Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
The Performance of Visual, Auditory, and Motor Cognitive Flexibility for Children with Autism Spectrum Disorder in Taiwan
Authors Lin CL ![]() , Shen CP, Lin CK
, Shen CP, Lin CK ![]()
Received 20 May 2022
Accepted for publication 5 September 2022
Published 23 September 2022 Volume 2022:18 Pages 2151—2158
DOI https://doi.org/10.2147/NDT.S372519
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Chien-Lin Lin,1 Ching-Ping Shen,2 Chin-Kai Lin3
1Department of Physical Medicine and Rehabilitation, China Medical University Hospital, Taiwan and School of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan; 2National Chung-Shan Institute of Science & Technology Shi-Yuan Polyclinic, Taipei, Taiwan; 3Program of Early Intervention, Department of Early Childhood Education, National Taichung University of Education, Taichung, Taiwan
Correspondence: Chin-Kai Lin, National Taichung University of Education, 140 Min-Shen Road, Taichung, 40306, Taiwan, Tel +886 4-22183007, Fax +886 4-22183380, Email [email protected]
Purpose: Few studies have tested the cognitive flexibility, specifically auditory and motor flexibility of children with ASD. This study was conducted to understand the relationship between cognitive flexibility and visual, auditory, and motor development in young children with ASD and autistic behaviors.
Participants and methods: A purposive sampling approach was used to screen nineteen four- to five-year-old ASD children. Tests included the Autism Behavior Checklist-Taiwan Version and Cognitive Flexibility Test, which included visual, auditory, and motor cognitive flexibility subtests.
Results: At the pre-switch and post-switch of three subtests, there were considerable variations in the number of ASD passing. According to the findings, children aged five had more visual cognitive flexibility than children aged four, but the lack of significant differences for the other flexibilities. The negative correlation of the three cognitive flexibilities with autistic behaviors was − 0.57∼-0.64.
Conclusion: Children with ASD have significant difficulties in switching rule tasks characterized by visual, auditory, and motor cognitive flexibility. The results suggest that visual cognitive flexibility had an age effect. The negative correlation of the three cognitive flexibilities with autistic behaviors was moderate.
Keywords: executive function, autistic behavior, preschooler, mental flexibility
Introduction
Executive function refers to a group of higher-order cognitive abilities that include planning, response inhibition, working memory, and cognitive flexibility. It is generally associated with prefrontal lobe structures of the human brain.1
Cognitive flexibility (CF) is considered one of the primary components of executive functioning,2 which enables individuals to freely engage and disengage from one activity, concept, or action, to another. Cognitive flexibility refers to the capacity to quickly adjust among different ideas and action plans and allows a person to perceive updated environmental information and transform their behavior to adjust according to the changes in surroundings.3–6 Cognitive flexibility develops dramatically in preschool around 4 to 5 years of age and continuously refines well into adolescence.3,7 Children who are cognitively rigid are at risk of cognitive developmental delays because they resist learning new materials or concepts. They are vulnerable to the steadfast insistence of monotony when dealing with emotional disturbances or interpersonal social problems.
The inflexibility manifests itself in a variety of aspects such as verbal expression, visual input, sensory motor, auditory, interest, eating4 and learning patterns. Although these behaviors are not specific to children with ASD, their prevalence is high in this population.8
A child with autistic spectrum disorder (ASD) has a neurodevelopmental disorder that is characterized by persistent deficits in social communication and social interaction in a variety of situations. Children with ASD demonstrate restricted, repetitive patterns of behavior (RRB), interests, or activities (APA, 2013) which are core symptom features of ASD.
The Wisconsin Card Sorting Test (WCST) is a standard neuropsychological measure widely used in research to measure executive function and cognitive flexibility. During a pre-switching task and a post-switching task, the children must sort cards based on task demands that involve two or three dimensions (color, shape, and number). The child must suppress previous sorting rules or irrelevant features and do as instructed by the examiner, memorizing the new rules of sorting cards into new categories based on new features.
Thus, the ability to show cognitive flexibility by switching tasks is not only due to inhibiting predominant features,9 but also due to inhibiting visual scanning patterns,10 suppressing previous attention to shift to the next dimension, monitoring and renewing information in working memory.2
Van Eylen (2011) and Reed (2018) found that when completing tasks according to the new rule, the child with ASD took longer, made more errors, or persevered less than the typical child.11,12 The more complex the task, the worse the performance, most likely due to working memory deficits in those children with ASD.12 The number of errors on WSCT could be associated with the difficulty of the task.13 So, in this study, the task difficulty was controlled by just one dimension at one time to decrease the component of working memory effect on the performance of those children with ASD. The Dimensional Change Card Sort (DCCS) fit the purpose of this study was utilized to remove excessive memory loading since the participants were instructed to sort according to only one dimension of card trait. Other related factors associated with WCST or DCCS scores included language performance,14 IQ.15 In our study, verbal performance and IQ domains were controlled so as not to confound the inferences of the findings.
A child with ASD may listen to the same voices or sounds repeatedly, such as a toilet flushing, or their own noise, such as word and sentence repetition, so that others become aware of their idiosyncratic language, and unreasonable persistence on particular motor mannerisms. Therefore, children with ASD experience a high degree of difficulty in adaptation to switching tasks with various sensory input including visual, auditory, and motor input. This current study not only examines the cognitive flexibility of the switching rule task characterized by vision, but also includes other senses, such as auditory, and motor flexibility in order to comprehensively understand the cognitive inflexibility of children with ASD in a multiple sensory situation.
When confronted with new problems in their daily activities, children with ASD perform poorly in shifting their thoughts or changing strategies. ASD is characterized by a lack of flexibility.12 They have difficulty in adopting new perspectives when facing challenges in social interactions or emotional reciprocity.11
Children with ASD exhibit obvious restricted and repetitive behaviors (RRB) in daily life, which may be interpreted as poor cognitive flexibility.6,11 Thus, RRB should be significantly correlated with flexibility difficulty.
However, outcomes in previous study results on the association between cognitive inflexibility in some research16 or clinical settings were inconsistent. There was poor performance in cognitive flexibility related to poor social communication function for the children with ASD who were IQ-matched to the typically developing group.17 The total symptoms of autistic behaviors occurred in various developmental domains of everyday performance. Thus, the dependent variables of this study were to test the multiple area of development, not just RRB.
This study hypothesized that 1. There are significant differences in the number of ASD who passed the pre-switching task and the number of ASD who passed the post-switching task. 2. Cognitive flexibility performance in 5-year-olds is significantly higher than in 4-year-olds. 3. A significant negative relationship exists between cognitive flexibility performance and autistic behavior.
Methods
Participants
Purposive sampling was used to screen cases from four medical institutions for young children with ASD: Tungs’ Taichung Metro Harbor Hospital, Jointhink Social Welfare Foundation and Jen Ho Clinic. The following were the inclusion criteria for these children: (1) 4 to 5 years of age; (2) diagnosed with ASD by physicians using the DSM-V at the Assessment Center for Child Development in Taiwan; (3) scored 11 points or more on the Autism Behavior Checklist-Taiwan Version; (4) ASD were able to perform speech in sentence; (5) they can recognize pictures on sorting cards and encode the features to discriminate the different colors, shape, and number of pictures in cards; (6) language comprehension level: they understand verbal communication. (7) IQ score of Wechsler Intelligence Scale for Children greater than 70. The exclusive criteria were as follows: (1) diagnosis of intellectual disability; (2) visual or hearing impairment (3) history of medical impairment, seizures, neuromuscular disorders, psychiatric or neurological disorders and brain injury. (4) children with ASDs who had participated in any training session focused on the ability of cognitive flexibility and executive function.
The researcher explained the research purpose and tasks to the children’s parents, but the participants were unaware of the study’s goal due to the blind design. After ensuring that the parents or primary caregivers (legal representatives of young children) fully understood all relevant information, agreed to participate in the research, and cooperated with the research plan, their children were enrolled in the study, and the parents signed informed consent forms. For those who chose not to participate in the research, their rights and benefits in the hospital were not affected. All subjects were allowed to withdraw from the study at any time if they felt uncomfortable during the tests. This research was in compliance with the Declaration of Helsinki and was approved by the Human Review Board, Tsaotun Psychiatric Center Ministry of Health and Welfare in 2018 (IRB code: 107015).
The total participants for this study included 19 high functioning children with ASD (the age range of 48~71 months old), 59.42 ± 7.51 months (10 children with ASD aged 4 years (52.6%), 9 ASD aged 5 years old (47.4%)). There were 16 boys (84.2%) and 3 girls (15.8%). There were no statistically significant differences between the number of age groups (χ2=0.53, p = 0.82).
Measurements
The Autism Behavior Checklist-Taiwan Version
The Autism Behavior Checklist-Taiwan version (ABCT) compiled by Krug, Arick, and Almond (1980);18 revised by Huang Jun-yu and Wu You-you (2013), published by Taiwan Psychology Publishing, was used in the study. The Checklist scale contains 47 items: 8 items pertaining to Sensory, 11 items to Relating, 12 items pertaining to Body and Object Use, 8 items pertaining to Language, and 8 items pertaining to Social and Self-Help. It is designed for children 3–15 years old. The scoring method gives 1 point for each “Yes” answer. The higher the score, the more severe the autistic behaviors. This scale has favorable content consistency, with a Cronbach α value between 0.75 and 0.87, retest reliability at 0.89.19 The content validity and reliability of the scale are satisfactory.
The Cognitive Flexibility Test
The Cognitive Flexibility Test included three subtests: visual cognitive flexibility from DCCS,20 auditory cognitive flexibility revised from Day-Night Test, and motor cognitive flexibility. The Visual cognitive flexibility task is an analogous rule-switching task for visual cognitive flexibility that employs a bivalent test card with two concurrent and distinct traits, describing an example of a card picture (eg, “rabbit” and “boats” have two different colors “red” and “blue”) to score children’s resorting behavior against pre-switching rules. Each test card and each target card have the same dimension and an opposite dimension, while the picture card has two dimensions of shape and color. The testing administration and instructions followed the recommendations in the standard DCCS (see Zelazo, 2006) and Day-Night Test21 In the day-night test, children were asked to say the word “day” when displayed a picture of the night sky, and to say “night” when looking at a card drawing of a daytime sky. There were no cards in front of the children in our revised Day-Night Test in this study, but the examiner gave oral instructions instead of cards. When the examiner says “day”, the child should say “night”, and vice versa. In the motor cognitive flexibility test, the tester performed six different movements in sequence, and the child was instructed to perform the paired movement for each. When the tester makes a fist, the child should open his/her hand; when the tester opens his/her hand, the child should make a fist, and vice versa. It included 12 test items for each subtest: visual (DCCS revised), auditory and motor. Each subtest contained 6 pre-switch items and 6 post-switch items. The dependent variable was the number of ASD who passed. Those who scored 5 or more points in the 6 trials at the pre-switch or post-switch phase were considered to pass, while those who scored 0 to 4 points were considered to fail.20 Participants received one point for each correctly answered item. The higher the test score, the greater the cognitive flexibility. The Cognitive Flexibility has a high level of internal consistency (Cronbach’s alpha.73, ICC.72) and construct validity. Three Cognitive Flexibility test constructs explain 65.66% of the variance from factor analysis.
Procedures
This study included tests on children with ASD who met seven recruitment criteria and were conducted in institutions. All of the test rooms were independent spaces with adequate lighting. During the test, there was only one examiner and one child in the independent space. Each child was tested individually. The examiner first interacted with the child to help reduce anxiety, then introduced himself/herself and explained the tasks that needed to be completed. The examiner went through the practice items for the visual, auditory, and motor cognitive flexibility tests in order. First, the examiner demonstrated the test and explained its rules. Each item was practiced until the participants understood what they needed to do during the tests. The tests would begin only after the test subject understood the rules. Regardless of the child’s sorting accuracy, the examiner would say “Next question” and proceed to the next test item. When the test was completed, the tester would present a small gift to the participants.
Data Analysis
This study used McNemar test, Mann Whitney U-test, and Spearman coefficient for data analysis. The Statistical Package for the Social Science (SPSS) version 20 (SPSS, Inc., Chicago, IL, USA) was used for all analyses and p < 0.05 was used to indicate statistical significance.
Results
The Performance of Pre-Switching Task and Post-Switch Task of Cognitive Flexibility
The McNemar test results revealed that the number of ASD passing changes (Table 1) were significantly different at the pre-switch and post-switch in visual cognitive flexibility (p = 0.004), auditory cognitive flexibility (p = 0.000), and motor cognitive flexibility (p = 0.000) (Table 1). All subjects with ASD passed at the phase pre-switch, but 15 in 19 subjects with ASD (78.9%) could not pass at the phase of post-switching subtest auditory cognitive flexibility subtest. For the perseverative performance on the motor cognitive flexibility subtest, 16 of 19 ASD subjects (84.2%) were unable to switch from their movements according to a reversal pair of rules.
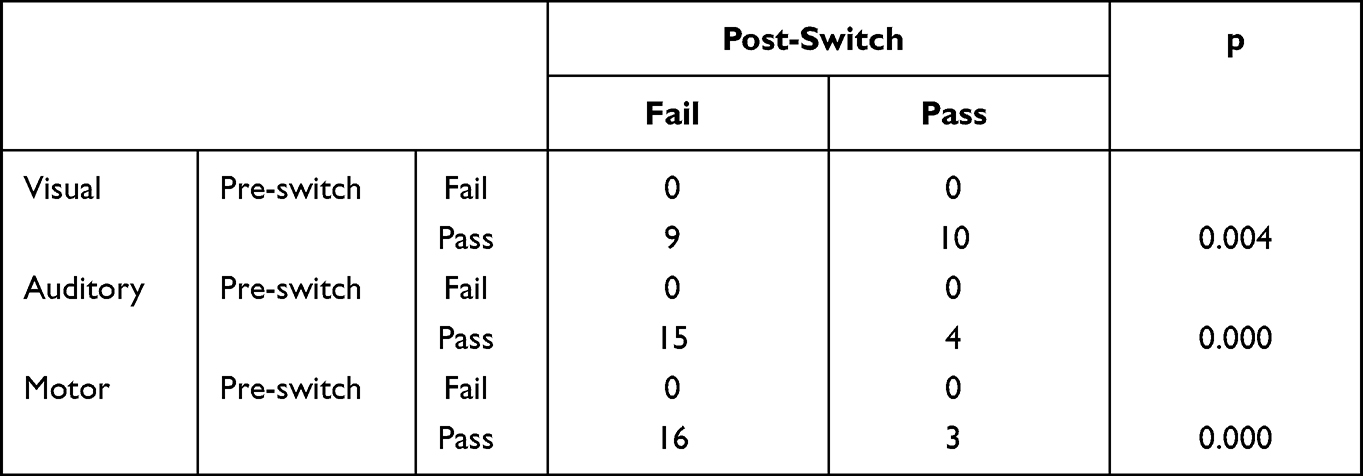 |
Table 1 The Number of ASD at Pre-and Post-Switching Phase of Cognitive Flexibility |
Age Effect on the Cognitive Flexibility
In the pre-switching task: there was no significant difference between 4 year olds and 5 year olds at the performance of the visual, auditory, and motor cognitive flexibility. In terms of total scores, 5 year olds performed significantly better than 4 year olds in visual cognitive flexibility (z=−2.17, P = 0.03) (Table 2). There was no significant difference in auditory and motor cognitive flexibility performance between 4 and 5 year olds.
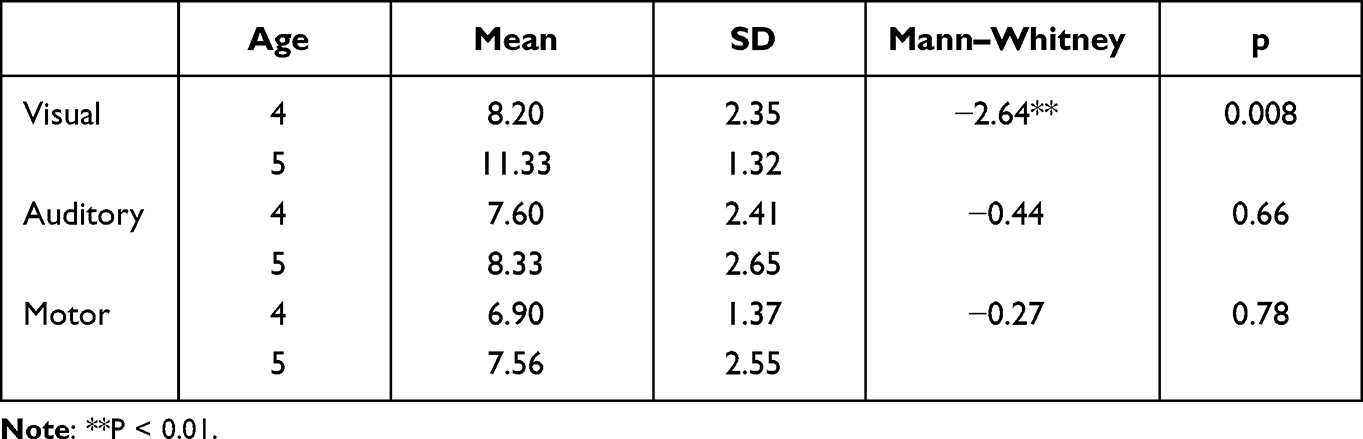 |
Table 2 Age on the Difference in Total Scores of the Cognitive Flexibility |
Relationship Between the Performance of Cognitive Flexibility and Autistic Behavior
The Spearman’s rho coefficient, which measures the severity of autistic behavior and visual, auditory, and motor cognitive flexibility, yielded the following values: −0.57 (p.01), −0.60 (p.01), and −0.64 (p.01). The Spearman’s rho coefficient produced values of −0.51 (p.05) for auditory cognitive flexibility and motor cognitive flexibility (Table 3). In this study, the model of multiple linear regression analysis is significant (F = 6.49, p = 0.005).
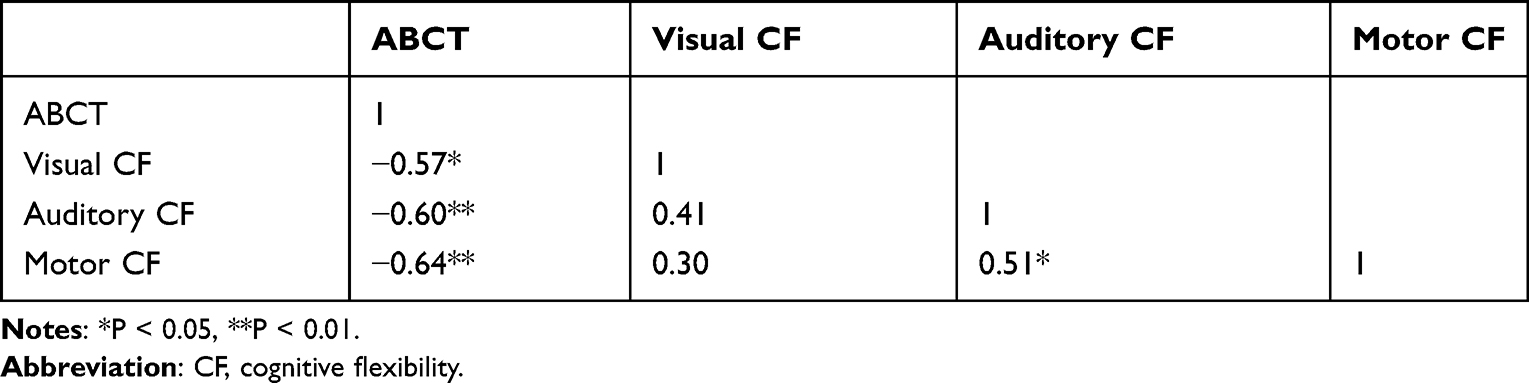 |
Table 3 The Spearman’s Rho Coefficient Among These Variables |
Discussion
The Performance of Pre-Switching Task and Post-Switch Task of Cognitive Flexibility
In three cognitive flexibilities, all subjects with ASD passed the pre-switch phase. However, there was a significant difference in the inability to pass at the post-switch phase in three cognitive flexibilities. As the difficulty of the task increases, so does the performance of those with ASD.12 Thus, the test manipulation in this study was designed to reduce task difficulty while removing the influence of confounding factors like working memory load or IQ. According to Zelazo (2013), the symptom of perseveration in children cannot be directly attributed to children’s memory limitations.22 The working memory demands was by means of controlling the number of dimensions used to sort the cards kept one for the pre- and post-switch of the visual cognitive flexibilities subtest. As a result, our data showed that children with ASD did not pass the post-switch task due to cognitive flexibility deficits. This study’s findings were similar to those of two other studies that found flexibility impairment in children with ASD when card sorting.17,23
Before administering the formal test of auditory cognitive flexibility, the examiner ensured that the subjects with ASD understood the meaning of opposite words (day and night, adult and child). Our findings indicated that children with ASD had difficulty with cognitive flexibility. This result could be due to the child’s inability to inhibit pre-switching information, reallocate their attention, and convert to an opposite word or movement after the examiner delivered the verbal command or movement, rather than their inability to retrieve the opposite word from memory. In our study, children with ASD had lower auditory and motor cognitive flexibility than they did visual cognitive flexibility. The possible reason was that subjects with ASD often rely on visual cues,24 the target cards may have been used as a basis of reference for sorting. The auditory cognitive flexibility subtest demanded that the brain quickly switch to the new rule, then re-integrate and execute speech output. In the motor cognitive flexibility subtest, participants were required not only to convert visual information about the examiner’s movements into motor representations, but also to quickly process the translation rules into output movements. Therefore, cognitive shifting with motor and auditory inputs was more difficult than cognitive shifting with visual inputs.
According to the concept of neural network models, latent representations process the efficacy of synapses and active representations process the sustained firing of neurons. When a subject with ASD exhibits cognitive inflexibility, latent representations of prior rules via synaptic connections are stronger than active representations of the current rule considered as a component of working memory.25
Age Effect on the Cognitive Flexibility
DCCD is commonly used to evaluate the ability to discriminate the visual feature of cards to sort, self-control, negative priming,26 antecedent to consequence27 and cognitive flexibility to preschool children. Therefore, the card sorting task involves the integration of many capabilities.
The Cognitive flexibility of vision continue to progress beyond age 722 and the majority of four-year-olds adjust correctly to the new dimension,26 children with ASD aged 5 performed better than those aged 4 in the visual cognitive flexibility test, but not in the auditory and motor subtests in the present study.
In the present study, age had a weaker effect on the auditory and motor cognitive flexibility of subjects with ASD. According to the data of this study, these two abilities were still underdeveloped at the age of four or five. At the post-switch phase, the average score was 1–2, and children with ASD passed all test items, earning a total of 6 points at the pre-switch phase. However, there was no data on typical children to compare in this study. However, the differences in the two phases of auditory and motor cognitive flexibility were significant, leading to the conclusion that children with ASD had auditory and motor cognitive inflexibilities at the age of 4–5 years.
Relationship Between the Performance of Cognitive Flexibility and Autistic Behavior
Previous studies have revealed inconsistent associations between repetitive behaviors and cognitive flexibility. There was high relation between cognitive flexibility with the restrictive, repetitive symptoms of ASD.28 However, the result of Kelly and Reed (2021) showed that cognitive flexibility was not significantly associated with stereotyped behavior tested by stimulus over-selectivity in individuals with ASD.16 In Kelly’s study, the Intra- dimensional/Extra-dimensional set-shifting task (ID/ED) was used to test the performance of cognitive flexibility. The different research tools used to study cognitive flexibility may be the reason for the different results. Another research indicated that the performance on the DCCS task did not predict the severity of autism symptoms at a mean age of 9.99 (2.78). In our study, overall symptoms of autistic behaviors were used, not just RRB, which may be the reason for the different findings of the relationship. A negative correlation indicated that lower activity in the right lateral prefrontal cortex was correlated with the severe stereotyped and persistent behaviors presented in children with ASD.29
Conclusions
There was a significant difference in the pass changes of subjects with ASD number between the pre-switching and post-switching tasks in visual cognitive flexibility, auditory cognitive flexibility, and motor cognitive flexibility. Although age had no effect on performance on the three cognitive flexibility tasks in the pre-switching phase, there was an age effect on the total score of visual cognitive flexibility (the performance of 5-year-olds with ASD was better than the 4-year-olds). The negative correlation of the three cognitive flexibilities with autistic behaviors was moderate.
This finding prompted additional research because research data on auditory and motor cognitive flexibility are scarce in comparison to visual cognitive flexibility. According to the findings, the motor and auditory cognitive flexibility scores were significantly lower than the visual cognitive flexibility score. Thus, this study suggests that early intervention practitioners or teachers might focus on auditory and motor rule switching task to enhance children’s cognitive flexibility when training children with ASD. Teachers may incorporate basic movements or activities with which children are already familiar for motor cognitive flexibility training. Teachers could use a one-on-one association game to train auditory cognitive flexibility. For example, the teacher could give the child several pairs of words, such as sun-moon, table-chair, teacher-student, child-adult, go in-go out, and father-mother. After giving this information, the teacher would say one of the words in the pair, and let the child say the other word. Playing this game may improve children’s auditory cognitive flexibility.
Only 19 children with ASD participated in this study. There were just a few number of participants; thus, the results cannot be generalized to all those with ASD. Although this study already controlled the confounding factor of working memory by means of one dimension at an item of test and selected children with ASD with IQ >70 and understanding verbal instruction of tests, no assessment measures were provided to evaluate the effect of working memory and language ability on cognitive flexibility. Children with ASD sometimes exhibited a combination of attention deficit behavior, and impulsive behavior that may have affected the scores during the administration of tests. Our study proposes investigating the difference in cognitive flexibility between subjects with ASD who have ADHD and those who do not.
In this study, the visual cognitive flexibility subtest was given first, then the auditory subtest, and finally, the motor subtest. For future references, the motor subtest should follow the visual subtest, with the auditory subtest given last. Because most ASD participants have a short attention span, scheduling the motor subtest between the other subtests may increase the attention span needed to complete the overall testing. To avoid order effects in future references, the sequence of subtests could be random.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mogadam A, Keller AE, Arnold PD, et al. Magnetoencephalographic (MEG) brain activity during a mental flexibility task suggests some shared neurobiology in children with neurodevelopmental disorders. J Neurodev Disord. 2019;11(1):1–12. doi:10.1186/s11689-019-9280-2
2. Doebel S, Zelazo PD. A meta-analysis of the dimensional change card sort: implications for developmental theories and the measurement of executive function in children. Dev Rev. 2015;38:241–268. doi:10.1016/j.dr.2015.09.001
3. Buttelmann F, Karbach J. Development and plasticity of cognitive flexibility in early and middle childhood. Front Psychol. 2017;8:1040. doi:10.3389/fpsyg.2017.01040
4. Rikhye RV, Gilra A, Halassa MM. Thalamic regulation of switching between cortical representations enables cognitive flexibility. Nat Neurosci. 2018;21(12):1753–1763. doi:10.1038/s41593-018-0269-z
5. Braem S, Egner T. Getting a grip on cognitive flexibility. Curr Dir Psychol Sci. 2018;27(6):470–476. doi:10.1177/0963721418787475
6. Lung SLM, Bertone A. Brief report: an exploration of cognitive flexibility of autistic adolescents with low intelligence using the Wisconsin card sorting task. J Autism Dev Disord. 2021;23:1–7.
7. Smidts DP, Jacobs R, Anderson V. The Object Classification Task for Children (OCTC): a measure of concept generation and mental flexibility in early childhood. Dev Psychol. 2004;26(1):385–401.
8. Melo C, Ruano L, Jorge J, et al. Prevalence and determinants of motor stereotypies in autism spectrum disorder: a systematic review and meta-analysis. Autism. 2020;24(3):569–590. doi:10.1177/1362361319869118
9. Perner J, Lang B. What causes 3‐year‐olds’ difficulty on the dimensional change card sorting task? Infant Child Develop Int J Res Pract. 2002;11(2):93–105. doi:10.1002/icd.299
10. Yi L, Liu Y, Li Y, Fan Y, Huang D, Gao D. Visual scanning patterns during the dimensional change card sorting task in children with autism spectrum disorder. Autism Res Treat. 2012;2012. doi:10.1155/2012/123053
11. Van Eylen L, Boets B, Steyaert J, Evers K, Wagemans J, Noens I. Cognitive flexibility in autism spectrum disorder: explaining the inconsistencies? Res Autism Spectr Disord. 2011;5(4):1390–1401. doi:10.1016/j.rasd.2011.01.025
12. Reed P. Behavioural flexibility of children with Autism Spectrum Disorder on a card-sorting task with varying task difficulty. Heliyon. 2018;4(10):e00842. doi:10.1016/j.heliyon.2018.e00842
13. De Vries M, Geurts HM. Cognitive flexibility in ASD; task switching with emotional faces. J Autism Dev Disord. 2012;42(12):2558–2568. doi:10.1007/s10803-012-1512-1
14. Memari AH, Ziaee V, Shayestehfar M, Ghanouni P, Mansournia MA, Moshayedi P. Cognitive flexibility impairments in children with autism spectrum disorders: links to age, gender and child outcomes. Res Dev Disabil. 2013;34(10):3218–3225. doi:10.1016/j.ridd.2013.06.033
15. Kopp B, Maldonado N, Scheffels JF, Hendel M, Lange F. A meta-analysis of relationships between measures of Wisconsin card sorting and intelligence. Brain Sci. 2019;9(12):349. doi:10.3390/brainsci9120349
16. Kelly M, Reed P. Examination of stimulus over-selectivity in children with autism spectrum disorder and its relationship to stereotyped behaviors and cognitive flexibility. Focus Autism Other Dev Disabl. 2021;36(1):47–56. doi:10.1177/1088357620943504
17. Faja S, Dawson G. Performance on the dimensional change card sort and backward digit span by young children with autism without intellectual disability. Child Neuropsychol. 2014;20(6):692–699. doi:10.1080/09297049.2013.856395
18. Krug DA, Arick J, Almond P. Behavior checklist for identifying severely handicapped individuals with high levels of autistic behavior. J Child Psychol Psychiatry. 1980;21(3):221–229. doi:10.1111/j.1469-7610.1980.tb01797.x
19. Huang J, Wu Y. Autism Behavior Checklist-Taiwan Version: User’s Manual. Taipei, Taiwan: Psychological Corporation; 2013.
20. Zelazo PD. The Dimensional Change Card Sort (DCCS): a method of assessing executive function in children. Nat Protoc. 2006;1(1):297–301. doi:10.1038/nprot.2006.46
21. Gerstadt CL, Hong YJ, Diamond A. The relationship between cognition and action: performance of children 312–7 years old on a stroop-like day-night test. Cognition. 1994;53(2):129–153. doi:10.1016/0010-0277(94)90068-X
22. Zelazo PD, Muller U, Frye D, et al. The development of executive function in early childhood. Monogr Soc Res Child Dev. 2003;68(3):
23. Chen S-F, Chien Y-L, Wu C-T, Shang C-Y, Wu -Y-Y, Gau S. Deficits in executive functions among youths with autism spectrum disorders: an age-stratified analysis. Psychol Med. 2016;46(8):1625–1638. doi:10.1017/S0033291715002238
24. Tomchek SD, Dunn W. Sensory processing in children with and without autism: a comparative study using the short sensory profile. Am J Occup Ther. 2007;61(2):190–200. doi:10.5014/ajot.61.2.190
25. Yerys BE, Munakata Y. When labels hurt but novelty helps: children’s perseveration and flexibility in a card‐sorting task. Child Dev. 2006;77(6):1589–1607. doi:10.1111/j.1467-8624.2006.00961.x
26. Kloo D, Perner J. Disentangling dimensions in the dimensional change card‐sorting task. Dev Sci. 2005;8(1):44–56. doi:10.1111/j.1467-7687.2005.00392.x
27. Zelazo PD, Frye D. Cognitive complexity and control: a theory of the development of deliberate reasoning and intentional action. In: Stamenov M, editor. Language Structure, Discourse, and the Access to Consciousness. Vol. 12. Amsterdam and Philadelphia John Benjamins; 1997:113–153.
28. Lopez BR, Lincoln AJ, Ozonoff S, Lai Z. Examining the relationship between executive functions and restricted, repetitive symptoms of autistic disorder. J Autism Dev Disord. 2005;35(4):445–460. doi:10.1007/s10803-005-5035-x
29. Yasumura A, Kokubo N, Yamamoto H, et al. Neurobehavioral and hemodynamic evaluation of cognitive shifting in children with autism spectrum disorder. J Behav Brain Sci. 2012;2(4):463–470. doi:10.4236/jbbs.2012.24054
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.