Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
The Need for and Perceptions of Interprofessional Education and Collaboration Among Undergraduate Students in Nursing and Medicine in South Korea
Received 7 February 2022
Accepted for publication 5 April 2022
Published 22 April 2022 Volume 2022:15 Pages 847—856
DOI https://doi.org/10.2147/JMDH.S359412
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hee-Young Song,1 Kyoung A Nam2
1Department of Nursing, Wonju College of Medicine, Yonsei University, Wonju-si, Gangwon-do, South Korea; 2School of Nursing, Research Institute of Nursing Science, Hallym University, Chuncheon-si, Gangwon-do, South Korea
Correspondence: Kyoung A Nam, School of Nursing, Research Institute of Nursing Science, Hallym University, 1 Hallymdaehak-gil, Chuncheon-si, 24252, Gangwon-do, South Korea, Tel +82 33 248 2717, Fax +82 33 248 2734, Email [email protected]
Purpose: Interprofessional education (IPE) for undergraduate students in the healthcare disciplines facilitates the acquisition of skills required for interprofessional collaboration, which is critical for patient care. This study assesses the need for and perceptions of IPE and interprofessional collaboration among undergraduate students in nursing and medicine in South Korea.
Participants and Methods: This was a cross-sectional survey of undergraduate students in nursing (n = 130) and medicine (n = 68), who had never been exposed to IPE, using a convenience sampling method. The Readiness for Interprofessional Learning Scale (RIPLS) (19 items), Interdisciplinary Education Perception Scale (IEPS) (12 items), and Interprofessional Education and Collaborative (IPEC) Competency Self-Assessment Scale (16 items) were used. Data were analyzed using descriptive statistics, χ2 test, and independent sample t-test.
Results: Students in both schools almost equally indicated the need for IPE and practice-based IPE in their clinical rotations, focusing on patients in general wards, and wanted to learn teamwork. The mean RIPLS scores were 68.5 ± 5.62 in nursing students and 67.5 ± 6.53 in medical students, and those of the IEPS were 57.0 ± 7.03 in nursing students and 58.7 ± 7.08 in medical students, without significant differences. Nursing students scored significantly higher on the positive professional identity subscale of the RIPLS, whereas medical students scored higher on the competency and autonomy and perceived need for cooperation subscales of the IEPS. The total scale scores on the IPEC Competency Self-Assessment Scale were 65.2 ± 3.35 for nursing students and 67.4 ± 2.96 for medical students, the latter having a significantly higher score.
Conclusion: This study revealed differences in needs and perceptions regarding IPE and interprofessional collaboration between schools. These findings warrant further research to design IPE program goals and strategies that are reflective of students’ needs.
Keywords: health discipline, teamwork, collaborative competency, clinical practice-based education
Introduction
The delivery of effective and high-quality patient care demands collaboration among healthcare professionals. Today, more than ever before, healthcare providers have realized that patients benefit more from interprofessional teams that mutually respect one another, communicate effectively, and coordinate patient care.1 The literature suggests that high levels of interprofessional collaboration lead to better patient outcomes, improved patient satisfaction, and higher workplace satisfaction among healthcare professionals.2,3 Accordingly, healthcare professionals are increasingly required to cooperate and collaborate more closely in the delivery of care.2
Interprofessional education (IPE), defined as two or more health or social care professionals learning knowledge and skills about, from, and with each other,4 is critical in creating effective collaboration between them, resulting in better patient outcomes. The benefits of IPE for the healthcare system were also reported, including employment and workplace culture and collaborative practice.5 After embedding IPE in curricula for students in nursing, medical, or allied healthcare profession, its effectiveness was described as follows: to provide a foundation to link to real-world experiences, enhance the confidence of individuals’ professional identity, and help students better understand the professional roles between disciplines.6–9 Most recently, an experimental study on IPE with a control group reported that the participants in the experimental group had higher scores in interprofessional knowledge and competence compared to the control group after the IPE intervention.10
Although learning through IPE can occur in either academic or clinical settings,11 the World Health Organization (WHO) recommends implementing IPE as an integral part of the curriculum of undergraduate medical and health-related professions.5 As the early interaction of students from different health disciplines facilitates the acquisition of the skills required to work effectively in a healthcare setting,1,12 IPE should start early, targeting undergraduate students.
The importance of IPE is gradually being recognized.2,13–15 In particular, the importance of close collaboration involving nurses and doctors equally and actively has been highlighted to ensure the quality of care and better outcomes in the delivery of healthcare.3 However, thus far, studies on IPE in nursing and medical education in Korea have mostly been conducted on introducing the IPE concept16,17 and faculty or student perceptions, thus revealing that both have fewer opportunities to experience a systematically designed formal IPE program. Hence, there is limited evidence on the levels and differences in student perceptions of IPE17,18 and that of their IPE competency.
Prior to designing IPE programs to develop competencies that result in favorable outcomes, assessing and prioritizing educational needs and perceptions would be valuable for health care students,18 particularly, for undergraduates.19 Also, assessing the needs of healthcare professionals equally and recognizing their diversity helps establish an ethical and transparent learning environment for IPE,20 which will ensure a beneficial program. Therefore, this study aimed to assess and compare IPE needs and perceptions among undergraduate students in nursing and medicine who are in an environment where IPE implementation has just begun. This study provides innovative and valuable information to verify the aspects that should be differentiated or assimilated in establishing early IPE program strategies for this population.
Materials and Methods
Setting and Participants
A cross-sectional study design was used with undergraduate students from the schools of nursing and medicine at two universities located in Gangwon Province in South Korea. The average number of students admitted every year in both the schools of nursing and medicine are 75 and 65, respectively. In these universities, the schools of nursing run four-year programs, and the schools of medicine run six-year programs since they have been established 30 years ago or more. These schools were selected based on the similarity of their curriculums: basic science courses and introductory courses related to the specialty in the second academic year, and major courses and a clinical practicum beginning in the third year until graduation. Neither school has officially incorporated IPE into its curriculum.
A convenience sampling method was used to recruit participants from each school. Students from the second through fourth academic years were selected because of the similarity in their levels of basic, introductory, and major courses taken and their availability at the time of data collection. Those who had previously experienced IPE were excluded.
The estimated sample size was calculated to be 170 with a significance level of α = 0.05, a statistical power of 80%, and an effect size (Cohen’s d) of 0.5, which is a medium effect size.21 The participants were recruited through flyers, on-and offline bulletins in student communities, and in-person contact by research assistants among all students enrolled in their second and fourth academic year from both universities at the time of data collection which was from June to September 2020. The number of nursing and medical students who voluntarily responded were 143 and 70, respectively, of which 198 who completed the questionnaire were included in the final analysis (7% attrition rate).
Measurement Instruments
A structured questionnaire was used to collect information on the participants’ demographic characteristics including sex, age, the duration of study, specialty, and the need for IPE. Three validated self-administered scales were used to assess the students’ perceptions of IPE and interprofessional collaboration. The Readiness for Interprofessional Learning Scale (RIPLS),22 Interdisciplinary Education Perception Scale (IEPS),23 and Interprofessional Education Collaborative (IPEC) Competency Self-Assessment Scale24 were validated, published in English, and licensed for public use.6 Specifically, the RIPLS was validated with Korean students in nursing, medicine, and other allied healthcare professions, such as physiotherapy, occupational therapy, and dental hygiene by Lee et al,25 and it was also used to measure the effectiveness of IPE for medical and nursing students.26
The other two instruments, the IEPS and IPEC Competency Self-Assessment Scale, were translated into Korean through a standard forward-backward translation procedure,27 as follows: The first translation was performed independently from English to Korean by one nursing professor and two nurses who were bilingual. Then, the Korean translation was independently translated back into English by two other bilingual translators who majored in nursing. Four professors from nursing and medicine then compared the back-translated version to the original and decided that it was acceptable, with a few minor changes in wording. The content validity was verified using the Content Validity Index (CVI) and a panel of six expert judges, consisting of a nurse, three nursing professors experienced in instrument translation and implementation research, and two professors from the school of medicine who had experience with IPE for students and research. To determine the CVI, members of the panel were asked to rate each scale item in terms of its relevance to the underlying construct using a Likert-type 4-point scale. Those items that received a rating of either 3 or 4 by the experts were judged to be relevant, and the CVI of the translated Korean version of the IEPS and IPEC Competency Self-Assessment Scale were 0.96 and 0.94, respectively. The scale is considered to have excellent content validity at a CVI of 0.90 or higher,28 thus the content validity of these scales was determined to be acceptable.
Readiness for Interprofessional Learning Scale (RIPLS)
The RIPLS consists of 19 items and was validated for eight health professions by Hu and Bentler.29 It contains four subscales: teamwork and collaboration, negative professional identity, positive professional identity, and roles and responsibilities. The Likert scale ranges from “strongly disagree” (1 point) to “strongly agree” (5 points); the higher the score, the more positive the attitude toward interprofessional learning. In a previous study using the Korean version of the RIPLS,25 for instrument reliability, Cronbach’s alpha was 0.880. In our study, Cronbach’s alpha for the total scale was 0.883, and those of subscales, ie teamwork and collaboration, negative professional identity, positive professional identity, and roles and responsibilities, were 0.858, 0.831, 0.814, and 0.752, respectively.
Interdisciplinary Education Perception Scale (IEPS)
The IEPS is a 12-item instrument that measures perceptions of interprofessional cooperation. The scale has three factors: competency and autonomy, perceived need for cooperation, and perception of actual cooperation.30 Items responded to are measured using a Likert scale ranging from “strongly disagree” (1 point) to “strongly agree” (6 points). A higher score indicates a more positive perception of interprofessional cooperation. The reliability, validity, and normative data of the IEPS for several allied health professions have been published.31 In this study, for the whole scale, the Cronbach’s α was 0.865, and the Cronbach’s α of the three subscales, competency and autonomy, perceived need for cooperation, and perception of actual cooperation, were 0.783, 0.742, and 0.870, respectively.
Interprofessional Education Collaborative (IPEC) Competency Self-Assessment Scale
To measure students’ perceptions of IPEC competency, a 16-item instrument consisting of two factors, interprofessional interaction and interprofessional values, was used. The interprofessional interaction subscale primarily comprises items from the teams and teamwork domain of the four IPEC domains originally defined by the IPEC expert panel,32,33 with one item each based on competencies from the interprofessional communication and values/ethics domains from the four IPEC domains. The interprofessional values subscale comprises items only from the values/ethics domain. Items are measured using a Likert scale ranging from “strongly disagree” (1 point) to “strongly agree” (5 points). A higher score indicates a better perception of competencies for interprofessional collaboration. In this study, for the whole scale, the Cronbach’s α was 0.924, and the Cronbach’s α of the two subscales, interprofessional interaction and interprofessional values, were 0.874 and 0.856, respectively.
Data Collection
Informed consent was obtained from each student prior to participating in the study. Data collection was conducted by two research assistants, each of whom had completed an 8-hour training session encompassing the ethical considerations and study objectives, from the survey context to a detailed explanation of the questionnaire and data collection procedure. Next, the research assistants administered it among themselves, and overviewed other aspects of the survey and research assistant role to ensure consistency. Using a set of standardized instructions, the research assistants explained to the participants the purpose of the study, the content of the questionnaire, and the fact that their participation was voluntary and would not affect their grades. Subsequently, the questionnaire was distributed to the students according to their schedules. During the survey, the participants were told to ask questions or for help whenever they needed, and no specific difficulties were reported. It took approximately 20 minutes to complete the questionnaire.
Data Analysis
Descriptive statistics were calculated for the demographic variables. The variables of interest were compared between the schools using the χ2 test and independent sample t-test. The significance level for two-tailed tests was set at 0.05. All analyses were performed using IBM SPSS Statistics, version 25 (IBM Corp., Armonk, NY, USA).
Ethical Considerations
The study protocol was approved by the Institutional Review Board of Wonju College of Medicine, Yonsei University (CR319091). Students who met the inclusion criteria were invited to participate in the study. Those who agreed to participate provided written informed consent after receiving an explanation of the purpose of the study, including assurance of privacy, potential benefits and risks, the voluntary nature of their participation, and the provision to withdraw without consequence.
Results
Participant Characteristics
As shown in Table 1, more than 70% of the participants were women and nursing students with a mean age of 21.7 ± 1.84 years old. With regard to year in school, 24.7% were sophomores, 35.9% were juniors, and 39.4% were seniors.
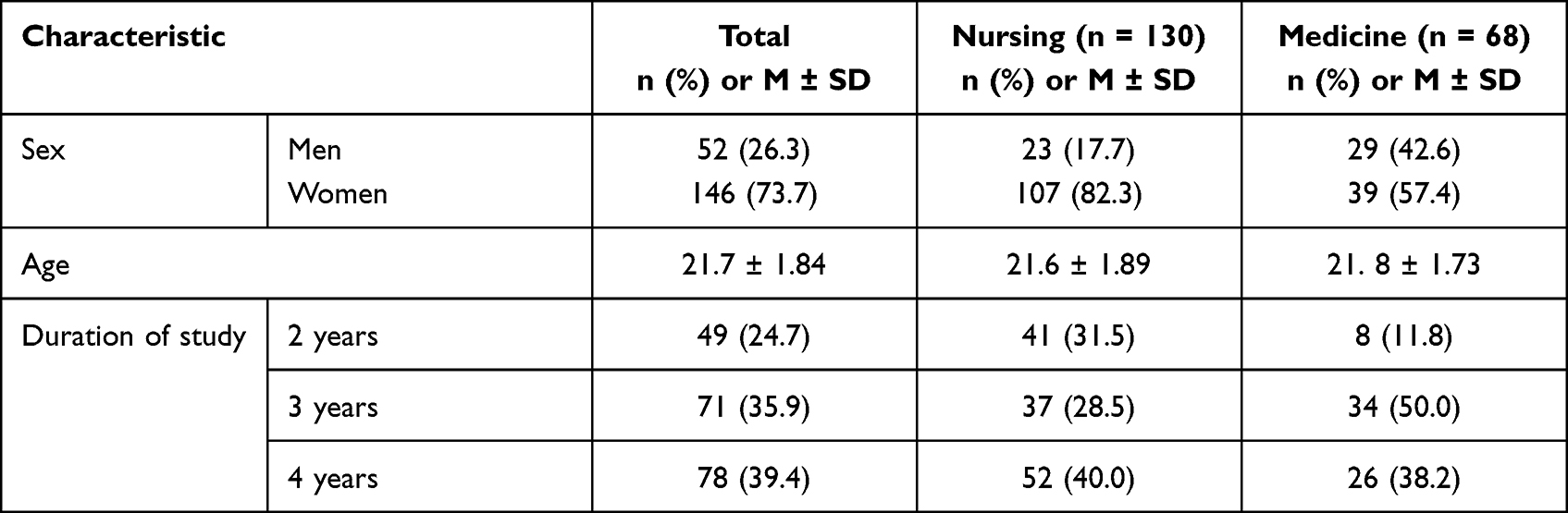 |
Table 1 General Characteristics of the Participants (N = 198) |
Comparison of IPE Needs Between Nursing and Medical Students
Almost all nursing (90.6%) and medical students (89.7%) indicated a need for IPE, without any significant difference between the schools. In addition, most students in both schools (nursing = 81.5%; medical = 88.2%) believed that IPE should be applied in the curriculum in the third and fourth years, and there was no significant difference. However, there were some significant differences regarding IPE contents, essential skills to be learned through IPE, and learning methods for IPE, as shown in Table 2.
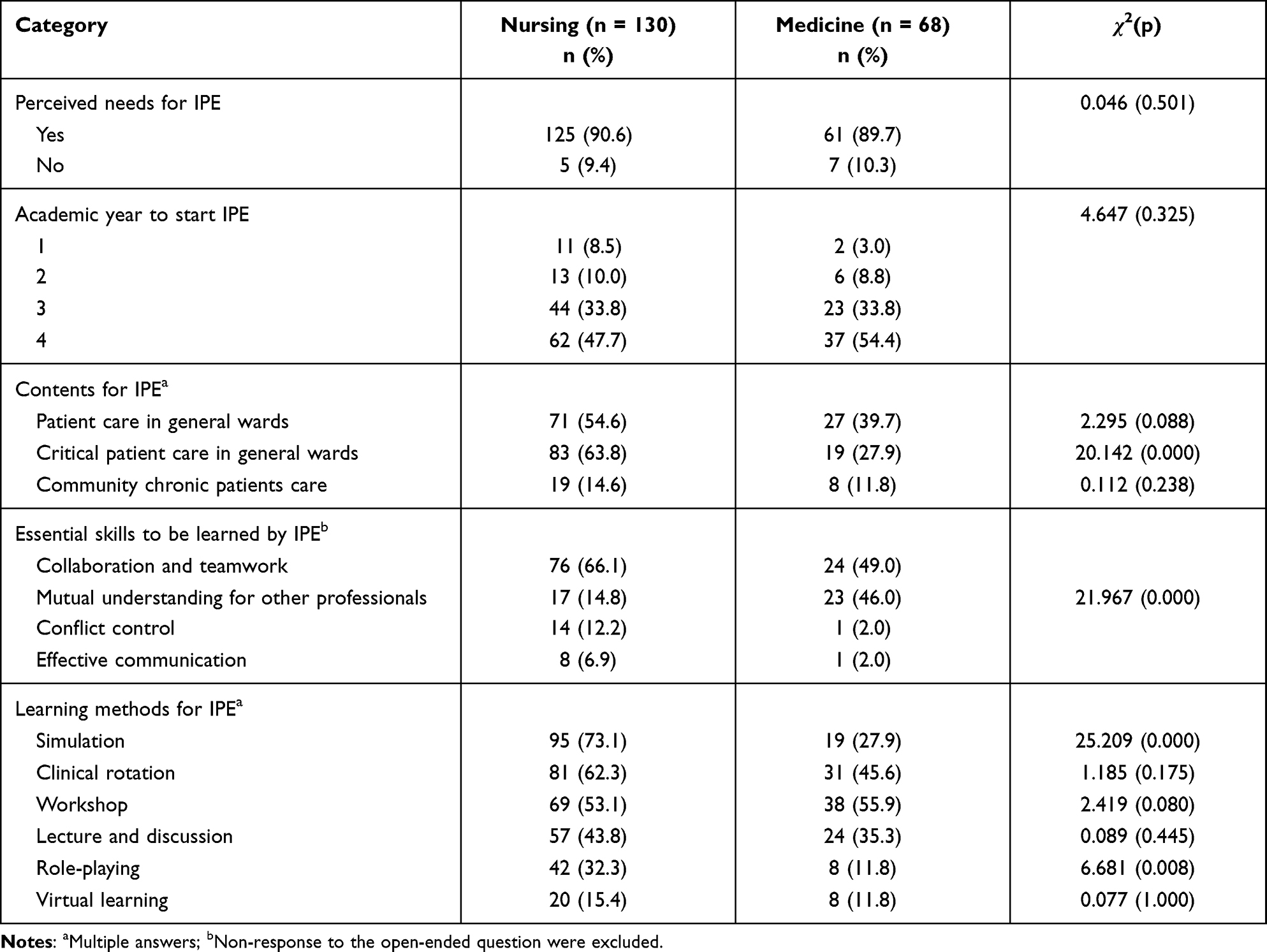 |
Table 2 Comparison of Interprofessional Education (IPE) Needs Between Schools (N = 198) |
Regarding IPE contents, both nursing and medical students almost equally listed ward patient care and community chronic patient care, whereas nursing students wanted to learn critical patient care in general wards more than medical students (χ2 = 20.142, p = 0.000). Regarding the essential skills to be learned by IPE, which was investigated by an open-ended question, more than half of nursing students (66.1%) claimed that IPE was necessary to learn collaboration and teamwork, whereas medical students assessed collaboration and teamwork, and mutual understanding for other professionals in a similar proportion (χ2 = 21.967, p = 0.000).
In terms of IPE learning methods, nursing students preferred simulation (χ2 = 25.209, p = 0.000) and role-playing (χ2 = 6.681, p = 0.008) compared to medical students. However, half of the students in both schools wanted IPE during clinical rotation with no significant difference between the two schools.
Comparison of Variables Between Nursing and Medical Students
RIPLS
The mean scores for the RIPLS were 68.5 ± 5.62 for nursing students and 67.5 ± 6.53 for medical students, with no significant difference between schools. The mean score for each RIPLS domain, and a comparison between nursing and medical students, are presented in Table 3. Nursing students gave significantly higher scores on the positive professional identity subscale than medical students (t = 2.469, p = 0.014).
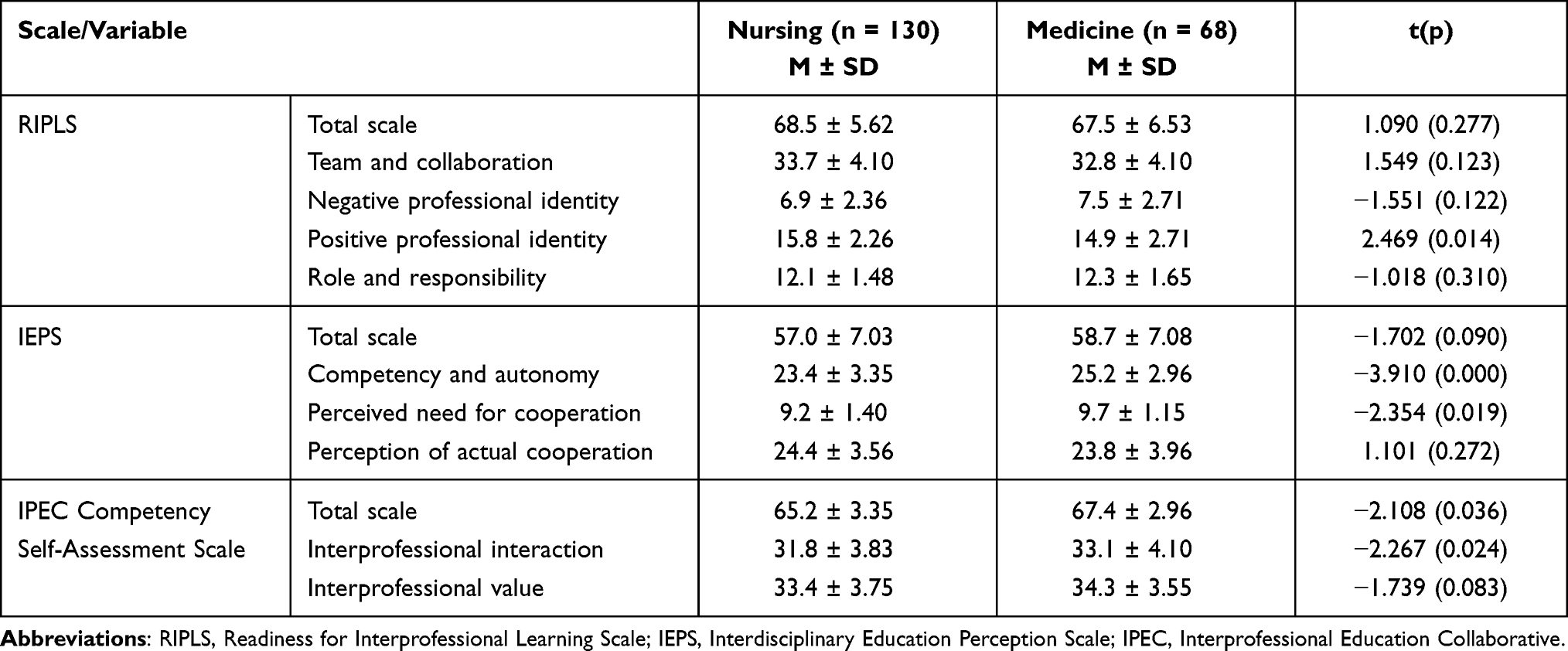 |
Table 3 Comparison of the Variables Between Schools (N = 198) |
IEPS
The mean scores for the IEPS total scale were 57.0 ± 7.03 for nursing students and 58.7 ± 7.08 for medical students, with no significant difference between schools. However, there were significant differences between the two groups in the domains of competency and autonomy (t = -3.910, p = 0.000), and perceived need for cooperation (t = -2.354, p = 0.019), with medical students having higher scores in both domains (see Table 3).
IPEC Competency Self-Assessment Scale
The total scale scores on the IPEC Competency Self-Assessment Scale were 65.2 ± 3.35 for nursing students and 67.4 ± 2.96 for medical students, with medical students having a significantly higher score (t = −2.108, p = 0.036). As Table 3 reveals, medical students also scored significantly higher on the interprofessional interaction subscale (t = −2.267, p = 0.024).
Discussion
This study explores and compares the overall need for and perceptions of IPE among undergraduate nursing and medical students with no previous experience of IPE. We employed prominent internationally-applied instruments to assess the participants’ perceptions. The study findings provide insight into IPE and suggest how healthcare educators should design them based on the needs and perceptions of nursing and medical students, who as future healthcare professionals, will be required to effectively collaborate as a healthcare team.
The results indicate that most students from both schools recognized the need for IPE to mutually understand other professionals and learn teamwork. This is in line with the findings of previous studies that suggest the need for IPE for collaborative teamwork and to cultivate roles and responsibilities to undergraduate students in medicine, nursing, pharmacy,34 and other allied healthcare programs (eg, clinical laboratory science and physiotherapy).6,34 Regarding the timing for starting IPE, most students indicated the fourth academic year; however, no existing evidence indicates the right time for health professionals to begin IPE. Berger-Estilita et al35 reported that a third of medical students indicated that IPE should start just before or during clinical training, while another third indicated that IPE should start as early as the first year of undergraduate education and training. Some studies have also suggested that IPE should be planned from the beginning of the undergraduate program.36–38 Given the inconsistent evidence on the ideal timing for IPE, further research is warranted to explore when to start IPE in terms of reflecting student needs and perspectives and ensuring the effectiveness of the training.
Regarding IPE contents, most participants indicated “ward patient care” and “critical patient care in general wards”, whereas “community chronic patient care” was included by less than 15% of students. The participants in this study seemed to focus more on patient care in the hospital, which may be related to the scope of their clinical placements during academic training. In professional healthcare education for undergraduate students in South Korea, most of the training takes place in inpatient wards and emphasizes the improvement of technical skills.39–41 In particular, the critical care of hospitalized patients requires the cooperation and collaboration of skilled professionals from multiple disciplines.42 Therefore, IPE related to critical inpatient care should be reflected in the education and training of nursing and medical students.
Regarding learning methods, nursing students preferred simulation and role-playing, whereas medical students preferred a workshop. These differences should be noted, as most IPE programs for nursing, medicine, and other healthcare professions in previous studies included simulation along with lectures,43 regardless of the participants’ characteristics and needs. Although simulation is a teaching method that provides immersive experiential learning and allows for disciplines to work together in a safe environment,44 the effectiveness of simulation-enhanced IPE and related factors has been questioned and is an area need of further investigation.43 In addition, gaps in student learning methods between professions should be taken into account to ensure the impact of IPE on participants’ outcomes.18 Nevertheless, students in both schools wanted IPE during their clinical rotation. This finding is in line with the suggestion that basic and clinical science be integrated into the IPE curriculum to contextualize theoretical learning in clinical practice,37 and that implementing practice-based IPE in students’ placement curricula would boost collaboration among healthcare providers.45 Therefore, an IPE program for nursing and medical students should be constructed in the clinical setting, during clinical placement, which can integrate theoretical learning into clinical practice.
Nursing students were more positive in their professional identity than medical students based on their RIPLS subscale scores. A well-developed professional identity is important to engage in teamwork.35 However, stronger definitions of individual professional roles and the uniprofessional socialization of healthcare providers may be significant barriers for interprofessional collaboration, causing healthcare professionals to work independently in meeting their own client care goals.46 Therefore, it is important for students to develop dual identities as members of the medical team and in their professional society for interprofessional practice.46
Contrary to a higher professional identity score, nursing students showed a lower competency and autonomy score on the IEPS, which measures attitudes toward interprofessional collaboration. Furthermore, nursing student scores on the “perceived need for cooperation” on the IEPS and “interprofessional interaction” on the IPEC Competency Self-Assessment Scale were also lower than those of medical students. Yune et al’s18 study reported similar results, indicating that medical students perceived their collaborative leadership competency to be higher than that of students in other majors, such as nursing and pharmacy. This results should be interpreted in consideration of the literature suggesting that the constructs underlying these subscales may be affected by experience and training.24 Student responses to the items may have been affected by individual experiences related to interprofessional collaboration in clinical placement or taking other courses that were not measured in this study.
Another related aspect to consider is the impact of gender stereotypes and power relations on self-evaluation of competency, autonomy, and the need for cooperation. Students are likely to evaluate themselves and their needs within the context of stereotypical structures of gender and power, in which men predominate the field of medicine and have more power, and women predominate the field of nursing and have less power. Given that gender stereotypes and power relations tend to be barriers to interprofessional collaboration among students from different professions,47 educational strategies to promote mutual understanding among the professions should be developed and introduced earlier in IPE courses for nursing and medical students, before students’ professional biases are established.37
To our knowledge, this study is the first to provide valuable information on IPE among nursing and medical students in South Korea. However, the generalizability of the results may be limited because of the possibility of selection bias related to the sample from only two universities in one province of South Korea. Future research should include a larger sample size and more schools. Moreover, this study was conducted during the COVID-19 pandemic, which raises the following considerations. First, in this period, healthcare professionals, especially nurses, were presented in the media as very important figures, more than ever before in South Korea.48 Thus, nursing students were likely to have an increased awareness of the importance and responsibility of their profession, which may have influenced the students responses to professional identity scores in this study. Previous research49 reporting an increase in professional identity scores among nursing students later in the first wave of COVID-19 (compared with the earlier phase of the COVID-19 pandemic) may be in line with this explanation. Second, during the COVID-19 pandemic, the clinical rotations of students in the healthcare profession were forced to be limited to reduce transmission and protect students from infection. This limited clinical experience may have impacted the students’ considerable learning needs in clinical practicum. Although these interpretations should be limited to this study, the COVID-19 crisis is a milestone in the development of IPE for healthcare professionals, as the need for interprofessional collaborative practice is emphasized more than ever by healthcare educators and students.50,51
Conclusions
This study found that students in nursing and medical schools agreed on the importance of implementing IPE in their programs. However, there were differences between nursing and medical students regarding the contents, essential skills to learn, and learning methods for IPE. Therefore, including IPE in the curriculum for this population should be according to their respective needs, as much as possible. In addition, differences between nursing and medical students in their readiness and perception of interprofessional relationships and competencies suggest that an early assessment of these issues is warranted. Thus, strategies that reflect these differences should be incorporated into IPE programs to establish effective IPE. Further studies are essential to evaluate the effectiveness of IPE tailored to the needs of students in diverse healthcare disciplines.
Funding
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT & Future Planning (2019R1F1A1044128) and the Hallym University Research Fund, 2021 (HRF-202111-005). The sponsors had no involvement at any stage, from study design to submission of the paper for publication.
Disclosure
The authors declare that they have no competing interests.
References
1. Arulappan J, Matua GA, Alzaabi O, et al. Knowledge and readiness for inter professional education and collaborative practice among undergraduate nursing students in a Middle Eastern country - a pilot study. Nurse Educ Today. 2021;100:104865. doi:10.1016/j.nedt.2021.104865
2. Pinto RM, Kay ES, Wall MM, Choi CJ. Interprofessional collaboration improves the odds of educating patients about PrEP over time. J Gen Intern Med. 2020;35(5):1444–1451. doi:10.1007/s11606-019-05616-0
3. Zambrotta ME, Aylward P, Roy CL, et al. Nurse-doctor co-teaching: a pilot study of the design, development, and implementation of structured interprofessional co-teaching sessions. Adv Med Educ Pract. 2021;12:339–348. doi:10.2147/AMEP.S300231
4. World Health Organization. Framework for action on interprofessional education & collaborative practice. Geneva, Switzerland: World Health Organization; 2010. Available from: https://www.who.int/publications/i/item/framework-for-action-on-interprofessional-education-collaborative-practice.
5. Shrader S, Hodgkins R, Bhattacharya S, Laverentz D, Johnston K, Jernigan S. Evaluating the impact of an interprofessional education program on workforce: recruitment, collaborative practice, and culture. J Interprof Educ Pract. 2022;2022:100495.
6. Alruwaili A, Mumenah N, Alharthy N, Othman F. Students’ readiness for and perception of Interprofessional learning: a cross-sectional study. BMC Med Educ. 2020;20(1):390. doi:10.1186/s12909-020-02325-9
7. Groessl JM, Vandenhouten CL. Examining students’ attitudes and readiness for interprofessional education and practice. Educ Res Int. 2019;2019:2153292. doi:10.1155/2019/2153292
8. Marrast LM, Chim C, Tocco J, et al. Expanding knowledge and changing attitudes about poverty: an interactive, interprofessional approach. J Prim Care Community Health. 2022;13:21501319221079446. doi:10.1177/21501319221079446
9. Sahoo R, Sahoo S, Kyaw Soe HH, Rai S, Singh J. Pre-University health professional students’ readiness and perception toward interprofessional education. Int J Appl Basic Med Res. 2022;12(1):4–8. doi:10.4103/ijabmr.ijabmr_440_21
10. Mette M, Baur C, Hinrichs J, Narciß E. Gaining interprofessional knowledge and interprofessional competence on a training ward. Med Teach. 2021;43(5):583–589. doi:10.1080/0142159X.2021.1885638
11. O’Connor S. An interprofessional approach: the new paradigm in nursing education. J Adv Nurs. 2018;74(7):1440–1442. doi:10.1111/jan.13530
12. Guraya SY, Barr H. The effectiveness of interprofessional education in healthcare: a systematic review and meta-analysis. Kaohsiung J Med Sci. 2018;34(3):160–165. doi:10.1016/j.kjms.2017.12.009
13. Khowaja-Punjwani S, Smardo C, Hendricks MR, Lantos JD. Physician-nurse interactions in critical care. Pediatrics. 2017;140(3):e20170670. doi:10.1542/peds.2017-0670
14. Ma C, Park SH, Shang J. Inter- and intra-disciplinary collaboration and patient safety outcomes in U.S. acute care hospital units: a cross-sectional study. Int J Nurs Stud. 2018;85:1–6. doi:10.1016/j.ijnurstu.2018.05.001
15. Reeves S, Zwarenstein M, Goldman J, et al. The effectiveness of interprofessional education: key findings from a new systematic review. J Interprof Care. 2010;24(3):230–241. doi:10.3109/13561820903163405
16. Han HY. Interprofessional education in medical education: can we break the silos? Korean Med Educ Rev. 2017;19(1):1–9. doi:10.17496/kmer.2017.19.1.1
17. Kim KH, Hwang E, Shin S. Current status and future direction of interprofessional education in nursing education. Korean Med Educ Rev. 2017;19(1):18–24. doi:10.17496/kmer.2017.19.1.18
18. Yune SJ, Park KH, Min YH, Ji E. Perception of interprofessional education and educational needs of students in South Korea: a comparative study. PLoS One. 2020;15(12):e0243378. doi:10.1371/journal.pone.0243378
19. van Gessel E, Picchiottino P, Doureradjam R, Nendaz M, Mèche P. Interprofessional training: start with the youngest! A program for undergraduate healthcare students in Geneva, Switzerland. Med Teach. 2018;40(6):595–599. doi:10.1080/0142159X.2018.1445207
20. Power A. Interprofessional education: shared learning for collaborative, high-quality care. Br J Midwifery. 2019;27(2):128–129. doi:10.12968/bjom.2019.27.2.128
21. Brydges CR. Effect size guidelines, sample size calculations, and statistical power in gerontology. Innov Aging. 2019;3(4):igz036. doi:10.1093/geroni/igz036
22. Parsell G, Bligh J. The development of a questionnaire to assess the readiness of health care students for interprofessional learning (RIPLS). Med Educ. 1999;33(2):95–100. doi:10.1046/j.1365-2923.1999.00298.x
23. Ennis KT. Assessing professional perceptions: design and validation of an interdisciplinary education perception scale. J Phys Ther Educ. 1990;4(2):95.
24. Lockeman KS, Dow AW, Randell AL. Validity evidence and use of the IPEC competency self-assessment, version 3. J Interprof Care. 2021;35(1):107–113. doi:10.1080/13561820.2019.1699037
25. Lee H, Kim IS, Lee TW, et al. Differences between perceived readiness for interprofessional learning in nursing and other health-related students. J Korean Acad Soc Nurs Educ. 2019;25(3):312–320. doi:10.5977/jkasne.2019.25.3.312
26. Park G, Kim S, Lee H, Cho J, Jin S, Yune S. Differences in attitudes to patient safety and readiness for interprofessional learning in medical students according by gender and grade. J Educ Innov Res. 2019;29(4):429–450.
27. Behling O, Law KS. Translating Questionnaires and Other Research Instruments: Problems and Solutions. Thousand Oaks, CA: SAGE Publications; 2000.
28. Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489–497. doi:10.1002/nur.20147
29. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. 1999;6(1):1–55. doi:10.1080/10705519909540118
30. Luecht RM, Madsen MK, Taugher MP, Petterson BJ. Assessing professional perceptions: design and validation of an Interdisciplinary Education Perception Scale. J Allied Health. 1990;19(2):181–191.
31. Lie DA, Fung CC, Trial J, Lohenry K. A comparison of two scales for assessing health professional students’ attitude toward interprofessional learning. Med Educ Online. 2013;18(1):21885. doi:10.3402/meo.v18i0.21885
32. Interprofessional Education Collaborative Expert Panel. Core competencies for interprofessional collaborative practice: report of an expert panel. Washington, DC: Interprofessional Education Collaborative; 2011. Available from: https://hsc.unm.edu/ipe/resources/ipec-2016-core-competencies.pdf.
33. Interprofessional Education Collaborative Expert Panel. Core competencies for interprofessional collaborative practice: report of an expert panel: 2016 update. Washington, DC: Interprofessional Education Collaborative; 2016. Available from: https://www.aacom.org/docs/default-source/insideome/ccrpt05-10-11.pdf.
34. Almalki A, Park YS, Tekian A. Needs assessment for interprofessional education: implications for integration and readiness for practice. Healthcare. 2021;9(4):411. doi:10.3390/healthcare9040411
35. Berger-Estilita J, Chiang H, Stricker D, Fuchs A, Greif R, McAleer S. Attitudes of medical students towards interprofessional education: a mixed-methods study. PLoS One. 2020;15(10):e0240835. doi:10.1371/journal.pone.0240835
36. Bridges DR, Davidson RA, Soule Odegard P, Maki IV, Tomkowiak J. Interprofessional collaboration: three best practice models of interprofessional education. Med Educ Online. 2011;16(1):6035. doi:10.3402/meo.v16i0.6035
37. Harden RM. Interprofessional education: the magical mystery tour now less of a mystery. Anat Sci Educ. 2015;8(4):291–295. doi:10.1002/ase.1552
38. Ketcherside M, Rhodes D, Powelson S, Cox C, Parker J. Translating interprofessional theory to interprofessional practice. J Prof Nurs. 2017;33(5):370–377. doi:10.1016/j.profnurs.2017.03.002
39. Jun SY, Park SH, Kong KR, Lee MI. A study on improvement of nursing clinical practice education: focusing on in-school practical education(fundamental nursing and health assessment). Korean Soc Nurs Res. 2020;4(1):51–64. doi:10.34089/jknr.2020.4.1.51
40. Kang S, Cho H, Kim D, Kwon H, Jung J. Medical Education Improvement Plan for Reinforcing Primary Care. Seoul, Korea: Korean Medical Association; 2017.
41. Lee SJ, Kim YM, Oh EG. Korean undergraduate nursing education: current status and developmental strategies as perceived by nursing educators and nurses. Korean J Adult Nurs. 2021;33(4):360–375. doi:10.7475/kjan.2021.33.4.360
42. Rettke H, Lehmann AI, Brauchli R, Bauer GF, Petry H, Spirig R. Capturing interprofessional collaboration between physicians and nurses in an acute care setting. A validation study of the revised German version of the Collaborative Practice Scales. J Interprof Care. 2020;34(2):211–217. doi:10.1080/13561820.2019.1629399
43. Rutherford-Hemming T, Lioce L. State of interprofessional education in nursing: a systematic review. Nurse Educ. 2018;43(1):9–13. doi:10.1097/NNE.0000000000000405
44. Aggarwal R, Mytton OT, Derbrew M, et al. Training and simulation for patient safety. Qual Saf Health Care. 2010;19(Suppl 2):i34–i43. doi:10.1136/qshc.2009.038562
45. Al-Jayyousi GF, Abdul Rahim H, Alsayed Hassan D, Awada SM. Following interprofessional education: health education students’ experience in a primary interprofessional care setting. J Multidiscip Healthc. 2021;14:3253–3265. doi:10.2147/JMDH.S318110
46. Khalili H, Orchard C, Laschinger HKS, Farah R. An interprofessional socialization framework for developing an interprofessional identity among health professions students. J Interprof Care. 2013;27(6):448–453. doi:10.3109/13561820.2013.804042
47. Meleis AI. Interprofessional education: a summary of reports and barriers to recommendations. J Nurs Scholarsh. 2016;48(1):106–112. doi:10.1111/jnu.12184
48. An J, Yi Y, Lee B. Analysis of media articles on COVID-19 and nurses using text mining and topic modeling. J Korean Acad Community Health Nurs. 2021;32(4):467–476. doi:10.12799/jkachn.2021.32.4.467
49. Tang M, Sun Y, Zhang K, et al. Associated factors of professional identity among nursing undergraduates during COVID-19: a cross-sectional study. Int J Nurs Sci. 2022;9(1):107–113. doi:10.1016/j.ijnss.2021.09.005
50. Castro MRH, Calthorpe LM, Fogh SE, et al. Lessons from learners: adapting medical student education during and post COVID-19. Acad Med. 2021;96(12):1671–1679. doi:10.1097/ACM.0000000000004148
51. Singh J, Matthees B. Facilitating interprofessional education in an online environment during the COVID-19 pandemic: a mixed method study. Healthcare. 2021;9(5):567. doi:10.3390/healthcare9050567
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.