Back to Journals » International Journal of General Medicine » Volume 17
The Pathology of Intestinal Mucosal Disruption; Implications for Muscle Loss and Physical Dependency from Late Adolescence to Octogenarians
Authors Qaisar R ![]() , Karim A
, Karim A ![]() , Iqbal MS, Muhammad T, Ahmad F, Alkahtani SA
, Iqbal MS, Muhammad T, Ahmad F, Alkahtani SA ![]()
Received 11 November 2024
Accepted for publication 7 December 2024
Published 12 December 2024 Volume 2024:17 Pages 6117—6126
DOI https://doi.org/10.2147/IJGM.S501358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Rizwan Qaisar,1– 3 Asima Karim,1 M Shahid Iqbal,4 Tahir Muhammad,5 Firdos Ahmad,1– 3 Shaea A Alkahtani6
1Basic Medical Sciences, College of Medicine, University of Sharjah, Sharjah, United Arab Emirates; 2Space Medicine Research Group, Sharjah Institute for Medical and Health Sciences, University of Sharjah, Sharjah, 27272, United Arab Emirates; 3Cardiovascular Research Group, Sharjah Institute for Medical and Health Sciences, University of Sharjah, Sharjah, 27272, United Arab Emirates; 4Department of Neurology and Stroke Medicine, Rehman Medical Institute, Peshawar, 25124, Pakistan; 5Department of Biochemistry, Gomal Medical College, Dera Ismail Khan, Pakistan; 6Exercise Physiology Department, College of Sport Sciences and Physical Activity, King Saud University, Riyadh, 11451, Saudi Arabia
Correspondence: Shaea A Alkahtani, College of Sport Sciences and Physical Activity, King Saud University, PO Box: 1949, Riyadh, 11451, Saudi Arabia, Tel +966118063040, Fax +966118063370, Email [email protected]
Background and Objectives: A pathological increase in intestinal permeability causes muscle loss and physical decline by inducing systemic inflammation and oxidative stress. However, most relevant studies investigate older adults, and the appropriate data across age spans remain elusive. This study aimed to examine the associations of intestinal permeability with muscle loss and physical decline across a large span of ages. We measured plasma zonulin, a marker of increased intestinal permeability, from adolescents to octogenarians in association with muscle health and gait speed.
Research Methods and Procedures: In this cross-sectional, observational study, we recruited healthy men, including young (age=18-35 years, n=135), middle-aged (age=35-59 years, n=118), and older (age=60-90 years, n=163) adults for evaluating - handgrip strength (HGS), skeletal muscle mass index (SMI), and gait speed. We also measured plasma zonulin, c-reactive proteins (CRP), and 8—isoprostanes using ELISA assays.
Results: Plasma zonulin gradually increased from young and middle-aged to older adults (all p< 0.05). Conversely, HGS and gait speed were progressively reduced from young and middle-aged to older adults (all p< 0.05). In addition, older adults also exhibited lower SMI than young and middle-aged men (both p< 0.05). Plasma zonulin exhibited significant negative correlations with HGS and gait speed and positive correlations with CRP and 8-isoprostanes in middle-aged and older men (all p< 0.05). We also found significant areas under the curve for the efficacy of plasma zonulin in diagnosing low HGS (< 27kg) and gait speed (0.8 m/s). After adjustment for age, plasma zonulin demonstrated robust negative correlations with HGS and gait speed and positive correlations with CRP and 8-isoprostanes in the cumulative cohort.
Conclusion: Altogether, an increasing intestinal leak from middle age onward contributes to muscle weakness and physical decline. Our data is clinically relevant in understanding and treating physical dependency in middle-aged and older adults.
Keywords: Handgrip strength, zonulin, intestinal permeability, gait speed
Introduction
The human intestine is a significant interface between the external environment and our body systems.1 A tightly packed layer of epithelial cells covers the external surface of the intestine. This enormous mucosal surface (200 m2 in area) ensures the controlled trafficking of microbes and their metabolites, nutrients, toxins, and other material between the intestinal interior and systemic circulation.1 Intestinal tight junctions between epithelial cells primarily control the selective permeability of intestinal mucosa.1,2 The intestinal mucosa releases selective materials into the systemic circulation in a healthy state. However, disease conditions and aging cause the disruption of the intestinal mucosal barrier and the release of several bacterial toxins into the circulation.1 These toxins cause immunosuppression and increase systemic inflammation and oxidative stress, which are implicated in the pathogenesis of several diseases.2,3
Zonulin, an enterotoxin released by the intestinal mucosal cells, is a critical regulator of tight junctions.1 Disruption of intestinal tight junctions results in zonulin release in the systemic circulation.2 Growing evidence suggests plasma zonulin as a marker of increased intestinal permeability. Moreover, elevated plasma zonulin is a signature feature of several chronic inflammatory diseases.2 A causal association between plasma zonulin levels and disease phenotype is also described as the inhibition of zonulin partly reduces disease severity in laboratory and clinical studies.4
A healthy skeletal muscle is critical for maintaining functional independence in the activities of daily living. However, the quality and quantity of skeletal muscle declines with advancing age, termed sarcopenia.5 The process of sarcopenia starts in the fourth decade of life and advances with advancing age.6 An estimated 10–16% of the global elderly population is affected by sarcopenia. Moreover, the prevalence of sarcopenia is higher in older adults with age-related diseases and a sedentary lifestyle.7 Sarcopenia is also a critical trigger of functional dependency and reduced activities of daily living. Several causative factors of sarcopenia are known.6–8 More recently, a pathological increase in intestinal permeability has been recognized as a contributor to muscle loss and functional dependency in advancing age.9 Specifically, we have reported negative associations of plasma zonulin with muscle strength, mass, and physical capacity in older adults with chronic obstructive pulmonary disease,10 heart failure,11 and Alzheimer’s disease.12 However, these studies were conducted in older adults with pathological sarcopenia. Conversely, how intestinal permeability relates to muscle loss and physical decline during physiological aging from early adulthood to advanced age is unknown. A rigorous dissection of such a relation is warranted since several factors independent of age can compromise skeletal muscle and physical capacity, such as a sedentary lifestyle, malnutrition, muscle unloading, and subclinical diseases.6,7,13,14 Therefore, it is critical to investigate the potential contribution of increased intestinal permeability to the loss of skeletal muscle and physical capacity from early adulthood to advanced age.
We hypothesize that intestinal leak is a critical contributor to muscle decline and the loss of physical capacity at various ages. To test this hypothesis, we measured plasma zonulin levels relevant to skeletal muscle mass, strength, and physical capacity during a wide range of age spectra from late adolescence to octogenarians.
Materials and Methods
Study Design & Participants
In this observational, cross-sectional study, we categorized the study participants into three groups, including young (age = 18–35 years, n = 135), middle-aged (age = 35–59 years, n = 118), and old (age = 60–90 years, n = 163) men after obtaining written informed consent. The age grouping was based on a previous study investigating changes in skeletal muscle and physical capacity across an extensive lifespan.15 A minimal sample size of 114 was determined for each age group to achieve a 95% confidence interval and 5% margin of error, given an expected population proportion of 8%. This sample size is sufficient to detect statistically and biologically meaningful results. This calculation was based on an estimated population proportion of 8%, ensuring the statistical and biological significance of our findings. Therefore, we are confident in the adequacy of our sample size for each age group.
The participants were recruited at the Gomal Medical College (GMC), Dera Ismail Khan, Pakistan, and Rehman Medical Institute (RMI), Peshawar, Pakistan. We have previously described the recruitment criteria in detail.16 Briefly, the participants with walking ability who provided written informed consent were included. Conversely, participants with uncontrolled hypertension, diabetes mellitus, organ failures, prolonged bed rest, and recent surgeries were excluded.17 Sarcopenia was diagnosed as having HGS ≤ 27 kg, SMI ≤ 7 kg/m2, and gait speed ≤ 0.8 m/s, according to the European Working Group on Sarcopenia in Older People-2.18 Prior ethics approval was obtained from the Human Research Ethics Committee of GMC and the Clinical Research Ethics Committee of RMI, Pakistan. This study was conducted under the declaration of Helsinki.19
HGS, Body Composition, and Gait Speed
The HGS was assessed by having participants seated on a chair with their elbows flexed at a 90-degree angle by the side of the body. The participants were requested to squeeze the dynamometer three times with maximal force without movements of the other body parts (CAMRY, South El Monte, CA, USA).20 The highest of the three readings was recorded for statistical analysis.21 Body composition, including fat and skeletal muscle mass index (ASMI) was assessed using a bioelectrical impedance analysis scale (RENPHO, Dubai, UAE) consistent with our previous report.10 Participants were asked to walk at their normal pace for six meters to assess gait speed. The time taken to complete the distance was recorded to calculate the gait speed in meters per second, aligning with the established methods.11
Measurement of Circulating Biomarkers
Blood samples were collected from the fasting participants between 8 am and 10 am. Plasma was immediately isolated through centrifugation and stored at −80°C for further analysis.22 The plasma levels of zonulin (Cat # K5601, Immundiagnostik AG, Bensheim, Germany),23 c-reactive proteins (CRP) (R&D Systems, Minneapolis, MN, USA),12 8–isoprostanes (Cayman Chemical, Ann Arbor, MI, USA),24 and creatine kinase (Catalog # EHCKMB, Thermo Fischer Scientific, Dubai, United Arab Emirates),25 were measured using ELISA assays according to the manufacturer’s instructions.
Statistical Analysis
The one-way analysis of variance with Tukey’s post-hoc test was used to compare the three groups for physical and biochemical markers. Linear regression analysis was used to measure the relations of plasma zonulin with plasma biochemistry and sarcopenia parameters. Receiver operating characteristics (ROC) curves were generated to investigate the potential of zonulin in diagnosing low HGS, gait speed, and SMI. The data are presented as mean and standard deviation, and the p-value < 0.05 was taken as statistically significant. Data were analyzed using GraphPad Prism v 8.0.
Results
Characteristics of the Participants
The details about the anthropometry, sarcopenia indices, plasma biochemistry, and comorbidities are described in Table 1. The middle-aged and older adults had lower BMI and phase angles than the younger group (both p < 0.01). Similarly, the HGS and gait speed were lower in middle-aged and older adults than in younger participants (p < 0.05). Older adults also exhibited lower SMI than the other two groups. The proportions of participants with the HGS and gait speed below the respective cutoff values were higher in the middle-aged and older adults than in the younger group (both p < 0.05) (Table 1). Conversely, a higher proportion of participants below the cutoff value for SMI was only found in older adults but not in the middle-aged group. We also found higher plasma zonulin, CRP, 8-isoprostanes, and creatine kinase in middle-aged than young participants, which further increased in older adults (all p <0.05). Lastly, the older adults also exhibited a higher occurrence of anemia, hyperlipidemia, and sarcopenia (all p < 0.05) (Table 1).
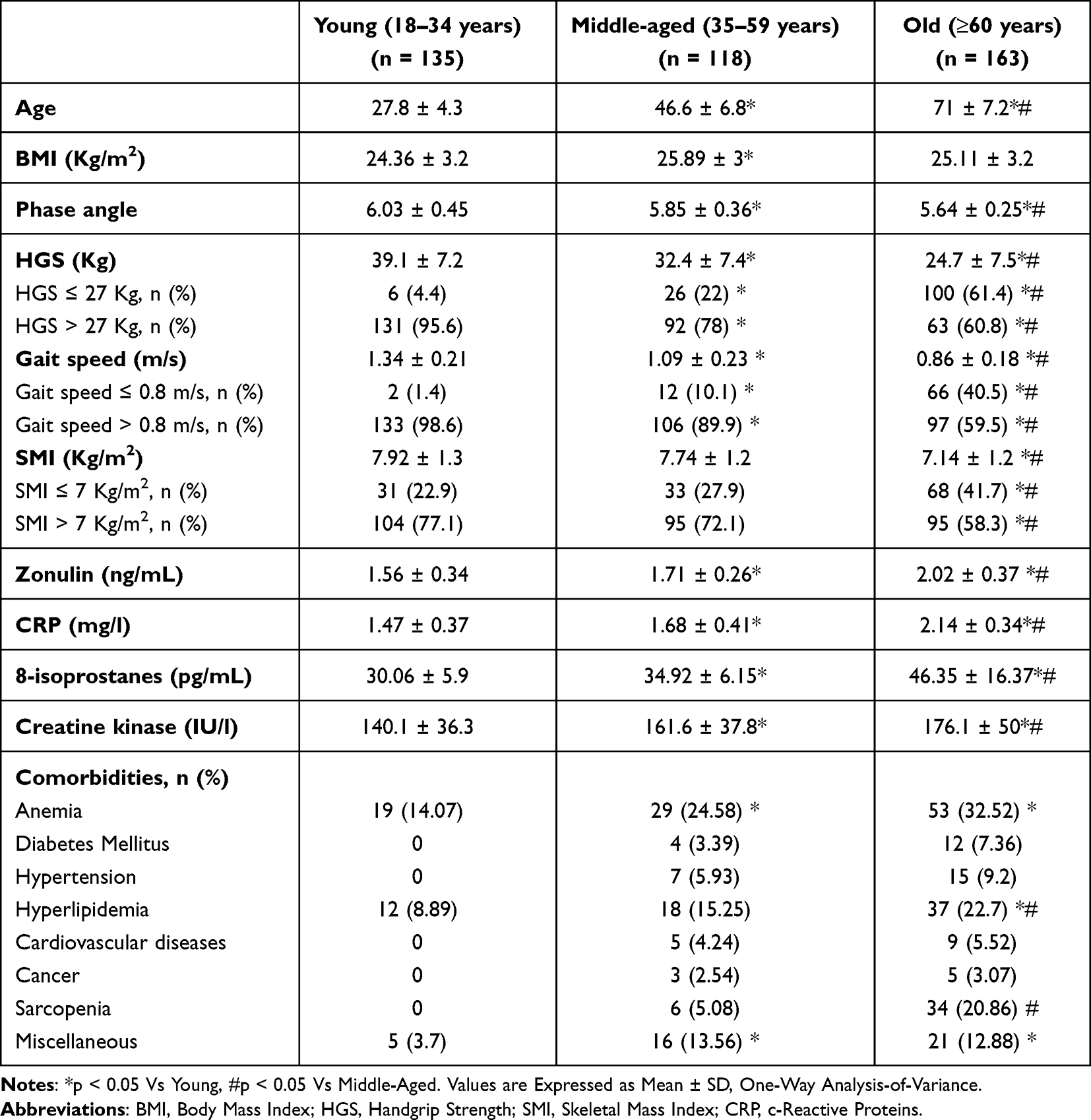 |
Table 1 Anthropometry, Body Composition, Comorbidities, and Plasma Biochemistry of the Study Population. |
Changes in Plasma Zonulin with Age and Plasma Biochemistry
We next asked if plasma zonulin levels correlate with age and plasma biomarkers of inflammation, oxidative stress, and muscle damage. Plasma zonulin exhibited no significant correlations with age in younger participants but exhibited moderate, albeit statistically significant correlations with age in middle-aged (r2 = 0.087, p < 0.05) and older (r2 = 0.071, p < 0.05) adults (Figure 1A). Similarly, we found no correlation of zonulin with plasma CRP in young participants but found significant correlations between zonulin and CRP in middle-aged (r2 = 0.085, p < 0.05) and older (r2 = 0.122, p < 0.05) adults (Figure 1B). Next, we investigated the correlations between plasma zonulin and 8-isoprostanes as markers of oxidative stress. We found significant correlations of plasma zonulin with 8-isoprostanes in all three groups of participants, including young (r2 = 0.097, p < 0.05), middle-aged (r2 = 0.135, p < 0.05), and older (r2 = 0.107, p < 0.05) adults (Figure 1C). Conversely, we found no significant correlation between plasma zonulin and creatine kinase levels as a marker of muscle injury (Figure 1D).
 |
Figure 1 Plasma zonulin levels according to age (A), CRP (B), 8-isoprostanes (C), and creatine kinase (D) in young (n=135), middle-aged (n=118), and older (n=163) adults, *p < 0.05. Abbreviation: CRP, c-reactive proteins. |
Changes in Plasma Zonulin with Skeletal Muscle Quality and Quantity
We next asked if plasma zonulin exhibits correlations with HGS, gait speed, SMI, and phase angles as markers of skeletal muscle quality and quantity. Plasma zonulin levels exhibited significant correlations with HGS in middle-aged (r2 = 0.127, p < 0.05) and older (r2 = 0.155, p < 0.05) adults (Figure 2A). Similarly, zonulin exhibited significant correlations with gait speed in middle-aged (r2 = 0.076, p < 0.05) and older (r2 = 0.164, p < 0.05) adults (Figure 2B). However, a significant correlation between zonulin and SMI was only observed in older adults (r2 = 0.067, p < 0.05) (Figure 2C). On the other hand, we found no correlation between zonulin and phase angle in any of the three age groups (Figure 2D).
 |
Figure 2 Plasma zonulin levels according to HGS (A), gait speed (B), SMI (C), and phase angle (D) in young (n=135), middle-aged (n=118), and older (n=163) adults, *p < 0.05. Abbreviations: HGS, handgrip strength; SMI, skeletal mass index. |
Diagnostic Potential of Plasma Zonulin for Low HGS, Gait Speed, and SMI
We next investigated the diagnostic potential of plasma zonulin for low HGS (≤ 27 kg), low SMI (≤ 7 kg/m2), and low gait speed (≤ 0.8 m/s) in the cumulative study cohort (Figure 3). Plasma zonulin demonstrated significant diagnostic potential for low HGS in the cumulative study pool (AUC = 0.758, 95% CI = 0.711─0.806, p < 0.001) (Figure 3A). We found a comparative diagnostic potential of plasma zonulin for low gait speed in the study population (AUC = 0.741, 95% CI = 0.686─0.794, p < 0.001) (Figure 3B). Conversely, plasma zonulin exhibited a weak, albeit statistically significant diagnostic potential for low SMI in the study population (AUC = 0.609, 95% CI = 0.554─0.664, p = 0.01) (Figure 3C).
 |
Figure 3 ROC curves showing the diagnostic potential of plasma zonulin for low HGS < 27 kg (A), low gait speed < 0.8 m/s (B), and low SMI < 7 kg/m2 (C) in the cumulative study pool (n=416). Abbreviations: ROC, receiver operating characteristic; HGS, handgrip strength; SMI, skeletal mass index. |
Regressions and Correlations of Plasma Zonulin
Lastly, we investigated the regressions and correlations of plasma zonulin with physical and plasma biochemical markers. Without adjustment for age, plasma zonulin exhibited various degrees of significant regressions and correlations with plasma CRP, 8-isoprostanes, HGS, and gait speed in the individual age groups (Table 2). Conversely, the cumulative study pool exhibited significant correlations of plasma zonulin with all three plasma biomarkers (CRP, 8-isoprostanes, and creatine kinase) and all four markers of skeletal muscle health (HGS, gait speed, SMI, and phase angle) (Table 2). After adjustment for age, we found robust correlations of plasma zonulin with HGS and gait speed, while relatively weaker but statistically significant correlations of plasma zonulin with CRP, 8-isoprostanes, and phase angle. Conversely, plasma zonulin exhibited no significant correlations with creatine kinase and SMI in age-adjusted analysis (Table 2).
 |
Table 2 Regression Values and Correlation Coefficients of Unadjusted and Age-Adjusted Values of Plasma Zonulin with CRP, 8-Isoprostanes, Creatine Kinase, HGS, Gait Speed, SMI, and Phase Angle in Young, Middle-Aged, Older Adults, and Cumulative Study Population. |
Discussion
This research aimed to investigate the potential contributions of intestinal leaks to muscle detriment and physical decline across an extensive range of age ranges. We found an age-associated increase in plasma zonulin levels and a reduction in HGS and gait speed. Plasma zonulin showed negative correlations with HGS and gait speed from middle age onward. Aging was also associated with increased plasma CRP, 8-isoprostanes, and creatine kinase levels, which provide a mechanistic connection between increased intestinal permeability and muscle decline. After adjustment for age, we found robust negative correlations of zonulin with HGS and gait speed and positive correlations with CRP, 8-isoprostanes, and creatine kinase. Together, these findings show the potential contribution of intestinal leak to muscle weakness and reduced gait speed, which may partly be due to heightened systemic inflammation and oxidative stress.
To our knowledge, this is the first study investigating plasma zonulin levels across the lifespan from late adolescence. However, an age-associated disruption of the intestinal mucosal barrier has previously been reported.26 Specifically, the intestinal tissues exhibited higher inflammatory cytokines and molecular signs of mucosal disruption with advancing age.26 Interestingly, a higher expression of claudin proteins was also reported in older vs younger adults.26 Claudin is a critical regular of intestinal permeability, and its higher expression is reported in patients with leaky gut.27 We have previously reported a moderate coupling between plasma claudin and zonulin levels in patients with intestinal leak and repair.17 These findings support our data on an age-associated increase in intestinal permeability.
We report robust associations of plasma zonulin with HGS and gait speed in middle-aged and older adults. These findings are consistent with the onset of the sarcopenia process from the fourth decade of life onward.6 Specifically, an age-related gradual decline in HGS and gait speed is reported from the fourth decade of life.28,29 We also found a gradual increase in plasma zonulin levels in middle-aged to older adults. The negative correlation of plasma zonulin with HGS is consistent with the previously established gut-muscle axis.30 Moreover, we have reported similar inverse correlations between plasma zonulin and HGS in older adults.10,12 Here, we extend these findings to show similar correlations in the middle-aged population. Our data indicate that the intestinal leak may be a potential trigger of the sarcopenia process in addition to its well-established contribution to ongoing sarcopenia in advanced age. We did not find a significant correlation between plasma zonulin and HGS in younger adults. Thus, within the physiological limits of young age, the intestinal mucosa and muscle strength do not exhibit potential coupling. Conversely, we propose an age-associated coupling between intestinal leak and muscle weakness as the pathologies of aging set in.
Gait speed is a critical measure of physical capacity, as people with low gait speed exhibit a higher risk of a dependent lifestyle.31 We found that the correlation of gait speed with plasma zonulin was modest in middle-aged and robust in older adults. Conversely, younger adults exhibited no significant correlation between gait speed and plasma zonulin levels. Our findings in older adults are consistent with our previous reports from sarcopenic men with age-related diseases.10,11 Muscle weakness is a significant cause of low gait speed. Thus, the intestinal leak may negatively affect gait speed by reducing the strength of lower limb muscles. However, gait speed is also affected by poor neural control and joint diseases.31 Intestinal leaks are also implicated in patients with neurodegeneration and arthritis.1 Together, these reports support our finding of a negative correlation between gait speed and plasma zonulin levels.
We found a modest correlation between plasma zonulin and SMI in older adults. Similarly, plasma zonulin exhibited low diagnostic efficacy for SMI below the cutoff limit of 7 kg/m2. In most muscle-wasting conditions, the onset of muscle weakness precedes muscle atrophy.32 This is partly due to an intrinsic defect in the muscle excitation-contraction coupling mechanism without affecting muscle quantity. Thus, it is possible that increased intestinal permeability primarily affects muscle quality more than quantity. This possibility is consistent with our previous reports in patients with intestinal leaks.10,12 In addition to muscle weakness, poor neural control and joint diseases may contribute to reduced gait speed.31 Previous studies have reported the potential contribution of intestinal leaks to neural decline and arthritis,1 which agrees with our findings.
The higher CRP and 8-isoprostanes in middle-aged and older adults represent the age-related increase in systemic inflammation and oxidative stress. The significant correlations of plasma zonulin with CRP and 8-isoprostanes unravel the intestinal leak as a potential contributor to elevated inflammation and oxidative stress of aging. Increased intestinal permeability causes the leakage of bacterial lipopolysaccharides and other toxins in the blood, which induce systemic inflammation and oxidative stress.1 It is generally well recognized that inflammation and oxidative stress cause or contribute to age-related degeneration of multiple body organs, including skeletal muscle.33,34 Thus, we propose that the intestinal leak partially reduces HGS and gait speed by inducing systemic inflammation and oxidative stress.
This study has certain strengths. A large and representative sample size of each age group ensures the biological significance of our data. All participants had similar ethnicity, cultural, and social backgrounds, which reduces the lifestyle and dietary variations associated with intestinal permeability and physical health. The major limitation of the study is the inclusion of only the male population. We did not monitor the diets of individual participants, which may affect intestinal permeability. We did not measure the knee extensor strength, which may be more relevant to activities of daily living, such as walking, climbing stairs, or rising from the bed.
In conclusion, we report an age-associated increase in plasma zonulin levels from middle-aged to octogenarians. The association of plasma zonulin with reduced HGS and gait speed shows a potential contribution of increased intestinal permeability to muscle decline. Future studies should dissect individual bacteria and their products about aging and physical compromise.
Data Sharing Statement
The data is available from the corresponding author on request.
Ethical Standards
The study was conducted under the standards set by the National Bioethics Committee of Pakistan.
Acknowldegment
This work was supported by a Researchers Supporting Project (number: RSP2023R277) to Shaea Alkahtani from King Saud University, Riyadh, Saudi Arabia.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Fasano A. All disease begins in the (leaky) gut: role of zonulin-mediated gut permeability in the pathogenesis of some chronic inflammatory diseases. F1000Res. 2020;9.
2. Camilleri M. Leaky gut: mechanisms, measurement and clinical implications in humans. Gut. 2019;68(8):1516–1526. doi:10.1136/gutjnl-2019-318427
3. Camilleri M. What is the leaky gut? Clinical considerations in humans. Curr Opin Clin Nutr Metab Care. 2021;24(5):473–482. doi:10.1097/MCO.0000000000000778
4. Troisi J, Venutolo G, Terracciano C, et al. The therapeutic use of the zonulin inhibitor AT-1001 (Larazotide) for a variety of acute and chronic inflammatory diseases. Curr Med Chem. 2021;28(28):5788–5807. doi:10.2174/0929867328666210104110053
5. Parvatiyar MS, Qaisar R. Editorial: skeletal muscle in age-related diseases: from molecular pathogenesis to potential interventions. Front Physiol. 2022;13:1056479. doi:10.3389/fphys.2022.1056479
6. Walston JD. Sarcopenia in older adults. Curr Opin Rheumatol. 2012;24(6):623–627. doi:10.1097/BOR.0b013e328358d59b
7. Nishikawa H, Fukunishi S, Asai A, et al. Pathophysiology and mechanisms of primary sarcopenia (Review). Int J Mol Med. 2021;48(2). doi:10.3892/ijmm.2021.4989
8. Qaisar R. Cellular and molecular mechanisms of muscle regeneration. Khyber Med Univ J. 2021;13(3):173–178. doi:10.35845/kmuj.2021.20319
9. de Marco Castro E, Murphy CH, Roche HM. Targeting the gut microbiota to improve dietary protein efficacy to mitigate sarcopenia. Front Nutr. 2021;8:656730. doi:10.3389/fnut.2021.656730
10. Karim A, Muhammad T, Shahid Iqbal M, et al. A multistrain probiotic improves handgrip strength and functional capacity in patients with COPD: a randomized controlled trial. Arch Gerontol Geriatr. 2022;102:104721. doi:10.1016/j.archger.2022.104721
11. Ahmad F, Karim A, Khan J, et al. Plasma zonulin correlates with cardiac dysfunction and poor physical performance in patients with chronic heart failure. Life Sci. 2022;311(Pt A):121150. doi:10.1016/j.lfs.2022.121150
12. Karim A, Iqbal MS, Muhammad T, et al. Elevated plasma zonulin and CAF22 are correlated with sarcopenia and functional dependency at various stages of Alzheimer’s diseases. Neurosci Res. 2022;184:47–53. doi:10.1016/j.neures.2022.08.004
13. Qaisar R, Karim A, Elmoselhi AB. Muscle unloading: a comparison between spaceflight and ground-based models. Acta Physiol. 2020;228(3):e13431.
14. Gurley JM, Ilkayeva O, Jackson RM, et al. Enhanced GLUT4-dependent glucose transport relieves nutrient stress in obese mice through changes in lipid and amino acid metabolism. Diabetes. 2016;65(12):3585–3597. doi:10.2337/db16-0709
15. Qaisar R, Karim A, Iqbal MS, et al. Tracking the plasma C-terminal agrin fragment as a biomarker of neuromuscular decline in 18- to 87-year-old men. Mol Diagn Ther. 2024;28(5):611–620. doi:10.1007/s40291-024-00724-y
16. Qaisar R, Karim A, Muhammad T, et al. Degradation of neuromuscular junction contributes to muscle weakness but not physical compromise in chronic obstructive pulmonary disease patients taking lipids-lowering medications. Respir Med. 2023;215:107298. doi:10.1016/j.rmed.2023.107298
17. Karim A, Muhammad T, Shah I, Khan J, Qaisar R. A multistrain probiotic reduces sarcopenia by modulating Wnt signaling biomarkers in patients with chronic heart failure. J Cardiol. 2022;80:449–455.
18. Karim A, Iqbal MS, Muhammad T, et al. Evaluation of sarcopenia using biomarkers of the neuromuscular junction in Parkinson’s disease. J Mol Neurosci. 2022;72(4):820–829. doi:10.1007/s12031-022-01970-7
19. World Medical A. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194.
20. Karim A, Muhammad T, Iqbal MS, et al. Elevated plasma CAF22 are incompletely restored six months after COVID-19 infection in older men. Exp Gerontol. 2023;171:112034. doi:10.1016/j.exger.2022.112034
21. Qaisar R, Karim A, Muhammad T, et al. Circulating MicroRNAs as biomarkers of accelerated sarcopenia in chronic heart failure. Glob Heart. 2021;16(1):56. doi:10.5334/gh.943
22. Gupta A, Jayakumar MN, Saleh MA, et al. SARS-CoV-2 infection- induced growth factors play differential roles in COVID-19 pathogenesis. Life Sci. 2022;304:120703. doi:10.1016/j.lfs.2022.120703
23. Karim A, Muhammad T, Ustrana S, et al. Intestinal permeability marker zonulin as a predictor of sarcopenia in chronic obstructive pulmonary disease. Respir Med. 2021;189:106662. doi:10.1016/j.rmed.2021.106662
24. Karim A, Muhammad T, Shah I, et al. Relationship of haptoglobin phenotypes with sarcopaenia in patients with congestive heart failure. Heart Lung Circ. 2022;31(6):822–831. doi:10.1016/j.hlc.2022.01.003
25. Qaisar R, Karim A, Muhammad T, et al. Prediction of sarcopenia using a battery of circulating biomarkers. Sci Rep. 2021;11(1):8632. doi:10.1038/s41598-021-87974-6
26. Man AL, Bertelli E, Rentini S, et al. Age-associated modifications of intestinal permeability and innate immunity in human small intestine. Clin Sci. 2015;129(7):515–527. doi:10.1042/CS20150046
27. Luettig J, Rosenthal R, Barmeyer C, et al. Claudin-2 as a mediator of leaky gut barrier during intestinal inflammation. Tissue Barriers. 2015;3(1–2):e977176. doi:10.4161/21688370.2014.977176
28. Dodds RM, Syddall HE, Cooper R, et al. Grip strength across the life course: normative data from twelve British studies. PLoS One. 2014;9(12):e113637. doi:10.1371/journal.pone.0113637
29. Bohannon RW. Comfortable and maximum walking speed of adults aged 20-79 years: reference values and determinants. Age Ageing. 1997;26(1):15–19. doi:10.1093/ageing/26.1.15
30. Zhao J, Huang Y, Yu X. A narrative review of gut-muscle axis and sarcopenia: the potential role of gut microbiota. Int J Gen Med. 2021;14:1263–1273. doi:10.2147/IJGM.S301141
31. Mehmet H, Robinson SR, Yang AWH. Assessment of Gait Speed in Older Adults. J Geriatr Phys Ther. 2020;43(1):42–52. doi:10.1519/JPT.0000000000000224
32. Lynch GS. Update on emerging drugs for sarcopenia - age-related muscle wasting. Expert Opin Emerg Drugs. 2008;13(4):655–673. doi:10.1517/14728210802544476
33. Bhaskaran S, Pollock N, C. Macpherson P, et al. Neuron-specific deletion of CuZnSOD leads to an advanced sarcopenic phenotype in older mice. Aging Cell. 2020;19(10):e13225. doi:10.1111/acel.13225
34. Dalle S, Rossmeislova L, Koppo K. The role of inflammation in age-related sarcopenia. Front Physiol. 2017;8:1045. doi:10.3389/fphys.2017.01045
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Interface of a Leaky Gut with Reduced Sarcopenia-Related Quality of Life (SarQoL) in Patients with Chronic Obstructive Pulmonary Disease
Qaisar R, Karim A, Muhammad T, Ahmad F, Marinho DA, Arkadianos I, Alkahtani S
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2049-2059
Published Date: 24 June 2025