Back to Journals » Risk Management and Healthcare Policy » Volume 16
The Influence of Diagnosis Intervention Packet Policy Intervention on Medication Structure and Drug Cost of Elderly Hypertensive Inpatients in China: A Multicenter Interrupted Time-Series Analysis
Authors Hong D, Lv D, Wu J, Li X, Zhao Q, Lu X, Li L
Received 24 April 2023
Accepted for publication 22 August 2023
Published 8 September 2023 Volume 2023:16 Pages 1781—1790
DOI https://doi.org/10.2147/RMHP.S418541
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Haiyan Qu
Dongsheng Hong,1,2 Duo Lv,1 Jiaying Wu,1 Xin Li,1 Qingwei Zhao,1 Xiaoyang Lu,1 Lu Li2
1Key Laboratory for Drug Evaluation and Clinical Research of Zhejiang Province, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2Department of Social Medicine of school of Public Health, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China
Correspondence: Xiaoyang Lu, Key Laboratory for Drug Evaluation and Clinical Research of Zhejiang Province, the First Affiliated Hospital, Zhejiang University School of Medicine, 79 Qingchun Road, Hangzhou, 310003, People’s Republic of China, Email [email protected] Lu Li, Department of Social Medicine of school of Public Health, Zhejiang University School of Medicine, 866 Yuhangtang Road, Hangzhou, 310058, People’s Republic of China, Email [email protected]
Background: DIP is a new medical insurance payment system developed in China which was implemented in Guangzhou in January 2018, but few studies have focused on its intervention effect on the drug burden of elderly hypertensive patients.
Methods: Nine medical institutions in Guangzhou, China, were selected, among which, daily full medical orders of elderly hypertensive inpatients from 2016 to 2020 were randomly collected. To assess the impact of DIP policy intervention on patient drug burden, we took the data after policy implementation in January 2018, as the intervention data, and applied a segmented regression model with interrupted time series to analyze the trend and changes in average daily drug costs per month and medication structure, stratified by age, sex, and inpatient department.
Results: A total of 34,276 elderly hypertensive patients’ daily full medical orders were obtained. The immediate level change of drug costs after intervention was − 23.884 RMB/month (P = 0.652), and the trend change was statistically significant (− 15.642 RMB/month, P = 0.002). The relative cumulative effect at the end of the study was − 78.860% (95% CI: − 86.087% to − 69.076%), and the intervention effect was more significant in surgical and male patients. The analysis of drug structure changes showed that after the implementation of the DIP policy intervention, the proportion of anti-infective drugs, anti-tumor drugs, and biological products all showed a significant downward trend (P < 0.05), while nutritional drugs showed a significant upward trend (P = 0.011), but no immediate horizontal change in slope was observed.
Conclusion: The typical practice in China showed that DIP policy intervention can improve the drug burden of elderly hypertensive hospitalized patients and has a stable long-term effect, and the intervention effect is not consistent across different clinical department and populations with different characteristics, and it would also cause changes in the medication structure.
Keywords: diagnosis-intervention packet policy, daily drug cost, interrupted time series analysis, elderly hypertension, medication structure
Introduction
The aging of the population and the increasing social demand for medical resources have caused the rapid growth of medical expenses in China.1,2 To control the unreasonable growth of medical expenses, the Chinese government is promoting the reform of multiple and compound medical insurance payment modes. Among them, Big Data Diagnosis-Intervention Packet (DIP) policy intervention,3 as original medical insurance payment mode, has been extensively piloted in many regions of China. With the continuous promotion of DIP policy, it can be predicted that shortly, China’s DIP policy will have an impact on the medical expenditure of hundreds of millions of inpatients.4
Previous studies have found that DIP policy has a positive effect on reducing the medical expenditure but mainly focusses on the total cost of inpatients.5,6 With the drug zero addition reform promoted in recent years, drug costs have become a huge cost burden for hospitals under the DIP policy. There are few studies that rigorously evaluate the effects of the DIP policy on the changes in drug expenditure and medication structure.
The other hand, the elderly hypertensive population has become one of the largest chronic patient populations in China, and the prevalence of hypertension among the elderly over 60 years old in China has exceeded 50%.7 Elderly patients with hypertension as a special group, often accompanied by a variety of diseases, increased access to a variety of drug treatment after hospitalization. With the aging of the population, the hospitalization burden of elderly hypertensive patients will increase further.8 Patients are the main stakeholders of the DIP policy, and the impact of policy on drug costs can directly reflect the implementation effect of the policy.9 Guangzhou City has fully implemented DIP policy since January 1, 2018.5 To scientifically evaluate the design and implementation of the DIP policy intervention, this study provides systematic evidence on the medication of elderly hypertensive hospitalized patients in Guangzhou, China. We used the medication data before and after the implementation of the DIP policy from January 2016 to December 2020, the changing trend of drug expenses and the change in medication structure were compared following policy intervention.
Methods
Study Design
This study evaluated the implementation effect of DIP policy intervention through interrupted time-series (ITS) analysis.10 Taking medical institutions in Guangzhou, China, as the research background, through 60 months of continuous study, changes in inpatient drug costs before intervention (January 2016–December 2017) and after intervention (January 2018–December 2020) for elderly hypertensive inpatients were evaluated. The study report follows the Transparent Reporting of Evaluations with Nonrandomized Designs (TREND) statement11 (Appendix 1) for improving the reporting quality of nonrandomized designs of public health interventions and the Template for Intervention Description and Replication (TIDieR) Checklist (Appendix 2).12
Data Sources
Data of this study are from the Hospital Prescription Cooperation Project (HPCP), which was initiated by the Hospital Pharmacy Professional Committee of the Chinese Pharmaceutical Association. These data have been utilized by previously published studies.13,14 The HPCP data were obtained by random sampling of the medication data of designated hospitals in China. This study adopted the medication data of hypertensive inpatients in Guangzhou in HPCP from 2016 to 2020 (Appendix 3 provides detailed hospital order information for different hospitals), from the departments where hypertensive patients are more, specifically including cardiology, neurosurgery, and cardiothoracic surgery departments. According to the standard for healthy Chinese older adults,15 the sampling method is extracting the daily full doctor orders of elderly inpatients diagnosed with hypertension and aged 60 years or older, not including hypertensive outpatients. The data extraction rule is 10 days are sampled in a quarter, including 2 non-consecutive Mondays to Fridays (national holidays are not sampled). Data extraction fields include prescription time, prescription number, prescription department, drug generic name, drug specification, the quantity of medicine taken, prescription amount, patient gender, patient age, and original diagnosis of prescription.
DIP Policy Intervention Measures
Guangzhou Healthcare Security Administration (GHSA) formulated specific intervention measures according to the overall requirements of China’s action plan for the reform of the medical insurance payment mode,16 which mainly includes four parts: the determination of the disease category grouping directory, the determination of the disease category score, the determination of the weight coefficient of medical institutions and the determination of the medical insurance payment fees. The intervention measures have been implemented since January 2018. The details are as follows:
- Determination of disease category grouping directory: based on the data of social medical insurance inpatient cases of designated medical institutions in Guangzhou from 2015 to 2017, according to the first clinical diagnosis code of discharged cases (ICD-10), combined with the surgery and operation code (ICD-9-CM-3), the relevant disease categories were selected and form a disease category directory for DIP.
- Determination of disease score: when determining the disease score, “acute appendicitis: appendectomy, laparoscopy (K35.9:47.0101)” was taken as the benchmark disease, and each disease category score was determined according to the ratio of the average cost of each disease to the average cost of the benchmark disease. Among them, for the cases whose cost is more than 2 times the average cost of the same level in the previous year, the disease type score would be added, and for the disease type whose cost is less than 50% of the average cost of the same level in the previous year, the settlement will be based on the actual score.
- Determination of the weight coefficient of medical institutions: the weight coefficient is composed of the basic weight coefficient and the addition coefficient. The basic weight coefficients of the third-level medical institutions, the second-level medical institutions and the first-level medical institutions are 1, 0.728 and 0.47, respectively. Appendix 4 provides the setting of the addition coefficient. The setting rules would be adjusted dynamically every year according to the actual situation.
- Determination of medical insurance payment expense: according to the total medical insurance fund budget used to pay for hospitalization expenses in Guangzhou, determined by the disease category score of cases received by medical institutions and the weight coefficient of medical institutions.
Outcome Measures
The main outcome indicator of this study is the average daily drug cost per month of elderly hypertensive inpatients, and stratified analysis was conducted according to internal medicine, surgery, gender and age (60–69, 70–79, 80 and above) to evaluate the intervention effect of DIP policy on outcome indicators of different clinical departments and patients with different characteristics.
The secondary outcome indicator of this study is the proportion of drug expenditure of each category per 100 RMB, so as to evaluate the intervention effect of DIP policy on the change of medication structure in medical institutions. Among them, drug categories are mainly divided into 18 categories by reference to anatomical treatment and chemical classification (ATC classification), including respiratory drugs, musculoskeletal system drugs, hormone drugs, biological products, anti-infective drugs, anti-tumor drugs, urinary system drugs, immune system drugs, vitamins and minerals drugs, nervous system drugs, digestive system drugs, nutrition drugs, electrolytes and acid–base balance drugs, specialized drugs, blood system drugs, digestive system drugs, cardiovascular system drugs and other drugs, also including Chinese patent medicine.
Statistical Analysis
The continuous variables were expressed in mean (standard deviation) or median (interquartile interval), and the categorical variables were expressed in percentage. This study evaluated the effect of DIP policy intervention from the perspective of drug utilization. The ITS model was applied to evaluate the impact of DIP policy intervention on drug costs and medication structure of patients. ITS is a commonly used method to evaluate the changes in longitudinal sequence after quasi-trial intervention at a fixed time point.10 The time when Guangzhou implemented the DIP policy in January 2018 is considered the intervention time point of ITS analysis. We utilized a piecewise regression model of baseline trend control to estimate the level and trend change of each outcome variable after DIP policy intervention. The assumption of model specification was that the introduction of DIP policy intervention would affect the drug cost and medication structure of inpatients, and ITS regression model constructed was as follows:
Yt=β0+β1×Tt+β2×Interventiont+β3×Timeafterinterventiont +εt
Yt was the outcome variable. β0 was the estimated value of the outcome variable baseline level at the beginning of the study; β1 was the slope before intervention; β2 was the immediate level change of outcome variables after intervention; β3 was the long-term trend of outcome variables after intervention; Tt was the time counting variable; Interventiont was the intervention indicator variable; Timeafterinterventiont was the time counting variable after intervention; εt was the estimated value of the random error at time t. The autocorrelation level of the model was estimated through the Durbin–Watson test.17 If there was autocorrelation, the Prais–Winston method was used to estimate the regression, and the adjusted Durbin–Watson (DW) value was used to judge the adjustment effect of the model on autocorrelation.18 The previously described method was used to estimate the relative and absolute changes of outcome variables,19 and the bootstrapping method was used to estimate the 95% confidence interval (CI) of the absolute and relative changes of cumulative effects.20 The normality test of model residuals was evaluated by the Shapiro–Wilk test. All statistical tests were conducted on both sides, and the difference was considered statistically significant if P < 0.05. R software was used for all statistical analysis, version 3.6.1 (http://www.R-project.org).
Results
Basic Characteristics
This study included 34,276 daily full medical orders of elderly hypertensive inpatients from 9 medical institutions in Guangzhou. The median value of the number of patients per month was 560 (quartile range: 478.25–707.25). The average age of patients was 73.76 years. Male patients accounted for 46.09%. Cardiology patients accounted for 87.15%. Local medical insurance patients accounted for 88.20%. Refer to Table 1 for data distribution in different years from 2016 to 2020; The data of 16,770 patients were included before DIP policy intervention, and 17,506 patients were included after DIP policy intervention. The average daily drug cost of patients decreased from 482.98 RMB in January 2016 to 240.79 RMB in December 2020, and the decrease rate is 50.14% (Figure 1).
 |
Table 1 Basic Characteristics of Daily Full Medical Orders in Sample Hospital from 2016 to 2020 |
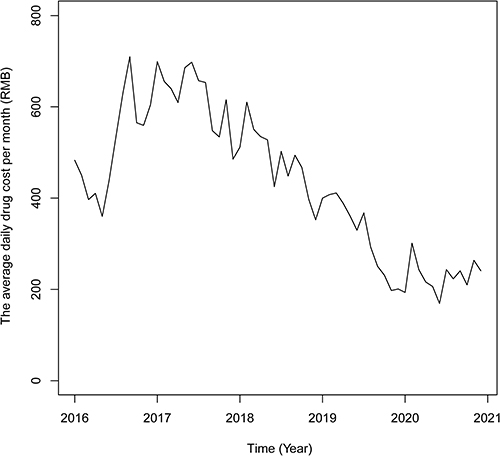 |
Figure 1 Trend of average daily expenses of elderly hypertensive inpatients in Guangzhou from 2016 to 2020. |
The Impact of DIP Policy Intervention on the Medication Structure
ITS modeling was carried out with the proportion of medication of each category per 100 RMB as the dependent variable. Autocorrelation test displayed that the distribution range of DW value or adjusted DW value was between 1.423 and 2.508. Table 2 provides detail model parameters. The results showed that after intervention, the use of anti-infective drugs, anti-tumor drugs and biological products showed significant downward trends, and the trend change was statistically significant, with data of −0.351%/month (P = 0.012), −0.227%/month (P = 0.019) and −0.076%/month (P = 0.025), respectively.
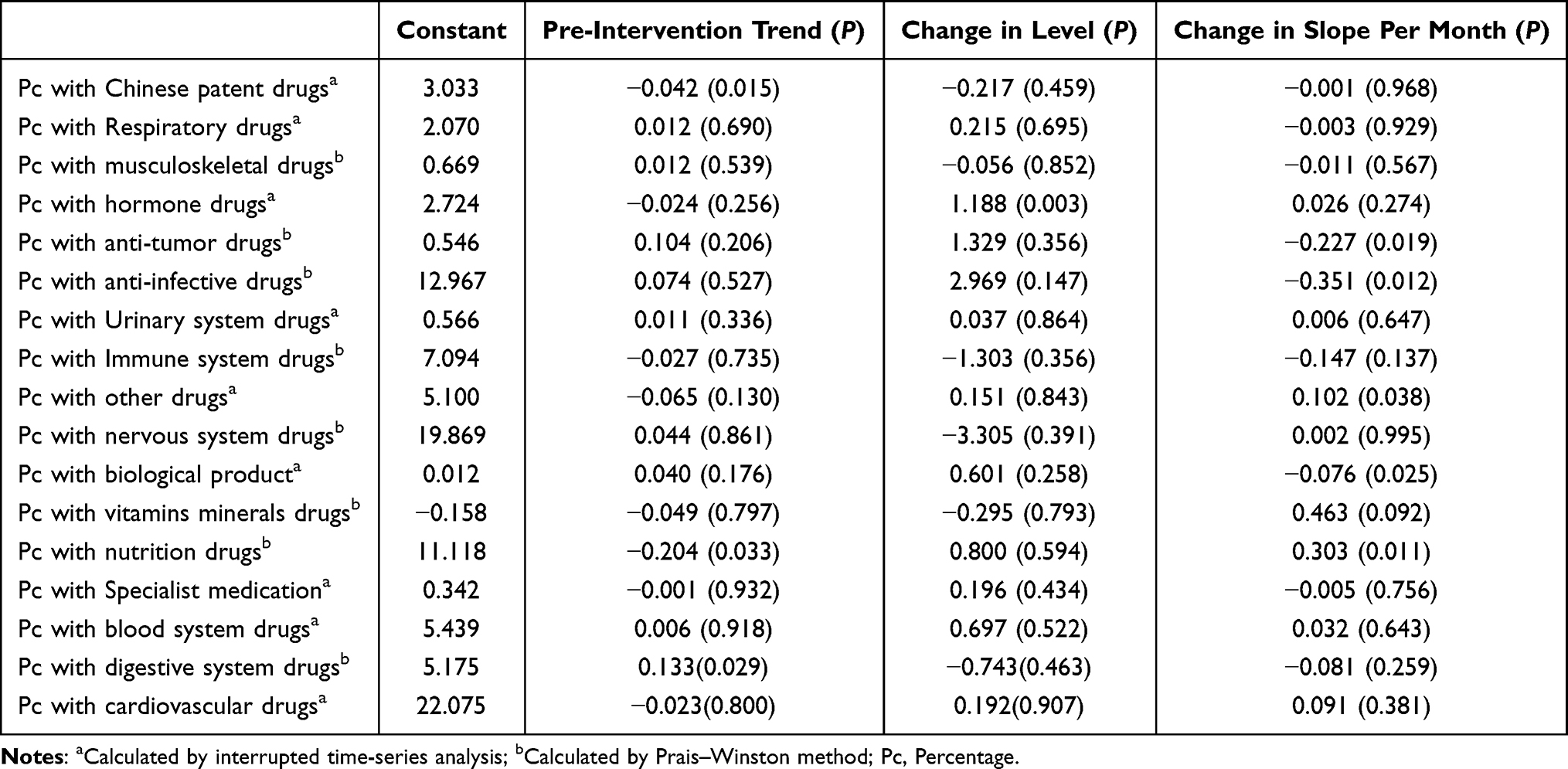 |
Table 2 Trends of the Proportion of Different Drugs Used After Implementation of DIP Policy Intervention |
In addition, before intervention, the proportion of medication in the digestive system showed an upward trend (0.133%/month, P = 0.029), and after intervention, the upward trend of the proportion of medication changed, with a trend of −0.081%/month (P = 0.259). The proportion of Chinese patent medication showed a downward trend before intervention (−0.042%/month, P = 0.015), and the downward trend of such drugs disappeared after the intervention. The proportion of nutritional medication showed a downward trend before intervention (−0.204%/month, P = 0.033), while after intervention, the proportion of such medication changed to an upward trend, which was statistically significant (0.303%/month, P = 0.011).
The Impact of DIP Policy Intervention on Drug Burden
ITS modeling was carried out based on the dependent variables of patients’ average daily drug cost per month. The DW value or adjusted DW value was from 1.835 to 2.043, indicating that the model data finally included in the analysis met the autocorrelation test requirements.21 Table 3 shows the model parameters. The results indicated that before intervention, the average daily drug cost of elderly hypertensive inpatients per month showed an upward trend (4.080 RMB/month, P = 0.271), and the immediate level change of drug cost after intervention decreased (−23.884 RMB/month, P = 0.652), and the trend change was statistically significant (−15.642 RMB/month, P = 0.002). At the end of the study, the estimated value of the relative cumulative effect was −78.860% (95% CI: −86.087% to −69.076%), suggesting that an average of −586.986 RMB was saved for each patient within 36 months after the intervention (Figure 2).
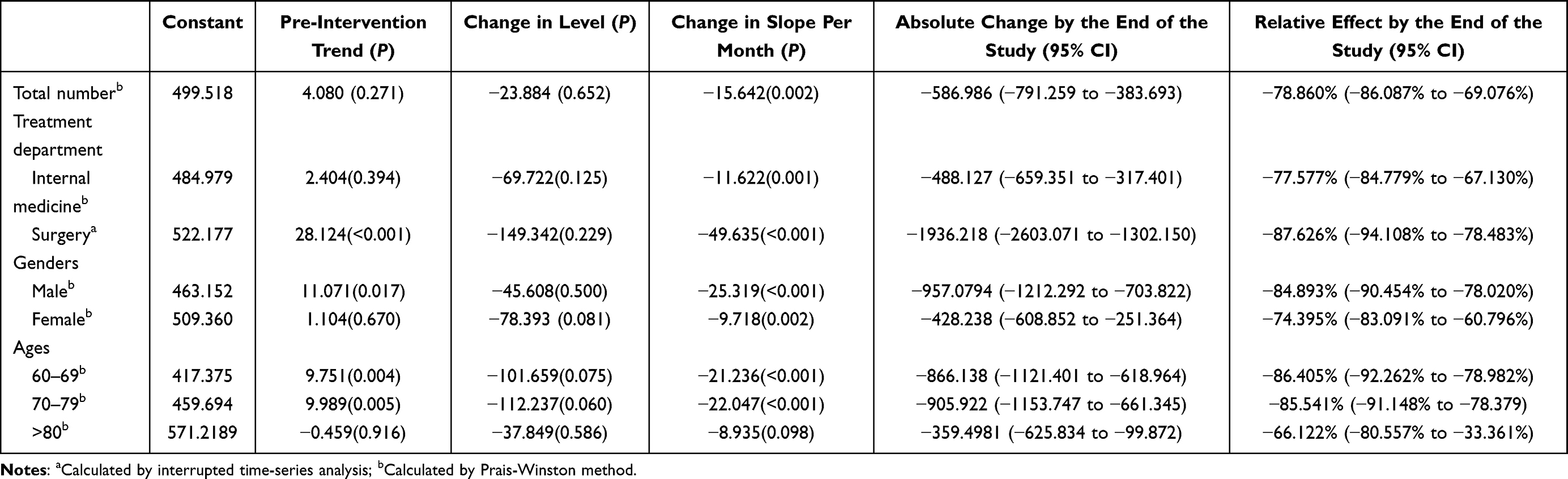 |
Table 3 Segmented Regression Analyses for the Average Daily Drug Cost per Month of Elderly Hypertensive Inpatients |
 |
Figure 2 Effect of Diagnosis-Intervention Packet (DIP) policy intervention on Drug Burden of Elderly Hypertensive Inpatients. Notes: (A) The intervention effect of all populations; (B) aged 60–69; (C) aged 70–79; (D) elderly people aged 80 and above. |
The subgroup analysis is shown in Table 3. The relative cumulative effect of surgical patients at the study cutoff point after DIP policy intervention was −87.626% (95% CI: −94.108% to −78.483%), and the trend change was −49.635 RMB/month (P < 0.001), displaying a more evident daily drug cost decrease compared to internal medicine patients. The relative cumulative effect of male patients at the study cutoff point was −84.893% (95% CI: −90.454% to −78.020%), and the trend change amount was −25.319 RMB/month (P < 0.001).
Compared with patients aged 60–69 years and 70–79 years, among patients aged 80 years and above, DIP policy intervention showed no significant impact on the trend change of patient monthly average daily drug costs (−8.935 RMB/month, P = 0.098) (Figure 2, Table 3).
Discussion
As far as we know, this study is the first to utilize the real-world medication data of sample hospitals, rather than survey data or public drug procurement data, and quantitatively analyzed the drug costs and medication structure of hypertensive inpatients before and after DIP policy intervention.
Our results indicated that DIP policy intervention can improve the drug burden of elderly hypertensive inpatients. The research conclusion is basically consistent with the previous qualitative research,5 which involves all disease types. Our study further found that during the period from 2016 to 2020, the implementation of DIP policy reduced the drug burden of elderly hypertensive inpatients by 78.860%, and its intervention effect was particularly significant among the elderly aged 60–69 and 70–79. With the continuous promotion of DIP policy,4 it can be predicted that shortly, China’s DIP policy will benefit a wider range of patients.
ITS design is considered to be the best quasi-experimental design to evaluate the vertical effect of policy intervention.22 Compared with randomized controlled trials (RCT), ITS analysis has broad population qualification and optimizes the external validity of the study.23 DIP policy is a payment mode based on the basic theory of diagnosis-related groups (DRGs),3 distinguishing the combination of disease types according to the disease classification logic of DRGs and formulating corresponding scores, and settles accounts according to the score. The disease combination of DIP is formed by exhausting the random combination of “disease diagnosis” and “treatment method” in real-world medical records, and the payment standard of each combination is determined, and then implemented by the hospital. The published research shows that since the implementation of the DIP policy in Guangzhou, the total health expenditure has decreased by 3.5%.5
Our study further found that for elderly hypertensive inpatients, the intervention effect on surgical patients was more significant, and the average daily drug cost decreased by 87.626%. In our study, among all the surgical departments, neurosurgery and cardiothoracic surgery were selected where the majority of hypertension population are received, because the two complications, stroke and cardiovascular disease, may be treated there.24,25 Generally, surgery is dominated by surgical treatment, while each disease in the DIP has a fixed score, and the drug costs have been converted into department medical costs.3,5 To obtain better benefits, surgeons are more motivated to reduce using non-essential drugs, thereby reducing drug expenditure.
In addition, the intervention effect on patients of different genders is not consistent, especially for male patients, whose drug cost decreased by 84.893% after intervention, which may be related to the difference in the comorbidity of hypertensive patients of different genders.26 Some studies have shown that male patients have a higher risk of developing diabetes,27 CCDs than female patients,28 and male patients are more likely to be accompanied by smoking, drinking and obesity,29 which leads to an increased number of comorbidities, and further give rise to drug costs.30 Therefore, before intervention, male patients may afford high drug costs and see large invention space. On the other hand, excessive reduction of drug costs may also cause insufficient treatment. Therefore, the difference in comorbidity patterns resulted from different patient characteristics should be taken into account in the control of drug costs for elderly hypertensive inpatients by DIP policy, and corresponding and targeted measures should be executed.
DIP policy will also cause changes in the drug structure of elderly hypertensive patients. The meaning of drug structure is the types of drugs used by patients during hospitalization. Our study shows that after the policy intervention, the uses of anti-infective drugs, anti-tumor drugs, and biological products all showed a significant downward trend, which may also be related to the “4+7” volume-based drug procurement (“4+7” policy) and National Reimbursement Drug List Negotiation (NRDLN) by the Chinese government.31,32 These two superimposed policies involve multiple anti-infective drugs and anti-tumor drugs. However, the price of “4+7” policy drugs and NRDLN drugs generally declined significantly, which may lead to superimposed effects on the results of this study.33 Moreover, it is worth noting that after DIP policy intervention, the proportion of nutritional medication showed a significant upward trend, and the clinic should be alert to the risk of such irrational medication.
Finally, this study has several limitations. Firstly, this study is only conducted in Guangzhou, which may not represent the overall situation in China. However, as a practical case, this study serves to illustrate that the rapid growth of drug costs can be effectively controlled in China. Secondly, the confusion of other policy interventions may lead to deviation in ITS analysis. For example, the “4+7” policy and NRDLN policy.32,33 Therefore, this study may overestimate the impact of DIP policy. In addition, for individual patients, we must further consider the consistency between diagnosis and treatment, between comorbidity states and treatment. The COVID-19 pandemic may also affect on medical expenditures and medical structure. Lastly, this study focused on the macro-policy level, and did not conduct follow-up studies on individual patients based on the consideration of data size and data accessibility. In the future, it is necessary to collect relevant data to study the change of drug burden from the individual patient level.
Conclusions
In this study, 34,276 daily full medical orders of elderly hypertensive patients from 9 medical institutions in Guangzhou from 2016 to 2020 were used to make ITS study, and to prove that DIP policy intervention can improve the drug burden of elderly hypertensive inpatients. The effect is higher on surgical inpatients than internal medical inpatients, higher on male patients than female patients. In addition, the implementation of the DIP policy intervention has also led to changes in the medication structure of patients. In the future, the Chinese government should continue to play a leading role, and pay attention to the impact of DIP policy on different characteristic patients and different departments of the hospital, so as to optimize medication structure and achieve reasonable control of drug costs.
Data Sharing Statement
The study was previously preregistered on the WHO International Clinical Trials Registry Platform (www.chictr.org, the registered number is ChiCTR2200066973), and Summary data used in this study are available from the corresponding author, upon reasonable request.
Ethics Approval and Informed Consent
This study has been approved by the Ethics Committee of the First Affiliated Hospital of Zhejiang University School of Medicine: Expedition review No. 342 in 2022. This study applied retrospective data for evaluation, without involving personal privacy or commercial interests, and has been exempted by the ethics committee to obtain informed consent from patients.
Acknowledgment
This research is supported by the Zhejiang Provincial Natural Science Foundation, China (NO. LYY21H310003), Pharmacoeconomics and Health Technology Evaluation of Zhejiang Pharmaceutical Society (NO. 2022ZYJ11), the Medical and Health Research Project of Zhejiang province (NO. 2021RC055), Funding of Zhejiang Pharmaceutical Association (NO. 2019ZYY13) and Hospital Pharmacy Innovation Project for the youth established by Chinese Pharmaceutical Association and Servier (Tianjin) Pharmaceutical Co., Ltd. NO. CPA-B04-ZC-2022-001.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revised or critically reviewed the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No external financial support was received for this study.
Disclosure
The authors declare no potential financial and non-financial competing interests in this work.
References
1. Jia H, Jiang H, Yu J, Zhang J, Cao P, Yu X. Total health expenditure and its driving factors in china: a gray theory analysis. Healthcare. 2021;9(2). doi:10.3390/healthcare9020207
2. Yip W, Fu H, Chen AT, et al. 10 years of health-care reform in China: progress and gaps in Universal Health Coverage. Lancet. 2019;394(10204):1192–1204. doi:10.1016/s0140-6736(19)32136-1
3. Xie H, Cui X, Ying X, Hu X, Xuan J, Xu S. Development of a novel hospital payment system – big data diagnosis & intervention Packet. Health Policy OPEN. 2022;3:100066. doi:10.1016/j.hpopen.2022.100066
4. He AJ. Scaling-up through piloting: dual-track provider payment reforms in China’s health system. Health Policy Plan. 2022. doi:10.1093/heapol/czac080
5. Lai Y, Fu H, Li L, Yip W. Hospital response to a case-based payment scheme under regional global budget: the case of Guangzhou in China. Soc Sci Med. 2022;292:114601. doi:10.1016/j.socscimed.2021.114601
6. Chen YJ, Zhang XY, Tang X, Yan JQ, Qian MC, Ying XH. How do inpatients’ costs, length of stay, and quality of care vary across age groups after a new case-based payment reform in China? An interrupted time series analysis. BMC Health Serv Res. 2023;23(1):160. doi:10.1186/s12913-023-09109-z
7. Dong Z. Current epidemiology of adult hypertension in China. Chin J Cardiovasc Med. 2020;25(06):513–515.
8. Fang EF, Xie C, Schenkel JA, et al. A research agenda for ageing in China in the 21st century (2nd edition): focusing on basic and translational research, long-term care, policy and social networks. Ageing Res Rev. 2020;64:101174. doi:10.1016/j.arr.2020.101174
9. Trastek VF, Hamilton NW, Niles EE. Leadership models in health care - A case for servant leadership. Mayo Clin Proc. 2014;89(3):374–381. doi:10.1016/j.mayocp.2013.10.012
10. Wagner AK, Soumerai SB, Zhang F, Ross-Degnan D. Segmented regression analysis of interrupted time series studies in medication use research. J Clin Pharm Ther. 2002;27(4):299–309. doi:10.1046/j.1365-2710.2002.00430.x
11. Des Jarlais DC, Lyles C, Crepaz N, Group T. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: the TREND statement. Am J Public Health. 2004;94(3):361–366. doi:10.2105/ajph.94.3.361
12. Hoffmann TC, Glasziou PP, Boutron I, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. Br Med J. 2014;348:g1687. doi:10.1136/bmj.g1687
13. Pang YY, Ma CL. Real-world pharmacological treatment patterns of patients with threatened miscarriage in China from 2014 to 2020: a cross-sectional analysis. J Clin Pharm Ther. 2022;47(2):228–236. doi:10.1111/jcpt.13536
14. Yu L, Feng J, Yu Z, Dai H. Trends of anti-seizure medication use in pediatric patients in six cities in China from 2013 to 2018. Epilepsy Res. 2020;167:106448. doi:10.1016/j.eplepsyres.2020.106448
15. Yu P, Wang J, Hu J, et al. The standard for healthy Chinese older adults (2022). Aging Med. 2022;5(4):244–245. doi:10.1002/agm2.12233
16. Su X, Hua X, Xin C, et al. Principle And Method Of The Big Data Diagnosis-Intervention Packet (DIP) Payment System. China Health Insurance. 2020:23–28. doi:10.19546/j.issn.1674-3830.2020.9.007
17. Savin NE, White KJ. The Durbin-Watson test for serial correlation with extreme sample sizes or many regressors. Econometrica: Journal of the Econometric Society. 1977;45(8):1989–1996. doi:10.2307/1914122
18. Turner SL, Forbes AB, Karahalios A, Taljaard M, McKenzie JE. Evaluation of statistical methods used in the analysis of interrupted time series studies: a simulation study. BMC Med Res Methodol. 2021;21(1):181. doi:10.1186/s12874-021-01364-0
19. Zhang F, Wagner AK, Soumerai SB, Ross-Degnan D. Methods for estimating confidence intervals in interrupted time series analyses of health interventions. J Clin Epidemiol. 2009;62(2):143–148. doi:10.1016/j.jclinepi.2008.08.007
20. Johnston MG, Faulkner C. A bootstrap approach is a superior statistical method for the comparison of non-normal data with differing variances. New Phytol. 2021;230(1):23–26. doi:10.1111/nph.17159
21. Durbin J, Watson GS. Testing for serial correlation in least squares regression. II. Biometrika. 1951;38(1–2):159–178. doi:10.1093/biomet/38.1-2.159
22. Bernal JL, Cummins S, Gasparrini A. Interrupted time series regression for the evaluation of public health interventions: a tutorial. Int J Epidemiol. 2017;46(1):348–355. doi:10.1093/ije/dyw098
23. Kontopantelis E, Doran T, Springate DA, Buchan I, Reeves D. Regression based quasi-experimental approach when randomisation is not an option: interrupted time series analysis. BMJ. 2015;350:h2750. doi:10.1136/bmj.h2750
24. Fuchs FD, Whelton PK. High Blood Pressure and Cardiovascular Disease. Hypertension. 2020;75(2):285–292. doi:10.1161/hypertensionaha.119.14240
25. Pierdomenico SD, Pierdomenico AM, Cuccurullo F. Morning blood pressure surge, dipping, and risk of ischemic stroke in elderly patients treated for hypertension. Am J Hypertens. 2014;27(4):564–570. doi:10.1093/ajh/hpt170
26. Ramirez LA, Sullivan JC. Sex differences in hypertension: where we have been and where we are going. Am J Hypertens. 2018;31(12):1247–1254. doi:10.1093/ajh/hpy148
27. Miranda JJ, Carrillo-Larco RM, Ferreccio C, et al. Trends in cardiometabolic risk factors in the Americas between 1980 and 2014: a pooled analysis of population-based surveys. The Lancet Global Health. 2020;8(1):e123–e133. doi:10.1016/S2214-109X(19)30484-X
28. J-w L, Shin S-J, Kim J, Kang H-T. Higher pulse pressure is associated with increased risk of cardio-cerebrovascular disease and all-cause mortality: a Korean national cohort study. Am J Hypertens. 2022;35(7):647–655. doi:10.1093/ajh/hpac043
29. Stringhini S, Carmeli C, Jokela M, et al. Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: a multicohort study and meta-analysis of 1·7 million men and women. Lancet. 2017;389(10075):1229–1237. doi:10.1016/S0140-6736(16)32380-7
30. Jamal A, Phillips E, Gentzke AS, et al. Current Cigarette Smoking Among Adults - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67(2):53–59. doi:10.15585/mmwr.mm6702a1
31. Lu J, Long H, Shen Y, et al. The change of drug utilization in China’s public healthcare institutions under the “4 + 7” centralized drug procurement policy: evidence from a natural experiment in China. Front Pharmacol. 2022;13:923209. doi:10.3389/fphar.2022.923209
32. Tang M, Song P, He J. Progress on drug pricing negotiations in China. Biosci Trends. 2019;13(6):464–468. doi:10.5582/bst.2019.01339
33. Yang Y, Tong R, Yin S, et al. The impact of “4 + 7” volume-based drug procurement on the volume, expenditures, and daily costs of antihypertensive drugs in Shenzhen, China: an interrupted time series analysis. BMC Health Serv Res. 2021;21(1):1275. doi:10.1186/s12913-021-07143-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.