Back to Journals » Infection and Drug Resistance » Volume 16
The New Changes of Epidemiology, Etiology, and Clinical Characteristics of Pyogenic Liver Abscesses: A Retrospective Study in a Hospital in Northern China
Received 21 April 2023
Accepted for publication 15 June 2023
Published 22 June 2023 Volume 2023:16 Pages 4013—4023
DOI https://doi.org/10.2147/IDR.S416860
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
JinHua Cui,1 YaMan Liu,2 Jian Li1
1Department of Hepatobiliary Surgery, Affiliated Hospital of Chengde Medical College, Chengde City, Hebei Province, People’s Republic of China; 2Department of Gynaecology, Affiliated Hospital of Chengde Medical College, Chengde City, Hebei Province, People’s Republic of China
Correspondence: Jian Li, Department of Hepatobiliary Surgery, Affiliated Hospital of Chengde Medical College, Chengde City, Hebei Province, People’s Republic of China, Tel +8615127811018, Email [email protected]
Purpose: To investigate the epidemiology, etiology, and clinical characteristics of patients with pyogenic liver abscesses (PLA) and provide guidance for clinical treatments.
Patients and Methods: A retrospective study was performed on a cohort of 402 hospitalized patients diagnosed with PLAs at the Affiliated Hospital of Chengde Medical College between January 2016 and December 2021. Patient demographics, drug sensitivity profiles, and microbiological culture results of drainage and blood samples were thoroughly analyzed to identify significant patterns or trends. Furthermore, clinical characteristics and treatments for patients with PLA were comprehensively assessed.
Results: Patients aged 50– 69 years had the highest incidence of PLA, accounting for 59.9% of all cases, and 91.5% of them had a fever. Bacterial culture analysis of the 200 patients revealed that Klebsiella pneumoniae (K. pneumoniae) was the most predominant pathogen, detected in 70.5% of cases, exhibiting an upward trend. Escherichia coli (E. coli) was the second most frequently detected pathogen, identified in 14.5% of cases, showing a downward trend. Coexisting diabetes mellitus (DM) was found to be the most common comorbidity for PLA, occurring in most patients with the condition. Patients with a history of abdominal surgery and malignancy had an increased risk for PLA, while those with gallstones had a decreased risk. Drainage combined with antibiotic therapy was identified as the primary treatment of PLA. In addition, multivariate analysis demonstrated that coexisting DM and the presence of gas in the abscess cavity were independent risk factors for septic shock in patients with PLA.
Conclusion: This study reveals a shift in the proportions of pathogens and risk factors in patients with PLA, underscoring the necessity for improved diagnostic and therapeutic strategies.
Keywords: pyogenic liver abscess, morbidity, pathogen, diabetes, Klebsiella pneumoniae
Introduction
A pyogenic liver abscess (PLA) is a severe infectious liver disease that results from the invasion of suppurative bacteria into the liver parenchyma through diverse routes, culminating in local inflammation, liquefaction necrosis, and formation of a collection of pus called an abscess.1–3 The incidence of PLAs in Asian countries has gradually increased, with a rate of 12–18 per 100,000 individuals.4 A PLA is a life-threatening condition, with reported mortality rates ranging from 3% to 20% during hospitalization.5 Klebsiella pneumoniae (K. pneumoniae) was first reported in Taiwan, China, in 1980 and has gradually become the leading agent of PLAs in Asia.6–8 This retrospective study analyzed the clinical characteristics, etiological changes, and treatment outcomes of the 402 PLA patients admitted to the Affiliated Hospital of Chengde Medical University between 2016 and 2021, To study the demographic changes, etiological changes and antibiotic sensitivity of common pathogens in PLA patients, in addition, to study risk factors for septic shock in PLA patients.
Materials and Methods
Research Subjects
A retrospective study was performed on a cohort of 402 hospitalized patients diagnosed with PLAs at the Affiliated Hospital of Chengde Medical College between January 2016 and December 2021.This study complies with the Declaration of Helsinki and was approved by the Institutional Ethics Committee.The need for informed consent was waived because of the retrospective nature of the study.
The study’s inclusion criteria were defined as follows: 1) Patients diagnosed with PLAs using imaging modalities, including computed tomography (CT), magnetic resonance imaging (MRI), or ultrasound, 2) those with symptoms such as fever, chills, and right upper abdominal pain, 3) those diagnosed with PLAs for puncture or surgery, 4) those whose blood or pus culture revealed pathogenic bacteria. Exclusion criteria involved: 1) Patients with incomplete information related to PLAs, or 2) those with amoebic, tuberculous, or parasitic liver abscesses.
Data Collection and Treatment Methods
In this study, patient demographics and clinical information, including gender, age, symptoms, laboratory and bacterial culture results, treatment modalities, complications, and length of hospital stay, were collected from medical records. The decision to proceed with percutaneous aspiration (PCA) or percutaneous catheter drainage (PCD) was guided by patient preference, the size of the suppurative liver abscess, and the response to antibiotic therapy. Generally, PCD is performed for PLA greater than 3 cm.The PCD procedure was performed under ultrasound guidance, utilizing a 10–12F pigtail catheter for drainage. Blood cultures were performed when PLA patients with a fever.Each patient was treated with antibiotics, The empirical antibiotics begun with parenteral third generation cephalosporins like cefoperazone sodium or with piperacillin tazobactam. The antibiotics were changed as per the sensitivity of the organism in the case of positive pus cultures. Patients underwent an intravenous antibiotic infusion for a minimum of 2 weeks, followed by oral administration of antibiotics for 2–4 weeks. The abdominal enhanced CT was examined 3–5 days after PCD to evaluate the therapeutic effect.Surgical intervention was recommended for patients who did not respond to antibiotics, PNA, or PCD treatment.
Pathogen Identification and Drug Susceptibility Test
After the PLA patients underwent PCA or PCD, A sterile syringe was used to extract 10mL of pus, which was placed in a culture bottle and sent for examination.For patients with fever, blood culture samples were drawn for testing.The pathogens were cultured by ALERT3D120 automatic blood culture instrument [Biomeriere Diagnostic Products (Shanghai) Co., LTD., France] and inoculated on blood plates and eosin-methylene blue plates.After 24 hours of culture, the pathogens were identified by the automatic microbial identification and drug sensitivity analysis system and the matching Gram-positive bacteria and negative bacteria identification card [Meriier Diagnostic Products (Shanghai) Co., LTD.]. Drug susceptibility test was performed by disk AGAR diffusion method (K-B method, drug susceptibility test paper and medium: Oxoid Company, UK).A drug susceptibility test paper was attached to the AGAR plate inoculated with the tested bacteria, and the growth of the tested bacteria was inhibited within the inhibitory concentration range around the paper. After incubation for 24 hours, the diameter of inhibition zone was taken by caliper, and the size of inhibition zone reflected the sensitivity of the tested bacteria to the measured drugs.
Statistical Analysis
The statistical analysis was conducted using IBM SPSS Statistics 23.0 (IBM Corp., Armonk, NY). Data were presented as frequencies and percentages. The χ2 test and t-test were employed for analyzing categorical variables and continuous variables, respectively, to determine significant differences between groups. Additionally, a logistic regression analysis was performed to examine the relationship between the incidence of septic shock and other factors.
Results
Demographics and Clinical Characteristics
In this study, for these three groups, a notable increasing trend was observed in the incident cases of PLAs. The mean age of onset for PLA was 59.02 ± 13.70 years, with a higher prevalence observed in males (n = 260, 64.7%). In the majority of cases, PLA was mainly located in the right liver lobe, and single abscesses were more commonly found. The primary symptom of the disease was fever. Other clinical characteristics of the patients are summarized in Table 1.
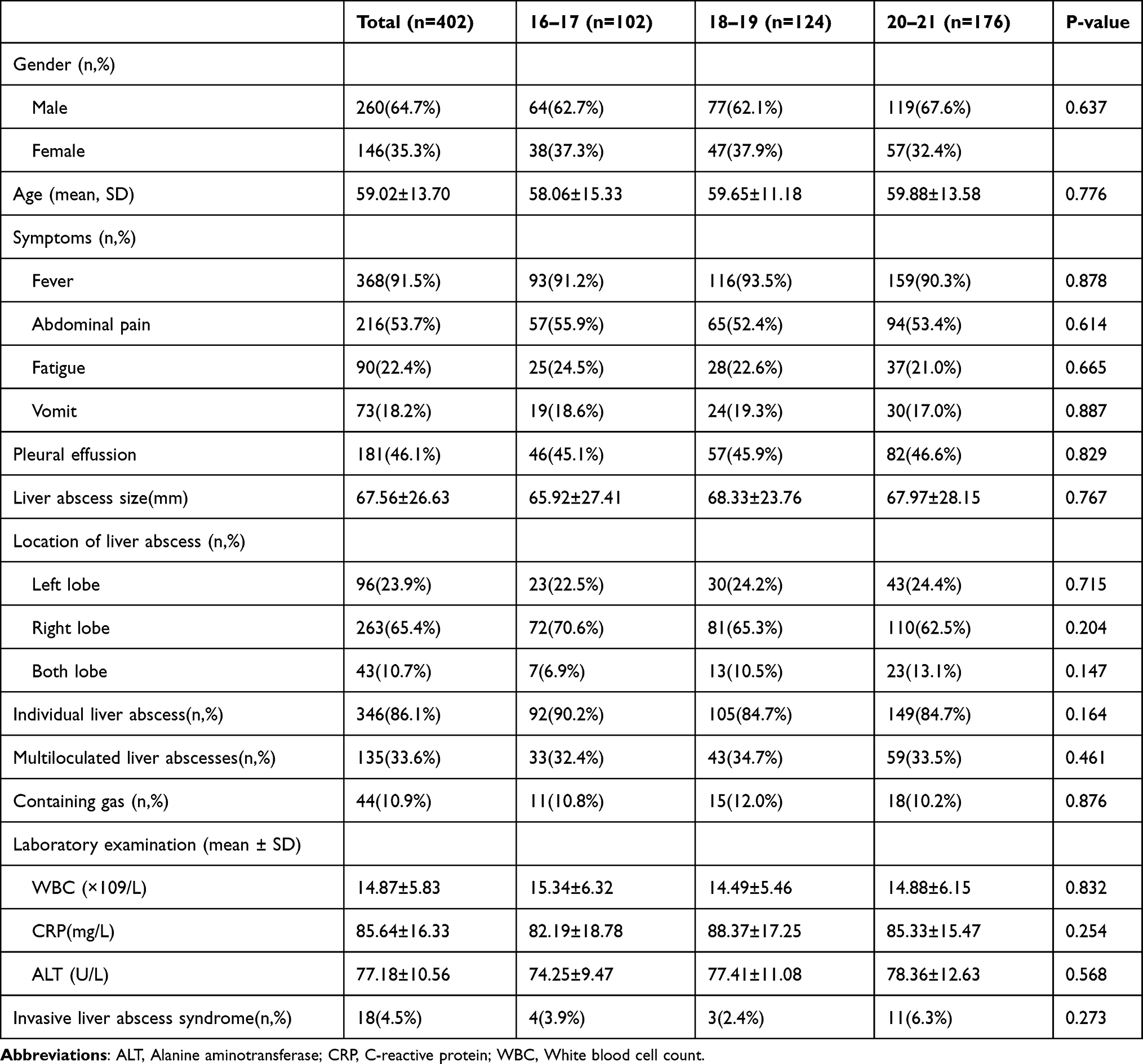 |
Table 1 Demographics and Clinical Characteristics of 402 PLA Patients |
Patients aged 50–69 years exhibited the highest incidence rate of PLAs, with a detailed distribution across other age groups shown in Figure 1.
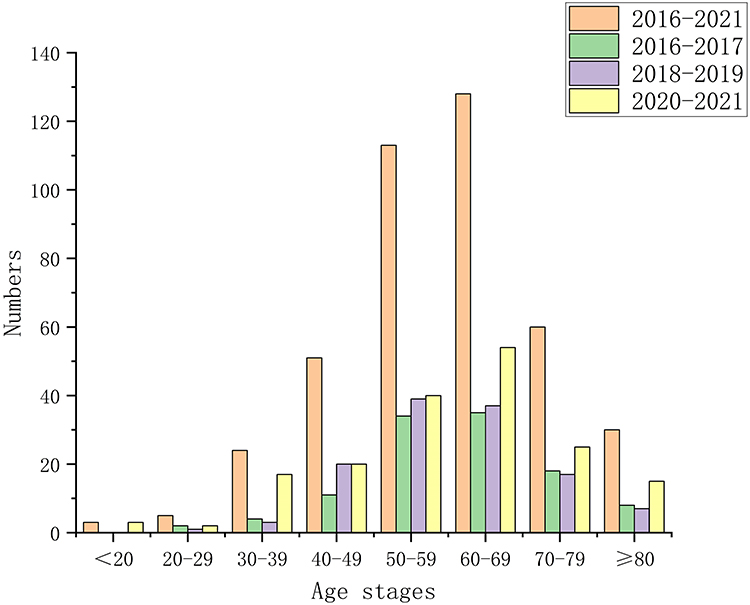 |
Figure 1 Age distribution of patients with pyogenic liver abscess. Note: Different colored columns represent patients with liver abscess at different periods. |
Comorbidities for PLAs
The predominant comorbidity for PLAs was found to be coexisting diabetes mellitus (DM), which was present in the majority of patients with the condition (n = 150, 37.3%). Patients with a history of abdominal surgery were also observed to have an increased risk of PLAs. Other common comorbidities for PLA are presented in Table 2 and Figure 2.
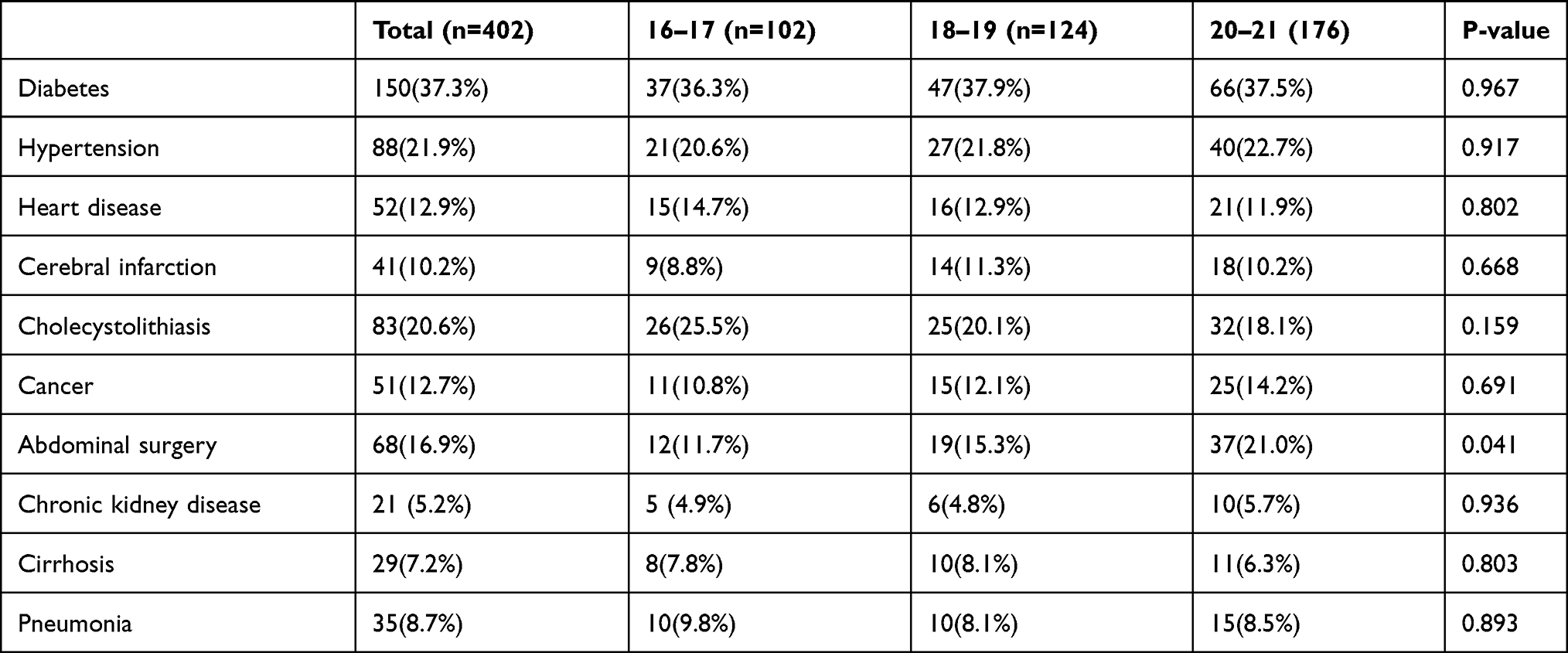 |
Table 2 Comorbidities for PLAs |
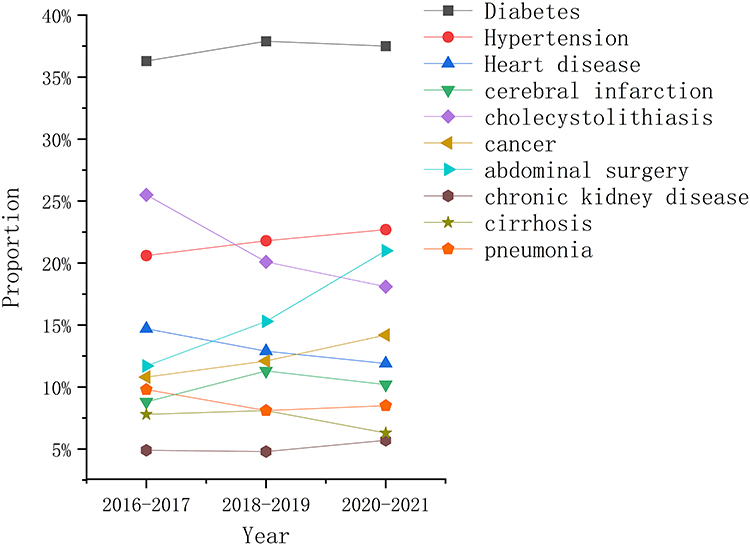 |
Figure 2 Comorbidities for PLAs. |
Etiological Changes in PLAs
Among 402 PLA patients, 200 patients (49.8%) showed positive results in pathogen culture analysis in blood or pus samples. K. pneumoniae was the predominant pathogen, accounting for 70.5% (n = 141) and exhibiting an uptrend, while E. coli was the second most detected pathogen, accounting for 14.5% (n = 29) and showing a downtrend. Other pathogens were rarely detected. The detailed results of bacterial culture are displayed in Table 3 and Figure 3.
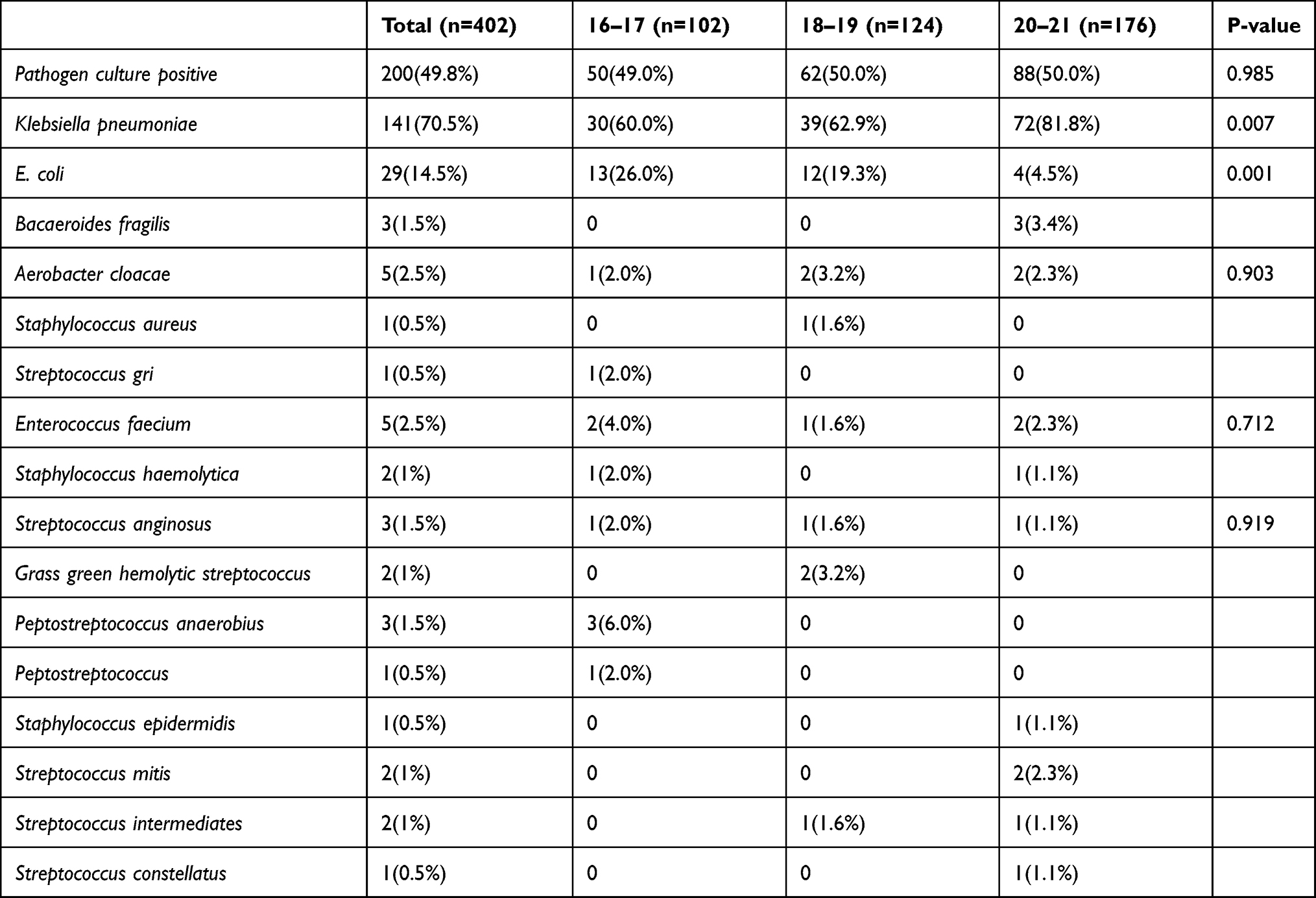 |
Table 3 Etiological Changes in PLAs |
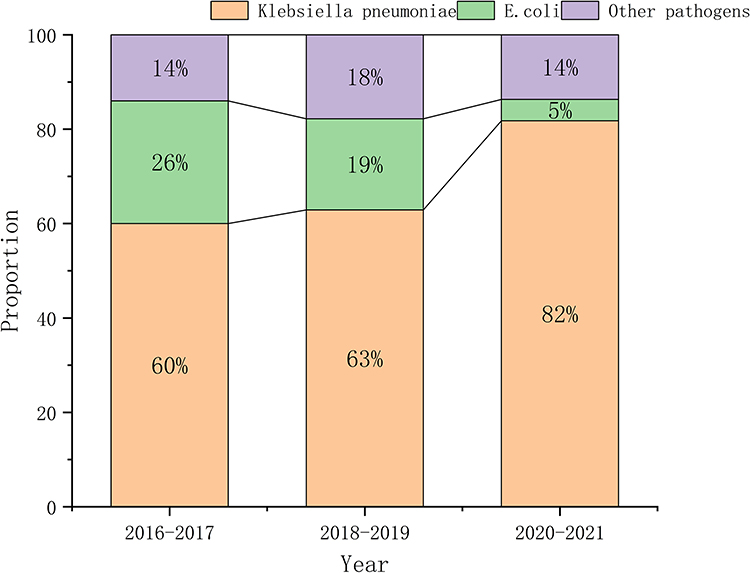 |
Figure 3 Common etiological changes in PLAs (K. pneumoniae and Escherichia coli). |
Resistance of K. pneumoniae and E. coli
Given that the bacterial cultures mostly consisted of K. pneumoniae and E. coli, a statistical analysis was undertaken to assess the antibiotic susceptibility patterns of the two bacteria (Figure 4). Notably, E. coli exhibited greater resistance to antibiotics compared with K. pneumoniae.
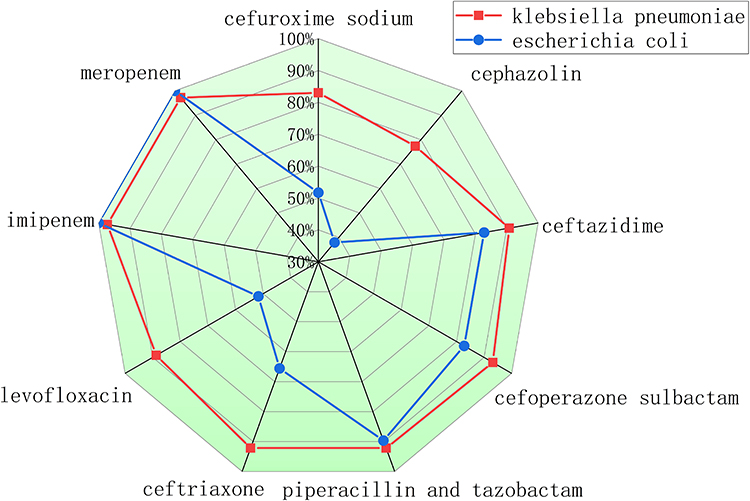 |
Figure 4 Comparison of the antibiotic susceptibility of common bacteria (K. pneumoniae and Escherichia coli). |
Treatment and Prognosis of PLA Patients
In the management of PLA, the primary therapeutic approach involved a combination of antibiotics and PCD (56.7%). The overall in-hospital mortality rate was 5.7%. Additional treatment modalities and associated complications are shown in Table 4.
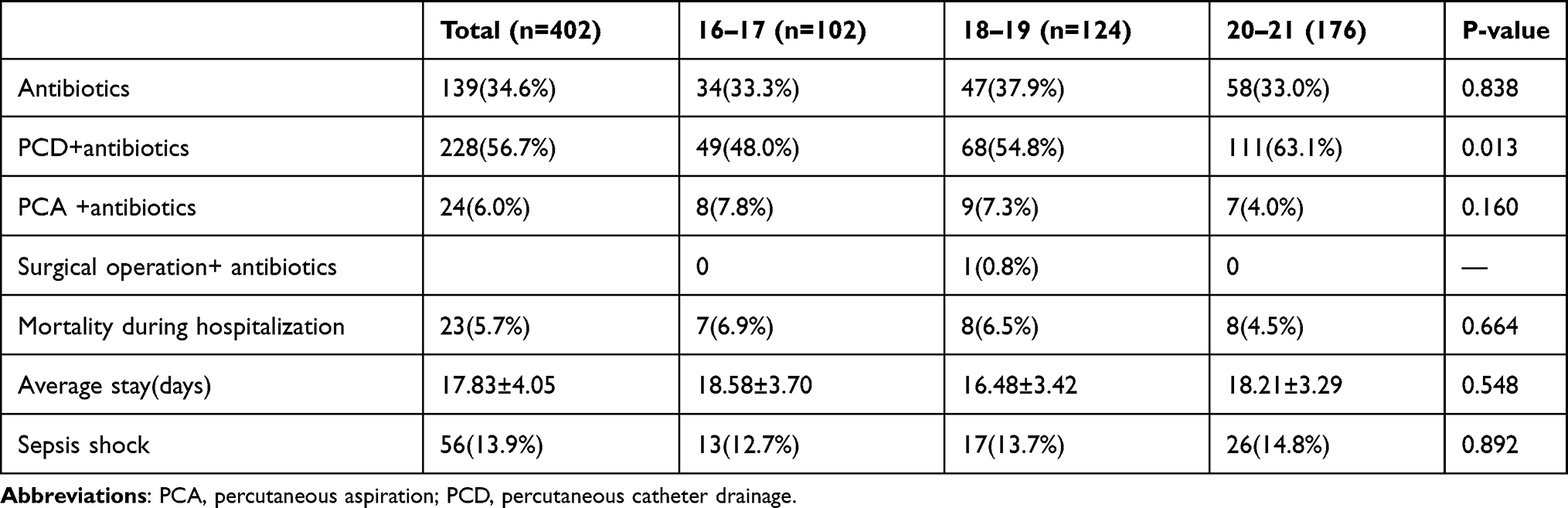 |
Table 4 Treatment and Prognosis of PLA Patients |
Risk Factors for Septic Shock
The prevalence of septic shock was determined to be 13.9%. Results of the multivariate analysis revealed that coexisting DM and the presence of gas in the abscess cavity (gas formation) were significant risk factors for septic shock (Table 5).
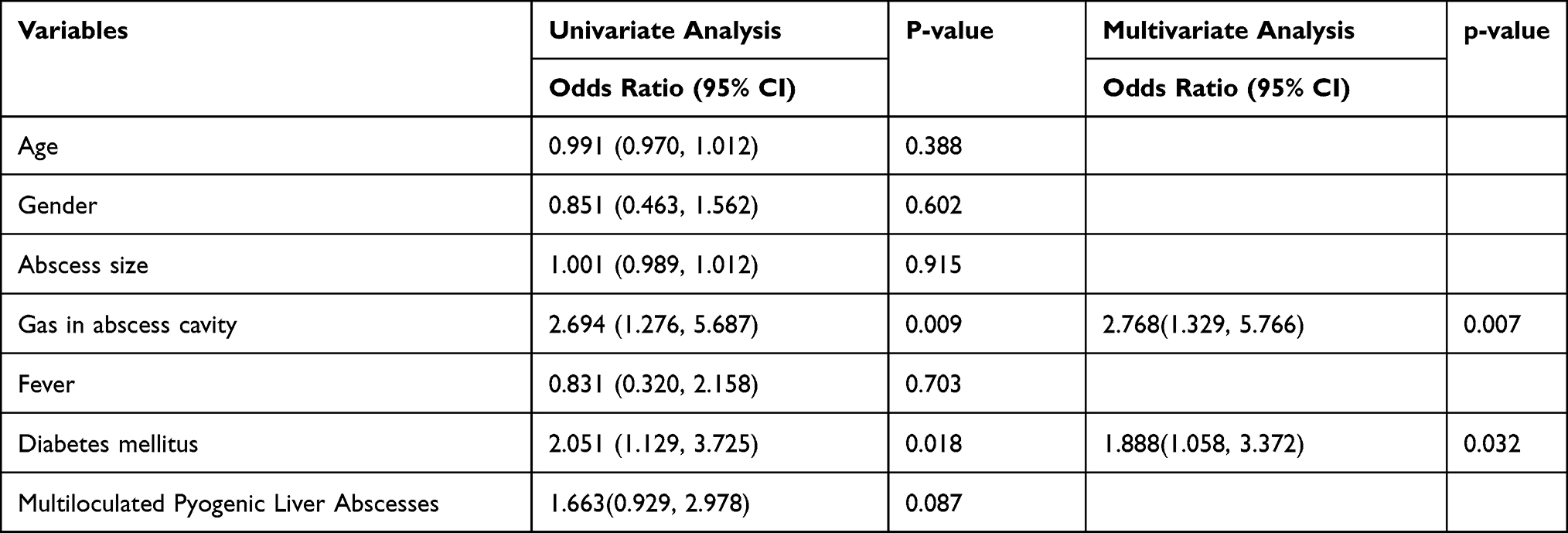 |
Table 5 Risk Factors for Septic Shock |
Discussion
A PLA is a prevalent intra-abdominal infectious disease caused by diverse bacterial species. The predominant pathogens for PLA in North America are Streptococci and E. coli, while in Asia, K. pneumoniae is the predominant pathogen.2,9–11 The management of PLAs involves antibiotic therapy, PCD, and surgical intervention, and the mortality rate has decreased with improved diagnostic and therapeutic capabilities.12 Selecting the appropriate antibiotics based on the bacterial culture results is crucial among these approaches.
This study demonstrated a rising trend in the incidence of PLAs, which is in accordance with previous reports.2,8,13 The age of onset for PLA patients tended to increase, as reported in most articles.14,15 The present study reported a mean age of onset of (59.02 ± 13.70) years, indicating a gradual increase in recent years. And advanced age is associated with increased mortality during hospitalization.16 PLAs are primarily found in the right liver lobe and more prevalent in males. Common clinical manifestations include fever and abdominal pain, consistent with the findings of previous studies by Zhang J and Wang YC.17,18
In Asia, K. pneumoniae has become the predominant pathogen causing PLAs.19,20 This study revealed a year-by-year increase in the proportion of K. pneumoniae in the pus or blood culture of PLA patients, with a significant increase to 81.8% in the last two years. Previous studies have shown that DM is the most common underlying disease in patients with K. pneumoniae liver abscesses (KPLAs).21 The higher incidence of KPLAs in DM patients may be attributed to functional abnormalities of neutrophil chemotaxis and phagocytosis. KPPLA is associated with higher overall metastatic complications but lower mortality. Lower mortality may be due to patients being younger and without underlying hepatobiliary disease or malignancy, and abscess characteristics (solitary and unilobar) permitting easier drainage.22 The detection rate of pathogens in this study was low, particularly the positive rate of pathogens in blood culture, which could be due to the administration of antibiotics before culture. Furthermore, E. coli, a less common pathogen, is becoming increasingly rare.
In this study, K. pneumoniae and E. coli were identified as the predominant contributors to PLAs. Therefore, administering empirical antibiotic therapy directed toward both bacterial species is recommended before obtaining the bacterial culture results. K. pneumoniae is intrinsically resistant to ampicillin.23 It exhibits high sensitivity to carbapenems (meropenem and imipenem), as well as to the third-generation cephalosporins, cefoperazone sodium/sulbactam sodium, and piperacillin-tazobactam, but lower sensitivity to levofloxacin and second-generation cephalosporins. E. coli, in contrast, has higher resistance to various antibiotics but is still susceptible to carbapenems, cefoperazone sodium/sulbactam sodium, piperacillin-tazobactam, and ceftazidime. Therefore, empirical treatment with cefoperazone sodium/ sulbactam sodium or piperacillin-tazobactam is recommended for newly diagnosed PLA patients in the absence of etiological evidence.24,25 In the case of treatment failure, a switch to carbapenems can be considered. However, once the results of bacterial drug sensitivity tests become available, the selection of an appropriate antibiotic therapy should be guided by the sensitivity profiles of the identified pathogens.
In this study, DM remained the prevailing comorbidity in patients with PLAs, accounting for about 37% of cases and exhibiting no significant change in recent years.26–29 Coexisting DM increases the risk of portal infection, weakens the liver’s immune response, and impairs the body’s ability to clear bacteria.30 The incidence of patients with PLAs was also observed to be elevated in patients with a history of abdominal surgery, particularly hepatobiliary and pancreatic procedures, which is thought to result from changes in the microbiome and intestinal barrier, as well as a compromised immune system.31 Moreover, vascular and biliary tract damage increases the risk of developing PLAs, and hypertension and malignancy have emerged as additional risk factors. Although combined biliary stones were once a notable contributor to the occurrence of PLAs, their incidence has decreased in recent years.
In recent years, the preferred approach for treating PLAs has shifted from surgical drainage to a combination of antibiotic therapy and PCD, as indicated by current literature.32,33 PCD has demonstrated comparable cure rates to surgical drainage, with the additional benefits of reduced trauma, fewer complications, and shorter hospital stays. Treatment with intravenous antibiotics is also a crucial aspect of management, with the duration of treatment ranging from two to six weeks, depending on the patient’s response.34
The results of this study revealed that 13.9% of the patients suffered from septic shock, which is consistent with previous reports.35–37 There has been no significant change in the incidence of septic shock over several years. Multivariate analysis identified coexisting DM and gas formation as risk factors for septic shock in PLA patients. K. pneumoniae is the most common pathogen isolated from patients with DM, and its aggressive nature weakens the liver’s ability to remove bacteria. The larger diameter of the liver abscess or a history of biliary surgery increases the risk of septic shock in gas-forming PLAs. The accumulation of gas impedes the transport of gases and nutrients, leading to local tissue damage and abscess formation.36 However, the results in some manuscripts suggesting that gas formation increases septic shock are inconclusive and need to be proved by further prospective studies.38 Healthcare providers should be cautious about the possibility of septic shock in patients with PLAs associated with DM or gas formation.
Conclusion
In these years, the demographics of PLA patients in northern China have undergone certain changes. There has been an increase in the number of patients with a history of abdominal surgery. K. pneumoniae has emerged as the most common pathogen, with the incidence of PLA caused by K. pneumoniae showing a rising trend, while that caused by E. coli has shown a decreasing trend. DM and gas formation as risk factors for septic shock in PLA patients.These shifts in pathogen prevalence highlight the need for improved diagnostic and therapeutic strategies.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval
Written informed consent for data use was obtained from all patients.This study was approved by the Ethics Committee of the Affiliated Hospital of Chengde Medical College.
Acknowledgments
We appreciate the linguistic assistance provided by TopEdit (www.topeditsci.com) in the preparation of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by a grant from the Chengde Municipal Science and Technology Plan Project (No.202204A076).
Disclosure
All authors declare that they have no conflict of interest.
References
1. Jepsen P, Vilstrup H, Schønheyder HC, et al. A nationwide study of the incidence and 30-day mortality rate of pyogenic liver abscess in Denmark, 1977–2002. Aliment Pharmacol Ther. 2005;21(10):1185–1188. doi:10.1111/j.1365-2036.2005.02487.x
2. Liisa M, Myers Robert P, James H, et al. A population-based study of pyogenic liver abscesses in the United States: incidence, mortality, and temporal trends. Am J Gastroenterol. 2010;105(1):117–124. doi:10.1038/ajg.2009.614
3. Losie Jennifer A, Lam John C, Gregson Daniel B, et al. Epidemiology and risk factors for pyogenic liver abscess in the Calgary Health Zone revisited: a population-based study. BMC Infect Dis. 2021;21(1):939. doi:10.1186/s12879-021-06649-9
4. Laupland Kevin B, Church Deirdre L, Melissa M, et al. Population-based study of the epidemiology of and the risk factors for invasive staphylococcus aureus infections. J Infect Dis. 2003;187(9):1452–1459. doi:10.1086/374621
5. Cristina S, Chiara E, Christian B, et al. Characteristics and management of pyogenic liver abscess: a European experience. Medicine. 2018;97(19):e0628. doi:10.1097/MD.0000000000010628
6. Hairui W, Yue R, Zhihui C, et al. The increased recurrence rate of liver abscess caused by extended-spectrum β-lactamase-producing Klebsiella pneumoniae. Eur J Clin Microbiol Infect Dis. 2020;39(7):1315–1320. doi:10.1007/s10096-020-03848-1
7. Siqin Z, Xiucai Z, Qing W, et al. Klebsiella pneumoniaeClinical, microbiological, and molecular epidemiological characteristics of -induced pyogenic liver abscess in southeastern China. Antimicrob Resist Infect Control. 2019;8(1):166. doi:10.1186/s13756-019-0615-2
8. Herwig C. Pyogenic liver abscess: differences in etiology and treatment in Southeast Asia and Central Europe. World J Gastroenterol. 2010;16(20):2458–2462.
9. Yun L, Ji-Yao W, Wei J. An increasing prominent disease of Klebsiella pneumoniae liver abscess: etiology, diagnosis, and treatment. Gastroenterol Res Pract. 2013;2013:258514. doi:10.1155/2013/258514
10. Jai Hoon Y, Youn Jeong K, Yoon Hee J, et al. Liver abscess due to Klebsiella pneumoniae: risk factors for metastatic infection. Scand J Infect Dis. 2014;46(1):21–26. doi:10.3109/00365548.2013.851414
11. Yun Q, Chi Chun W, Sanchuan L, et al. A retrospective study of pyogenic liver abscess focusing on Klebsiella pneumoniae as a primary pathogen in China from 1994 to 2015. Sci Rep. 2016;6(1):38587. doi:10.1038/srep38587
12. Wenfei L, Hongjie C, Shuai W, et al. A comparison of pyogenic liver abscess in patients with or without diabetes: a retrospective study of 246 cases. BMC Gastroenterol. 2018;18(1):144. doi:10.1186/s12876-018-0875-y
13. Tony P, Thomas F, Jaswinder S, et al. Pyogenic liver abscess: an audit of 10 years’ experience. World J Gastroenterol. 2011;17(12):1622–1630. doi:10.3748/wjg.v17.i12.1622
14. Zhang J, Zhaoqing D, Jianbin B, et al. Comparison of clinical characteristics and outcomes of pyogenic liver abscess patients < 65 years of age versus ≥ 65 years of age. BMC Infect Dis. 2019;19(1):233. doi:10.1186/s12879-019-3837-2
15. Law S-T, Li KK. Older age as a poor prognostic sign in patients with pyogenic liver abscess. Int J Infect Dis. 2013;17(3):e177–e184. doi:10.1016/j.ijid.2012.09.016
16. Chan KS, Junnarkar SP, Low JK, et al. Aging is associated with prolonged hospitalisation stay in pyogenic liver abscess-a 1:1 propensity score matched study in elderly versus non-elderly patients. Malays J Med Sci. 2022;29(5):59–73. doi:10.21315/mjms2022.29.5.7
17. Zhang J, Gao Y, Du Z, et al. Clinical features and prognosis of gas-forming and non-gas-forming pyogenic liver abscess: a comparative study. Surg Infect. 2021;22(4):427–433. doi:10.1089/sur.2020.245
18. Wang YC, Yang KW, Lee TP, et al. Increased risk of pyogenic liver abscess in patients with alcohol intoxication: a population-based retrospective cohort study. Alcohol. 2017;64:23–28. doi:10.1016/j.alcohol.2017.05.003
19. Ping-Feng W, Yea-Yuan C, Yi-Tsung L, et al. Clinical characteristics and economic consequence of Klebsiella pneumoniae liver abscess in Taiwan. J Microbiol Immunol Infect. 2015;48(2):190–197. doi:10.1016/j.jmii.2013.08.014
20. Feng-Chiao T, Yu-Tsung H, Luan-Yin C, et al. Pyogenic liver abscess as endemic disease, Taiwan. Emerg Infect Dis. 2008;14(10):1592–1600. doi:10.3201/eid1410.071254
21. Ning-Ping F, Kuo-Tai C, Hung-Jung L, et al. Characteristics of pyogenic liver abscess patients with and without diabetes mellitus. Am J Gastroenterol. 2010;105(2):328–335. doi:10.1038/ajg.2009.586
22. Chan KS, Chia CTW, Shelat VG. Demographics, radiological findings, and clinical outcomes of Klebsiella pneumonia vs. non-Klebsiella pneumoniae pyogenic liver abscess: a systematic review and meta-analysis with trial sequential analysis. Pathogens. 2022;11(9):976. doi:10.3390/pathogens11090976
23. Shelat Vishal G, Qiao W, Chia Clement L, et al. Patients with culture negative pyogenic liver abscess have the same outcomes compared to those with Klebsiella pneumoniae pyogenic liver abscess. Hepatobiliary Pancreat Dis Int. 2016;15(5):504–511. doi:10.1016/S1499-3872(16)60127-3
24. Lee C, Lee JH, Park KS, Jeon JH. Klebsiella pneumoniae antimicrobial resistance of hypervirulent: epidemiology, hypervirulence-associated determinants, and resistance mechanisms. Front Cell Infect Microbiol. 2017;7:483. doi:10.3389/fcimb.2017.00483
25. Moore R, O’Shea D, Geoghegan T, et al. Community-acquired Klebsiella pneumoniae liver abscess: an emerging infection in Ireland and Europe. Infection. 2013;41(3):681–686. doi:10.1007/s15010-013-0408-0
26. Fei W, Jingwen Y, Wenjie C, et al. Clinical characteristics of diabetes complicated by bacterial liver abscess and nondiabetes-associated liver abscess. Dis Markers. 2022;2022:7512736. doi:10.1155/2022/7512736
27. Dalong Y, Changyong J, Shugeng Z, et al. Clinical characteristics and management of 1572 patients with pyogenic liver abscess: a 12-year retrospective study. Liver Int. 2021;41(4):810–818. doi:10.1111/liv.14760
28. Jeong-Ju. Y, Tae Kyu L, Dae-Sung. K, et al. A population-based study of pyogenic liver abscess in Korea: incidence, mortality and temporal trends during 2007–2017. Liver Int. 2021;41(11):2747–2758. doi:10.1111/liv.15034
29. Kim J-K, Chung DR, Wie SH, et al. Risk factor analysis of invasive liver abscess caused by the K1 serotype Klebsiella pneumoniae. Eur J Clin Microbiol Infect Dis. 2009;28:109–111.
30. Gonzalez-Regueiro JA, Moreno-Castaneda L, Uribe M, et al. The role of bile acids in glucose metabolism and their relation with diabetes. Ann Hepatol. 2017;16(Suppl. 1: s3–105):16–21. doi:10.5604/01.3001.0010.5672
31. Wen C, Tao M, Xueli B, et al. Pyogenic liver abscess after pancreaticoduodenectomy: a single-center experience. J Surg Res. 2019;239:67–75. doi:10.1016/j.jss.2018.12.004
32. Lee CH, Jo HG, Cho EY, et al. Maximal diameter of liver abscess independently predicts prolonged hospitalization and poor prognosis in patients with pyogenic liver abscess. BMC Infect Dis. 2021;21(1):171. doi:10.1186/s12879-021-05873-7
33. Du ZQ, Zhang LN, Lu Q, et al. Clinical characteristics and outcome of pyogenic liver abscess with different size: 15-year experience from a single center. Sci Rep. 2016;6(1):35890. doi:10.1038/srep35890
34. JinHua C, YaMan L, Jian L. Double pigtail tube drainage for large multiloculated pyogenic liver abscesses. Front Surg. 2023;9:1106348. doi:10.3389/fsurg.2022.1106348
35. Hyunyoung C, Eu Sun L, Yoon-Seon L, et al. Predictors of septic shock in initially stable patients with pyogenic liver abscess. Scand J Gastroenterol. 2017;52(5):589–594. doi:10.1080/00365521.2017.1288757
36. Kong H, Yu F, Zhang W, et al. Clinical and microbiological characteristics of pyogenic liver abscess in a tertiary hospital in East China. Medicine. 2017;96(37):e8050. doi:10.1097/MD.0000000000008050
37. Juanita P-E, Wagner R-Q, Daniel Alejandro C-R, et al. Increased incidence of and microbiologic changes in pyogenic liver abscesses in the Mexican population. World J Hepatol. 2020;12(10):816–828. doi:10.4254/wjh.v12.i10.816
38. Thng CB, Tan YP, Shelat VG. Gas-forming pyogenic liver abscess: a world review. Ann Hepatobiliary Pancreat Surg. 2018;22(1):11–18. doi:10.14701/ahbps.2018.22.1.11
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.