")
Back to Journals » Vascular Health and Risk Management » Volume 19
The Mediating Effect of Self-Efficacy on Health Literacy and Social Support in Young and Middle-Aged Patients with Coronary Heart Disease After PCI
Authors Liu W, Yang W , Qian S
Received 3 May 2023
Accepted for publication 16 June 2023
Published 21 June 2023 Volume 2023:19 Pages 341—349
DOI https://doi.org/10.2147/VHRM.S417401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Wenqin Liu, Weili Yang,* Shuyan Qian*
DSA Center, The Second Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuyan Qian, DSA Center, The Second Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang Province, People’s Republic of China, Email [email protected]
Objective: To investigate the mediating effect of self-efficacy in the relationship between social support and health literacy among young and middle-aged patients with coronary heart disease following PCI.
Methods: A cross-sectional study was conducted on convenience samples of 325 young and middle-aged patients with coronary heart disease who underwent PCI within 1 to 3 months. The data were collected from the outpatient department of a tertiary general hospital in Wenzhou, China, between July 2022 and February 2023. The questionnaire format was utilized to gather data on demographic characteristics, social support, self-efficacy, and health literacy. A structural equation model was employed to establish and validate the pathways.
Results: The mean age of the patients included in the study was 45.32 years old, while their levels of health literacy, self-efficacy, and social support were 64.12± 7.45, 27.71± 4.23, and 65.53± 6.43 respectively. Significant associations were observed between social support and health literacy in the CHD population, with self-efficacy playing a partial mediating role. Together, social support and self-efficacy accounted for 53.3% of the variance in health literacy. The Pearson correlation analysis revealed a significant positive association between health literacy and both social support (r = 0.390, P < 0.01) and self-efficacy (r = 0.471, P < 0.01).
Conclusion: Social support exerted a direct impact on health literacy and an indirect effect on health literacy through self-efficacy among patients with CHD.
Keywords: social support, self-efficacy, health literacy, young and middle-aged patients, coronary heart disease, structural equation modelling
Introduction
Coronary heart disease (CHD), also known as coronary atherosclerotic heart disease, is a cardiovascular condition caused by the narrowing or obstruction of the coronary artery lumen, leading to myocardial ischemia, hypoxia or necrosis,1 it has a high incidence rate and mortality rate, and can result in various complications. Health literacy refers to the process of acquiring, comprehending, and utilizing health information and services in order to make informed decisions that promote personal well-being.2 Studies have demonstrated a significant correlation between lifestyle and disease coping styles with the onset and progression of chronic illnesses.3 Compared to solely focusing on clinical treatment effects, enhancing the self-health management level of patients with coronary heart disease is more significant in improving disease outcomes and quality of life,4 and the extent of self-health management is largely contingent upon an individual’s level of health literacy.5 Studies have indicated that individuals with low health literacy face challenges in accurately comprehending disease-related information, as well as accessing and evaluating health resources.6 Consequently, effective self-management of their health becomes difficult, leading to a higher incidence and prevalence of chronic conditions such as coronary heart disease, exacerbated physical discomfort symptoms, frequent mood fluctuations, increased activity limitations, and significant decline. The escalation of medical expenses.7
Hong demonstrated a strong correlation between health literacy and both educational attainment and race, thereby designating health literacy as the sixth vital sign following pain.8 Studies conducted by Driessens et al indicate that assessing patients’ health literacy during diagnosis and treatment is crucial for effective communication and the provision of comprehensive medical services.9 A number of domestic studies have demonstrated that individuals with higher levels of social support exhibit superior capacity to acquire health-related information and knowledge, as well as better control over disease symptoms, ultimately leading to improved patient health status and enhanced quality of life.10,11 Li et al discovered that social support had a positive impact on self-efficacy levels, while self-efficacy in turn facilitated the utilization of social support.12
Currently, research suggests a progressive increase in the incidence of coronary heart disease among young and middle-aged individuals aged 18–59 in China.13 Middle-aged and young individuals, as the primary workforce in society, occupy pivotal positions in both their professional and personal lives. If accompanied by coronary heart disease, it can have a more significant impact on their work and life, increase the economic burden, and exert immense pressure on society at large. Due to the increasing incidence of coronary heart disease among young and middle-aged patients in recent years, it is crucial to prevent recurrent cardiovascular events through cardiac rehabilitation after coronary angiography or stent implantation. This will enable patients to reintegrate into society with their illness while maintaining their ability to work and lead a fulfilling life.14 However, the majority of scholars tend to concentrate on the negative outcomes resulting from insufficient health literacy, while often neglecting the influence of social support systems on health literacy. Social support is a crucial determinant of psychological stress and health-related behaviors.15 Social support has a direct impact on an individual’s self-efficacy, promoting the establishment and adoption of healthy behaviors, as well as enhancing their adherence to treatment and self-management of health.16
The effectiveness of percutaneous coronary intervention (PCI) in improving myocardial blood flow, reducing coronary stenosis and occlusion, and decreasing mortality risk has been well-established. Additionally, research has demonstrated a 75% increase in hospital readmissions for coronary heart disease among individuals with low health literacy.17 The main aim of this study was to assess the health literacy levels of patients who underwent percutaneous coronary intervention (PCI) for coronary heart disease, with a specific focus on those in the young and middle-aged age groups. The study aimed to explore the determinants of health literacy among patients with coronary heart disease, and to establish a clear link between social support, self-efficacy, and health literacy in this population. Therefore, a structural equation model was constructed in order to investigate these variables. The aim of this study was to validate the relationship among the three variables, examine whether self-efficacy acts as a mediator between social support and health literacy, and establish a more robust theoretical foundation for self-management interventions in young and middle-aged patients with coronary heart disease after PCI. Additionally, it can serve as a basis for healthcare professionals to develop scientific and effective health education strategies that enhance patients’ self-management abilities.
Materials and Methods
Study Design and Participants
The convenient sampling method was utilized to administer a questionnaire survey among 325 young and middle-aged patients who had followed up with the cardiology outpatient department of a tertiary general hospital in Wenzhou, Zhejiang, China. The survey included the General Information Questionnaire, General Self-Efficacy Scale, Perceived Social Support Scale, and Health Literacy Scale. Data collected from July 2022 to February 2023. Inclusion Criteria: (1) Conform diagnostic criteria for coronary heart disease; (2) 18≤ aged <60, good cognitive and communication skills; (3) Agree and voluntarily participate in this research. The exclusion criteria are: (1) Severe mental disorders; (2) Patients with stage III or IV heart failure.
Measures
Demographic Questionnaire
This study employed a self-designed questionnaire to gather demographic information from participants, including age, gender, education level, marital status, monthly income, occupation type, medical insurance coverage and presence of other chronic illnesses.
Health Literacy Scale for Chronic Diseases
The scale was originally developed by Professor Jordan in 2010 and subsequently adapted by Professors Haolin Sun and Hua Fu, demonstrating its versatility across different contexts.18 The scale consisted of 4 different dimensions: information access (9 items), communication and interaction ability (9 items), willingness to improve health (4 items), and financial support (2 items), with a total of 24 items. The total score is between 24~120 points, the higher the score, the higher the level of health literacy, China’s assessment of health literacy level is: if the respondents score more than 80% (96 points), they have health literacy.19 Cronbach’s a in each dimension of the scale is 0.885~0.925; The retest reliability is 0.918.
General Self-Efficacy Scale
The source scale was compiled by Schwarzer, the Chinese version of the scale was translated and revised by Wang et al. The Cronbach’s a coefficient of the Chinese scale was 0.87, while the Cronbach’s a measured in this study was 0.89. The scale contained 10 items and was a single-dimension scale. The four-level scale was adopted, and the higher the score, the better the general self-efficacy of individuals. 10–19 is low level, 20–30 is medium level, and 31–40 is high level.20
Perceived Social Support Scale (PSSS)
The research scale was compiled by21 and revised by Qianjin Jiang. The scale consists of 12 items, 3 dimensions: family support (4 items), other support (4 items), friend support (4 items), and uses a Likert rating of 7, 1 means “strongly disagree”, 2 means “strongly disagree”, 3 means “slightly disagree”, 4 means “neutral”, 5 means “slightly agree”, 6 means “strongly agree”, 7 means “strongly agree”, a total score of 84 points, the higher the score is, the higher the water level is. Scores of 12 to 36 were low support, 37 to 60 were intermediate support, 61 to 84 were high support.22 The Cronbach’s α of the scale was 0.921, and the Cronbach’s α of family support, friend support and other support dimensions were 0.882, 0.886 and 0.793, respectively. The retest reliability is 0.926.
Data Collection
Participants are required to complete a set of questionnaires, including the Population Questionnaire, Chinese Health Literacy Scale, General Self-Efficacy Scale, and Perceived Social Support Scale. All questionnaires were completed by participants and collected by two trained researchers. In cases of illiteracy, the researchers verbally administered the questionnaire items and recorded responses on behalf of the subjects. During the process of data collection, patients who had undergone PCI for coronary heart disease were informed both orally and in writing about the confidential nature of the study as well as its voluntary participation requirements. Participants have the autonomy to withdraw from the study at any point in time and can rest assured that their decision will not impact the services they receive. Before we got any data, the participants signed some forms to give their consent. We made sure to keep all the info in a safe spot. The results are presented as an overview and do not relate to any one person specifically. We only used this data for our study and then destroyed it once we published our findings. Patients could fill out the questionnaire on their own or with help from us, and it took about 20–30 minutes in a quiet room at the clinic.
Statistical Analysis
The data analysis in this study was performed using SPSS version 25.0 and AMOS version 4.1, while demographic data was presented through frequency and percentage distributions to describe the types and prevalence. Mean and standard deviation were utilized to depict the aggregate scores of Health literacy (HL), Self-efficacy (SE) and Perceived social support (PSS). Any questionnaire containing more than three missing data points was excluded from the analysis due to its potential impact on the validity and reliability of the results. The independent samples t-test and ANOVA were employed to investigate the differences in demographic characteristics among individuals with hearing loss, speech disorders, and phonological processing deficits. The Pearson correlation coefficient was employed to assess the association among HL, SE, and PSS. A significance level of p<0.05 was considered statistically significant. Regression analysis was conducted using the testing program.23 Equation 1 examines the regression coefficient between the independent variable (social support) and dependent variable (health literacy); Equation 2 tests the regression between social support as an independent variable and self-efficacy as a dependent variable; Equation 3 performs a regression test with health literacy as a dependent variable, while self-efficacy and social support serve as independent variables.
Results
Distribution of Related Variables and Associations Among Them
In this study, a total of 325 young and middle-aged patients aged 18–59 years were assessed for their health literacy after undergoing percutaneous coronary intervention (PCI), comprising of 246 males and 79 females, with an average age of (45.32±7.07) years old. Univariate analysis revealed statistically significant associations between patients’ health literacy and gender, age, place of residence (Live), occupation, education level, marital status, number of children, income status, medical insurance coverage, smoking habits, disease course duration, number of health problems experienced by the patient, number of stents implanted and family history of CHD (P < 0.05) See Table 1.
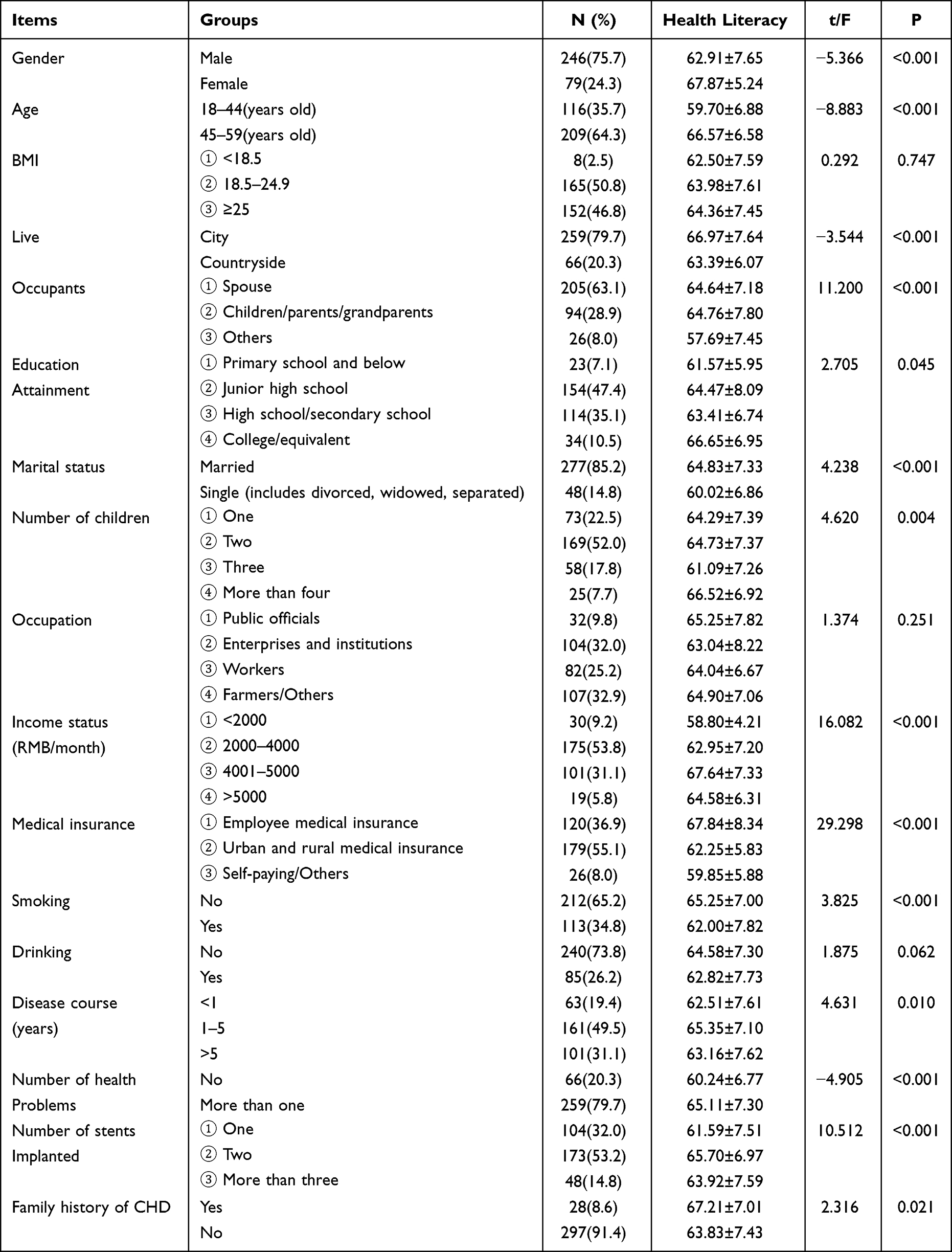 |
Table 1 Univariate Analysis of Health Literacy in Young and Middle-Aged Patients with PCI (N=325) |
Health Literacy, Self-Efficacy, and Social Support Among Young and Middle-Aged Patients Following Percutaneous Coronary Intervention for Coronary Heart Disease
The overall health literacy score was (64.12±7.45), with mean scores for each dimension of health literacy as follows: communication and interaction (26.96±3.498), information acquisition ability (17.46±3.70), economic support (4.90±1.39), and general understanding of health-related topics (14.80±2.29). The CHD patients’ total score in this survey ranged from 49 to 79 points, indicating low and insufficient health literacy levels. The self-efficacy scores of young and middle-aged patients with coronary heart disease who underwent PCI in this survey ranged from 16 to 38 points, with an average score of (27.71±4.23). The score for perceived of social support was (65.53±6.43), with family support (22.13±2.93), other support (relatives, colleagues, etc.) (21.82±3.36), and friend support (21.58±3.79) comprising the three dimensions assessed; notably, family support received a higher score See Table 2.
 |
Table 2 Scores of Health Literacy, Self-Efficacy and Comprehension of Social Support (N=325) |
Correlation Between Social Support and Health Literacy
The Pearson correlation analysis revealed a positive association between the scores and total scores of health literacy in young and middle-aged patients after PCI with the overall score of self-efficacy and social support (P<0.05). Table 3 presents the findings of the correlation analysis among health literacy, social support, and self-efficacy. In terms of health literacy as the dependent variable, a significant positive association was observed between social support and health literacy (r = 0.39, P < 0.01), as well as between self-efficacy and health literacy (r = 0.47, P < 0.01) See Table 3.
 |
Table 3 Correlation Among of Health Literacy, Self-Efficacy and Social Support (N=325) |
Test of the mode
Test of the mediating effect of self-efficacy in the association between health literacy and social support: employing social support as X, health literacy as Y, and self-efficacy as mediator M, while controlling for other relevant variables, we examined the mediating effect using Bootstrap sampling method with 2000 samples. The results are presented in Table 4 and Table 5, along with Figure 1.
 |
Table 4 Results of Process Distribution Regression Mediation Effect Test (N=325) |
 |
Table 5 Results of the Bootstrap Mediation Effect Test (N=325) |
 |
Figure 1 Diagram of the mediation effect model. Note: ***P<0.001. |
Based on the results of the distributed regression method’s mediation effect test, in the first step (model 1), there is a significant relationship between social support and health literacy (β=0.47, P<0.001), indicating that the total effect is valid. In the second model test, social support exerted a significant impact on the mediating variable’s self-efficacy (β=0.24, P<0.001). Furthermore, in the third step (model 3) test, both social support (β=0.32, P<0.001) and self-efficacy (β=0.64, P<0.001) significantly influenced health literacy. Therefore, the established model suggests a partial mediating effect of self-efficacy.
According to the analysis results presented in Table 5, it is evident that self-efficacy plays a significant mediating role in the model as tested by Bootstrap technique. The indirect effect value of 0.16 with a 95% confidence interval [0.10, 0.22] indicates that the indirect effect is valid and confirms the importance of self-efficacy in this model. Furthermore, the direct effect test’s confidence interval does not contain zero, indicating its significance. Based on the proportion of effects, self-efficacy accounts for 33% of the variance.
Discussion
Patients’ accurate comprehension of disease knowledge and relevant information serves as an indicator for evaluating the level of national health service development. This not only has a positive impact on maintaining their psychological and physiological well-being, but also plays a crucial role in reducing medical resource consumption and alleviating mounting medical pressure.24 In recent years, there has been a significant increase in the prevalence of coronary heart disease among young and middle-aged individuals, posing a pressing public health concern that cannot be overlooked.25 Relevant scholars posit that enhancing patients’ health literacy is conducive to elevating their self-health management proficiency, which holds significant value for disease prognosis and quality of life.26 Relevant scholars posit that enhancing patients’ health literacy is conducive to elevating their self-health management proficiency, which holds significant value for disease prognosis and quality of life.27 The findings of the survey indicate that young and middle-aged patients with coronary heart disease exhibit low levels of health literacy following PCI, as evidenced by their scores on measures assessing information acquisition and financial support. Notably, these scores were lower than those observed among hypertensive patients.28 The capacity to obtain information empowers patients to make informed health decisions by perusing health manuals, screening and applying the assimilated health information, thereby comprehending medical knowledge. Patients’ willingness to provide financial support denotes their behavioral aptitude to bear medical expenses for enhancing their well-being.29
The relationship among Social Support (SS), Self-Efficacy (SE), and Health Literacy (HL) in patients with chronic diseases has been the focus of numerous studies.30,31 However, the utilization of correlation or regression techniques can only uncover the direct impact on health literacy (HL). To date, few studies have elucidated the indirect effects among social support (SS), self-efficacy (SE), and HL in patients with coronary heart disease (CHD). Therefore, this current study has established an interaction pathway between SS, SE, and HL in CHD patients by constructing a model. The study’s findings suggest that patients with coronary heart disease possess a moderate level of health literacy, and there is a positive correlation between higher levels of health literacy and improved quality of life, which is consistent with previous research.32
Structural equation models demonstrate that Self-efficacy (SE) plays a crucial mediating role in the relationship between social support (SS) and health literacy (HL) among patients with coronary heart disease. SE exerts both direct and positive effects on HL, while also indirectly influencing it through its impact on SS (with an indirect effect coefficient of 0.16). Therefore, self-efficacy plays a crucial role as a mediator between social support and health literacy in patients with coronary heart disease. The impact of health literacy on these patients is moderated by their level of self-efficacy, which significantly influences other variables. The total effect of health literacy on patients is significantly indirect, with a total effect size of 0.47.33,34 Patients with higher levels of health literacy are more likely to engage in healthy behaviors and exhibit better disease management, as well as possess a heightened sense of self-efficacy.35 Furthermore, social support has a direct impact on health literacy, with a coefficient of 0.32. Empirical evidence suggests that social support can foster patients’ self-efficacy, alleviate psychological distress, and enhance their health literacy levels.3 Patients with higher levels of social support exhibit superior communication and interaction abilities. By increasing their disease awareness, patients develop a strong motivation to enhance their health, leading to an augmented demand for health-related knowledge and skills, ultimately resulting in improved health literacy. Patients with high levels of health literacy are able to effectively utilize the social support system in order to obtain both material and psychological support, which enables them to more effectively cope with their disease and improve their overall quality of life.
The study conducted had certain limitations that require attention. Firstly, the pathway linking Health Literacy (HL), Self-Efficacy (SE), and Social Support (SS) was derived from a cross-sectional study database. Therefore, it is crucial to conduct longitudinal and experimental studies in order to determine the causal approach within the model. Additionally, the study’s use of convenience sampling limits generalization of findings solely to patients with coronary heart disease in other countries. Thirdly, there exist other modifiable factors that may exert an impact on health literacy, and future research could expand upon the previous framework by taking these variables into account. Fourthly, the HL measurements employed in this study were functional and did not encompass infectious and critical literacy, which may be insufficient. However, functional HL is the most commonly used measurement method in Chinese mainland. These limitations should be taken into account in future studies.
Conclusions
The aim of this study was to assess the correlation among Patient Social Support (SS), Self-Efficacy (SE), and Health Literacy (HL) in patients with coronary heart disease (CHD), as well as to explore the direct and indirect effects between these variables. The results suggest a direct positive influence of self-efficacy on health literacy, and the combined effects of perceived social support for health and self-efficacy account for 67% of the total variance. Additionally, perceived social support for health not only exerts a direct impact on health literacy but also an indirect effect through self-efficacy. These research findings can be applied by healthcare professionals to enhance the quality of life among patients with coronary heart disease. Given the direct impact of social and emotional factors on quality of life, enhancing social and emotional well-being is crucial to improving the quality of life for individuals with CHD. One potential strategy to achieve this goal is to enhance health literacy. In clinical nursing, attention should be paid to the patient’s age, gender, marital status and other factors that may affect health education. This will help improve the self-management ability of patients with coronary heart disease and assist them in achieving better health outcomes through a scientific and reasonable health education system.
Ethical Approval
This study was approved by the Institutional Review Board of Directors of the Second Affiliated Hospital of Wenzhou Medical University, China (2022-K-77-02) in accordance with the principles outlined in the Declaration of Helsinki. Participants were informed that they could withdraw from or refuse participation at any time without penalty. All samples were deidentified prior to use.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sun C, Tan X. Development and trend of chronic disease research methods. Health Educ Health Promot. 2022;17(1):54–56.
2. Czerska I. Health literacy and its role in relational communication with patients: the study of literature and concepts. Eur Res Stud J. 2022;25(1):1.
3. Cui X, Wang J, Zhou S. Study on the status quo and influencing factors of health literacy in patients with coronary heart disease. Nurs Res. 2018;32(20):5. doi:10.12102/j.issn.1009-6493.2018.20.021
4. Huang Y, Gu Z, Sun G, Liu C, Gao C, Hu X. Correlation between health information literacy and self-management behavior and quality of life in patients with chronic heart failure. J Pract Clin Med. 2022;2022:1.
5. Wang Z, Shan Q, Liang L, et al. Correlation between mental health literacy and self-management behavior in elderly patients with coronary heart disease. Henan Med Res. 2022;31(8):4.
6. Bai J, Zheng S, Jiang B, Guo S. Mediating role of health literacy between social support and self-management in patients with unstable angina pectoris. J Beihua Univ. 2021;22(3):7. doi:10.11713/j.issn.1009-4822.2021.03.020
7. Wang Q, Xu X, Liu X. Relationship between health literacy and SSRS score in patients with angina pectoris after PCI. Chin Convalescent Med. 2022. doi:10.13517/j.cnki.ccm.2022.07.025
8. Hong J, Shin Y, Chang KW. Development of oral health literacy assessment tool for fifth and sixth grade elementary school students. J Korean Acad Oral Health. 2017;41(3):214. doi:10.11149/jkaoh.2017.41.3.214
9. Driessens H, van Wijk L, Buis CI, Klaase JM. Low health literacy is associated with worse postoperative outcomes following hepato-pancreato-biliary cancer surgery. HPB. 2022;24(11):1869–1877. doi:10.1016/j.hpb.2022.07.006
10. Liu L, Tian J, Zhang H, Li Y, Chen Y, Liu Y. Disease-related health literacy and social support in middle-aged and elderly hospitalized patients with coronary heart disease. J Nurs Adm. 2016;1:3.
11. Liu Z, Liu D, Guan J, Fan Y. Correlation analysis of health literacy, social support and health status in middle-aged and elderly patients with chronic diseases. Healthcare Guide. 2019;15:376. doi:10.3969/j.issn.1006-6845.2019.15.356
12. Li L, Xu N, Wang L. Moderating role of self-efficacy on the associations of social support with depressive and anxiety symptoms in Chinese patients with rheumatoid arthritis. Neuropsychiatr Dis Treat. 2017;13:2141–2150. doi:10.2147/NDT.S137233
13. Hu S, Yang Y, Zheng Z, et al. China cardiovascular disease report 2018. Chin Circ J. 2019;34(3):12.
14. Hu S, Wang L, Guo L. Expert consensus on sports rehabilitation after percutaneous coronary intervention. J Shanghai Univ. 2018;24(1):7. doi:10.12066/j.issn.1007-2861.2000
15. Liu L, Feng X. Study on health behavior and influencing factors of patients after coronary stent implantation. Essential Reading for Health. 2021;25:16–17.
16. Graven LJ, Grant JS. Social support and self-care behaviors in individuals with heart failure: an integrative review. Int J Nurs Stud. 2014;51(2):320–333. doi:10.1016/j.ijnurstu.2013.06.013
17. Rymer JA, Kaltenbach LA, Anstrom KJ, et al. Hospital evaluation of health literacy and associated outcomes in patients after acute myocardial infarction. Am Heart J. 2018;198:97–107. doi:10.1016/j.ahj.2017.08.024
18. Sun H, Peng H, Fu H. Study on reliability and validity of health literacy scale for chronic disease patients. Fudan J Med Edition. 2012;03:268–272.
19. Sun Y, Wang W, Lang Y, Zhang S, Yang F. Study on the status quo and influencing factors of health literacy of Chinese residents. Health Educ Health Promot. 2022;17(4):379–382.
20. Wang C, Hu Z, Liu Y. Research on the reliability and validity of general self-efficacy scale. J Appl Psychol. 2001;7(1):4. doi:10.3969/j.issn.1006-6020.2001.01.007
21. Dahlem NW, Zimet GD, Walker RR. The multidimensional scale of perceived social support: a confirmation study. J Clin Psychol. 1991;52(6):756–761. doi:10.1002/1097-4679(199111)47:63.0.CO;2-L
22. Yu Y, Yang Y, Xu M, Qin Z, Fu C, Li J. Understanding the mediating effect of social support on self-esteem and anxiety in patients with coronary heart disease; 2021.
23. Wen Z, Hou J, Zhang L. Comparison and application of moderating and mediating effects. Acta Psychol Sin. 2005;2:1.
24. Liao H, Xue L, Jiang J, Xue M. Health literacy of middle-aged and elderly patients with coronary heart disease and analysis of related factors. Prev Med South China. 2021;47(3):4.
25. Li X, Qiu H. Effects of self-management behavior on social support and quality of life in young and middle-aged patients with coronary heart disease. Chin Sanitary Eng. 2020;19(3):3.
26. Zhu R, Jiang Y. Study on correlation between health literacy and self-management behavior of rehabilitation exercise in stroke patients. Chin Sci Technol J Database Med. 2022;8:4.
27. Xie K, Wang Y, Zang X. The effect of health literacy on self-management behavior in patients with hypertension. Chin Gener Pract. 2020;23(3):6. doi:10.12114/j.issn.1007-9572.2019.00.780
28. Sang T, Ding S, Lu Y, Zhang W. The effect of health literacy on self-management behavior in patients with essential hypertension. Nurs Res. 2017;31(11):4. doi:10.3969/j.issn.1009-6493.2017.33.015
29. Fan H, Ma M, Zheng H, et al. Health literacy status and influencing factors of patients after first percutaneous coronary intervention. J Nurs. 2020;27(16):5. doi:10.16460/j.issn1008-9969.2020.16.035
30. Lee MK, Oh J. Health-related quality of life in older adults: its association with health literacy, self-efficacy, social support, and health-promoting behavior. Healthcare. 2020;8(4):407. doi:10.3390/healthcare8040407
31. Schmidt K, Faerch K, Zoffmann V, Amadid H, Varming AR. The process of health behaviour change following participation in a randomised controlled trial targeting prediabetes: a qualitative study. Diabet Med. 2022;39(4):e14748. doi:10.1111/dme.14748
32. Wang X, Tian X, Dong J, et al. Study on health literacy status and influencing factors of outpatients in general hospital. Chin Gener Pract. 2022;25(19):7. doi:10.12114/j.issn.1007-9572.2022.00.007
33. Chen X. To explore the influence of diversified health education on self-behavior management and self-efficacy in patients with coronary heart disease after percutaneous coronary intervention (PCI). Chin Sci Technol Period Database Med Health. 2022;10:3.
34. Lai X. Effects of cardiac rehabilitation exercise combined with self-efficacy intervention on health promotion behavior and quality of life in patients with PCI. Medical Diet Health. 2022;003:020.
35. Zhang Q, Zhu L, Jing L, Wang F, Zhang X, Xing F. Effect of self-efficacy and knowledge level of coronary heart disease on health literacy of young and middle-aged patients with coronary heart disease. Chin J Behav Med Brain Sci. 2018;27(3):4. doi:10.3760/cma.j.issn.1674-6554.2018.03.013
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.