Back to Journals » Cancer Management and Research » Volume 18

The Luo-Dingyuan Thyroid Vascular-Lymphatic Segmentation Classification: A Functional Anatomy-Based Framework to Facilitate Precision Management and Thyroid Function Preservation
Authors Luo D ![]()
Received 8 March 2026
Accepted for publication 7 May 2026
Published 19 May 2026 Volume 2026:18 607765
DOI https://doi.org/10.2147/CMAR.S607765
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kattesh Katti
Dingyuan Luo1– 3
1Department of Thyroid Surgery, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 2Department of Nutrition, University of California, Davis, CA, USA; 3Guangdong Provincial Key Laboratory of Malignant Tumor Epigenetics and Gene Regulation, Medical Research Center, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China
Correspondence: Dingyuan Luo, Email [email protected]
Background: Hypothyroidism remains a common and clinically significant consequence of thyroid surgery, frequently necessitating long-term or lifelong thyroid hormone replacement therapy, which may be associated with adverse effects on cardiovascular health and bone metabolism. In the era of treatment de-escalation, active surveillance and local ablation have emerged as important management. However, both require precise anatomical localization and rational definition of treatment boundaries. Therefore, a precise anatomical framework that enables function-preserving management without compromising oncologic safety is urgently needed. The study proposes and comprehensively describes a novel, anatomy-based segmental classification of thyroid, the Luo-Dingyuan Segmental Classification (Luo Segmental Classification), to explore its potential clinical applications.
Methods: The Luo Segmental Classification was developed through an integrated analysis of classical thyroid anatomy, vascular territories, and lymphatic drainage patterns. Each thyroid lobe is divided longitudinally into upper, middle, and lower thirds and further subdivided into anterior and posterior segments according to depth and vascular-lymphatic orientation, resulting in six reproducible segments per lobe. The isthmus and pyramidal lobe are defined as an independent anatomical unit. Potential clinical applications were evaluated conceptually in imaging, surgery, active surveillance, and ablation.
Results: The thyroid can be consistently divided into anatomically and functionally meaningful segments corresponding to distinct vascular and lymphatic territories. Based on this principle, the classification enabled standardized anatomical localization of thyroid nodules across ultrasonography (US), computed tomography (CT), and magnetic resonance imaging (MRI). Segment-based localization allowed precise description of tumor position, facilitated individualized treatment planning, and provided a unified anatomical language bridging radiology, surgery, pathology, and interventional therapy. Overall, this framework supported standardized reporting, individualized management, and potential reduction of unnecessary thyroid tissue loss and permanent hypothyroidism.
Conclusion: The Luo Segmental Classification provides an anatomy-based framework to promote precise and individualized management of thyroid cancer, support function-preserving strategies, and address unmet clinical needs.
Keywords: thyroid cancer, Luo segmental classification, vascular-lymphatic anatomy, hypothyroidism, function-preserving surgery
Introduction
Thyroid surgery is a cornerstone in the management of thyroid cancer.1 However, the traditional thyroid surgery, often based on lobectomy or total thyroidectomy, has been increasingly questioned.2,3 While these approaches ensure oncologic safety, they may lead to overtreatment in patients with low-risk disease. And the postoperative hypothyroidism remains one of the most frequent long-term complications, primarily resulting from the loss of functional thyroid tissue during surgical resection.4,5 A substantial proportion of patients require long-term or lifelong thyroid hormone replacement therapy, although generally safe, which may be associated with chronic adverse effects involving multiple organ systems, particularly the cardiovascular system and bone metabolism.6–8 These issues have prompted growing concern regarding the long-term quality of life of thyroidectomy patients.
Concurrently, high-resolution ultrasonography has enabled the detection of increasingly smaller thyroid nodules, leading to a rapid rise in the diagnosis of thyroid microcarcinomas.9,10 Accumulating evidence indicates that most thyroid microcarcinomas demonstrate indolent biological behavior, characterized by slow growth, limited invasion, and a low incidence of regional or distant metastasis.11 As a result, active surveillance has been widely accepted as a management option for carefully selected patients.12,13 During surveillance, tumor progression should be assessed using predefined and reproducible criteria, incorporating changes in tumor size, location-specific extension, and emerging features of lymphatic spread. A segment-oriented anatomical framework may facilitate consistent interpretation of serial imaging, enable earlier identification of clinically meaningful progression, and support timely transition from observation to intervention.
Current imaging modalities, including ultrasound (US), computed tomography (CT), and magnetic resonance imaging (MRI), generally localize thyroid tumors at the level of the right, left lobe, the isthmus, without further anatomic subdivision. However, papillary thyroid carcinoma (PTC) exhibits marked heterogeneity in lymphatic drainage, progression, and metastatic risk depending on intrathyroidal tumor location.14,15 Existing risk stratification systems largely treat the thyroid lobe as a homogeneous unit, which may explain the variability observed in lymph node metastasis and treatment outcomes.16–18 Prior attempts at thyroid segmentation have been limited to simple descriptive terms such as “upper/middle/lower thirds” in some surgical series, and no standardized vascular-lymphatic-based segmentation system has been established. However, comprehensive perioperative imaging-based structural assessment and longitudinal anatomical tracking are critical for evaluating treatment response and predicting long-term outcomes in patients with thyroid cancer.
With the increasing adoption of de-escalated management strategies, such as active surveillance, limited surgical resection, and image-guided ablation,18–20 there is a growing need for a reproducible, anatomy-based thyroid segmentation system that can be consistently identified on imaging and correlated with surgical and pathological findings. A refined segmental framework may facilitate a shared language among radiologists, surgeons, and endocrinologists, improve localization-specific risk assessment, and support more precise decision-making regarding intervention thresholds, and treatment extent. Therefore, the development of a functionally and anatomically grounded thyroid segmentation system represents an important step toward precision management of thyroid cancer.
Based on this background, we propose the Luo-Dingyuan Thyroid Vascular-Lymphatic Segmentation Classification (Luo Segmental Classification), a novel anatomical framework based on thyroid morphology, vascular territory, and lymphatic drainage patterns. This classification aims to facilitate precision-oriented thyroid management, and ultimately reduce the incidence of permanent hypothyroidism.
Methods
Anatomical Basis of the Luo Segmental Classification
Thyroid Morphology and Vertical Zonation
The thyroid gland is a three-dimensional organ with distinct upper, middle, and lower regions along its longitudinal axis, which consists of two lateral lobes connected by an isthmus, with an additional pyramidal lobe present in a subset of individuals, located anterior to the trachea and inferior to the larynx. Each thyroid lobe demonstrates a characteristic craniocaudal elongation, extending from the level of the thyroid cartilage superiorly to the upper tracheal rings inferiorly.21 This vertical morphology represents a fundamental structural feature of the thyroid and provides an essential anatomical basis for precise anatomical segmentation.
Arterial Supply and Its Role in Segmentation
The superior thyroid artery typically supplies the upper vertical zone of each lobe, including both anterior and posterior segments, and aligns with superficial and deep lymphatic pathways in this region. The inferior thyroid artery predominantly supplies the lower vertical zone, with branches extending to posterior segments that are closely related to the central compartment and tracheoesophageal groove. The middle vertical zone represents a transitional area with overlapping arterial territories from both superior and inferior sources, supporting its designation as a distinct functional region. Branching patterns also correlate with anterior-posterior differentiation. Anterior segments generally receive more direct, superficial arterial branches, whereas posterior segments are supplied by deeper branches following the posterior surface.22,23 Common vascular variations include absence of the inferior thyroid artery (up to 5% of individuals), presence of a thyroidea ima artery (3–10%), and accessory superior thyroid arteries.24 These variations may affect segmental boundary definition, but the classification remains applicable based on typical anatomy, and variations should be recognized preoperatively. This vascular orientation reinforces segmental boundaries and provides an anatomical rationale for functional and oncologic segmentation.
Venous Drainage and Its Role in Segmental Classification
Venous drainage of the thyroid gland follows a structured yet regionally differentiated pattern that complements arterial supply and lymphatic outflow. Rather than serving as an independent basis for segmentation, venous anatomy provides supportive evidence for functionally coherent intrathyroidal units. The superior thyroid veins predominantly drain the upper vertical zone of each lobe and accompany the superior thyroid artery, while the inferior thyroid veins primarily drain the lower zone through an inferior venous plexus. The middle thyroid veins contribute variably to venous outflow from the middle zone, reinforcing its transitional vascular character. Together, these venous pathways mirror the longitudinal organization of the thyroid gland. Venous drainage also differs by depth. Anterior portions of the thyroid tend to drain through more superficial venous channels, whereas posterior portions exhibit deeper venous outflow closely related to the tracheoesophageal groove and central compartment anatomy.23 This depth-dependent venous pattern aligns with the anterior-posterior differentiation incorporated in segmental classification.
Lymphatic Drainage and Its Segmental Implications
Lymphatic drainage of the thyroid gland demonstrates a structured and regionally oriented pattern that closely reflects intrathyroidal anatomy and tumor behavior. Along the longitudinal axis, lymphatic drainage from the upper thyroid region tends to follow superior cervical pathways, whereas lymphatic outflow from the lower region more frequently converges toward the central compartment. The middle region exhibits overlapping drainage patterns, consistent with its transitional anatomical position.15,25 This vertical organization parallels the upper-middle-lower framework used in the Luo Segmentation Classification.
Depth-related differences in lymphatic drainage further support anterior-posterior differentiation. Anterior portions of the thyroid are more commonly associated with superficial lymphatic channels, while posterior portions demonstrate closer anatomical relationships with the tracheoesophageal groove and central compartment lymphatics.26 These depth-dependent pathways are clinically relevant, as posteriorly located lesions may have a higher propensity for central compartment involvement.
Within the Luo Segmental framework, lymphatic drainage is incorporated as a primary anatomical determinant alongside arterial territories, with venous outflow serving as a complementary feature. The convergence of arterial supply, lymphatic orientation, and supportive venous drainage reinforces the concept that each segment represents a functionally coherent anatomical unit rather than an arbitrary geometric subdivision.
Definition of the Luo Segmental Classification
Segment Delineation
In the Luo Segmental Classification, each thyroid lobe is divided into three vertical zones-upper, middle, and lower-by two transverse planes approximating equal thirds of the lobe height. Each zone is further subdivided into anterior and posterior segments based on depth relative to the anterior thyroid capsule and vascular-lymphatic orientation. The arterial supply, venous drainage, and lymphatic drainage corresponding to each segment are summarized in Table 1, highlighting the vascular-lymphatic territories that form the basis of the Luo segmentation framework.
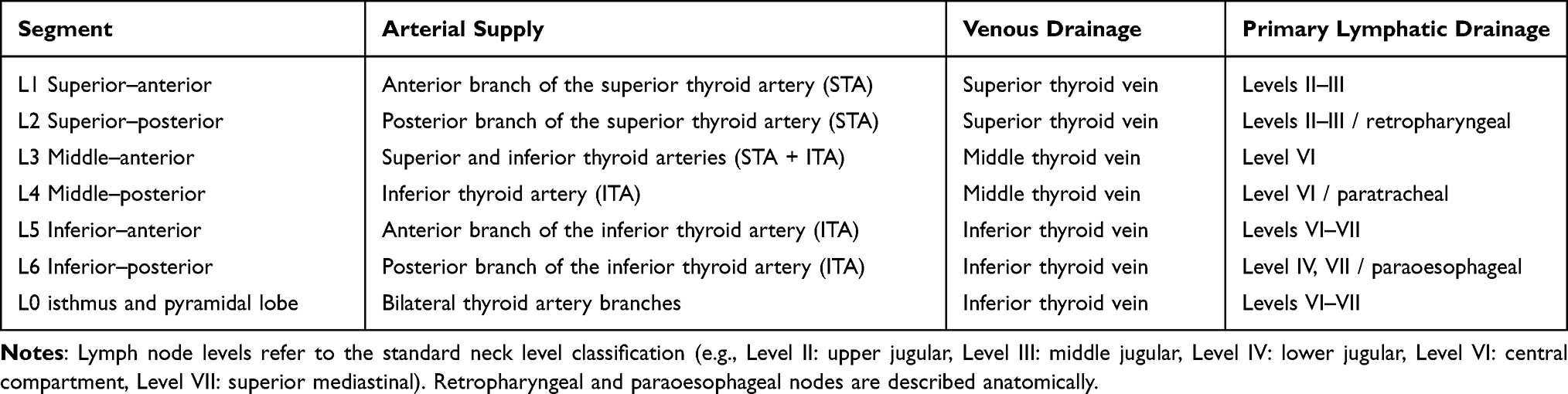 |
Table 1 Segmental Vascular Territories and Lymphatic Drainage of the Thyroid Gland |
This results in 6 reproducible Luo segments (L segments) per lobe (Figure 1):
- L1, Upper-Anterior Segment
- L2, Upper-Posterior Segment
- L3, Middle-Anterior Segment
- L4, Middle-Posterior Segment
- L5, Lower-Anterior Segment
- L6, Lower-Posterior Segment
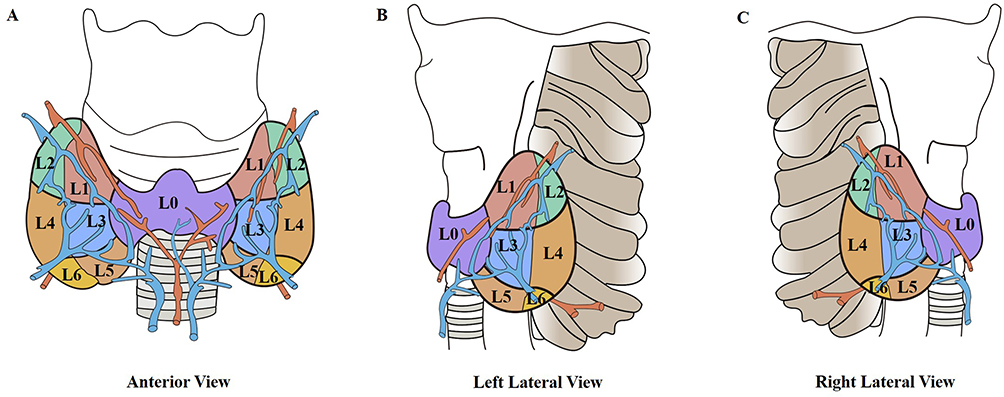 |
Figure 1 The Luo Segmental Classification of the Thyroid Gland. (A) Anterior view showing the six segments per lobe (L1-L6) and the isthmus/pyramidal lobe as Segment 0 (L0). (B) Left lateral view illustrating showing the left lateral six segments (L1-L6) and segment 0 (L0). (C) Right lateral view illustrating showing the right lateral six segments (L1-L6) and segment 0 (L0). |
The thyroid isthmus and pyramidal lobe are designated as an independent anatomical unit, referred to as Segment 0 (L0), owing to its unique morphology, vascular supply, and lymphatic drainage.
Relationship to Critical Structures
Posterior segments demonstrate closer proximity to the recurrent laryngeal nerve and parathyroid glands, whereas anterior segments are more superficial and amenable to minimally invasive intervention. Upper segments are closely related to the superior thyroid vessels and the external branch of the superior laryngeal nerve, while lower segments are anatomically associated with inferior thyroid vessels and central compartment lymphatics. Posterior segment depth is particularly relevant for assessing risk of local invasion into the trachea, esophagus, or recurrent laryngeal nerve, whereas anterior segment involvement is less likely to invade these structures.
Results
Applications in Ultrasonography, CT, and MRI Imaging
Imaging plays a central role in thyroid nodule evaluation, risk stratification, and treatment planning.27 The Luo Segmental Classification represents a standardized framework that provide a unified anatomical language, and may support more consistent cross-sectional and longitudinal interpretation of thyroid imaging across ultrasonography (US), computed tomography (CT), magnetic resonance imaging (MRI), and related modalities.
In US, segment-based localization enables more precise and reproducible description of nodule position relative to vertical level and depth within the thyroid lobe. While ultrasound is operator-dependent and less objective than CT for segmentation, the proposed segmental landmarks (vertical thirds and anterior-posterior depth) are readily identifiable on high-resolution thyroid US. Standardized training and the use of consistent acoustic windows may improve reproducibility. CT and MRI offer complementary objectivity, especially for posterior segments. Segmental annotation may also assist in correlating sonographic findings with surgical and pathological records.
CT and MRI offer complementary value in defining thyroid anatomy, particularly in assessing posterior segments and their relationship to the tracheoesophageal groove, esophagus, and central compartment. Within the framework, segment-based interpretation may facilitate evaluation of tumor extent, suspected extrathyroidal extension, and regional nodal involvement. This approach may be especially relevant in complex or recurrent disease, where precise anatomical localization is critical.
By providing a unified segmental reference applicable across imaging modalities, the classification may facilitate communication among radiologists, surgeons, and interventional specialists, thereby supporting more precise, individualized, and function-preserving management strategies.
Surgical Implications
Surgical management of thyroid cancer requires a balance between oncologic adequacy and preservation of thyroid function.28 The Luo Segmental Classification offers an anatomy-based framework that may support preoperative planning, intraoperative orientation, and postoperative documentation.
Segment-based localization enables more precise description of tumor position relative to vertical level and depth within the thyroid lobe, which may support individualized determination of surgical extent. By delineating functionally coherent vascular-lymphatic units, this framework may facilitate selective resection strategies aimed at preserving uninvolved thyroid tissue without compromising oncologic safety. Such an approach may be particularly relevant for low-risk, localized disease in which overtreatment remains a recognized concern. By “selective resection strategy” we refer to partial resection of a single segment (eg, L1 only for a small upper-pole tumor) or limited resection of two adjacent segments while preserving the rest of the lobe, rather than performing a conventional lobectomy or total thyroidectomy. This approach is analogous to segmentectomy in other organs (eg., lung or liver).
Intraoperatively, segmental orientation may improve spatial awareness of posterior segments adjacent to the tracheoesophageal groove and central compartment, potentially supporting assessment of recurrent laryngeal nerve risk and parathyroid preservation. Postoperatively, segment-based reporting may enhance consistency in operative records and facilitate correlation with imaging and pathological findings.
Overall, by providing a unified anatomical language, the classification may support more precise, function-preserving surgical decision-making and improve multidisciplinary communication in thyroid cancer management.
Role in Active Surveillance
Active surveillance (AS) has emerged as a management strategy for carefully selected low-risk thyroid cancers, emphasizing minimal intervention while monitoring disease progression.29 Within this context, the Luo Segmental Classification provides a standardized anatomical framework that may enhance the precision and reproducibility of nodule localization during follow-up.
Segment-based annotation allows for accurate longitudinal tracking of tumor position relative to vertical levels and anterior-posterior depth, improving the ability to detect subtle changes over time. This may facilitate consistent communication among radiologists, endocrinologists, and surgeons, and support early recognition of lesions that could necessitate intervention. In addition, segmental mapping can help correlate imaging findings with historical surgical or pathological records when evaluating recurrent or multifocal disease.
By integrating vascular-lymphatic architecture with AS protocols, segment-based localization may support function-preserving decision-making, minimize unnecessary surgery while maintain oncologic safety. Overall, the classification offers a practical tool to standardize anatomical reporting and optimize patient monitoring in the setting of active surveillance.
Guidance for Thermal Ablation
Thermal ablation has become an increasingly utilized minimally invasive treatment option for selected thyroid nodules, particularly low-risk papillary thyroid carcinomas, and symptomatic benign nodules.30 Segment-based localization enables precise identification of tumor position within vertical and anterior-posterior axes, which may support accurate probe placement and energy delivery while minimizing injury to adjacent critical structures such as the recurrent laryngeal nerve and parathyroid glands. By delineating functionally coherent vascular-lymphatic units, the classification may also assist in predicting potential pathways of tumor spread and in evaluating proximity to vessels that could affect ablation efficacy.
During follow-up, segment-based mapping allows consistent documentation of ablation sites and facilitates correlation with imaging, surgical, or pathological records when necessary. Overall, incorporating segmental anatomy into thermal ablation planning and monitoring may enhance precision, support function-preserving strategies, and improve multidisciplinary communication in thyroid cancer management.
Discussion
The Luo Segmental Classification represents a functionally oriented and anatomically precise approach to thyroid anatomy, developed to support precision medicine and contemporary strategies for treatment de-escalation. By integrating vertical zonation, anterior-posterior depth, arterial supply, venous drainage, and lymphatic architecture, the system provides clinically actionable anatomical resolution while remaining intuitive, reproducible, and readily applicable across imaging, surgical, and interventional contexts. This framework facilitates segment-based localization of tumors, supports function-preserving strategies, and enables standardized reporting that may improve multidisciplinary communication among radiologists, surgeons, and pathologists.
Importantly, the Luo classification is intended to complement, rather than replace, existing staging and risk stratification systems. While AJCC staging and ATA risk stratification primarily focus on prognostic factors,18,31 the Luo system emphasizes spatial localization, functional preservation, and the anatomical basis for individualized management. For small, early-detected PTC showing molecular, cytologic, or imaging features suggestive of high malignant potential, this framework may support selective, function-preserving thyroid resection. By providing a shared anatomical language, it also helps bridge the gap between diagnostic imaging, intraoperative orientation, and postoperative assessment, thereby enhancing the precision and consistency of patient care. This approach may be particularly relevant in low-risk or localized disease, where overtreatment is a recognized concern, as well as in complex or recurrent cases that require meticulous preoperative planning. The segmental classification may also be applicable to ectopic thyroids. For example, lingual or sublingual ectopic thyroids could correspond to upper segments (L1-L2), while mediastinal ectopic thyroids might involve lower segments (L5-L6) and possible thyroidea ima artery involvement. However, direct anatomical validation is currently lacking.
It is important to acknowledge several limitations of the present study. This work is conceptual and based on anatomical and imaging analyses. Future studies should assess interobserver reproducibility, correlations between segment-based localization and oncologic outcomes, and the impact of segment-guided management on postoperative thyroid function, complication rates, and patient quality of life. Integration of the Luo classification into guideline-based management algorithms, as well as its application in active surveillance, thermal ablation, and minimally invasive procedures, will be essential to fully realize its clinical utility. Moreover, the potential for incorporating emerging imaging modalities and computational tools, such as three-dimensional reconstruction and artificial intelligence-assisted mapping, may further enhance the applicability and precision of segment-based management in the future.
In summary, the Luo Segmental Classification provides a standardized, functionally oriented anatomical framework with the potential to address unmet needs in contemporary thyroid cancer care. By combining anatomical precision with practical clinical applications, it offers a platform for individualized, function-preserving management and may serve as a unifying reference across imaging, surgery, pathology, and interventional therapies. Continued validation and integration into clinical practice are necessary to determine its impact on patient outcomes and to establish its role within multidisciplinary thyroid cancer management strategies.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Scheller B, Culie D, Poissonnet G, Dassonville O, D’Andrea G, Bozec A. Recent advances in the surgical management of thyroid cancer. Curr Oncol. 2023;30(5):4787–8. doi:10.3390/curroncol30050361
2. Chen W, Li J, Peng S, et al. Association of total thyroidectomy or thyroid lobectomy with the quality of life in patients with differentiated thyroid cancer with low to intermediate risk of recurrence. JAMA Surg. 2022;157(3):200–209. doi:10.1001/jamasurg.2021.6442
3. Menegaux F, Lifante JC. Controversy: for or against thyroid lobectomy in>1cm differentiated thyroid cancer? Ann Endocrinol. 2021;82(2):78–82. doi:10.1016/j.ando.2021.03.004
4. Hu QL, Chen L, Kuo EJ, et al. A national study of postoperative thyroid hormone supplementation rates after thyroid lobectomy. Surgery. 2024;175(4):1029–1033. doi:10.1016/j.surg.2023.11.016
5. Shearn-Nance G, Politano S, Cabrera CI, et al. Development of hypothyroidism following hemithyroidectomy: a population-based study. Am J Otolaryngol. 2024;45(3):104239. doi:10.1016/j.amjoto.2024.104239
6. Holley M, Razvi S, Farooq MS, Dew R, Maxwell I, Wilkes S. Cardiovascular and bone health outcomes in older people with subclinical hypothyroidism treated with levothyroxine: a systematic review and meta-analysis. Syst Rev. 2024;13(1):123. doi:10.1186/s13643-024-02548-7
7. Li X, Zhang T, Zhang H, Liu S, Tian L. Effects of levothyroxine therapy on bone and mineral metabolism in hypothyroidism: a systematic review and meta-analysis. BMC Endocr Disord. 2025;25(1):11. doi:10.1186/s12902-024-01819-7
8. Yi W, Kim BH, Kim M, et al. Heart failure and stroke risks in users of liothyronine with or without levothyroxine compared with levothyroxine alone: a propensity score-matched analysis. Thyroid. 2022;32(7):764–771. doi:10.1089/thy.2021.0634
9. Jeon MJ, Kim WG, Chung KW, Baek JH, Kim WB, Shong YK. Active surveillance of papillary thyroid microcarcinoma: where do we stand? Eur Thyroid J. 2019;8(6):298–306. doi:10.1159/000503064
10. Bashir AA, El-Zaheri MM, Bashir AA, et al. Papillary thyroid microcarcinoma in thyroid surgical practice: incidental vs non-incidental: a ten-year comparative study. Cancers. 2025;17(12):2029. doi:10.3390/cancers17122029
11. Wang Z, Ji X, Zhang H, Sun W. Clinical and molecular features of progressive papillary thyroid microcarcinoma. Int J Surg. 2024;110(4):2313–2322. doi:10.1097/JS9.0000000000001117
12. Jeon MJ, Kim WG, Kim TY, Shong YK, Kim WB. Active surveillance as an effective management option for low-risk papillary thyroid microcarcinoma. Endocrinol Metab. 2021;36(4):717–724. doi:10.3803/EnM.2021.1042
13. Molinaro E, Campopiano MC, Pieruzzi L, et al. Active surveillance in papillary thyroid microcarcinomas is feasible and safe: experience at a single Italian center. J Clin Endocrinol Metab. 2020;105(3):e172–80. doi:10.1210/clinem/dgz113
14. Dou Y, Hu D, Chen Y, Xiong W, Xiao Q, Su X. PTC located in the upper pole is more prone to lateral lymph node metastasis and skip metastasis. World J Surg Oncol. 2020;18(1):188. doi:10.1186/s12957-020-01965-x
15. Shu X, Tang L, Hu D, et al. Prediction model of pathologic central lymph node negativity in cN0 papillary thyroid carcinoma. Front Oncol. 2021;11:727984. doi:10.3389/fonc.2021.727984
16. Tuttle RM, Alzahrani AS. Risk stratification in differentiated thyroid cancer: from detection to final follow-up. J Clin Endocrinol Metab. 2019;104(9):4087–4100. doi:10.1210/jc.2019-00177
17. Petranovic Ovcaricek P, Verburg FA, de Keizer B, et al. The 2025 ATA guidelines for differentiated thyroid Cancer - Ten years of professional debate and measured progress. Eur J Nucl Med Mol Imaging. 2025.
18. Ringel MD, Sosa JA, Baloch Z, et al. 2025 American Thyroid Association Management guidelines for adult patients with differentiated thyroid cancer. Thyroid. 2025;35(8):841–985. doi:10.1177/10507256251363120
19. Sturgeon C, Shaha AR, Yip L. Great debate: molecular testing and extent of surgery in well-differentiated thyroid cancer. Ann Surg Oncol. 2025;32(7):4597–4603. doi:10.1245/s10434-025-17348-z
20. Trimboli P, Deandrea M, Scappaticcio L, Piantanida R, Piccardo A. Thermal Ablation of T1N0M0 Thyroid Cancer. Radiology. 2025;317(1):e251383. doi:10.1148/radiol.251383
21. Ostrowski P, Bonczar M, Iwanaga J, et al. The prevalence and anatomy of the pyramidal lobe of the thyroid gland: a meta-analysis with implications for thyroid surgery. Clin Anat. 2023;36(6):937–945. doi:10.1002/ca.24062
22. Bruna-Mejias A, Perez-Farias C, Prieto-Heredia T, et al. A systematic review of anatomical variations of the inferior thyroid artery: clinical and surgical considerations. Diagnostics. 2025;15(15).
23. Mnatsakanian A, Al Khalili Y. Anatomy, Head and Neck, Thyroid Muscles. In: StatPearls. Treasure Island (FL): StatPearls; 2025.
24. Ozguner G, Sulak O. Arterial supply to the thyroid gland and the relationship between the recurrent laryngeal nerve and the inferior thyroid artery in human fetal cadavers. Clin Anat. 2014;27(8):1185–1192. doi:10.1002/ca.22448
25. Khafif A, Yosef LM. Para-tracheal neck dissection - is dissection of the upper part of level VI necessary? World J Otorhinolaryngol Head Neck Surg. 2020;6(3):171–175. doi:10.1016/j.wjorl.2020.02.009
26. Qian W, Ying W, Zhenlong Z, et al. Characterization of thyroid lymphatic drainage on real-time contrast-enhanced ultrasound: a mapping study in vivo. Ann Anat. 2025;264:152765. doi:10.1016/j.aanat.2025.152765
27. Bin Saeedan M, Aljohani IM, Khushaim AO, Bukhari SQ, Elnaas ST. Thyroid computed tomography imaging: pictorial review of variable pathologies. Insights Imaging. 2016;7(4):601–617. doi:10.1007/s13244-016-0506-5
28. Melcarne R, Giacomelli L, Grani G, et al. The overlooked outcome: decision regret in the surgical management of differentiated thyroid cancer. Ann Ital Chir. 2025;96(11):1427–1429. doi:10.62713/aic.4284
29. Yoon JH, Choi W, Park JY, Hong AR, Kim HK, Kang HC. Active surveillance for low-risk papillary thyroid carcinoma as an acceptable management option with additional benefits: a comprehensive systematic review. Endocrinol Metab. 2024;39(1):152–163. doi:10.3803/EnM.2023.1794
30. Zhao ZL, Wang SR, Kuo J, et al. 2024 International Expert Consensus on US-guided Thermal Ablation for T1N0M0 Papillary Thyroid Cancer. Radiology. 2025;315(1):e240347. doi:10.1148/radiol.240347
31. Santamaria-Barria JA, Graff-Baker AN, Chang SC, et al. Disparities in the impact of the AJCC 8th edition staging system on differentiated thyroid cancer outcomes. Head Neck. 2022;44(10):2129–2141. doi:10.1002/hed.27122
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.