Back to Journals » Nature and Science of Sleep » Volume 15
The Interplay Among Natural Menopause, Insomnia, and Cognitive Health: A Population-Based Study
Authors Shieu MM, Braley TJ, Becker J, Dunietz GL ![]()
Received 23 November 2022
Accepted for publication 8 February 2023
Published 14 February 2023 Volume 2023:15 Pages 39—48
DOI https://doi.org/10.2147/NSS.S398019
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Monica M Shieu,1 Tiffany J Braley,1 Jill Becker,2 Galit Levi Dunietz1
1Neurology, Medical School, University of Michigan, Ann Arbor, MI, USA; 2Psychology, Medical School, University of Michigan, Ann Arbor, MI, USA
Correspondence: Monica M Shieu, Division of Sleep Medicine, Department of Neurology, University of Michigan, Neurology, C728 Med Inn Building, 1500 E. Medical Center Dr, Ann Arbor, MI, 48109, USA, Tel +1 734-764-5415, Fax +1 734-232-9986, Email [email protected]
Purpose: The interrelationships among age at menopause, sleep, and brain health have been insufficiently studied. This study sought to examine the influence of age at natural menopause and insomnia symptoms on long-term cognitive function among US women.
Patients and Methods: Our study included a nationally representative cohort of US adults age 50+ from the Health and Retirement Study (2008– 2018). We restricted this cohort to 5880 women age 50+, from a diverse racial and ethnic groups. Age at menopause was retrieved from baseline (2008) for women having natural menopause. Five questions were used to identify women with insomnia symptoms (2010 and 2012): trouble falling asleep, nighttime awakenings, early morning awakenings, feelings of nonrestorative sleep, and use of sleep aids. A battery of four neuropsychological tests was conducted biennially (years) to evaluate cognitive function. Longitudinal associations between age at natural menopause and cognitive function were estimated with mixed effects models with a random intercept. Insomnia symptoms were examined as potential mediators or modifiers in the pathway between age at menopause and cognition.
Results: One year earlier in age at menopause was associated with a 0.49 lower mean in composite cognitive score, in any given survey year (adjusted p = 0.002). Earlier age at menopause was associated with higher risk of developing insomnia symptoms (eg, trouble falling asleep OR = 0.97; 95% CI: 0.96, 0.99), and insomnia symptoms were associated with worse cognitive performance (eg, trouble falling asleep, beta = − 0.5, p-value = 0.02). Therefore, insomnia symptoms could potentially mediate the association between age at natural menopause and cognition.
Conclusion: Earlier age at menopause is associated with a lower score in cognitive performance. This association may be mediated by insomnia symptoms. Our findings spotlight that among women who experience early menopause, there is the need for studies of sleep-based interventions to mitigate cognitive decline.
Keywords: age at menopause, cognitive performance, mediation, effect modification, natural menopause, population-based study
Introduction
Menopause is defined as the time of permanent cessation of ovarian function and transition from a reproductive to a non-reproductive phase of life. Menopausal transition is associated with changes in hormonal, physiological, and psychosocial symptoms which typically begins between age 45 and 55 and usually lasts about seven years.1 The average age at menopause for women in the US is 52 years (y).2 However, some women will experience menopause early, between age 40 to 45y (early menopause) and before age 40y (premature menopause). Early menopause has been linked to several adverse health effects including cardiovascular diseases, poor mood, sexual dysfunction, osteoporosis, cognitive impairment, and dementia.3,4
The association between reproductive aging and brain health, particularly cognitive impairment and dementia, has gained substantial attention recently. Prior studies have shown that women who transition to menopause early, either surgically5,6 or naturally,7,8 have an increased risk of cognitive impairment and dementia in late adulthood. During the menopausal transition, cognitive function may be affected in certain domains such as object recognition, object location performance, executive function, verbal memory and fluency, and verbal and spatial working memory.9
As sex hormones influence sleep, the declining ovarian function in postmenopausal women increases their risk of developing sleep disturbances and disorders, such as poor sleep quality, insufficient sleep duration, obstructive sleep apnea (OSA), restless legs syndrome, and insomnia.10 Sleep disorders, especially insomnia and OSA that are more likely to occur post-menopause, have been associated with worse cognitive functioning in women aged 50+.11,12 Specifically, OSA has been linked to cognitive impairment in attention, memory, executive function, psychomotor function, visuospatial deficits, and language abilities,13 while insomnia has been primarily linked to cognitive domains of attention, memory, and executive function.14 Furthermore, treatment of OSA showed a protective effect on incidence of cognitive disorders in older women and men.15
Poor sleep during menopausal transition is common and often negatively impact health in women.16,17 Among older women and men, insomnia has been linked to development and/or progression of Alzheimer’s disease (AD) through accumulation of amyloid-β, neurodegeneration-induced neuroinflammation, and disrupting neurogenesis.18 Previous reports have shown relationships between menopausal transition, insomnia symptoms and cognitive impairment, yet the joint influence of age at menopause and insomnia symptoms on cognitive function has been under-studied. Two separate pathways involving menopause, insomnia, and cognition were established in the literature. These relationships suggest that the pathway between age at menopause and cognitive function may be broken down into two separate pathways: 1) age at menopause and insomnia, and 2) insomnia and cognition. Yet, it is still unclear whether the causal pathway between age at menopause and cognitive impairment is mediated by insomnia (ie, insomnia as a consequence of menopause and determinant of cognitive function) or moderated by insomnia (ie, the effect of menopause on cognition is different among women with/without insomnia). Moreover, longitudinal assessments of domain-specific cognitive function rather than clinical diagnoses of cognitive impairment provide an earlier opportunity to monitor the trajectory of cognitive function post-menopause.
Therefore, this study examined associations among age at natural menopause, insomnia symptoms, and cognitive performance among midlife and older women, utilizing data from the Health and Retirement Study (HRS). Furthermore, we investigated the potential role of insomnia as a mediator or moderator of the associations between age at menopause and cognitive function. We hypothesized that insomnia symptoms would both mediate and moderate the association between menopause timing and cognitive function. Confirmation of these hypotheses could inform future research that targets sleep-based risk factors for cognitive impairment in women according to their menopausal transition experiences to mitigate cognitive decline in women in old adulthood.
Materials and Methods
The Health and Retirement Study (HRS)
A large, prospective longitudinal, nationally representative and diverse cohort of American adults age 50+, designed to investigate health implications of aging in the US population. Beginning in 1992, the biennial survey collects a wide-range of data on economics, sociology, demography, psychology, epidemiology, and medicine, with an oversample of Blacks and Hispanics. In each biennial interview, about 20,000 participants complete an extensive interview lasting a few hours. Half of the sample receives face-to-face interview while the other half is assigned to telephone interview and then modes are alternated each wave. Participants are followed longitudinally until death (an exit interview is conducted with a proxy) and a new sample is replenished every six years with individuals aged 51–56.19 Prior to each interview, study participants are provided with a written informed consent form. All participants are read a confidentiality statement, and give oral consent by agreeing to do the interview. The HRS follow the University of Michigan Health Sciences/Behavioral Sciences Institutional Review Board Protocol (HUM00061128).20
In our study, health information of the HRS participants from the core dataset from 2008 (baseline) up to 2018 were utilized, as detailed menopausal-related questions became available in the 2008 wave. To examine cognitive consequences of natural transition to menopause, we excluded women who reported hysterectomy, as their final menstrual period is unknown, or women who reported surgical transition to menopause through oophorectomy.
This study was given “exempt and not regulated” status by the Medical School Institutional Review Board (IRBMED) at the University of Michigan (HUM00204196).
Study Variables
Exposure: Age at Menopause
In the 2008 wave, the HRS included questions on menopause timing and type of menopause. Women who reported natural menopause prior to surgical menopause or went through natural menopause were included in the analysis. Age at menopause was derived from the question “about how old were you when you finished going through menopause?”. Women who reported age at menopause before age 18y (n = 23) or women whose had missing age at menopause (n = 994) were excluded from the analysis due to potentially atypical, pathological trajectory of reproductive aging. Age at menopause was retrieved from baseline information.
Cognitive Outcomes
A battery of cognitive tests was asked in the HRS core interviews to objectively examine cognitive function among study participants. Cognitive tests were primarily drawn from the Telephone Interview for Cognitive Status (TICS) screen while keeping the cognitive assessment sufficiently short to minimize respondent burden. The TCIS has excellent sensitivity and specificity in differentiating AD from normal cognition.21 The battery of cognitive tests included immediate and delayed 10-noun recall, serial seven subtraction test, and backwards number counting. A 27-point composite cognitive score composed of scores from the immediate (assess memory; maximum: ten points) and delayed 10-noun recall test (assess memory; maximum: ten points), serial seven subtraction test (assess working memory; maximum: five points), and a backwards count from 20 test (assess attention and mental processing speed; maximum: two points) were calculated using a validated algorithm.22,23 Imputed data of cognitive measurement provided by the HRS were used to account for missing data. Imputations were performed for respondents with missing cognition data using a multivariate, regression-based procedure with Imputation and Variance Estimation (IVEware) software. A combination of relevant demographic, health, and economic variables, along with prior and current wave cognitive variables were included to assist imputations.24
Potential Mediator or Moderator: Insomnia Symptoms
Four insomnia symptoms data were collected in 2010 and 2012; trouble falling asleep, nighttime awakenings, early morning awakenings, and feelings of nonrestorative sleep. Women were classified as having insomnia symptoms if they responded “most of the time” to any symptom, versus “sometimes” and “rarely or never”. In addition, usage of sleep aids was dichotomized into yes/no. We then constructed an insomnia composite score from these four symptoms (ie, trouble falling asleep, nighttime awakenings, early morning awakenings, and feelings of nonrestorative sleep). Insomnia symptoms that were reported occurring “most of the time” were included in the composite score (range: 0–4).
Covariates
Baseline (2008) demographic variables included age, sex, and race/ethnicity. Based on their race/ethnicity, women were classified into four groups: Hispanic; non-Hispanic White; non-Hispanic Black/African American; and non-Hispanic/other race. Hypertension and diabetes were defined by either of two criteria: self-report of physician diagnosis or self-reported use of condition-specific medications. Depression was defined by positive answer to “During the last 12 months, was there ever a time when you felt sad, blue, or depressed for two weeks or more in a row?” and answers of all day long or most of the day to “During that time did the feelings of being sad, blue, or depressed usually last all day long, most of the day, about half the day, or less than half the day?” or answers of every day or almost every day to “During those two weeks, did you feel this way every day, almost every day, or less often than that?”. Marital status was classified as married or cohabiting respondents versus others. Parity was obtained from the question “How many children have you given birth to?”. This question excluded miscarriages, still-births, adopted or step-children. Physical activity was presented as a Metabolic Equivalent (MET) score, accounting for frequency of mild activity, moderate activity, and vigorous activity.25 The final MET score ranged from 0 to 16.33.
Statistical Analysis
Descriptive statistics were presented as proportions (categorical variables) and as means and standard errors (continuous variables). We calculated the weighted prevalence and mean for the entire sample. Total individual weights were divided by household size within a household to balance the sum of the individual weights with the number of people in that household.
In sub-sample analysis we utilized appropriate procedures to estimate unbiased standard errors.
We investigated the longitudinal associations between age at menopause and cognitive performance. Repeated cognitive scores (composite) obtained from 2008 to 2018 were modeled as the outcome. Each individual cognitive test score was treated as repeated outcome in separate models. Survey weights were included in all regression models to account for differential selection probabilities and potential non-response bias. Best final models were selected by likelihood ratio tests. Sandwich variance estimators were calculated for the fixed effect and the variance. Adjusted coefficient (β) and p value were obtained in weighted mixed models with a random intercept and unstructured covariance. All models were adjusted for age at baseline, race/ethnicity, education, parity, physical activity, survey year with the interaction term of age at baseline and age at menopause. We considered diabetes, hypertension, and depression as potential mediators in the pathway between age at menopause and cognitive performance, thus they were excluded from the regression models.
We further examined whether insomnia symptoms modified the association between age at menopause and cognitive performance in a sample stratified by individual insomnia symptom (trouble falling asleep, nighttime awakenings, early morning awakenings, feelings of nonrestorative sleep, usage of sleep aids, and insomnia composite score). Mixed linear models with a random intercept and unstructured covariance were adjusted for age at baseline, race/ethnicity, education, parity, physical activity, and survey year with the interaction term of age at baseline and age at menopause.
Finally, as formal mediation analysis is not available for repeated outcomes, we examined the potential mediation role of insomnia symptoms by deconstructing the indirect pathway between age at menopause and cognitive performance, through insomnia into two pathways. First, we estimated associations between age at menopause and insomnia symptoms, and then examined the relationship between insomnia symptoms and cognitive performance. Logistic regression and linear regression models were used to investigate the first pathway, between age at menopause and insomnia symptoms as categorical and continuous outcomes, respectively. Mixed linear models with a random intercept and unstructured covariance were applied to the second pathway, between insomnia symptoms and cognitive performance. All models were adjusted for age at baseline, race/ethnicity, education, parity, physical activity, and survey year.
SAS 9.4 was used to perform all the analyses. Strata, 2008 HRS household-level, and respondent-level survey weights were accounted for in the models.
Results
This analysis included 5880 women. Weighted summary statistics of demographic, health, and lifestyle characteristics by timing of the menopausal transition are presented in Table 1. The mean age of HRS participants was 74.7 years (±0.1) and 82% were non-Hispanic Whites.
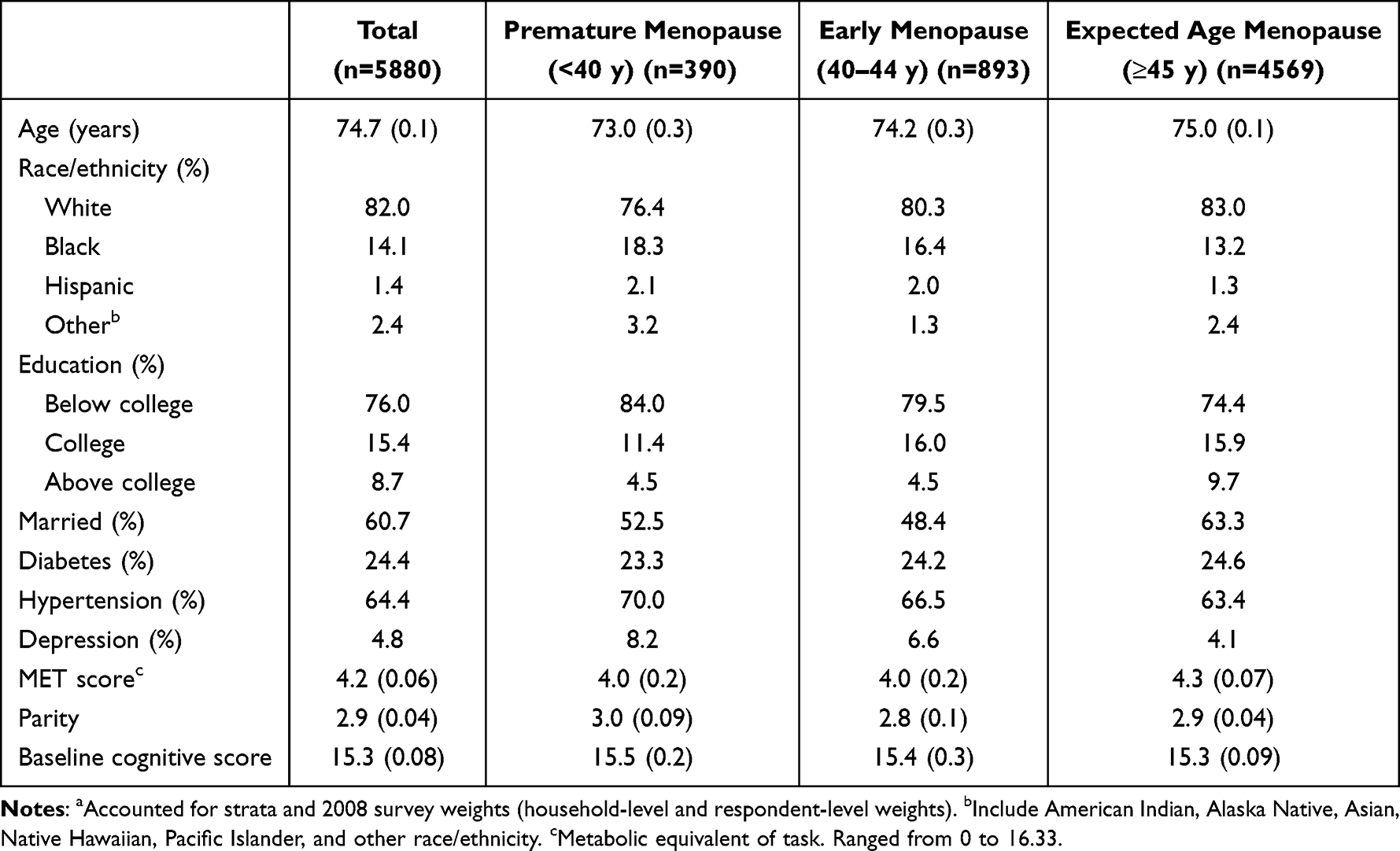 |
Table 1 Summary Statistics-Weighteda Proportion (%) or Weighteda Mean (and Standard Error)-of Selected Variables, by Menopause Group; Total Study Population, Baseline (2008) |
Table 2 displays longitudinal associations between age at menopause and composite cognitive scores among all respondents from linear mixed models with a random intercept. Overall, one year earlier in age at menopause was associated with a 0.49 lower mean in composite cognitive score, in any given survey year (p = 0.002).
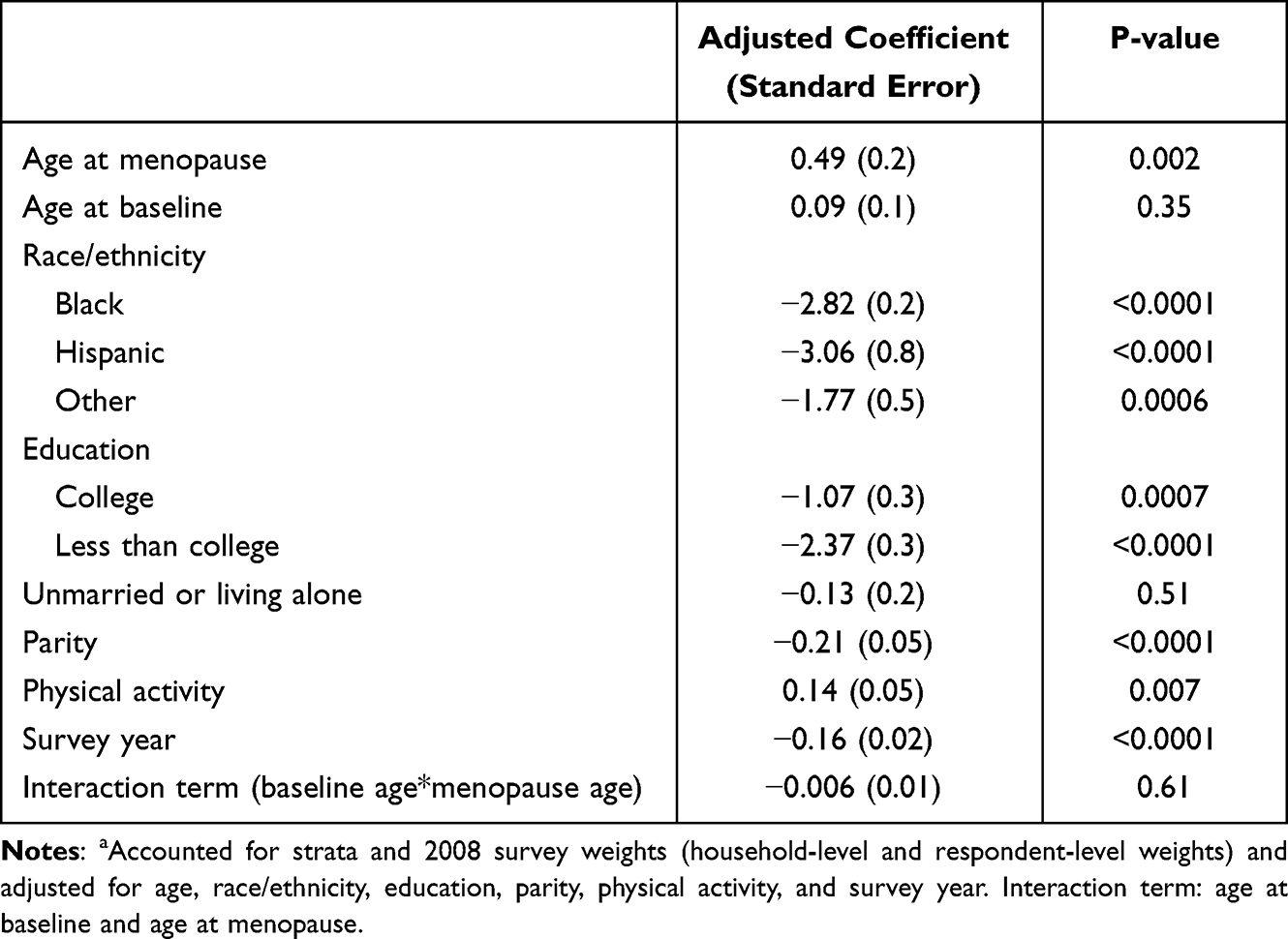 |
Table 2 Estimated Association (Adjusteda Coefficient and Standard Error) Between Age at Menopause (Exposure) and Composite Cognitive Score (Outcome) for the Total Study Population from the Linear Mixed Model with a Random Intercept, 2008–2018 |
Results from mixed linear models with individual cognitive tests are presented in Table 3, suggesting that in any given survey year, one year earlier in age at menopause was associated with a 0.14 lower mean in immediate word recall score (p = 0.01). No significant differences were seen with delayed word recall score, the serial 7’s task, or backward count scores.
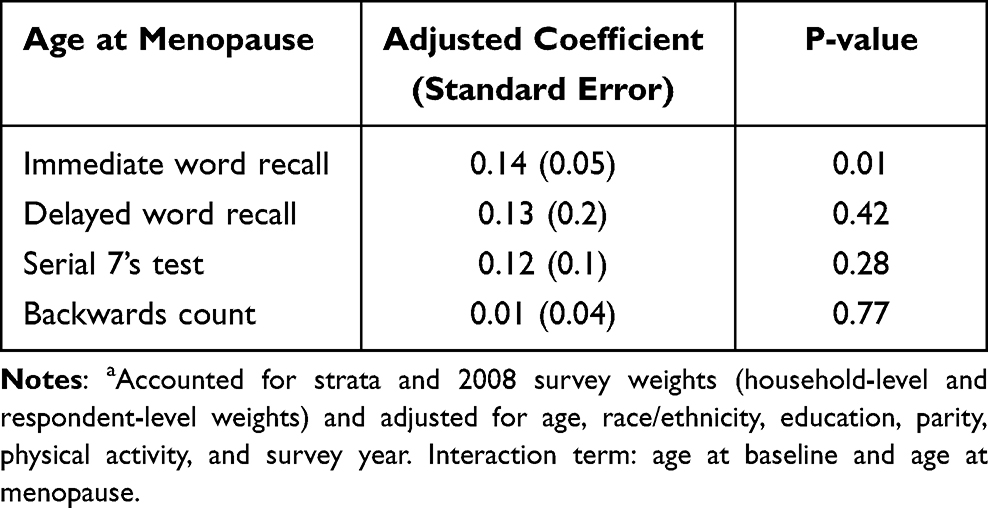 |
Table 3 Estimated Association (Adjusteda Coefficient and Standard Error) Between Age at Menopause (Exposure) and Individual Cognitive Score (Outcome) for the Total Study Population from the Linear Mixed Model with a Random Intercept, 2008–2018 |
In a stratified analysis, we examined the potential moderation of insomnia symptoms on the association between age at menopause and composite cognitive score (Table 4). We found statistically significant associations between age at menopause and composite cognitive score in stratified sample by insomnia symptoms. However, interaction terms (age at menopause and insomnia symptoms) in our regression models were not statistically significant, suggesting the absence of moderation by insomnia. The greatest magnitude in the association between age at menopause and composite cognitive score was shown in women who reported usage sleep aids; one year earlier in age at menopause was associated with a 0.96 lower mean in composite cognitive score, in any given survey year (p = 0.002).
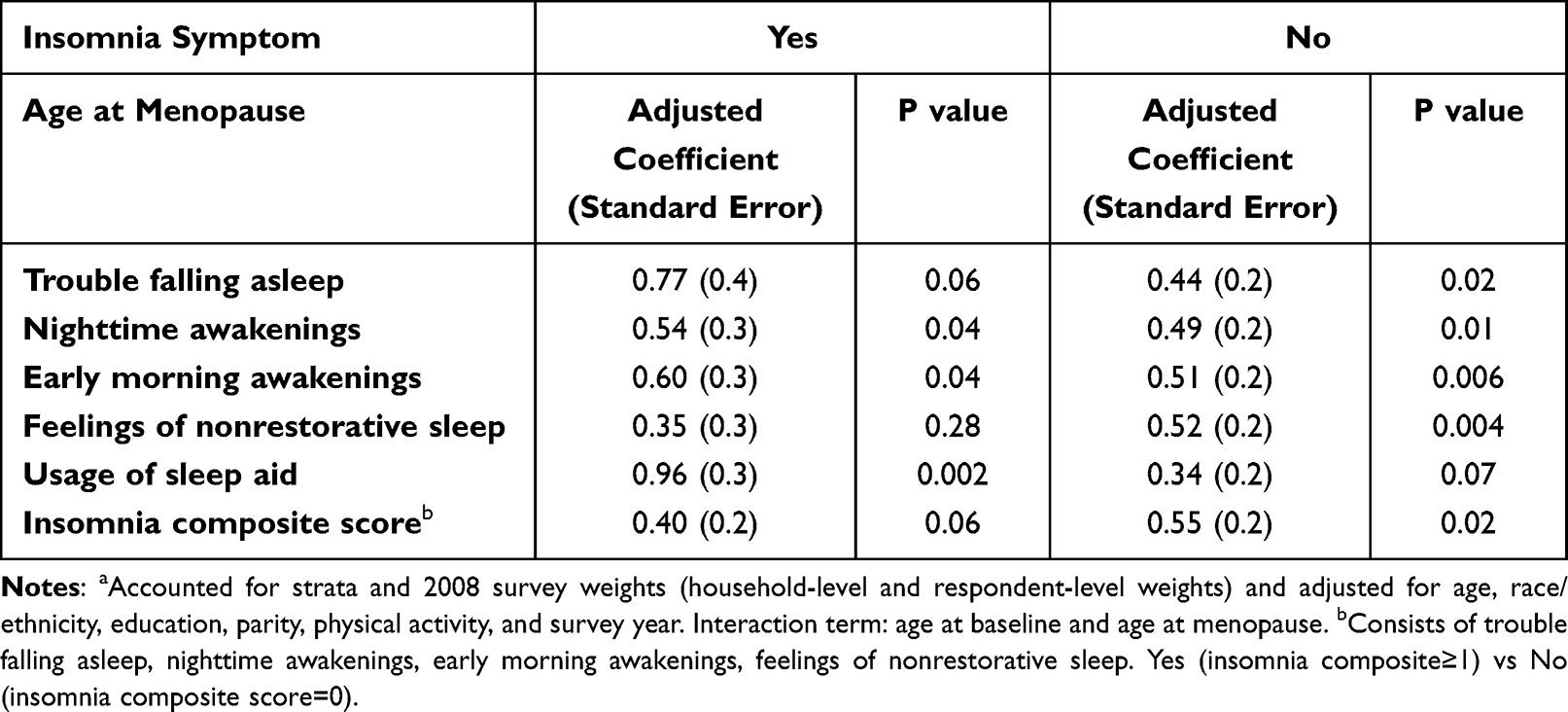 |
Table 4 Estimated Association (Adjusteda Coefficient and Standard Error) Between Age at Menopause (Exposure) and Cognitive Score (Outcome) for the Total Study Population from the Linear Mixed Model with a Random Intercept, by Insomnia Symptom, 2008–2018 |
As formal mediation analysis is not available for repeated outcomes, we conducted two separate analyses to examine the potential mediating role of insomnia symptoms in the pathway between age at menopause and cognitive function. First, we considered age at menopause as an exposure and insomnia symptoms as separate outcomes (Table 5), while in the second analysis insomnia symptoms were modeled as exposures and cognition as outcome (Table 6). Our results suggest that one-year increase in the age at menopause was associated with lower risk of developing trouble falling asleep (OR = 0.97, 95% CI: 0.96, 0.99), nighttime awakenings (OR = 0.98, 95% CI: 0.97, 0.99), feelings of nonrestorative sleep (OR = 0.97, 95% CI: 0.95, 0.99), and lower insomnia composite score (β =−0.01, 95% CI: −0.019, −0.007). Associations with early morning awakenings and use of sleep aids approached statistical significance (OR = 0.99, 95% CI: 0.97, 1.0) and (OR = 0.99, 95% CI: 0.97, 1.0), respectively.
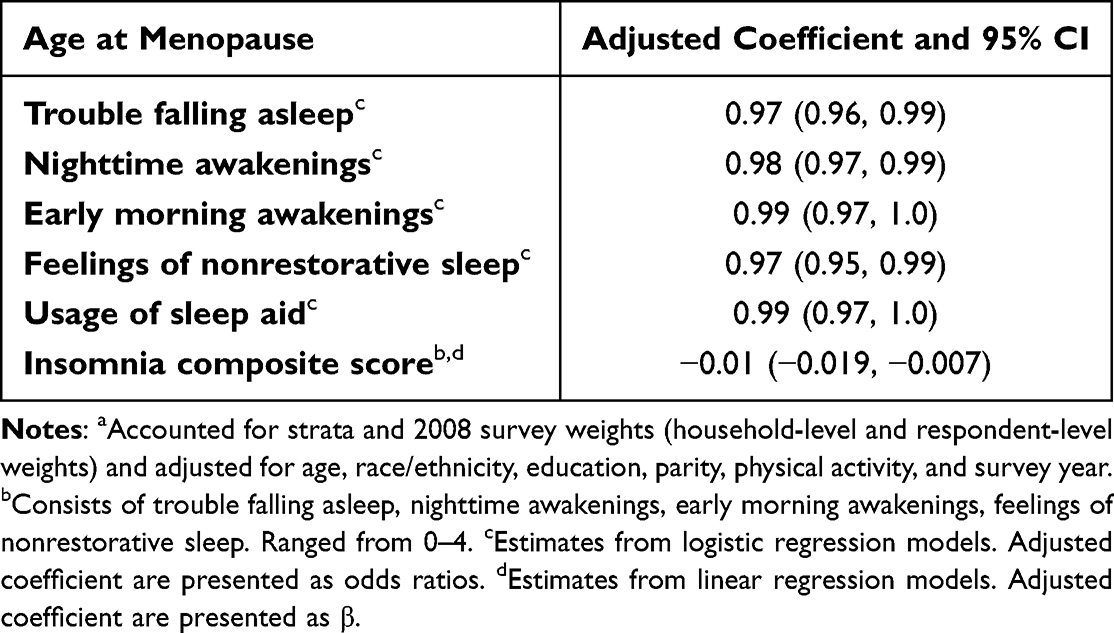 |
Table 5 Estimated Association (Adjusteda Coefficient and 95% CI) Between Age at Menopause (Exposure) and Insomnia Symptom (Outcome) for the Total Study Population from Regression Models, by Insomnia Symptom, 2008–2018 |
 |
Table 6 Estimated Association (Adjusteda Coefficient and Standard Error) Between Insomnia Symptom (Exposure) and Cognitive Score (Outcome) for the Total Study Population from the Linear Mixed Model with a Random Intercept, 2008–2018 |
Moreover, insomnia symptoms, ie, having trouble falling asleep and early morning awakenings, were associated with lower mean cognitive composite score of 0.5 (p = 0.02) and 0.76 (p = 0.002), respectively, in any given year (Table 6).
Discussion
Our study investigated the relationships between age at menopause, insomnia symptoms, and cognitive function assessed through a battery of neuropsychological tests. In a large and diverse cohort of 5880 of middle-aged and older women, a substantial proportion (15.2%) reported premature or early menopause. The association between age at menopause and cognitive function has been explained by two separate pathways: 1) menopause and insomnia, and 2) insomnia and cognition. Our analysis suggests insomnia mediates but does not moderate the association between age at menopause and cognition. We found that cognitive performance declines with each year that menopause is advanced. These cognitive differences are largely driven by the immediate word recall test. While insomnia symptoms did not moderate the association between age at menopause and cognition, their potential role as mediators in the association between age at menopause and cognition was indirectly apparent (earlier age at menopause was associated with developing insomnia and insomnia was associated with worse cognition). These findings link earlier age at menopause to poorer cognitive performance and highlight insomnia symptoms as potential mediators in the pathway between age at menopause and cognition.
Our study showed that one-year earlier in age at menopause was associated with a 0.49 lower mean in composite cognitive score. This positive association is congruent with prior reports. Data from the Swedish Twin Registry (n = 5804 women) showed that age at menopause was inversely associated with risk of cognitive impairment, assessed by a validated telephone interview for identifying dementia.26 Furthermore, a US-based cohort of 4047 women associated natural menopause before 47.4y with a 19% elevated risk of dementia, as identified by medical records (hazard ratios = 1.19, 95% CI: 1.07–1.31).8 Similarly, premature natural menopause, ≤40y, was associated with worse cognitive performance in certain areas (verbal fluency, visual memory, psychomotor speed, and global cognitive) in a French cohort study with 868 older women.27 These findings suggest the potential protective effect of reproductive hormones on cognitive aging among women. In contrast, age at menopause was not associated with neurological outcomes, including cognition decline, neuropathological measures, and clinical diagnosis of AD, among 1228 US women who transitioned to menopause naturally.28 This discrepancy could be attributed to difference in study designs and outcome assessments methodology.
Although we found statistically significant associations between age at menopause and composite cognitive score in stratified sample by insomnia symptoms, there was no evidence for moderation of these associations with insomnia symptoms. Instead, the greatest magnitude in cognitive decline during the follow-up was shown in women who reported use of sleep aids (β = 0.96, p-value=0.002). While the use of sleep aids is not a component of insomnia composite score, the proportion of women who had insomnia symptoms (insomnia composite score > 0) was much higher in those who used sleep aids (weighted prevalence: 59%) than those who did not (weighted prevalence: 36%). Indeed, frequent usage of sleep aids was associated with self-reported cognitive decline and with functional difficulties.29 Furthermore, long-term treatment with benzodiazepines has been linked to cognitive impairment in visuospatial ability, speed of processing, and verbal learning domains.30 Future work is needed to examine whether the use of sleep aids moderates or mediates the association between insomnia and cognitive impairment in the aging brain.
The role of sleep disturbances, insomnia symptoms, and OSA, as mediators and moderators in the pathway between age at menopause and cognitive function is plausible. Assessment of the relationships between age at menopause, sleep disturbances, and cognitive performance could uncover differential impact of early menopause on cognitive outcomes in specific subgroups and highlight sleep as a potential target for intervention in women who transition to menopause prematurely.
Pathological mechanisms underlying these relationships were not the focus of the present study; however, prior research suggests that early transition to menopause could contribute to cognitive impairment through hormonal mechanisms.31 There are abundant estradiol receptors localized in the brain responsible for memory and executive function. Through the neurotransmitter systems, estradiol employs its neurotrophic and neuroprotective function by enhancing synaptic plasticity, neurite growth and hippocampal neurogenesis and protecting against neural injury and apoptosis on the brain.32,33 Consequently, drastic changes in gonadal hormones during menopause have a notable influence on the central nervous system and are responsible for changes in cognition and other central nervous system function.34 On the other hand, decreased levels of gonadal hormones during menopause could result in nighttime vasomotor symptoms and therefore affecting sleep quality and nocturnal awakenings.35 Moreover, predisposing factors, ie, hormonal changes and aging, precipitating factors, ie, poor health and occurrence of other sleep disorders, and perpetuating factors, ie, hot flashes and negative influence on mood, could exacerbate insomnia symptoms during menopause.36 Therefore, insomnia could be a potential mediator in the pathway between age at menopause and cognition.
Our study has several strengths. First, this study consisted of a large, racially and ethnically diverse sample. Secondly, cognitive outcomes were measured by comprehensive and objective cognitive testing. Furthermore, five different questions related to symptoms of insomnia were measured in this sample, allowing for stratification and examination of their role as potential moderators and mediators. Finally, availability of rich information on covariates including comorbidities and socioeconomic status provided opportunities to adjust for potential confounders in the regression models.
Some limitations of the study should be noted. Missing values in cognitive outcomes were observed. Challenges of missing data are common in studies that assess cognitive function in older populations and could decrease power and bias the effect estimates. However, we used the imputed cognitive outcome data described in Langa et al, 2020.37 Secondly, menopause related questions became available in 2008. At that time, most of the women in this sample had already experienced menopause either naturally or surgically. Nevertheless, we adjusted for age and examined potential interactions between baseline age and age at menopause to account for the confounding effect of baseline age on the association between age at menopause and cognitive function. Age at menopause was self-reported, thus it may be susceptible to some misclassification. However, epidemiologic studies have showed that women could recall age at menopause consistently.38 Thirdly, information on the frequency and type of sleep aids use was not available. With the exception of sleep aids and hypertensive drugs, medications that could influence sleep quality were not available. Finally, this study did not collect data on hormone replacement therapy. However, hormone replacement therapy is a potential mediator in the pathway between age at menopause and cognitive function, thus its inclusion in the models would result in over adjustment and bias effect estimates.39 While some studies have shown potential influence of hormones such as estradiol and cortisol on the sleep quality of menopausal women,40–42 these hormones were not assessed by the HRS.
Conclusion
In a cohort of women who transitioned to menopause naturally, we found that earlier age at menopause is associated with a lower cognitive performance score. This association was further exacerbated and mediated, but not moderated by insomnia symptoms. Our findings support the potential mediating role of insomnia, as both a consequence of menopause and a risk factor for poor cognition in aging women. The vulnerability of midlife women to poor sleep highlights the need for strategies to address menopause-related insomnia symptoms to improve their well-being. Moreover, sleep-based interventions could mitigate cognitive decline in women as they transition to menopause, particularly among those who experience early menopause.
Acknowledgments
The abstract of this paper was presented at the conference SLEEP 2022 as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in SLEEP as “Age at menopause and insomnia in a racially diverse cohort” (https://academic.oup.com/sleep/article/45/Supplement_1/A26/6592274?login=false).
Disclosure
Dr Shieu is supported by a T32 grant from National Heart, Lung, and Blood Institute (T32HL110952). Drs. Braley and Dunietz report funding from the National Institute on Aging, Award Number R01AG074342. Dr Braley also reports grants from National Center for Complementary and Integrative Health/NIH 1R01AT011341, outside the submitted work. In addition, Dr Braley has a patent Sleep apnea treatment US and European patents (assigned to the Regents of the University of Michigan) US-10172920-B2/EP2861244B1 issued to University of Michigan. The authors report no other conflicts of interest in this work.
References
1. NIH. What is menopause. Available from: https://www.nia.nih.gov/health/what-menopause.
2. Shifren JL, Gass MLS, Kagan R, et al. The North American Menopause Society recommendations for clinical care of midlife women. Menopause. 2014;21(10):1038–1062. doi:10.1097/gme.0000000000000319
3. Shuster LT, Rhodes DJ, Gostout BS, Grossardt BR, Rocca WA. Premature menopause or early menopause: long-term health consequences. Maturitas. 2010;65(2):161–166. doi:10.1016/j.maturitas.2009.08.003
4. Faubion SS, Kuhle CL, Shuster LT, Rocca WA. Long-term health consequences of premature or early menopause and considerations for management. Climacteric. 2015;18(4):483–491. doi:10.3109/13697137.2015.1020484
5. Rocca WA, Bower JH, Maraganore DM, et al. Increased risk of cognitive impairment or dementia in women who underwent oophorectomy before menopause. Neurology. 2007;69(11):1074–1083. doi:10.1212/01.wnl.0000276984.19542.e6
6. Phung TKT, Waltoft BL, Laursen TM, et al. Hysterectomy, oophorectomy and risk of dementia: a nationwide historical cohort study. Dement Geriatr Cogn Disord. 2010;30(1):43–50. doi:10.1159/000314681
7. Kuh D, Cooper R, Moore A, Richards M, Hardy R. Age at menopause and lifetime cognition: findings from a British birth cohort study. Neurology. 2018;90(19):E1673–E1681. doi:10.1212/WNL.0000000000005486
8. Gilsanz P, Lee C, Corrada MM, Kawas CH, Quesenberry CP, Whitmer RA. Reproductive period and risk of dementia in a diverse cohort of health care members. Neurology. 2019;92(17):E2005–E2014. doi:10.1212/WNL.0000000000007326
9. Pertesi S, Coughlan G, Puthusseryppady V, Morris E, Hornberger M. Menopause, cognition and dementia – a review. Post Reprod Heal. 2019;25(4):200–206. doi:10.1177/2053369119883485
10. Pengo MF, Won CH, Bourjeily G. Sleep in Women Across the Life Span. Chest. 2018;154(1):196–206. doi:10.1016/j.chest.2018.04.005
11. Dzierzewski JM, Dautovich N, Ravyts S. Sleep and Cognition in Older Adults. Sleep Med Clin. 2018;13(1):93–106. doi:10.1016/j.jsmc.2017.09.009
12. El Khoudary SR, Aggarwal B, Beckie TM, et al. Menopause transition and cardiovascular disease risk: implications for timing of early prevention: a scientific statement from the American Heart Association. Circulation. 2020;142(25):e506–e532. doi:10.1161/CIR.0000000000000912
13. Olaithe M, Bucks RS, Hillman DR, Eastwood PR. Cognitive deficits in obstructive sleep apnea: insights from a meta-review and comparison with deficits observed in COPD, insomnia, and sleep deprivation. Sleep Med Rev. 2018;38:39–49. doi:10.1016/j.smrv.2017.03.005
14. Brownlow JA, Miller KE, Gehrman PR. Insomnia and Cognitive Performance. Sleep Med Clin. 2020;15(1):71–76. doi:10.1016/j.jsmc.2019.10.002
15. Shieu MM, Zaheed A, Shannon C, et al. Positive airway pressure and cognitive disorders in adults with obstructive sleep apnea: a systematic review of the literature. Neurology. 2022;99(4):e334–e446. doi:10.1212/WNL.0000000000200383
16. Vaccaro CM, Capozzi A, Ettore G, et al. What women think about menopause: an Italian survey. Maturitas. 2021;147:47–52. doi:10.1016/j.maturitas.2021.03.007
17. Baker FC, Willoughby AR, Sassoon SA, Colrain IM, de Zambotti M. Insomnia in women approaching menopause: beyond perception. Psychoneuroendocrinology. 2015;60:96–104. doi:10.1016/j.psyneuen.2015.06.005
18. Kitamura T, Miyazaki S, Bin SH, Akaike R, Ito Y, Suzuki H. Insomnia and obstructive sleep apnea as potential triggers of dementia: is personalized prediction and prevention of the pathological cascade applicable? EPMA J. 2020;11(3):355–365. doi:10.1007/s13167-020-00219-w
19. Sonnega A, Faul JD, Ofstedal MB, Langa KM, Phillips JWR, Weir DR. Cohort profile: the Health and Retirement Study (HRS). Int J Epidemiol. 2014;43(2):576–585. doi:10.1093/ije/dyu067
20. Health and Retirement Study. Institutional review board information. Available from: https://www.google.com/url?client=internal-element-cse&cx=014263126735541338401:u1ebznw786e&q=https://hrs.isr.umich.edu/sites/default/files/biblio/HRS_IRB_Information%2528web%2529_08_2018.pdf&sa=U&ved=2ahUKEwjy6b6Q9Mr8AhWhm4kEHT1uDGEQFnoECAEQAg&usg=AOvVaw.
21. Fong TG, Fearing MA, Jones RN, et al. Telephone interview for cognitive status: creating a crosswalk with the Mini-Mental State Examination. Alzheimers Dement. 2009;5(6):492–497. doi:10.1016/j.jalz.2009.02.007
22. Langa KM, Plassman BL, Wallace RB, et al. The Aging, Demographics, and Memory Study: study design and methods. Neuroepidemiology. 2005;25(4):181–191. doi:10.1159/000087448
23. Langa KM, Larson EB, Karlawish JH, et al. Trends in the prevalence and mortality of cognitive impairment in the United States: is there evidence of a compression of cognitive morbidity? Alzheimers Dement. 2008;4(2):134–144. doi:10.1016/j.jalz.2008.01.001
24. Cross-wave imputation of cognitive functioning measures 1992–2018. Available from: https://hrsdata.isr.umich.edu/data-products/cross-wave-imputation-cognitive-functioning-measures-1992-2018.
25. He XZ, Baker DW. Differences in leisure-time, household, and work-related physical activity by race, ethnicity, and education. J Gen Intern Med. 2005;20(3):259–266. doi:10.1111/j.1525-1497.2005.40198.x
26. Rasgon NL, Magnusson C, Johansson ALV, Pedersen NL, Elman S, Gatz M. Endogenous and exogenous hormone exposure and risk of cognitive impairment in Swedish twins: a preliminary study. Psychoneuroendocrinology. 2005;30(6):558–567. doi:10.1016/j.psyneuen.2005.01.004
27. Ryan J, Scali J, Carrière I, et al. Impact of a premature menopause on cognitive function in later life. BJOG. 2014;121(13):1729–1739. doi:10.1111/1471-0528.12828
28. Bove R, Secor E, Chibnik LB, et al. Age at surgical menopause influences cognitive decline and Alzheimer pathology in older women. Neurology. 2014;82(3):222–229. doi:10.1212/WNL.0000000000000033
29. Lee JE, Ju YJ, Chun KH, Lee SY. The frequency of sleep medication use and the risk of subjective cognitive decline (SCD) or SCD with functional difficulties in elderly individuals without dementia. J Gerontol a Biol Sci Med Sci. 2020;75(9):1693–1698. doi:10.1093/gerona/glz269
30. Stewart SA. The effects of benzodiazepines on cognition. J Clin Psychiatry. 2005;66(Suppl 2):9–13.
31. Rocca WA, Shuster LT, Grossardt BR, et al. Long-term effects of bilateral oophorectomy on brain aging: unanswered questions from the Mayo Clinic cohorts study of oophorectomy and aging. Womens Heal. 2009;5(1):39–48. doi:10.2217/17455057.5.1.39
32. Frick KM. Molecular mechanisms underlying the memory-enhancing effects of estradiol. Horm Behav. 2015;74:4–18. doi:10.1016/j.yhbeh.2015.05.001
33. Morgan KN, Derby CA. Cognitive changes with reproductive aging, perimenopause and menopause. Obs Gynecol Clin North Am. 2018;45(4):751–763. doi:10.1016/j.ogc.2018.07.011
34. Gava G, Orsili I, Alvisi S, Mancini I, Seracchioli R, Meriggiola MC. Cognition, mood and sleep in menopausal transition: the role of menopause hormone therapy. Med. 2019;55:10. doi:10.3390/medicina55100668
35. Joffe H, Crawford S, Economou N, et al. A gonadotropin-releasing hormone agonist model demonstrates that nocturnal hot flashes interrupt objective sleep. Sleep. 2013;36(12):1977–1985. doi:10.5665/sleep.3244
36. Proserpio P, Marra S, Campana C, et al. Insomnia and menopause: a narrative review on mechanisms and treatments. Climacteric. 2020;23(6):539–549. doi:10.1080/13697137.2020.1799973
37. Langa KM, Weir DR, Kabeto M, Sonnega A. Langa-Weir classification of cognitive function (1995 Onward). J Gerontol B sci. 2020;66. doi:10.1093/geronb/gbr048
38. Den Tonkelaar I. Validity and reproducibility of self-reported age at menopause in women participating in the DOM-project. Maturitas. 1997;27(2):117–123. doi:10.1016/S0378-5122(97)01122-5)
39. Schisterman EF, Cole SR, Platt RW. Overadjustment bias and unnecessary adjustment in epidemiologic studies. Epidemiology. 2009;20(4):488–495. doi:10.1097/EDE.0b013e3181a819a1
40. Galvan T, Camuso J, Sullivan K, et al. Association of estradiol with sleep apnea in depressed perimenopausal and postmenopausal women: a preliminary study. Menopause. 2017;24(1):112–117. doi:10.1097/GME.0000000000000737
41. Hollander LE, Freeman EW, Sammel MD, Berlin JA, Grisso JA, Battistini M. Sleep quality, estradiol levels, and behavioral factors in late reproductive age women. Obstet Gynecol. 2001;98(3):391–397. doi:10.1016/s0029-7844(01)01485-5
42. Haba-Rubio J, Ouanes S, Franc Y, et al. Do diurnal cortisol levels mediate the association between sleep disturbances and cognitive impairment? Neurobiol Aging. 2018;69:65–67. doi:10.1016/j.neurobiolaging.2018.05.001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.