")
Back to Journals » International Journal of General Medicine » Volume 16
The Influence of Patent Foramen Ovale on the Clinical Features of Migraine without Aura: A Cross-Sectional Study
Authors Tong Q, Yao Y, Xia Y, Chen Z, Ji G, Chen L, Jin R , Dong W
Received 9 June 2023
Accepted for publication 11 August 2023
Published 21 August 2023 Volume 2023:16 Pages 3645—3654
DOI https://doi.org/10.2147/IJGM.S423296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Qiuling Tong,1,2 Yu Yao,3 Yanhuo Xia,4 Zhibo Chen,2 Gangze Ji,2 Liuzhu Chen,2 Rujun Jin,2 Wanli Dong1
1Department of Neurology, The First Affiliated Hospital of Soochow University, Suzhou, People’s Republic of China; 2Department of Neurology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China; 3Department of Neurology, Ningbo First Hospital, Ningbo, People’s Republic of China; 4Department of Intensive Care Unit, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China
Correspondence: Wanli Dong, Department of Neurology, The First Affiliated Hospital of Soochow University, Suzhou, People’s Republic of China, Tel +8651265223637, Fax +8657755579318, Email [email protected]
Objective: To investigate the influence of patent foramen ovale (PFO) on the clinical features of migraine without aura (MoA).
Methods: We consecutively enrolled 390 MoA patients and compared the frequency of headache, episode duration, and the Visual Analogue Scale (VAS), Headache Impact Test 6 (HIT-6), and European Health Interview Survey-Quality of Life 8-item index (EUROHIS-QOL8) scores of patients with and without PFO, those with the mild right-to-left shunt (RLS) and moderate to large RLS, and those with permanent RLS and latent RLS using a nonparametric Mann–Whitney U-test. In addition, we analyzed the clinical features of migraine in 39 MoA patients before and after PFO closure treatment using the paired Wilcoxon test.
Results: The prevalence of PFO in the 390 MoA patients was 44.4%. Patients with PFO had significantly higher frequency of headaches, VAS scores, HIT-6 scores, and incidence of white matter lesions than those without PFO (all p< 0.05). Patients with moderate to large RLS had significantly higher VAS scores than those with mild RLS (p = 0.002). Additionally, 39 MoA patients underwent PFO closure, which remarkably decreased their frequency of headache, episode duration, VAS scores, and HIT-6 scores, and increased their EUROHIS-QOL8 scores.
Conclusion: The migraine features in MoA patients could be influenced by PFO, especially in patients with moderate to large shunt, in whom PFO closure improved the symptoms.
Keywords: migraine without aura, patent foramen ovale, clinical features, closure treatment
Introduction
Migraine is a ubiquitous, prevalent, chronic neuro-vascular disorder characterized by headache attacks. It severely affects people’s health and quality of life and is a leading cause of disability worldwide in people younger than 50, especially in women.1 There are over 1 billion migraine cases worldwide.2,3 In China, a 1-year prevalence of migraine was up to 9% and was the cause of 331 years lived with disability (YLDs) per 100,000 people per year amounting to 5.5 million YLDs.4 Moreover, inadequate awareness of migraine and clinically improper treatment, especially in underdeveloped regions, lead to chronic migraine, drug abuse and addiction, as well as medication overuse headache,5,6 thereby augmenting public health burdens. Unfortunately, the pathophysiology of migraine remains incompletely elucidated.
Migraine can be classified into two subtypes: migraine with aura (MA) and migraine without aura (MoA). Recent evidence suggests a correlation between the presence of patent foramen ovale (PFO) and MA.7 PFO is present in 20% to 25% of the general population,8,9 but the prevalence of PFO in patients with MA is more than twice as high as that in the general population.8,10 More importantly, MA patients with moderate or large PFO have significantly higher frequencies of headaches, Headache Impact Test (HIT-6) scores, and migraine disability assessment scores (MIDAS) than those with mild PFO or without PFO.11 The frequency and duration of headaches can effectively be reduced, and the quality of life can be improved after PFO closure treatment.12 Overall, these findings suggest that the presence of PFO is an underlying factor in the pathogenesis of MA.
Clinically, approximately 75% of migraineursareMoA.13 However, the correlation between PFO and MoA receives insufficient attention. The clinical features of MoA patients with and without PFO have not been systematically analyzed. The efficacy of PFO closure for patients with MoA remains debatable to date. Here, to comprehensively investigate the influence of PFO on MoA, we consecutively enrolled 390 MoA patients and analyzed the migraine characteristics under different statuses of PFO. In addition, we analyzed the efficacy of PFO closure in 39 patients with MoA.
Materials and Methods
Participants and Ethics Statement
MoA patients who visited the outpatient clinic of the Department of Neurology of the Affiliated First Hospital of Wenzhou Medical University between April 2018 and January 2021 were consecutively enrolled in this study. MoA was diagnosed according to the third edition beta of the International Classification of Headache Disorders (ICHD-III-beta).14 Figure 1 displays the flow diagram of MoA patients’ enrollment. The exclusion criteria were: (1) Under 18 years old; (2) Patients who were unable to perform the Valsalva Maneuver; (3) Severe cerebral arterial stenosis; (4) Unavailability of brain magnetic resonance imaging (MRI) or contrast transthoracic echocardiography (cTTE) examination results; (5) right-to-left shunt (RLS) due to other causes.
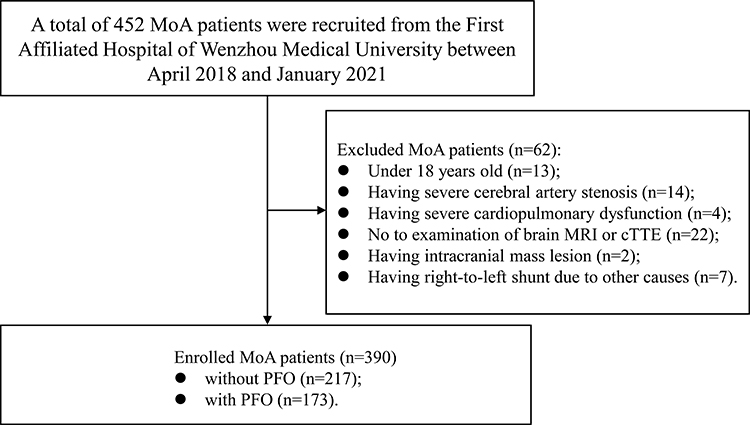 |
Figure 1 Flow diagram of participant enrollment. Abbreviations: PFO, patent foramen ovale; MoA, Migraine without Aura; MRI, Magnetic Resonance Imaging; cTTE, contrast transthoracic echocardiography. |
Additionally, 39 patients with MoA who underwent percutaneous PFO closure from August 2019 to February 2022 were included in the study. The inclusion criteria were in accordance with the management strategy of PFO recommended by experts, China.15 All patients with MoAexhibited PFO with moderate or large RLS. The percutaneous PFO closure was performed by experienced physicians, and the closure effect was assessed by cTTE immediately after procedure and was re-evaluated after a 6-month follow-up. All of these patients received anti-platelet therapy within 6 months after PFO closure. Besides, either their use of other migraine medications remained similar pre- and post-PFO closure, or they used no other migraine medications after PFO closure.
Our study was conducted to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University (No. KY2021-R064). Informed consent was obtained from participants or their legal representatives.
Identification of PFO
The diagnosis of PFO was based on cTTE. The PFO was graded according to the number of bubbles in the middle cerebral artery detected by contrast transcranial Doppler (cTCD): microemboli (MBs) ≤ 10 (mild shunt); 10 ˂ MBs ≤ 25 (moderate shunt); MBs > 25 or curtain (large shunt). Patients with shunt observable by cTTE during rest were classified as having permanent RLS, while those with a shunt only observable during the Valsalva Maneuver were classified as having latent RLS.
The Definition of WMLs
To determine the presence of white matter lesions (WMLs), all patients underwent MRI examination including T1- and T2-weighted sequences, FLAIR and DWI sequences. WMLs were defined as lesions in the deep or subcortical white matters with hyper-intense focal lesions on FLAIR sequences and iso- or hypo-intense on T1-weighted sequences.
Collection of Clinical Data
We collected the demographic data and migraine characteristics (features of headache, family history, age of onset, headache frequency, duration of disease, and episode duration) of all patients. To evaluate headache intensity, degree of disability, and quality of life, all patients completed the Visual Analogue Scale (VAS), Headache Impact Test 6 (HIT-6), and European Health Interview Survey-Quality of Life 8-item index (EUROHIS-QOL8) questionnaires. Other clinical data (eg, MRI, cTTE, or cTCD results) were collected from medical records.
The above clinical data were also collected from the 39 patients with MoA who underwent percutaneous PFO closure treatment, both before and after closure. Additionally, a detailed medication history was recorded prior to and following the closure.
Statistical Analysis
All statistical analyses were performed using SPSS version 24.0 (SPSS Inc., Chicago, IL, USA). Categorical variables were expressed as frequencies and percentages. For continuous variables, we calculated the median and interquartile range (IQR) or range. We compared the continuous variables of the different groups using the nonparametric Mann–Whitney U-test. We compared categorical variables using the χ2 test or the Fisher exact test. Finally, we compared the clinical parameters of patients with MoA before and after PFO closure using the paired Wilcoxon test. The p value was adjusted based on the false discovery rate for the multiple comparisons. Differences were considered statistically significant when two-sided p< 0.05.
Results
Clinical Characteristics of the Enrolled MoA Patients
As shown in Table 1, 390 MoA patients (288 females and 102 males) were enrolled. The median age was 43 years (IQR, 35–49 years). The median age at onsetofMoAwas 31 years (IQR, 23–38.5 years). The median duration of MoA was 10 years (IQR, 5–16.5 years). The median frequency of headaches was 2.5 times/month (IQR, 1–4 times/month). The median episode duration was 24 h (IQR, 6–24 h). The median VAS, HIT-6, and EUROHIS-QOL 8 scores were 7 (6–8), 62 (56–68), and 30 (25–33), respectively. The incidence of white matter lesions (WML) was 29% (113/390). A total of 173 patients had PFO (PFO+), and 217 patients did not (PFO−).
 |
Table 1 Demographic and Clinical Characteristics of 390 MoA Patients |
The Differences in the Migraine Clinical Features Between MoA Patients with PFO and Those without PFO
To investigate the association between PFO and MoA, we compared the clinical features of PFO+ and PFO− patients. As shown in Table 1, the frequencies of headaches were 2.5 times/month (IQR, 1.5–4.5 times/month) in the PFO+ group and 2 times/month (IQR, 1–4 times/month) in the PFO− group (p = 0.001). The VAS and HIT-6 scores were higher in the PFO+ group than in the PFO− group (both p< 0.001)]. The incidence of WML was 37.6% (65/173) in the PFO+ group and 22.1% (48/217) in the PFO− group (p = 0.0008). The other clinical features were similar (all p> 0.05).
The VAS Scores Were Higher in MoA Patients with Moderate to Large RLS Than Those with Mild RLS
Among the 173 MoA patients with PFO, 133 had undergone a cTCD examination. Based on the cTCD results, we graded the RLS and found 96 patients with mild shunt, 11 patients with moderate shunt, and 26 patients with large shunt. Next, we compared the clinical features of the patients with mild RLS and moderate to large RLS. As shown in Table 2, the VAS scores were significantly higher in patients with moderate to large RLS [8 (IQR, 7–9)] than in patients with mild RLS [7 (IQR, 6–8), p = 0.002]. The frequency of headache, episode duration, HIT-6 score, EUROHIS-QOL 8 score, and the incidence of WML were not different (all p> 0.05).
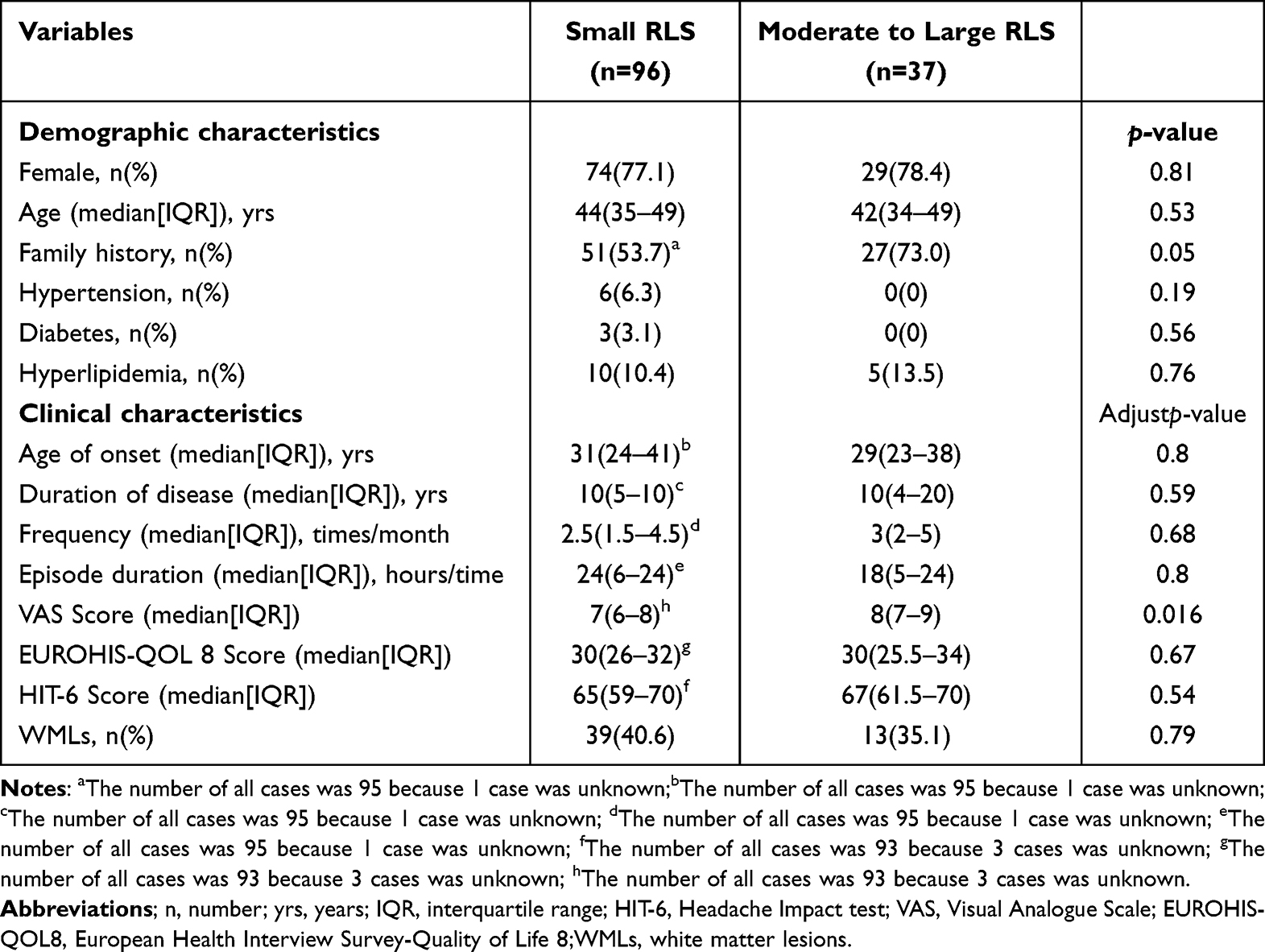 |
Table 2 Demographic and Clinical Characteristics in Different RLS Among 133 MoA Patients with PFO |
The Migraine Clinical Features Were No Difference Between Permanent and Latent RLS
We compared the clinical features of the 130 patients with permanent RLS and 43 patients with latent RLS among the 173 PFO+ patients. As shown in Table 3, the median age of patients with latent RLS was 41.5 years (IQR, 33–47 years), and that of patients with permanent RLS was 47 years (IQR, 39–51 years) (p= 0.014). The other clinical features, namely headache frequency, episode duration, VAS score, HIT-6 score, EUROHIS-QOL8 score, and the incidence of WML, were similar (all p> 0.05).
 |
Table 3 Demographic and Clinical Characteristics in Different PFO Status Among 173 MoA Patients with PFO |
Improvement of the Clinical Features of Migraine in MoA Patients After PFO Closure
To further investigate the relationship between MoA and PFO, we observed the effects of PFO closure in 39 patients with MoA. Among them, 7 had moderate RLS and 32 had large RLS. The median follow-up time was 20 months (range, 7–48 months). Besides anti-platelet medication, 16 patients used no medication after PFO closure, while 23 patients had similar migraine medication uses pre- and post-PFO closure. Complete PFO closure, assessed by cTTE, was achieved in 38 patients; the remaining patient had minimal residual shunt. Table 4 displays the demographic and clinical data of the 39 patients. Next, we analyzed the migraine features before and after PFO closure (Figure 2A). After PFO closure, headache frequency decreased from 4.5 times/month (IQR, 2.5–10 times/month) to 1.5 times/month (IQR, 0.42–4 times/month) (p< 0.0001). The episode duration decreased from 24 h (IQR, 12–36 h) to 12 h (IQR, 4–24 h) (p< 0.0001). The PFO closure also significantly decreased the VAS score [Before: 7.5 (IQR, 6–8) vs after: 4.5 (IQR, 3–6)] and HIT-6 score [before: 66 (IQR, 59–69) vs after: 50 (IQR, 42–58)] (both p< 0.0001). Finally, PFO closure remarkably increased the EUROHIS-QOL8 score from 26 (IQR, 20–30) to 30 (IQR, 28–34) (p< 0.0001).
 |
Table 4 Demographic and Clinical Characteristics of 39 Patients with MoA for PFO Closure |
 |
Figure 2 The effects of migraine headaches after PFO closure in 39 MoA patients. (A) Episode duration, frequency, VAS, HIT-6 and EUROHIS-QOL 8 scores before and after PFO closure in 39 MoA patients; (B) The reduction of migraine days per month after PFO closure compared to before closure; (C) The reduction of frequency of migraine per month after PFO closure compared to before closure. |
As shown in Figure 2B, migraine headaches disappeared in three patients (7.7%) after PFO closure. The number of migraine days per month decreased by more than 50% in 28 patients (71.8%), and by less than 50% in 4 patients (10.3%). The migraine days per month remained unchanged in 2 patients (5.1%), and 2 patients (5.1%) reported a persistent worsening of their headaches. The frequency of headaches decreased by more than 50% in 24 patients (61.5%), decreased by less than 50% in 6 patients (15.4%), remained unchanged in 3 patients (7.7%), and increased in 3 patients (7.7%) (Figure 2C). Overall, our results indicate that PFO closure remarkably improved migraine symptoms in MoA patients.
Discussion
The relationship between MoA and PFO is unclear so far. Previous studies showed that the prevalence of PFO among patients with MoA was similar to that in the general population.16–18 Dalla et al reported that 16.2% (12/74) of MoA patients had PFO.17 Carod-Artal et al found that the prevalence of PFO among MoA patients was 33.7% (28/83).16 Domitrz et al reported 15 patients with PFO among 60 MoA patients.18 These studies only included small patient numbers. In the present study, we enrolled 390 patients with MoA. To minimize selection bias, we recruited patients with MoA through consecutive enrollment. The prevalence of PFO among patients with MoA was 44.4% in our study. Recently, a community-based cross-sectional study recruited 3741 participants. Among them, 255 had MoA, and 44.3% of these had PFO. 19 A multi-center case-control study also showed that the prevalence of RLS was 39.9% in 691 MoA patients, which is higher than that in the general population.20 The prevalence of PFO in the two studies was consistent with that in our study. Interestingly, these two studies also recruited patients with MoA from China, while the other mentioned studies included patients from Poland, Italy, and Brazil. Thus, race and region should be considered as factors affecting the prevalence of PFO.
We found that 72.2% of MoA patients with PFO had small RLS, 8.3% had moderate RLS, and 19.5% had large RLS. Meanwhile, 7% of MA patients with PFOhave small RLS and 48% have large RLS.21 In a multi-center and large scale study, the prevalence of large RLS in the MA and MoA groups was 32.1% and 16.5%, respectively.20 To summarize, MoA patients mainly have small RLS, and the prevalence of large RLS is higher in MA patients than in MoA patients.
The physiopathology of migraine is complex and multiple factors, such as genetics and environment, play important roles.22 The idea of the relationship between PFO and migraine is mainly based on the hypothesis that substances in the blood, such as vasoactive chemicals or microemboli, entered the brain through the PFO (bypassing the lung), which could induce headache attacks.7,23 In the present study, the frequency of headaches, VAS score, andHIT-6 score were significantly higher in MoA patients with PFO than in those without PFO. The VAS scores were higher in patients with moderate to large RLS than in those with mild RLS. These results were consistent with those in patients with MA.11 A propensity-matched cross-sectional study showed that individuals who had a PFO with large shunts were 1.69 times more likely to report experiencing MoA.19 The incidence of WMLs was significantly higher in MoA patients with PFO than in those without PFO. Iwasaki et al had reported that the prevalence of RLS was significantly increased in the WMLs positive patients, and was independently associated with the presence of WMLs in patients with migraine (OR=6.15, p=0.003).24 Park et al found that migraine patients with RLS more frequently had small deep WMLs, and were identified as independent predictors for small dWMLs.25 These results are consistent with our study. Altogether, these findings indicated that PFO could increase the risk of MoA and influence the clinical features of MoA, especially with moderate to large shunts, suggesting that there could be a relationship between PFO and MoA. However, it’s worth noting that PFO can also be found in some individuals without a history of migraine, including the general population, Therefore, further investigation into the physiopathological mechanisms underlying PFO in patients with MoA is warranted.
We found that the migraine symptoms of 39 MoA patients with moderate and large RLS were remarkably reduced after PFO closure. Among them, headaches disappeared in 3 patients, and 28 patients had a more than 50% decrease in the number of migraine days per month. Previous studies also confirmed that percutaneous PFO closure significantly improved clinical features in patients with MoA and MA by comparing their migraine symptoms before and after PFO closure.12,26 Even so, the efficacy of PFO closure for migraine patients remained clinically controversial up to now. Three previous large randomized controlled trials (MIST, PRIMA and PREMIUM) have concluded on its inefficacy,27–29 as it failed to reach the endpoints (complete cessation of migraine and ≥ 50% reduction of the number of headache days). There are some explanations for the inefficacy. In our study, we enrolled 39 patients undergoing PFO closure were MoA with moderate or large RLS, while the majority of subjects enrolled in the three large randomized controlled trials were migraine with aura except PREMIUM which included subjects with migraine (with and without aura). Moreover, all subjects in the three trials suffered from severe and refractory migraines that were unresponsive to at least two classes of prophylactic treatments. The achievement of significant treatment effects for these patients may be a challenge to any form of intervention. Additionally, 38 patients achieved complete PFO closure and one patient had minimal residual shunt in our study, while 6.2%,12%, and 18% of patients in MIST, PRIMA and PREMIUM trials have significant residual right-to-left shunt after PFO closure, respectively. A previous study had reported that complete PFO closure can reduce a 4-fold migraine burden.30 The residual right-to-left shunt following PFO closure in these trials may potentially mitigate the effect of PFO closure, and may be associated with the failure to achieve the primary endpoints. Nevertheless, the migraine days per month were decreased after treatment compared to pre-treatment. Additionally, the days of reduction in closure group were more than those in the non-closure group in these large randomized controlled trials.27–29 Subjects with MA had a higher incidence of complete migraine cessation following PFO closure.31 Some patients with MoA do respond to PFO closure, and migraine attacks were significant reduced in PREMIUM trials.28 These results are in accordance with our study. Altogether, these findings indicated that some patients with migraine could benefit from PFO closure. In addition, there were some limitations in our study. Because only a small number of patients with PFO closure were enrolled and this was a non-randomized trial, our results insufficiently explain the effects of PFO closure. To better investigate the effects of PFO closure in migraineurs, large scale clinical studies with a long-term follow-up are needed.
Conclusions
The headache frequency, incidence of WML, VAS score, and HIT-6 score in MoApatients with PFO were significantly higher than in those without PFO. The VAS score was higher in patients with moderate to large RLS than in those with mild RLS. PFO closure effectively reduced migraine symptoms and improved the quality of life of MoA patients with moderate to large RLS. Overall, these findings confirm the existence of a relationship between PFO and MoA.
Abbreviations
IQR, interquartile range; PFO, patent foramen ovale; HIT-6, Headache Impact test; VAS, Visual Analogue Scale; EUROHIS-QOL8, European Health Interview Survey-Quality of Life 8; WML, white matter lesions; MA, migraine with aura; MoA, migraine without aura; RLS, right to left shunt; PFO, patent foramen ovale; ICHD-III-beta, the International Classification of Headache Disorders; VM, Valsalva Maneuver; MRI, magnetic resonance imaging; cTTE, contrast transthoracic echocardiography; cTCD, contrast transcranial Doppler; MBs, microembolism.
Data Sharing Statement
All datasets presented in this study are included in the article material. The data supporting the results of this study are available from the corresponding author upon reasonable request from any qualified investigator.
Ethics Approval and Informed Consent
The study was conducted by the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University (No. KY2021-R064). Informed consent was obtained from participants or their legal representatives.
Consent for Publication
All authors approved the publishing of the final manuscript.
Acknowledgments
We are very grateful to all patients who participated in this study for their contributions. Thanks for the funding support of Wenzhou Municipal Scientific and Technological Program Projects (no. Y20210911).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ashina M, Katsarava Z, Do TP, et al. Migraine: epidemiology and systems of care. Lancet. 2021;397(10283):1485–1495. doi:10.1016/s0140-6736(20)32160-7
2. Ashina M, Ropper AH. Migraine. N Engl J Med. 2020;383(19):1866–1876. doi:10.1056/NEJMra1915327
3. Vos T, Abajobir AA, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–1259. doi:10.1016/s0140-6736(17)32154-2
4. Yao C, Wang Y, Wang L, et al. Burden of headache disorders in China, 1990–2017: findings from the Global Burden of Disease Study 2017. J Headache Pain. 2019;20(1):102. doi:10.1186/s10194-019-1048-2
5. Katsuki M, Matsumori Y, Kawahara J, et al. Headache education by leaflet distribution during COVID-19 vaccination and school-based on-demand e-learning: Itoigawa Geopark Headache Awareness Campaign. Headache. 2023;63(3):429–440. doi:10.1111/head.14472
6. Schwedt TJ, Hentz JG, Sahai-Srivastava S, et al. Headache characteristics and burden from chronic migraine with medication overuse headache: cross-sectional observations from the medication overuse treatment strategy trial. Headache. 2021;61(2):351–362. doi:10.1111/head.14056
7. Kumar P, Kijima Y, West BH, Tobis JM. The connection between patent foramen ovale and migraine. Neuroimaging Clin N Am. 2019;29(2):261–270. doi:10.1016/j.nic.2019.01.006
8. Zhao Q, Liu R, Zhou J, Dong Z, Chen Y. Prevalence and grade of RLS in migraine: a prospective study of 251 migraineurs by synchronous test of c-TTE and c-TCD. Medicine. 2021;100(4):e24175. doi:10.1097/md.0000000000024175
9. Hara H, Virmani R, Ladich E, et al. Patent foramen ovale: current pathology, pathophysiology, and clinical status. J Am Coll Cardiol. 2005;46(9):1768–1776. doi:10.1016/j.jacc.2005.08.038
10. Guo Y, Shi Y, Zhu D, Liu R, Qi Y, Luo G. Clopidogrel can be an effective complementary prophylactic for drug-refractory migraine with patent foramen ovale. J Investig Med. 2020;68(7):1250–1255. doi:10.1136/jim-2020-001342
11. He Q, Zhang Y, Wang F, et al. Impact of right-to-left shunt and transcatheter closure on the clinical features of migraine. Int J Neurosci. 2020;130(3):270–275. doi:10.1080/00207454.2019.1672681
12. Qi Y, Zhang Y, Luo X, et al. Efficacy of patent foramen ovale closure for treating migraine: a prospective follow-up study. J Investig Med. 2021;69(1):7–12. doi:10.1136/jim-2020-001323
13. Merikangas KR. Contributions of epidemiology to our understanding of migraine. Headache. 2013;53(2):230–246. doi:10.1111/head.12038
14. Olesen J. Headache classification committee of the International Headache Society (IHS) the international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
15. Zhang Y, Zhu X, Jiang S. Recommendations from Chinese experts on management of patients with patent foramen ovale. Chin Heart J. 2015;27:373–379.
16. Carod-Artal FJ, da Silveira Ribeiro L, Braga H, Kummer W, Mesquita HM, Vargas AP. Prevalence of patent foramen ovale in migraine patients with and without aura compared with stroke patients. A transcranial Doppler study. Cephalalgia. 2006;26(8):934–939. doi:10.1111/j.1468-2982.2006.01156.x
17. Dalla VG, Guindani M, Zavarise P, Griffini S, Pezzini A, Padovani A. Prevalence of patent foramen ovale in a large series of patients with migraine with aura, migraine without aura and cluster headache, and relationship with clinical phenotype. J Headache Pain. 2005;6(4):328–330. doi:10.1007/s10194-005-0223-9
18. Domitrz I, Mieszkowski J, Kamińska A. Relationship between migraine and patent foramen ovale: a study of 121 patients with migraine. Headache. 2007;47(9):1311–1318. doi:10.1111/j.1526-4610.2006.00724.x
19. Tang Y, Peng A, Peng B, et al. Association between patent foramen ovale and migraine without aura: a community-based cross-sectional study in China. BMJ open. 2022;12(3):e056937. doi:10.1136/bmjopen-2021-056937
20. Wang SB, Liu KD, Yang Y, et al. Prevalence and extent of right-to-left shunt on contrast-enhanced transcranial Doppler in Chinese patients with migraine in a multicentre case-control study. Cephalalgia. 2018;38(4):690–696. doi:10.1177/0333102417708203
21. Liboni W, Molinari F, Allais GB, et al. Patent foramen ovale detected by near-infrared spectroscopy in patients suffering from migraine with aura. Neurol Sci. 2008;29(Suppl 1):S182–S185. doi:10.1007/s10072-008-0920-7
22. Post MC, Luermans JG, Plokker HW, Budts W. Patent foramen ovale and migraine. Catheter Cardiovasc Interv. 2007;69(1):9–14. doi:10.1002/ccd.20931
23. Caputi L, Usai S, Carriero MR, et al. Microembolic air load during contrast-transcranial Doppler: a trigger for migraine with aura? Headache. 2010;50(8):1320–1327. doi:10.1111/j.1526-4610.2010.01621.x
24. Iwasaki A, Suzuki K, Takekawa H, et al. The relationship between right-to-left shunt and brain white matter lesions in Japanese patients with migraine: a single center study. J Headache Pain. 2017;18(1):3. doi:10.1186/s10194-016-0714-x
25. Park HK, Lee SY, Kim SE, Yun CH, Kim SH. Small deep white matter lesions are associated with right-to-left shunts in migraineurs. J Neurol. 2011;258(3):427–433. doi:10.1007/s00415-010-5771-5
26. Wahl A, Praz F, Tai T, et al. Improvement of migraine headaches after percutaneous closure of patent foramen ovale for secondary prevention of paradoxical embolism. Heart. 2010;96(12):967–973. doi:10.1136/hrt.2009.181156
27. Dowson A, Mullen MJ, Peatfield R, et al. Migraine Intervention WithSTARFlex Technology (MIST) trial: a prospective, multicenter, double-blind, sham-controlled trial to evaluate the effectiveness of patent foramen ovale closure with STARFlex septal repair implant to resolve refractory migraine headache. Circulation. 2008;117(11):1397–1404. doi:10.1161/circulationaha.107.727271
28. Tobis JM, Charles A, Silberstein SD, et al. Percutaneous closure of patent foramen ovale in patients with migraine: the PREMIUM trial. J Am Coll Cardiol. 2017;70(22):2766–2774. doi:10.1016/j.jacc.2017.09.1105
29. Mattle HP, Evers S, Hildick-Smith D, et al. Percutaneous closure of patent foramen ovale in migraine with aura, a randomized controlled trial. Eur Heart J. 2016;37(26):2029–2036. doi:10.1093/eurheartj/ehw027
30. Mahmoud AN, Mentias A, Elgendy AY, et al. Migraine and the risk of cardiovascular and cerebrovascular events: a meta-analysis of 16 cohort studies including 1 152 407 subjects. BMJ Open. 2018;8(3):e020498. doi:10.1136/bmjopen-2017-020498
31. Mojadidi MK, Kumar P, Mahmoud AN, et al. Pooled analysis of PFO occluder device trials in patients with PFO and migraine. J Am Coll Cardiol. 2021;77(6):667–676. doi:10.1016/j.jacc.2020.11.068
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.