Back to Journals » OncoTargets and Therapy » Volume 14
The Plasma Concentration of D-Dimer is Associated with Neoadjuvant-Chemotherapy Efficacy and the Prognosis in Osteosarcoma
Authors Huang Y, Shen Z, Yao Y, He A, Min D
Received 21 August 2020
Accepted for publication 23 December 2020
Published 11 January 2021 Volume 2021:14 Pages 213—220
DOI https://doi.org/10.2147/OTT.S278139
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr William C. Cho
Yujing Huang, Zan Shen, Yang Yao, Aina He, Daliu Min
Department of Oncology, Affiliated Sixth People’s Hospital of Shanghai Jiaotong University, Shanghai, People’s Republic of China
Correspondence: Daliu Min Tel +86 18930170332
Email [email protected]
Purpose: This retrospective study explored the clinical value of the plasma D-dimer level in osteosarcoma.
Materials and Methods: We measured the plasma D-dimer level before neoadjuvant chemotherapy (D0) and the plasma D-dimer level after four courses of neoadjuvant chemotherapy (D1) in 103 patients with stage-IIB high-grade osteosarcoma of the limb. The change in the D-dimer level (ΔD) was defined as D1 minus D0. The chi-square test was used to compare categorical variables. Analyses of receiver operating characteristic (ROC) curves were undertaken to determine the optimal cutoff points for D0, D1, and ΔD. The area under the ROC (AUC) of D0, D1, and ΔD was calculated to evaluate their discriminatory abilities in monitoring the response to neoadjuvant chemotherapy (tumor necrosis). Survival curves were generated according to Kaplan–Meier analyses and compared using the Log rank test. Univariate analyses and multivariate analyses were carried out to determine independent prognostic factors.
Results: Kaplan–Meier curves showed that a high D-dimer level at D0 and tumor diameter ≥ 8 cm were associated significantly with worse overall survival (OS) (P< 0.05). Multivariate Cox regression analyses revealed a high D-dimer level at D0 (hazard ratio, 3.92; 95% confidence interval, 1.756– 5.804; P=0.000) was an independent unfavorable prognostic factor. The chi-square test showed ΔD to be associated significantly with tumor necrosis. Analyses of ROC curves showed the D-dimer level at D0 and ΔD had better ability compared to that at D1 to discriminate the response to neoadjuvant chemotherapy.
Conclusion: The D-dimer level was correlated with the prognosis and response to chemotherapy in patients with stage-IIB high-grade osteosarcoma of the limb. The D-dimer level may serve as a risk factor of the response to chemotherapy and prognosis of localized osteosarcoma.
Keywords: D-dimer, osteosarcoma, necrosis, prognosis, neoadjuvant chemotherapy
Introduction
Osteosarcoma is the most prevalent primary cancer of bone, with an incidence of 4.4 per million in children and adolescents.1 Before the 1970s, osteosarcoma was treated by simple surgical excision, and carried a 5-year survival of ~10% to ~20%.2,3 Multidisciplinary treatment (neoadjuvant chemotherapy, surgery, adjuvant chemotherapy) has improved 5-year survival to ~70%.4,5 However, little clinically significant improvement in survival has been made over the last four decades, though more patients have had access to combination chemotherapy within and outside clinical trials.6
Although primary metastases, large tumor diameter, axial or proximal extremity tumor sites, increased serum levels of alkaline phosphatase (ALP) and lactate dehydrogenase (LDH), and older age have been found to be prognostic factors, the response to preoperative chemotherapy has been found to be the most important prognostic factor.1,7–9
Neoadjuvant chemotherapy is the preferred initial treatment on account of the vital prognostic information provided by the tumor response.10 Tumor response to neoadjuvant chemotherapy has an important role in subsequent care of patients with localized osteosarcoma. Patients who experience a “good” response (≥90% tumor necrosis) to preoperative chemotherapy tend to achieve long-term survival.11 However, tumor necrosis (representative of the histological response to neoadjuvant chemotherapy) can be estimated only after resection. Therefore, a noninvasive method that can predict the tumor response accurately is beneficial to determining an appropriate treatment strategy in individual patients.
A coagulation abnormality is associated with poor outcomes in cancer patients.12,13 Coagulation products have been reported to be associated with the growth, progression and metastasis of cancer cells, and angiogenesis.14,15 A high level of D-dimer (a degradation product of crosslinked fibrin16) is used not only as an indicator of thrombosis17 but also as an independent predictor for increasing cancer incidence.18 An increased plasma level of D-dimer has been reported to be an adverse prognostic factor in patients with colorectal cancer,19 gastric cancer,20 esophageal cancer,21 breast cancer,22 non-small-cell lung cancer,23 or gynecological tumors.24 Moreover, D-dimer serves as a predictive biomarker for chemotherapy response in gastric cancer,25 colorectal cancer,26 non-small-cell lung cancer,27 and ovarian cancer.28
Previously, we found that the D-dimer level not only predicted the prognosis but also correlated with the response to second-line chemotherapy.29 Here, we assessed the value of the D-dimer level in patients with stage-IIB high-grade osteosarcoma of the limb who underwent neoadjuvant chemotherapy.
Materials and Methods
Ethical Approval of the Study Protocol
The study was conducted in accordance with the Declaration of Helsinki 1964 and its later amendments. The ethics committee of Shanghai Sixth People’s Hospital (Shanghai, China) approved the study protocol. All patients provided written informed consent to have their data used.
Inclusion Criteria
The inclusion criteria were patients: (i) with histologically proven, high-grade, localized osteosarcoma of the extremity; (ii) who received neoadjuvant chemotherapy and had tumor necrosis; (iii) who had available D-dimer measurements at biopsy before neoadjuvant chemotherapy (D0) and after four courses of neoadjuvant chemotherapy (D1).
Exclusion Criteria
The exclusion criteria were patients: (i) with acute illness within the 2 weeks of measurement of the D-dimer level; (ii) who took anticoagulants at the start of neoadjuvant chemotherapy; (iii) with other types of primary malignancy; (iv) with incomplete data.
Patients
A total of 103 patients with stage-IIB high-grade osteosarcoma of the limb treated in our department between January 2010 and June 2012 were included in this retrospective study.
Data Collection
Data on clinical characteristics (sex, age, Karnofsky Performance Scale (KPS) score, pathological fracture, necrosis severity, survival) were collected. Measurement of the D-dimer level was done at D0 and D1. The difference in the D-dimer level (ΔD) was defined as D1 minus D0.
Statistical Analyses
The D-dimer level is presented as the mean ± standard deviation. The D-dimer level at D0, D1, and ΔD was compared using Wilcoxon signed-rank tests. With 5-year overall survival (OS) as the endpoint, we undertook analyses of receiver operating characteristic (ROC) curves to determine the optimal cutoff point for the D-dimer level at D0, D1, and ΔD. The area under the ROC curve (AUC) of D0, D1, and ΔD was calculated to evaluate their discriminatory abilities in monitoring the response to neoadjuvant chemotherapy (tumor necrosis). OS was defined as from the date of the diagnosis until the final follow-up date or death. Relapse-free survival (RFS) was defined as from the date of the operation until the relapse date or death. Survival curves were generated according to Kaplan–Meier analyses and compared using the Log rank test. Univariate analyses and multivariate analyses were undertaken to determine independent prognostic factors. The chi-square test was used to compare categorical variables. P < 0.05 (two-sided) was considered significant. Statistical analyses were undertaken using SPSS 19.0 (IBM, Armonk, NY, USA).
Results
Patient Characteristics
There were 65 male and 38 female patients (Table 1). The median age of the study cohort was 14 years. All patients had a KPS score ≥80. Also, 88.3% of patients agreed to undergo a salvage procedure. In addition, 48.5% of cases had tumor necrosis ≥90%. Twelve patients had a pathological fracture. Patients accepted 4–8 courses of neoadjuvant chemotherapy.
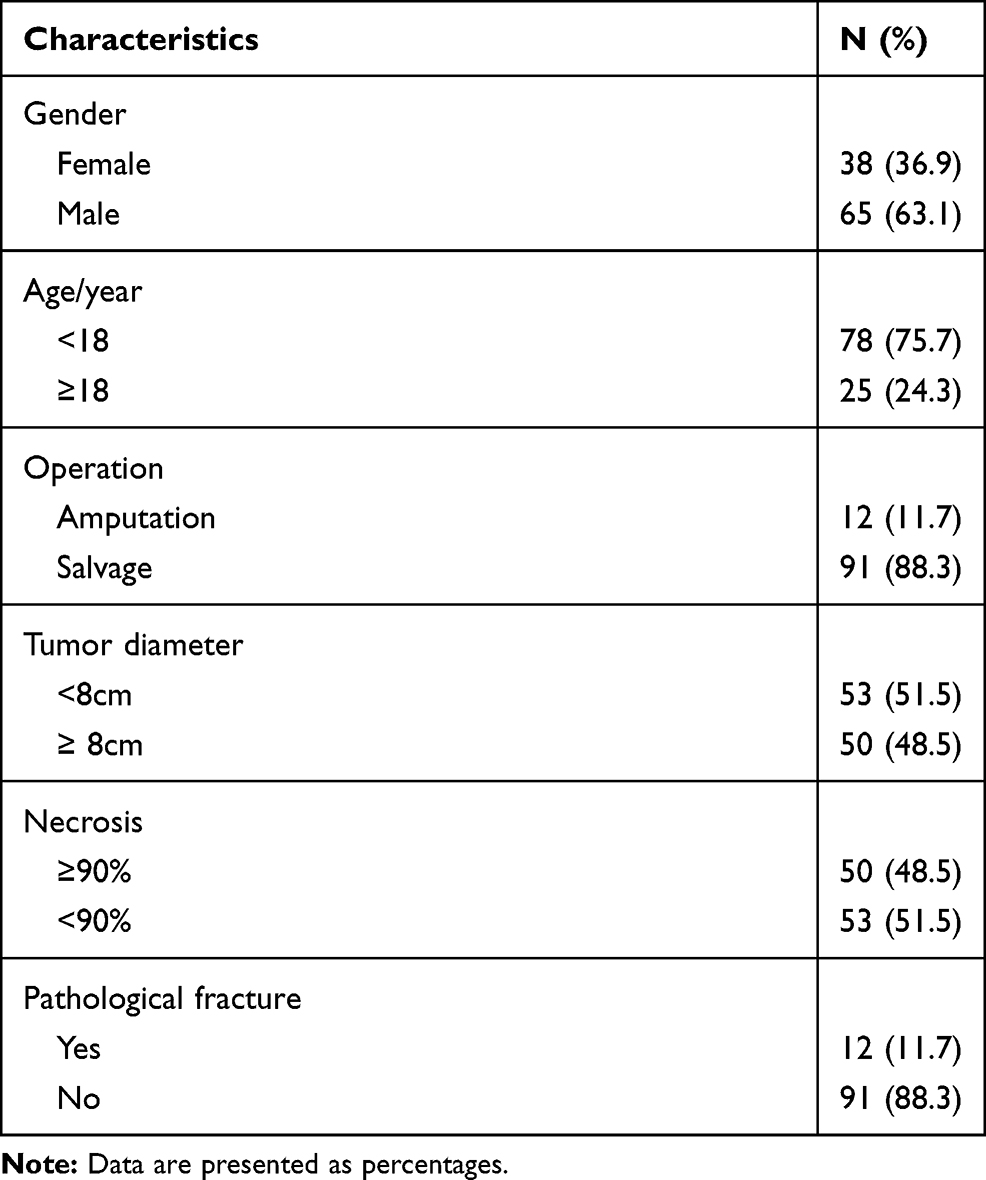 |
Table 1 Baseline Characteristics of the Patients |
Correlation Between the Plasma Level of D-Dimer and Survival
The median plasma concentration (in mg/mL) of D-dimer at D0, D1, and ΔD was 1.05 (range, 0.02 to 21.02), 0.59 (0.13 to 17.99), and −0.27 (−18.48 to 5.17), respectively. According to analyses of ROC curves, the optimal threshold (in mg/mL) of D-dimer at D0, D1, and ΔD was 3.91 (Youden Index, 0.279), 2.165 (0.258), and −0.053 mg/mL (0.212), respectively (Figure 1 and Table 2). Patients were categorized into two groups according to these cutoff values.
 |
Table 2 Predictive Value of D-Dimer Levels for Predicting 5-Year Overall Survival |
 |
Figure 1 ROC curves of D-dimer levels to predict prognosis. Abbreviations: ROC, receiver operating characteristic; AUC, the area under the ROC curve; D0, the plasma D-dimer level before neoadjuvant chemotherapy; D1, the plasma D-dimer level after four courses of neoadjuvant chemotherapy; ΔD, the change in the D-dimer level (D1 minus D0). |
The median OS was 61.4 (range, 8.8–86.8) months. The survival curve indicated that a high D-dimer level at D0 and tumor diameter ≥8 cm were associated significantly with worse OS according to the Log rank test (P < 0.05) (Figure 2).
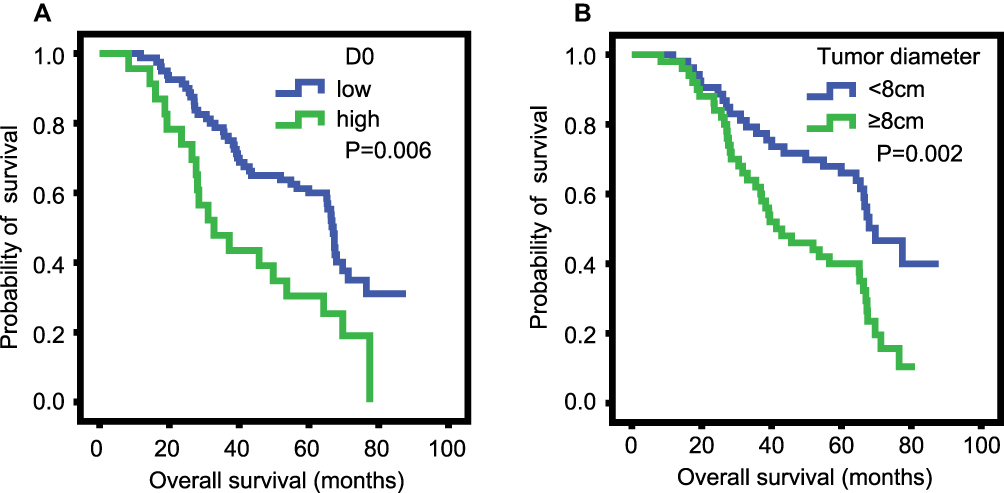 |
Figure 2 Kaplan–Meier curves for overall survival. (A) D0, the plasma D-dimer level before neoadjuvant chemotherapy; (B) tumor diameter. |
In the univariate analyses, the D-dimer level at D0 (P = 0.008) and tumor diameter (P = 0.002) were associated significantly with OS (Table 3). Multivariate analyses revealed that a high D-dimer level at D0 (hazard ratio, 3.92; 95% confidence interval [CI], 1.756–5.804; P = 0.000) was an independent unfavorable prognostic factor.
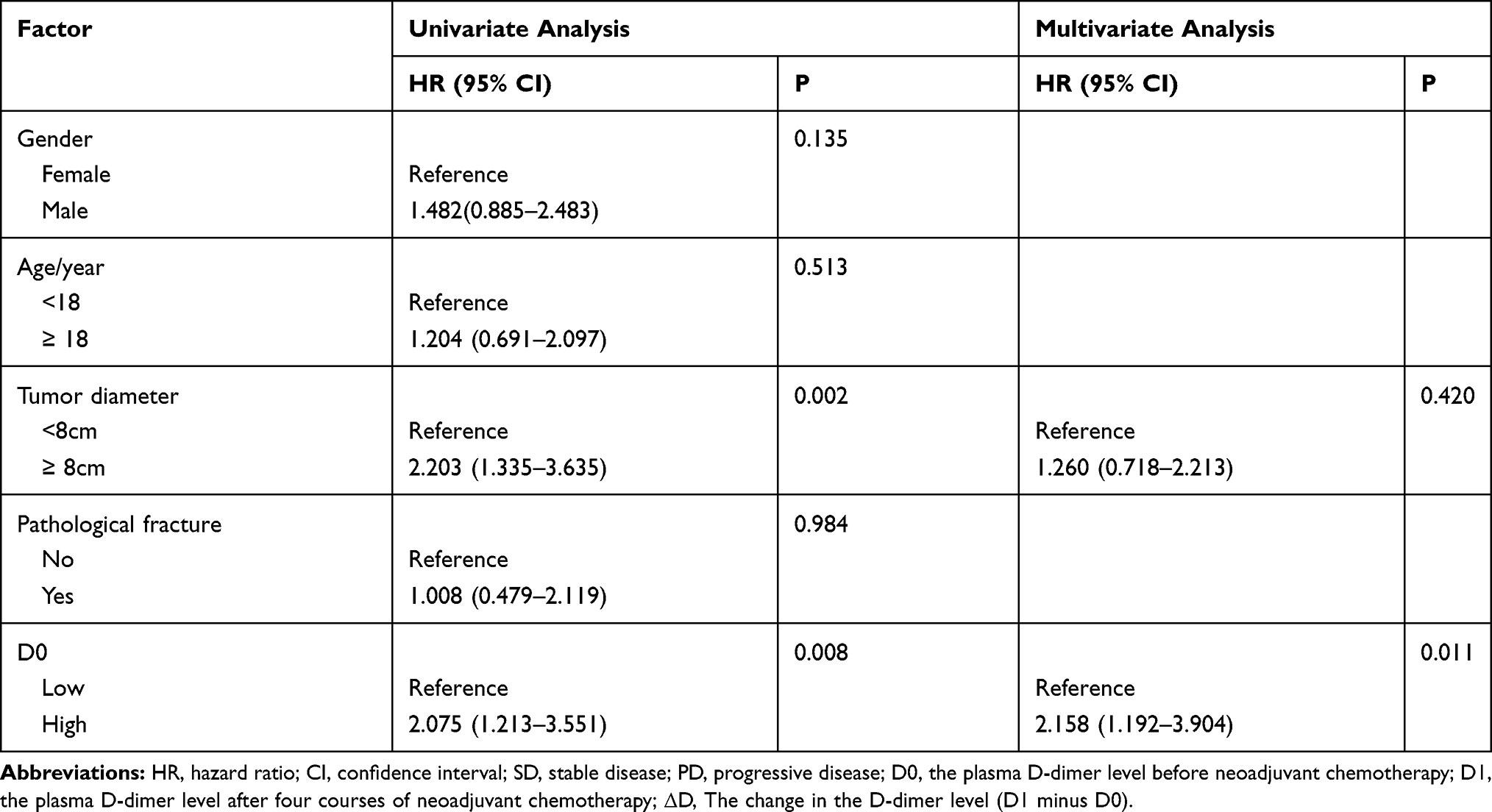 |
Table 3 Univariate and Multivariate Cox Proportional Hazard Regression Analyses of Overall Survival |
The median RFS was 38.9 (range, 1.8–84.9) months. According to the survival curve, there were no significant differences between high level and low level of D0 (P =0.162), D1 (P =0.250), and ΔD (P =0.064). And no of the D-dimer levels at D0, D1, and ΔD correlated significantly with any types of relapse (Table 4).
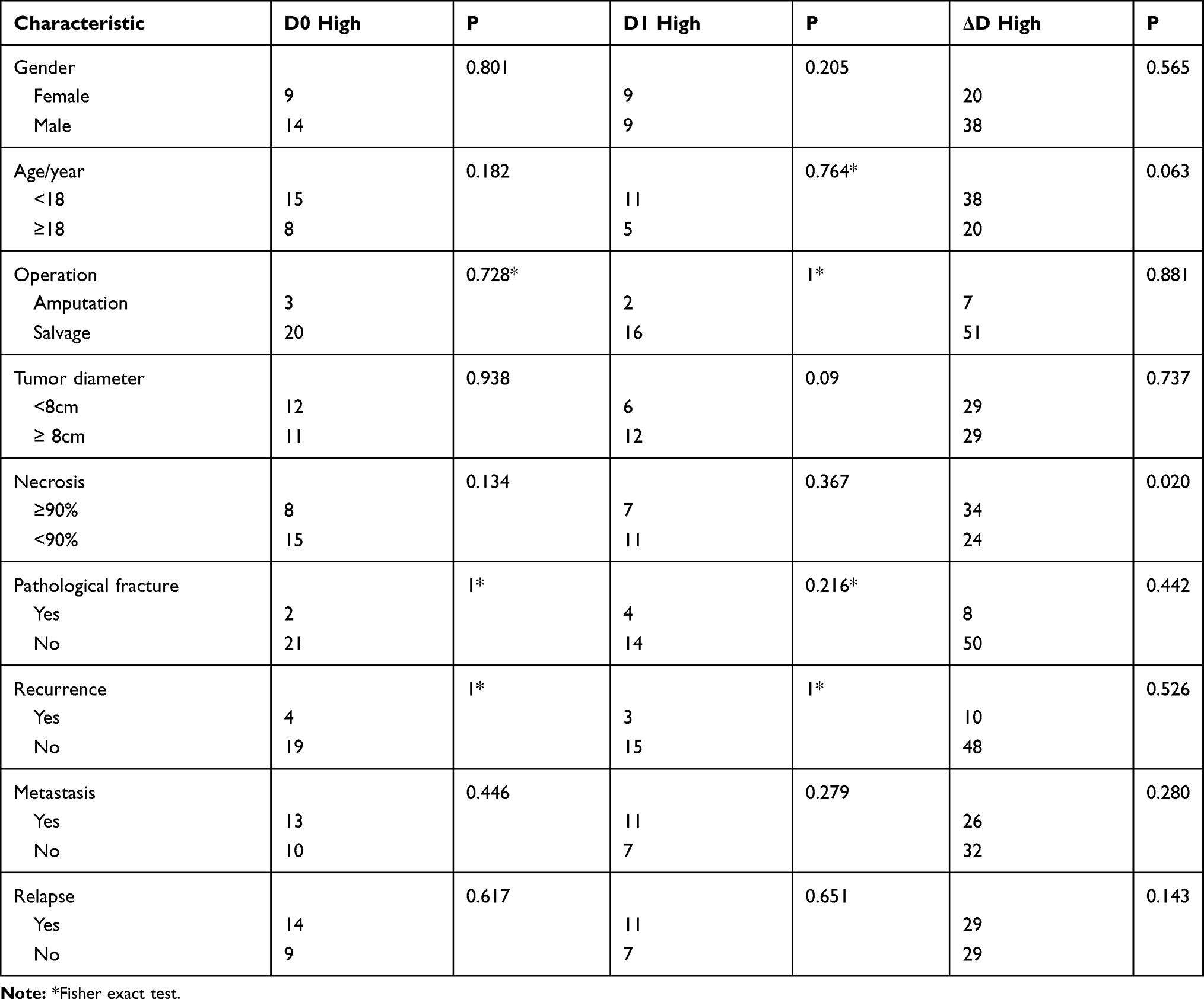 |
Table 4 Correlations Between Plasma D-Dimer and Patient Clinical Characteristic |
Correlation Between the Plasma Level of D-Dimer and Clinical Characteristics
According to analyses of ROC curves with 5-year OS as the endpoint, there were 23 (22.3%), 18 (17.5%), and 58 (56.3%) patients with a high D-dimer level at D0, D1, and ΔD, respectively. ΔD was correlated with necrosis (P = 0.020) rather than other clinical characteristics (Table 4). By contrast, neither the D-dimer level at D0 nor D1 correlated significantly with any clinical characteristic.
Discriminatory Ability of the D-Dimer Level in Response to Neoadjuvant Chemotherapy
Analyses of ROC curves indicated that the AUC at D0, D1, and ΔD was 0.372 (95% CI, 0.265–0.479; P = 0.025), 0.459 (0.347–0.571; 0.474) and 0.640 (0.533–0.747; P = 0.014), respectively, for predicting the response to chemotherapy. According to the AUC, the D-dimer level at D0 and ΔD had better discriminatory ability than the D-dimer level at D1 (Figure 3).
 |
Figure 3 Comparison of the area under the ROC curve to assess whether D-dimer levels could predict chemotherapy response. Abbreviations: ROC, receiver operating characteristic; AUC, the area under the ROC curve; D0, the plasma D-dimer level before neoadjuvant chemotherapy; D1, the plasma D-dimer level after four courses of neoadjuvant chemotherapy; ΔD, the change in the D-dimer level (D1 minus D0). |
Discussion
Tumors have been reported to induce the inflammatory response, release cytokines, and injure vascular walls directly or indirectly by releasing tissue factor, which can activate the coagulation cascade and cause coagulation dysfunction.30 Cancer patients have been shown to have a significantly higher D-dimer level than that of healthy controls31 in situations of enhanced fibrin formation and fibrinolysis. Moreover, the D-dimer level has been reported to be not only an adverse prognostic factor but also a biomarker for the response to chemotherapy in several types of cancer.20,22,28,32,33
Previously, we found that the D-dimer level was an unfavorable independent prognostic factor for patients with metastatic osteosarcoma, and correlated with the response to second-line chemotherapy.29 To further evaluate the value of D-dimer in osteosarcoma, we analyzed the D-dimer level before and after four courses of neoadjuvant chemotherapy in patients receiving multidisciplinary treatment (neoadjuvant chemotherapy, surgery, adjuvant chemotherapy).
Tumor necrosis is the strongest prognostic factor for osteosarcoma patients.5 Prediction of a poor response to neoadjuvant chemotherapy can stop use of time-consuming and ultimately non-efficacious treatments and prevent unnecessary adverse events. However, aside from the degree of tumor necrosis, a consistently reliable marker for use in prognostication in response to chemotherapy is lacking.34
Recently, different markers have been used to predict the tumor response preoperatively: receptor activator of nuclear factor kappa-Β ligand (RANKL),35 proteome,36 hypoxia-inducible factor-1α37 P16,38 and ALP.39 However, the predictive value of these markers was ascertained from small-cohort studies. Moreover, those studies included patients with different stages and locations of tumors.
We enrolled 103 patients with stage-IIB high-grade osteosarcoma of the limb. The results showed that ΔD was associated significantly with tumor necrosis. According to the AUC, the D-dimer level at D0 and ΔD had better discriminatory ability than the D-dimer level at D1. Hence, the D-dimer had predictive value.
We also assessed the prognostic value of the D-dimer level in osteosarcoma. Survival curves indicated that a high D-dimer level at D0 and tumor diameter ≥8 cm were correlated with a poor prognosis. A high D-dimer level at D0 and tumor diameter were associated significantly with OS in univariate analyses. Multivariate analyses of these factors revealed that a high D-dimer level at D0 was an independent unfavorable prognostic factor. Hence, the D-dimer level could be used as a risk factor in osteosarcoma management.
18F-fluorodeoxyglucose-positron emission tomography/computed tomography and magnetic resonance imaging are used for assessment of the osteosarcoma response after neoadjuvant chemotherapy. Compared with imaging examinations, measurement of the D-dimer level is straightforward and inexpensive. Establishing a new model by measuring the D-dimer level may be very instructive, particularly for low-income groups.
Our study had four main limitations. First, this retrospective, single-institution, small-sample-size study provided a lower level of evidence compared with that elicited from a randomized controlled trial. Second, heterogeneity among treatment strategies was present. Third, we included only patients for whom complete clinical data were available. Also, we set the timepoint D1 after four courses of chemotherapy, but patients accepted 4–8 courses of neoadjuvant chemotherapy: a selection bias may have occurred. Finally, our results could also have been biased by the cutoff points of the D-dimer level because they were calculated via analyses of ROC curves.
Conclusions
The D-dimer level was correlated with the prognosis and response to chemotherapy in patients with stage-IIB high-grade osteosarcoma of the limb. The D-dimer level may serve as a risk factor of the response to chemotherapy and prognosis of localized osteosarcoma. Validation studies are required before clinical application.
Funding
The study was supported by grants from the National Natural Science Foundation of China (No. 81001191) and Science, Technology Commission of Shanghai, China (No. 10PJ1408300), Seed Fund Program of Shanghai University of Medicine & Health Sciences (No. SFP-18-20-14-002), Science Research Project of Shanghai Municipal Commission of Health and Family Planning (No. 201840039), and Natural science foundation project of Shanghai science and technology commission (No.19ZR1439100).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mirabello L, Troisi RJ, Savage SA. Osteosarcoma incidence and survival rates from 1973 to 2004: data from the surveillance, epidemiology, and end results program. Cancer. 2009;115(7):1531–1543. doi:10.1002/cncr.24121
2. Arndt CA, Crist WM. Common musculoskeletal tumors of childhood and adolescence. N Engl J Med. 1999;341(5):342–352. doi:10.1056/NEJM199907293410507
3. Jeon DG, Song WS. How can survival be improved in localized osteosarcoma? Expert Rev Anticancer Ther. 2010;10(8):1313–1325. doi:10.1586/era.10.79
4. Longhi A, Errani C, De Paolis M, Mercuri M, Bacci G. Primary bone osteosarcoma in the pediatric age: state of the art. Cancer Treat Rev. 2006;32(6):423–436. doi:10.1016/j.ctrv.2006.05.005
5. Bielack S, Kempf-Bielack B, Delling G, et al. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: an analysis of 1702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol. 2002;20(3):776–790. doi:10.1200/JCO.2002.20.3.776
6. Whelan JS, Bielack SS, Marina N, et al. EURAMOS-1, an international randomised study for osteosarcoma: results from pre-randomisation treatment†. Ann Oncol. 2015;26(2):407–414. doi:10.1093/annonc/mdu526
7. Davis A, Bell R, Goodwin P. Prognostic factors in osteosarcoma: a critical review. J Clin Oncol. 1994;12(2):423–431. doi:10.1200/JCO.1994.12.2.423
8. Bramer J, van Linge J, Grimer R, Scholten R. Prognostic factors in localized extremity osteosarcoma: a systematic review. Eur J Surg Oncol. 2009;35(10):1030–1036. doi:10.1016/j.ejso.2009.01.011
9. Zamborsky R, Kokavec M, Harsanyi S, Danisovic L. Identification of prognostic and predictive osteosarcoma biomarkers. Med Sci. 2019;7(2):2. doi:10.3390/medsci7020028
10. Bacci G, Ferrari S, Longhi A, et al. Neoadjuvant chemotherapy for high grade osteosarcoma of the extremities: long-term results for patients treated according to the rizzoli IOR/OS-3b protocol. J Chemother. 2001;13(1):93–99. doi:10.1179/joc.2001.13.1.93
11. Bacci G, Mercuri M, Longhi A, et al. Grade of chemotherapy-induced necrosis as a predictor of local and systemic control in 881 patients with non-metastatic osteosarcoma of the extremities treated with neoadjuvant chemotherapy in a single institution. Eur J Cancer. 2005;41(14):2079–2085. doi:10.1016/j.ejca.2005.03.036
12. Connolly GC, Francis CW. Cancer-associated thrombosis. Hematology Am Soc Hematol Educ Program. 2013;2013(1):684–691. doi:10.1182/asheducation-2013.1.684
13. Chew HK, Wun T, Harvey D, Zhou H, White RH. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med. 2006;166(4):458–464. doi:10.1001/archinte.166.4.458
14. Wojtukiewicz MZ, Sierko E, Klement P, Rak J. The hemostatic system and angiogenesis in malignancy. Neoplasia. 2001;3(5):371–384. doi:10.1038/sj.neo.7900184
15. Ruf W, Yokota N, Schaffner F. Tissue factor in cancer progression and angiogenesis. Thromb Res. 2010;125(Suppl 2):S36–38. doi:10.1016/S0049-3848(10)70010-4
16. Meade TW, Mellows S, Brozovic M, et al. Haemostatic function and ischaemic heart disease: principal results of the Northwick Park Heart Study. Lancet. 1986;2(8506):533–537. doi:10.1016/S0140-6736(86)90111-X
17. Tripodi A. D-dimer testing in laboratory practice. Clin Chem. 2011;57(9):1256–1262. doi:10.1373/clinchem.2011.166249
18. Simes J, Robledo KP, White HD, et al. D-dimer predicts long-term cause-specific mortality, cardiovascular events, and cancer in patients with stable coronary heart disease: LIPID study. Circulation. 2018;138(7):712–723. doi:10.1161/CIRCULATIONAHA.117.029901
19. Watanabe A, Araki K, Harimoto N, et al. D-dimer predicts postoperative recurrence and prognosis in patients with liver metastasis of colorectal cancer. Int J Clin Oncol. 2018;23(4):689–697. doi:10.1007/s10147-018-1271-x
20. Go S-I, Lee MJ, Lee WS, et al. D-dimer can serve as a prognostic and predictive biomarker for metastatic gastric cancer treated by chemotherapy. Medicine. 2015;94(30):e951. doi:10.1097/MD.0000000000000951
21. Feng JF, Yang X, Chen S, Zhao Q, Chen QX. Prognostic value of plasma d-dimer in patients with resectable esophageal squamous cell carcinoma in China. J Cancer. 2016;7(12):1663–1667. doi:10.7150/jca.15216
22. Batschauer AP, Figueiredo CP, Bueno EC, et al. D-dimer as a possible prognostic marker of operable hormone receptor-negative breast cancer. Ann Oncol. 2010;21(6):1267–1272. doi:10.1093/annonc/mdp474
23. Kaseda K, Asakura K, Kazama A, Ozawa Y. Prognostic significance of preoperative plasma D-dimer level in patients with surgically resected clinical stage I non-small cell lung cancer: a retrospective cohort study. J Cardiothorac Surg. 2017;12(1):102. doi:10.1186/s13019-017-0676-3
24. Wang H, Tang M, Ou L, et al. Biological analysis of cancer specific microRNAs on function modeling in osteosarcoma. Sci Rep. 2017;7(1):5382. doi:10.1038/s41598-017-05819-7
25. Park K, Ryoo B, Ryu M, et al. Incidence of venous thromboembolism and the role of D-dimer as predictive marker in patients with advanced gastric cancer receiving chemotherapy: a prospective study. World J Gastrointest Oncol. 2017;9(4):176–183. doi:10.4251/wjgo.v9.i4.176
26. Inanc M, Er O, Karaca H, et al. D-dimer is a marker of response to chemotherapy in patients with metastatic colorectal cancer. J BUON. 2013;18(2):391–397.
27. Wang Y, Wang Z. Predictive value of plasma D-dimer levels in patients with advanced non-small-cell lung cancer. Onco Targets Ther. 2015;8:805–808. doi:10.2147/OTT.S78154
28. Liu P, Wang Y, Tong L, et al. Elevated preoperative plasma D-dimer level is a useful predictor of chemoresistance and poor disease outcome for serous ovarian cancer patients. Cancer Chemother Pharmacol. 2015;76(6):1163–1171. doi:10.1007/s00280-015-2900-y
29. Huang Y, Liu B, Sun Y, Zhang J, Yao Y, He A. The prognostic value of D-dimer levels in metastatic osteosarcoma patients treated with second-line chemotherapy. Oncotarget. 2016;7(40):65568–65576. doi:10.18632/oncotarget.11571
30. Cui L, Sun YH, Chen J, et al. Analysis of prethrombotic states in patients with malignant tumors. Asian Pac J Cancer Prev. 2015;16(13):5477–5482. doi:10.7314/APJCP.2015.16.13.5477
31. Yu J, Li D, Lei D, et al. Tumor-specific D-dimer concentration ranges and influencing factors: a cross-sectional study. PLoS One. 2016;11(11):e0165390. doi:10.1371/journal.pone.0165390
32. Liu L, Zhang X, Yan B, et al. Elevated plasma D-dimer levels correlate with long term survival of gastric cancer patients. PLoS One. 2014;9(3):e90547. doi:10.1371/journal.pone.0090547
33. Ge LP, Li J, Bao QL, Chen P, Jiang Q, Zhu LR. Prognostic and predictive value of plasma D-dimer in advanced non-small cell lung cancer patients undergoing first-line chemotherapy. Clin Transl Oncol. 2015;17(1):57–64. doi:10.1007/s12094-014-1198-2
34. Clark JCM, Dass CR, Choong PFM. A review of clinical and molecular prognostic factors in osteosarcoma. J Cancer Res Clin Oncol. 2008;134(3):281–297. doi:10.1007/s00432-007-0330-x
35. Lee JA, Jung JS, Kim DH, et al. RANKL expression is related to treatment outcome of patients with localized, high-grade osteosarcoma. Pediatr Blood Cancer. 2011;56(5):738–743. doi:10.1002/pbc.22720
36. Li Y, Dang T, Shen J, et al. Plasma proteome predicts chemotherapy response in osteosarcoma patients. Oncol Rep. 2011;25(2):303–314. doi:10.3892/or.2010.1111
37. Chen Y, Yang Y, Yuan Z, Wang C, Shi Y. Predicting chemosensitivity in osteosarcoma prior to chemotherapy: an investigational study of biomarkers with immunohistochemistry. Oncol Lett. 2012;3(5):1011–1016. doi:10.3892/ol.2012.604
38. Kosemehmetoglu K, Ardic F, Karslioglu Y, Kandemir O, Ozcan A. p16 expression predicts neoadjuvant tumor necrosis in osteosarcomas: reappraisal with a larger series using whole sections. Hum Pathol. 2016;50:170–175. doi:10.1016/j.humpath.2015.09.043
39. Khoury J, Ben-Arush M, Weintraub M, et al. Alkaline phosphatase level change in patients with osteosarcoma: its role as a predictive factor of tumor necrosis and clinical outcome. Isr Med Assoc J. 2014;16(1):26–32.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.