")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Influence of Mother’s Employment, Family Income, and Expenditure on Stunting Among Children Under Five: A Cross-Sectional Study in Indonesia
Authors Rahayuwati L , Komariah M , Sari CWM , Yani DI , Hermayanti Y , Setiawan A, Hastuti H, Maulana S, Kohar K
Received 18 April 2023
Accepted for publication 7 August 2023
Published 14 August 2023 Volume 2023:16 Pages 2271—2278
DOI https://doi.org/10.2147/JMDH.S417749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Laili Rahayuwati,1 Maria Komariah,2 Citra Windani Mambang Sari,1 Desy Indra Yani,1 Yanti Hermayanti,3 Arlette Setiawan,4 Hediati Hastuti,5 Sidik Maulana,5 Kelvin Kohar6
1Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Fundamental Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 3Department of Maternity Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 4Department of Pediatric Dentistry, Faculty of Dentistry, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 5Internship Nursing Program, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 6Clinical Clerkship Program, Faculty of Medicine, Universitas Indonesia, Dr. Cipto Mangunkusumo National Central Hospital, Jakarta, Special Capital Region of Jakarta, Indonesia
Correspondence: Laili Rahayuwati, Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Bandung-Sumedang KM. 21, Hegarmanah, Jatinangor, Kabupaten, Sumedang, West Java, 45363, Indonesia, Tel +62 08122138385, Fax +62 022 7795596, Email [email protected]
Introduction: It is widely acknowledged that the socioeconomic circumstances of a family income are correctly reflected in that family expenditures. The dietary habits of families are influenced by socioeconomic circumstances that may affect stunting. Therefore, this study aims to investigate the household economic predictor stunting (mother’s employment, family income, and family expenditure) in children under five.
Methods: This study used a cross-sectional design. Six districts and cities have been chosen as study areas based on the areas with the highest incidence of stunting in West Java, Indonesia. This study conducted specifically from October to December 2018. Data were examined using descriptive statistics (frequency distribution) and a Spearman Rank bivariate test. A logistic regression was employed to determine the elements that serve as predictors of stunting.
Results: A total of 731 women with children under five participated in the study. A bivariate analysis showed that mother’s employment had an association with stunting among children under five (p = 0.014). Meanwhile, family income and expenditure are not statistically significant associated with stunting (p > 0.05). A multivariate analysis showed that mother’s employment was a stunting predictor with odd ratio (OR) 1.810 (p = 0.017). The OR value means that mothers who do not work have a 1.810 chance for their children to experience stunting compared with mothers who have work. However, family income and expenditure have negative projected values (p = 0.580 and p = 0.398, respectively).
Conclusion: Children under five who are stunted are potentially predictive with mothers’ employment, with a chance is higher in mother who do not work. However, family income and expenditure are not predictive of stunting.
Keywords: family economic, family expenditure, mother’s employment, stunting, socioeconomic
Introduction
Infants and young children are most vulnerable to malnutrition due to their high nutritional needs for growth and development. The most common nutritional problem experienced by toddlers worldwide is stunting.1 More than just a public health problem, this is an obstacle to global poverty eradication, productivity and economic growth. Ending malnutrition would eliminate an estimated 32% of the global burden of disease.2 Stunting can be referred to by measuring the height index based on the age of children.3 Based on WHO child growth standards for age and sex, a child is said to be in the very short category if his length or height is below −2SD. This is usually related to several aspects such as poverty, poor maternal health and nutrition as well as inappropriate feeding and care in the early phases of a child’s life. As for children with stunting, research has shown that stunting has long-term effects on individuals and society, leading to reduced cognitive and academic performance, poorer behavioral development, and poorer cognitive skills than non-stunted children. Stunted children may exhibit more apathetic attitudes, less exploratory behavior, and impaired memory. In terms of physical health, stunting can also have an impact on increasing individual susceptibility to the accumulation of body fat, increasing the risk of infection and non-communicable diseases, and being at higher risk of experiencing several conditions such as hypertension and diabetes.4,5
One region with many cases of stunting is Asia. Southeast Asia has the second highest prevalence, with a stunting incidence of 29.4%.6 In South Asia, the prevalence of stunting reached 35% in 2017. Although this figure decreased compared to 2000, which was 51%, it is still relatively high when compared to international standards because it is far above the prevention threshold of 30% (trigger value to be used as a basis public health decision).7,8 Indonesia, which is located in Southeast Asia, is a country that’s still experiencing cases of stunting. Research shows that stunting rates often vary widely across Indonesia. This may be due to urbanization and the differences in location of the large part of the rural population. Meanwhile, stunting rates are usually higher in eastern Indonesia than in western Indonesia.9,10
Previous studies shows that there are several factors that influence the incidence of stunting, such as mother’s knowledge, role of parents, weight of new baby born, incomplete immunization, consistency of complementary feeding, and inadequate access to healthcare facilities.11–13 A study conducted by Beal et al, on stunting of determinants in Indonesia concluded that short and uneducated mothers, premature babies, poor families, and children in poor urban areas, especially rural areas are particularly vulnerable to stunting.14 Another research by Kustanto, shows that several regions in Indonesia have poverty below the national average and above the national average for cases of toddlers experiencing stunting. These things show that family socio-economic is one aspect that has a lot to do with the incidence of stunting.15
It is widely acknowledged that the socioeconomic circumstances of a family income are correctly reflected in that family expenditures. The dietary habits of families are influenced by socioeconomic circumstances that may affect stunting. Households and people with lower socioeconomic status (SES) are more likely to have poor health. As a result, unforeseen health incidents can be particularly devastating for low-income households, as they can disrupt employment, create new household economic needs and increase the burden on households.16 Estimating the prevalence or risk factors for stunting can help inform improved public health initiatives.9
The employment status of mothers is another crucial predictor to consider. Maternal employment can have both positive and negative effects on child health and well-being. On one hand, maternal employment can potentially increase family income, improve access to resources, and positively influence child health outcomes. On the other hand, It may also lead to reducing the time available for maternal caregiving and increased reliance on alternative childcare arrangements, which can potentially have negative implications for child nutrition and growth. By knowing these determinants, it is hoped that the incidence of stunting may decrease when preventive efforts are made. Prevention requires a range of initiatives involving community involvement and immediate caregiver parents. Moreover, investigating the determinants can provide valuable insights into the interplay between maternal work, family, dynamics, and child health. On this basis, this study aims to investigate the mother’s employment, family income, and expenditure as predictors factors that influence the stunting of children under five years of age in Indonesia. Those predictors were selected based on several important considerations. Specifically, it is hypothesized that children of employed mothers, those from families with higher income, and those with higher family expenditures are less likely to experience stunting compared to their counterparts. By examining this hypothesis, the study seeks to contribute to the existing literature on the determinants of stunting, and provide insights into the potential strategies that could be implemented to reduce stunting. The implications of this research could inform policy and programmatic interventions aimed at reducing stunting and improving child health outcomes in Indonesia.
Our data were collected from diverse households across different districts in west java, ensuring broad representation. For analysis, we utilized bivariate correlation and regression to examine the associations between the variables. The key strength of our study lies in providing preliminary insights into the relationships between mother’s employment, family income, expenditure, and stunting, despite the simplicity of the analytical approach. These findings can serve as a basis for future research to explore more complex relations and interactions among variables.
Methods
Study Design
This research used a cross-sectional design approach with the purpose of investigating the predictor stunting in children under five. This took three months, especially from October to December 2018.
Recruiting and Sampling
The study was conducted on couples of childbearing age with the criteria of first to third-trimester pregnant women or having children under five years of age. Participants in this study came from 6 provinces in West Java, Indonesia, namely Bandung Regency, Bandung City, Garut Regency, West Bandung Regency, Subang Regency, and Sumedang Regency. The six districts or cities are designated as research areas based on the areas with the highest incidence of stunting in West Java (Bappenas, 2017).
The minimum sample size is based on the total population according to the sample table of Isaac and Michael with a significance level of 1% ± 550,000 population. With a total of 534,652 from the six areas, the minimum sample size required is 665–810 respondents. In this study, the final sample used consisted of 801 respondents. In recruiting, the cluster sampling technique was used from 6 sub-districts or 6 urban villages with KB villages. Thus, the number of respondents from each area was represented by 135 respondents. As for the total sample of 801 respondents, 731 participated in the study because they met the criteria for this study. (See Figure 1).
 |
Figure 1 STROBE Diagram. |
Data Collecting
This study utilized data from the Ministry of Health of the Republic of Indonesia, and the instruments used were based on established guidelines. Validity checks through content validity and internal validity would have been valuable in ensuring that the study instrument accurately measured the intended constructs and controlled for confounding factors. Data collection was carried out using a questionnaire that measures sociodemographic factors such as employment, income, and family expenses. Researchers carried out the categorization of child stunting from respondents. To detect children’s growth retardation, physical observations are carried out using anthropometric measurements, so that the child’s health status can be known. Information was also collected based on patient records from MCH (Maternal and Child Health Books) to study stunting as part of the health status of mothers and children.
Statistical Analysis
Data in this study were analyzed using descriptive statistics (frequency distribution) and a bivariate test with Spearman Rank. Furthermore, an analysis was also carried out with logistic regression to determine the factors that are predictors of stunting. The entire statistical analysis was carried out using the Jamovi software.
Ethical Clearance
This study strictly adheres to the ethical principles outlined in the Declaration of Helsinki. This study has received approval from the Research Ethics Commission of Padjadjaran University with letter number 1206/UN6/KEP/EC/2018. Before carrying out the research, informed consent to participate in the study was provided by parents of the respondents. To protect the confidentiality of the participants, all data were collected and stored using unique identification codes or pseudonyms instead of using their actual names. Access to identifiable information was limited to only authorized research team members, and data were securely stored with restricted access.
Results
Characteristics of Included Studies
A total of 731 participants entered the study based on the included criteria. The result showed that 79.9% mothers unemployed, 45.5% of the mothers with family income <1.500.000, 42.1% have family expenses of >1.500.000–2.000.000, and 56.1% are classified into the good environmental category based on the activities carried out. Therefore, most of the participants had children with normal height, which was 72.8%. There were also children who were included in the short category at 18.7% and very short at 5.3%. It can be seen in Table 1.
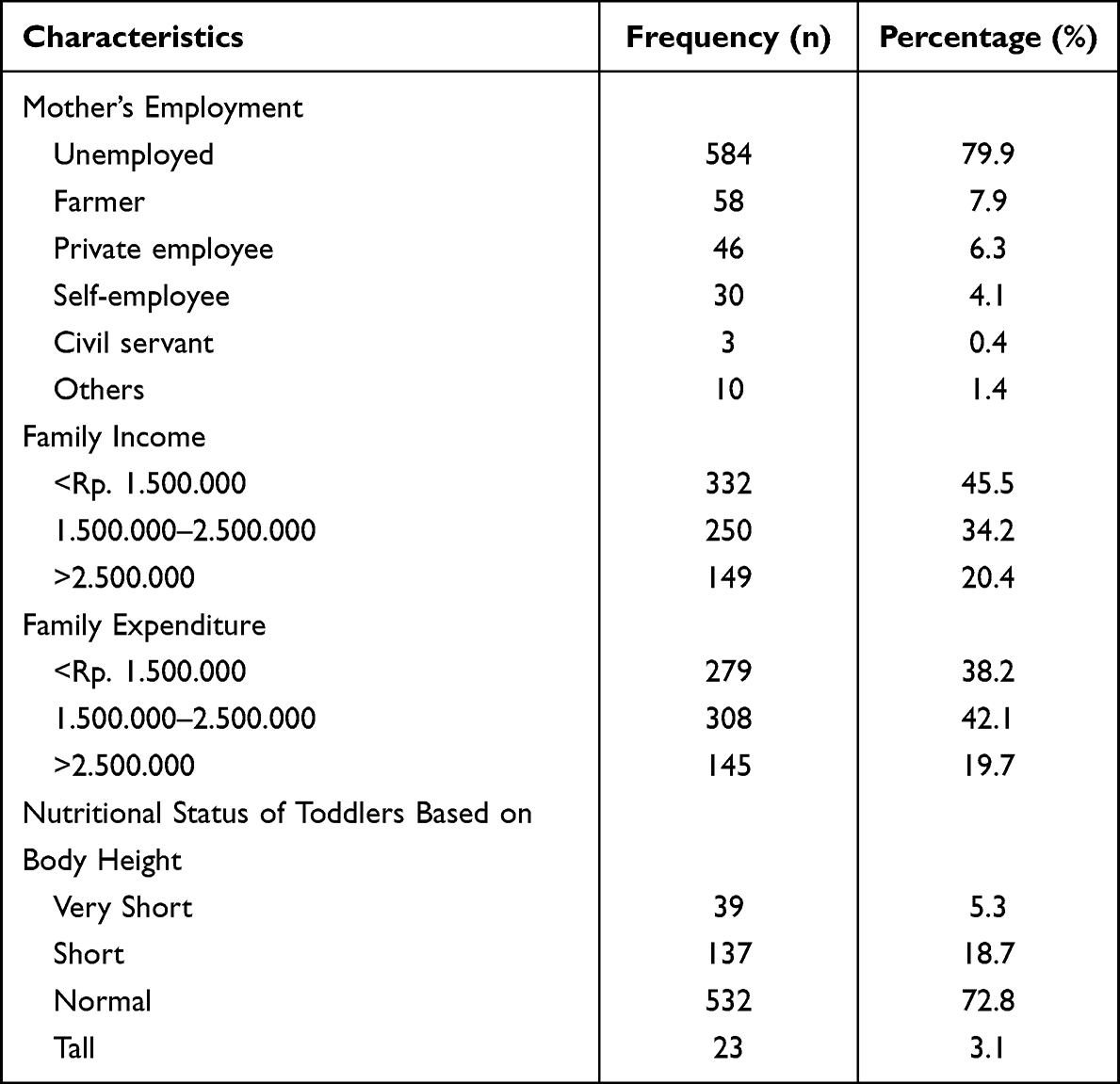 |
Table 1 Baseline Data of Participants (n=731) |
Study Outcome
Relation Between Mother’s Employment, Family Income and Expenditure with Stunting
Table 2 shows the relation between mother’s employment, family income, and family expenditure with stunting. According to the analysis of the relation between the mother’s employment, family income, and expenditure, the results showed that only mother’s employment (p-value< 0.005) had a relationship with stunting. Meanwhile, other factors showed insignificant results with the incidence of stunting.
 |
Table 2 Relation Between Mother’s Employment, Family Income and Expenditure with Stunting |
Factor’s Affecting Stunting
The results of the multivariate analysis showed that only mother’s employment was a factor that affected stunting, with a p-value= 0.017 (OR = 1.810). The OR value means that mothers who do not work have a 1.810 chance for their children to experience stunting compared with mothers who have work. In addition, there is a variable with negative estimated value, namely family expenditure. Although the variable showed no significant result as a predictor of stunting, the negative estimated value obtained shows that families with low expenditure have a lower probability of stunting. It can be seen in Table 3.
 |
Table 3 Factors Affecting Stunting |
Discussion
Principal Finding
The present study discussed the relationship between socio-economic factors and stunting among children under five in West Java Province, Indonesia. Stunting in children under five is a major concern in low-middle income countries, particularly Indonesia. It is common knowledge that family expenditure accurately reflects the socioeconomic circumstances of that family income. When a family is unable to meet its financial obligations, its purchasing power falls and starvation occurs. Socioeconomic factors affect family eating patterns.17 The eating behavior of the family must be evaluated owing to the influence of the selection and consumption of food, as well as the quality of household food.
Previous studies have demonstrated a strong correlation between stunting and socioeconomic status. De Silva and Sumarto and Mani et al provided evidence that increased household higher income expenditure spending per capita reduces the prevalence of childhood stunting.18,19 A previous study in Indonesia showed that households in the top quintile of animal-source food expenditure had a lower risk of stunting in urban poor children (AOR 0.87, 95% CI [0.85, 0.90]) and rural children under five (AOR 0.78, 95% [0.74, 0.81]).20 This study confirmed that family income and expenditure are not correlated with stunting among children under five. Only mothers’ employments are associated with stunting in children under five, where the mother unemployed is more vulnerable to stunting than the mother employed. Our finding of an overall higher risk of stunting among children of mothers’ employments is consistent with earlier findings from an Ethiopia study that found stunting incident more highly among children with mother unemployed and poor child nutritional status in slums and stunting incident highly among children with mother’s employed.21–23 This finding may correlate with higher difficulties with child care as a result of financial issues.24
This study contributes theoretically and practically to the understanding of predictor stunting from the socioeconomic household in Indonesia. This work contributes to the theoretical understanding of stunting prevalent and their drivers in socioeconomic views. From a practical standpoint, the varying drivers of stunting by household socioeconomic (degree of mother employment, family income, and family expenditure) need a variety of strategies to combat stunting. Based on our findings, an additional food assistance program for children under five years for families with low incomes may be able to prevent stunting due to malnutrition related to family finances. Some studies also indicate that providing children with supplementary feeding and multiple micronutrients enhances linear growth.25–28 Moreover, one of these programmatic approaches is the Preventing Malnutrition in Children Under 2 Years of Age Approach (PM2A), which is a food-assisted maternal and child health and nutrition (FA-MCHN) program model for women and children during the first 1000 days. PM2A was made to give women and children in the first 1000 days a set of interventions that would improve food security in the home and the diets and health of mothers and children. A current study by Olney et al showed that a well-designed FA-MCHN program that focused on pregnant women and children up to 24 months old could significantly improve linear growth and reduce stunting in the first 1000 days.29
Strengths and Limitation
To the best of our knowledge, this study is the first of its kind to investigate the correlation between mother’s employment, family income, and family expenditure with stunting at the stunting locus in West Java, Indonesia. However, the study had several limitations that should be acknowledged. First, the cross-sectional design limited the inference of causality. Secondly, there was the potential for bias because many of the variables were self-reported, and uncontrolled confounding factors could not be ruled out. Finally, we cannot explain culturally how the perceptions and eating patterns of children with stunting. Culture-based studies may be able to explain further, so an explanatory study is needed to examine more deeply the perceptions and eating patterns that are determinants of stunting.
Implication for Practice and Further Research
The findings of this study have important implications for practice and further research. First, the study highlights the need for policies and programs that promote maternal employment, particularly in low-income households, as a means of reducing the prevalence of stunting among children under five. This could include initiatives such as job training and placement services, as well as policies that provide support for working mothers, such as paid parental leave and flexible working hours.
Second, the study suggests that while family income and expenditure may not be significant predictors of stunting, they still play an important role in child health outcomes. Therefore, future research should examine the complex relationships between income, expenditure, and stunting in more detail, and explore the potential mechanisms underlying these relationships.
While our study focused on investigating the predictors of stunting among children under five, we acknowledge that there may be other factors that could play significant roles in the prevalence of stunting in our specific area. Future research in this field should explore additional variables such as the quality of healthcare services, access to sanitation facilities, cultural practices related to child feeding, and maternal health status. These factors may provide further insights into the complex dynamics associated with stunting. As for the specific explanation regarding the relationship between maternal work variables and stunting toddlers, we hypothesize that it may be attributed to the potential challenges faced by working mothers in ensuring optimal nutrition and caregiving for their children. Factors such as time constraints, lack of support systems, and limited resources may contribute to suboptimal feeding practices and reduced attention to a child’s nutritional needs. However, further research is needed to delve deeper into these aspects and to gain a comprehensive understanding of the underlying mechanisms involved. By expanding our investigations and exploring a wider range of factors, we aim to provide a more holistic view of the stunting issue and identify potential interventions that can effectively address this pressing public health concern.
Conclusion
The present study concluded that mothers’ employment is a potential predictor of stunting among children under five. However, family income and expenditure cannot predict stunting. Additional analyses are encouraged to provide new insights and further address the complexity of the factors influencing stunting, which may involve exploring potential interactions among these variables or considering other relevant determinants in a complex model context using the Structural Equation Model (SEM). Furthermore, to reduce the prevalence of stunting, the government should consider implementing policies and programs that provide nutritional support and empowerment programs for pregnant women and children, particularly those from low-income households. This could include initiatives such as providing access to affordable and nutritious food, promoting healthy feeding practices, and increasing access to healthcare services.
Data Sharing Statement
The data contains personal information that our participants consented to being used for research purposes only and not for public disclosure. To protect the privacy and confidentiality of our participants, we are required to keep the data restricted and limit access to authorized individuals only. The data that support the findings of this study are available from the first author (LR), upon reasonable request.
Acknowledgment
We would like to thank the Indonesian Population Board, and Ministry of Research, Technology and Higher Education, Universitas Padjadjaran, and also the community leaders and the community leaders and the community itself in all Regencies and Cities in West Java Province for the participation in our study.
Funding
This research is conducted by financial support from Indonesian Population Board, and Ministry of Research, Technology and Higher Education and Universitas Padjadjaran with contract numbers 4414/HK.03.01/J.6/2018, 591/UN6.L/PKS/2018 and 1827/UN6.3.1/LT/2020. Morover, this APC was paid by Directorate for Research and Community Engagement, Universitas Padjadjaran.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Yani DI, Rahayuwati L, Sari CWM, Komariah M, Fauziah SR. Family household characteristics and stunting: an update scoping review. Nutrients. 2023;15(1):233. doi:10.3390/nu15010233
2. World Health Organization. Malnutrition. Available from: https://www.who.int/health-topics/malnutrition#tab=tab_1.
3. Utami RA, Setiawan A, Fitriyani P. Identifying causal risk factors for stunting in children under five years of age in South Jakarta, Indonesia. Enferm Clin. 2019;29:606–611. doi:10.1016/j.enfcli.2019.04.093
4. De Sanctis V, Soliman A, Alaaraj N, Ahmed S, Alyafei F, Hamed N. Early and long-term consequences of nutritional stunting: from childhood to adulthood. Acta Bio Med. 2021;92(1):e2021168. doi:10.23750/abm.v92i1.11346
5. World Health Organization. Nutrition. Available from: https://www.who.int/nutrition/topics/2_background/en/index1.html.
6. Rosiyati E, Pratiwi EAD, Poristinawati I, et al. Determinants of stunting children (0–59 months) in some countries in Southeast Asia. J Kesehat Komunitas. 2019;4(3):88–94. doi:10.25311/keskom.vol4.iss3.262
7. de Onis M, Borghi E, Arimond M, et al. Prevalence thresholds for wasting, overweight and stunting in children under 5 years. Public Health Nutr. 2019;22(1):175–179. doi:10.1017/S1368980018002434
8. United Nations Children’s Fund. Four out of ten of the world’s stunted children live in South Asia; 2022. Available from: http://www.unicefrosa-progressreport.org/stopstunting.html.
9. Kragel EA, Merz A, Flood DMN, Haven KE. Risk factors for stunting in children under the age of 5 in rural guatemalan highlands. Ann Glob Health. 2020;86(1):8. doi:10.5334/aogh.2433
10. Titaley CR, Ariawan I, Hapsari D, Muasyaroh A, Dibley MJ. Determinants of the stunting of children under two years old in Indonesia: a multilevel analysis of the 2013 Indonesia basic health survey. Nutrients. 2019;11(5):1106. doi:10.3390/nu11051106
11. Mishra K, Kumar P, Basu S, Rai K, Aneja S. Risk factors for severe acute malnutrition in children below 5 y of age in India: a case-control study. Indian J Pediatr. 2014;81(8):762–765. doi:10.1007/s12098-013-1127-3
12. Silas L, Rantetampang AL, Tingginehe R, Mallongi A. The factors affecting stunting child under five years in sub province mimika. Int J Sc Healthc Res. 2018;3(2):99.
13. Torlesse H, Cronin AA, Sebayang SK, Nandy R. Determinants of stunting in Indonesian children: evidence from a cross-sectionalsurvey indicate a prominent role for the water, sanitation and hygiene sector in stunting reduction. BMC Public Health. 2016;16:669. doi:10.1186/s12889-016-3339-8
14. Beal T, Tumilowicz A, Sutrisna A, Izwardy D, Neufeld LM. A review of child stunting determinants in Indonesia. Matern Child Nutr. 2018;14(4):12617. doi:10.1111/mcn.12617
15. Kustanto A. The prevalence of stunting, poverty, and economic growth in Indonesia: a panel data dynamic causality analysis. J Dev Econ. 2021;6(2):150. doi:10.20473/jde.v6i2.22358
16. Leonard T, Hughes AE, Pruitt SL. Understanding how low-socioeconomic status households cope with health shocks: an analysis of multi-sector linked data. Ann Am Acad Pol Soc Sci. 2017;669(1):125–145. doi:10.1177/0002716216680989
17. Black RE, Victora CG, Walker SP, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382(9890):427–451. doi:10.1016/S0140-6736(13)60937-X
18. De Silva I, Sumarto S. Child malnutrition in Indonesia: can education, sanitation and healthcare augment the role of income? J Int Dev. 2018;30(5):837–864. doi:10.1002/jid.3365
19. Mani S. Socioeconomic determinants of child health: empirical evidence from Indonesia. Asian Econ J. 2014;28(1):81–104. doi:10.1111/asej.12026
20. Sari M, de Pee S, Bloem MW, et al. Higher household expenditure on animal-source and nongrain foods lowers the risk of stunting among children 0–59 months old in Indonesia: implications of rising food prices. J Nutr. 2010;140(1):195S–200S. doi:10.3945/jn.109.110858
21. Ahmed M, Zepre K, Lentero K, et al. The relationship between maternal employment and stunting among 6–59 months old children in Gurage Zone Southern Nation Nationality People’s region, Ethiopia: a comparative cross-sectional study. Front Nutr. 2022;9:964124. doi:10.3389/fnut.2022.964124
22. Eshete H, Abebe Y, Loha E, Gebru T, Tesheme T. Nutritional status and effect of maternal employment among children aged 6–59 months in Wolayta Sodo town, Southern Ethiopia: a cross-sectional study. Ethiop J Health Sci. 2017;27(2):155–162. doi:10.4314/ejhs.v27i2.8
23. Negash C, Whiting SJ, Henry CJ, Belachew T, Hailemariam TG. Association between maternal and child nutritional status in Hula, rural SouthernEthiopia: a cross sectional study. PLoS One. 2015;10(11):e0142301. doi:10.1371/journal.pone.0142301
24. Tette EMA, Sifah EK, Nartey ET, Nuro-Ameyaw P, Tete-Donkor P, Biritwum RB. Maternal profiles and social determinants of malnutrition and the mdgs: what have we learnt? BMC Public Health. 2016;16(1):214. doi:10.1186/s12889-016-2853-z
25. Christian P, Shaikh S, Shamim AA, et al. Effect of fortified complementary food supplementation on child growth in ruralBangladesh: a cluster-randomized trial. Int J Epidemiol. 2015;44(6):1862–1876. doi:10.1093/ije/dyv155
26. Panjwani A, Heidkamp R. Complementary feeding interventions have a small but significant impact on linear and ponderal growth of children in low- and middle-income countries: a systematic review and meta-analysis. J Nutr. 2017;147(11):2169S–2178S. doi:10.3945/jn.116.243857
27. Shafique S, Sellen DW, Lou W, Jalal CS, Jolly SP, Zlotkin SH. Mineral- and vitamin-enhanced micronutrient powder reduces stunting in full-term low-birth-weight infants receiving nutrition, health, and hygiene education: a 2 × 2 factorial, cluster-randomized trial in Bangladesh. Am J Clin Nutr. 2016;103(5):1357–1369. doi:10.3945/ajcn.115.117770
28. Adu-Afarwuah S, Lartey A, Okronipa H, et al. Small-quantity, lipid-based nutrient supplements provided to women during pregnancy and 6 mo postpartum and to their infants from 6 mo of age increase the mean attained length of 18-mo-old children in semi-urban Ghana: a randomized controlled trial. Am J Clin Nutr. 2016;104(3):797–808. doi:10.3945/ajcn.116.134692
29. Olney DK, Leroy J, Bliznashka L, Ruel MT. PROCOMIDA, a food-assisted maternal and child health and nutrition program, reduces child stunting in Guatemala: a cluster-randomized controlled intervention trial. J Nutr. 2018;148(9):1493–1505. doi:10.1093/jn/nxy138
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.