Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
The Neural Correlates of the Social Perception Dysfunction in Schizophrenia: An fMRI Study
Authors Gao X ![]() , Huang Z, Li J, Zhou Z
, Huang Z, Li J, Zhou Z ![]() , Zhou H
, Zhou H
Received 14 June 2023
Accepted for publication 10 August 2023
Published 21 August 2023 Volume 2023:19 Pages 1799—1808
DOI https://doi.org/10.2147/NDT.S425926
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yu-Ping Ning
Xuezheng Gao,1 Zixuan Huang,2 Jiangjuan Li,3 Zhenhe Zhou,1,3 Hongliang Zhou4
1Department of Psychiatry, The Affiliated Wuxi Mental Health Center of Nanjing Medical University, Wuxi City, 214151, People’s Republic of China; 2Department of Music and Wellbeing, School of Music, University of Leeds, Leeds City, UK; 3Department of Psychiatry, The Affiliated Mental Health Center of Jiangnan University, Wuxi City, 214151, People’s Republic of China; 4Department of Psychology, The Affiliated Hospital of Jiangnan University, Wuxi City, 214151, People’s Republic of China
Correspondence: Zhenhe Zhou, Department of Psychiatry, The Affiliated Wuxi Mental Health Center of Nanjing Medical University, Wuxi City, 214151, People’s Republic of China, Tel +86-13358118986, Fax +86-510-83219366, Email [email protected] Hongliang Zhou, Department of Psychology, The Affiliated Hospital of Jiangnan University, Wuxi City, 214151, People’s Republic of China, Tel +86-18341654302, Fax +86-510-85808820, Email [email protected]
Purpose: Patients with schizophrenia show deficits in facial emotion recognition and emotional intensity assessment, and also exhibit structural and functional irregularities in specific brain regions. In this study, we aimed to examine differences in active brain regions involved in processing the Emotion Intensity Recognition Task (EIRT), which can serve as an indicator of emotion recognition and ability to perceive intensity, between patients with schizophrenia and healthy controls (HCs). The purpose of this study was to investigate dysfunctional brain regions and investigate the role of the amygdala in social cognition deficits in patients with schizophrenia by focusing on alterations in amygdala activity linked to facial emotion recognition.
Participants and Methods: Twenty-two patients who met a diagnostic criteria for schizophrenia according to DSM-IV and 27 HCs participated in an MRI scan while completing the EIRT. Behavioral and MRI data were collected and analyzed.
Results: Behavioral results showed that patients with schizophrenia made significantly more errors in recognizing surprise, happiness, sadness, fear, and neutral expressions, and patients with schizophrenia exhibited significantly slower response times in recognizing happy facial expressions. Imaging results showed that schizophrenia patients found hypoactivation in several inferior parietal and temporal regions, in the cerebrum and anterior cingulate; and decreased amygdala activation in individuals with schizophrenia was associated with impaired recognition of fear in facial expressions.
Conclusion: Facial emotion processing deficits are emotion-specific (surprise, happiness, sadness, fear, and neutral expressions) in schizophrenia. Hypoactivation in several inferior parietal and temporal regions, in the cerebrum and anterior cingulate, was thought to contribute to symptom formation in schizophrenia. Reduction in amygdala activation in schizophrenia patients was associated with impairment of the fear-emotional process.
Keywords: schizophrenia, social cognition, functional magnetic resonance imaging, emotion, facial affect recognition, amygdala
Introduction
Schizophrenia is a serious and complex mental disorder, which has a lifetime prevalence of about 1%, causing great pain to patients and accounting for a huge health care burden.1 Schizophrenia patients suffer from positive symptoms including delusions and hallucinations, negative symptoms, such as amotivation and social withdrawal, and significant cognitive deficits.2 Social cognitive dysfunction, especially deficits in emotion perception, is one of the core features of schizophrenia and strongly predicts functional outcomes, such as employment, relationships, and independent living.3 In addition, it has reached a general consensus that schizophrenia alters the way the brain processes emotional material, such as facial expressions, body gestures, verbal information, behavior, text and physiological signal recognition, etc.2 Many years ago, Bleuler found that disturbance of emotion was one of the important features of schizophrenia patients.3 Empirical studies have consistently shown that schizophrenia patients perform poorly in emotion recognition.4 Functional magnetic resonance imaging (fMRI) studies have reported various patterns of brain activation abnormalities during facial emotion perception in patients with schizophrenia.5 Affective neuroscience research has shown that amygdala disturbances play an important role in emotional processing deficits in schizophrenia patients. However, the precise role of this brain region in various forms of facial emotion remains unclear.6
Since the humankind’s primary emotions, including anger, happiness, surprise, fear, disgust, and sadness, can be signaled by various facial expressions, recognizing primary facial expressions is a fundamental brain ability for social communication.7 Facial emotion recognition is a key component of social cognition and plays a crucial role in interpersonal relationships. The Emotion Intensity Recognition Task (EIRT) can be used to evaluate facial emotion recognition of neutral, positive (happiness/surprise) and negative emotions (fear/sadness/disgust/anger) of different intensities.8 Decades of researches have suggested that patients with schizophrenia struggle with recognizing basic facial emotions and evaluating their intensities.9 However, there is a lack of consistency in reporting which categories of emotions schizophrenia patients find difficult to recognize. While some studies suggest impaired recognition of negative emotions, such as sadness and fear.10,11 Other evidence suggests that individuals with schizophrenia also struggle with recognizing neutral and happy emotions.12
The amygdala is a brain region associated with processing emotional recognition, and its structural and functional anomalies are believed to underlie social cognitive deficits in individuals with mental illnesses. Over the past few years, researches have accumulated supporting the role of the human amygdala in facilitating cortex processing emotion-laden images.13 Researches have shown that the amygdala, along with a significant limitation in activation in a “social brain” system that includes the ventral temporal-basal ganglia-prefrontal cortex, may play a central role in patients’ difficulties when processing facial emotions.14 Evidence of hypoactivation of the amygdala during the processing of negative facial emotions have been found in some, but not all, imaging studies.15,16
Therefore, both functional abnormalities of the amygdala and poor emotion recognition performance have been documented in patients with schizophrenia. Therefore, the amygdala disturbances during facial emotional processing may underlie impairments in facial expression recognition and intensity evaluation in patients with schizophrenia. However, the relationship between them has not been extensively researched. As far as we know, some studies have confirmed that reduced amygdala volume in patients with schizophrenia is related to impaired facial emotion recognition, but they did not conduct MRI scans while patients performed tasks.17,18 Although many studies have demonstrated atypical amygdala functioning in patients with schizophrenia, findings are inconsistent regarding whether the amygdala exhibits hypo-responsivity or hyper-responsivity to facial emotional stimuli.14,19 The heterogeneity of the results of low activity and hyperactivity in the amygdala may be due to differences in research methods, including (but not limited to) emotions that must be identified, as well as different task paradigms and analysis methods.20
In this study, we aimed to examine the discrepancies in active brain regions involved in processing the EIRT, which can serve as an indicator of facial emotion recognition ability and is affected by amygdala function, between patients with schizophrenia and healthy controls (HCs). The purpose of this study was to investigate the role of the amygdala in social cognition deficits in people with schizophrenia by focusing on alterations in amygdala activity linked to recognition of facial emotions.
Methods
Participants
A total of 60 subjects from the ages of 18 to 55 were enrolled in the study. Eight patients with schizophrenia and three HCs were excluded due to non-compliance with the standards and withdrawal. Forty-nine participants completed the experiment. Participants were divided into two groups: schizophrenia patients (SCZ; N = 22) and healthy controls (HC; N = 27). Schizophrenia patients were primarily recruited from either the inpatient or outpatient at the Department of Psychiatry of Wuxi Mental Health center. Meanwhile, HCs were recruited from the local community through online and print advertisements. Psychiatric interviews were necessary to make sure every member of HCs had no mental disorders. Each member of the health control group is required to provide a physical health report for the past year. Patients were diagnosed with Schizophrenia-spectrum disorders through the use of the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV). For schizophrenic patients, the dose of antipsychotic medication was calculated based on chlorpromazine equivalence. The number of schizophrenia patients taking medication (Clozapine/Olanzapine/Quetiapine/Risperidone/Aripiprazole) was 2, 3, 6, 8 and 3 respectively. During the preliminary screening, all participants provided informed consent and were informed of their right to withdraw at any time. The study was approved by the Ethics Review Committee of Affiliated Wuxi Mental Health Center of Nanjing Medical University and was in accordance with the Helsinki Declaration.
Exclusion Criteria
Regardless of grouping, general exclusion criteria that applied to all participants included (1) an IQ < 70, (2) an acute, unstable or uncontrolled physical disease, (3) a personal or first-degree family history of psychiatric disorders, (4) a neurological disorder (5) a substance abuse in the past 6 months, (6) contraindications for undergoing MRI examinations such as pregnancy, claustrophobia, metal implants, and others, (7) an identification as left-handed or (8) a history of Modified Electra convulsive Therapy treatment in the past 12 months. For HCs, additional exclusion criteria comprised (1) no diagnosis of psychiatric disorders according to DSM-IV criteria, and (2) no current use of medications affecting cognitive function.
Clinical Assessments
Clinically stable patients with schizophrenia were evaluated by two trained clinicians. The Positive and Negative Syndrome Scale (PANSS) was utilized to assess psychopathology.21 The PANSS was developed out of the need for a well-operationalized method of assessing these syndromes, ie, Positive syndromes, Negative syndromes and General psychopathology, in schizophrenia patients, including their relationship to one another and to global psychopathology. To evaluate basic perceptual ability regarding emotional facial expression intensity, the EIRT was administered.
MRI Acquisition and Analysis
All participants underwent an MRI scan using a 3.0 T Siemens Trio machine with software version “syngo MR E11”. The 3D-MPRAGE sequences had the following scanning parameters: an echo time (TE) of 30 millisecond (ms), a repetition time (TR) of 2000 ms, an inversion time (TI) of 900 ms, a percent phase field of view of 100, a field of view (FOV) of 384◊384 millimeter (mm)2 in the axial slice plane, a slice thickness of 3.5 mm and a slice number of 32. Each functional run consisted of 630 brain volumes, each comprising 32 axial slices. T1-weighted anatomical images were recorded with a total of 192 slices at a thickness of 0.9mm (TR = 2300 ms; TE = 2.32 ms; flip angle = 8°, matrix = 64◊64, a percent phase field of view of 100). Stimulus presentation and behavioral data were obtained using E-prime software 3.0 (Psychology Software Tools, Inc, Sharpsburg, GA).
Statistical Parametric Mapping 12.0 (SPM 12.0) was employed to analyze the functional imaging data. The preprocessing steps for image data included slice time correction, realignment, normalization to the standard EPI template, and smoothing with a three-dimensional 6-mm, full-width half-maximum Gaussian filter. A specific 1st-level analysis was conducted for the functional imaging data, modeling the fit of the imaging data and facial emotional recognition conditions. The main effect of group and the interaction between group and conditions were analyzed in a specified 2nd-level analysis using a full factorial approach by applying a 2 (group)◊6 (emotion) mixed-effects model.
Emotion Intensity Recognition Task
The experimental procedure followed the methodology of Adolphs et al.8 It comprised of two runs, namely Run 1 and Run 2, with each consisting of 4 blocks that evaluated 3 fundamental emotional terms and a neutral emotion. Each block comprised of 42 facial stimuli that included six faces expressing happiness, fear, sadness, disgust, anger, surprise, and six neutral faces. These stimuli were selected from the Chinese Facial Affective Picture system.22 In each block, the set of 42 face stimuli was presented randomly and the participant had no more than 5 seconds to identify and evaluate the intensity of the emotional face stimuli on a scale of 0 (no intensity) to 3 (very intense). The participant was instructed to identify the emotion as quickly as possible by button press. After fully evaluating one emotion term, the participant had to evaluate other emotion terms in subsequent blocks. Hence, in each block, participants identified and evaluated the intensity of all six basic emotions for each stimulus. As shown in Figure 1.
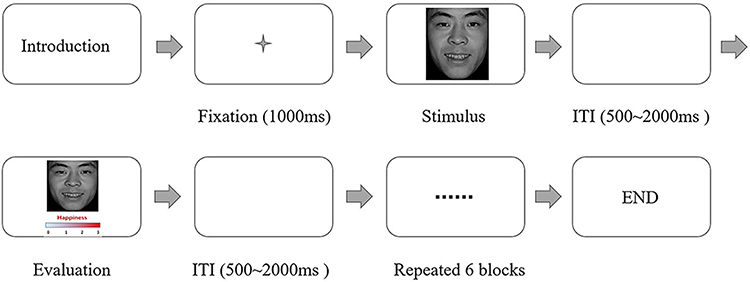 |
Figure 1 Example of the item and user interface of the emotion intensity recognition task. Abbreviation: ITI, inter-trial interval. |
The behavioral data was analyzed using SPSS V25. The number of accurate trials and response times were analyzed through repeated measures ANOVAs with 2 (group) ◊6 (emotion) design. Group comparisons for the number of accurate responses in trials with neutral facial expressions, and post hoc group comparisons of reaction times (RTs) and emotion intensity were conducted using two-sample t-tests.
Results
Demographics and Clinical Sample Characteristics
As shown in Table 1, 27 healthy participants (mean age 30.26 ± 5.59, 11 female) and 22 schizophrenia patients (mean age 32.09 ± 7.97, 10 female) took part in our experiment. As shown in Table 1, there was no significant difference in age, sex and years of education between the patient group and the control group. All patients had a chronic illness. Their average age of onset was 23.17 (SD = 4.25), and the average duration of illness was 8.91 (SD = 5.52). All patients were being treated with a stable dose of antipsychotic medication. According to previous study,23 the average dose of drug (mg/day, chlorpromazine equivalent) was 345.12 (SD = 97.25). Experienced clinical physician assessed schizophrenic psychopathology in the patient group, the mean performance on the PANSS Positive scores was 16.96 (SD = 10.62), the mean performance on PANSS Negative was 20.86 (SD = 4.61), and the mean performance on the PANSS General was 28.96 (SD = 8.13).
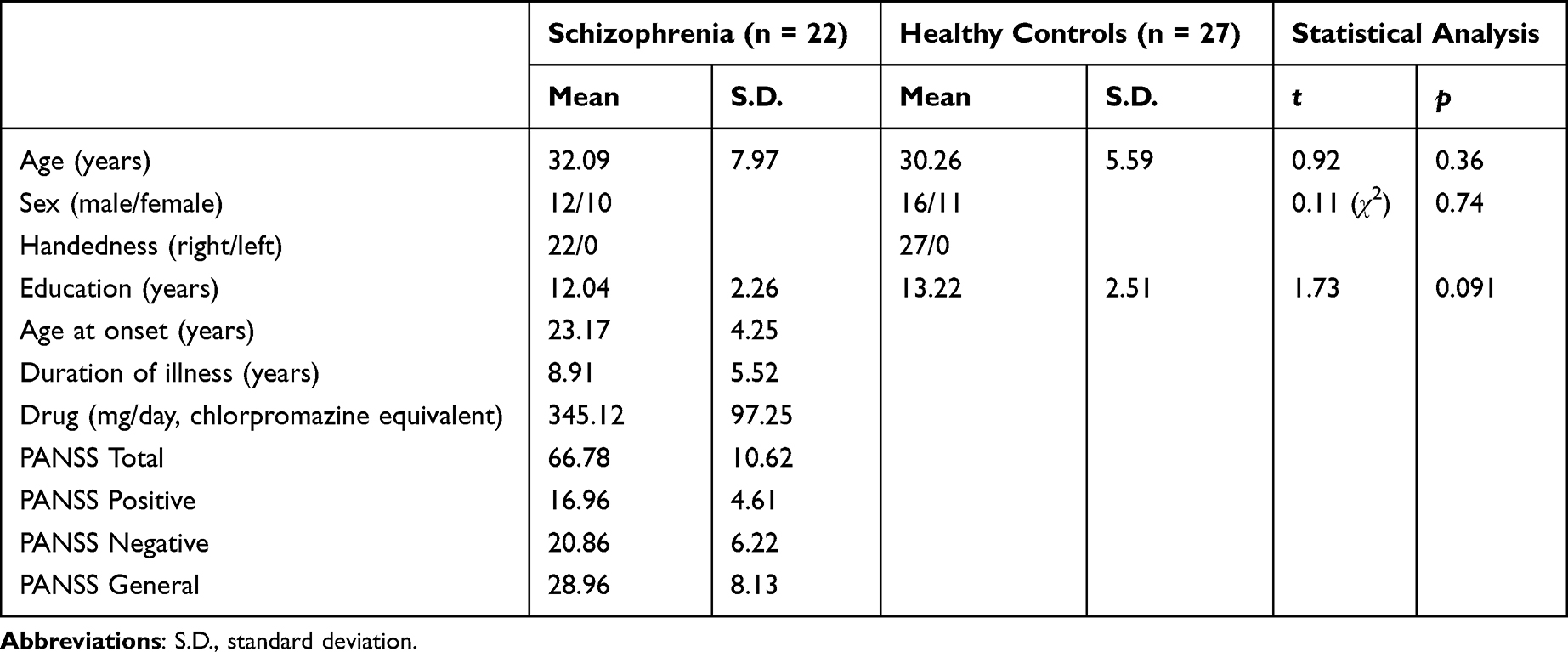 |
Table 1 Demographic, Clinical and Neuropsychological Characteristics of Subjects |
Behavioral Results
As shown in Table 2 and Figure 2a, the average number of correctly recognized facial emotions was 29.35 (69.88% of the trials, S.D. = 8.52), indicating that participants effectively understood and fulfilled the experimental requirements. Analysis of the correct emotion trials between groups revealed that participants with schizophrenia exhibited significantly more errors in facial expression recognition (t = −7.97, p < 0.001). Furthermore, between-group comparison of the trials with different emotions showed that schizophrenia subjects made significantly more errors in recognizing surprise, happiness, sadness, fear, and neutral expressions. Additionally, as shown in Figure 2b, patients with schizophrenia displayed longer response times compared to healthy controls during the task. Although there was no significant difference in response times for recognizing surprise, happiness, sadness, fear, and neutral facial expressions between the two groups, patients with schizophrenia exhibited significantly slower response times in recognizing happiness facial expression.
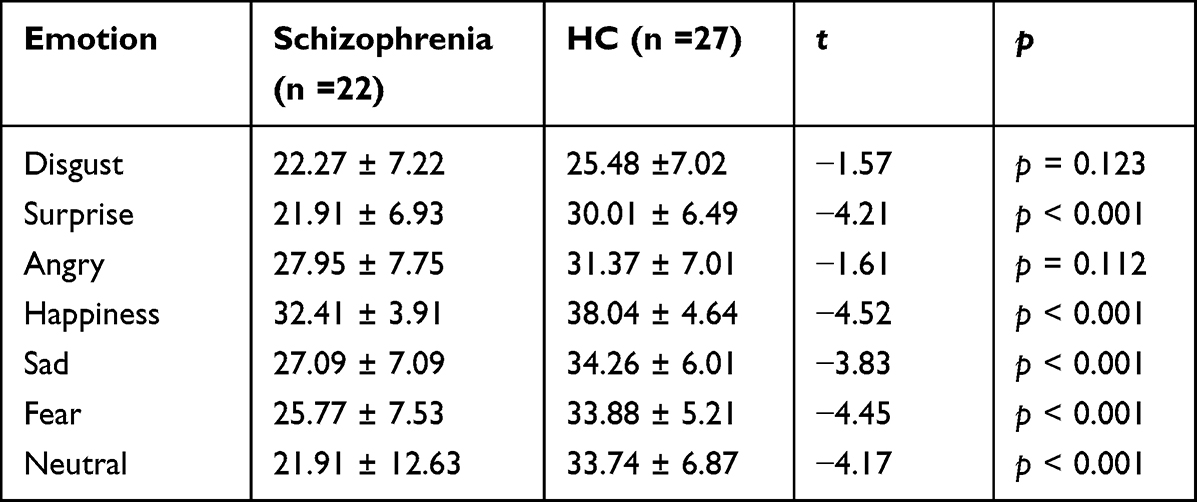 |
Table 2 Number of Correct Trials of the Healthy Control (HC) and Schizophrenia Group (Mean ± S.D.) |
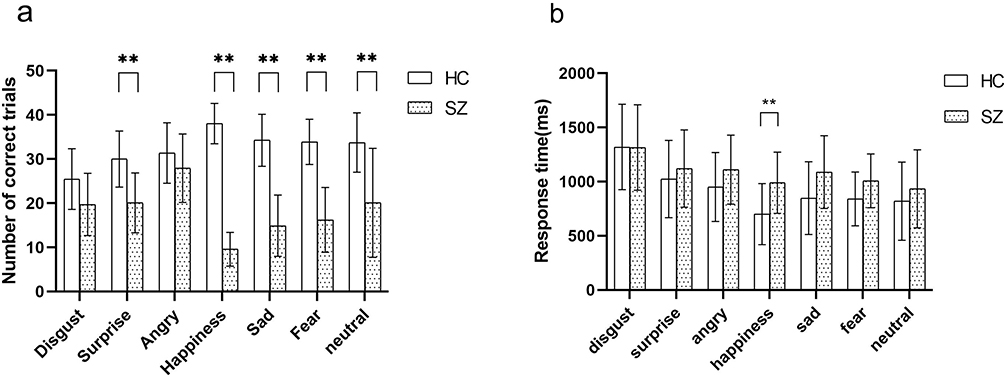 |
Figure 2 Comparing the emotional recognition performance of SZ (schizophrenia patients) and HC (healthy controls), the following measures were taken into consideration: (a) Number of correctly recognized trials, categorized by emotions, and (b) response time to recognize emotions. The data presented shows mean values with standard deviation bars. Any significant differences between groups are indicated by asterisks (**p<0.001). |
Functional Brain Imaging Results
As shown in Table 3 and Figure 3a and b, the comparison between the two groups revealed hypoactivation in patients with schizophrenia in multiple inferior parietal and temporal areas, as well as in the cerebrum and anterior cingulate. Moreover, the comparison between the two groups indicated higher activation in the bilateral amygdala in healthy controls as opposed to patients with schizophrenia. Furthermore, the ROI analysis for the amygdala demonstrated significant hypoactivation in the bilateral amygdala for subjects with schizophrenia (left amygdala coordinates: −24 −2 16, t = 6.02, p = 0.005 sv-corrected, k = 28; right amygdala coordinates: 24 −4 12, t = 5.99, p = 0.001 sv-corrected, k = 31). Finally, a whole-brain analysis revealed a significant interaction in the area of the right putamen and right insula.
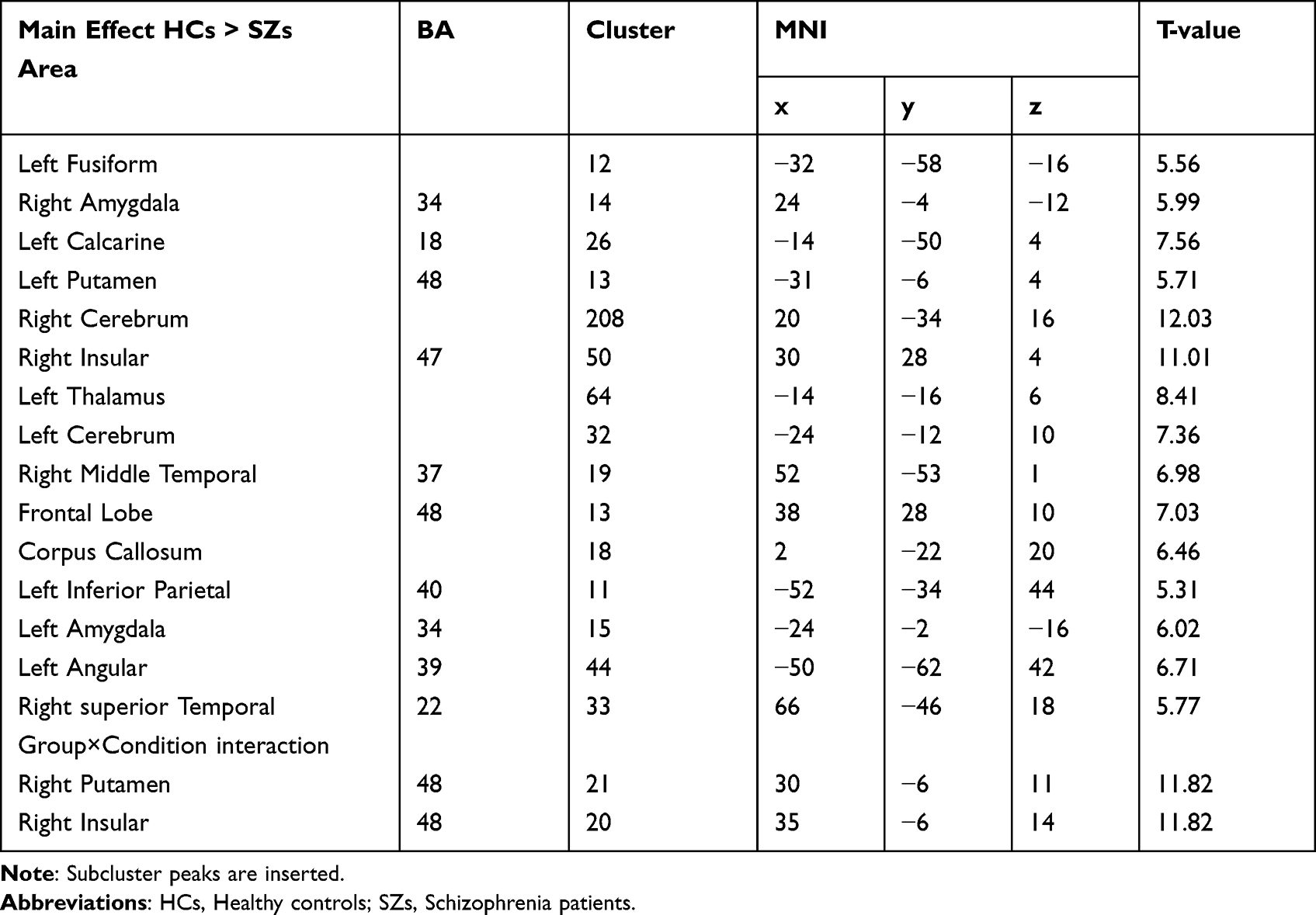 |
Table 3 Functional Brain Imaging Results for the Main Effects of Group and the Group by Condition Interaction (p < 0.005 FEW-Corrected) |
 |
Figure 3 Increased right amygdala activation in the group of healthy control relative to patients with schizophrenia during the process of facial emotion recognition task (left amygdala coordinates: −24 −2 16, t = 6.02, p = 0.005 sv-corrected, k = 28, (a) right amygdala coordinates: 24 −4 12, t = 5.99, p = 0.05 sv-corrected, k = 31, (b)). An analysis of two-factor ANOVA showed that there was a significant reduction in amygdala activation in the patient group for fear (**p < 0.05), (c). |
To investigate the differences in amygdala activation between groups based on the recognized emotion type, a directed interaction analysis was performed, testing the hypothesis that individuals with schizophrenia display reduced activation while recognizing emotional faces. As shown in Figure 3c, we extracted data from the amygdala region and averaged it. Data from amygdala ROI were extracted and averaged. An analysis of two-factor ANOVA showed that amygdala activity was hypoactive in schizophrenia patients when they recognized emotions, while it was active in controls. Compared with the different activation between groups, there was a significant reduction in amygdala activation in the patient group for fear (p < 0.05).
Discussion
The current study was designed to explore the differences in active brain areas in processing the task of the EIRT between schizophrenic patients and healthy controls, and to examine the role of the amygdala in social cognition deficits in schizophrenia patients by focusing on facial emotion recognition-related changes in amygdala activation. In order to avoid difficulties in explaining experimental results due to different task paradigm designs, we applied the task paradigm previously used, which minimizes the impact of differences in results between groups caused by experimental design. The study yielded three main findings: (1) schizophrenia patients found poor performance in recognizing facial emotions, specifically happiness, surprise, sadness, fear, and neutrality; (2) schizophrenia patients found hypoactivation in several inferior parietal and temporal regions, in the cerebrum and anterior cingulate; and (3) reduced amygdala activation in individuals with schizophrenia was associated with impaired recognition of fear in facial expressions.
Schizophrenia patients were found poorly performance in facial emotion recognition tasks. This defect is evident in the recognition of facial expressions of emotions, the present study found that subjects with schizophrenia made significantly more errors in recognizing surprise, happiness, sadness, fear, and neutrality. Although the reaction time for all emotions except disgust in schizophrenia patient group is generally longer, recognition defects only occurred when recognizing positive expressions; Compared to the control group, patients with schizophrenia exhibited negative bias and more often viewed happiness and neutral facial expressions as negative. This result was confirmed in Mier’s study,19 which differs from previous studies that have mostly indicated that patients with schizophrenia have comprehensive emotional facial expression recognition deficits.24 In addition, some studies have showed that individuals diagnosed with schizophrenia may encounter challenges in perceiving negative emotions, but their cognitive ability to process positive emotions is relatively similar to levels observed in healthy controls.25 However, more recent studies have found that schizophrenia patients have difficulty recognizing happiness emotions and have focused on the unique phenomenon of negative biases.9 The previous interpretation was that this is the result of negative symptoms in patients with schizophrenia, However, such a view finds little further support from the pattern of emotional expression recognition found in our study. To our surprise, the accuracy of recognizing disgust as an emotion proved comparable between the schizophrenia patient group and the control group. Tsoi et al research also discovered that patients with schizophrenia exhibited a specific deficit in recognizing happy facial expressions, while they were more likely to attribute any facial emotion as fearful or sad in nature.26 Therefore, we cannot attribute the deficiency in emotional recognition to negative symptoms. In summary, at the behavioral level, we find evidence to suggest that patients with schizophrenia have longer reaction times when recognizing faces with happy emotions, and their ability to recognize surprise, happiness, sadness, fear, and neutral facial expressions is insufficient.
In terms of brain activation, patients diagnosed with schizophrenia exhibited decreased activation in several brain regions, such as the fusiform, amygdala, insula, and temporo-parietal junction, in contrast to control subjects. These findings suggest an impairment of social cognitive networks, leading to a negative effect on facial emotion recognition abilities, and ultimately hindering social functioning.27 This finding aligns with a recent meta-analysis, which showed a marked inactivation of the amygdala, accompanied by a substantial limitation in activation throughout a ventral temporal-basal ganglia-prefrontal cortex “social brain” system may contribute to the challenges faced by patients when processing facial expressions of emotion.14 In addition, a group of emotional interactions occurred in the right insular and right putamen. Previous studies have found that self-regulation acquired in the insula cortex of schizophrenia patients can improve their emotional recognition ability and brain network connectivity.28,29 Reduced responses to human faces in the left insular region among those with schizophrenia may be associated with a fundamental deficit in facial processing. Various models of facial emotion processing suggest that the left hemisphere of the brain is specialized in tasks that demand thorough analysis of facial feature recognition, whereas the right hemisphere plays a role in tasks that require global, holistic processing such as facial affect recognition.30 In summary, the pattern of hypoactivation suggests a less automatic perception of facial emotional expressions in schizophrenia.
Previous research has noted diminished amygdala activity among individuals with schizophrenia when recognizing emotional expressions, but not when recognizing neutral facial expressions. In addition, structural abnormalities in the amygdala and impaired facial emotion recognition have been reported in schizophrenia. Reduced amygdala volumes in schizophrenia patients, and impaired recognition of facial emotional expressions have also been reported.31 We found that impaired facial emotion recognition in schizophrenia patients is emotion-specific (surprise, happiness, sadness, and fear). Our findings extend the evidence for the relationship between amygdala inactivation and facial emotion recognition deficits in schizophrenic patients. Our findings are partially consistent with recent meta-analyses of amygdala activation, suggesting decreased amygdala activation in schizophrenia.32 As a result, we can infer the following: first, in schizophrenia subjects, the amygdala does not generally respond to facial emotional stimuli with hypoactivity; second, they confirm studies that show schizophrenics process negative and positive facial information differently; third, the amygdala plays an important role in the recognition and processing of fear in schizophrenic patients.
Limitations
Our research has some limitations that need to be noted. First, we cannot completely rule out the possibility that medications and duration of illness may have contributed to our findings. However, we observed similar cognitive deficits in emotional face recognition in both first-episode drug-free patients and medicated patients in our discovery sample. In the meantime, it remains a challenge to describe whether, and how, medication affects the cognitive function of facial emotion recognition in schizophrenia patients.33 Second, gender of the participants was not matched between the groups. Existing research suggests that there may be gender differences in responsiveness to social cues and physiological reactions to emotional stimuli, with some studies indicating that women may show greater sensitivity in these areas. Third, the cross-sectional design of this study could have been improved. A prospective longitudinal study, where the same patients are scanned repeatedly during different mood state, would allow for more robust inferences regarding the trait- versus state-dependency of these abnormalities.
Conclusion
In schizophrenia patients, facial emotion processing deficits are emotion-specific (surprise, happiness, sadness, fear, and neutral). Moreover, schizophrenia patients were found hypoactivation in several inferior parietal and temporal areas, in cerebrum and anterior cingulate, and the amygdala reduced activation in these patients was associated with impaired recognition of fear in facial expressions.
Acknowledgments
We are grateful to everyone who generously participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This study is supported by Wuxi Municipal Health Commission Major Project (No. 202107) and Wuxi Taihu Talent Project (No. WXTTP2020008 and WXTTP 2021).
Disclosure
The authors report no conflicts of interest in this work.
References
1. McCutcheon RA, Reis Marques T, Howes OD. Schizophrenia-an overview. JAMA Psychiatry. 2020;77(2):201–210. doi:10.1001/jamapsychiatry.2019.3360
2. Mier D, Kirsch P. Social-cognitive deficits in schizophrenia. Curr Top Behav Neurosci. 2017;30:397–409. doi:10.1007/7854_2015_427
3. Berrios GE. Eugen Bleuler’s place in the history of psychiatry. Schizophr Bull. 2011;37(6):1095–1098. doi:10.1093/schbul/sbr132
4. Mothersill O, Knee-Zaska C, Donohoe G. Emotion and theory of mind in schizophrenia-investigating the role of the cerebellum. Cerebellum. 2016;15(3):357–368. doi:10.1007/s12311-015-0696-2
5. Fiorito AM, Aleman A, Blasi G, et al. Are brain responses to emotion a reliable endophenotype of schizophrenia? An image-based functional magnetic resonance imaging meta-analysis. Biol Psychiatry. 2023;93(2):167–177. doi:10.1016/j.biopsych.2022.06.013
6. Sabharwal A, Kotov R, Mohanty A. Amygdala connectivity during emotional face perception in psychotic disorders. Schizophr Res. 2021;228:555–566. doi:10.1016/j.schres.2020.11.030
7. Adolphs R. Neural systems for recognizing emotion. Curr Opin Neurobiol. 2002;12(2):169–177. doi:10.1016/S0959-4388(02)00301-X
8. Adolphs R, Tranel D, Damasio H, Damasio A. Impaired recognition of emotion in facial expressions following bilateral damage to the human amygdala. Nature. 1994;372(6507):669–672. doi:10.1038/372669a0
9. Gao Z, Zhao W, Liu S, et al. Facial emotion recognition in schizophrenia. Front Psychiatry. 2021;12:633717. doi:10.3389/fpsyt.2021.633717
10. Amminger GP, Schäfer MR, Papageorgiou K, et al. Emotion recognition in individuals at clinical high-risk for schizophrenia. Schizophr Bull. 2012;38(5):1030–1039. doi:10.1093/schbul/sbr015
11. Kohler CG, Martin EA. Emotional processing in schizophrenia. Cogn Neuropsychiatry. 2006;11(3):250–271. doi:10.1080/13546800500188575
12. Kohler CG, Turner TH, Bilker WB, et al. Facial emotion recognition in schizophrenia: intensity effects and error pattern. Am J Psychiatry. 2003;160(10):1768–1774. doi:10.1176/appi.ajp.160.10.1768
13. Helmuth L. Cognitive neuroscience. Fear and trembling in the amygdala. Science. 2003;300(5619):568–569. doi:10.1126/science.300.5619.568
14. Li H, Chan RC, McAlonan GM, et al. Facial emotion processing in schizophrenia: a meta-analysis of functional neuroimaging data. Schizophr Bull. 2010;36(5):1029–1039. doi:10.1093/schbul/sbn190
15. Brunet-Gouet E, Decety J. Social brain dysfunctions in schizophrenia: a review of neuroimaging studies. Psychiatry Res. 2006;148(2–3):75–92. doi:10.1016/j.pscychresns.2006.05.001
16. Marwick K, Hall J. Social cognition in schizophrenia: a review of face processing. Br Med Bull. 2008;88(1):43–58. doi:10.1093/bmb/ldn035
17. Namiki C, Hirao K, Yamada M, et al. Impaired facial emotion recognition and reduced amygdalar volume in schizophrenia. Psychiatry Res. 2007;156(1):23–32. doi:10.1016/j.pscychresns.2007.03.004
18. Exner C, Boucsein K, Degner D, et al. Impaired emotional learning and reduced amygdala size in schizophrenia: a 3-month follow-up. Schizophr Res. 2004;71(2–3):493–503. doi:10.1016/j.schres.2004.02.023
19. Mier D, Lis S, Zygrodnik K, et al. Evidence for altered amygdala activation in schizophrenia in an adaptive emotion recognition task. Psychiatry Res. 2014;221(3):195–203. doi:10.1016/j.pscychresns.2013.12.001
20. Kandilarova S, Stoyanov D, Popivanov ID, et al. Application of functional magnetic resonance imaging in psychiatric clinical evaluation: controversies and avenues. J Eval Clin Pract. 2018;24(4):807–814. doi:10.1111/jep.12906
21. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–276. doi:10.1093/schbul/13.2.261
22. Gong X, Huang Y-X, Wang Y, et al. Revision of the Chinese facial affective picture system. Chin Mental Health J. 2011;25(1):40–46.
23. Woods SW. Chlorpromazine equivalent doses for the newer atypical antipsychotics. J Clin Psychiatry. 2003;64(6):663–667. doi:10.4088/JCP.v64n0607
24. Kohler CG, Walker JB, Martin EA, et al. Facial emotion perception in schizophrenia: a meta-analytic review. Schizophr Bull. 2010;36(5):1009–1019. doi:10.1093/schbul/sbn192
25. Edwards J, Jackson HJ, Pattison PE. Emotion recognition via facial expression and affective prosody in schizophrenia: a methodological review. Clin Psychol Rev. 2002;22(6):789–832. doi:10.1016/S0272-7358(02)00130-7
26. Tsoi DT, Lee KH, Khokhar WA, et al. Is facial emotion recognition impairment in schizophrenia identical for different emotions? A signal detection analysis. Schizophr Res. 2008;99(1–3):263–269. doi:10.1016/j.schres.2007.11.006
27. Yamada Y, Okubo R, Tachimori H, et al. Pharmacological interventions for social cognitive impairments in schizophrenia: a protocol for a systematic review and network meta-analysis. Front Psychol. 2022;13:878829. doi:10.3389/fpsyg.2022.878829
28. Ruiz S, Lee S, Soekadar SR, et al. Acquired self-control of insula cortex modulates emotion recognition and brain network connectivity in schizophrenia. Hum Brain Mapp. 2013;34(1):200–212. doi:10.1002/hbm.21427
29. Yao S, Becker B, Geng Y, et al. Voluntary control of anterior insula and its functional connections is feedback-independent and increases pain empathy. Neuroimage. 2016;130:230–240. doi:10.1016/j.neuroimage.2016.02.035
30. Holt DJ, Kunkel L, Weiss AP, et al. Increased medial temporal lobe activation during the passive viewing of emotional and neutral facial expressions in schizophrenia. Schizophr Res. 2006;82(2–3):153–162. doi:10.1016/j.schres.2005.09.021
31. Rich AM, Cho YT, Tang Y, et al. Amygdala volume is reduced in early course schizophrenia. Psychiatry Res Neuroimaging. 2016;250:50–60. doi:10.1016/j.pscychresns.2016.02.006
32. Zhu T, Wang Z, Zhou C, et al. Meta-analysis of structural and functional brain abnormalities in schizophrenia with persistent negative symptoms using activation likelihood estimation. Front Psychiatry. 2022;13:957685. doi:10.3389/fpsyt.2022.957685
33. Harvey PD, Isner EC. Cognition, social cognition, and functional capacity in early-onset schizophrenia. Child Adolesc Psychiatr Clin N Am. 2020;29(1):171–182. doi:10.1016/j.chc.2019.08.008
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of Magnetic Seizure Therapy in Patients with Schizophrenia and Combined fMRI-EEG to Explore the Regulatory Mechanisms of Brain Networks
Wei S, Chen B, Guo Z, Zhang H, Li J, Hu X, Yang C, Li J, Li X, Liu Z, Xu Y, Liu S
Neuropsychiatric Disease and Treatment 2025, 21:323-334
Published Date: 19 February 2025