")
Back to Journals » International Journal of Women's Health » Volume 15
The Outcome of Sacrocolpopexy/Sacrohysteropexy for Patients with Pelvic Organ Prolapse and Predictors of Anatomical Failure
Authors Alsahabi JA , Alsary S, Abolfotouh MA
Received 22 March 2023
Accepted for publication 11 July 2023
Published 18 July 2023 Volume 2023:15 Pages 1093—1105
DOI https://doi.org/10.2147/IJWH.S413729
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Jawaher A Alsahabi,1,2 Saeed Alsary,1,2 Mostafa A Abolfotouh2
1Department Urogynecology & Reconstructive Female Pelvic Surgery, King Abdul-Aziz Medical City, King Saud Ben Abdu Aziz University for Health Sciences (KSAU-HS), Ministry of National Guard-Health Affairs, Riyadh, 22490, Saudi Arabia; 2King Abdullah International Medical Research Center (KAIMRC), King Saud Ben Abdul Aziz University for Health Sciences (KSAU-HS), Ministry of National Guard-Health Affairs, Riyadh, 11481, Saudi Arabia
Correspondence: Mostafa A Abolfotouh, King Abdullah International Medical Research Center/ King Saud bin Abdulaziz University for Health Sciences, Riyadh/Ministry of National Guard Health Affairs, POB 22490, Riyadh, 11426, Saudi Arabia, Email [email protected]
Background: Pelvic organ prolapse (POP) is a medical condition that profoundly impacts women’s quality of life. Unfortunately, the literature lacks long–term predictors and risk factors for its recurrence. This study aims to assess the efficacy and safety of Sacrocolpopexy/Sacrohysteropexy and to identify the predictors of recurrence in a Saudi setting.
Methods: In a retrospective cohort study, all patients who underwent Sacrocolpopexy (n=144) and Sacrohysteropexy (n=56) between 2009– 2021 were followed up. Electronic medical records were examined to collect data on the following: Patient characteristics [age, parity, BMI, and past medical and surgical history], prolapse-related characteristics/symptoms, Surgery-related characteristics [type and approach of surgery, mesh type, and concomitant surgery], and Outcome characteristics. Postoperative anatomical success and failure rates were determined according to the Baden-Walker classification. Logistic regression analysis was applied to identify the predictors of overall anatomical failure of Sacrocolpopexy. Significance was considered at p< 0.05.
Results: Success rates of 96.8%, 99.4%, and 85.2% were detected in the anterior, apical, and posterior vaginal prolapse, respectively, with an overall success rate of 83.1%. The overall failure rate was 15.9%, with an incidence density of 5.98 per 100 women-years. The onset of failure in 27 failure cases ranged from 40 days to 11.5 years postoperative. After adjustment for the possible potential confounders, older age (OR=1.06, 95% CI:1.01‒1.13, p=0.03) and the presence of diabetes (OR=4.93, 95% CI:1.33‒18.33, p=0.02) were the only significant predictors of operation failure. As for complications, six cases (3.6%) required reoperation, two cases (1.2%) had a bowel obstruction two and seven years after surgery, and one patient (0.6%) had vaginal mesh exposure.
Conclusion: The outcomes of Sacrocolpopexy/Sacrohysteropexy in our study are comparable to those in previous studies. Diabetes and elder age at the time of the surgery played a role in predicting recurrence. Sacrocolpopexy has a long–term profile of safety and efficacy. These findings could be key to stratifying surgical plans for pelvic organ prolapse cases.
Keywords: pelvic organ prolapse, Sacrocolpopexy, Sacrohysteropexy, laparoscopy, mesh complications, prolapse recurrence, surgical failure, success rate
Introduction
Pelvic organ prolapse (POP) is a medical condition that profoundly impacts women’s quality of life and usually affects middle–aged to older women.1 It is prevalent in 20–30% of women over the age of 20 years worldwide.2–5 In Saudi Arabia, a cross-sectional study of over 2000 women showed a prevalence of 23.4%.6 The most significant contributing factors were high parity and increasing age.4 As the population ages, it is expected that the need for pelvic reconstructive surgery will increase as well.7 Sacrocolpopexy is the standard procedure for apical prolapse correction with a higher success rate, lower recurrence rate, and less dyspareunia than the vaginal approach,8 with reported success rates of 78% and 92%, respectively.1,9 However, long-term data of approximately seven years reported a higher prevalence of POP recurrence, about 48%.10–12 In addition, the CARE trial12 reported that POP recurrence rates gradually increased with more prolonged follow–up. Furthermore, several reports highlighted that certain complications might only become apparent many years after the initial operation. Moreover, mesh exposure or erosion rate was reported to be 2% in 4 years of follow–up and as high as 10.5% after seven years.12,13
To our knowledge, the literature lacks long–term predictors and risk factors for prolapse recurrence after Sacrocolpopexy,14 with no studies done in Saudi Arabia, so far. Therefore, this study aimed to assess the efficacy and safety of Sacrocolpopexy, and to identify the predictors of recurrence in a Saudi setting.
Methods
Study Design
A retrospective cohort study design.
Study Participants
All patients who underwent Sacrocolpopexy (n=144) and Sacrohysteropexy (n=56) at a tertiary referral center between 2009 and 2021. One experienced urogynecologist performed all cases using a standardized technique. Sacrocolpopexy procedures were performed open, robotically assisted, or laparoscopically. Safety and efficacy of Sacrocolpopexy were assessed for 170 patients who attended the clinic for postoperative follow up. The difference between those who were followed up and those who were not was not statistically significant as regards to age (p=0.16), BMI (p=0.21), parity (p=0.58), history of bronchial asthma (p=0.76), diabetes mellitus (p=0.92) or previous surgery (p=0.14).
Study Setting
This study was conducted in Riyadh’s urogynecology and reconstructive pelvic surgery division at King Abdulaziz Medical City (KAMC). KAMC is a tertiary center. The division provides a high standard of care and has three consultants; however, only one performs Sacrocolpopexy surgery. Generally, cases are referred from central and peripheral Saudi Arabia.
Surgical Technique
Bladder dissection is carried out to the level of the trigone to correct any anterior vaginal prolapse accompanied by the apical prolapse. Polypropylene mesh (density of 44 g/m2) was attached to the anterior vaginal wall using fine stitches of ethibond non–absorbable suture. The main support and correction of the prolapse were done by attaching the mesh to the cervix using one or two stitches of ethibond non-absorbable sutures. Then, the mesh was fixed to the longitudinal intervertebral ligament using one stitch of non-absorbable suture. Our practice is to close the peritoneum to minimize mesh contact with adjacent organs.
Furthermore, most of the cases required posterior vaginal repair trans–vaginally. Initially, the surgeon used double mesh in a few cases, meaning another piece of mesh was attached to the dissected posterior vaginal wall 4 cm downward below the uterosacral ligaments. Then, the practice was shifted to using anterior mesh only, as a concern of the postoperative de novo constipation was raised by some patients.
Concomitant surgeries were added according to the presentation if a patient experienced stress urinary incontinence (SUI) measured using Sandvik score of more than three; then, a mid–urethral sling (trans obturator tape) was placed. Hysterectomy was suggested for all patients above 45 years old, especially those with uterine pathology such as abnormal uterine bleeding. All hysterectomies were subtotal, except in cases of cervical changes, in which a total hysterectomy was performed, and the vaginal vault was closed in two layers to minimize mesh erosion. Bilateral salpingectomy was performed in all patients who underwent a hysterectomy.
Regarding the surgeon’s initial experience, few cases were done using open and robotic-assisted procedures; however, in the following years since 2010, all cases were done using laparoscopic procedures, and the surgeon built an excellent experience using the laparoscopic technique.
Data Collection Methods
Electronic medical records were examined to collect data on the following:
- Patient characteristics include age, parity, weight and height, and medical and surgical history.
- Prolapse-related characteristics: These include; (1) symptoms of POP, (2) urinary symptoms, (3) bowel symptoms, and sexual dissatisfaction. For each Patient, data on clinical examination for the most recent Sacrocolpopexy/Sacrohysteropexy were taken, and the pre-and postoperative assessment was conducted using Baden walker grade.
- Surgery-related characteristics: These include; the approach of surgery (laparotomy, laparoscopy, or robotic), type of surgery (Sacrocolpopexy or Sacrohysteropexy), type of mesh used (anterior or double), and any concomitant surgery (hysterectomy, anterior, posterior vaginal repair or “TVTO”).
- Outcome characteristics: Subjective and objective preoperative and postoperative data were collected to assess postoperative success and failure rates, as follows:
● For subjective assessment, prolapse symptoms were collected from patients’ records pre– and post–operatively, based on a previously validated tool of data collection.7 All cases were given yearly follow–ups in the same institute, and all were evaluated by the surgeon or by a senior team member under his supervision. Every case was evaluated after surgery for symptoms of prolapse (feeling bulge, vaginal protrusion, and back pain), urge urinary incontinence, stress urinary incontinence (SUI), voiding dysfunction, constipation, and sexual dissatisfaction, and compared to the preoperative status, by asking a direct question about if each symptom was present, improved, or absent pre– and post–operatively.
● For objective assessment, all patients were examined pre– and post–operatively for recurrence and mesh exposure using the Baden walker classification of prolapse15 for each vaginal compartment, namely anterior, apical, and posterior compartments. It consists of grades: grade 0 - no prolapse, grade 1 - halfway to the hymen, grade 2 - to the hymen, grade 3 - halfway past the hymen, and grade 4 - maximum descent. The anatomical success of each vaginal compartment was considered if the grade was 0 or 1. Overall success was considered when all vaginal compartments showed anatomical success, and overall failure was considered when any of these vaginal compartments showed anatomical failure. The success rate of Sacrocolpopexy/Sacrohysteropexy was measured for each vaginal compartment, and the overall success was estimated by using the equation for calculation of attributable proportion16 as follows:
[(The preoperative percentage of cases with prolapse degree of 0 and 1 minus the postoperative percentage of patients with prolapse degree of 0 and 1) / the preoperative percentage of subjects with prolapse degrees of 0 and 1]. The same equation was used to measure the success rate of symptoms associated with pelvic organ prolapse in all cases. The degree of severity of preoperative prolapse was categorized into Severe (POP grade ≥3) and others (grade <3).
Data Analysis
The data in this study were collected and entered into MS Excel. The data were entered into Statistical Package for Social Science (SPSS) version 28 for analysis. The data were checked for normality using the Shapiro–Wilk test. Categorical variables were described using frequency and percentages. Mean, and Standard Deviation (SD) were used for continuous variables, such as age, weight, and laboratory results, if normally distributed; otherwise, median and interquartile range (IQR) were used. Density incidence of POP surgical failure was calculated. Wilcoxon signed-rank test was applied to test the association between the grades of prolapse before and after surgery. The association between the surgical outcome and some possible predictors was tested using the Chi–square test and analysis of variance. The strength of association was calculated using the odds ratio (OR) and the corresponding 95% confidence interval (CI). Significant predictors of surgical outcome were identified using the logistic regression analysis, adjusting for the following: posterior repair, parity, obesity, type of mesh (single vs double), and preoperative severity of the prolapse. A sensitivity analysis was performed excluding hysteropexy cases, for whom only four cases of failure were detected. Statistical significance was set at p <0.05.
Ethical Considerations
The study was approved by the Institutional Review Board (IRB) of the Ministry of National Guard- Health Affairs (MNG-HA) by study number NRC22R/371/08. The IRB of the MNG-HA waived the requirement for informed consent because of the study’s retrospective nature. All methods were carried out following relevant guidelines and regulations to ensure data confidentiality. This study was conducted in compliance with the Declaration of Helsinki.
Results
Patients’ Characteristics
From 2009–2021, a total of 200 patients underwent surgery, Sacrocolpopexy (144, 72%) and Sacrohysteropexy (56, 28%). Of those, 85% (170 cases) were seen and evaluated postoperatively, and 30 cases were not physically present at the clinic. The participants’ mean age and BMI at the surgery were 51.02±10.52 years and 30.9±5.0 kg/m2, respectively. More than one-half of patients (55.4%) were obese, Table 1.
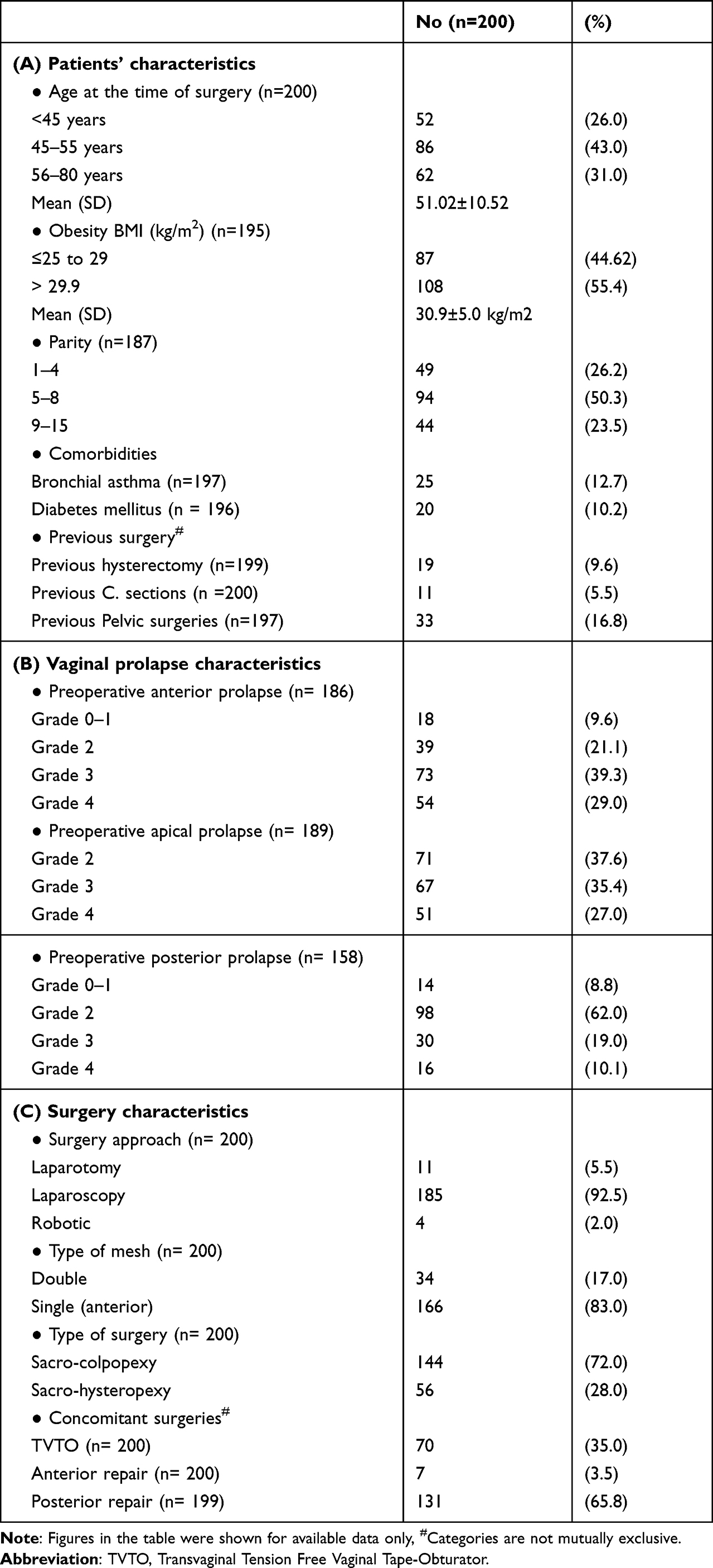 |
Table 1 Clinical and Demographic Information of Patients Who Underwent Sacrocolpopexy/Sacrohysteropexy from Year 2009 to Year 2021 at King Abdulaziz Medical City, Riyadh, Saudi Arabia |
Comorbidities included diabetes mellitus (10.2%) and bronchial asthma (12.7%). In addition, patients experienced prior hysterectomy (9.6%), prior cesarean sections (5.5%), and previous pelvic surgery (16.8%). Preoperative prolapse grading for each vaginal compartment was evaluated using the Baden-walker classification. All cases had apical prolapse grade two or more (37.2% grade two, 35.1% grade three, and 26.7% grade four). Posterior vaginal prolapse was presented in grades two (62%), three (19%), and four (10.1%). Anterior vaginal prolapse gradings were in 21.1%, 39.3%, and 29.0% of cases for grades two, three, and four, respectively, Table 1.
Concerning Surgery-related characteristics, most cases were treated using laparoscopy (185 cases, 92.5%), 11 using laparotomy (5.5%), and four cases using robotic-assisted procedures (2%). The most commonly used mesh type was the single anterior mesh (83%). A few cases (17%) had double mesh, which was anterior and posterior. Patients underwent posterior vaginal repair (65.8%), and anterior vaginal repair (3.5%). TVTO Transvaginal Tension Free Vaginal Tape-Obturator was done for 70 patients (35%), Table 1.
The Outcome of Sacrocolpopexy
The median duration from Sacrocolpopexy to the last follow–up visit for all participants was 1.7 years (IQR, 0.6–4.2), with a range of 0.1–12 years. Of all patients, 89.2%, 100%, and 91.1% presented with grade ≥2 anterior, apical, and posterior vaginal prolapse, respectively, and these proportions were reduced significantly after surgery to only 2.9%, 0.6%, and 13.5% respectively, with the success rates of 96.8%, 99.4% and 85.2% in the three compartments, respectively (p<0.001). The overall success rate was 83.1%, with an overall failure rate of 15.9% Table 2. The density incidence of failure was 5.98%.
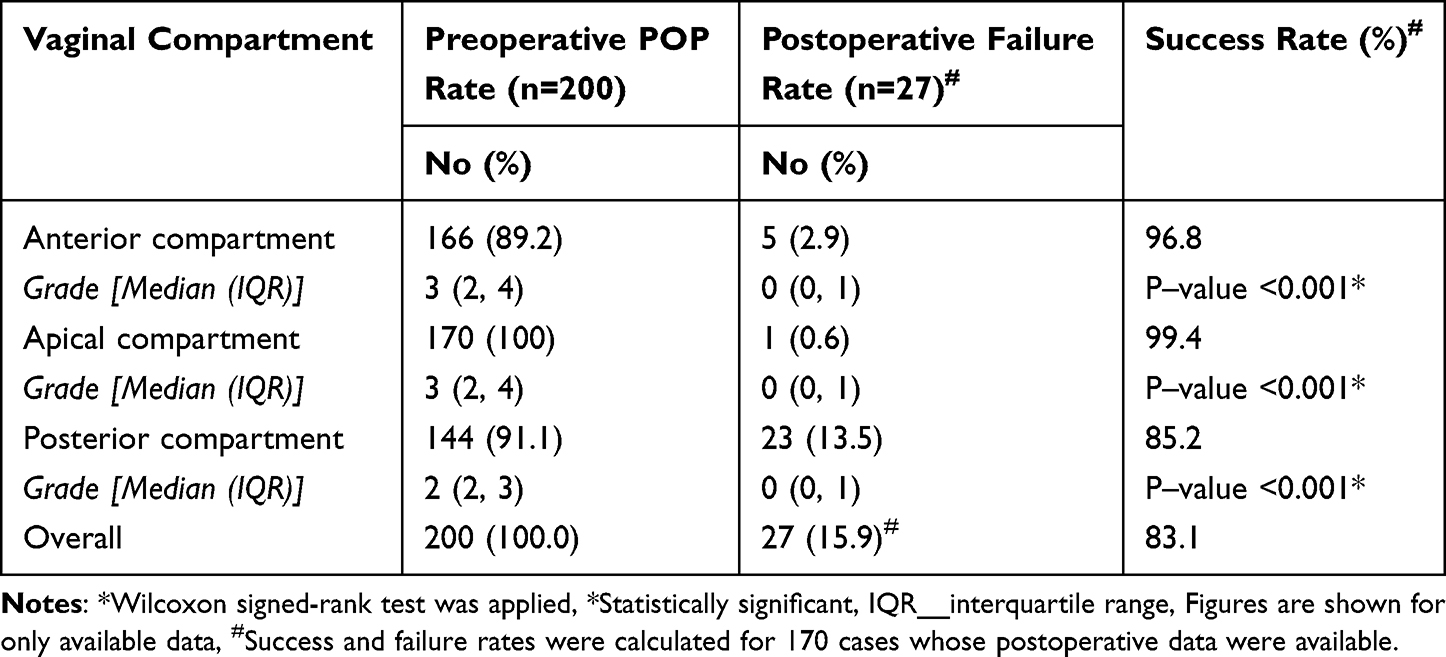 |
Table 2 Rate of POP Anatomical Failure Before and After Sacrocolpopexy and Surgery Success Rate |
The onset of failure ranged from 40 days to 11.5 years after the operation, with a median duration of 3.9 years (IQR, 0.8–6.9 years). For six patients (22%), failure occurred during the first year of operation, and another six patients (22%), had a failure during the first five years after the operation. For nine patients (34%), failure occurred five years and beyond. For six cases (22%) cases, the onset of failure was missing, Figure 1.
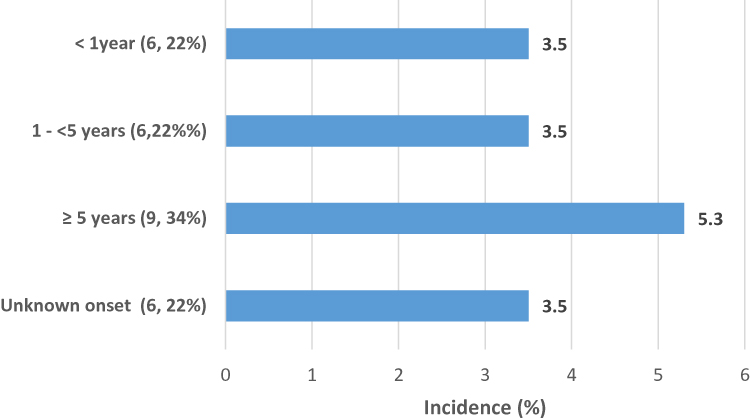 |
Figure 1 Incidence of postoperative failure. |
Figure 2 shows the subjective success rate of POP-related symptoms. The rate of symptoms reduced significantly after the operation as follows; sexual dissatisfaction (40% versus 10%, p<0.001, 75% success rate), constipation (40.9% versus 28.8%, p<0.001, 29.6% success rate), voiding dysfunction (34.1 versus 9.9%, p<0.001< 70.9% success rate), SUI (49.6% versus 20.0%, p<0.001, 59.7% success rate), urgency (68.6% versus 34.7%, p<0.001, 49.4% success rate), and POP symptoms (97.3% versus 2.1%, p<0.001, 97.9% success rate). De novo symptoms were noticed after surgery for the following symptoms; constipation (8.3%), voiding dysfunction (5.5%), SUI (5.6%), and Urgency (6.6%).
 |
Figure 2 Preoperative and postoperative symptoms associated with pelvic organ prolapse and success rate of Sacrocolpopexy [SR__success rate]. |
Predictors of Surgery Failure
In bivariate analyses, Sacrocolpopexy failure was positively associated with the age of 56–80 years (χ2=4.5, OR=1.2, 95% CI: 1.0‒1.5, p=0.04), and diabetes (χ2=13.5, OR= 6.2, 95% CI:2.1 ‒18.0), and was negatively associated with Concomitant posterior repair (χ2=7.7, OR=0.31, 95% CI: 0.13–0.73, p<0.006), (Table 3). Table 4 shows a comparison between Sacrocolpopexy and Sacrohysteropexy cases with regard to personal, surgery and outcome characteristics. Patients who underwent Sacrohysteropexy showed significantly younger mean age (40.06 versus 55.15 years, t=13.11, p<0.001), and lower mean parity (4.80 versus 7.19, t=6.39, p<0.001).
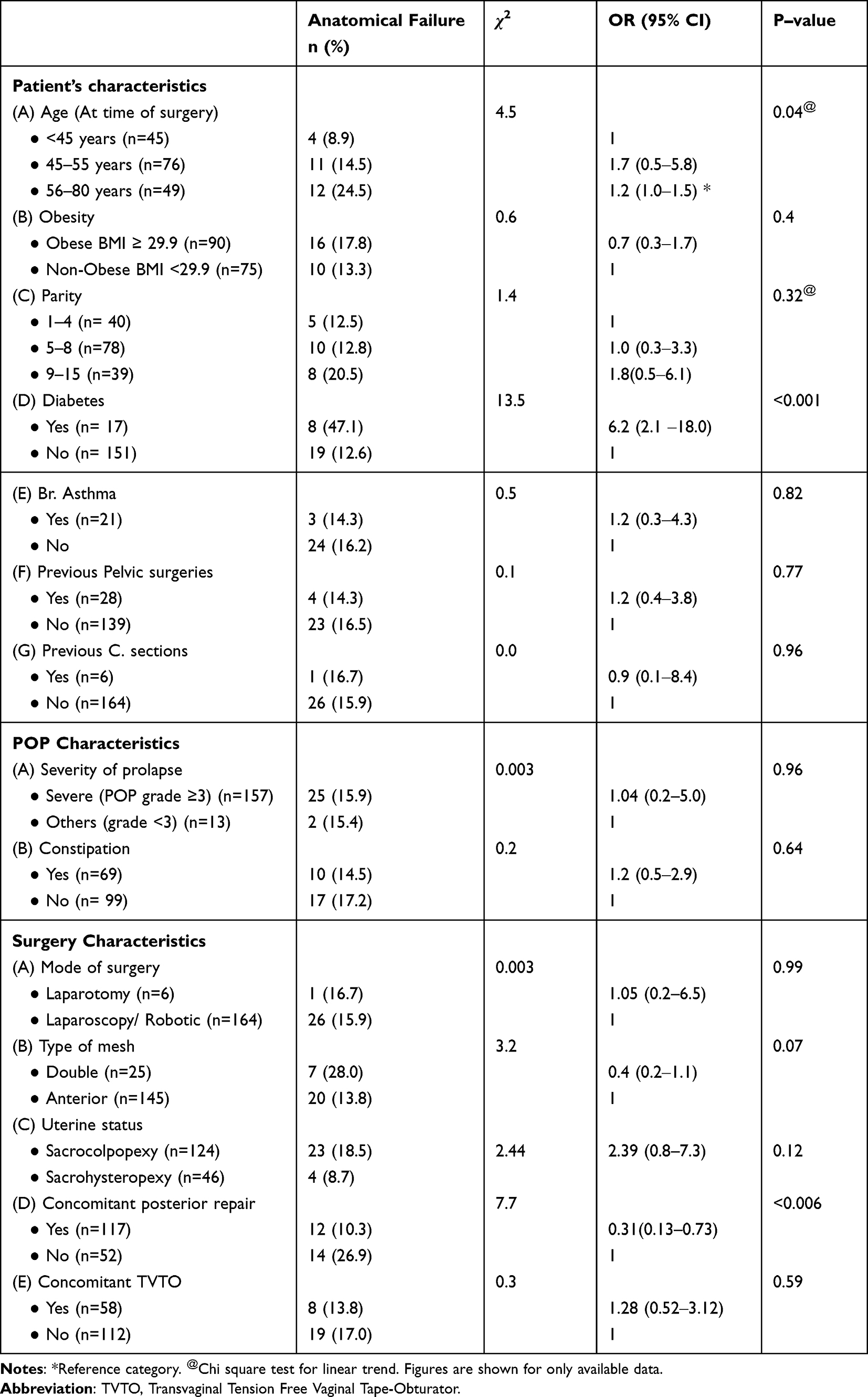 |
Table 3 Incidence of Anatomical Failure (Recurrence and Persistence) of Sacrocolpopexy According to Patient, Prolapse, and Surgery Characteristics |
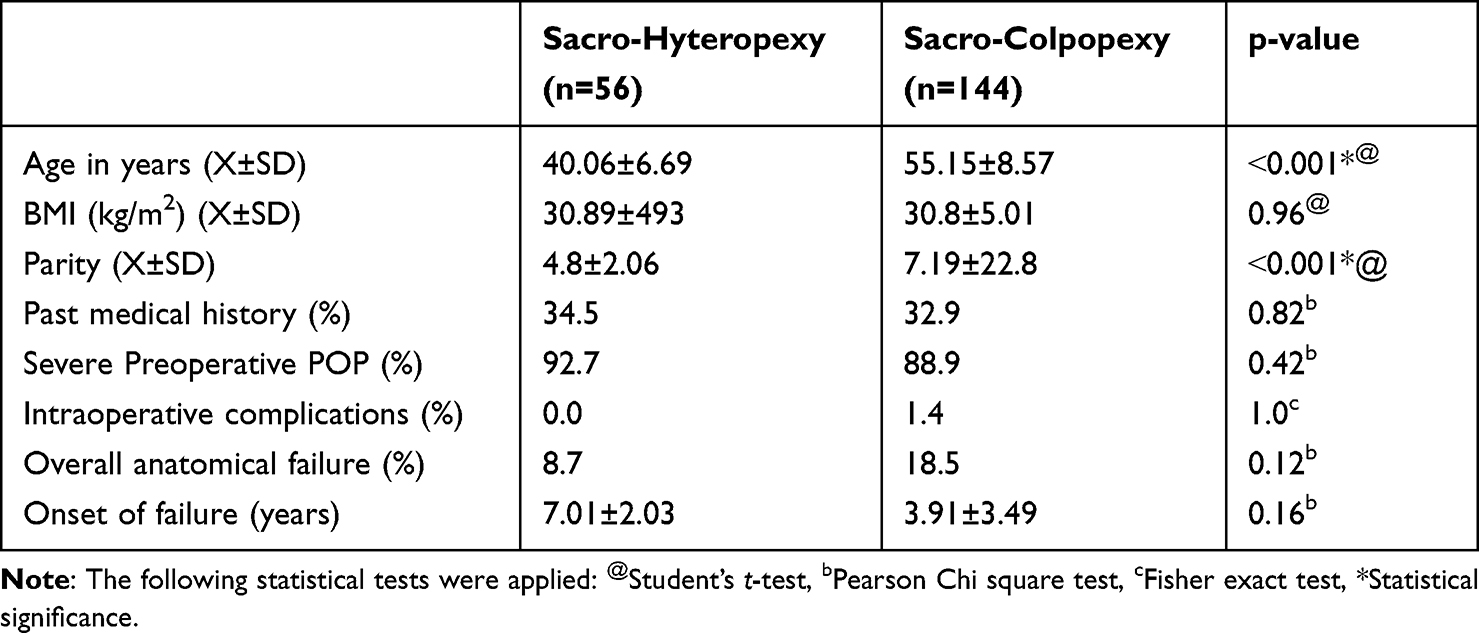 |
Table 4 Personal Characteristics and Outcome of Sacro-Hyteropexy and Sacro-Colpopexy Cases |
After adjustment for posterior repair, parity, BMI, type of mesh (anterior versus double), and preoperative POP grade, older age (OR=1.o6, 95% CI:1.01–1.13, p=0.03) and diabetes (OR=4.93, 95% CI: 1.33–18.33, p=0.02) were the only significant predictors of operation failure among Sacrocolpopexy cases. People with diabetes were nearly five times more likely to contract operation failure than non-diabetics Table 5.
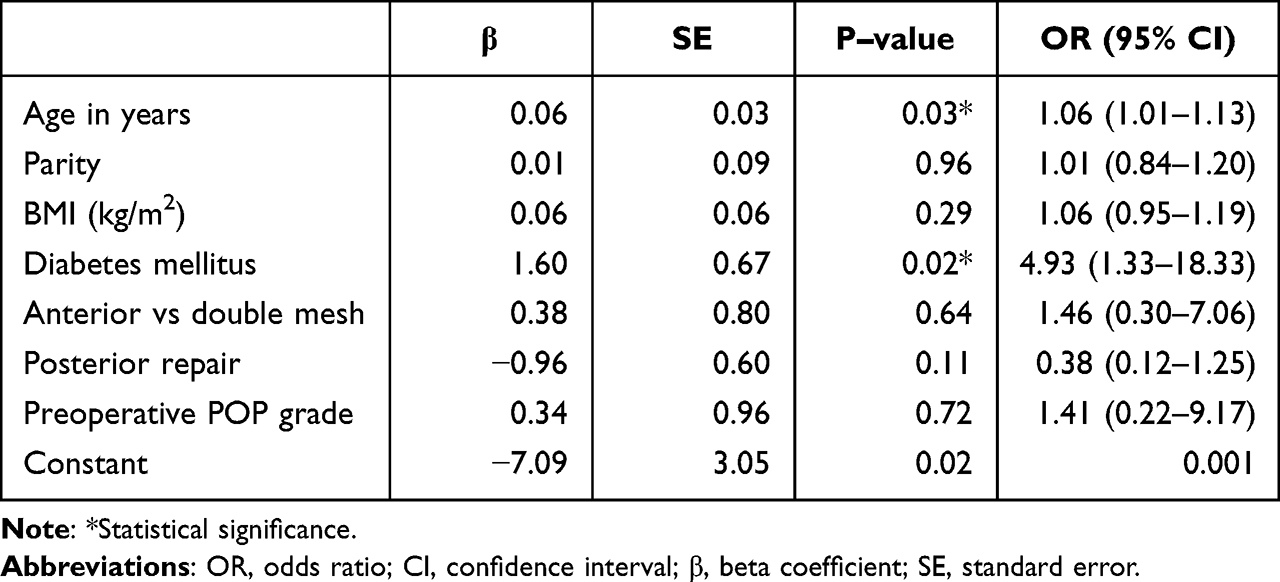 |
Table 5 Logistics Regression Analysis of the Predictors of Anatomical Failure (Recurrence /Persistence) After Sacrocolpopexy |
Complications
The most frequent cause of reoperation was SUI. Five cases required TVTO (three reported worsening SUI postoperatively, two refused to have vaginal mesh preoperatively, and one reported de novo SUI postoperatively, requiring surgical intervention). Surgery for recurrent prolapse was done for three cases (one needed posterior repair, one required anterior repair and TVTO mesh excision after pregnancy, and the third one required anterior and posterior vaginal repair). Two patients had a bladder injury intraoperative, and two required blood transfusions. One case developed pulmonary embolism two weeks after surgery, Table 6.
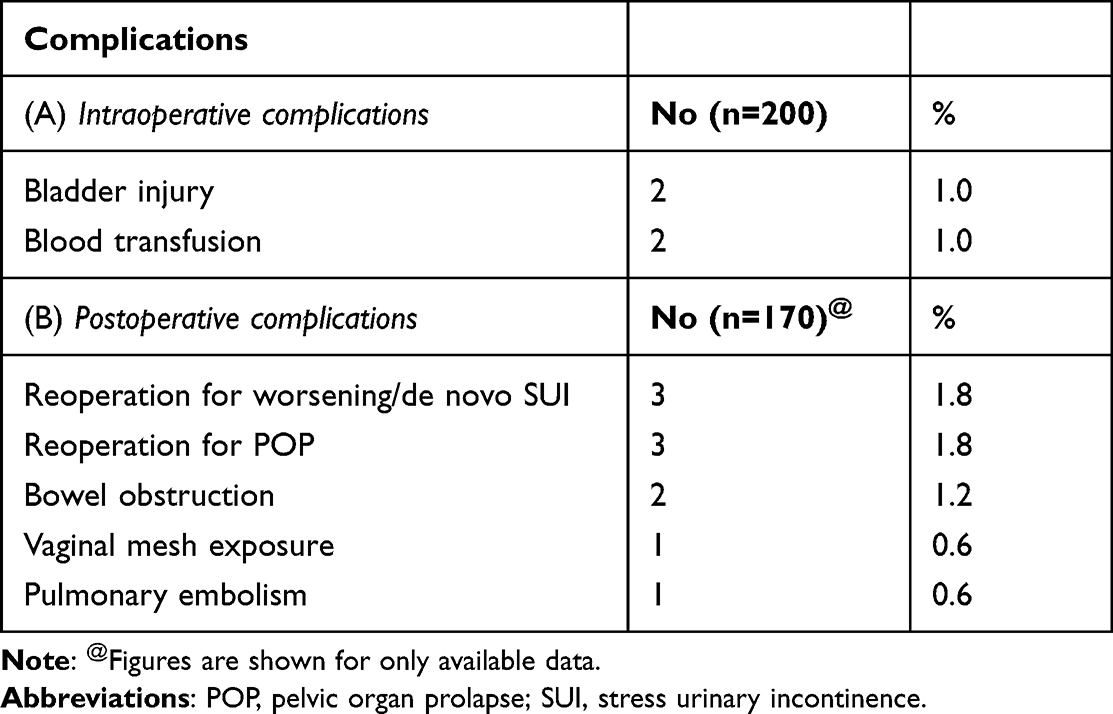 |
Table 6 Rate of Sacrocolpopexy-Related Complications |
Regarding Sacrocolpopexy mesh complications, in two patients, the mesh was entirely removed per the patients’ requests. Mesh was partially excised in a patient who presented with bowel obstruction seven years after the initial surgery. In another patient, mesh was released two years after surgery for bowel obstruction. However, no bowel resection was required in those two cases. Vaginal exposure of 0.5 cm mesh in the posterior vaginal wall was diagnosed in one patient immediately after surgery and was treated with local estrogen cream, Table 6.
Discussion
In our study of 200 patients who underwent Sacrocolpopexy and followed for a period of 0.1 to 12 years, Success rates of 96.8%, 99.4%, and 85.2% were shown in the anterior, apical, and posterior vaginal compartments, respectively, with an overall success rate of 83.1 percent. The overall failure rate was 15.9%, with a density incidence of 5.98 per 100 women-years. This finding was in agreement with the findings of others in previous studies, where the long-term results for approximately seven years showed a recurrence rate of 16.2%–22%.1,9,17,18 The most frequent failure in our study was in the posterior compartment (13.5%), a similar finding reported in a prospective study (18% were recurrence of the posterior vaginal prolapse),19 While in another previous study showed that 62% of recurrence were in anterior compartment.18 However, these differences might be due to different surgical strategies and the extent of bladder dissection.18,20
The onset of failure in 27 failure cases ranged from 40 days to 11.5 years after the operation. Six patients had a failure during the first year after the procedure (3.5% failure rate). Sato et al21 reported three cases (6.5%) of failure out of 46 post Sacrocolpopexy during the first year, while a higher failure rate of 104 cases out of 709 (14.7%) was reported by Thomas et al.7 In our study, another six patients (3.5% failure rate) had a failure during the first five years after surgery. Failure rates of 9%, 13.9%, and 3%, were reported in previous studies during the same period following surgery.1,17,18 Nine cases (5.3% failure rate) had failure five years and beyond. A recurrence rate was reported by Ganatra et al9 of 28 cases out of 66 patients (42%) followed up for more than five years. These differences in failure rate could be attributed to the different definitions used across studies.
Predictors of Surgery Failure
In our study, after adjustment for possible potential confounders, older age and the presence of diabetes were the only significant predictors of operation failure, while parity, obesity, type of mesh and severity of preoperative POP were not significant predictors of POP recurrence. Isık et al22 reported having diabetes mellitus and hypertension double the risk of having primary pelvic organ prolapse; therefore, it may support the same concept of having a higher chance of failure postoperatively.22 In our study, people with diabetes were nearly five times more likely to contract operation failure than non-diabetics. This finding agreed with a recent study that reported that women with diabetes mellitus were almost four times as likely to experience anterior vaginal prolapse recurrence over time.23 Other previous studies failed to report diabetes as a risk factor for POP recurrence,24–26 which indicates that diabetes mellitus control might play a role. However, diabetes control was not evaluated in our study. Recent studies highlighted a higher incidence of mesh–related complications in diabetes mellitus patients.26
Age as a risk factor for POP recurrence showed inconsistent results.5 In two previous studies, younger age was a significant risk factor for POP recurrence after surgery,27,28 and this finding was in contrast to our study’s finding, where older women showed significantly higher rates of POP recurrence and overall failure, even after adjusting for other variables. This association might be attributed to the menopausal status and tissue quality in older women.17 However, our cohort is younger than its counterpart cohorts in the previous studies,27,28 where most of the women in our study were below the age of 55 years. This association between age and POP recurrence could be nonlinear, in the form of a J shape, with an association between POP recurrence and younger and older women. However, further studies are necessary to prove this hypothesis. In other previous studies,17,28–30 no significant association was reported between age and POP recurrence.
There are contradictory reports in the literature regarding the impact of reconstructing the posterior vaginal prolapse on the chance of recurrence.17,31 In our study, women who underwent a concurrent posterior colporrhaphy had significantly lower odds of POP recurrence; yet, after adjusting for possible confounders, the posterior repair was not a significant predictor of POP recurrence. According to patients’ main symptoms, tailoring management may be the key to successful surgery. Therefore, for patients having symptomatic posterior vaginal prolapse, with defecatory symptoms may benefit posterior vaginal reconstructive repair.17
Subjective Outcomes
In our study, all POP-related symptoms were reduced significantly after the operation, with success rates that ranged from 29.6% to 97.9%. Feeling bulge symptoms showed the highest success rate of 97.9%. In our study. This rate was similar to rates of 96.6% and 88% reported in previous studies.7,18 Nearly 60% of our patients who had SUI preoperatively reported improvement in their symptoms, compared to 20.8% and 43% of patients in previous studies.7,19 In our study, for patients with symptoms of urge/urge incontinence, a success rate of 49% was detected after surgery. This finding was in agreement with a success rate of 46% in a previous study19 and higher than 26.8% and 39% success rates in other studies.1,7 However, comparing our results with those in the literature might not be valid due to the different methodologies used in diagnosing urge/urge incontinence. Our study showed a significant improvement of 70.9% in voiding dysfunction. High rates of improvement (85.7%) were reported in the literature when objective evaluation using urodynamic assessment was utilized.20
In our study, a success rate of 29.6% was noticed for constipation. A higher success rate of 42% was reported in a previous study.19 However, different surgical techniques and the multifactorial nature of constipation might play a role in the success rate. Despite that Sacrocolpopexy is known to have a lower rate of dyspareunia compared to the vaginal approach,8 a wide range of postoperative sexual dysfunction was reported in the literature (0–47%).9 In our study, the rate of sexual dissatisfaction was reduced from 40% before surgery to 10% after, with a success rate of 75%. Sexual dissatisfaction is a multifactorial issue that may result in different outcomes.
Complications
In our cohort, de novo symptoms were 5.6% for SUI and 8.3% for constipation, compared to 7.5% and 6.5% in a previous study.1 A lower incidence of postoperative de novo voiding dysfunction (5.5%) was reported by our patients versus 9.6% and 10.4% in published data based on objective assessment via urodynamic.13,20 Eight of our patients (6.6%) reported de novo symptoms of urge/urge incontinence, as compared to lower incidences (0–3%) reported in the literature.13,20 Three cases (1.8%) of our patients required reoperation for SUI. This figure was similar to what was reported by Sato et al,21 who reported that 2.2% of patients needed sling surgery after Sacrocolpopexy. Another three cases (1.8%) of our patients required reoperation for prolapse; none was for the apical compartment. This finding was consistent with the results in the literature, where an overall reoperation for prolapse was required for 0.4–5.3% of cases, with most cases being non-apical prolapse.1,24,25
Regarding mesh complications postoperatively, there is a possibility that some patients had asymptomatic mesh exposure; however, in our study, irrespective of symptoms, patients were examined postoperatively for mesh exposure detection. One Patient had vaginal mesh exposure immediately after surgery, which was managed conservatively. Similar to reported cases by Orhan et al,13 2.1% of vaginal mesh exposure was all treated conservatively. Bowel obstruction associated with Sacrocolpopexy was reported in two cases, in our study; one was two years after surgery, and the second was seven years after surgery. Wadensweiler et al32 in 2021 reported an incidence of 1% average presentation time (2.5–8.8 years). Pue et al33 said a similar delayed incidence approximately 14 years after surgery.
Strengths and Limitations
This study’s major strength was that most previous studies had multiple surgeons, at least two. In contrast, our study had one surgeon who performed all surgeries, so surgical techniques and skills were unified for all cases. However, our study has some limitations. These limitations were those inherent to all retrospective analyses. Subjective data on symptoms of prolapse were collected from records, and these data might be subjected to a recall bias. Some patients might not attend the follow-up visits, especially those with no symptoms or complications, which might overestimate the success rate. The outcome was estimated based on the Baden-Walker grading system, which was the only staging system available in the hospital records during the study period, rather than POP-Q exam stage, different anatomic follow–up periods, and the use of anterior vaginal mesh was the predominantly used approach to Sacrocolpopexy which might not be the classically prescribed approach. In addition, some patients were more likely to return for a follow–up due to the recurrence of prolapse. Moreover, this study was conducted on patients who attended only one health center, and all of them were operated on by only one surgeon, which may not allow for the generalization of our conclusion. Moreover, other confounding variables not included in this study such as; diabetic control and preoperative and postoperative HbA1c levels; were not considered in the analysis. Further multicenter studies are recommended.
Conclusions
The outcomes of Sacrocolpopexy in our study are comparable to those in previous studies. Diabetes and advanced age at the time of the surgery played a role in predicting recurrence. Sacrocolpopexy has a long–term profile of safety and efficacy. These findings could be viewed as a key to stratifying surgical plans for pelvic organ prolapse cases. Further multicenter studies are recommended to address more relevant information regarding sacrocolpopexy.
Abbreviations
POP, Pelvic organ prolapse; CARE, Colpopexy and urinary reduction efforts; SUI, stress urinary incontinence; KAMC, King Abdulaziz Medical City; TVTO, Transvaginal Tension Free Vaginal Tape-Obturator; BMI, body mass index; IRB, institutional review board.
Data Sharing Statement
Most of the data supporting our findings are contained within the manuscript, and all others, excluding identifying/confidential patient data, will be shared upon request by contacting the corresponding author [Mostafa Abolfotouh [email protected]].
Acknowledgments
This study was initiated by King Abdullah International Medical Research Center, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia. All individuals included in this section have consented to the acknowledgement.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Sawada Y, Kitagawa Y, Hayashi T, et al. Clinical outcomes after laparoscopic sacrocolpopexy for pelvic organ prolapse: a 3‐year follow‐up study. Int J Urol. 2021;28(2):216–219. doi:10.1111/iju.14436
2. Nygaard I, Bradley C, Brandt D; Women’s Health Initiative. Pelvic organ prolapse in older women: prevalence and risk factors. Obstet Gynecol. 2004;104(3):489–497. doi:10.1097/01.AOG.0000136100.10818.d8
3. Hendrix SL, Clark A, Nygaard I, Aragaki A, Barnabei V, McTiernan A. Pelvic organ prolapse in the Women’s Health Initiative: gravity and gravidity. Am J Obstet Gynecol. 2002;186(6):1160–1166. doi:10.1067/mob.2002.123819
4. Masenga GG, Shayo BC, Rasch V. Prevalence and risk factors for pelvic organ prolapse in Kilimanjaro, Tanzania: a population based study in Tanzanian rural community. PLoS One. 2018;13(4):e0195910. doi:10.1371/journal.pone.0195910
5. Vergeldt TF, Weemhoff M, IntHout J, Kluivers KB. Risk factors for pelvic organ prolapse and its recurrence: a systematic review. Int Urogynecol J. 2015;26:1559–1573. doi:10.1007/s00192-015-2695-8
6. Al-Badr A, Saleem Z, Kaddour O, et al. Prevalence of pelvic floor dysfunction: a Saudi national survey. BMC Womens Health. 2022;22(1):27. doi:10.1186/s12905-022-01609-0
7. Thomas TN, Davidson ER, Lampert EJ, Paraiso MF, Ferrando CA. Long-term pelvic organ prolapse recurrence and mesh exposure following sacrocolpopexy. Int Urogynecol J. 2020;31:1763–1770. doi:10.1007/s00192-020-04291-8
8. Maher C, Feiner B, Baessler K, Schmid C. Surgical management of pelvic organ prolapse in women. Cochrane Database of Systematic Rev. 2013;2013(4):154.
9. Ganatra AM, Rozet F, Sanchez-Salas R, et al. The current status of laparoscopic sacrocolpopexy: a review. Eur Urol. 2009;55(5):1089–1105. doi:10.1016/j.eururo.2009.01.048
10. Unger CA, Paraiso MF, Jelovsek JE, Barber MD, Ridgeway B. Perioperative adverse events after minimally invasive abdominal sacrocolpopexy. Am J Obstet Gynecol. 2014;211(5):547–e1. doi:10.1016/j.ajog.2014.07.054
11. Brubaker L, Nygaard I, Richter HE, et al. Two-year outcomes after sacrocolpopexy with and without burch to prevent stress urinary incontinence. Obstet Gynecol. 2008;112(1):49. doi:10.1097/AOG.0b013e3181778d2a
12. Nygaard I, Brubaker L, Zyczynski HM, et al. Long-term outcomes following abdominal sacrocolpopexy for pelvic organ prolapse. JAMA. 2013;309(19):2016–2024. doi:10.1001/jama.2013.4919
13. Orhan A, Ozerkan K, Vuruskan H, et al. Long-term follow-up of laparoscopic sacrocolpopexy: comparison of two different techniques used in urology and gynecology. Int Urogynecol J. 2019;30:623–632. doi:10.1007/s00192-018-03858-w
14. Jefferis H, Price N, Jackson S. Laparoscopic hysteropexy: 10 years’ experience. Int Urogynecol J. 2017;28:1241–1248. doi:10.1007/s00192-016-3257-4
15. Baden WF, Walker TA, Lindsey JH. The vaginal profile. Tex Med. 1968;64:56–58.
16. Centers for Disease Control and Prevention. Principles of epidemiology. Centers for Disease Control and Prevention; 2023. Available from: https://www.cdc.gov/csels/dsepd/ss1978/lesson3/section6.html.
17. Chang OH, Davidson ER, Thomas TN, Paraiso MF, Ferrando CA. Predictors for pelvic organ prolapse recurrence after sacrocolpopexy: a matched case-control study. Urogynecology. 2021;27(1):e165–70.
18. Wong V, Guzman Rojas R, Shek KL, Chou D, Moore KH, Dietz HP. Laparoscopic sacrocolpopexy: how low does the mesh go? Ultrasound Obstetr Gynecol. 2017;49(3):404–408. doi:10.1002/uog.15882
19. Claerhout F, De Ridder D, Roovers JP, et al. Medium-term anatomic and functional results of laparoscopic sacrocolpopexy beyond the learning curve. Eur Urol. 2009;55(6):1459–1468. doi:10.1016/j.eururo.2008.12.008
20. Blanco-Montenegro I, De Ritis R, Chiappini M. Imaging and modelling the subsurface structure of volcanic calderas with high-resolution aeromagnetic data at Vulcano (Aeolian Islands, Italy). Bull Volcanol. 2007;69:643–659. doi:10.1007/s00445-006-0100-7
21. Sato H, Abe H, Ikeda A, Miyagawa T, Sato K. Complications and clinical outcomes of laparoscopic sacrocolpopexy for pelvic organ prolapse. J Obstet Gynaecol. 2021;41(1):128–132. doi:10.1080/01443615.2020.1724914
22. Isık H, Aynıoglu O, Sahbaz A, Selimoglu R, Timur H, Harma M. Are hypertension and diabetes mellitus risk factors for pelvic organ prolapse? Eur J Obstetr Gynecol Reprod Biol. 2016;197:59–62. doi:10.1016/j.ejogrb.2015.11.035
23. Eckhardt S, Laus K, DeAndrade S, Lee J, Nguyen J. The impact of diabetes mellitus on pelvic organ prolapse recurrence after robotic sacrocolpopexy. Int Urogynecol J. 2023;25:1–8.
24. Linder BJ, Chow GK, Elliott DS. Long‐term quality of life outcomes and retreatment rates after robotic sacrocolpopexy. Int J Urol. 2015;22(12):1155–1158. doi:10.1111/iju.12900
25. Baines G, Price N, Jefferis H, Cartwright R, Jackson SR. Mesh-related complications of laparoscopic sacrocolpopexy. Int Urogynecol J. 2019;30:1475–1481. doi:10.1007/s00192-019-03952-7
26. Ringel NE, de Winter KL, Siddique M, et al. Surgical outcomes in urogynecology—assessment of perioperative and postoperative complications relative to preoperative hemoglobin A1c—A Fellows Pelvic Research Network Study. Female Pelvic Med Reconstr Surg. 2022;28(1):7–13. doi:10.1097/SPV.0000000000001057
27. Whiteside JL, Weber AM, Meyn LA, Walters MD. Risk factors for prolapse recurrence after vaginal repair. Am J Obstet Gynecol. 2004;191(5):1533–1538. doi:10.1016/j.ajog.2004.06.109
28. Diez-Itza I, Aizpitarte I, Becerro A. Risk factors for the recurrence of pelvic organ prolapse after vaginal surgery: a review at 5 years after surgery. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(11):1317–1324. doi:10.1007/s00192-007-0321-0
29. Salvatore S, Athanasiou S, Digesu GA, et al. Identification of risk factors for genital prolapse recurrence. Neurourol Urodyn. 2009;28(4):301–304. doi:10.1002/nau.20639
30. Tegerstedt G, Hammarstrom M. Operation for pelvic organ prolapse: a follow-up study. Acta Obstet Gynecol Scand. 2004;83(8):758–763. doi:10.1111/j.0001-6349.2004.00468.x
31. Grimes CL, Lukacz ES, Gantz MG, et al. What happens to the posterior compartment and bowel symptoms after sacrocolpopexy? Evaluation of 5-year outcomes from E-CARE. Urogynecology. 2014;20(5):261–266.
32. Wadensweiler P, Whitcomb EL, Jeney SE, et al. Bowel obstruction after sacrocolpopexy: a case series. Female Pelvic Med Reconstr Surg. 2021;27(11):e677–80. doi:10.1097/SPV.0000000000001095
33. Pue LB, Lo TS, Wu PY, Tan YL. Strangulated small bowel 14 years after abdominal sacrocolpopexy. J Obstetr Gynaecol Res. 2014;40(2):611–613. doi:10.1111/jog.12174
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.