")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
The Predictive Value of Essen and SPI-II on the Risk of 5-Year Recurrence in Chinese Patients with Acute Ischemic Stroke
Authors Zhao J, Wang D , Liu X , Wang Y , Zhao X
Received 1 August 2023
Accepted for publication 18 October 2023
Published 24 October 2023 Volume 2023:19 Pages 2251—2260
DOI https://doi.org/10.2147/NDT.S433383
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Jing Zhao,1 Dandan Wang,1 Xinmin Liu,1 Yu Wang,1,2 Xingquan Zhao1– 4
1Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 2National Clinical Research Center for Neurological Diseases, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 3Research Unit of Artificial Intelligence in Cerebrovascular Disease, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 4Department of Beijing Institute of Brain Disorders, Collaborative Innovation Center for Brain Disorders, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Xingquan Zhao, Email [email protected]
Background: The risk prediction score for stroke recurrence is an important tool for stratifying patients based on the risk of cerebrovascular events and selecting potential preventive treatments.
Objective: The study aimed to validate the Essen Stroke Risk Score (ESRS) and Stroke Prognosis Instrument II (SPI-II) for predicting long-term risk of stroke recurrence and combined vascular events in Chinese patients with acute ischemic stroke (AIS).
Methods: A total of 876 consecutive patients with non-atrial fibrillation AIS were recruited. The Kaplan-Meier (KM) method was used to estimate the cumulative incidence of stroke recurrence and combined vascular events in different subgroups stratified by the ESRS and SPI-II scores. The area under the receiver operating characteristic curve (AUC) was calculated to evaluate the predictive value of the two scores for stroke recurrence and combined vascular events.
Results: The KM estimate for 5-year cumulative incidence of stroke recurrence and combined vascular events was 28.7% (95% confidence interval [CI], 25.4– 32.0) and 35.6% (95% CI, 32.3– 38.9), respectively, in Chinese AIS patients. The risk of stroke recurrence and combined vascular events were increased significantly with increasing ESRS and SPI-II scores. The ESRS and SPI-II scores had similar predictive accuracy for stroke recurrence (AUC 0.57 [95% CI 0.52– 0.64] vs 0.59 [95% CI 0.55– 0.64]) and combined vascular events (AUC 0.59 [95% CI 0.55– 0.63] vs 0.62 [95% CI 0.58– 0.66]) at 5 years.
Conclusion: In Chinese patients with AIS, both ESRS and SPI-II scores were able to stratify the risk of 5-year recurrent stroke and combined vascular events. The predictive power of the two scores were modest and a prediction model suitable for Chinese IS populations is needed.
Keywords: Essen Stroke Risk Score, stroke prognosis instrument II, recurrent stroke, long-term risk prediction
Background
The cumulative risk of stroke recurrence at 1 year after first-ever acute ischemic stroke (AIS) was 4%-12%,1–3 which decreased annually by 5% after the second year, but the incidence of cardiovascular death due to stroke increased annually.4 Stroke has a high recurrence rate, and the risk of disability and death following recurrence is 9.4 times greater than that of initial stroke.5–7 Therefore, in clinical practice, identification of patients at high risk for stroke recurrence is key to both inpatient and outpatient treatment. The risk prediction score is an important tool for stratifying patients based on the risk of future cerebrovascular events and for selecting effective preventive treatment. The use of risk prediction scores to identify high-risk patients is essential to optimize cost-benefit relationship under the pressure of ever-tightening healthcare budgets.
At present, there are only a few predictive scores to predict patients at high risk of stroke recurrence. The Essen Stroke Risk Score (ESRS) and the stroke prognosis instrument II (SPI-II) scales are simple, feasible and easy to use clinically, which have been well validated in stroke patients in Western countries.8–11 However, given the differences in environmental factors, genetic background, living habits, hygiene level, and treatment strategies between Chinese and Western ethnic groups, the predictive value of these scales in Chinese stroke patients needs to be further confirmed. In addition, previous clinical studies mostly investigate the predictive value of ESRS and SPI-II for short-term stroke recurrence within one year, there is a lack of studies that evaluate the value of these two scores in predicting long-term risk of recurrence stroke. Due to the fact that stroke is characterized by a high rate of long-term recurrence, validation of risk prediction scores that have good predictive performance and can be used to quantify the risk of long-term stroke recurrence could facilitate the development of active and effective secondary prevention measures in high-risk population, thus preventing stroke recurrence effectively. Therefore, the aim of this study was to validate the ESRS and SPI-II in a prospective cohort study of Chinese patients with AIS for the prediction of long-term risk of recurrent stroke.
Subjects and Methods
Study Population
A detailed patient recruitment flowchart is illustrated in Figure 1. Participants were diagnosed with non-atrial fibrillation AIS, and hospitalized in the Department of Neurology of our hospital from December 2012 to June 2016 were recruited consecutively. The study was approved by the Institutional Review Board (IRB) of Beijing Tiantan Hospital (IRB No. KY2014-023-02). Informed consent was obtained from patients or their legal relatives before participating in this study.
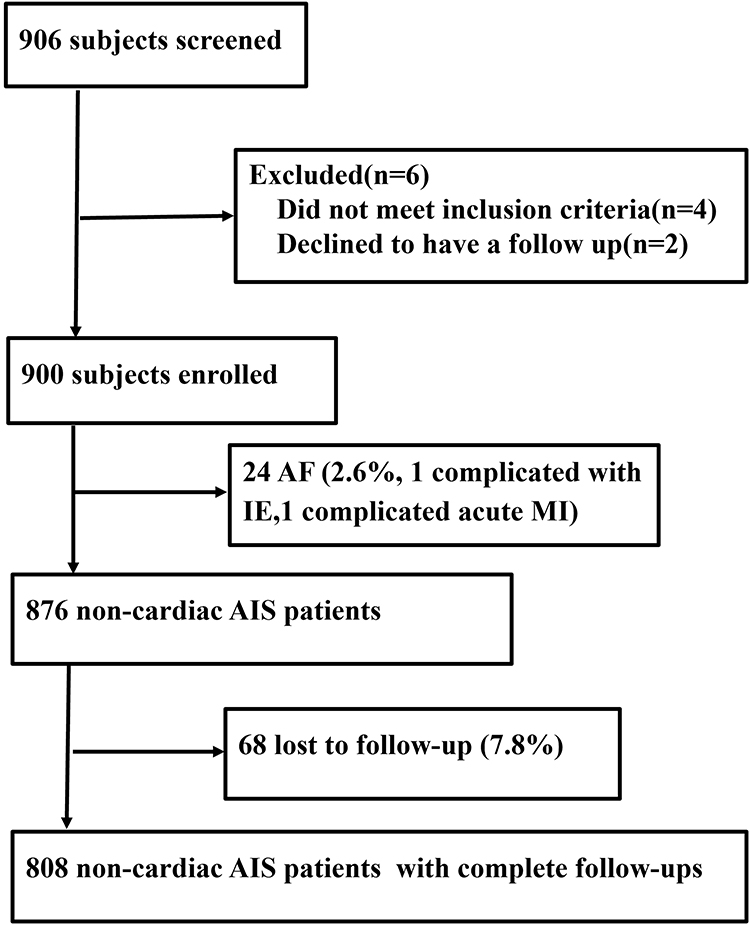 |
Figure 1 Flowchart of the subject enrollment. Abbreviations: AF, atrial fibrillation; MI, myocardial infarction. |
Inclusion criteria were: 1) patients who were hospitalized and were >18 years of age; 2) clinical diagnosis of AIS, which was defined according to the WHO diagnostic criteria;12 3) the diagnosis was confirmed by magnetic resonance imaging. Exclusion criteria were: 1) non-cerebrovascular disease events; 2) silent stroke; 3) patients who refused to participate in the study.
Data Collection
1) Baseline data: baseline demographic characteristics, such as sex, age, height, and weight. 2) Vascular risk factors: smoking history, history of hypertension, diabetes, peripheral arterial disease, cerebral infarction or transient ischemic attack, myocardial infarction, combined cardiovascular diseases (coronary heart disease, valvular heart disease, cardiomyopathy, congestive heart failure). 3) Neurologic deficit severity, measured using the National Institutes of Health Stroke Scale (NIHSS).13
ESRS and SPI-II Scores
The patients completed the ESRS and SPI-II scores within 7 days of admission. According to the ESRS scores, patients were divided into a low-risk group (0–2 points, annual risk of recurrent stroke, <4%) and a high-risk group (3–9 points).14 According to the SPI-II scores, patients were divided into a low-risk group (0–3 points, two-year risk for recurrent stroke or death, 10%), a medium-risk group (4–7 points, two-year risk for recurrent stroke or death, 19%) and a high-risk group (8–15 points, two-year risk for recurrent stroke or death, 31%).10 These 2 scores were calculated as shown in Table S1.
Follow-Up and Outcome Assessment
All enrolled patients completed at least 60 months of follow-up. Information on functional status, such as NIHSS score and modified Rankin scale score, and clinical outcomes was collected. Clinical outcomes included: 1) recurrent stroke was defined as a newly diagnosed ischemic stroke in a patient, confirmed by MRI; 2) combined vascular events, defined as any event including recurrent stroke, myocardial infarction and cardiovascular death. Follow-up was conducted via telephone interviews by a professionally trained and qualified staff.
Statistical Analysis
Continuous variables are presented as mean ± standard deviation (SD) or median (interquartile range, IQR), categorical variables are presented as proportions. Comparisons between the two groups were made using independent samples t test or Mann–Whitney test, and chi-square test, or Fisher’s exact test. The Kaplan-Meier (KM) method was used to generate survival curves of stroke recurrence in different subgroups stratified by the ESRS and SPI-II scores, and the differences in the survival curves between groups were compared using the log rank test. The ability of ESRS and SPI-II scores to predict the risk of recurrent stroke/combined vascular events was assessed using time-dependent receiver operating characteristic (ROC) curves, and the area under the ROC curve (AUC) was calculated, 95% confidence interval (CI) of the AUC was estimated with 1000 bootstrap samples. The statistical analysis was performed with SPSS 22.0 software and R 4.1.2 software, and a two-sided P<0.05 was considered statistically significant.
Results
Patient Characteristics and Follow-Up Results
Among these 876 eligible patients included in the study, 808 (92.2%) patients completed the follow-up, 68 patients (7.8%) lost to follow-up. The univariate analysis displayed that previous stroke or cerebral ischemia, coronary heart disease and higher ESRS and SPI-II scores were the influence factors for the recurrence of stroke (Table 1). After 60 months of follow-up, recurrent stroke occurred in 212 (26.2%) patients. Other vascular events (including myocardial infarction, pulmonary embolism, peripheral artery disease and cardiovascular death) occurred in 163 (20.1%), combined vascular events occurred in 279 (34.5%) patients.
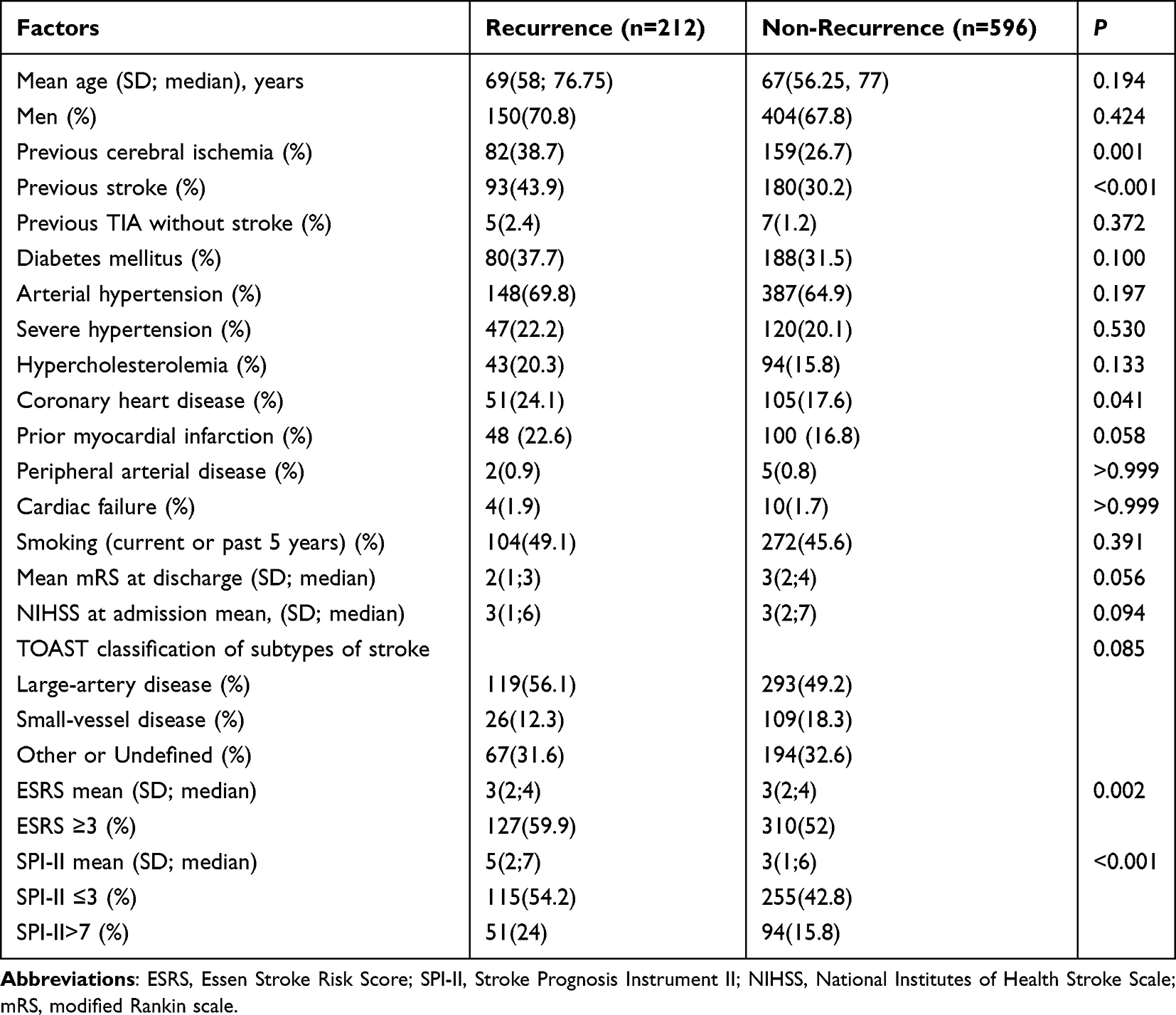 |
Table 1 Baseline Characteristics of Patients Between Recurrence Group and Non-Recurrence Group |
Prospective Evaluation of the ESRS and SPI-II Scores
In the 5-year follow-up cohort, the KM estimate for cumulative incidence of stroke recurrence was 28.7% (95% CI, 25.4–32.0) and the combined vascular events were 35.6% (95% CI, 32.3–38.9).
On stratification by the ESRS score (Figure 2), the KM estimate for cumulative incidence of stroke recurrence was 23.7% (95% CI, 19.2–28.2) in the low-risk group (<3 points), and 33.2% (95% CI, 28.3–38.1) in the high-risk group (≥3 points). There was a steady increase in the rate of combined vascular events with increasing ESRS (Table S2).
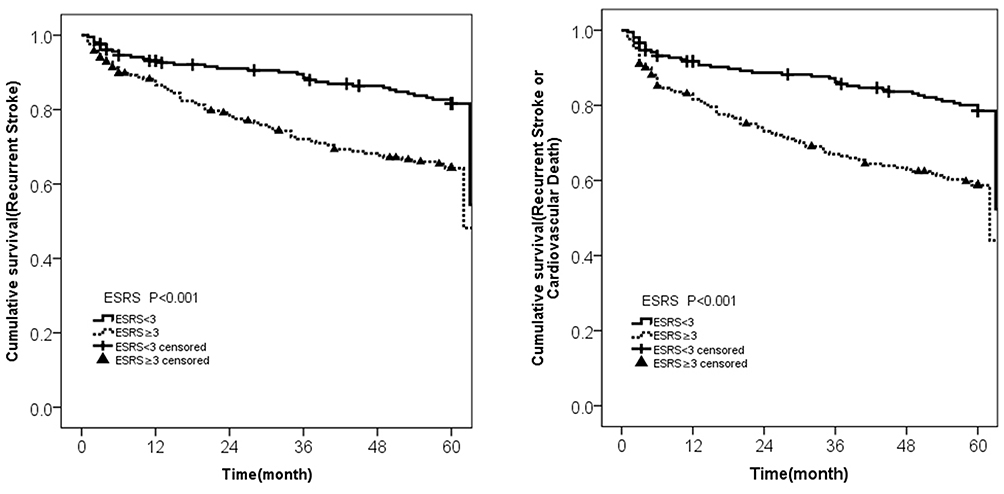 |
Figure 2 Kaplan-Meier curve of survival free of recurrent stroke and combined vascular events stratified by ESRS<3 versus ≥3 (n=437). |
On stratification by the SPI-II score (Figure 3), the KM estimate for cumulative incidence of stroke recurrence was 23.3% (95% CI, 19.2–27.4) in the low-risk group (0–3 points), 31.9% (95% CI, 25.2–38.2) in the medium-risk group (4–7 points), and 41.7% (95% CI, 32.7–50.7) in the high-risk group (8–15 points). For combined vascular events, a steady increase was likewise observed with increasing SPI-II (Table S3).
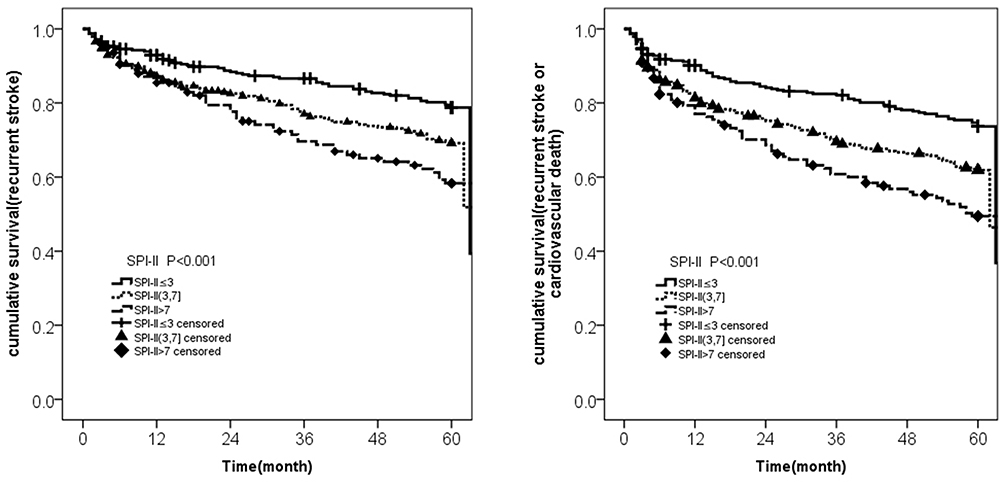 |
Figure 3 Kaplan-Meier curve of survival free of recurrent stroke and combined vascular events stratified by SPI-II≤3 versus 3<SPI-II≤7 (n=225) versus SPI-II>7 (n=145). |
Predictive Value of the ESRS and SPI-II Scores for Stroke Recurrence and Combined Vascular Events
The predictive value of these two scores for stroke recurrence and combined vascular events at 1–5 years is shown in Table 2. For the stroke recurrence at 5 years, the AUC of ESRS and SPI-II was 0.57 (95% CI 0.52–0.64) and 0.59 (95% CI 0.55–0.64), respectively. For the combined vascular events, the AUC of the two scores was 0.59 (95% CI 0.55–0.63) and 0.62 (95% CI 0.58–0.66), respectively.
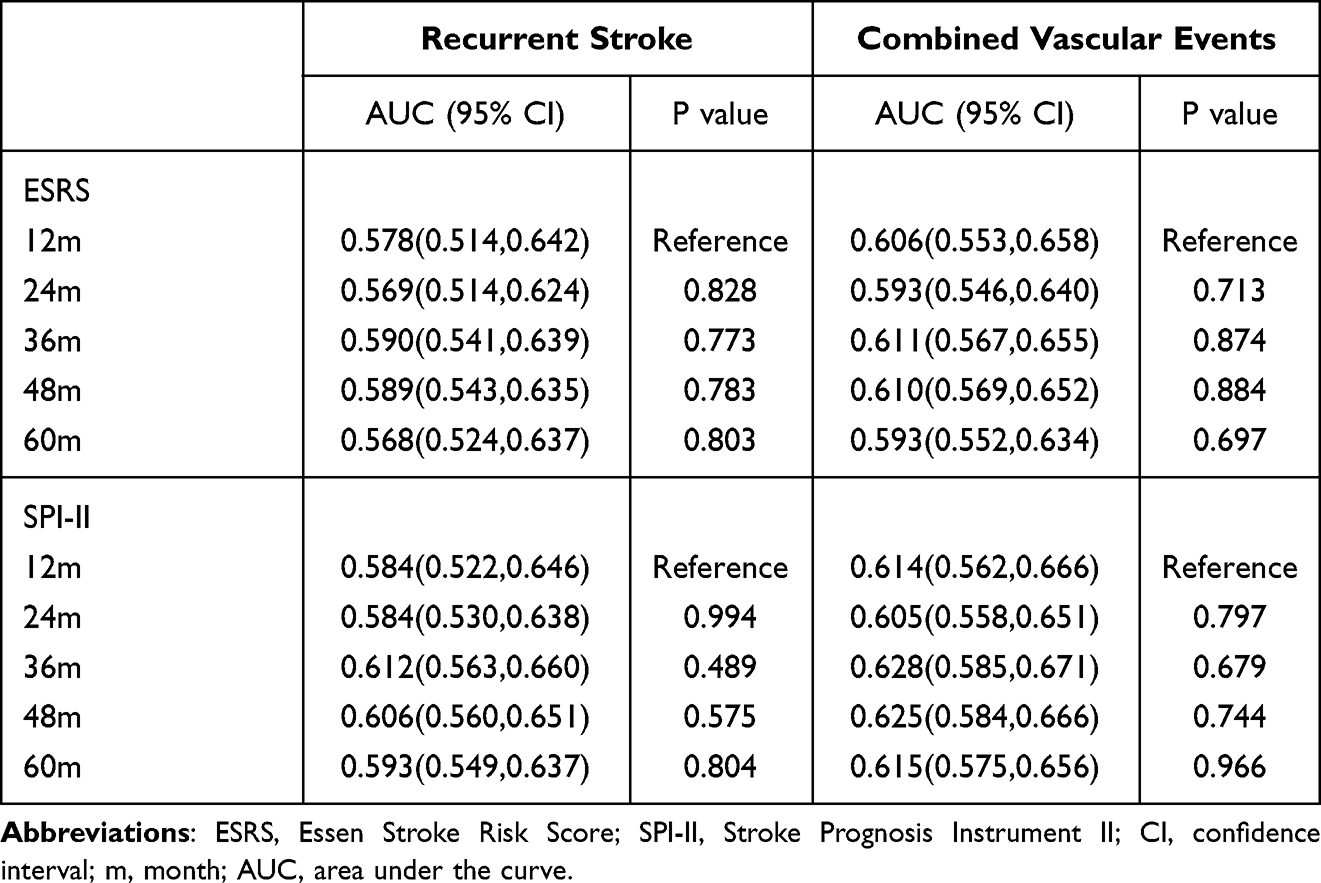 |
Table 2 Predictive Accuracy of ESRS and SPI-II Scores for Recurrent Stroke and Combined Events at 1–5 Years |
The sensitivity, specificity, positive predictive values, and negative predictive values of the ESRS and SPI-II for recurrent stroke and combined vascular events at 5 years are shown in Table 3.
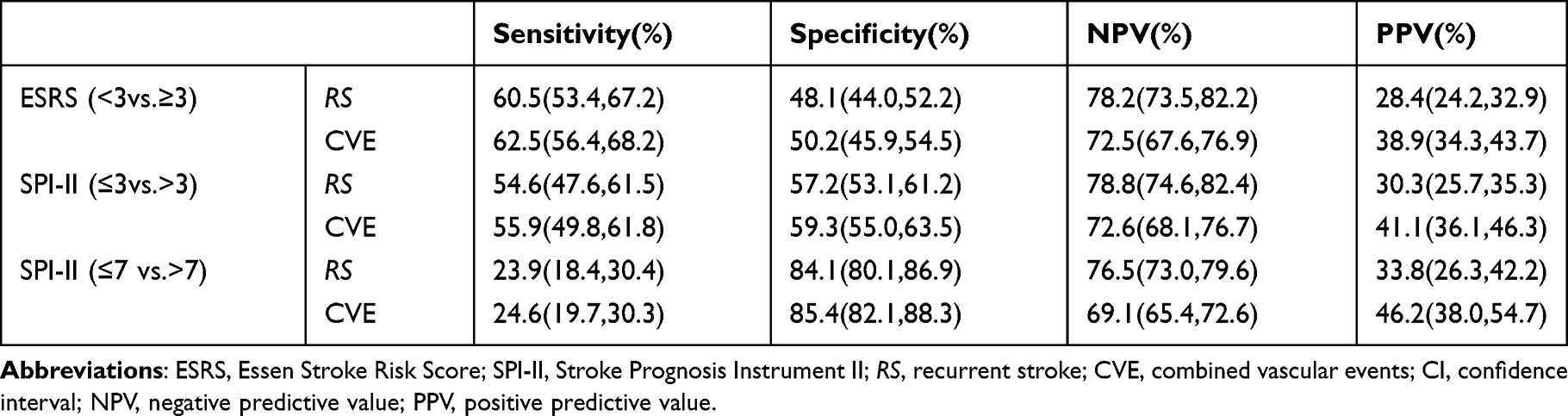 |
Table 3 Predictive Accuracy of the ESRS and SPI-II at Recommended Cut Points for Five-Year Recurrent Stroke or Combined Vascular Events with 95% CI |
Discussion
This study validated the efficacy of ESRS and SPI-II in predicting the long-term follow-up of Chinese AIS cohort by evaluating stroke recurrence and combined vascular events. The results showed that after 5 years of follow-up, the cumulative stroke recurrence rate was 28.7% and the combined vascular events rate was 35.6%, which was higher than previously reported.15 Both ESRS and SPI-II scores were able to stratify the risk of recurrent stroke and the combined vascular events.
Evaluation of a prediction model for ischemic stroke recurrence requires consideration of clinical utility and extrinsic realism, indicating that the predictive model should have clinical significance and application value, and should be easy to use, ie, the variables included in the model should be easy to collect in the clinical setting. ESRS is a risk factor-based prediction model that was developed from the data of the stroke subgroup from the clopidogrel versus aspirin among non-atrial fibrillation (AF) patients at risk of ischemic events (CAPRIE) trial.9,16 ESRS has been externally validated in two observational studies and the European Stroke Prevention Study II (ESPS-2).17–19 The SPI-II was developed on the basis of the original SPI-I score. New predictive variables identified in the European Stroke Prevention Study II (ESPS-2) are incorporated into the SPI-II score.20 The SPI-II has been validated in 3 independent cohorts.10 In the present study, the results showed that the ESRS and SPI-II scores could be applied to stratify the risk of stroke recurrence and combined events.
In the original ESRS trial, ESRS stratifies the 1-year risk of ischemic stroke recurrence, a score of 0–2 points is considered low risk, with annual stroke recurrence risk of ≤4%, a score of 3–6 points is high risk, with annual stroke recurrence risk of approximately 7–9%, and a score of ≥ 6 is very high risk, with annual stroke recurrence risk of up to 11%. A prospective observational cohort study (Systemic Risk Score Evaluation in Ischemic Stroke Patients (SCALA)) conducted in Germany validate the ESRS score, further analysis was performed after 17.5 months of follow-up and found that patients with an ESRS ≥ 3 had a significantly higher risk of recurrent stroke or cardiovascular death than those with an ESRS < 3 (9.7% vs 5.1%; odds ratio (OR): 2.00), suggesting that high-risk patients with ESRS ≥ 3 should be treated with a intensified secondary prevention strategy.18 Similarly, in the original SPI-II derivation study, SPI-II assigns patients to 3 risk groups (low, medium, high) based on the risk of stroke recurrence and death, the 2-year risk of recurrent stroke or death was 10%, 19%, and 31%, respectively for low-, medium-, and high-risk groups. In the present study, we analyzed the ability of ESRS and SPI-II scores in stratifying the risk of events within 5 years, the results showed that the 5-year risk of stroke recurrence or combined vascular events increased significantly with increasing ESRS and SPI-II scores, which are consistent with the above-mentioned previous studies. Patients at high risk identified by a high ESRS and SPI-II do have a significantly elevated risk of stroke recurrence. Therefore, it makes sense to identify these patients for an intensified therapy.
Previous studies have shown that high-risk patients with an ESRS score ≥3 accounted for 50% of all patients in the CAPRIE study, 58% in the SCALA study. And high-risk patients with annual recurrence risk of greater than 4% accounted for more than 70% of all patients in the REduction of Atherothrombosis for Continued Health (REACH) registry study. In the present study, patients with a baseline ESRS score ≥3 accounted for 54% of all patients included. From the aforementioned findings, it can be seen that more than 50% of the study populations are at high risk for recurrent stroke or cardiovascular events. The ESRS and SPI-II scores can help clinicians identify high risk patients early, and determine more active secondary prevention measures. Previous retrospective studies16,19 showed that for patients with an increased risk of stroke recurrence evaluated according to ESRS scores, dipyridamole combined with aspirin or clopidogrel alone could obviously reduce the risk of stroke recurrence compared with aspirin alone. Therefore, the use of predictive scores to stratify patients according to the risk of recurrent stroke may further optimize treatment and modify risk factors for stroke.
In the present study, the AUC value was calculated for the ESRS and SPI-II scores. The ability of these two scores in predicting stroke recurrence and combined vascular events at 1-, 2-, 3-, 4-, 5-year follow-ups were analyzed and compared. The results showed that the ESRS score had AUC values of 0.58 and 0.61, respectively, for prediction of stroke recurrence and combined vascular events at 1 year, which are similar to the findings from the SCALA study (AUC, 0.56, 0.61),14 the REACH study (AUC, 0.56, 0.60),16 and China National Stroke Registry (CNSR) study (AUC, 0.59, 0.60),21 indicating that predictive value of the ESRS score is not high. A previous study showed that the SPI-II score had an AUC of 0.63 for prediction of stroke or death within 2 years in independent research population.10 Another study11 evaluated the performance of the SPI-II in predicting of 1-year risk of stroke or death in 5575 AIS patients, and further compared the predictive accuracy of the SPI-II in predicting different outcome events, they found that the SPI-II had an AUC of 0.55 for predicting recurrent stroke without death, 0.62 for predicting recurrent stroke or death, and 0.64 for predicting death, suggesting that the SPI-II score has poor predictive ability for the recurrence of isolated stroke, but can effectively identify stroke patients at high risk of death. In the present study, the SPI-II score had AUC values of 0.58 and 0.61, respectively, for predicting recurrent stroke or combined events, which also supports the above-mentioned findings. Previous studies have verified and compared the predictive accuracy of the ESRS, SPI-II, Life-Long after Cerebral Ischemia (LiLAC) score22 and Hankey score,23 and found that these four scores had similar predictive value, but none of these scores reached an AUC value above 0.70.
In addition, this study verified the performance of ESRS and SPI-II scores in predicting 5-year risk of stroke recurrence and combined vascular events in Chinese AIS patients. Results from time-dependent ROC suggested that ESRS and SPI-II scores had similar predictive value for 5-year stroke recurrence or combined vascular events, with an AUC of 0.57 and 0.59, respectively. These results are consistent with a previous study24 showing that ESRS and SPI-II could not predict the risk of early recurrence. The previous study24 only included patients with minor stroke (NIHSS score of ≤5), while in this study, AIS patients with different degrees of severity were included, indicating the broader applicability of these two scores.
The reasons for the poor prediction performance of the two scales in the 5-year follow-up of this study are as follows: the accuracy of predicting stroke recurrence depends on a variety of clinical risk factors, and the baseline characteristics of the included patients are directly related to stroke recurrence. For example, this study lacks the inclusion of cerebrovascular imaging examinations closely related to recurrence,25 the evaluation of the stability of intracranial and extracranial large artery plaque,26 the compliance with post-stroke secondary prevention and the patient’s education, economic situation, and psychological factors,27–29 which all play an important role in stroke recurrence. Besides, that those two scales were developed in Western countries and failed external validation to a different population and longer time-frames.
This study has two major limitations. First, this is a single-center study, selection bias may exist, our hospital is located in an urban area, has a relatively high level of outpatient or inpatient care compared to prefecture-level and county-level hospitals. Therefore, rates of recurrent stroke and vascular events may be underestimated in this study. Additionally, our stroke center is an advanced stroke center, so the vast majority of hospitalized patients have severe AIS, and significant proportion of patients with mild AIS are not included. Second, follow-up was conducted via telephone interviews or questionnaires, information was obtained from patients or family physicians, relatives or caregivers. Therefore, it was not possible to complete the follow-up questionnaire in all cases.
Conclusions
Our findings suggest that both ESRS and SPI-II scores were able to stratify the risk of 5-year recurrent stroke and the combined vascular events in Chinese AIS patients. However, both scales did not perform well in predicting the 5-year outcome of stroke recurrence, a more accurate tools for predicting long-term prognosis of vascular event are needed.
Abbreviations
AIS, acute ischemic stroke; ESRS, Essen Stroke Risk Score; SPI-II, stroke prognosis instrument II scale; NIHSS, National Institutes of Health Stroke Scale; KM, Kaplan-Meier method; ROC, receiver operating characteristic curve; AUC, area under the ROC curve.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the ethics committee of Beijing Tiantan Hospital, Capital Medical University, and followed the principles of the Declaration of Helsinki. Informed consents to participate in this study were obtained from all patients.
Acknowledgments
We gratefully appreciate all the participants and staff for their contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by the National Science and Technology Major Project (2017ZX09304018); CAMS Innovation Fund for Medical Sciences (2019-I2M-5-029); Beijing Municipal Committee of Science and Technology (Z201100005620010); Beijing key clinical specialty; National Key Research and Development Program of China (Grant No. 2018YFC1312200 /2018YFC1312204).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Hankey GJ. Long-term outcome after ischaemic stroke/transient ischaemic attack. Cerebrovasc Dis. 2003;16:14–19. doi:10.1159/000069936
2. Chen Z-M. CAST: randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. CAST (Chinese Acute Stroke Trial) Collaborative Group. Lancet. 1997;349(9066):1641–1649. doi:10.1016/S0140-6736(97)04010-5
3. Liu M, Wu B, Wang WZ, Lee LM, Zhang SH, Kong LZ. Stroke in China: epidemiology, prevention, and management strategies. Lancet Neurol. 2007;6(5):456–464. doi:10.1016/S1474-4422(07)70004-2
4. Touzé E, Varenne O, Chatellier G, Peyrard S, Rothwell PM, Mas JL. Risk of myocardial infarction and vascular death after transient ischemic attack and ischemic stroke: a systematic review and meta-analysis. Stroke. 2005;36(12):2748–2755. doi:10.1161/01.STR.0000190118.02275.33
5. Feng W, Hendry RM, Adams RJ. Risk of recurrent stroke, myocardial infarction, or death in hospitalized stroke patients. Neurology. 2010;74(7):588–593. doi:10.1212/WNL.0b013e3181cff776
6. Dhamoon MS, Sciacca RR, Rundek T, Sacco RL, Elkind MS. Recurrent stroke and cardiac risks after first ischemic stroke: the Northern Manhattan Study. Neurology. 2006;66(5):641–646. doi:10.1212/01.wnl.0000201253.93811.f6
7. Hankey GJ, Jamrozik K, Broadhurst RJ, et al. Long-term risk of first recurrent stroke in the Perth Community Stroke Study. Stroke. 1998;29(12):2491–2500. doi:10.1161/01.str.29.12.2491
8. Weimar C, Benemann J, Michalski D, et al.; German Stroke Study Collaboration. Prediction of recurrent stroke and vascular death in patients with transient ischemic attack or nondisabling stroke: a prospective comparison of validated prognostic scores. Stroke. 2010;41(3):487–493. doi:10.1161/STROKEAHA.109.562157
9. CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet. 1996;348(9038):1329–1339. doi:10.1016/s0140-6736(96)09457-3
10. Kernan WN, Viscoli CM, Brass LM, et al. The stroke prognosis instrument II (SPI-II): a clinical prediction instrument for patients with transient ischemia and nondisabling ischemic stroke. Stroke. 2000;31(2):456–462. doi:10.1161/01.str.31.2.456
11. Navi BB, Kamel H, Sidney S, Klingman JG, Nguyen-Huynh MN, Johnston SC. Validation of the stroke prognostic instrument-II in a large, modern, community-based cohort of ischemic stroke survivors. Stroke. 2011;42(12):3392–3396. doi:10.1161/STROKEAHA.111.620336
12. WHO MONICA Project Principal Investigators. The World Health Organization MONICA Project (monitoring trends and determinants in cardiovascular disease): a major international collaboration. J Clin Epidemiol. 1988;41(2):105–114. doi:10.1016/0895-4356(88)90084-4
13. Lyden P, Brott T, Tilley B, et al. Improved reliability of the NIH stroke scale using video training. NINDS TPA stroke study group. Stroke. 1994;25(11):2220–2226. doi:10.1161/01.str.25.11.2220
14. Weimar C, Goertler M, Röther J, et al.; SCALA Study Group. Systemic risk score evaluation in ischemic stroke patients (SCALA): a prospective cross sectional study in 85 German stroke units. J Neurol. 2007;254(11):1562–1568. doi:10.1007/s00415-007-0590-z
15. Mohan KM, Wolfe CDA, Rudd AG, et al. Risk and cumulative risk of stroke recurrence: a systematic review and meta-analysis. Stroke. 2011;42(5):1489–1494. doi:10.1161/STROKEAHA.110.602615
16. Diener HC, Ringleb PA, Savi P. Clopidogrel for the secondary prevention of stroke. Expert Opin Pharmacother. 2005;6(5):755–764. doi:10.1517/14656566.6.5.755
17. Weimar C, Diener HC, Alberts MJ, et al.; REduction of Atherothrombosis for Continued Health Registry Investigators. The Essen stroke risk score predicts recurrent cardiovascular events: a validation within the REduction of Atherothrombosis for Continued Health (REACH) registry. Stroke. 2009;40(2):350–354. doi:10.1161/STROKEAHA.108.521419
18. Weimar C, Goertler M, Röther J, et al.; SCALA Study Group. Predictive value of the Essen Stroke Risk score and Ankle Brachial Index in acute ischaemic stroke patients from 85 German stroke units. J Neurol Neurosurg Psychiatry. 2008;79(12):1339–1343. doi:10.1136/jnnp.2008.146092
19. Diener HC. Modified-release dipyridamole combined with aspirin for secondary stroke prevention. Aging Health. 2005;1:19–26. doi:10.2217/1745509X.1.1.19
20. Viscoli CM, Brass LM, Kernan WN, Sarrel PM, Suissa S, Horwitz RI. A clinical trial of estrogen-replacement therapy after ischemic stroke. N Engl J Med. 2001;345(17):1243–1249. doi:10.1056/NEJMoa010534
21. Meng X, Wang Y, Zhao X, et al. Validation of the Essen Stroke Risk Score and the stroke prognosis instrument II in Chinese patients. Stroke. 2011;42(12):3619–3620. doi:10.1161/STROKEAHA.111.624148
22. van Wijk I, Kappelle LJ, van Gijn J, et al.; LiLAC study group. Long-term survival and vascular event risk after transient ischaemic attack or minor ischaemic stroke: a cohort study. Lancet. 2005;365(9477):2098–2104. doi:10.1016/S0140-6736(05)66734-7
23. Hankey GJ, Slattery JM, Warlow CP. Transient ischaemic attacks: which patients are at high (and low) risk of serious vascular events? J Neurol Neurosurg Psychiatry. 1992;55(8):640–652. doi:10.1136/jnnp.55.8.640
24. Chandratheva A, Geraghty OC, Rothwell PM. Poor performance of current prognostic scores for early risk of recurrence after minor stroke. Stroke. 2011;42(3):632–637. doi:10.1161/STROKEAHA.110.593301
25. Zhang J, Zhu P, Liu B, et al. Time to recurrence after first-ever ischaemic stroke within 3 years and its risk factors in Chinese population: a prospective cohort study. BMJ open. 2019;9(12):e032087. doi:10.1136/bmjopen-2019-032087
26. Chen J, Zhao N, Ruan Y, et al. Socioeconomic status and the risk of stroke recurrence in Chinese patients. Neuroepidemiology. 2019;53(3–4):180–186. doi:10.1159/000501276
27. Han J, Mao W, Ni J, et al. Rate and determinants of recurrence at 1 year and 5 years after stroke in a low-income population in rural China. Front Neurol. 2020;11:2. doi:10.3389/fneur.2020.00002
28. Prabhakaran S, Liebeskind DS, Cotsonis G, et al.; MYRIAD Investigators. Predictors of early infarct recurrence in patients with symptomatic intracranial atherosclerotic disease. Stroke. 2021;52(6):1961–1966. doi:10.1161/STROKEAHA.120.032676
29. Kelly PJ, Camps-Renom P, Giannotti N, et al. A risk score including carotid plaque inflammation and stenosis severity improves identification of recurrent stroke. Stroke. 2020;51(3):838–845. doi:10.1161/STROKEAHA.119.027268
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.