")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
The Paradox of Surplus and Shortage: A Policy Analysis of Nursing Labor Markets in Indonesia
Authors Efendi F , Aurizki GE , Auwalin I, Kurniati A , Astari LD, Puspitasari IT, Chong MC
Received 16 December 2021
Accepted for publication 22 February 2022
Published 29 March 2022 Volume 2022:15 Pages 627—639
DOI https://doi.org/10.2147/JMDH.S354400
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ferry Efendi,1,2 Gading Ekapuja Aurizki,1,2 Ilmiawan Auwalin,3 Anna Kurniati,4 Lita Dwi Astari,4 Ias Tarina Puspitasari,4 Mei Chan Chong5
1Faculty of Nursing, Universitas Airlangga, Surabaya, East Java, Indonesia; 2Community Health, Geriatric and Family Nursing Research Group, Universitas Airlangga, Surabaya, East Java, Indonesia; 3Faculty of Economics and Business, Universitas Airlangga, Surabaya, East Java, Indonesia; 4Center for Planning and Management of Human Resources for Health, BPPSDMK, Ministry of Health of the Republic of Indonesia, Jakarta, Indonesia; 5Department of Nursing Science, Faculty of Medicine, University Malaya, Kuala Lumpur, Malaysia
Correspondence: Ferry Efendi, Fakultas Keperawatan, Universitas Airlangga, Campus C Mulyorejo, Surabaya, East Java, 60115, Indonesia, Tel +62 813-3153-3805, Fax +62 31 5913257, Email [email protected]
Purpose: Resolving nursing resources constraints should rely on robust nursing labor market analysis; however, no current study analyzes the dynamics of nursing labor markets in Indonesia. This study aimed to investigate the production, inflow and outflow, maldistribution and inefficiencies, and private sector regulations of the nursing labor market in Indonesia.
Patients and Methods: This study used descriptive qualitative and document analysis approaches via focus group discussion (FGD) among various stakeholders in Indonesia. The FGD was conducted once attended by representatives from various sectors, including health, education, manpower, professional associations, and private. Policies on training, inflow and outflow, maldistribution and efficiencies, and private sector regulation were analyzed. Document analysis was used to triangulate the qualitative data.
Results: There is a structured policy regarding production, inflow and outflow, distribution, and involvement of the private sector. The number of nursing production shows an excess when entering the labor markets; however, the health-care providers reported a nursing workforce shortage. Policies on outflow encourage the deployment of Indonesian nurses overseas despite various challenges. Private sector involvement cannot be denied, especially in the placement of Indonesian nurses abroad. In addition, there is an absence of an integrated nursing labor market platform which may lead to inaccurate supply and demand.
Conclusion: Establishing an integrated and comprehensive platform of the nursing labor market in Indonesia is imperative. Addressing the surplus and shortage of nursing workforce requires reliable data to inform the policy. These analyses highlight the need to understand how the existing environment affects the market for Indonesian nurses nationally and globally.
Keywords: health worker, Indonesian nurses, nursing policy, nursing workforce, nurse migration, nursing education
Introduction
Nurses are the largest workforce group in the health-care sector, totaling 27.9 million personnel or around 59% of total health professions worldwide.1 Despite the enormous number within the health-care group, the shortage of nurses and midwives is estimated to be about 9 million in 2030.2 Many countries are struggling in terms of the availability, distribution, and performance of health workers, including nurses.3 Achievement of Sustainable Development Goals (SDGs) and universal health coverage (UHC) requires a sufficient number of competent nurses. According to the World Health Organization, an approximately 4.45 health workers including doctors, nurses and midwives are required to serve every 1000 population in order to achieve the SDGs.1 The importance of nurses in the global market landscape shows us that the world needs investment in the nursing area, particularly amid the COVID-19 pandemic.4 Resolving nursing resources constraints should rely on robust nursing labor market analysis, a deeper understanding of which would inform the intersectoral policy to operate in effective, efficient, and sustainable ways.5
Although globally there is a nursing workforce shortage, some Asian countries including China and the Philippines experience surpluses due to a high number of graduates from nursing schools.6 Indonesia reported to experience the similar situation.7 The most recent published data from the Ministry of Health (MoH) confirmed that Indonesia has an adequate supply of nurses and is likely to encounter a temporary excess.8 The national target of the nursing workforce density of 2 nurses per 1000 population by 2025 has been surpassed at 2.46 nurses per 1000 population in 2018.8 However, the MoH acknowledged that the sufficiency of nursing workforce supply is still challenged by the imbalanced distribution across regions.9 It means that some health facilities in certain regions may experience shortages while other regions reported having surpluses. The MoH estimated that an additional 5000 nurses are required in 2019, while in 2020 approximately more than 4000 nurses are required to meet the minimum staffing standard in public health centers.9 The persistent shortages of nursing workforce in public health centers are attributable to the lack of hiring capacity by the local government. Health is a decentralized affair to the local government, yet the hiring capacity has been a great challenge for the local government due to the budget constraint and the dependency of civil servant quota from the national government.10 The Indonesian nursing labor market analysis reported that there was 219,757 net excess of nurses supply in 2018.11 This finding was based on the data retrieved from the Indonesian National Labor Forces Survey by calculating the gap between the total nursing labor forces and ideal demand based on the target ratio of 180 nurses per 100,000 population.11 However, due to various data related to nursing labor market analysis in Indonesia the situation may not be captured correctly.
Surplus of nursing workforce has been regarded as a justification to send nurses abroad.7 Indonesia has been actively engaged in deploying its nurses to work overseas since 1996, mainly to Asian (eg, Taiwan, Japan and Singapore) and Gulf countries (eg, Saudi Arabia, Kuwait and United Arab Emirates).11,12 The international deployment of Indonesian nurses is an interesting area to explore as it may be related to under utilization and high production level of nurses,10,13 or the absence of a robust nursing labor market.
As found in Indonesia’s case, formulating human resources for health (HRH) policies based on the number of health workers required to meet the population needs is actually common in many low- and middle-income countries.14 Although this needs-based approach can inform the demand of health workers, it is insufficient to capture the dynamics of the health labor market. As the result, the HRH policies often overemphasize the training of more health workers. Consequently, if the country does not have sufficient capacity to absorb the newly trained health workers into the labor market, it could end up with an oversupply situation and potentially increase unemployment, brain drain and the loss of competent HRH.15 Therefore, instead of relying on one simple parameter, ie, population needs, the HRH planning should consider the dynamics of the labor market analyzed by an evidence-based approach.16 Nevertheless, there was no current labor market analysis that comprehensively portrays the policy dimensions of the nursing workforce management in Indonesia.
There is a framework that summarizes policy groups that affect health labor market situation. The framework was initially developed to determine the supply of HRH,17 and later generally used to formulate policies concerning health workforce in the UHC era.15 This framework has been used in some high-level documents on HRH planning and the labor market.16,18 The health labor market framework incorporates dimensions related to the production of qualified health workers and the health labor market dynamics.15 In the Indonesian context, the existing evidence has yet to discuss this framework as the basis to explore the HRH policies, particularly in the development of the nursing labor market. Therefore, we are interested to see the interplays of various aspects in shaping the Indonesian nursing labor market and how the policies affect the current situation of the nursing workforce. This paper provides some insights on the interplays of various aspects in shaping the Indonesian nursing labor market and how the policies affect the current situation of the nursing workforce.
Materials and Methods
Design and Participants
This study was a descriptive qualitative study design by employing a nursing policy approach in examining the view of stakeholders within the indicators of the nursing labor market. The qualitative data were collected through focus group discussion (FGD) and in-depth interview involving the representatives from numerous ministries and agencies in Indonesia as the participants. The FGD and interviews were conducted in October 2020 at Jakarta which was jointly facilitated by the MoH. The stakeholders represented the health sector, education, manpower, professional association, and private sector, as depicted in Table 1. These stakeholders were selected purposively based on their involvement in the Indonesian nursing labor market. The investigators sent out a formal invitation to the stakeholder’s institutions to send their representatives to participate in the discussion. The FGD and interview were led by the principal investigator and first author, a PhD who was trained at the postgraduate level to undertake the qualitative study. Furthermore, document analysis was used to triangulate the qualitative data.19,20 The documents collected were grey literature related to the topic, including public policy documents, legal instruments, official reports, and databases. All documents analysed were available publicly or did not require any permission to use it.
 |
Table 1 Participants at Focus Group discussion |
Instrument and Analysis
The instrument for the FGD and in-depth interview was developed and modified from the National Health Workforce Accounts (NHWA) modules.21 The semi-structured questions focused on 12 topics, namely nurses supply; education and training; education and training regulation and accreditation; education finances; nursing labor market flows; employment characteristics and working conditions; income, remuneration, and nurse career development; nursing workforce composition in hospitals; government regulation regarding nurses; health workforce information system; nurse mobility abroad; and deployment and protection of Indonesian nurses. The participants’ answers were recorded using a voice recorder device and transcribed by the research team.
The data analysis was conducted deductively driven by the Sousa et al’s framework, consisting of four groups of policies and selected primary indicators reflecting the labor market dynamics: 1) policies on production; 2) policies to address inflow and outflow; 3) policies to address maldistribution and inefficiencies; and 4) policies to regulate the private sectors.14,15 The investigators repeatedly read the participants’ answers and grouped them following the framework. The investigators validated their answers by searching relevant documents, which then were incorporated into the discussion.
Ethics Approval and Informed Consent
This study obtained ethical clearance approval from the Health Research Ethics Committee, Faculty of Nursing, Universitas Airlangga (1968-KEPK). The participants were invited and agreed to join the FGDs. They were informed that they can withdraw at any time without providing any particular reason. Each participant gave their written consent before the data collection started.
Results
As shown in Table 2, the nursing workforce situation in Indonesia is indicated from some components, namely the current stock and density of nurses; skill mix across selected health professionals; nurses’ characteristic distributions; employment at primary health centers and hospitals; migration overseas; needs-based estimation; and remuneration. The density represents the number of available health workers per 1000 people. The number of fresh graduates in 2018 was 138,206 nurses from various higher education levels. The nurse stock was 639,356 certified nurses (registered and associate nurses) or 2.46 nurses per 1000 people. In total, Indonesia has 1,072,598 health workers employed in various health facilities, or 4.25 active personnel per 1000 people. This figure includes health professionals and management and support staff. There were 1.21 nurses and 0.81 midwives per 1000 people (n = 320,772 and 214,687, respectively). The proportion of nurses and midwives among all health workers was 49.9%, outnumbering other non-physician health workers proportion (42.9%). Meanwhile, the density of physicians (general practitioners and specialists) was 0.43 per 1000 people, which covered 7.2% of total health workers.
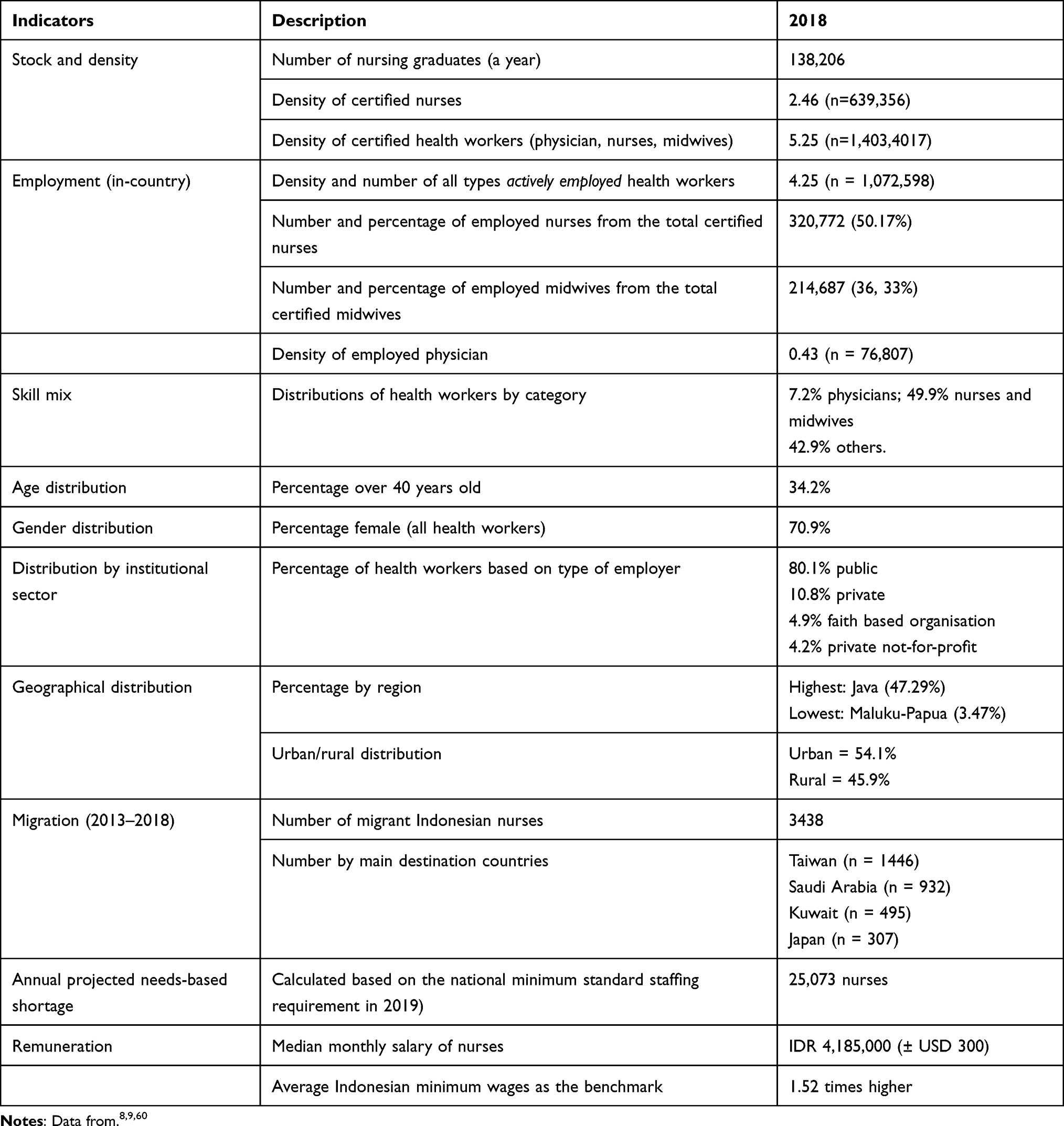 |
Table 2 Selected Health Workforce Indicators Related to the Health Labor Market Based on MoH Indonesia’s Reports |
Results of the focus group discussion, guided by the framework of labor market analysis, are summarized in Table 3. In terms of production, there were discussions concerning the nursing education and enrollment mechanism and the quality assurance system. To address inflows and outflows of nursing workforce, stakeholders pointed out some policies related to regulations on certification of nursing competency, international migration and the information system of human resources for health as an instrument to inform policy makers regarding the active stock of health workers.
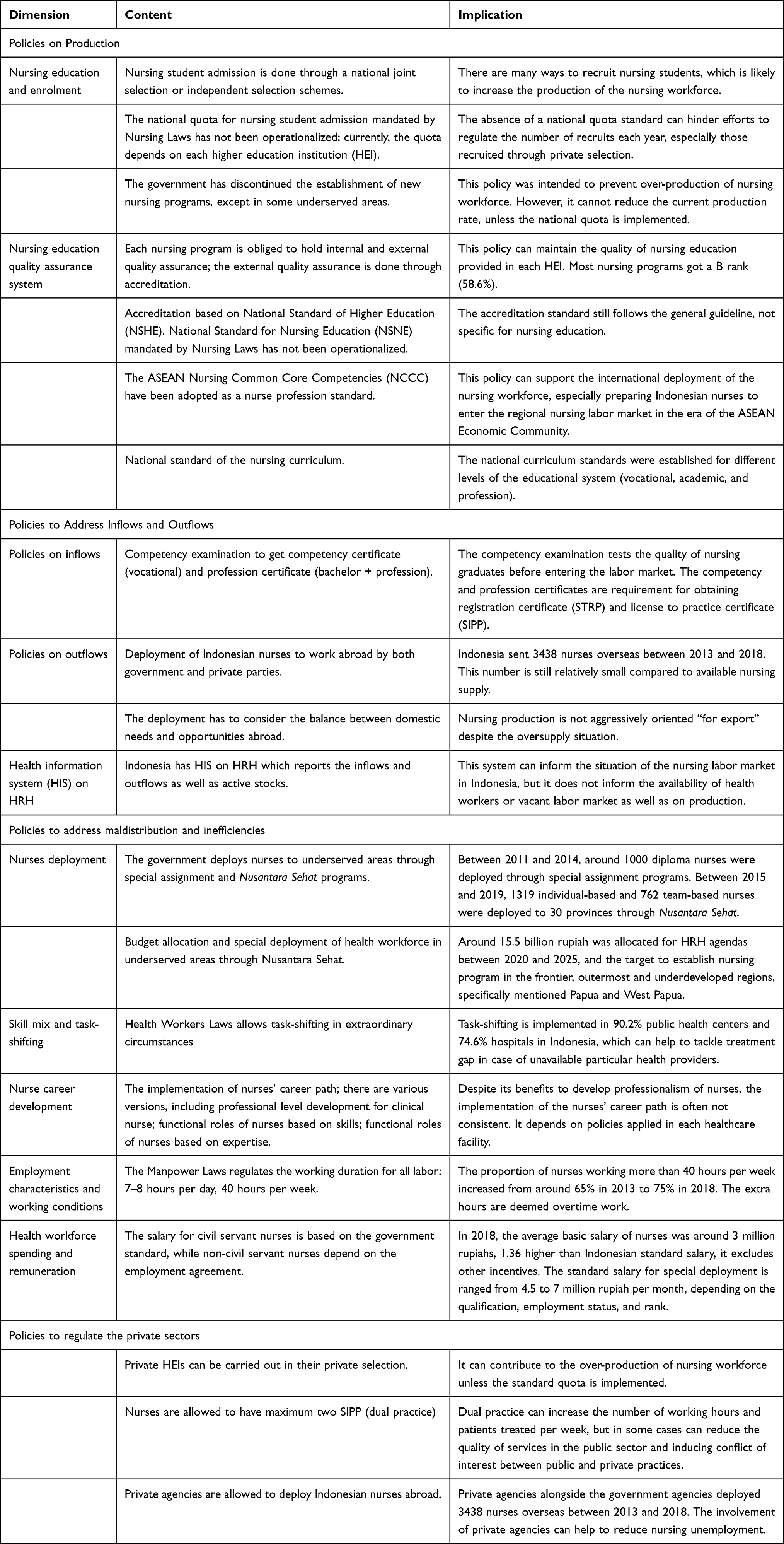 |
Table 3 Summary of the Focus Group discussion on Policies Related to the Labor Market Analysis |
Discussion
In general, all sets of policies described in Sousa et al’s framework are covered in the current policies implemented in Indonesia,15 especially in the laws level. However, some aspects that have been mandated by the laws have yet to be operationalized through implementation guidelines. For instance, there is no specific policy to prevent nursing graduates to opt-out of the nursing occupation and attract them back into the health sector. In the United States and Australia, there are various reasons why nurses give up nursing jobs, among them personal reasons, workplace conditions, retirement, and low interest in a nursing career.22,23 In the Indonesian context, it could be induced by nurses’ oversupply, which limits the availability of decent nursing jobs and encourages nursing graduates to take any job opportunities available. Furthermore, the absence of policies regulating this issue may be related to the consideration that nurses taking a job outside nursing is a better option than unemployment. The following sections will describe the policies that shape the nursing labor market in Indonesia.
Policies on Production
Nursing Education and the Enrolment
The production of a health workforce is determined by policies on the education sector. In Indonesia, these policies are mainly derived from the Laws No. 12th of 2012 on Higher Education.24 This law recognizes six types of higher education institutions (HEIs): university, institute, sekolah tinggi (college), polytechnic, academy and community academy; each can be public or private. The HEIs can provide three types of education: vocational, academic and professional. The establishment, change and discontinuation of public and private colleges, including the study programs, are operationalized through Minister of Education and Culture (MoEC) Regulation No. 7th of 2020.25 The nursing education in particular is specifically regulated through Laws No. 38th of 2014 on Nursing.26 The types of nursing education and degree still refer to the Higher Education Laws, with an exception that the vocational nursing program must be at least Diploma 3 degree. Accordingly, all types of HEIs except community academy (only for Diploma 1 and 2) can provide nursing education. The student admission quota on each program is determined by the HEIs after considering the infrastructures, staff, services and other resources. Meanwhile, the Nursing Laws has mandated that the enrolment of nursing students must follow the national admission quota regulated by the education minister in coordination with the Minister of Health (MoH), which has yet to be enacted.
Considering nurses’ overproduction, the HRH Development Plan 2011–2025 has recommended to, first, discontinue the substandard nursing programs; second, reduce the student admission quota; and, third, withhold permission to establish a new program.27 Among these recommendations, the last one has been implemented since 2011. The MoEC’s Directorate General of Higher Education (DGHE) issued Circular Letter No. 1643/E/T/2011 on the Moratorium of Health Study Programs,28 which informs the proposals for the establishment of new nursing and midwifery study programs in diploma and bachelor levels will not be approved. The moratorium may be exempted for particularly underserved areas determined by DGHE discretion based on the country’s needs. In 2020, the DGHE confirmed that the moratorium is still valid, except for the establishment of bachelor and professional nursing programs in HEI that has a Diploma 3 nursing program with accreditation status at least “B” or “Very Good”.29 The latest Indonesia country profile in 2019 showed that the average number of nursing graduates each year was 203, 221 for nursing professionals and 173,432 for nursing associate professionals during 2015–2018.8 Structured and proportional policies on the production of nursing education should be harmonized with the labour market situation.
Nursing Education Quality Assurance System
The Higher Education Laws regulates a system that can maintain the quality of HEI graduates. This system is based on the standard of higher education set at the national and HEI levels. The HEI-level standard is determined and evaluated internally by the HEI, while the national standard is used as the basis for determining the criteria for external quality assurance system through accreditation.24 The current regulation concerning National Standard of Higher Education (NSHE) is the MoEC Regulation No. 3/2020, which operationalizes the standard of higher education, including competency, learning contents and processes, teachers and staff, evaluation, infrastructures and financing standards.30 Additionally, the Nursing Laws mandates the development of National Standard for Nursing Education (NSNE), which must refer to the NSHE and is enacted by the education minister.26 However, there is no regulation governing the NSNE at this moment. As a comparison, the National Standard of Medical Education has been enacted in 2018.31
The NSHE set the standard of curriculum which must be followed by every study program. The curriculum can also refer to the framework set by each association of the study program. For instance, the curriculum for nursing bachelor and professional programs currently refers to the Core Curriculum of Indonesian Nurse Education 2015 developed by the Association of Indonesian Nursing Education Center (AINEC). This curriculum is reviewed every five years. Meanwhile, the Diploma 3 curriculum is developed by the Association of Vocational Nursing Education Institution of Indonesia (AIPViKI). The representatives from the AINEC and AIPViKI revealed the curriculums adopted the ASEAN Nursing Common Core Competencies (NCCC), which consist of ethics and legal practice, professional nursing practice, leadership and management, education and research, and professional and quality development. The details of the NCCC are operationalized through MoH Decree on Nurse Profession Standard.32 This policy was influenced by international context, where the global nurse shortage situation enforces many countries, including Indonesia, to actively participate in deploying nurses overseas.6,13 Differences in nursing licensure examination made the realization of this programme hindered.33
According to the Higher Education Laws, the NSHE becomes the reference for the accreditation process, which is currently operationalized through an MoEC Regulation.34 The HEI and study program accreditations are, respectively, undertaken by the National Accreditation Board for Higher Education (BAN-PT) and an independent accreditation board, which is specific to the program branch of science. For health study programs, including nursing, the accreditation is specifically undertaken by the Independent Accreditation Boards for Indonesian Health Higher Education (LAM-PTKes).35 The accreditation status is valid for five years, after which the program must renew it through reaccreditation. In 2019, out of 1224 nursing programs from all degrees, 58.6% had “B” accreditation status (n = 705). Only 6% got the highest “A” (n = 74). Meanwhile, 21.2% (n = 260) were not yet accredited.36 The quality assurance system of nursing education in place and should be accompanied by supportive policies to ensure sustained quality improvement.
Policies to Address Inflows and Outflows
Policies on Inflows
Despite the numerous types of programs available, based on the Nursing Laws, there are only two pathways to get registered as a nurse in Indonesia: the vocational and professional pathways. After completing the nursing degree, the vocational or professional program graduate has to take a competency examination to obtain a competency or profession certificate, respectively.26 This certificate is a requirement for getting the nurse registration certificate (STRP) from the Nursing Council, which is part of the Indonesian Health Profession Council (KTKI).26 This registration requirement is also mandated by the Health Workers Laws.37
The possession of STRP is the parameter by which the nurse is officially recognized and pooled as a qualified health worker and eligible to get a nurse license to practice certificate (SIPP) from the local authority. The nurses are allowed to have a maximum of two SIPPs, which means they can undertake dual practice. This dual practice can increase the nurses’ working hours and the number of patients treated. However, in many cases, it can reduce the quality of public health services and induce conflict of interest. Many health workers working in public service refer their patients to be treated in private practice.38
The implementation of nursing registration and practice is operationalized through MoH Regulation on the Implementation of Nursing Laws39 and on Health Workers Registration.40 The foreign nurses and foreign-educated Indonesian nurses can obtain the STRP and SIPP after passing the competency evaluation process. The empowerment of foreign and foreign-education nurses is regulated through the Government Regulation on Health Workers Management.41 Furthermore, Laws No. 44th of 2009 on Hospitals obligates every health worker working in hospitals to have registration and license to practice certificates.42
According to AINEC representative, the nurse graduates cannot directly take a nursing job because they have to take the competency examination first, which is normally held at least three months after the graduation. The examination process can hinder the graduates to enter the labor market considering its fail rate is fairly high. Between 2015 and 2020, 44.6% of professional graduates and 30.2% of diploma graduates did not pass the nursing competency examination.43 The competency examination is operationalized through an MoEC Regulation concerning the Procedures of Competency Examination for Health Students.44 Policies on inflows should consider the stock of nursing workforce from upstream to downstream. The flows of nursing human resources affect the current and future workforce over the country and should be seen as critical point.
Policies on Outflows
In 2014, the Health Workers Laws set a general rule that the utilization of health workers abroad can be done by considering the balance between the domestic needs and the opportunities abroad. This policy was initially operationalized through the MoH Regulation focusing on Health Workers Empowerment Overseas.45 It was further regulated by a higher hierarchical policy enacted in 2019, ie, Government Regulation on Health Workers Management.41 The latter regulation governs many aspects of health workers’ inflows and outflows, including the procedures of deploying health workers overseas. Despite the oversupply situation, Indonesia has not aggressively changed its nursing education and management orientation “for export”, such as the Philippines,46 especially considering the country has a so-called “temporary surplus”, in which it is expected that, at some point, the government has capacity to absorb all nursing graduates into the labor market.10,11
The HRH Development Plan 2011–2015 reveals that Indonesia has ratified the WHO Global Code of Practice, which discourages member states from actively recruiting health workers from countries with critical shortages of health workers.47 In 2006, Indonesia was included in the list of 57 countries facing critical shortages of health workers.48 This inclusion has become a barrier for the international deployment given the list is often used as a reference for decision-making concerning health workforce in recent years though it was reported nearly 15 years ago.49,50 Despite being included on the list, Indonesia has sent nursing workforce to some countries. Between 2013 and 2018, 3438 Indonesian nurses were deployed overseas, though the quantity was drastically reduced since 2015. Considering the significant number in nurses production, the policies of outflow should align with the supply and demand side.
Policies to Address Maldistribution and Inefficiencies
Nurses Deployment
The deployment of health workers is regulated through the Health Workers Laws, in which the central and local government can determine the placement for health workers through three schemes: (1) appointment as civil servants; (2) appointment as government officer with employment agreement; and (3) special assignments. The special assignment of the health workers is operationalized through MoH Regulation No. 9th of 2013, which is aimed to increase access and service quality on the frontier, outermost, and underdeveloped regions.51 Before the Health Workers Laws was enacted, there were special assignments for Diploma 3 nurses, and around 1000 individuals deployed to these underserved regions from 2011 to 2014. In 2015, the deployment of Diploma 3 nurses was discontinued, and changed into Nusantara Sehat program (literally Healthy Archipelago), regulated through MoH Regulation No. 23/2015 on Special Assignment of Team-Based Health Workers to Support Nusantara Sehat Program.52 Between 2015 and 2019, the government deployed 1319 individual-based and 762 team-based nurses in 30 provinces across Indonesia.
The individual and team-based special assignments are featured in the National Medium-term Development Plan (RPJMN) 2020–2025 as main strategies to address unequal distribution of HRH. In addition, Papua and West Papua are specifically mentioned as the priority destinations for the special assignments. The total state budget allocated for HRH agendas in 2020–2025 is 15,523.3 billion rupiahs. The RJPMN 2015–2019 also mandated the establishment of nursing academies and health polytechnics in the frontier, outermost, and underdeveloped regions,53 while the RJPMN 2020–2025 planned to provide scholarships and continuing education for health workers from these underserved areas.54 These approaches correspond with the authors’ previous study, which found students from underserved areas were more likely intended to work in these areas than students from outside these areas.55 A good management and a conducive working environment are two factors why Indonesian health students are willing to work in underserved areas.56 The approach is not to push the students to go out and find nursing education elsewhere, but to provide affordable and accessible nursing education in their areas. It is more sustainable than the current Nusantara Sehat program, which is intended as temporary solution due to its short-term deployment. The deployment of nurses has been done through several initiative approach focusing on rural and remote areas. Policies on maldistribution problems especially in urban areas need to be done to ensure fair and equity access to the population.
Skill Mix and Task-Shifting
Skill mix and task-shifting are among strategies used to address maldistribution of health workers in Indonesia. Based on the Workforce Research in the Health Sector 2017 (RISNAKES), 8752 public health centers (90.2%) and 1732 hospitals surveyed (74.6%) had health workers undertaking tasks beyond their educational background or competency.57,58 The Health Workers Laws allows health workers to perform interventions beyond their authority in extraordinary circumstances, where the particular service requiring particular health providers is not available in a particular place and at a particular time. Moreover, the Nursing Laws authorizes nurses to undertake medical interventions in the absence of medical workers in a particular area. This authority can be fully delegated or mandated with supervision.
Nurse Career Development
According to the MoH Regulation No. 40/2017, there are four types of clinical levels for nurses; each has five sub-levels obtained through credentialing.52 Furthermore, the Minister of Administrative and Bureaucratic Reform Regulation No. 35th of 2019 regulates there are three categories of nurse’s function based on skill and four categories based on expertise.52 These regulations are actually aimed to develop the nurses’ professionalism and quality improvement. However, according to the Indonesian National Nurses Association (INNA) representative, the implementation of these career levels and functional roles is often inconsistent. There is no obligation for the hospitals to enforce it into practice. Meanwhile, according to an officer from the Center for HRH Quality Improvement, CPMHRH, the clinical levels of nurses and the functional roles are not compatible to each other, so the credentialing process should be through competency examination. Guidance on the nurse levels and functional is still being developed.
Policies to Regulate the Private Sectors
Most of the regulations mentioned above have actually regulated both public and private sectors. For instance, the Higher Education Laws also addresses private HEIs, though there are different regulations in some aspects, including admission scheme and financing. According to the Health Laws and Health Workers Laws, the health workers can work at health-care facilities owned by the governments or private parties, all with similar responsibilities. Moreover, the Government Regulation No. 67th of 2019 allows private agencies or individuals to become the executors of the health workers’ placement abroad.41 The Manpower Laws also has regulations that govern all employers regardless of public or private ownerships. Also, the HRH quality improvement and service delivery aspects have been regulated in these policies. Moreover, the RJPMN 2020–2015 emphasized that private sectors are actively involved in developing a public health-care workforce in Indonesia through public–private partnerships. The partnership includes the deployment of private health workers to the regions with staffing shortage and the provision of private in-service training for the health workers, among others.59
Limitation
This article only discussed the current policies implemented and should be interpreted inside of this context.
Conclusion
Nursing labor market analysis in Indonesia requires robust policies in harmonizing the supply and demand of nursing workforce data from various stakeholders. Achieving a sustainable nursing workforce would rely on reliable and integrated data across sectors. In addition, the policymakers should address the current surplus and shape policy to deploy Indonesian nurses in the national and global market. Government policy shifts are needed to respond to the current challenges nursing workforce data especially at production and employment stage.
Abbreviations
AINEC, Association of Indonesian Nursing Education Center; AIPViKI, Association of Vocational Nursing Education Institution of Indonesia; ASEAN, Association of Southeast Asian Nations; BAN-PT, National Accreditation Board for Higher Education; DGHE, Directorate General of Higher Education; INNA, Indonesian National Nurses Association; HEI, higher education institution; HRH, human resources for health; KTKI, Konsil Tenaga Kesehatan Indonesia (Indonesian Health Profession Council); LAM-PTKes, Independent Accreditation Boards for Indonesian Health Higher Education; MoEC, Minister of Education and Culture; MoH, Ministry of Health; MRTHE, Minister of Research, Technology, and Higher Education; NCCC, nursing common core competencies; NSHE, national standard of higher education; NSNE, national standard for nursing education; RPJMN, National Medium-term Development Plan; STRP, surat tanda registrasi perawat (nurse registration certificate); SIPP, surat izin praktik perawat (nurse license to practice certificate); UHC, universal health coverage.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Kementerian Riset, Teknologi, dan Pendidikan Tinggi Republik Indonesia (Direktorat Riset dan Pengabdian Masyarakat, Deputi Bidang Penguatan Riset dan Pengembangan Kementerian Riset dan Teknologi/Badan Riset dan Inovasi Nasional) through “Penelitian Dasar Unggulan Perguruan Tinggi” (PDUPT) grant number 896/UN3.14/PT/2020. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. State of the World’s Nursing 2020: Investing in Education, Jobs and Leadership. WHO; 2020.
2. WHO. Nursing and midwifery; 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/nursing-and-midwifery.
3. McPake B, Maeda A, Araújo EC, Lemiere C, El Maghraby A, Cometto G. Why do health labour market forces matter? Bull World Health Organ. 2013;91(11):841–846. doi:10.2471/BLT.13.118794
4. WHO. WHO and partners call for urgent investment in nurses. World Health Organization; 2020. Available from: https://www.who.int/news/item/07-04-2020-who-and-partners-call-for-urgent-investment-in-nurses/. Accessed on January 27, 2021
5. WHO. Health labour markets; 2021. Available from: https://www.who.int/hrh/labour-market/en/.
6. Matsuno A. Nurse Migration: The Asian Perspective. ILO/EU Asian Program Gov Labour Migr; 2009.
7. Kurniati A, Astari LD, Efendi F, et al. Analisis Kebijakan Pemenuhan Pasar Kerja Tenaga Kesehatan Di Tingkat Global (The Policy Analysis of the Labor Markets Fulfillment for Global Health Workers). Badan Pengembangan dan Pemberdayaan SDMK Kemenkes RI; 2020.
8. Ministry of Health. Human Resources for Health Country Profiles: Indonesia. Kemenkes; 2019. http://perpustakaan.bppsdmk.kemkes.go.id//index.php?p=show_detail&id=6544
9. CPMHRH-MOH. Rencana Kebutuhan SDM Kesehatan nasional Tahun 2020 (National Health Workforce Requirement Plan 2020). 2019. https://www.academia.edu/41101831/HUMAN_RESOURCES_FOR_HEALTH_COUNTRY_PROFILE_OF_INDONESIA
10. Efendi F, Chen C-M, Kurniati A, Nursalam N, Yusuf A. The situational analysis of nursing education and workforce in Indonesia. Malaysian J Nurs. 2018;9(4):21–29.
11. Ministry of Manpower. Analisis Pasar Kerja: Ketersediaan Dan Kebutuhan Tenaga Kerja Perawat (Labor Markets Analysis: Supply and Demand of Nursing Workforce). Kementerian Ketenagakerjaan Republik Indonesia; 2019.
12. Connell J. Migration of Health Workers in the Asia Pacific Region. University of New South Wales; 2010.
13. Raharto A, Noveria M. Nurse migration and career development: the Indonesian case. In: Tsujita Y, Komazawa O, editors. Human Resources for the Health and Long-Term Care of Older Persons in Asia. ERIA; 2020:63–102.
14. Sousa A, Scheffler RM, Koyi G, et al. Health labour market policies in support of universal health coverage: a comprehensive analysis in four African countries. Hum Resour Health. 2014;12(1):55. doi:10.1186/1478-4491-12-55
15. Sousa A, Scheffler RM, Nyoni J, Boerma T. A comprehensive health labour market framework for universal health coverage. Bull World Health Organ. 2013;91(11):892–894. doi:10.2471/BLT.13.118927
16. WHO. Force 2030: Towards a Global Strategy on Human Resources for Health. Synth Pap Themat Work Groups; 2015:1–40.
17. Vujicic M, Zurn P. The dynamics of the health labour market. Int J Health Plann Manage. 2006;21(2):101–115. doi:10.1002/hpm.834
18. WHO. Global Strategy on Human Resources for Health: Workforce 2030. WHO; 2016.
19. Frey BB. Document analysis. In: The SAGE Encyclopedia of Educational Research, Measurement, and Evaluation. SAGE Publications, Inc.; 2018. doi10.4135/9781506326139.n209
20. Bowen GA. Document analysis as a qualitative research method. Qual Res J. 2009;9(2):27–40. doi:10.3316/QRJ0902027
21. WHO. Framing the Health Workforce Agenda for the Sustainable Development Goals. WHO; 2017.
22. Black L, Spetz J, Harrington C. Nurses working outside of nursing: societal trend or workplace crisis? Policy Polit Nurs Pract. 2008;9(3):143–157. doi:10.1177/1527154408319288
23. Duffield C, Pallas LO, Aitken LM. Nurses who work outside nursing. J Adv Nurs. 2004;47(6):664–671. doi:10.1111/j.1365-2648.2004.03155.x
24. Republic of Indonesia. Laws No. 12th of 2012 on Higher Education; 2012.
25. Ministry of Education and Culture of the Republic of Indonesia. Minister of Education and Culture Regulation No. 7th of 2020 on the establishment, amendment, dissolution of public higher education institutions, and establishment, amendment, revocation of private higher education institutions; 2020.
26. Republic of Indonesia. Laws No. 38th of 2014 on nursing; 2014.
27. Ministry of Health. Rencana Pengembangan Tenaga Kesehatan Tahun 2011–2025: Berdasarkan Kemenkokesra Nomor 54 Tahun 2013 (Health Workers Development Plan of 2011-2015: Based on the Coordinating Minister of Public Welfare Regulation Number 54 of 2013). Kementerian Kesehatan Republik Indonesia; 2014.
28. Ministry of Education and Culture of the Republic of Indonesia. The Directorate General of Higher Education’s Circular Letter No. 1643/E/T/2011 on the moratorium of health study programs; 2011.
29. Ministry of Education and Culture of the Republic of Indonesia. The Directorate General of Higher Education’s letter No. 637/E.E3/OT/2020 on proposal for the establishment and change of private higher education institutions and the opening of study programs in 2020.; 2020.
30. Ministry of Education and Culture of the Republic of Indonesia. Minister of Education and Culture Regulation No. 3rd of 2020 on national standard of higher education; 2020.
31. Ministry of Research Technology and Higher Education of the Republic of Indonesia. Minister of Research, Technology, and Higher Education Regulation No. 18th of 2018 on national standard of medical education; 2018.
32. Ministry of Health of the Republic of Indonesia. Minister of Health Decree No. HK.01.07/MENKES/425/2020 on nurse profession standard.; 2020.
33. Efendi F, Nursalam N, Kurniati A, Gunawan J. Nursing qualification and workforce for the Association of Southeast Asian Nations Economic Community. Nurs Forum. 2018;53(2):197–203. doi:10.1111/nuf.12243
34. Ministry of Education and Culture of the Republic of Indonesia. Minister of Education and Culture Regulation No. 5th of 2020 on the accrediations of study programs and higher education institutions; 2020.
35. Ministry of Education and Culture of the Republic of Indonesia. Minister of Education and Culture Decree No. 291/P/2014 on recognition of the establishment of an independent accreditation agency for health higher education.; 2014.
36. Ministry of Education and Culture. Pangkalan Data Pendidikan Tinggi (PD DIKTI) (Higher Education Database); 2020.
37. Republic of Indonesia. Laws No. 36th of 2014 on health workers; 2014.
38. Gonzalez P, Montes‐Rojas G, Pal S. Dual practice of health workers: theory and evidence from Indonesia. SSRN Electron J. 2019. doi:10.2139/ssrn.3306812
39. Ministry of Health of the Republic of Indonesia. Minister of Health Regulation No. 26th of 2019 on the implementation of nursing laws; 2019.
40. Ministry of Health of the Republic of Indonesia. Minister of Health Regulation No. 83th of 2019 on health workers registration; 2019.
41. President of the Republic of Indonesia. Government Regulation No. 67th of 2019 on health workers management; 2019.
42. Republic of Indonesia. Laws No. 44th of 2009 on hospitals; 2009.
43. Ministry of Education and Culture. Data statistik (Statistical Data). 2022. Available from: http://ukners.kemdikbud.go.id/pages/statistik_lulus/.
44. Ministry of Education and Culture of the Republic of Indonesia. Minister of Education and Culture Regulation No. 2 of 2020 on the procedures of competency examination for health students; 2020.
45. Ministry of Health of the Republic of Indonesia. Minister of Health Regulation No. 37th of 2015 on health workers empowerment overseas; 2015.
46. Brush BL, Sochalski J. International nurse migration: lessons from the Philippines. Policy Polit Nurs Pract. 2007;8(1):37–46. doi:10.1177/1527154407301393
47. WHO. The WHO global code of practice on the international recruitment of health personnel - sixty-third world health assembly - WHA63.16. 2010:12.
48. WHO. Working Together for Health: The World Health Report 2006. World Health Organization; 2006.
49. Cometto G, de Courcelles S, Afzal M, et al. Analysis of the commitments made by national governments of 57 countries at the Third Global Forum on human resources for health. 2015.
50. Global Health Workforce Alliance. Global health workforce alliance annual report 2014. 2015:1–22.
51. Ministry of Health of the Republic of Indonesia. Minister of Health Regulation No. 9th of 2013 on special assignments for health workers; 2013.
52. Ministry of Health of the Republic of Indonesia. Minister of Health Regulation No. 23th of 2015 on special assignment of team-based health workers to support Nusantara Sehat Program; 2015.
53. Republik Indonesia. Rencana Pembangunan Jangka Menengah Nasional (RPJMN) 2015–2019: Buku III Agenda Pembangunan Wilayah (National Middle-Term Development Plan of 2015-2019: Book 3 Regional Development Agendas); 2015.
54. Republik Indonesia. Rencana Pembangunan Jangka Menengah Nasional 2020–2025: Narasi (National Middle-Term Development Plan of 2020-2025: Narration); 2020.
55. Firdaus A, Efendi F, Hadisuyatmana S, Aurizki GE, Abdullah KL. Factors influencing the intention of Indonesian nursing students to work in rural areas. Fam Med Community Health. 2019;7(3):e000144. doi:10.1136/fmch-2019-000144
56. Efendi F, Chen C, Nursalam N, Andriyani NW, Kurniati A, Nancarrow SA. How to attract health students to remote areas in Indonesia: a discrete choice experiment. Int J Health Plann Manage. 2016;31(4):430–445. doi:10.1002/hpm.2289
57. Ministry of Health. Buku 1 Laporan Riset Ketenagaan Di Bidang Kesehatan (RISNAKES) 2017: Puskesmas (Book 1 Report for Basic Health Workforce Research 2017. Public Health Centers). Badan Penelitian dan Pengembangan Kesehatan, Kementerian Kesehatan RI; 2018.
58. Ministry of Health. Buku 2 Laporan Riset Ketenagaan Di Bidang Kesehatan (RISNAKES) 2017: Rumah Sakit (Book 2 Report for Basic Health Workforce Research 2017). Badan Penelitian dan Pengembangan Kesehatan, Kementerian Kesehatan RI; 2018.
59. Health Policy Plus. Improving and supplementing the public healthcare workforce with public-private partnerships in Indonesia. HP+ Policy Br. 2020.
60. Ministry of Health. Data Dan Informasi Profil Kesehatan Indonesia Tahun 2019 (Data and Information of 2019 Indonesia Health Profile). Kementerian Kesehatan Republik Indonesia; 2019. https://pusdatin.kemkes.go.id/resources/download/pusdatin/profil-kesehatan-indonesia/Profil-Kesehatan-indonesia-2019.pdf
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.