Back to Journals » Patient Related Outcome Measures » Volume 7
The Long-Term Conditions Questionnaire: conceptual framework and item development
Authors Peters M, Potter C, Kelly L, Hunter C, Gibbons E, Jenkinson C ![]() , Coulter A, Forder J, Towers A, A'Court C, Fitzpatrick R
, Coulter A, Forder J, Towers A, A'Court C, Fitzpatrick R
Received 19 January 2016
Accepted for publication 26 April 2016
Published 30 August 2016 Volume 2016:7 Pages 109—125
DOI https://doi.org/10.2147/PROM.S104552
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Howland
Michele Peters,1 Caroline M Potter,1 Laura Kelly,1 Cheryl Hunter,1 Elizabeth Gibbons,1 Crispin Jenkinson,1 Angela Coulter,1 Julien Forder,2 Ann-Marie Towers,2 Christine A’Court,3,4 Ray Fitzpatrick1
1Health Services Research Unit, Nuffield Department of Population Health, University of Oxford, Oxford, 2Personal Social Services Research Unit, University of Kent, Canterbury, 3Nuffield Department of Primary Health Care Sciences, University of Oxford, Oxford, 4Broadshires Health Centre, Carterton, UK
Purpose: To identify the main issues of importance when living with long-term conditions to refine a conceptual framework for informing the item development of a patient-reported outcome measure for long-term conditions.
Materials and methods: Semi-structured qualitative interviews (n=48) were conducted with people living with at least one long-term condition. Participants were recruited through primary care. The interviews were transcribed verbatim and analyzed by thematic analysis. The analysis served to refine the conceptual framework, based on reviews of the literature and stakeholder consultations, for developing candidate items for a new measure for long-term conditions.
Results: Three main organizing concepts were identified: impact of long-term conditions, experience of services and support, and self-care. The findings helped to refine a conceptual framework, leading to the development of 23 items that represent issues of importance in long-term conditions. The 23 candidate items formed the first draft of the measure, currently named the Long-Term Conditions Questionnaire.
Conclusion: The aim of this study was to refine the conceptual framework and develop items for a patient-reported outcome measure for long-term conditions, including single and multiple morbidities and physical and mental health conditions. Qualitative interviews identified the key themes for assessing outcomes in long-term conditions, and these underpinned the development of the initial draft of the measure. These initial items will undergo cognitive testing to refine the items prior to further validation in a survey.
Keywords: long-term conditions, conceptual framework, qualitative interviews, patient-reported outcome measure
Introduction
Patient-reported outcome measures (PROMs) have been proposed as a means to measure what matters to patients to strengthen patient involvement in their care, to enable individualization of care,1 and to evaluate the performance and quality of care.2 It is generally agreed that a PROM should have a clear underlying conceptual framework,3–5 which specifies the specific goal of the measure, its intended use, and the target population.3,4 Although these criteria have been highlighted in particular for PROMs used in clinical trials, it is equally important that PROMs developed for use in other contexts, such as clinical practice or performance monitoring, are also developed to a high standard. It is recommended that an initial hypothesized conceptual framework be based on a literature review and expert opinion, and that this framework be further refined as domains and items are developed on the basis of in-depth qualitative and cognitive interviews.5
Long-term chronic conditions are the main challenge facing health and social care services today, due to their increasing prevalence, complexity, and impact on quality of life.6–10 Multimorbidity adds further to this challenge. Enhancing quality of life for people with long-term conditions (LTCs) by monitoring PROM scores is a key goal of health and social care policy in England and in other countries.11–14 The use of PROMs has been pilot-tested for six LTCs in primary care.15 This pilot study highlighted a number of challenges, including the reporting of PROM data (for one generic and six disease-specific PROMs) in a meaningful and concise manner across multiple LTCs.16 As no PROM exists to capture outcomes across all LTCs, the EuroQol five-dimension questionnaire (EQ-5D) is used in England to assess LTC outcomes, eg, as part of the GP Patient Survey.17 However, the EQ-5D may not capture all issues of importance to patients and clinicians. Therefore, professional and lay stakeholders support the development of a new measure for LTCs.18 The intention of this measure would be to capture issues of importance across LTCs and to offer a practical, easily interpretable, and useful method to assess outcomes across a range of health and social care services.
The aim was to develop a short self-completed questionnaire about issues of importance when living with LTCs. The intention was to develop a measure for use by adults with single and multiple morbidities, including both physical and mental health conditions. We intend it to be used for individual care and for population monitoring across all health and social care settings. The domains and items are intended to be complementary to those of the EQ-5D, and to reflect both traditional domains (ie, aspects of quality of life) and less traditional domains of importance in LTCs (eg, empowerment) that can be assessed by patient self-report. Following scoping reviews of the literature covering 12 key domains that can be assessed through patient reports and a stakeholder consultation,18 an initial conceptual framework was developed (see Table 1 for the initial framework).3,4 This article describes the refinement of the conceptual framework and the development of the thematic domains and initial items.
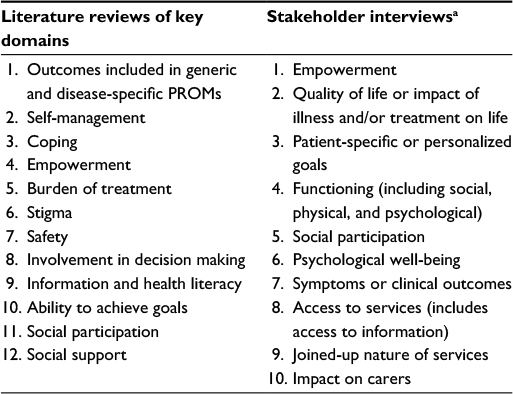 | Table 1 Initial domains in the conceptual framework for the development of the Long-Term Conditions Questionnaire Notes: aAdapted from Hunter C, Fitzpatrick R, Jenkinson C, et al. Perspectives from health, social care and policy stakeholders on the value of a single self-report outcome measure across long-term conditions: a qualitative study. BMJ Open. 2015;5(5):e006986.18 Abbreviation: PROMs, patient-reported outcome measures. |
Materials and methods
Qualitative interviews
Recruitment
Eight primary care practices in England (four in Oxfordshire and four in London) agreed to recruit people with at least one of ten specified LTCs from their patient database. The ten LTCs were selected by a panel composed of the authors, PROM experts, and lay advisors. The aim was to select maximally diverse LTCs (in terms of symptoms, bodily systems, disease trajectory, prevalence, likelihood of comorbidities, burden of disease and care, and level of self-management). To aid this process, the panel was provided with information on bodily systems, the World Health Organization Global Burden of Disease study,19 a study on multimorbidity,7 and the LTCs included in the Quality and Outcomes Framework (http://www.nice.org.uk/aboutnice/qof/qof.jsp). The following LTCs were selected: cancer, chronic obstructive pulmonary disease (COPD), ischemic heart disease (IHD), diabetes, depression, inflammatory bowel disease (IBD), multiple sclerosis (MS), osteoarthritis, schizophrenia, and stroke. Seven of these were selected by over half the panel, and three (IBD, MS, and schizophrenia) were selected by at least one panel member and included to contrast maximally with the other seven LTCs.
Practice staff conducted a search on the database comprised of the electronic patient record of all individuals registered with the practice. Search criteria were followed according to instructions developed and tested by one of the authors (CA). This search produced a list of patients with the relevant LTCs. Practices fed back the number of patients identified per LTC. The researchers used an online randomization tool (www.random.org) to generate random patient numbers per LTC. Practice staff then selected patients according to the randomization numbers from the list, and checked each patient against the inclusion and exclusion criteria. A total of 360 eligible patients were invited into the study. For LTCs with lifelong implications (COPD, diabetes, IBD, IHD, MS, osteoarthritis, and stroke), eligibility was defined as the presence of the LTC. Where full prolonged remission or cure is possible (cancer, depression, and schizophrenia), additional criteria in relation to duration of disease and/or current treatment were determined, similarly to the approach taken by Barnett et al.7 Additionally, the diagnosis needed to have been confirmed more than 12 months ago, to ensure that patients had time to adjust to their diagnosis and had experienced a range of services and strategies for the management of their LTC(s). Only adult patients were included (ie, 18 years of age and above). There was no upper age limit.
No participants with schizophrenia were recruited through primary care; therefore, the data were supplemented with interviews from a study conducted in 2013–2014 by RF and MP on outcomes valued by people with schizophrenia.20 Participants had been recruited through an email invitation by Rethink Mental Illness (https://www.rethink.org/about-us) and snowball sampling. The exact number of people receiving the invitation is not known, but 47 people made contact to participate. Of these 47, 13 were excluded due to not reporting a diagnosis of schizophrenia or schizoaffective disorder, five people refused to be interviewed, and seven failed to respond to emails after their initial contact. For the purposes of the study presented here, six transcripts of diverse participants (in terms of age and sex) were selected for secondary analysis.
Data collection
Eligible patients were sent a letter of invitation by the primary care practice and were asked to contact the researchers if they were interested in participating. Following initial contact that included confirmation of eligibility, the researchers arranged an interview time and location according to the preference of the participant; most interviews took place in participants’ homes, their workplace, or the University of Oxford. All participants gave written consent. The semi-structured interviews were conducted by CH, LK, and CP. All interviews were digitally audio-recorded.
The topic guide for the primary care participants (Table 2) was informed by our previous scoping literature reviews on PROMs and the key domains (Table 1), health care-policy documents (such as the National Health Service Outcomes Framework and the Social Care Outcomes Framework),21,22 and the stakeholder interviews.18 It focused on impacts and outcomes of LTCs, personal self-care strategies, help needed or received in managing LTCs (including experiences of health, social care, or community/voluntary services), and goals or problems regarding LTC management. In later interviews, participants were also invited to comment on emerging themes that were being considered as candidate items for a new PROM for LTCs. The schizophrenia topic guide (Table 2) was developed on the basis of a stakeholder consensus meeting and the literature.
 | Table 2 Topic guide for interviews |
Data analysis and development of items
The interviews were transcribed verbatim by a professional transcription company. All transcripts were verified and anonymized by the interviewers before analyzing the data in QSR NVivo 10, a qualitative software package. An iterative framework analysis was used.23 According to this approach, eight interviews were analyzed according to an initial coding framework drawing on the literature review and the stakeholder interviews.18 After discussion among the authors, the coding framework was expanded to take account of emerging themes, particularly those relating to social care; a further 18 interviews were analyzed using the expanded framework. CH, CP, and LK conducted the analysis, and MP and RF analyzed ten interview transcripts (five each). These ten transcripts were selected to represent a range of LTCs. The analysis framework was then discussed and further refined, before the remaining 22 interview transcripts (including the six schizophrenia transcripts) were analyzed. Once all transcripts had been coded, the framework was reviewed again, with no further changes made. Earlier transcripts were then recoded to incorporate the additional codes from the final framework.
A data-saturation table was created to evaluate if thematic saturation had been achieved. Saturation was defined as “the point in the data collection process when no new concept-relevant information is being elicited from individual interviews or focus groups”.4 The interview data were analyzed systematically and subsequently, and concurrently with data collection, using a constant comparison method moving between the codebook, the saturation table, and full transcripts,24 to determine if new themes emerged. Data collection was considered complete when no new relevant themes were emerging. As described earlier, the analysis framework was established following a review of the framework based on the analysis of 18 interviews. No further themes were added to the framework during the subsequent analysis.
Individual team members (MP, CH, LK, RF, CJ, and AMT) drafted candidate items based on a number of dimensions. Each dimension represented either one theme or subtheme from the qualitative analysis or two merged themes/subthemes. All the dimensions represented the refined conceptual framework underpinning the new measure. The candidate items were discussed in team meetings to identify and reach consensus on individual candidate items. Criteria for retaining candidate items included that they represented issues identified as important in the interviews (either to all the participants or important subgroups, such as social care users) and that they were deemed clear and easy to understand. Usually, duplicate items or those that significantly overlap (ie, represent similar underlying concepts) would also be removed in this process. However, the first draft of the questionnaire included a small number of items that were duplicates (as they were either worded positively and negatively) or that represented similar concepts. While this meant some items were very similar, it allowed pretesting differently worded items with people with LTCs in cognitive interviews.
Ethical approval
For the primary care participants, ethical approval was obtained through the National Research Ethics Service Committee London – Bromley. Ethical approval for the schizophrenia study had been gained through the East of Scotland Research Ethics Service. All participants signed an informed consent form.
Results
Participants
A total of 48 people with LTCs (42 recruited through primary care and six through the schizophrenia study) were interviewed (Tables 3 and S1 for details on participants). Participants reported a wide range of LTCs, in addition to the index LTC. Information on the use of social care was only available for the participants recruited through primary care, as the schizophrenia study did not directly ask about this.
 | Table 3 Characteristics of interview participants Abbreviations: LTCs, long-term conditions; COPD, chronic obstructive pulmonary disease; IHD, ischemic heart disease; TIA, transient ischemic attack; IBD, inflammatory bowel disease; MS, multiple sclerosis; OA, osteoarthritis. |
The overarching concepts and themes
Following the analysis, three overarching organizing concepts were identified to focus thinking about the emerging patterns of data in relation to living with LTCs: impact of LTC(s), experiences of services and support, and self-care. The three overarching concepts contained 22 themes; 16 themes were analyzed at this level only, and six themes contained 17 subthemes (Table 4). Impact of LTC(s) encompassed the largest range of themes with 15 themes, experience of services and support included four themes, and self-care was composed of three themes. The majority of the participants discussed aspects of each of the three overarching concepts.
 | Table 4 The three main overarching concepts, with their themes (•) and subthemes (○) identified within the interviews Abbreviation: LTCs, long-term conditions. |
Impact of LTC(s)
Participants described how their lives had been affected by their LTCs (Table 4). This included such issues as impact on day-to-day activities, emotional or mental well-being, and social participation, mentioned by more than 75% of participants, to such themes as impact on family or carers and loneliness, discussed by fewer than 35% of participants (Table 5).
 | Table 5 Themes, subthemes, numbers, and rank of interviews endorsing theme Note: Themes/subthemes in bold were considered for item development. Abbreviation: LTCs, long-term conditions. |
A 64-year-old woman with COPD, stroke, arthritis, agoraphobia, depression, IHD, gout, and stenosis of the spine described the impact of her LTC(s) on her physical health and daily activities:
[...] I can dress myself, except for when it comes to my feet, because I can’t get that far on my back, and my knees don’t move properly [...] so I can’t do that [...]. I’ll cook with a microwave, but I can’t prepare vegetables, but I can cook, but I can’t hold hot saucepans, and hot things, so if it’s just a matter of putting something in a microwave, I can do that. I just look to do the things I can do, like I can dust, my husband hoovers, I can’t manage the Hoover [...].
The ability to achieve personal goals was discussed by over half of the participants. Personal goals could relate to anything that participants valued; however, mostly it centered on work and family, but could also focus on the ability to look after pets or keep up with hobbies or physical activity. A 58-year-old woman explained how schizophrenia impacted on her work:
[...] I have a degree in psychology, I am a qualified counselor; I wanted to become an analyst. I mean, my career: every time I had a breakdown, it falls apart [...].
Maintenance of independence or becoming dependent formed a significant part of the impact of LTC(s). A 65-year-old woman with MS explained how a parking permit for disabled drivers helped her keep mobile and independent:
[...] I have a condition which is incurable, and in general what happens is you just get worse until you end up in a wheelchair, so I mean obviously my priority is keeping mobile, keeping independent, so independence and mobility is what would be my aim [...]. I think I’m independent, but frankly my blue badge is important to me for independence [...].
Experiences of services and support
In this concept, participants described the types of health and/or social care services they had used, their various types of support, and the burden caused by the services and care needed to manage their LTC(s). Support included help given by people or organizations outside health and social services, such as family members, friends or charities. The most frequently discussed themes (by over 75% of participants) were support by either services or others, and burden of treatment (Table 5). A 77-year-old man with IHD explained how hospital appointments could be difficult to manage:
[...] and it’s also planning sort of like work around hospital [...]. I seem to have so many hospital appointments these days, just seem to be [...] I get the impression that once they get hold of you, they’re never going to let you go [...].
In contrast, a 69-year-old man with cancer had found the input by health services helpful:
[...] impressed with the health service. One of the things that’s difficult I personally think is, like most others I suspect, it’s difficult to get a GP appointment when you actually want one, but I think once you’ve been identified as having something they have to treat, or believe that they will be able to help with treatment, I have to say I haven’t looked back. The treatment and care and the response I get from even the GP, I was transformed by that [...].
Additionally, as to whether services provide adequate support, participants also talked about how they were treated by health care professionals. A 66-year-old woman with cancer and IBD talked about contrasting experiences when consulting different doctors:
[...] there was only the two main doctors: the first one [doctor], he seemed very abrupt, very “doctorerfied” if that makes sense, whereas the other one was very casual in his mannerisms, and you felt you could talk to him [...].
However, it is not only health services that provide support. The importance of social support is explained by a 35-year-old male with IBD and chronic renal failure:
[...] we travel a lot. That’s partly because actually my wife forces me to, or has forced me to, and now I do it a lot more, and I enjoy it and I get a lot out of it. One role of the partner I think is potentially quite interesting: you know, I’ve had some amazing travel experiences over the last 4 years, partly because I’m with somebody I don’t worry as much about what might happen if I were ill and I was away, and also she absorbs [...] quite a lot of my angst, so that enables me to do those things [...].
Self-care
Self-care focused on actions or strategies that participants used to look after themselves and their LTC(s) or strategies to cope with their LTC(s). This included both active strategies, such as planning around the LTC(s), or passive strategies, such as acceptance of their limitations and reframing priorities. The most widely discussed theme (by over 75% of participants) was coping with LTC(s). Self-care had the potential to influence positively or negatively the impact of LTC(s). Participants differed in the extent to which they felt able to take positive actions, such as adopting healthier behaviors. There was also a time impact, with participants discussing variations in how well they could self-care during different time periods. When participants struggled with self-care, other problems could occur or the impact of LTC(s) could increase, or worsen the impact of the LTC(s), as explained by a 31-year-old man with depression and medication-induced psychosis:
[...] I’ve still got depression, I fight every day, I do fight it every day, but before where I’d let it sort of overtake me [...]. I could sit indoors for 2 weeks. I think there was about a time of 2–3 months where I was going to bed at 12 o’clock in the day and sleeping until 9 o’clock at night and then I’d wake up, and I’d sit the whole night like just watching TV, and all I’d eat was a bowl of Weetabix. I went down to 9 stone, I looked anorexic, and it just spiraled out of control [...].
A certain degree of own judgment and flexibility was often needed to find the best way to deal with the LTC(s). A 68-year-old woman described how she adapted to cope with the dietary changes needed to manage her diabetes:
[...] Initially I had to reeducate myself diet-wise [...] by nature I have a very bad sweet tooth, so I had to restrict my intake of sweets. But otherwise it wasn’t [...] but I’m somebody [that] once I know I have to do something, I condition my mind and just get on with it [...].
Acceptance of LTC(s), and the limitations this might impose, was explained by a 72-year-old man with four different morbidities, including diabetes and arthritis:
[...] I’ve had these various problems, starting with polio and asthma when I was very young. I’ve missed a fair bit of schooling through the polio, you just get sort of used to it, and you get one more thing to put up with and you get on with it. There’s no point in sitting around: you’ve got to make the best of things and you know, and fight back basically [...].
Item development
As it is the intention to develop a short measure for LTCs, it was not feasible to include items for each theme or subtheme from the interviews, although the three organizing concepts are represented in the items. Twenty themes or subthemes were taken into account in item development. These 20 themes or subthemes mostly ranked highly in terms of the number of interviews in which they were discussed. The lowest level of analysis was used for the ranking, meaning 18 themes and 17 subthemes. The 20 themes/subthemes selected for item development are highlighted in bold in Table 5, and they underpinned 17 dimensions (some themes collapsed for item development, eg, “Impact on day-to-day activities” and “Impact on emotional or mental well-being” were collapsed into “Impact of LTCs”) that were used to develop items (Table 6). The dimensions, representing the refined conceptual framework on which item development was based, are defined in Table 6, together with further illustrative quotes from the interviews. Themes that ranked less highly either significantly overlapped (ie, represented a similar underlying concept) with a more highly ranked theme (such as loneliness overlapping with social participation) or they were considered important for less represented groups in the sample. In line with the aim to develop a short measure, a small number of items (one to three) were developed per dimension to give a total of 23 initial items. These 23 items will undergo cognitive testing in further interviews with people with LTCs.
 | Table 6 LTCQ dimensions, qualitative themes, and illustrative quotes Abbreviations: LTC, long-term condition; LTCQ, Long-Term Conditions Questionnaire; MS, multiple sclerosis; COPD, chronic obstructive pulmonary disease; OA, osteoarthritis; IHD, ischemic heart disease; EPO, erythropoietin; IBD, inflammatory bowel disease; NHS, National Health Service; GP, general practitioner. |
Discussion
The aim of this study was to develop a measure for LTCs. The aim of this new PROM is to be relevant to adults with single or multiple LTCs (both physical and mental health conditions) and is intended for use at both an individual and a population-based level across all health and social care services. This qualitative study served to refine further the conceptual framework that was initially developed on the basis of literature reviews and stakeholder interviews. The use of in-depth qualitative interviews serves to enhance content validity of a newly developed measure.25
The in-depth interviews identified outcomes of importance to people with single and multiple morbidities. Due to the sampling strategies, the ten preselected LTCs were more commonly represented, but 23 additional morbidities were reported by the participants. The ten LTCs were chosen on the basis of their diversity, and together with other reported morbidities, a good spread of LTCs was reported by the 48 participants. The interviews generated rich data on a wide range of issues of importance to outcomes in LTC(s). These themes and subthemes formed three concepts: impact of LTC(s), experiences of services and support, and self-care.
Many of the themes, in particular those coded in “Impact of LTC(s)”, resonate with those that are often included in PROMs;26 however, some themes, such as self-management, empowerment, experiences of services, suitability of housing, or safety, may be explored less frequently as part of a PROM. These latter outcomes represent outcomes of care, rather than the more traditional outcomes of the condition or disease, but they are nonetheless important in LTCs. Also, these are frequently assessed by patient self-report, eg, self-management can be assessed by the Self-Management Ability Scale (SMAS)-30 questionnaire.27 Empowerment, on the other hand, is still considered ill-defined, and the need for a specific PROM to assess empowerment has been identified.28 Some would argue that experience of services is a process, not an outcome; however, recently it is becoming more widely recognized that health care and treatment, in particular in multimorbidity, can place a burden on people.29 Therefore, as the new measure intends to cover a broad range of issues of relevance in potentially very diverse LTCs, these issues have been included in the item development. The majority of themes/subthemes that underpinned item development ranked highly in terms of the number of participants who discussed them. There were some exceptions, eg, loneliness, safety, and suitability of housing, were talked about by fewer participants. However, these are considered important, either due to their impact on LTCs or due to their relevance to specific groups of people with LTCs. For example, such issues as suitability of housing and safety are of high importance for social care recipients, as demonstrated by the fact that such items are included in the Adult Social Care Outcomes Toolkit (ASCOT).30 Therefore, items based on these themes were also developed for the Long-Term Conditions Questionnaire (LTCQ).
While some PROMs, such as the SMAS-30 or the ASCOT, give scope to assess specific outcomes (self-management and outcomes in social care, respectively) in more depth, the ambition of the new measure is to be short and practical while assessing issues of importance in a wide range of LTCs. If outcomes in LTCs are to be assessed within clinical care or on a routine basis, it would not be practical if multiple different tools needed to be used with the same patient and across health and social care services. The items developed for the measure include less traditional but important outcomes. It is hoped that this approach will result in making the LTCQ a measure that is practical for use in the context of clinical care and routine PROM data collection. The candidate items for the new measure will be pretested in cognitive interviews before a large-scale survey is conducted to test the psychometric properties of the measure.
Some limitations of the study need to be acknowledged. First, although the sample included participants with a wide range of LTCs, there were proportionally fewer participants with mental health problems and few participants with experience of social care. This was not unexpected, as they represent smaller groups of people. In the process of selecting themes and refining the conceptual framework, it was ensured that themes that were valued by participants who were less represented were not excluded on the basis that they were not discussed by the majority of the participants. Also, the mental health sample was supplemented by interviews from a study on outcomes in schizophrenia, as no patient with schizophrenia invited through primary care agreed to participate. Although the method of recruitment and interview-topic guides differed between the two studies, many issues of importance (eg, treatment burden) overlapped with those reported in the primary care sample, as shown in Table 5. Also, plans for future testing will aim to include larger samples of people with mental health conditions and social care experience. A second limitation might be that a single method of data collection was used. Differences may have been found through using focus groups, although the extensive literature searches and stakeholder consultations give confidence that the main issues of importance for LTCs have been covered. A final limitation may be that LTCs were self-reported, even though participants were selected by GP practices on the basis of a formal diagnosis of a specific LTC. Participants may not have reported all their LTC(s), and issues of importance in relation to these would not have been discussed. Nevertheless, a wide range of LTCs has been included, and thematic saturation was achieved in the interviews. This gives confidence that the main issues of LTCs have been included, and that the resulting measure will have wide relevance.
Conclusion
This article describes the development of items for a new PROM for LTCs. On the basis of previously published interviews with stakeholders, literature reviews, and in-depth qualitative interviews, a conceptual framework was developed and refined. This framework served to develop 23 items to form the first draft of the new PROM. These items will be pretested in cognitive interviews to make any necessary amendments to ensure its relevance and validity before the new PROM – the LTCQ – is administered to a larger sample of people with LTCs in a survey to test its psychometric properties.
Acknowledgments
We would like to thank the participants with long-term conditions for taking part in this study, the CRN (Clinical Research Network) for supporting the recruitment of primary care practices, and the primary care practice staff for supporting the recruitment of people with long-term conditions. Furthermore, we would like to acknowledge the panel of experts who helped select the ten long-term conditions, and Dr Helen Lloyd and Dr Joanne Lloyd for conducting the schizophrenia interviews. This work was funded by the Policy Research Programme (PRP) in the Department of Health and by the National Institute for Health Research (NIHR). PRP funds the Policy Research Unit in the Quality and Outcomes of Person-Centred Care (QORU), a collaboration involving researchers in health and social care from the universities of Kent and Oxford and the London School of Economics (LSE). The NIHR funds the Oxford Collaboration for Leadership in Applied Health Research and Care (CLAHRC). The schizophrenia project was funded by the European Federation of Associations of Families with Mental Illness (EUFAMI).
Author contributions
RF, MP, CJ, AC, and JF conceived the study. CP, LK, and CH conducted and analyzed the qualitative interviews. CA developed and tested the search strategy for identifying eligible participants. MP led the writing of the manuscript, with the contribution of all other authors. All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work. The views expressed in this paper are those of the authors, and not necessarily those of the National Health Service, the NIHR, or the Department of Health.
References
Appleby J, Devlin NJ. Getting the Most out of PROMs: Putting Health Outcomes at the Heart of NHS decision-making. London: King’s Fund; 2010. | ||
Black N. Patient reported outcome measures could help transform healthcare. BMJ. 2013;346:f167. | ||
Turner RR, Quittner AL, Parasuraman BM, Kallich JD, Cleeland CS. Patient-reported outcomes: instrument development and selection issues. Value Health. 2007;10 Suppl 2:S86–S93. | ||
Rothman ML, Beltran P, Cappelleri JC, Lipscomb J, Teschendorf B. Patient-reported outcomes: conceptual issues. Value Health. 2007;10 Suppl 2:S66–S75. | ||
US Food and Drug Administration. Guidance for Industry: Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims. Silver Spring (MD): FDA; 2009. | ||
Pearson W, Bhat-Schelbert K, Probst J. Multiple chronic conditions and the aging of America: a challenge for primary care physicians. J Prim Care Community Health. 2012;3(1):51–56. | ||
Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43. | ||
Moth G, Vestergaard M, Vedsted P. Chronic care management in Danish general practice: a cross-sectional study of workload and multimorbidity. BMC Fam Pract. 2012;13:52. | ||
Anderson G, Horvath J. The growing burden of chronic disease in America. Public Health Rep. 2004;119:263–270. | ||
Fortin M, Lapointe L, Hudon C, Vanasse A, Ntetu A, Maltais D. Multimorbidity and quality of life in primary care: a systematic review. Health Qual Life Outcomes. 2004;2:51. | ||
UK Department of Health. The NHS Outcomes Framework 2013/14. London: MH; 2012. | ||
UK Department of Health. The Adult Social Care Framework 2014/15. London: MH; 2013. | ||
McGrail K, Bryan S, Davis J. Let’s all go to the PROM: the case for routine patient-reported outcome measurement in Canadian healthcare. Healthc Pap. 2012;11(4):8–13. | ||
Hjollund NH, Larsen LP, Biering K, Johnsen SP, Riiskjaer E, Schougaard LM. Use of patient-reported outcome (PRO) measures at group and patient levels: experiences from the generic integrated PRO System, WestChronic. Interact J Med Res. 2014;3(1):e5. | ||
Peters M, Crocker H, Jenkinson C, Doll H, Fitzpatrick R. The routine collection of patient-reported outcome measures (PROMs) for long-term conditions in primary care: a cohort survey. BMJ Open. 2014;4(2):e003968. | ||
Peters M, Crocker H, Dummett S, et al. Pilot Study of Patient Reported Outcome Measures (PROMs) in Primary Care. Oxford: University of Oxford; 2013. | ||
Mujica-Mota RE, Roberts M, Abel G, et al. Common patterns of morbidity and multi-morbidity and their impact on health-related quality of life: evidence from a national survey. Qual Life Res. 2015;24(4):909–918. | ||
Hunter C, Fitzpatrick R, Jenkinson C, et al. Perspectives from health, social care and policy stakeholders on the value of a single self-report outcome measure across long-term conditions: a qualitative study. BMJ Open. 2015;5(5):e006986. | ||
Murray CJL, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197–2223. | ||
Lloyd H, Lloyd J, Fitzpatrick R, Peters M. Outcomes that matter to people with schizophrenia: an in-depth study. Submitted. 2015. | ||
UK Department of Health. The 2013/14 Adult Social Care Outcomes Framework. London: DH; 2012. | ||
UK Department of Health. The NHS Outcomes Framework 2014/15. London: DH; 2013. | ||
Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In: Bryman A, Burgess R, editors. Analysing Qualitative Data. Abingdon, UK: Routledge; 1994. | ||
Kerr C, Nixon A, Wild D. Assessing and demonstrating data saturation in qualitative inquiry supporting patient-reported outcomes research. Expert Rev Pharmacoecon Outcomes Res. 2010;10(3):269–281. | ||
Brod M, Tesler LE, Christensen TL. Qualitative research and content validity: developing best practices based on science and experience. Qual Life Res. 2009;18(9):1263–1278. | ||
Fitzpatrick R, Davey C, Buxton M, Jones D. Evaluating patient-based outcome measures for use in clinical trials. Health Technol Assess. 1998;2(14):1–74. | ||
Schuurmans H, Steverink N, Frieswijk N, Buunk BP, Slaets JP, Lindenberg S. How to measure self-management abilities in older people by self-report: the development of the SMAS-30. Qual Life Res. 2005;14(10):2215–2228. | ||
McAllister M, Dunn G, Payne K, Davies L, Todd C. Patient empowerment: the need to consider it as a measurable patient-reported outcome for chronic conditions. BMC Health Serv Res. 2012;12:157. | ||
Eton DT, Ridgeway JL, Egginton JS, et al. Finalizing a measurement framework for the burden of treatment in complex patients with chronic conditions. Patient Relat Outcome Meas. 2015;6:117–126. | ||
Malley J, Towers AM, Netten A, Brazier J, Forder J, Flynn T. An assessment of the construct validity of the ASCOT measure of social care-related quality of life with older people. Health Qual Life Outcomes. 2012;10:21. |
Supplementary material
 | Table S1 LTCQ interview participants Abbreviations: LTC, long-term condition; LTCQ, Long-Term Conditions Questionnaire; COPD, chronic obstructive pulmonary disease; TIA, transient ischemic attack; IBD, inflammatory bowel disease; IHD, ischemic heart disease; MS, multiple sclerosis; OA, osteoarthritis. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.