Chin J Cancer Res. 2014;26(3):309–314. doi:10.3978/j.issn.1000-9604.2014.06.10
34. Wang W, Wang B, Lin T, et al. Distribution, drug resistance, and risk factors of infection in liver transplant recipients with liver failure. Transplant Proc. 2025;57(2):305–311. doi:10.1016/j.transproceed.2025.01.003
35. Pedersen M, Seetharam A. Infections after orthotopic liver transplantation. J Clin Exp Hepatol. 2014;4(4):347–360. doi:10.1016/j.jceh.2014.07.004
36. Kim SI. Bacterial infection after liver transplantation. World J Gastroenterol. 2014;20(20):6211–6220. doi:10.3748/wjg.v20.i20.6211
37. Wang X, Chen X, Guan X, et al. The neutrophil-to-lymphocyte ratio is associated with clinical symptoms in first-episode medication-naïve patients with schizophrenia. Schizophrenia. 2024;10(1):13. doi:10.1038/s41537-024-00437-5
38. Buonacera A, Stancanelli B, Colaci M, et al. Neutrophil to lymphocyte ratio: an emerging marker of the relationships between the immune system and diseases. Int J Mol Sci. 2022;23(7):3636. doi:10.3390/ijms23073636
39. Cai XH, Tang YM, Chen SR, et al. Prognostic value of neutrophil-to-lymphocyte ratio in end-stage liver disease: a meta-analysis. World J Hepatol. 2024;16(3):477–489. doi:10.4254/wjh.v16.i3.477
40. Riff A, Haem Rahimi M, Delignette MC, et al. Assessment of neutrophil subsets and immune checkpoint inhibitor expressions on T lymphocytes in liver transplantation: a preliminary study beyond the neutrophil-lymphocyte ratio. Front Physiol. 2023;14:1095723. doi:10.3389/fphys.2023.1095723
41. Zhang T, Ye B, Shen J. Prognostic value of albumin-related ratios in HBV-associated decompensated cirrhosis. J Clin Lab Anal. 2022;36(4):e24338. doi:10.1002/jcla.24338
42. Sheng Y, Zeng Y, Luo W, et al. Predictive value of the prothrombin time-international normalized ratio to albumin ratio in the prognosis of patients with Hepatitis B virus-related acute-on-chronic liver failure. Int J Gen Med. 2023;16:4565–4572. doi:10.2147/IJGM.S434572
43. Zou J, Li J, Wang X, et al. Neuroimmune modulation in liver pathophysiology. J Neuroinflammation. 2024;21(1):188. doi:10.1186/s12974-024-03181-w
44. Hazarapetyan L, Zelveian PH, Grigoryan S. Inflammation and coagulation are two interconnected pathophysiological pathways in atrial fibrillation pathogenesis. J Inflamm Res. 2023;16:4967–4975. doi:10.2147/JIR.S429892
45. Mcmillan DC. Systemic inflammation, nutritional status and survival in patients with cancer. Curr Opin Clin Nutr Metab Care. 2009;12(3):223–226. doi:10.1097/MCO.0b013e32832a7902
46. Abedi F, Zarei B, Elyasi S. Albumin: a comprehensive review and practical guideline for clinical use. Eur J Clin Pharmacol. 2024;80(8):1151–1169. doi:10.1007/s00228-024-03664-y
47. Srivastava A, Bodnar J, Osman F, et al. Serum albumin level before kidney transplant predicts post-transplant BK and possibly cytomegalovirus infection. Kidney Int Rep. 2020;5(12):2228–2237. doi:10.1016/j.ekir.2020.09.012
48. Mohammadi A, Inanloo SH, Rezaeian A, et al. Hypo-albuminemia and perioperative renal transplant-related infections: a systematic review and meta-analysis. Urol J. 2024;21(5):274–282. doi:10.22037/uj.v21i.7943
49. Li Y, Liu X, Jiang Y, et al. Low preoperative prealbumin predicts the prevalence of complications following liver transplantation. BMC Gastroenterol. 2021;21(1):233. doi:10.1186/s12876-021-01818-1
50. Pompili E, Zaccherini G, Baldassarre M, et al. Albumin administration in internal medicine: a journey between effectiveness and futility. Eur J Intern Med. 2023;117:28–37. doi:10.1016/j.ejim.2023.07.003
51. Kaido T, Mori A, Ogura Y, et al. Pre- and perioperative factors affecting infection after living donor liver transplantation. Nutrition. 2012;28(11–12):1104–1108. doi:10.1016/j.nut.2012.02.007
52. Moraes ACO, Oliveira PC, Fonseca-Neto O. The impact of the meld score on liver transplant allocation and results: an integrative review. Arq Bras Cir Dig. 2017;30(1):65–68. doi:10.1590/0102-6720201700010018
53. Juntermanns B, Manka P, Hoyer DP, et al. Infectious complications in the era of MELD. Ann Transplant. 2015;20:297–302. doi:10.12659/AOT.893122
54. Mora-Jiménez I, Tarancón-Rey J, Álvarez-Rodríguez J, et al. Artificial intelligence to get insights of multi-drug resistance risk factors during the first 48 hours from ICU admission. Antibiotics. 2021;10(3). doi:10.3390/antibiotics10030239
55. Jiang YH, Zhao R, Bai YX, et al. Development and validation of a nomogram to predict bacterial blood stream infection. Eur J Med Res. 2025;30(1):404. doi:10.1186/s40001-025-02617-0
56. Zhou X, Zhang Z, Wang X, et al. Study on the predictive value of APACHE II score and neurogenic dysphagia in carbapenem-resistant Klebsiella pneumoniae. Medicine. 2024;103(50):e40858. doi:10.1097/MD.0000000000040858
57. Li H-Y, Li S-J, Yang N, et al. Evaluation of nosocomial infection risk using APACHE II scores in the neurological intensive care unit. J Clin Neurosci. 2014;21(8):1409–1412. doi:10.1016/j.jocn.2013.11.036
58. Li Z, Rammohan A, Gunasekaran V, et al. Biliary complications after adult-to-adult living-donor liver transplantation: an international multicenter study of 3633 cases. Am J Transplant. 2024;24(7):1233–1246. doi:10.1016/j.ajt.2024.02.023
59. Fasullo M, Patel M, Khanna L, et al. Post-transplant biliary complications: advances in pathophysiology, diagnosis, and treatment. BMJ Open Gastroenterol. 2022;9(1):e000778. doi:10.1136/bmjgast-2021-000778
60. Fang C, Yan S, Zheng S. Bile Leakage after Liver Transplantation. Open Med. 2017;12:424–429. doi:10.1515/med-2017-0062
61. Cushieri S. The STROBE guidelines. Saudi J Anaesth. 2019;13(Suppl 1):S31–S34. doi:10.4103/sja.SJA_543_18
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Affecting Duration of Hospital Stay in Deceased COVID-19 Patients
Kurtipek E, Mermer M, Yıldırım B, Yazar MA, Duran M, Duksal F
International Journal of General Medicine 2023, 16:929-936
Published Date: 13 March 2023
Predictive Value of the Neutrophil-to-Lymphocyte Ratio and C-Reactive Protein in Patients with Idiopathic Facial Nerve Palsy
Xu L, Guo T, Sheng X, Du H, Tang Y
International Journal of General Medicine 2024, 17:2635-2642
Published Date: 7 June 2024