Back to Journals » Cancer Management and Research » Volume 11
The Prediction Of Epidermal Growth Factor Receptor Mutation And Prognosis Of EGFR Tyrosine Kinase Inhibitor By Serum Ferritin In Advanced NSCLC
Received 17 May 2019
Accepted for publication 24 August 2019
Published 7 October 2019 Volume 2019:11 Pages 8835—8843
DOI https://doi.org/10.2147/CMAR.S216037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Zhen Wu, Yu Dai, Liang-An Chen
Respiratory Department, Chinese PLA General Hospital, Beijing, People’s Republic of China
Correspondence: Liang-An Chen
Respiratory Department of Chinese PLA General Hospital, IMB 16th Floor, Room 16-104 28, Fuxing road, Haidian district, Beijing 100853, People’s Republic of China
Tel +86 10 6693 6184
Email [email protected]
Purpose: To investigate the association between level of serum ferritin (SF) and epidermal growth factor receptor (EGFR) mutations and to analyse the impact of SF level on survival times in advanced non-small-cell lung cancer (NSCLC) patients taking EGFR tyrosine kinase inhibitors (EGFR-TKIs).
Methods: A total of 301 patients who were admitted to the Chinese PLA general hospital from August 2015 to August 2017 were enrolled. The association between tumour markers, including SF, CEA, and EGFR mutation, and their impact on the prognosis of patients taking EGFR-TKIs was investigated.
Results: In all patients, the percentage of patients with EGFR mutations was 52.5% (158/301). EGFR mutations were more likely to be detected in younger (<60 years old), adenocarcinoma patients, non-smokers, women, CEA≥5 μg/L and serum ferritin ≥129 μg/L for females or ≥329 μg/L for males (p<0.05). Increased serum ferritin was an independent factor for predicting EGFR mutations (odds ratio (OR)=4.593, 95% CI (2.673–7.890); P <0.001), and an area under curve (AUC) of 0.711 was shown to predict EGFR mutations with a sensitivity of 81.7% and a specificity of 65.2% in women. Sensitivity increased to 91.1% when combining SF and CEA in all patients. SF was also an independent factor (HR=3.531, 95% CI (2.288–5.448); P<0.001) for predicting progression-free survival (PFS) of patients on EGFR-TKIs, analysed by a Cox proportional hazard model, as PFS was shorter in patients with higher SF (15.0 mo. (SF < 129 μg/L for females or <329 for males) vs 10.0 mo. (129–258 μg/L for females or 329–658 μg/L for males) vs 7.3 mo. (>258 μg/L (>258 μg/L for females or >658 μg/L for males) p<0.001).
Conclusion: SF was a significant predictor of EGFR mutation with moderate diagnostic accuracy, and combining SF and CEA increased the diagnostic sensitivity and specificity for EGFR mutations. SF was also useful for predicting survival in EGFR-TKIs.
Keywords: EGFR mutation, serum ferritin, EGFR-TKI, lung cancer, prognosis
Introduction
Lung cancer is the leading cause of cancer-related mortality and morbidity worldwide, with 154,050 related-deaths in America every year.1 Non-small cell lung cancer accounts for more than 80% of these cases. Although the 5-year relative survival rate of lung cancer in all stages remains at only 18%, precise molecular-targeted treatment significantly promotes the overall survival of lung cancer patients, especially for NSCLC.2,3 EGFR-TKI is the most common targeted therapy for advanced NSCLC. Tissue biopsy was regarded as a “standard procedure” for molecular detection to choose the proper therapy and predict the prognosis. However, tumour tissue is often not available due to the invasiveness of the procedure and the failure to get enough tumour tissue for further detection of gene variations.4 Non-invasive biomarkers to predict the status of EGFR mutation and prognosis are warranted. Previous studies have demonstrated the relationship between EGFR gene mutation and serum CEA level in patients with lung adenocarcinomas, and the rate of EGFR alteration is increased as the serum CEA level increases.5,6 Many tumour biomarkers, including serum CEA, CYFRA21-1 and NSE levels, are also related to the efficacy of EGFR-TKIs.6–8 However, the diagnostic value of non-invasive biomarkers for EGFR mutations remains unclear. In the current retrospective study, the value of serum ferritin in diagnosing EGFR variations and predicting progression-free survival and overall survival in patients receiving first-line EGFR-TKIs was investigated.
Materials And Methods
Patients
A total of 589 advanced NSCLC patients seen between August 2015 and August 2017 comprised the current retrospective study population. The inclusion criteria were as follows: 1) having a new diagnosis of NSCLC and not receiving any anticancer therapy before; 2) undergoing the detection of EGFR mutation in tumour tissue by next-generation sequencing; 3) having complete case and follow-up data; and 4) the patient or a family member signing informed consent for the publication of case details. Among the 589 patients, all of these criteria were met in 301 patients. Therefore, we selected 301 patients for this study. The research was approved by the ethics committee of the Chinese PLA general hospital, and patients’ informed consent allowed their clinical data to be used for research purposes.
The clinical data of these patients are summarized in Table 1. This study included 150 females and 151 males, with a mean age of 60 years. One hundred and sixty-eight patients were never-smokers, while the remaining 133 patients were former or current smokers. Patients with adenocarcinoma accounted for 79% (238/301), and 59% of patients had distant organ metastasis. The Eastern Cooperative Oncology Group (ECOG) score of every patient was no more than 2 points.
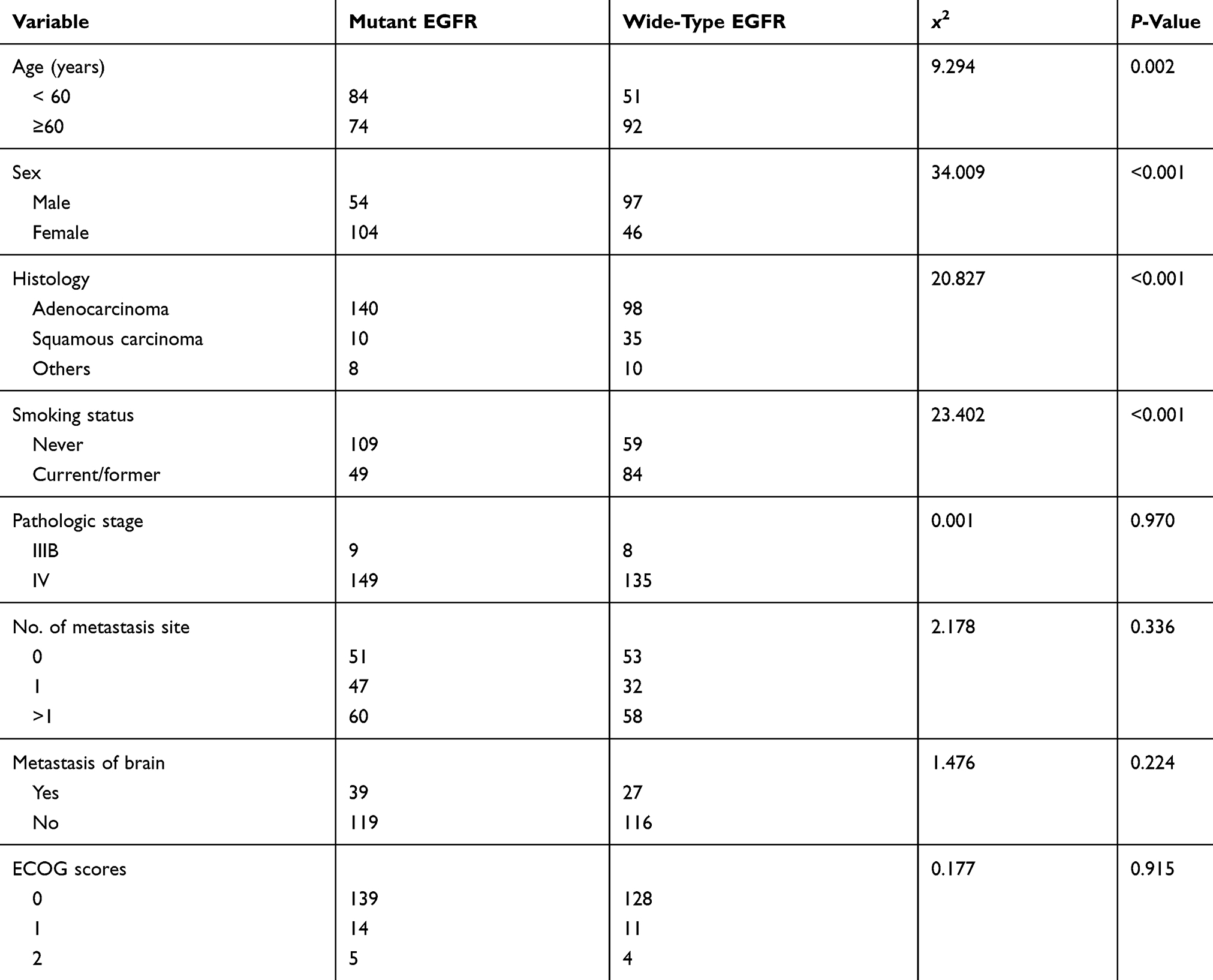 |
Table 1 Comparison Of Clinicopathologic Features Between Wild-type EGFR And Mutant EGFR Advanced NSCLC Patients |
Treatment And Follow-Up
According to the results of gene mutation testing with tumour tissue, patients with EGFR mutations were given a first-line EGFR-TKI, including gefitinib, erlotinib or icotinib, while patients without mutations received chemotherapy according to the guidelines’ suggestions. Follow-up was begun on the day of treatment and finished on the last day of follow-up or when the patient died. The methods of follow-up were conducted mainly by hospital visits and by telephone. The overall survival (OS) was calculated from the first day of treatment to the last day of follow-up or to patient death. The progression-free survival (PFS) was the period from the beginning of treatment to the day when progressed diseases were discovered for the first time. All of these were calculated in months. The last follow-up visit occurred in April 2019.
Statistical Methods
SPSS 22.0 statistical analysis software package (Chicago, USA) was applied for data analysis. The χ2 test was adopted for comparison of categorical variables and the diagnostic accuracies of markers. For the combinations of 2 markers, the test was considered positive if either or both exceeded the cutoff value. The Kaplan–Meier method was used to analyse the survival rate; the log rank test was applied for single-factor analysis; the Cox proportional hazard model was employed for multiple-factor analysis; and logistic analysis was used to analyse the relationship between EGFR gene mutation and multiple factors. P < 0.05 was regarded as statistically significant.
Results
Correlation Between Clinicopathological Factors And EGFR Mutations
Based on the results of the initial detection of EGFR gene mutations, a positive result was found in 158 patients (52.50%). In total, 84 EGFR mutation-positive patients (53.2%) were less than 60 years old; 104 female patients and 54 male patients were found to have EGFR mutations; 140 of them (88.61%) had adenocarcinomas, 10 (6.32%) had squamous carcinomas, 109 (69.00%) had never smoked, 49 (31.00%) were smoking or had ever smoked, and 149 (94.30%) had stage IV disease. The remaining patients had stage IIIB disease. According to the comparisons between EGFR-mutated and wild-type groups in terms of clinicopathological factors, patients aged less than 60 years, females, those with adenocarcinoma, and nonsmokers were prone to EGFR mutations (Table 1).
Relationship Between Tumour Markers And EGFR Mutations
Within 1–2 weeks before initial treatment, all these patients underwent conventional detection of tumour biomarkers, including CEA, neuron-specific enolase (NSE), cytokeratin (Cyfra21-1) and serum ferritin. The results showed that the level of CEA in EGFR-mutated patients was increased more frequently (P<0.05), whereas changes in SCC and Cyfra21-1 levels demonstrated no difference between patients with and without EGFR mutations. In all, 118 patients (74.7%) with EGFR mutations demonstrated an abnormal elevated serum ferritin level, which was more than that 53 patients (37.1%) in the wild-type group (Table 2). It was shown that EGFR mutation was significantly associated with an elevated level of serum ferritin at the time of initial diagnosis of lung cancer (p<0.001). The rates of EGFR mutation in advanced NSCLC patients with CEA level <5, 5–20, and >20 μg/L were 41.52%, 54.79%, and 62.39%, respectively (P=0.008). For patients with higher serum ferritin, the rates of EGFR mutation were also increased with increasing ferritin levels (females: 38.8%, 83.9% and 84.4% for ferritin < 129, 129–258, >258 µg/L, p<0.001; males: 25.9%, 47.7% and 48.1% for ferritin <329, 329–658, >658 µg/L, p=0.014). Logistic regression analysis was performed on the clinicopathological factors that probably influenced EGFR mutation prediction, to analyse the correlation between EGFR mutation and the levels of serum ferritin and CEA, and the results suggested that serum ferritin and CEA levels were 2 independent factors in predicting the status of EGFR gene mutation (Table 3).
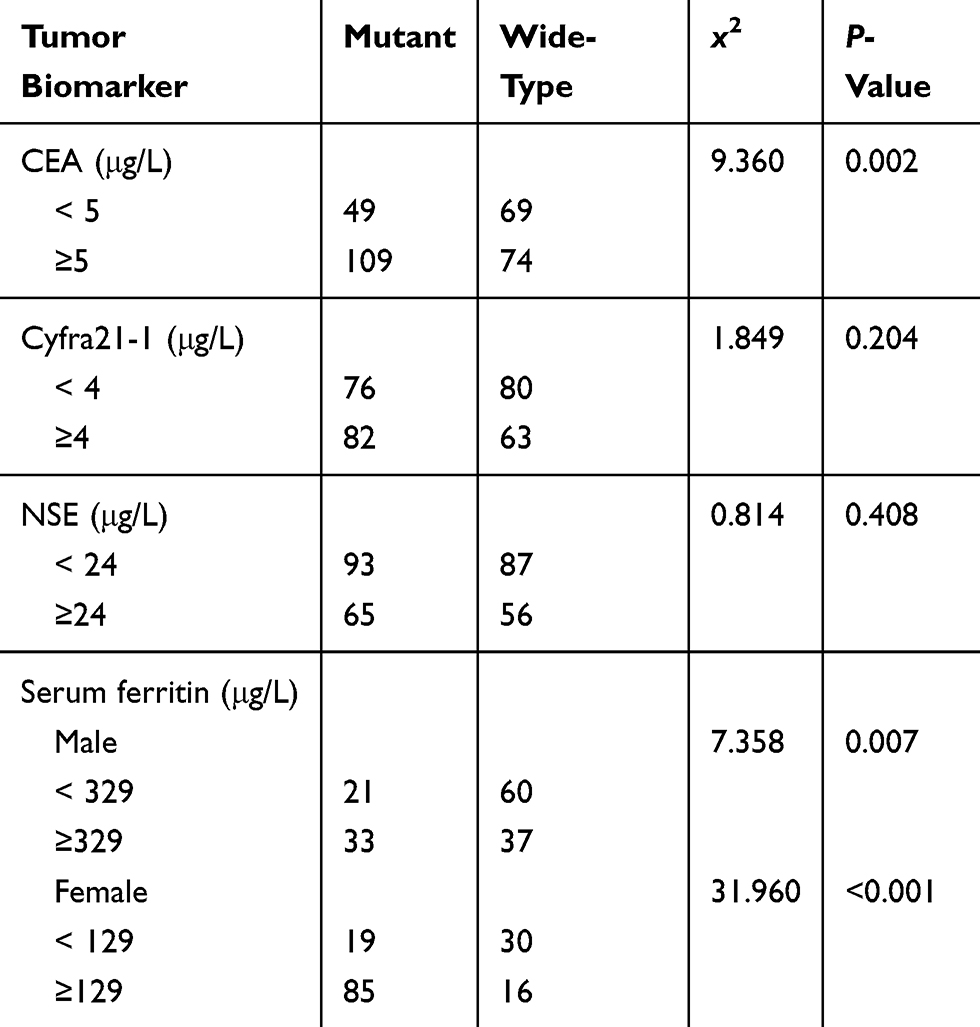 |
Table 2 Status Of EGFR Mutation And Tumor Biomarkers |
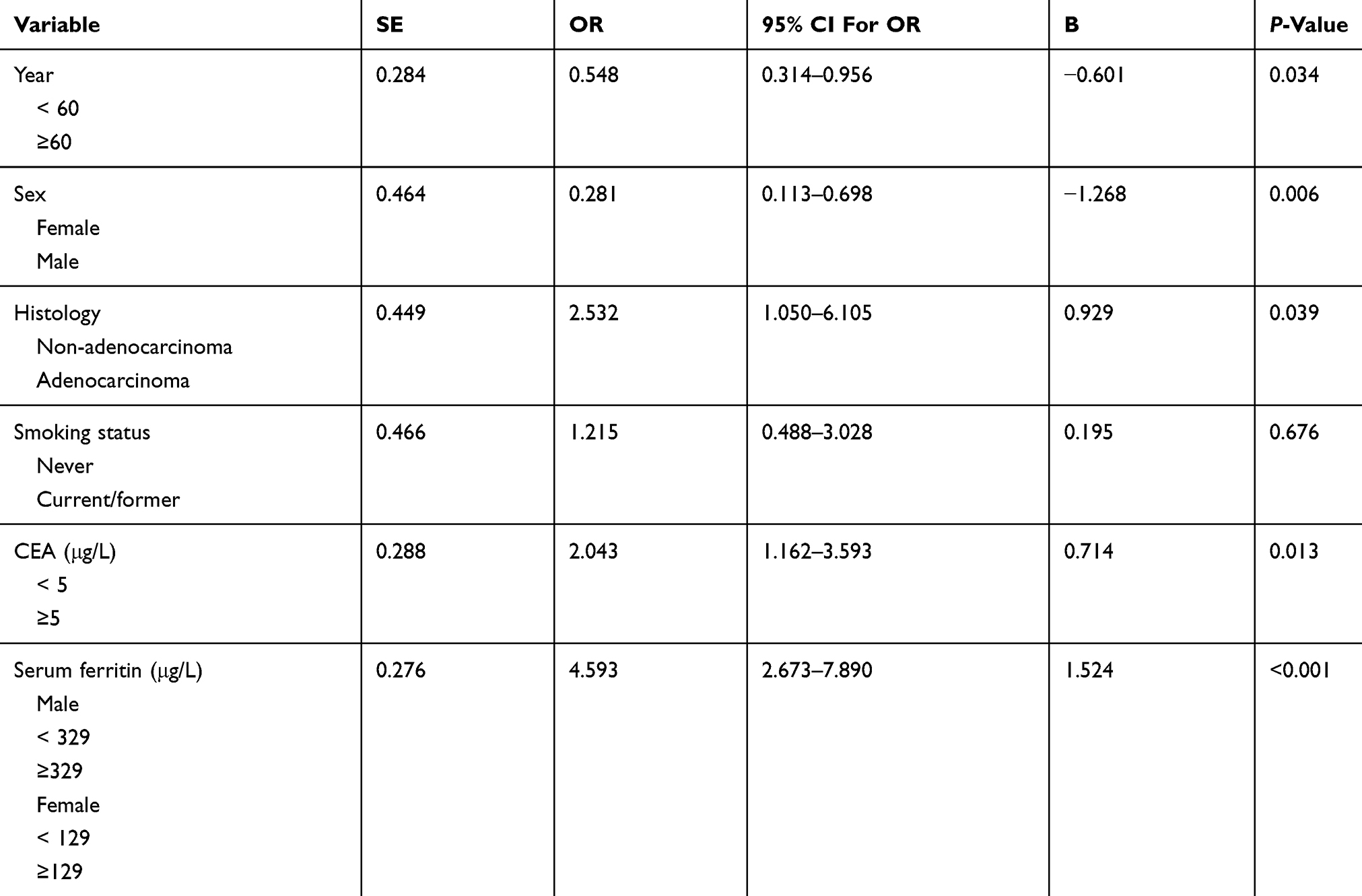 |
Table 3 Prediction Of Factors Associated With The Incidence Of EGFR Mutation With Logistic Analysis |
Diagnostic Value Of Serum Ferritin And Serum CEA For EGFR Mutations
The sensitivity, specificity and positive predictive values of each single biomarker and the combination of the 2 markers to distinguish EGFR-mutated from wild-type patients are summarized in Table 4. The optimal cutoff values of serum ferritin were 129.0 µg/L for females and 329.0 µg/L for males, while those of CEA were 5 µg/L for females and males. The AUC for serum ferritin was 0.690 (95% CI: 0.630–0.751, P=0.031), with a sensitivity of 74.7% and a specificity of 62.9%. In the subgroup of females, the AUC for serum ferritin was increased to 0.711 (95% CI: 0.617–0.804, P=0.048), with a sensitivity of 81.7% and a specificity of 65.2%. For male patients, the AUC for ferritin was decreased to 0.637 (95% CI: 0.543–0.730, P=0.048), with a sensitivity of 61.1% and a specificity of 61.9%. The AUC for CEA was 0.586 (95% CI: 0.522–0.651, P=0.033), with a sensitivity of 69.0% and a specificity of 48.3%, while it improved to 0.624, with a sensitivity of 68.3% and specificity of 56.5%, in the female group, and it decreased to 0.574, with a sensitivity of 70.4% and specificity of 44.3%, in the male group. When CEA and serum ferritin were combined, the sensitivity increased to 91.1% under the condition that the two biomarkers were detected together.
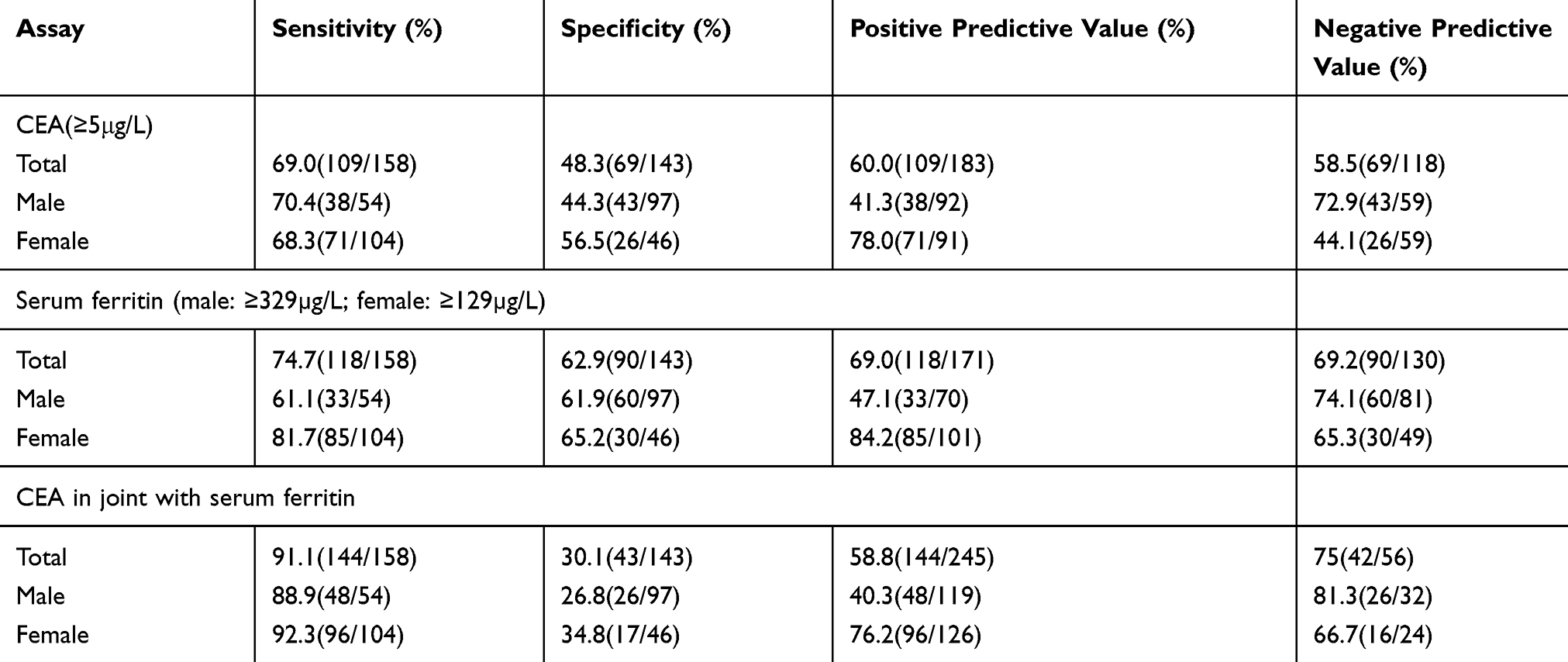 |
Table 4 Sensitivity, Specificity And Positive Predictive Value For CEA And Serum Ferritin To Diagnose EGFR Mutation |
Influence Of Serum Ferritin Level On The Survival Time Of NSCLC Patients Receiving EGFR-TKIs
A total of 158 patients with EGFR mutations received EGFR-TKIs as the initial treatment. One hundred and eighteen patients showed an increase in serum ferritin level, and 109 patients had an elevated level of CEA. The survival curve of the patients with 3 levels of serum ferritin showed that the progression-free survival (PFS) time of patients with lower pretreatment ferritin level was significantly better (15.0 mo. [ferritin < 129 µg/L for females or <329 for males] vs 10.0 mo. [129–258 µg/L for females or 329–658 µg/L for males] vs 7.3 mo. [>258 µg/L for females or >658 µg/L for males], p<0.001) (Figure 1). The PFS of patients with higher CEA was also shorter than that of patients with lower CEA (12.0 mo. vs 9.6 mo., p=0.013) (Figure 2). As demonstrated by the Cox proportional hazard model analysis, female sex (HR = 0.506; p<0.001), decreased serum ferritin (HR = 0.284; p<0.001) and lower serum CEA (HR = 0.647; p<0.001) were independent factors affecting PFS in NSCLC patients. None of the factors showed a correlation with overall survival.
 |
Figure 1 The progression-free survival (PFS) of patients receiving EGFR-TKI presented by Kaplan–Meier survival curve around a threshold of SF level < 129µg/L, 129–258µg/L and >258µg/L for female and level < 329µg/L, 329–658µg/L and >658µg/L for male. |
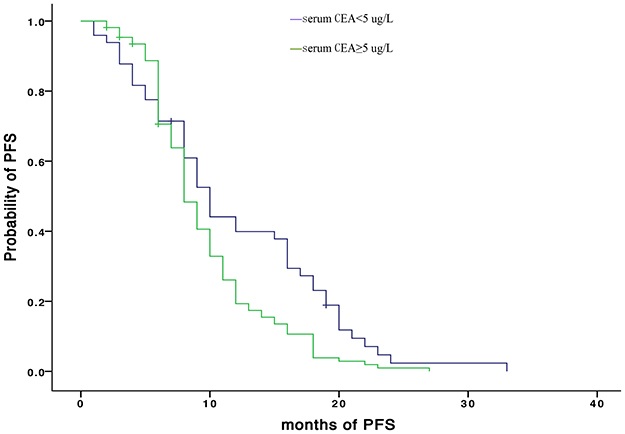 |
Figure 2 The progression-free survival (PFS) of patients receiving EGFR-TKI presented by Kaplan–Meier survival curve around a threshold of CEA level ≥ 5µg/L. |
Discussion
Molecular targeted therapy has improved the overall survival of advanced NSCLC patients with gene mutations.2,3 EGFR mutation is the most common target in precise treatments, accounting for 50–60% in Asian advanced NSCLC patients.9 Undoubtedly, EGFR mutations, whether detected in tumour tissue or liquid samples, predict the prognosis of advanced NSCLC patients taking EGFR-TKIs.2,10,11 However, adequate tissue samples for the detection of EGFR mutations are not often available,12,13 especially in patients with advanced disease. It has been reported that circulating tumour DNA (ctDNA) and circulating tumour cells (CTCs) from peripheral circulation used for analysis of gene variation, known as liquid biopsies, are alternative non-invasive methods for molecular diagnosis and treatment monitoring.14 Despite easy access and relatively high sensitivity, standardized and generally accepted methods are needed to cover the clinical needs. For example, molecular analysis based on CTCs requires a specific, microfluidic-based device to collect and identify the real ones, which remains a challenge.15,16 For ctDNA, a variety of technologies are available to analyse variations in ctDNA, including the amplification-refractory mutation system (ARMS), next-generation sequencing (NGS), and digital PCR platforms. Multiple studies have shown that the sensitivity of different methods varies from 10% to 0.01%,17–19 which limits the utility of liquid biopsy, as does the lack of standardization of these techniques. Therefore, it is urgently needed to find a more accessible and valuable way to predict EGFR mutation.
Previous research has mentioned that tumour biomarkers are associated with EGFR mutations. CEA is the product of the CEACAM5 gene, and abnormally elevated CEA levels have been found in almost 30–70% of patients with NSCLC, especially in adenocarcinoma and advanced-stage carcinoma.20,21 It has been reported that the rate of EGFR gene alterations was higher in the group of patients with increased serum CEA level.6 The possible explanation for these results is that activation of the downstream signalling pathway of EGFR promotes anti-apoptosis, leading to the enhanced expression level of CEA due to EGFR mutation.6,7 Our research also demonstrated that the percentage of EGFR mutations increased as serum CEA level increased (41.52%, 54.79%, and 62.39% for CEA <5, 5–20, and >20 μg/L, p=0.008), which was consistent with previous studies.5
The present study also showed that another tumour marker, SF, was correlated with EGFR mutation. To our knowledge, this is the first study to demonstrate the relationship between SF and EGFR mutation in NSCLC. According to the different cut-off points measured by the ROC curve in the subgroups of females and males, the rates of EGFR mutation were 38.8%, 83.9% and 84.4% with SF < 129, 129–258, >258 µg/L (p<0.001) for female patients, respectively, while they were 25.9%, 47.7% and 48.1% (p=0.014) with SF <329, 329–658, >658 µg/L in the group of male patients. As a useful biomarker to distinguish multiple cancers from healthy controls, SF has been shown to be significantly higher in cancer patients, particularly in advanced cancer stages and grades.22,23 However, no previous study has tested the relationship between serum ferritin level and EGFR mutation in advanced NSCLC. This study showed that elevated serum ferritin was correlated with EGFR mutation, since the rate of EGFR mutation was higher as the level of SF increased. The potential mechanism remains unknown, but it might be that EGFR mutation enhances the synthesis and release of ferritin or impacts the clearing ability of SF through the activation of downstream molecules more than wild-type EGFR. And Wang et al proved that activation of EGFR increased the cell surface transferrin receptor 1 (TfR1) expression, which was required for cellular iron import.24
To explore the value of serum CEA and ferritin for EGFR mutation prediction, both univariate and multivariate analyses were applied, indicating that the serum CEA and ferritin levels were associated with EGFR mutation (higher serum CEA or ferritin level predicted a higher incidence of EGFR gene mutation). The result that CEA was predictive which was similar to the finding of Shoji that higher CEA was independently correlated with EGFR gene mutation, with an OR of 4.70 (p=0.036),5 while this was the first study to illustrate that higher serum ferritin was independently associated with the incidence of EGFR mutation, with an OR of 4.593 (p<0.001). Moreover, a deep exploration into the diagnostic value of higher CEA (≥5 µg/L) for EGFR mutation showed an AUC of 0.586 (95% CI: 0.522–0.651, P=0.033), with a sensitivity of 69.0% and a specificity of 48.3%, which was similar to previous findings by Gao.20 For serum ferritin, the cut-off points were different in the subgroup of men (329 µg/L) and women (129 µg/L): the AUC was 0.711, with a sensitivity of 81.7% and a specificity of 65.2%, for females, which were better than those in male patients, where the AUC was 0.637, with a sensitivity of 61.1% and a specificity of 61.9%. The final sensitivity increased to 91.1% if serum ferritin was combined with CEA. The combination of serum ferritin and CEA can make the prediction of EGFR mutation more accurate.
Several studies have reported the relationship between tumour markers and the effect of NSCLC therapy, including EGFR-TKIs. CEA level has been demonstrated to be associated with the prognosis of patients on EGFR-TKIs and other treatments for NSCLC.7,25,26 In our study, a higher CEA level was associated with a poor outcome of EGFR-TKI (9.6 mo. vs 12.0 mo., HR: 1.594, p=0.013), which was consistent with some previous results. While SF was demonstrated to be correlated with the prognosis of patients taking an EGFR-TKI as first-line therapy, the PFS was increasingly shorter as the ferritin level increased (15.0 mo. vs 10.0 mo. vs 7.3 mo. with ferritin level 1 [<129 µg/L for females and < 329 µg/L for males], level 2 [129 µg/L -258 µg/L for females, 329 µg/L - 658 µg/L for males], and level 3 [>258 µg/L for females and >658 µg/L for males]). Little is known about the relationship between ferritin and the prognosis of patients taking EGFR-TKIs. The VeriStrat system, a serum- or plasma-based assay, makes detections by mass spectrometry based on protein signature and has been reported to be prognostic for patients on EGFR-TKIs.27,28 Fidler et al proved that SF was associated with the results of the VeriStrat system, but a relationship between SF and EGFR-TKI was not demonstrated.29 Our Cox proportional hazard model showed that the higher level of SF was an independent factor impacting the PFS for NSCLC patients receiving EGFR-TKIs (HR = 3.531; P<0.001).
To summarize, our research revealed an association between the expression level of serum ferritin and EGFR mutation. NSCLC patients with high serological levels of serum ferritin exhibited a higher rate of EGFR mutations. Moreover, SF was proven to be an effective tumour biomarker to distinguish between patients with and without EGFR mutations. In advanced female NSCLC patients, serum ferritin exhibited an AUC of 0.711, with a sensitivity of 81.7% and a specificity of 65.2%. When combining SF and CEA, the sensitivity increased to 91.1%, which provides a simpler and more accessible way to diagnose the status of EGFR mutation when tissue biopsy is not available. However, these findings need to be confirmed in a large number of patients, and the potential mechanism for the relationship between the expression of SF and CEA and EGFR mutation needs further exploration. Moreover, for those patients receiving EGFR-TKIs, SF was also a good predictor for survival time. Patients with decreased SF levels responded more effectively to EGFR-TKIs, and the proper patients for EGFR-TKIs can be selected according to the level of SF.
Acknowledgment
We thank all patients and their families’ supports to our work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68:7–30. doi:10.3322/caac.21442
2. Mok TS, Wu YL, Thongprasert S, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361:947–957. doi:10.1056/NEJMoa0810699
3. Zhou C, Wu YL, Chen G, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12:735–742. doi:10.1016/S1470-2045(11)70184-X
4. Mao C, Yuan JQ, Yang ZY, et al. Blood as a substitute for tumor tissue in detecting EGFR mutations for guiding EGFR TKIs treatment of nonsmall cell lung cancer: a systematic review and meta-analysis. Medicine. 2015;94:e775. doi:10.1097/MD.0000000000000874
5. Shoji F, Yoshino I, Yano T, et al. Serum carcinoembryonic antigen level is associated with epidermal growth factor receptor mutations in recurrent lung adenocarcinomas. Cancer. 2007;110:2793–2798. doi:10.1002/cncr.23101
6. Cai Z. Relationship between serum carcinoembryonic antigen level and epidermal growth factor receptor mutations with the influence on the prognosis of non-small-cell lung cancer patients. Onco Targets Ther. 2016;9:3873–3878. doi:10.2147/OTT.S102199
7. Okamoto T, Nakamura T, Ikeda J, et al. Serum carcinoembryonic antigen as a predictive marker for sensitivity to gefitinib in advanced non-small cell lung cancer. Eur J Cancer. 2005;41:1286–1290. doi:10.1016/j.ejca.2005.03.011
8. Zhi Q, Wang Y, Wang X, et al. Predictive and prognostic value of preoperative serum tumor markers in resectable adenosqamous lung carcinoma. Oncotarget. 2016;7:64798–64809. doi:10.18632/oncotarget.11703
9. Shi Y, Au JS, Thongprasert S, et al. A prospective, molecular epidemiology study of EGFR mutations in Asian patients with advanced non-small-cell lung cancer of adenocarcinoma histology (PIONEER). J Thorac Oncol. 2014;9:154–162. doi:10.1097/JTO.0000000000000033
10. Mok T, Wu YL, Lee JS, et al. Detection and dynamic changes of EGFR mutations from circulating tumor DNA as a predictor of survival outcomes in NSCLC patients treated with first-line intercalated erlotinib and chemotherapy. Clin Cancer Res. 2015;21:3196–3203. doi:10.1158/1078-0432.CCR-14-2594
11. Wang Z, Cheng Y, An T, et al. Detection of EGFR mutations in plasma circulating tumour DNA as a selection criterion for first-line gefitinib treatment in patients with advanced lung adenocarcinoma (BENEFIT): a phase 2, single-arm, multicentre clinical trial. Lancet Respir Med. 2018;6:681–690. doi:10.1016/S2213-2600(18)30264-9
12. Xue C, Hu Z, Jiang W, et al. National survey of the medical treatment status for non-small cell lung cancer (NSCLC) in China. Lung Cancer. 2012;77:371–375. doi:10.1016/j.lungcan.2012.04.014
13. Xu C, Zhou Q, Wu YL. Can EGFR-TKIs be used in first line treatment for advanced non-small cell lung cancer based on selection according to clinical factors? – A literature-based meta-analysis. J Hematol Oncol. 2012;5:62. doi:10.1186/1756-8722-5-62
14. Thompson JC, Yee SS, Troxel AB, et al. Detection of therapeutically targetable driver and resistance mutations in lung cancer patients by next generation sequencing of cell-free circulating tumor DNA. Clin Cancer Res. 2016;22:5772–5782. doi:10.1158/1078-0432.CCR-16-1231
15. Mayo C, Ortega FG, Gimenez-Capitan A, et al. CK-coated magnetic-based beads as a tool to isolate circulating tumor cells (CTCs) in human tumors. Transl Lung Cancer Res. 2013;2:65–71. doi:10.3978/j.issn.2218-6751.2013.02.06
16. Chinen LT, de Carvalho FM, Rocha BM, et al. Cytokeratin-based CTC counting unrelated to clinical follow up. J Thorac Dis. 2013;5:593–599. doi:10.3978/j.issn.2072-1439.2013.09.18
17. Li JY, Ho JC, Wong KH. T790M mutant copy number quantified via ddPCR predicts outcome after osimertinib treatment in lung cancer. Oncotarget. 2018;9:27929–27939. doi:10.18632/oncotarget.25332
18. Kang JH, Shin JY, Kim JO, et al. EGFR mutations in tumor tissue and blood collected from lung cancer patients by Insight Onco NGS technique. J Clin Oncol. 2016;34:e20017–e20017. doi:10.1200/JCO.2016.34.15_suppl.e20017
19. Shaozhang Z, Ming Z, Haiyan P, et al. Comparison of ARMS and direct sequencing for detection of EGFR mutation and prediction of EGFR-TKI efficacy between surgery and biopsy tumor tissues in NSCLC patients. Med Oncol. 2014;31:926. doi:10.1007/s12032-014-0374-0
20. Gao Y, Song P, Li H, Jia H, Zhang B. Elevated serum CEA levels are associated with the explosive progression of lung adenocarcinoma harboring EGFR mutations. BMC Cancer. 2017;17:484. doi:10.1186/s12885-017-3474-3
21. Matsuoka K, Sumitomo S, Nakashima N, Nakajima D, Misaki N. Prognostic value of carcinoembryonic antigen and CYFRA21-1 in patients with pathological stage I non-small cell lung cancer. Eur J Cardiothorac Surg. 2007;32:435–439. doi:10.1016/j.ejcts.2007.05.014
22. Singh KJ, Singh SK, Suri A, et al. Serum ferritin in renal cell carcinoma: effect of tumor size, volume grade, and stage. Indian J Cancer. 2005;42:197–200.
23. Yildirim A, Meral M, Kaynar H, Polat H, Ucar EY. Relationship between serum levels of some acute-phase proteins and stage of disease and performance status in patients with lung cancer. Med Sci Monit. 2007;13:Cr195–Cr200.
24. Wang B, Zhang J, Song F, et al. EGFR regulates iron homeostasis to promote cancer growth through redistribution of transferrin receptor 1. Cancer Lett. 2016;381:331–340. doi:10.1016/j.canlet.2016.08.006
25. Han J, Li Y, Cao S, et al. The level of serum carcinoembryonic antigen is a surrogate marker for the efficacy of EGFR-TKIs but is not an indication of acquired resistance to EGFR-TKIs in NSCLC patients with EGFR mutationsm. Biomed Rep. 2017;7:61–66. doi:10.3892/br.2017.914
26. Kappers I, Vollebergh MA, van Tinteren H, et al. Soluble epidermal growth factor receptor (sEGFR) and carcinoembryonic antigen (CEA) concentration in patients with non-small cell lung cancer: correlation with survival after erlotinib and gefitinib treatment. Ecancermedicalscience. 2010;4:178.
27. Carbone DP, Ding K, Roder H, et al. Prognostic and predictive role of the VeriStrat plasma test in patients with advanced non-small-cell lung cancer treated with erlotinib or placebo in the NCIC clinical trials group BR.21 trial. J Thorac Oncol. 2012;7:1653–1660. doi:10.1097/JTO.0b013e31826c1155
28. Taguchi F, Solomon B, Gregorc V, et al. Mass spectrometry to classify non-small-cell lung cancer patients for clinical outcome after treatment with epidermal growth factor receptor tyrosine kinase inhibitors: a multicohort cross-institutional study. J Natl Cancer Inst. 2007;99:838–846. doi:10.1093/jnci/djk195
29. Fidler MJ, Fhied CL, Roder J, et al. The serum-based VeriStrat(R) test is associated with proinflammatory reactants and clinical outcome in non-small cell lung cancer patients. BMC Cancer. 2018;18:310. doi:10.1186/s12885-018-4242-8
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.