Back to Journals » International Medical Case Reports Journal » Volume 18
The Oncogenic Human Papillomavirus Involvement as a Risk Factor of Measles, Mumps, and Rubella Vaccine Immunotherapy Failure in Anogenital Warts
Authors Achdiat PA ![]() , Ismiranty D
, Ismiranty D ![]() , Hindritiani R
, Hindritiani R ![]() , Rizqandaru T
, Rizqandaru T ![]() , Usman HA
, Usman HA ![]() , Maharani RH
, Maharani RH ![]()
Received 1 October 2024
Accepted for publication 4 January 2025
Published 14 January 2025 Volume 2025:18 Pages 83—90
DOI https://doi.org/10.2147/IMCRJ.S498892
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Pati Aji Achdiat,1 Dyah Ismiranty,1 Reti Hindritiani,1 Trustia Rizqandaru,1 Hermin Aminah Usman,2 Retno Hesty Maharani1
1Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin Hospital, Bandung, Indonesia; 2Department of Anatomical Pathology, Faculty of Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin General Hospital, Bandung, Indonesia
Correspondence: Pati Aji Achdiat, Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin Hospital, Jl. Pasteur 38, Bandung, West Java, Indonesia, 40161, Tel +6281225955478 ext. 3449, Fax +62222032426, Email [email protected]
Abstract: Anogenital warts (AGW) including multiple types of human papillomavirus (HPV) are prevalent. In this context, oncogenic HPV infection leads to anogenital cancers and the lesion is more persistent. Several research on AGW therapy with measles, mumps, and rubella (MMR) vaccine injections have been successful without adverse effects. However, the effects of MMR immunotherapy for AGW on multiple HPV infections have not been reported. This research is a case report of AGW in a 17-year-old male treated with MMR. The inclusion criteria specified young age, indicative of a strong immunological status. Meanwhile, the exclusion criteria comprised immunocompromised conditions, such as HIV confirmed to be negative. Dermatological examination showed that the pubic region and penile shaft presented 51 verrucous papules for 6 months, with histopathological results supporting the diagnosis of AGW. Polymerase chain reaction (PCR) examination reported the inclusion of HPV types 6, 11, and 16. The subcutaneous MMR vaccine was injected into the deltoid area every 2 weeks for three sessions. Meanwhile, the treatment response was assessed by counting the number and measuring the size of the lesion. After three sessions of MMR immunotherapy, there was no improvement in the size or quantity of lesions. Based on previous reports, a higher clearance rate for MMR immunotherapy was found in warts with a duration of < 6 months, while oncogenic HPV genotypes, particularly HPV type 16, take longer to clear than others. The efficacy of subcutaneous MMR injection for AGW treatment was unfavorable due to oncogenic HPV types. AGW treated with MMR immunotherapy should investigate oncogenic HPV genotype. However, further research needs to be carried out to justify this conclusion due to the limitations.
Keywords: anogenital warts, immunotherapy, MMR vaccine, multiple HPV infections
Introduction
Anogenital warts (AGW) are benign proliferative lesions on the epithelium of the skin and mucous membrane of the genitalia, anus, and perianal area, as well as inguinal and pubic regions.1,2 AGW is the most prevalent sexually transmitted infection (STI) ranking as the third most common disease in 2007–2011 based on the data from 12 teaching hospitals in Indonesia.3–5 The global incidence ranges between 160–289 cases per 100,000 population per year.1 The incidence of AGW is most prevalent in females and males less than 24 years old and 25–29 years old.3 Based on data from Dr. Hasan Sadikin General Hospital Bandung from 2018 to 2023, 260 AGW cases attended the venereology outpatient clinic.
AGW are caused by human papillomavirus (HPV) infection, primarily types 6 and 11.1,6 Oncogenic types of HPV, such as types 16 and 18, may also be detected in AGW lesions (Table 1).1 Coinfection with multiple types is prevalent but the impact on persistence and the development of malignancies remains unclear.7 Research in Latin America found that 28% were infected or coinfected with high-risk HPV.8 Individuals with AGW persisting for a duration of 1–6 months were found to be three times more prone to having oncogenic HPV infection compared to those with warts lasting less than 1 month.9 Approximately 90% resolve spontaneously within 2 years by the immune system of the body. However, some infections can lead to clinical manifestations and complications, including AGW, recurrent respiratory papillomatosis, and various forms of cancer.7
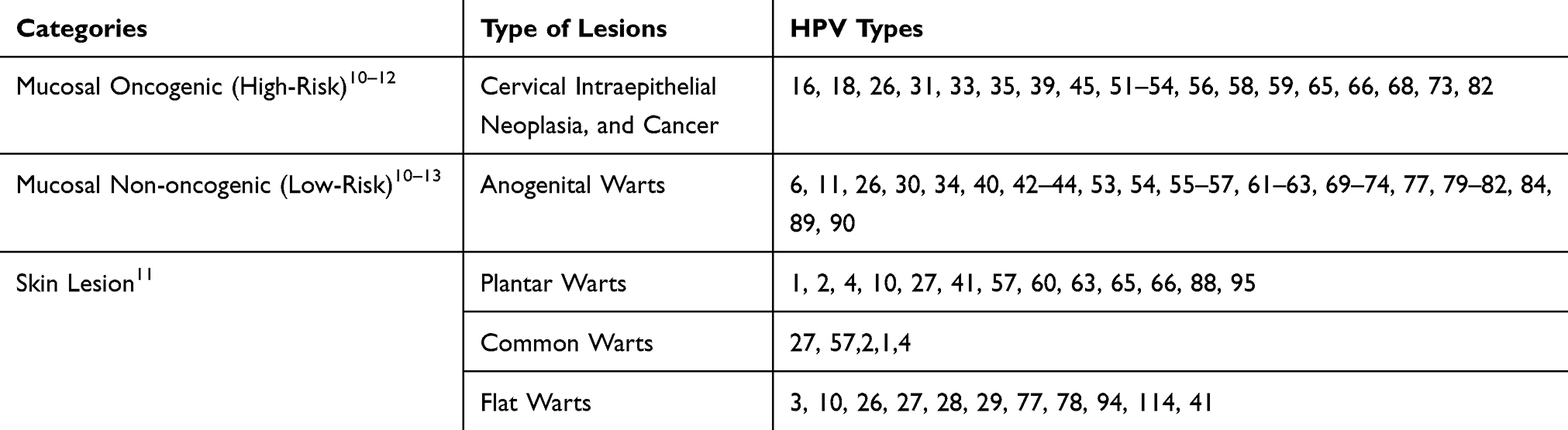 |
Table 1 Types of HPV and Their Association with Different Clinical Manifestations |
Treatment for AGW is painful, time-consuming, and requires clinician assistance since recurrence is common.14 The condition can be treated with immunotherapy, as well as surgical methods such as electrocautery.2,15 Immunotherapy aims to destroy warts, even those located far from the injection site to prevent recurrence.16 The immunotherapy agents observed are the measles, mumps, and rubella (MMR) vaccine.17 The MMR vaccine is a live attenuated strain of the MMR virus.18 Several research on the therapy of AGW with MMR injection were successful and showed no serious adverse effects.16,18,19 Limitations of MMR immunotherapy include the contraindication in specific populations, such as pregnant women and immunocompromised individuals who are at a higher risk of infection. Previous research reported that the success rate of MMR immunotherapy for warts varied significantly, with success rates ranging from 58.7% to 87.8%.16 Meanwhile, the complete response rate for AGW was 63.64%.4 There was no recurrence even though the recurrence data was limited to 6 months.16 Previous research on MMR immunotherapy for AGW caused by multiple HPV infections have not been reported. A case of AGW caused by multiple HPV types (low-risk type 6, 11, and high-risk type 16) in the pubic region and penile shaft in a 17-year-old male was reported. The AGW was unsuccessfully treated with a subcutaneous MMR injection but the lesions were removed by electrocauterization. Therefore, this research aimed to evaluate the immune response to MMR immunotherapy in patients with AGW of oncogenic and non-oncogenic HPV types.
Clinical Case
A 17-year-old male presented to the Venereology Clinic with a chief complaint of multiple itchy, brownish papules located in the pubic region and on the penile shaft. The skin lesions initially appeared 6 months before the visit in the form of small papules that appeared in a few numbers. The papules multiplied and showed confluence, causing some lesions to increase in size. The patient had not obtained any medication for the complaint. The patient was not yet married but had engaged in sexual intercourse since 14 years old with approximately eight female sexual workers without protection. Additionally, the patient smoked approximately 20 cigarettes daily, had no history of narcotic or alcohol use, had urethral discharge approximately 1 month ago and went to a general physician for medical attention. The physician informed the patient of a possible gonorrheal infection and administered treatment through an intramuscular injection.
On physical examination, the important signs were within normal limits, the patient was of normal weight, and no lymph node enlargement was found. Venereological examination reported lesions in the pubic region and penile shaft, presenting as 51 verrucous papules. Additionally, no abnormalities were observed in the hair, nails, palms, or soles and the acetowhite test results were negative. Blood serum tests for human immunodeficiency virus (HIV), hepatitis B surface antigen (HBsAg), Treponema pallidum hemagglutination assay (TPHA), and venereal disease laboratory (VDRL) titers were non-reactive. A dermoscopic examination of the lesion reported a knob-like appearance, as shown in Figure 1. An excisional shave biopsy was obtained from a skin lesion in the pubic region and sent to the Department of Pathological Anatomy for investigation. Histopathological examination showed hyperkeratosis, papillomatosis, acanthosis, koilocytosis (Figure 2), and lymphocyte infiltration, supporting the diagnosis of AGW and condyloma acuminata. PCR genotyping reported that HPV types 6, 11, and 16 were found in warts on the base of the penis obtained by shave biopsy.
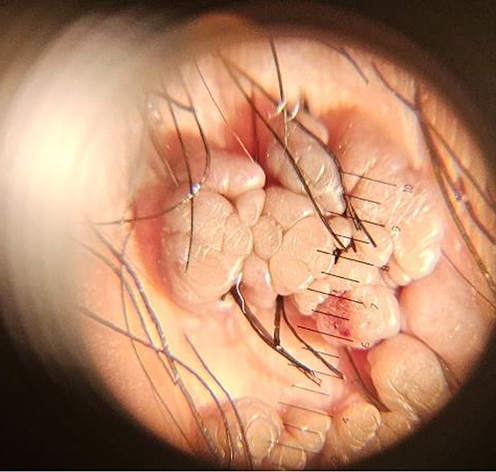 |
Figure 1 Dermoscopic results showed a knob-like appearance. |
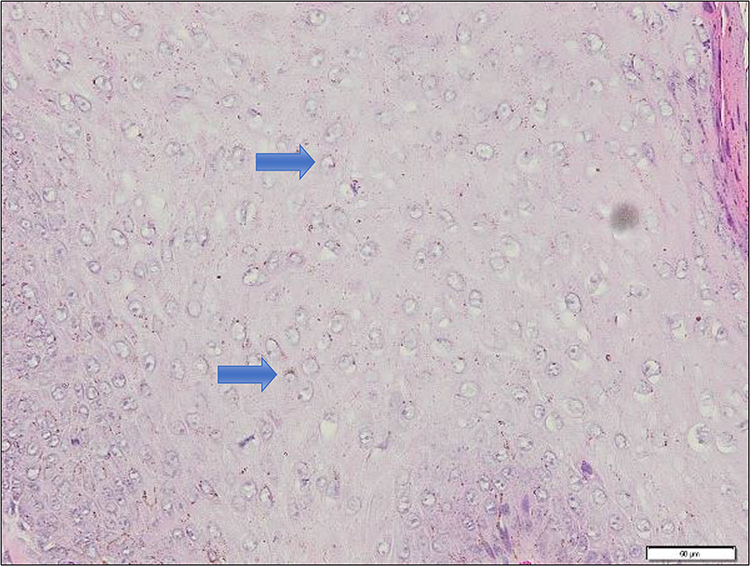 |
Figure 2 Histopathological results with hematoxylin-eosin staining showed koilocytosis of the nucleus (blue arrow), magnification 400x. |
The patient was treated with a subcutaneous MMR vaccine injection in the right upper arm every 2 weeks for three sessions and avoided any sexual contact during treatment. The dose of injected MMR vaccine was 0.5 mL and there were no signs of swelling, nodules, blisters, or abscesses at the injection sites. Treatment effectiveness was evaluated by measuring the size and quantity of warts at each subsequent visit. However, at the 1-month follow-up after the third injection, there was no discernible improvement in the size or quantity of the lesions (Figure 3A and B). The patient complied to avoid any sexual contact during treatment which was carried out with a sexual worker. The itching sensation was diminished after the third injection. Additionally, there were no reports of pain, itching, redness, swelling, or flu-like symptoms. The remaining lesions were completely removed by electrocautery (Figure 4) and no recurrence was observed during the 6 months following immunotherapy.
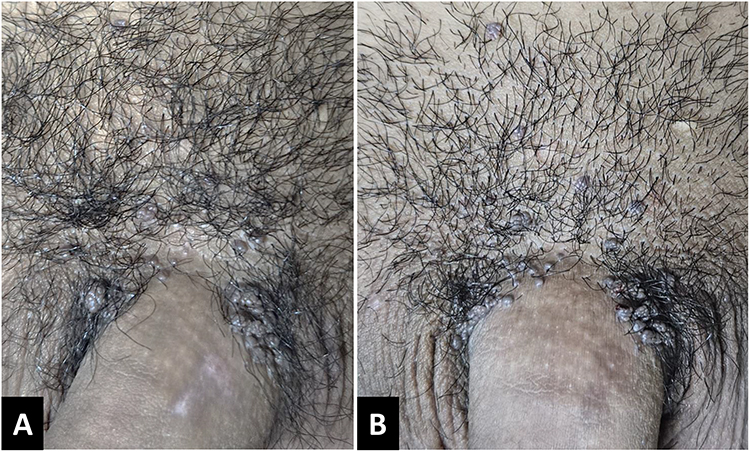 |
Figure 3 The genital warts lesion before therapy (A) and after the third subcutaneous MMR vaccine injection (B). |
 |
Figure 4 Lesions after treatment with electrocautery. |
Discussion
AGW is the most common viral infection transmitted through sexual contact,15 affecting an estimated 160–289 cases per 100,000 individuals annually worldwide. This disease poses a significant public health concern.1 AGW is most commonly found in females under 24 and males between the ages of 25 and 29.15 The significant associations between multiple HPV infections and the detection of warts include smoking more than 10 cigarettes/day, having more than five female partners, and condom use less than half the time during vaginal sex in the past 3 months. These estimates of association were higher for multiple-type infection than for single-type HPV infection.20 The patient is a male who had coitarche at 14 years old, had another sexually transmitted disease, had eight female sexual partners without condom use, and smoked about 20 cigarettes daily.
HPV is a small, double-stranded deoxyribonucleic acid (DNA) virus belonging to the Papillomaviridae family.10,21 HPV types are classified into cutaneous and mucosal, while the mucosal are divided into low-risk (non-oncogenic) and high-risk (oncogenic).11 Low-risk HPV or the cause of AGW are HPV 6, 11, 26, 30, 34, 40, 42–44, 53, 55–57, 61–63, 69, 70, 72, 73, 77, and 79–82. High-risk HPV includes oncogenic types causing oropharyngeal cancer as well as anogenital cancers such as cervical, anal, vulva, vagina, and penis cancers, consisting of HPV types 16, 18, 31, 33, 35, 39, 45, 51, 52, 54, 56, 58, 59, 65, 67, and 68.10,12 AGW is transmitted through sexual contact and is mainly caused by HPV types 6 and 11 in 95% of cases.1,13 Several types, including high-risk genotypes such as types 16 and 18, can also be detected in AGW lesions.1 Based on the PCR sequencing of the AGW tissue, HPV types 6, 11, and 16 were found, reporting the presence of high-risk HPV types of the lesions and a tendency toward the development of precancerous lesions.
Research by Wu et al in China detected the presence of low-risk HPV types 6, 11, and 42, and high-risk HPV types 16, 18, 31, 33, 52, 56, 58, 59, and 68 from the cervical swabs of 50 women with AGW.22 In another research in China, Zhu et al found that the four most prevalent HPV types causing AGW were 6, 11, 16, and 52. Detectable rates of low-risk HPV are higher than high-risk HPV types. Additionally, high-risk HPV in AGW is common and can act as reservoirs of cancer-related types.23 Research from Kuwait found that HPV type 16 was the most common genotype detected in AGW (28.2%) while type 6 was only 10.3%.9 In research conducted in the United States, the most prevalent types of HPV detected in AGW among men were types 6 (43.8%), 11 (10.7%), and 16 (9.8%).24 Another research conducted in Colombia reported that HPV type 6 was predominant in women (62%) and men (56%), with HPV type 11 at 20%. Furthermore, HPV type 16 ranked third in prevalence, with 16% of patients testing positive.8 HPV types 6, 11, and 16 are prevalent in AGW across various regions globally.23
Intralesional immunotherapy has been successfully used in the treatment of warts with the potential advantages of good efficacy, high safety profile, low recurrence rate, and clearance of untreated distant warts compared to conventional therapy.25 Different methods of immunotherapy are used to treat warts, including imiquimod, intralesional interferon, oral medications such as levamisole, cimetidine, and zinc sulfate, intralesional antigens namely Candida albicans antigen, tuberculin or purified protein derivative (PPD),26,27 Mycobacterium w, bacillus Calmette–Guérin (BCG);28 the MMR vaccine.25,29–31 The MMR vaccine injection is not routinely used to treat AGW. Several research have reported successful outcomes but larger randomized trials must be conducted to prove the effectiveness of MMR vaccine injection as a treatment for AGW. The advantages compared to other therapeutic modalities are the low recurrence rate, minimal side effects, and convenience of use.19 Mohta et al suggested that the mechanism of action was by increasing the T helper 1 (Th1) immune response, tumor necrosis factor-α (TNF-α), interleukin-2 (IL-2), IL-4, IL-5, and interferon-gamma (IFN-γ). The stimulated immune response can eliminate all lesions outside the treated lesion.16 In immunocompetent individuals, Th1 (CD4+) cells secrete various types of cytokines, including IFN-γ, IL-2, and IL-12. Additionally, IL-2 stimulates the maturation of cytotoxic T cells and increases the natural killer (NK) to eliminate virus-infected cells.32
Different research assessed and compared the effectiveness of MMR vaccines in genital and extragenital warts. In an open-label research, Sharma and Agarwal evaluated the use of a 0.5 mL MMR vaccine in 35 patients with AGW at 3-week intervals. The research found that the therapy responded in 98% of patients after 9 weeks, after the third injection.4 Meena et al reported two cases of AGW that responded to 0.5 mL intralesional injection of MMR vaccine at 3-week intervals.17 Mohta et al used 0.2–0.3 mL intralesional MMR vaccine injection for recalcitrant extragenital warts. The patient was given 0.5 mL of the injection at the largest wart at 3-week intervals for a maximum of three sessions. The results showed a complete cure within 3 weeks and the patient was given only one injection.16 Al-Qassabi et al conducted a dual-case investigation on AGW treated with the MMR vaccine. In different cases, 0.6 mL and 1.2 mL were administered to two and four lesions because of the extensive nature of the condition. Injections were administered every 2 weeks, and cryotherapy was combined with immunotherapy to boost effectiveness.19 Similarly, 0.5 mL of MMR vaccine was injected subcutaneously every 2 weeks for three sessions and the lesions were observed for 6 weeks. There was no clearance of the lesions or significant decrease in the size. We considered electrocautery for all lesions in the sixth week of observation.
An Indian research comparing intralesional and subcutaneous MMR vaccines in common warts was conducted in 2021. The result found a significant reduction in the total number of warts in both treatments. Subcutaneous MMR also promises an effective therapeutic modality in multiple warts, specifically where intralesional injection is difficult to administer. However, this is inferior to intralesional MMR for the local and distant clearance of warts.18 In the case report, the patient showed no measurable improvement in the lesions. Complete clearance was not achieved because of the short follow-up period and the inclusion of multiple HPV types. Cross-sectional research by Al-Awadhi et al reported that the likelihood of developing an AGW infected with HPV types 16, 18, 33, or 38 increased when wart persisted for a duration of 1–6 months. High-risk HPV genotypes take a longer time to clear than others.9 For further research such as cohorts can be considered to support Al-Awadhi et al hypothesis. The presence of multiple HPV infections in men at the initial assessment has been connected to HPV persistence. Therefore, coinfection with various HPV types may be developed as a significant risk factor for HPV-related cancers.20 Previous research showed that the duration of warts also influenced the clinical response to MMR immunotherapy. A higher clearance rate was found in warts that had a duration of less than 6 months. A lower clearance rate was found in warts present for more than 2 years.33 This patient had an AGW for more than 6 months, which might be a factor influencing the unresponsiveness to immunotherapy.
The recurrence rate of AGW is quite high (25–65%) but very low for immunotherapy. Previous research reported that the recurrence rate in AGW treated with MMR vaccine injection was low (6.45%) after 6 months of therapy.34 The lesions did not recur during the 6-month observation period.
Conclusion
In conclusion, the effectiveness of MMR immunotherapy in the patient was unfavorable due to the inclusion of oncogenic HPV type 16, which resulted in prolonged infection and a poor immune response. In cases of AGW treated with immunotherapy, PCR testing identified the HPV genotype since the method influenced therapeutic response.
Ethics Statement
The publication of images was included in the consent of patients for the publication of the case. Institutional approval was obtained to publish the case details from Dr. Hasan Sadikin Hospital Ethical Committee with ethical approval number DP.04.03/D.XIV.6.5/375/2024.
Consent Statement
The authors obtained all appropriate patient consent forms. The patient signed a consent form for the publication of case details and images.
Acknowledgments
The authors would like to thank the staff of the Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gilson R, Nugent D, Werner RN, Ballesteros J, Ross J. 2019 IUSTI‐Europe guideline for the management of anogenital warts. J Eur Acad Dermatol Venereol. 2020;34(8):1644–1653. doi:10.1111/jdv.16522
2. Golušin Z. Genital warts: new approaches to the treatment/Genitalne bradavice-novi pristupi u lečenju. Serbian J Dermatology Venereol. 2009;1(3):107–114. doi:10.2478/v10249-011-0010-3
3. Altaha L. Evaluation of podophyllin and trichloroacetic acid for the treatment of genital warts in Iraqi female patients. Al-Kindy Coll Med J. 2022;18(1):65–67. doi:10.47723/kcmj.v18i1.276
4. Sharma S, Agarwal S. Intralesional immunotherapy with measles mumps rubella vaccine for the treatment of anogenital warts: an open-label study. J Clin Aesthet Dermatol. 2020;13(8):40.
5. Ratnasari DT. Kondiloma Akuminata. J Ilm Kedokt Wijaya Kusuma. 2018;5(2):18–21. doi:10.30742/jikw.v5i2.336
6. Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1.
7. Bhatia N, Lynde C, Vender R, Bourcier M. Understanding genital warts: epidemiology, pathogenesis, and burden of disease of human papillomavirus. J Cutan Med Surg. 2013;17(6_suppl):S47–54.
8. Hernandez-Suarez G, Pineros M, Vargas JC, et al. Human papillomavirus genotypes in genital warts in Latin America: a cross-sectional study in Bogota, Colombia. Int J STD AIDS. 2013;24(7):567–572. doi:10.1177/0956462412474538
9. Al-Awadhi R, Al-Mutairi N, Albatineh AN, Chehadeh W. Association of HPV genotypes with external anogenital warts: a cross sectional study. BMC Infect Dis. 2019;19(1):375. doi:10.1186/s12879-019-4005-4
10. Kombe AJ, Li B, Zahid A, et al. Epidemiology and burden of human papillomavirus and related diseases, molecular pathogenesis, and vaccine evaluation. Front Public Health. 2021;8:552028. doi:10.3389/fpubh.2020.552028
11. Mlynarczyk-Bonikowska B, Rudnicka L. HPV infections—classification, pathogenesis, and potential new therapies. Int J Mol Sci. 2024;25(7616):7616. doi:10.3390/ijms25147616
12. Gross G. Genitoanal human papillomavirus infection and associated neoplasias. In: Human Papillomavirus. Karger Publishers; 2014:98–122.
13. Winer RL, Koutsky LA. Genital human papillomavirus infection. In: Holmes KK, Sparling PF, Stamm WE, Piot P, Wasserheit JN, Cory L, editors. Sexually Transmitted Disease.
14. Özkaya DB, Erfan G, Çıtamak B. The Effectiveness of Genital Wart Treatments. J Urol Surg. 2023.10:179–188.
15. Akhavan S, Mousavi A, Modaresgilani M, Alibakhshi A. Genital Warts (Anogenital warts). J Obstet Gynecol Cancer Res. 2022;2(1):1.
16. Mohta A, Kushwaha RK, Agrawal A, Sharma MK, Gautam U, Jain SK. Evaluation of the efficacy of intralesional measles, mumps, and rubella vaccine with intralesional vitamin D3 as immunotherapies in the treatment of recalcitrant cutaneous warts in adult-A randomized placebo-controlled study. Indian Dermatol Online J. 2021;12(6):879. doi:10.4103/idoj.IDOJ_573_20
17. Meena D, Sharma S, Chauhan P. Measles, mumps, and rubella vaccine in genital warts: a case report of two patients. Indian J Sex Transm Dis AIDS. 2018;39(2):133. doi:10.4103/ijstd.IJSTD_44_16
18. Saha A, Bahalia I, Agarwal S, Banerjee A, Bandyopadhyay D. Comparison of effectiveness and safety of immunotherapy of warts with intralesional versus subcutaneous MMR vaccine: an open label randomized, parallel group, clinical trial. Indian J Dermatol. 2022;67(2):99. doi:10.4103/ijd.ijd_960_21
19. Al-Qassabi AM, Al-Farsi F. Intralesional measles-mumps-rubella vaccine for genital warts: report of two cases with a review of literature. Sultan Qaboos Univ Med J. 2022;22(3):413. doi:10.18295/squmj.6.2021.093
20. Nielson CM, Harris RB, Flores R, et al. Multiple-type human papillomavirus infection in male anogenital sites: prevalence and associated factors. Cancer Epidemiol Biomarkers Prev. 2009;18(4):1077–1083. doi:10.1158/1055-9965.EPI-08-0447
21. Yanofsky VR, Patel RV, Goldenberg G. Genital warts: a comprehensive review. J Clin Aesthet Dermatol. 2012;5(6):25.
22. Wu X-L, Zhang C-T, Zhu X-K, Wang Y-C. Detection of HPV types and neutralizing antibodies in women with genital warts in Tianjin City, China. Virol Sin. 2010;25(1):8–17. doi:10.1007/s12250-010-3078-4
23. Zhu C, Wang Y, Mao W, Zhang H, Ma J. Prevalence and distribution of HPV types in genital warts in Xi’an, China: a prospective study. BMJ Open. 2019;9(5):1–6. doi:10.1136/bmjopen-2018-023897
24. Anic GM, Lee J, Stockwell H, et al. Incidence and human papillomavirus (HPV) type distribution of genital warts in a multinational cohort of men: the HPV in men study. J Infect Dis. 2011;204(12):1886–1892. doi:10.1093/infdis/jir652
25. Ju HJ, Park HR, Kim JY, Kim GM, Bae JM, Lee JH. Intralesional immunotherapy for non-genital warts: a systematic review and meta-analysis. Indian J Dermatol Venereol Leprol. 2022;88:724–737. doi:10.25259/IJDVL_1369_20
26. Achdiat PA, Antariksa NC, Rowawi R, et al. Success of intralesional purified protein derivative immunotherapy in the treatment of anogenital warts: a case report. J Exp Pharmacol. 2022;Volume 14:131–135. doi:10.2147/JEP.S347241
27. Achdiat PA, Suwarsa O, Hidayat YM, et al. Efficacy and safety profile of tuberculin protein purified derivative injection as immunotherapy for the treatment of cutaneous and anogenital warts: a review article. ImmunoTargets Ther. 2024;Volume 13:123–150. doi:10.2147/ITT.S446938
28. Achdiat PA, Suwarsa O, Hidayat YM, et al. Successful treatment of anogenital warts with single dose Bacillus Calmette Guerin vaccine without prior sensitization in tuberculosis endemic country: two case report. Hum Vaccin Immunother. 2023;19(1):2187591. doi:10.1080/21645515.2023.2187591
29. Othman NE, Safan FA. Immunotherapy for the treatment of female anogenital wart with purified protein derivative and measles mumps rubella vaccine: a comparative clinical and immunological study. J Pharm Negat Results. 2023;2023:640–649.
30. Aldahan AS, Mlacker S, Shah VV, et al. Efficacy of intralesional immunotherapy for the treatment of warts: a review of the literature. Dermatol Ther. 2016;29(3):197–207. doi:10.1111/dth.12352
31. Achdiat PA, Yunitasari, Usman HA, Maharani RH. Case of genital and extragenital warts unresponsive to immunotherapy using measles, mumps, rubella vaccine. Int Med Case Rep J. 2023;16:739–746. doi:10.2147/IMCRJ.S426665
32. Rezai MS, Ghasempouri H, Marzidareh OA, Cherati JY, Rokni GR. Intralesional injection of the measles-mumps-rubella vaccine into resistant palmoplantar warts: a randomized controlled trial. Iran J Med Sci. 2019;44(1):10. doi:10.1002/path.4496
33. Na CH, Choi H, Song SH, Kim MS, Shin BS. Two‐year experience of using the measles, mumps and rubella vaccine as intralesional immunotherapy for warts. Clin Exp Dermatol. 2014;39(5):583–589. doi:10.1111/ced.12369
34. Nofal AA, Elkholy BM, Abd-Elmonsef ER, Nofal HO. Triple intralesional antigen immunotherapy versus monoantigen in the treatment of multiple recalcitrant warts. Dermatol Ther. 2022;12(5):1225–1237. doi:10.1007/s13555-022-00725-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Case of Genital and Extragenital Warts Unresponsive to Immunotherapy Using Measles, Mumps, Rubella Vaccine
Achdiat PA, Yunitasari, Usman HA, Maharani RH
International Medical Case Reports Journal 2023, 16:739-746
Published Date: 15 November 2023
Efficacy and Safety Profile of Tuberculin Protein Purified Derivative Injection As Immunotherapy For the Treatment of Cutaneous and Anogenital Warts: A Review Article
Achdiat PA, Suwarsa O, Hidayat YM, Shafiee MN, Dwiyana RF, Hindritiani R, Sutedja E, Pudjiati SR, Hilmanto D, Dhamayanti M, Parwati I, Maharani RH, Sutedja EK, Avriyanti E, Yunitasari
ImmunoTargets and Therapy 2024, 13:123-150
Published Date: 5 March 2024
Complete Regression of Anogenital Warts Following Intralesional Measles-Mumps-Rubella (MMR) Vaccine: A Case of Two
Achdiat PA, Dwigunasari PR, Suwarsa O, Tsaqilah L, Maharani RH
Clinical, Cosmetic and Investigational Dermatology 2025, 18:2119-2125
Published Date: 1 September 2025