Back to Journals » Infection and Drug Resistance » Volume 13
The Performance of the Abbott Real Time MTB RIF/INH Compared to the MTBDRplus V2 for the Identification of MDR-TB Among Isolates
Authors David A ![]() , Singh L, Da Silva P
, Singh L, Da Silva P ![]() , Scott L
, Scott L ![]() , Stevens W
, Stevens W
Received 28 January 2020
Accepted for publication 8 August 2020
Published 28 September 2020 Volume 2020:13 Pages 3301—3308
DOI https://doi.org/10.2147/IDR.S247524
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eric Nulens
Anura David,1 Lyndel Singh,1 Pedro Da Silva,1,2 Lesley Scott,1 Wendy Stevens1,2
1Department of Molecular Medicine and Haematology, University of the Witwatersrand, Johannesburg, South Africa; 2National Priority Program, National Health Laboratory Services, Johannesburg, South Africa
Correspondence: Anura David
Department of Molecular Medicine and Haematology, University of the Witwatersrand, 7 York Road, Parktown, Johannesburg 2193, South Africa
Tel +27 10 001 3914
Email [email protected]
Background: The GenoType MTBDRplus V2 line-probe assay (LPA) is routinely used in clinical patient management to characterise the susceptibility of Mycobacterium tuberculosis complex to rifampicin (Rif) and isoniazid (INH) directly from sputum and cultured isolates. The laboratory workflow requires skill and three separate areas to minimize contamination and banding pattern interpretation requires experienced laboratory personnel. We explored the use of the RT MTB RIF/INH assay performed on the Abbott m 2000 platform as an alternative laboratory platform.
Methods: Isolates (n=93) consisting of fully susceptible, Rif- or INH-mono-resistant and multi-drug resistant (MDR) strains were tested on both MTBDRplus v2 and RT MTB RIF/INH assays. Both assays target the rpoB, katG and inhA genes for resistance-detection mutations. Concordance was assessed using percent agreement and the kappa statistic. Those specimens with discordant results were further assessed using Sanger sequencing.
Results: A total of 89% (83/93) of cultured isolates generated successful results on the RT MTB/RIF-INH assay and MTBDRplus assays. Of the 10 discordant results, where sequencing was used as the reference method, the RT MTB RIF/INH assays misclassified six resistance isolates, while the LPA misclassified seven.
Discussion: Overall, the RT MTB RIF/INH demonstrated good agreement with the LPA, and a better correlation with sequencing on discrepant isolates specifically with mutations occurring in codon 511 of the rpoB gene. The RT MTB RIF/INH therefore can be used to complement existing laboratory algorithms determining Rif and INH resistance profiles, with less emphasis on manual laboratory processing.
Keywords: molecular diagnostics, tuberculosis, line-probe assay
Introduction
Molecular technology is well applied in current tuberculosis (TB) diagnostic algorithms, with no better example than the Xpert MTB/RIF (Xpert), with a footprint in >130 countries.1 Although this technology simultaneously detects the presence of Mycobacterium tuberculosis complex (MTBC) and susceptibility to rifampicin (Rif) across several clinical specimen types, it is not designed to detect resistance to isoniazid (INH). According to the World Health Organisation (WHO), globally 8% TB cases show monoresistance to INH. In South Africa’s current TB diagnostic algorithm, INH resistance is detected using the GenoType MTBDRplus V2 line-probe assay {LPA}2 (HAIN Lifesciences, Nehren, Germany), that can be performed directly on decontaminated sputum and indirectly off Mycobacterial Growth Indicator tubes (MGIT) isolates. This LPA is based on DNA Strip technology and is used for the determination of resistance to Rif and INH in MTBC.3–6 Version 1 of this assay was endorsed by the WHO in 2008.7 At the time, the assay had the advantage of enabling rapid detection of MTBC and resistance profiling (in less than 48 hours) and was also available as a high-throughput technology (48 specimens per batch using the GT Blot 48 [HAIN Lifesciences, Nehren, Germany]). However, due to the performance of the assay, the WHO recommended the version 1 LPA for use on smear-positive sputum specimens only.7 In 2012, version 2 of the LPA became available with recommendations for use on both smear-positive and smear-negative sputum specimens. However, despite its improvements, assay performance is still affected by bacillary load.5 The sensitivity and specificity of the LPA assay for MTBC detection varies across studies. A study conducted in South Africa demonstrated a sensitivity of 73.1% (95% CI: 59.8–83.2%) and a specificity of 100% (95% CI: 80.6–100%)6 whilst in Ethiopia, the sensitivity and specificity of the assay was determined as 96.4% (95% CI: 81.7–99.9) and 100% (95% CI: 88.8–100)4 respectively, with other countries reporting sensitivities around 88–99%.8–10 Sensitivity of the LPA on smear-negative sputum in the above-mentioned studies was reported as 57–79%. For Rif resistance, the LPA assay demonstrates sensitivity ranging between 88.2% and 98.1% and for INH resistance, between 92% and 94%.8–10 LPA performance on cultured isolates has previously been evaluated with a sensitivity for Rif resistance of100% (95% CI: 76.8–100) and specificity of 87.9% (95% CI: 78.9–94.1); INH resistance detection with a sensitivity of 100% (95% CI: 91.8–100) and specificity of 94.4% (95% CI: 84.6–98.8).11 However, the LPA is labour intensive since the DNA extraction, preparation for amplification, hybridisation (if using the Twincubator) and result interpretation are manual processes (unless using a Genoscan® for automated result interpretation). The operation and interpretation requires a higher degree of skill and a laboratory infrastructure with three separate rooms to prevent contamination. An in-house study investigating the subjectivity of LPA strip interpretation using different light sources (personal communication Robert Coombs) demonstrated that strip interpretation is difficult and subjective due to differing band intensities read under different lighting conditions (normal fluorescent lighting, sunlight and an i-Phone light). Of 15 strips prepared from clinical isolates and read by eight individuals, four strips produced varying outcomes with the highest discordance being seen under normal fluorescent lighting. This led to an investigation of alternative molecular platforms that potentially could provide less subjective result outcomes.
One such technology is the m2000 (Abbott Molecular, Des Plaines, IL, United States), which in South Africa has shown to be a reputable and robust platform for high-throughput HIV-1 testing since 2010,12 and also investigated as a platform for integrated HIV/TB diagnostics. The RT MTB assay which is performed on the m2000 system is a qualitative in vitro molecular assay for the direct detection of MTBC, with an optional reflex feature to the RT MTB RIF/INH assay for detection of Rif and INH resistance. The pooled sensitivity of RT MTB for detecting TB is reported in a meta-analysis as 96.0% (95% CI: 88.0–99.0) and specificity of 97% (95% CI: 93.0–99.0).13 For DR-TB, four studies were included to evaluate the diagnostic accuracy of RT MTB RIF/INH. The pooled sensitivity was 88% (95% CI, 82.0–93.0) and specificity 99% (95% CI: 96.0–99.0).13 Studies from Johannesburg, South Africa14 and Hong Kong15 similarly reported that 30% specimens identified by the RT MTB assay could not generate a result with the reflex assay, RT MTB RIF/INH, due to the limit of detection (LOD). Although this is a disadvantage compared to the Xpert or Xpert MTB/RIF Ultra (Ultra) assays, these latter assays are unable to report INH susceptibility. The ability of the RT MTB RIF/INH assay to be performed either in direct testing mode or in reflex mode following a positive RT MTB result16 provides flexibility for this assay to be performed on MGIT cultures isolates, which have higher bacillary loads. The performance of the RT MTB RIF/INH was therefore investigated in comparison to the LPA, as an option to improve laboratory workflow through automation with the m2000 system and capitalize on the large footprint (>400 m2000 instruments supported by >50 field service support staff) across sub-Sahara African countries (personal communication Abbott Molecular (November 2019)).
Materials and Methods
Study Isolates
Stored cultured isolates (−80°C) from the Clinical Laboratory Services biorepository (n=32) as well as residual culture isolates from the National Health Laboratory Services (NHLS) Mycobacteriology Referral Laboratory (n=61) were tested in this evaluation. Cultured isolates (1 mL) were re-subcultured into MGIT. Once these flagged positive on the MGIT 960 instrument (Becton Dickinson, Sparks, MD, USA) and confirmed to be positive for acid-fast bacilli (AFB) by Ziehl Neelsen (ZN) staining, testing was performed using the LPA and the RT MTB RIF/INH assays according to the manufacturer’s instructions17 and as previously described.2,14
Genotyping Assay Description
For the LPA, manual DNA extraction was performed on 1 mL of culture using the GenoLyse® (HAIN Lifesciences, Nehren, Germany) extraction kit, followed by amplification using a Techne TC-512 thermocycler (Labotec Pty Ltd, Johannesburg, South Africa) and hybridisation using the automated GT-Blot 48. Testing was performed in two batches, to accommodate the 93 tests, followed by a manual interpretation of the strips. The LPA assay identifies Rif resistance through the detection of the most significant associated mutations of the rpoB gene (coding for the β-subunit of the RNA polymerase). For detection of INH resistance, the katG gene (coding for the catalase peroxidase) and the promoter region of the inhA gene (coding for the NADH enoyl ACP reductase) are examined. The assay is, therefore, able to provide information on the level of INH resistance detected (mutations in the katG regions are associated with high-level resistance while mutations in the inhA gene region are associated with low-level INH resistance). In certain instances, the absence of a wild-type (WT) band with an absence of the corresponding mutant band indicates that a specific resistance conferring mutation cannot be identified and resistance can then only be inferred. Updates to the interpretation of the LPA strips in the HAIN Lifescience Instructions for Use (IFU) resulted in a re-evaluation of strip interpretation in 2019.18
For the RT MTB RIF/INH assay, 500 μL of culture was inactivated in a ratio of 1 (culture): 3 (inactivation reagent) for a period of 1 hour. This was followed by nucleic acid extraction on the m2000sp instrument and amplification and detection on the m2000rt instrument. For each of the three gene targets, results are provided as WT if no resistance is detected. If resistance is detected, the absence of the relevant probe is provided for the rpoB gene or the relevant mutation is provided for the katG and inhA genes. Similarly, to the LPA, inferred resistance can also be detected in the RT MTB RIF/INH assay, where specific mutation information is not provided.
Those specimens with discordant results were further assessed using targeted Sanger sequencing (performed at the South African Medical Research Council Centre for tuberculosis research at Stellenbosch University) of the rpoB, katG and inhA genes.
Concordance between the RT MTB RIF/INH reflex assay and the LPA assay was assessed using percent agreement and the kappa statistic using Stata version 14 (StataCorp, College Station, TX, USA).
Ethics Statement
Ethics approval was obtained from the University of the Witwatersrand Human Research Ethics Committee for the use of residual specimens received for routine diagnostic testing (M150160: Research and Development (R&D) Programme).
Results
Biorepository Isolate Composition Determined by the Standard-of-Care (SOC) MTBDRplus V2 and the RT MTB RIF/INH Assays
Of the 87 isolates, which produced results on the LPA, 83 produced valid resistance profiles. Similarly, on the RT MTB RIF/INH assay, 83 isolates produced valid resistance profiles but not all reportable results were produced on the same isolates as the LPA. Both assays, therefore, produced indeterminate results on the same number of isolates (n=10). No repeat testing was performed on either assay. Table 1 outlines the standard of care (SOC) results reported by LPA and the results reported by the RT MTB RIF/INH assay. The LPA categorised the resistant isolates as 51.5% (34/66) resistant to both Rif and INH, 28.8% (19/66) resistant to Rif only and 19.7% (13/66) resistant to INH only. 19.5% (17/87) were categorised as susceptible to Rif and INH and 4.6% (4/87) indeterminate for both Rif and INH.
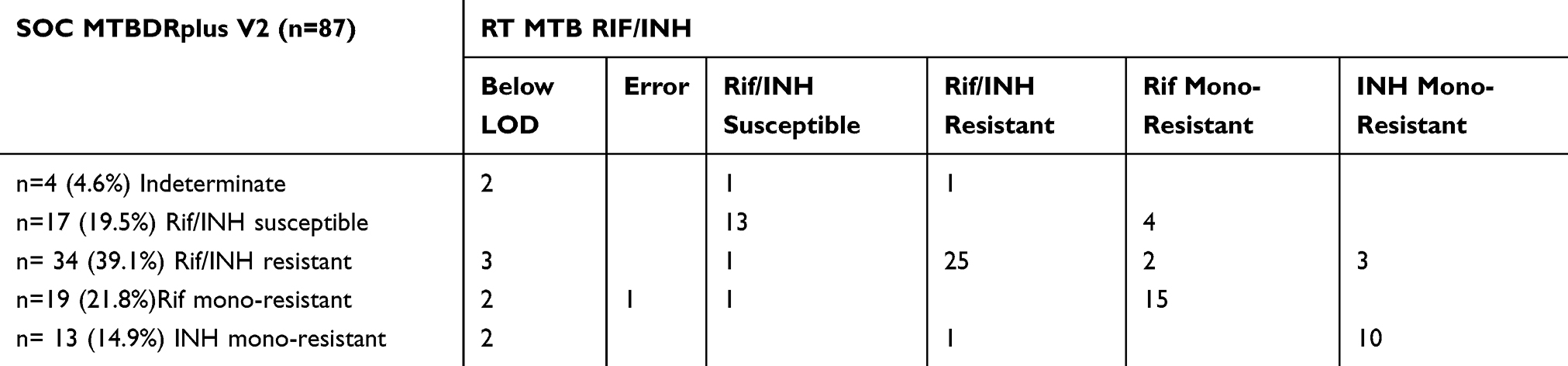 |
Table 1 Rif and INH Resistance Profile Determined by the SOC MTBDRplus V2 and the RT MTB RIF/INH |
Rif Genotyping
The most common rpoB gene mutation identified by the LPA assay as outlined in Table 2 was the S531L (n=15 [28.3%]), followed by the D516V mutation in 18.9% (n=10) of isolates. The LPA inferred resistance in 26.4% (n=14) of isolates. On the RT MTB RIF/INH assay (Table 3), Probe 4 was missing in 35.3% (n=18) of isolates indicating a mutation/s in codons 531–533 of the rpoB gene. 21.6% (n=11) of isolates demonstrated a missing Probe 2 with another 21.6% demonstrating a missing Probe 5 indicating mutation/s in codons 513–516 and 519–522, respectively. Inferred resistance was detected in one isolate on the RT MTB RIF/INH assay. Of the 73 isolates which demonstrated valid Rif resistant results for both assays, 89.0% (n=65) showed substantial agreement between the 2 assays (Kappa: 0.765).
 |
Table 2 Summary of Mutations Reported by the GenoType ® MTBDRplus V2 Assay |
 |
Table 3 Summary of Mutations Reported by the Abbott RT MTBRIF/INH Assay |
INH Genotyping
The most common mutation on the LPA for INH resistance was the S315T1 mutation on the katG gene which accounted for 44.7% (n=21) of resistance (Table 2). Co-occurring mutations (S315T and either a T8A or C15T) accounted for a further 34% (n=16) of resistance. On the RT MTB RIF/INH assay, the S315T mutation on the katG gene was reported in 76.7% (n=33) of isolates. The frequency of the inhA −15 mutation was 16.3% (n=7). Co-occurring mutations (S315T and −15T) accounted for a further 2.3% (n=1) of resistance. Of the 75 isolates which demonstrated valid INH resistant results for both assays, 96.0% (n=72) showed almost perfect agreement between the two assays (Kappa: 0.919).
Discordant Genotype Results
Targeted sequencing of the rpoB, katG and inhA genes was performed on 10 isolates that reported discordant results between the LPA and RT MTB RIF/INH assays as listed in Table 4. The LPA incorrectly classified 6/10 isolates as Rif susceptible, among codon 511 and 533, while the RT MTB RIF/INH assay misclassified 2/10 isolates as Rif susceptible, among codon 526 and 531. The LPA missed a deletion in Codon 262 of the katG gene in 2/10 isolates and incorrectly identified these two isolates as INH susceptible. In addition, 1/10 of isolates were incorrectly classified as INH resistant (demonstrated a dual S315T mutation in the katG gene and a C15T mutation in the inhA gene). The RT MTB RIF/INH assay incorrectly classified 4/10 isolates as INH susceptible. Deletions in Codon 262 were missed in three isolates as well as in an isolate where the deletion co-occurred with an S315T1 mutation.
 |
Table 4 List of Discrepant Results and Validation with Sequencing |
These results demonstrate that with the SOC LPA testing, six isolates were incorrectly identified as drug susceptible (Rif resistance was confirmed both by the RT MTB RIF/INH assay and sequencing) and another isolate was incorrectly identified resistant to INH (susceptibility to INH was confirmed both by the RT MTB RIF/INH assay and sequencing). If the RT MTB RIF/INH results have been used in the diagnostic algorithm, six isolates would have been incorrectly identified as fully susceptible (Rif resistance was confirmed in two isolates and INH resistance in the other four isolates by sequencing).
Discussion
For Rif, the S531L mutation is the most common mutation in the rpoB gene accounting for 29%-80% of global resistance19–21 and is considered a high-confidence mutation.22 The isolates selected for this study were a combination of those containing this S531L and katG (S315T) mutations in addition to some with less frequent rpoB D516V and H526Y mutations. These mutations appear to vary widely across geographical areas as demonstrated by Van Deun A et al23 who reported D516V mutation frequencies of 3.4% and 7.1%; and H526Y mutation frequencies of 9.7% and 2.4% from Bangladesh and Kinshasa, respectively. Although both assays produced the same number of indeterminate results (n=10), the RT MTB RIF/INH was able to correctly detect Rif and/or INH susceptibility in one more isolate than the LPA, thereby providing more accurate genotyping result reporting based on reference sequencing outputs. For the Rif only and INH only resistant isolates, the RT MTB RIF/INH assay demonstrated better performance on Rif resistance detection than the LPA (21 vs 19), while both assays demonstrated similar performance for INH resistance detection. Although both assays demonstrated good agreement for Rif resistance detection among the more frequently occurring mutations, the RT MTB RIF/INH assay was able to provide additional information on the rare mutations in codon 511 on 5 more isolates than the LPA assay. Deficiencies of the RT MTB RIF/INH assay include missed mutations in codons 526 (global frequency of 0.2%-1%)20,21 and S531L (this mutation was detected in 11/12 [92%] isolates). A misdiagnosis for Rif on the RT MTB RIF/INH assay has also been demonstrated previously on H526D, H526R and L533P mutations.24,25 For the 10 discordant isolates, and using sequencing as the reference, the LPA misclassified five isolates for Rif resistance profiling versus 2 on the RT MTB RIF/INH assay. The LPA, therefore, missed three additional Rif resistant isolates as compared to the RT MTB RIF/INH assay. This is in line with a previous study that demonstrated the LPA misses some mutations (del 517, D516Y, S522P, L530L, S531L and L553P) in the rpoB gene.26 Of the five isolates, the missed mutation is the minimal-confidence L511P mutation (demonstrated to occur at a frequency of 3%)20 in 45.5% of isolates. The banding patterns on the LPA for these five isolates did, however, display weaker WT2 band staining than the other WT bands on the strips, which usually occurs in the case of an L511P or L533P mutation (personal communication with HAIN Lifesciences). In addition, a similar feint WT8 band was displayed for the isolate which contained the L533P mutation. These strips highlight the requirement for experienced laboratory personnel for the interpretation of banding patterns.
For INH, both assays demonstrated almost perfect agreement but the LPA was able to provide one additional INH resistance profile compared to the RT MTB RIF/INH assay. The most common mutation detected by both assays is the S315T mutation which occurs at a frequency of 64%.27 The RT MTB RIF/INH assay misclassified four isolates (compared to sequencing for INH) compared to three on the LPA. On the LPA, for the culture isolate, which demonstrated resistance in the katG region, the intensity of the MUT1 band indicates that a mixed infection may be present. On the RT MTB RIF/INH assay, the deletion that was missed (Codon 262, Position 1 (A)) in the katG gene is a deletion that was also missed by the LPA in 2/4 (50%) of isolates displaying this mutation in this study. The RT MTB RIF/INH assay also missed an S315T mutation in the katG gene in one isolate but this mutation was correctly detected in the other 19 (95%) isolates.
Alternative molecular technologies other than the LPA are becoming available (WHO interim report) and provide resistance profiles for Rif and INH, which are automated with high-throughput capability as outlined in Table 5. These technologies include the cobas MTB and MTB RIF/INH assays, FluoroType MDRTB, BD MAX MTBDR and Abbott RT MTB and MTB RIF/INH assays’. All these assays are based on real-time PCR. The cobas® MTB assay (Roche Molecular Diagnostics, Pleasanton, CA, USA) detects MTBC by targeting the 16S rRNA and 5 esx genes and can generate results for 94 tests in 3.5 hours. Testing on the cobas MTB RIF/INH assay can be performed in an additional 3.5 hours.18 The MAX MDR-TB is performed on the BD MAX System to detect MTBC through targeting IS6110, IS1081 and devR19 with 24 specimens tested per batch and results reported within 4 hours. The FluoroType® MTBDR assay (Hain Lifescience, Nehren, Germany) uses LATE-PCR amplification and lights-on/lights-off chemistry to detect MTBC by targeting the rpoB gene.19 Results are generated within 4 hours and 94 specimens tested in a batch. Rif and INH resistance profiling for all three assays (cobas® MTB RIF/INH, FluoroType® MTBDR and BD MDR-TB) is performed through the detection of mutations in the rpoB gene, katG gene and inhA promoter region. Both the BD MDR-TB and the FluoroType MTBDR offer the advantage of differentiating between high- and low-level INH resistance but only the FluoroType MTBDR results include specific mutations identified for the three gene targets. The Xpert and BD tests are “closed” cartridge and cassette-based assays, whereas the RT MTB assay, RT MTB RIF/INH and cobas® MTB and MTB-RIF/INH are assays that may be performed independently. The Abbott, Roche and Cepheid platforms also address system efficiencies through multidisease testing available on a single platform to potentially simplify workflow, increase access and improve disease management.13 The Fluorocycler as with the current Xpert and Ultra assays isolate whole MTBC from inactivated specimens prior to DNA extraction.
 |
Table 5 Summary of High-Throughput Rif and INH Genotyping Technologies |
Conclusions
Overall, the RT MTB RIF/INH demonstrated good agreement with the LPA and compared better with sequencing on discordant isolates than the LPA. RT MTB RIF/INH, therefore, shows good potential to be used in current testing algorithms for the determination of Rif and INH clinically relevant mutations.
Acknowledgments
The authors would like to thank Kate Shearer (Department of Molecular Medicine and Haematology, University of the Witwatersrand, Johannesburg, SA) and Gabriel Eisenberg (Department of Molecular Medicine and Haematology, University of the Witwatersrand, Johannesburg, SA) for statistical analysis input, Robert Coombs (University of Washington, Seattle and the AIDS clinical Trial Group) for input into the internal LPA strip-reading experiment, HAIN Lifesciences for providing the MTBDRplus kit (free of charge), Abbott Molecular for providing the MTB Real Time RIF/INH kits (free of charge).
Disclosure
Lesley Scott reports Abbott Molecular and Hain LifeSciences provided kits for assay evaluation and funding for laboratory support to retrieve bio-bank specimens. In addition, Professor Lesley Scott has a patent USP 8709712 (related to standardised material for molecular TB tests) with royalties paid to University of the Witwatersrand, Johannesburg, South Africa.
Wendy Stevens, Lesley Scott and Anura David received funding support from the South African Medical Research Council with funds received from the South African National Department of Health, and the UK Medical Research Council, with funds received from the UK Government’s Newton Fund under the UK/South Africa Newton Fund (no. 015NEWTON TB). The authors report no other potential conflicts of interest for this work.
References
1. Tanna GLD, Khaki AR, Theron G, et al. Effect of Xpert MTB/RIF on clinical outcomes in routine care settings: individual patient data meta-analysis. Lancet Glob Health. 2019;7(2):91–99. doi:10.1016/S2214-109X(18)30458-3
2. Berhanu RH, David A, da Silva P, et al. Performance of Xpert MTB/RIF, Xpert Ultra, and Abbott Real Time MTB for the diagnosis of pulmonary tuberculosis in a high HIV burden setting. J Clin Microbiol. 2018;56(12):e00560–e00518. doi:10.1128/JCM.00560-18
3. Bai Y, Wang Y, Shao C, Hao Y, Jin Y. GenoType MTBDRplus Assay for Rapid Detection of Multidrug Resistance in Mycobacterium tuberculosis: A Meta-Analysis. PLoS One. 2016;11:3.
4. Meaza A, Kebede A, Yaregal Z, et al. Evaluation of genotype MTBDRplus VER 2.0 line probe assay for the detection of MDR-TB in smear positive and negative sputum samples. BMC Infect Dis. 2017;17(1):280. doi:10.1186/s12879-017-2389-6
5. Seifert M, Ajbani K, Georghiou SB, et al. A Performance Evaluation of MTBDRplus (version 2) for the Diagnosis of Multidrug-resistant Tuberculosis. Int J Tuberc Lung Dis. 2016;20(5):631–637. doi:10.5588/ijtld.15.0788
6. Barnard M, Gey van Pittius NC, van Helden PD, Bosman M, Coetzee G, Warren RM. The Diagnostic Performance of the GenoType MTBDRplus Version 2 Line Probe Assay Is Equivalent to That of the Xpert MTB/RIF Assay. Journal Clin Microbiol. 2012;50(11):3712–3716. doi:10.1128/JCM.01958-12
7. WHO. Molecular Line Probe Assays for Rapid Screening of Patients at Risk of Multi-Drug Resistant Tuberculosis (MDR-TB). Geneva, Switzerland: World Health Organization; 2008.
8. Madhuri K, Deshpande S, Dharmashale S, Bharadwaj R. Utility of Line Probe Assay for the Early Detection of Multidrug-Resistant Pulmonary Tuberculosis. J Glob Infect Dis. 2015;7(2):60–65. doi:10.4103/0974-777X.157237
9. Ahmed S, Shukla I, Fatima N, Varshney SK, Shameem M. Evaluation of genotype MTBDRplus line probe assay in detection of rifampicin and isoniazid resistance in comparison to solid culture drug susceptibility testing in a tertiary care centre of western Uttar Pradesh. Indian J Med Microbiol. 2017;35:568–574.
10. Crudu V, Stratan E, Romancenco E, Allerheiligen V, Hillemann A, Moraru N. First evaluation of an improved assay for molecular genetic detection of tuberculosis as well as rifampin and isoniazid resistances. J Clin Microbiol. 2012;50(4):1264–1269. doi:10.1128/JCM.05903-11
11. Maningi NE, Malinga LA, Antiabong JF. Comparison of line probe assay to BACTEC MGIT 960 system for susceptibility testing of first and second-line anti-tuberculosis drugs in a referral laboratory in South Africa. BMC Infect Dis. 2017;17:795.
12. Scott LE, Carmona S, Gous N, Horsfield P, MacKay M, Stevens W. Use of a Prequalification Panel for Rapid Scale-Up of High-Throughput HIV Viral Load Testing. J Clin Microbiol. 2012;50(12):4083–4086. doi:10.1128/JCM.01355-12
13. Wang MG, Xue M, Wu SQ, et al. Abbott RealTime MTB and MTB RIF/INH assays for the diagnosis of tuberculosis and rifampicin/isoniazid resistance. Infect Genet Evol. 2019;71:54–59. doi:10.1016/j.meegid.2019.03.012
14. Scott LE, David A, Noble L, et al. Performance of the Abbott RealTime MTB and MTB RIF/INH Assays in a Setting of High Tuberculosis and HIV Coinfection in South Africa. J Clin Microbiol. 2017;55(8):2491–2501. doi:10.1128/JCM.00289-17
15. Tam KK, Leung K, To SW, et al. Direct detection of Mycobacterium tuberculosis and drug resistance in respiratory specimen using Abbott RealTime MTB detection and RIF/INH resistance assay. Diagn Microbiol Infect Dis. 2017;89(2):118–124. doi:10.1016/j.diagmicrobio.2017.06.018
16. Kostera J, Leckie G, Abravaya K, Wang H. Performance of the Abbott RealTime MTB RIF/INH resistance assay when used to test Mycobacterium tuberculosis specimens from Bangladesh. Infect Drug Resist. 2018;11(11):695–699. doi:10.2147/IDR.S158953
17. GenoType MTBDRplus Instructions for Use. Hain Lifesciences; 2018.
18. GmbH HL GenoType MTBDR Plus, VER 2.0, Instructions for Use, IFU-304A-09 Germany2019. Available from: https://www.hain-lifescience.de/en/instructions-for-use.html. Accessed September 4, 2020.
19. Zaw MT, Emran NA, Lin Z. Mutations inside rifampicin-resistance determining region of rpoB gene associated with rifampicin-resistance in Mycobacterium tuberculosis. J Infect Public Health. 2018;11(5):605–610. doi:10.1016/j.jiph.2018.04.005
20. Kapur V, Li L, Lordanescu S, et al. Characterization by Automated DNA Sequencing of Mutations in the Gene (rpoB) Encoding the RNA Polymerase 3 Subunit in Rifampin-Resistant Mycobacterium tuberculosis Strains from New York City and Texas. J Clin Microbiol. 1994;32(4):1095–1098. doi:10.1128/JCM.32.4.1095-1098.1994
21. Georghiou SB, Seifert M, Catanzaro D, et al. Frequency and Distribution of Tuberculosis Resistance-Associated Mutations between Mumbai, Moldova, and Eastern Cape. Antimicro Agents Chemother. 2016;60:3994–4004.
22. Miotto P, Tessema B, Tagliani E, et al. A standardised method for interpreting the association between mutations and phenotypic drug resistance in Mycobacterium tuberculosis. Eur Respir J. 2017;50(6):1701354. doi:10.1183/13993003.01354-2017
23. Van Deun A, Aung KJ, Bola V, et al. Rifampin drug resistance tests for tuberculosis: challenging the gold standard. J Clin Microbiol. 2013;51(8):2633–2640. doi:10.1128/JCM.00553-13
24. Ruiz P, Causse M, Vaquero M, Guitierrez JB, Casal M. Evaluation of a new automated Abbott RealTime MTB RIF/INH assay for qualitative detection of rifampicin/isoniazid resistance in pulmonary and extra-pulmonary clinical samples of Mycobacterium tuberculosis. Infect Drug Resist. 2017;10:463–467. doi:10.2147/IDR.S147272
25. Hoffmann-Thiel S, Molodtsov N, Duffner C, et al. Capacity of Abbott RealTime MTB RIF/INH to detect rifampicin- and isoniazid-resistant tuberculosis. Int J Tuberc Lung Dis. 2019;23(4):458–464. doi:10.5588/ijtld.18.0615
26. Rahman A, Sahrin M, Afrin S, et al. Comparison of Xpert MTB/RIF Assay and GenoType MTBDRplus DNA Probes for Detection of Mutations Associated with Rifampicin Resistance in Mycobacterium tuberculosis. PLoS One. 2016;11(4):4. doi:10.1371/journal.pone.0152694
27. Seifert M, Catanzaro D, Catanzaro A, Rodwell TC. Genetic Mutations Associated with Isoniazid Resistance in Mycobacterium tuberculosis: A Systematic Review. PLoS One. 2015;10(3):e0119628. doi:10.1371/journal.pone.0119628
28. Vinuesa V, Navarro D, Poujois S, Zaragoza S, Borras R. Performance characteristics of the new Abbott Real Time MTB assay for detection of Mycobacterium tuberculosis complex in respiratory specimens. Diagn Microbiol Infect Dis. 2016;84(3):212–214. doi:10.1016/j.diagmicrobio.2015.11.001
29. Tang N, Frank A, Pahalawatta V, et al. Analytical and clinical performance of Abbott RealTime MTB, an assay for detection of Mycobacterium tuberculosis in pulmonary specimens. Tuberculosis. 2015;95(5):613–619. doi:10.1016/j.tube.2015.05.010
30. Chen JH, She KK, Kwong TC, et al. Performance of the new automated Abbott RealTime MTB assay for rapid detection of Mycobacterium tuberculosis complex in respiratory specimens. Eur J Clin Microbiol Infect Dis. 2015;34(9):1827–1832. doi:10.1007/s10096-015-2419-5
31. Kostera J, Leckie G, Tang N, et al. Analytical and clinical performance characteristics of the Abbott RealTime MTB RIF/INH Resistance, an assay for the detection of rifampicin and isoniazid resistant Mycobacterium tuberculosis in pulmonary specimens. Tuberculosis. 2016;101:137–143. doi:10.1016/j.tube.2016.09.006
32. Helb D, Jones M, Story E, et al. Rapid Detection of Mycobacterium tuberculosis and Rifampin Resistance by Use of On-Demand, Near-Patient Technology. J Clin Microbiol. 2010;48(1):229–237. doi:10.1128/JCM.01463-09
33. Blakemore R, Story E, Helb D, et al. Evaluation of the analytical performance of the Xpert MTB/RIF assay. J Clin Microbiol. 2010;48(7):2495–2501. doi:10.1128/JCM.00128-10
34. Chakravorty S, Simmons AM, Rowneki M, et al. The New Xpert MTB/RIF Ultra: improving Detection of Mycobacterium tuberculosis and Resistance to Rifampin in an Assay Suitable for Point-of-Care Testing. mBio. 2017;8(4):e00812. doi:10.1128/mBio.00812-17
35. Murray P, Cooper C, Maus C. Comparative Performance of BD MAX MDR-TB and Cepheid Xpert MTB/RIF Assays. J Clin Microbiol. 2019;57(9):e00779. doi:10.1128/JCM.00779-19
36. de Vos M, Derendinge RB, Dolby T, et al. Diagnostic accuracy and utility of FluoroType MTBDR, a new molecular assay for multidrug-resistant tuberculosis. J Clin Microbiol. 2018;56(9). doi:10.1128/JCM.00531-18
37. Hillemann D, Haasis C, Andres S, Behn T, Kranzer K. Validation of the FluoroType MTBDR Assay for Detection of Rifampin and Isoniazid Resistance in Mycobacterium tuberculosis Complex Isolates. J Clin Microbiol. 2018;56(6):e00072. doi:10.1128/JCM.00072-18
38. Obasanya J, Lawson L, Edwards T, et al. FluoroType MTB system for the detection of pulmonary tuberculosis. ERJ Open Res. 2017;3:2.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.