")
Back to Journals » Journal of Inflammation Research » Volume 16
The Independent Value of Neutrophil to Lymphocyte Ratio in Gouty Arthritis: A Narrative Review
Authors Chen Y , Liu J , Li Y , Cong C, Hu Y , Zhang X, Han Q
Received 16 July 2023
Accepted for publication 9 October 2023
Published 16 October 2023 Volume 2023:16 Pages 4593—4601
DOI https://doi.org/10.2147/JIR.S430831
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monika Sharma
Yiming Chen,1,2 Jian Liu,1– 3 Yang Li,1 Chengzhi Cong,1 Yuedi Hu,1 Xianheng Zhang,1 Qi Han1
1Department of Rheumatology, the First Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, Anhui Province, People’s Republic of China; 2Anhui Key Laboratory of Application and Development of Internal medicine of Modern Chinese Medicine, Anhui University of Chinese Medicine, Hefei, Anhui Province, People’s Republic of China; 3National Traditional Chinese Medicine Inheritance and Innovation Center, Hefei, Anhui Province, People’s Republic of China
Correspondence: Jian Liu, Department of Rheumatology, the First Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, Anhui Province, People’s Republic of China, Tel +86 13955109537, Email [email protected]
Abstract: Since the incidence of gouty arthritis (GA) exhibits yearly increases, accurate assessment and early treatment have significant values for improving disease conditions and monitoring prognosis. Neutrophil to lymphocyte ratio (NLR) is a common indicator in blood routine, which has the characteristics of easy access and low cost. In recent years, NLR has been proven to be an effective indicator for guiding the diagnosis, treatment, and prognosis of various diseases. Moreover, NLR has varying degrees of relationship with various inflammatory biomarkers, which can affect and reflect the inflammatory response in the body. This paper reviews the independent value of NLR for GA and its underlying molecular pathological mechanisms, intending to contribute to the further application of NLR.
Keywords: neutrophil to lymphocyte ratio, gouty arthritis, inflammatory response, neutrophils, disease activity
Introduction
Gouty arthritis (GA) is one of the most common forms of inflammatory arthritis, bringing huge economic and social burdens.1,2 According to the study data of the Global Burden of Disease, there are 41.2 million GA patients worldwide as of 2017.3 The estimated global age-standardized incidence rate and annual incidence rate of GA are 510.6 and 91.8 per 100,000 people, respectively, which increases by 7.2% and 5.5% compared with 1990.4,5 These changes are more pronounced in economically developed countries or regions.6
The gold standard for GA diagnosis is the presence of birefringent urate crystal in synovial fluid under a polarization microscope.1 However, patients show low acceptance due to the invasive nature of this procedure. Currently, the examination methods for GA include X-ray, ultrasound, computed tomography, magnetic resonance imaging, etc. However, these imaging techniques are complex, restrictive, and expensive.7,8 The indicators reflecting the inflammatory activity of GA include C-reactive protein, erythrocyte sedimentation rate and IL-1β, etc.9 However, the sensitivity and specificity of these indicators are not excellent.10 There are many comorbidities in patients with GA, which are the main causes of death in patients with GA.11 At present, the method to accurately predict the risk and prognosis of GA comorbidities has not been found. Therefore, it is urgent to find a simpler, cheaper, and less restrictive assessment method for GA while ensuring its effectiveness.
During the GA process, there exists a persistent immune inflammatory response mediated by inflammatory biomarkers such as immune cells, inflammatory mediators, and chemokines.12 Emerging evidence has indicated that biomarkers can be used as characteristic indicators to evaluate the activity and prognosis of GA, facilitating the optimization of treatment plans.9,13–15 Neutrophil to lymphocyte ratio (NLR) is a composite biomarker obtained by dividing the neutrophil count by the lymphocyte count in blood routine, which is the most common test in clinical practice.16,17 In recent years, NLR has been found to predict the activity and prognosis of rheumatic diseases (including GA).17–21 This review summarizes existing evidence on the relationship between NLR and GA, evaluates whether NLR can guide clinical measures, explores the potential pathophysiological mechanisms of NLR, and thereby provides a foundation for future research.
Overview of NLR
NLR is a parameter in blood routine testing, which is easy to obtain, cost-effective, rapid to test, and integrates two different but complementary immune pathways. As a composite biomarker, NLR is more capable of reflecting systemic inflammation than individual biomarkers, and its potential role in clinical practice is supported by its ability to predict the occurrence and development of various diseases.22,23
The NLR value of healthy adults ranges from 0.78 to 3.53, with an average of 1.65.24 Elevated NLR often indicates that the disease is in a high-risk stage of progression, leading to ineffective treatment and poor prognosis.25 NLR is also positively correlated with a variety of hematology parameters, such as erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), mean platelet volume (MPV), and platelet distribution width (PDW).26,27
Keisuke Toya et al believed that NLR could independently predict the healing time of pancreatic fistula after distal pancreatectomy, indicating that elevating NLR may shorten the healing time after surgery.28 Cheng et al suggested that a higher NLR was significantly associated with an increased risk of depression, and the increase in NLR was more pronounced among depression patients with suicidal behavior.16 Dowlati et al pointed out that in cerebral vasospasm after aneurysmal subarachnoid hemorrhage, Hunt-Hess score > 2, NLR > 8.0, and early fevers were predictive of the need for multiple endovascular interventions, and these patients had poorer functional outcomes and higher rates of complications.29 Li et al demonstrated that NLR could predict the mortality rate of patients with cerebral hemorrhage, showing positive significance in observing disease conditions and guiding clinical treatment.30 All the above findings indicate that NLR can be used for early diagnosis and prognosis monitoring of various benign and malignant tumors, cardiovascular diseases, infectious diseases, and immune system diseases.
However, some researchers hold that the clinical value of NLR does not have a significant advantage. A study on prosthetic joint infections showed that the diagnostic specificity and sensitivity of NLR were not superior to those of ESR and CRP.31 Mukadder Korkmaz et al believed that NLR seemed to be unrelated to the degree of upper respiratory obstruction and therefore could not be used to evaluate the systemic inflammatory status of obstructive sleep apnea syndrome.32
To sum up, NLR is of positive significance in diagnosing diseases and judging activity, but large-sample randomized controlled trials are warranted to clarify the clinical value of NLR for some diseases (such as GA).
NLR is Related to GA Activity
The role of NLR in GA diagnosis, activity evaluation, and prognosis has been extensively studied. The early increase in NLR after acute inflammation may be the reason why NLR is more sensitive than other laboratory indicators. A study33 assigned 106 gout patients who met the diagnostic criteria of the American College of Rheumatology (ACR) to Group I (active phase) and Group II (intermittent phase), with 148 age and gender-matched healthy individuals as the control group. Statistical analysis showed that there was a significant difference in NLR levels between Group I and Group II (2.88 vs 2.19, P < 0.001), proving that NLR can serve as an inflammatory marker to indicate the activity of certain systemic diseases. The NLR levels in Group II were also higher than those in the healthy control group (P < 0.001). Therefore, NLR may function as an effective marker of disease activity in GA patients.
Similarly, Kadiyeran et al21 included 110 GA patients and 90 healthy volunteers as controls and collected blood samples within 24 to 48 hours of GA onset according to ACR 2012 standards. Their results showed that the NLR (P < 0.001), platelet to lymphocyte ratio (PLR), monocyte to lymphocyte ratio (MLR), MPV (P < 0.05), ESR (P < 0.001), and CRP (P < 0.001) of GA patients in the onset period were higher than those in the intermittent period and the control group. In the correlation analysis during the onset period, the authors found a positive correlation between serum uric acid (SUA) (P < 0.001), CRP (P < 0.001) and NLR. Linear stepwise regression analysis showed that there was an independent strongly correlated material between GA attacks and NLR (P = 0.014), SUA (P < 0.001), ESR (P < 0.001), CRP (P < 0.001), MLR (P < 0.001). Therefore, NLR can serve as an independent predictor of GA onset, which is more effective than NE count in reflecting systemic inflammatory status. NLR is also associated with test indicators including SUA, ESR, CRP, PLR, and MLR in GA, which contributes to judging the disease condition of GA. The results of AŞahin were also consistent with this study.34
Another monocentric and retrospective study35 also supports this viewpoint, but there are differences. Compared with healthy controls, gout patients showed a significant increase in NLR and PLR (P < 0.001), but a significant decrease in MPV (P < 0.001). The authors found that NLR was positively correlated with inflammatory factors such as ESR (R = 0.253, P = 0.006) and CRP (R = 0.367, P < 0.001), but the intensity of all correlations was weak (all R < 0.5). Therefore, the authors believed that NLR was not an independent predictor of GA activity and needed to be used together with other hematology parameters. At last, the authors drew the receiver operating characteristic (ROC) curve of NLR in predicting gout attacks. The area under the curve (AUC) was 0.765. When the cut-off value of NLR was 3.810, the sensitivity was 57.9% and the specificity was 78.3%. Thus, it could be seen that NLR had low sensitivity and specificity in predicting GA attacks and was not a reliable predictive indicator.
The above studies are presented in Table 1. The reliability of NLR as an inflammatory marker to judge the activity of GA has been recognized, but there is still a lack of multi-center large-sample observational studies to further verify it. The sensitivity and specificity of NLR with different cut-off values in predicting GA attack, as well as the correlation strength between NLR and inflammatory markers such as ESR and CRP, still need to be observed.
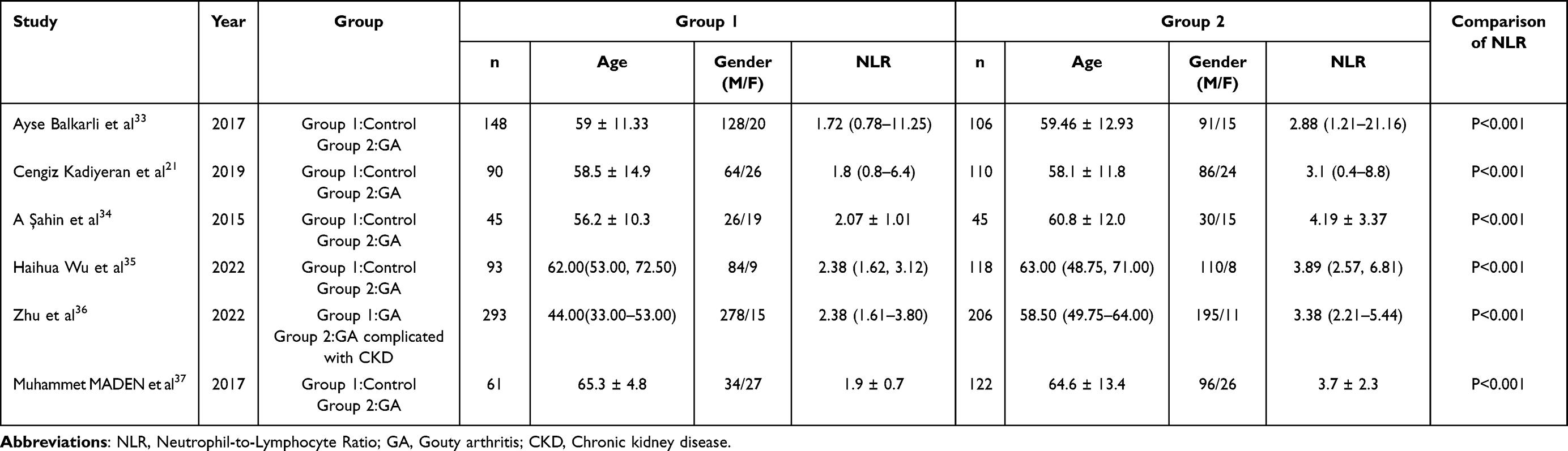 |
Table 1 Summary of the Studies of GA Mentioned in This Review |
NLR and GA Comorbidities
The common complications of GA include cardiovascular diseases,38,39 diabetes,40 renal function impairment,41 sexual dysfunction,42 and ophthalmic diseases.43 Recent studies have found that NLR may be able to predict the risk and outcome of GA comorbidities.
A retrospective study on the relationship between NLR and renal function impairment in GA patients by Zhu et al36 included 499 GA patients and divided them into the chronic kidney disease (CKD) group and the non-CKD group. Statistical results showed that the NLR of the CKD group was significantly higher than that of the non-CKD group (P < 0.001). Multivariable logistic regression analysis indicated that NLR was associated with an increased risk of renal dysfunction in GA patients (OR = 1.122, 95% CI: 1.036–1.215). ROC curve analysis showed that the AUC of NLR for predicting CKD in GA patients was 0.646 (95% CI: 0.597–0.694), with a sensitivity of 60.19% and a specificity of 60.41%. Consistently, we also assume that elevated NLR may be associated with enhanced inflammation and reduced estimated glomerular filtration rate, both of which increase the risk of renal function impairment in GA patients. NLR can serve as an effective biomarker for predicting renal function impairment in GA patients and also evaluate the degree of inflammatory response in CKD patients at different stages, representing an independent predictor of advanced CKD progression.
In 2017, a cohort study37 included 122 GA patients and 61 healthy controls. The survival period, history of atherosclerosis, NLR and MPV were recorded during an average follow-up period of 105 months. The researchers only observed that the NLR of GA patients was higher than the healthy controls, but there was no sufficient evidence that NLR can independently predict the outcomes of GA patients complicated with atherosclerosis. In contrast, multivariate analysis suggested the only independent adverse prognostic factor was the initial MPV value.
The above studies are also presented in Table 1. In summary, monitoring the NLR of GA patients is necessary, which may help identify the risk of comorbidities in GA.36,37 However, further research is needed to confirm these findings and determine the optimal cutoff value for NLR to predict the risk and outcome of comorbidities in GA patients.
NLR Elevation is Characterized by an Increase in NEs
NE and Lym are key cellular components of the human defense system.44,45 NE is involved in innate immunity and mediates inflammatory reactions through chemotaxis, phagocytosis, and cytokine release.46 Lym mainly represents specific immune system regulatory pathways.47 The composite marker NLR that combines the two can reflect the dynamics and balance of innate and specific immunity in immune function.48
Inflammation of GA is mainly mediated by NE and macrophage.6 Lym primarily participates in chronic inflammatory responses, and no conclusive evidence has been found that Lym such as innate lymphoid cells and natural killer T cells are involved in acute inflammation of GA, which may be related to the rapid onset of GA and the intense inflammatory response. Another view is that when inflammation occurs in an acute manner, a large amount of Lyms in the peripheral blood will quickly migrate to the damaged tissues, resulting in a decrease in the number of Lyms in the blood.49
The increase in NE count alone leading to an increase in NLR is mainly seen in the following situations:48 bacterial infection, stroke, myocardial infarction, trauma, cancer, and any disease characterized by inflammatory responses, as the early stages of inflammation are characterized by a pro-inflammatory state, while NE mainly mediates this process.50 As an important participant in innate immunity, massive NEs recruits, activates, and encodes other immune cells, as well as secrets a series of pro-inflammatory factors, immune regulatory factors, and chemokines, enhancing the recruitment and function of immune cells.46 Therefore, an increase in NLR is typically characterized by an increase in NEs.
NLR and GA Inflammatory Mechanisms
Classical Mechanisms
The NLRP3 inflammasome-caspase-1-IL-1β signaling produced by NE is currently recognized as the classical mechanism of GA inflammatory responses.51–54 During the acute onset of GA, monosodium urate (MSU) crystals induce massive infiltration of immune cells such as NEs to the local response site and activate NLRP3. Then, the activated NLRP3 produces caspase-1 and promotes the secretion of IL-1β. IL-1β activates the release of pro-inflammatory cytokines and chemokines, which further exacerbates the chemotaxis and infiltration of NE, forming a rapid and intense inflammatory cascade reaction.55
NE and Protein-MSU Complexes
MSU can bind to various serum proteins to form protein-MSU complexes, such as the C1q, C5, and C6 part of complements, Fc fragments of IgG and IgM, and apolipoprotein.56–58 The physical and chemical properties of the complex will not change, but the spatial structure will change into a form more conducive to the recognition of NE and phagocytosis of macrophage.59
IgG and apolipoprotein can occupy the surface of MSU crystals and mediate the process of NE stimulation during the inflammatory activity and regression phases.60 Xu et al59 discovered an intriguing relationship between type II collagen-MSU complex (CII-MSU) and NE. CII-MSU enhanced the secretion of CC chemokine ligand 2 and C-X-C chemokine ligand 2, thereby promoting the ability of NE to recruit to inflammatory sites in migration experiments. The number of NEs in the synovium of mice injected with CII-MSU was significantly higher than that of mice injected with MSU. CII-MSU mainly mediated the TLRs/MyD88/NF-κΒ pathway in an ITGB1-dependent manner, thereby promoting the recruitment and activation of NE.
In brief, different protein-MSU complexes may affect the inflammatory effect of NE through different pathways to mediate the inflammatory response of GA.61 Understanding the formation process and inflammatory regulation ability of different protein-MSU complexes may help elucidate the novel relationship between GA and NE.
NE and Intestinal Microbiota in GA Patients
At least 100 trillion bacteria live in the human intestinal micro-ecosystem and participate in the metabolism, immune regulation, and internal environment homeostasis.62–64 The intestine is an important organ for the excretion of uric acid outside the kidneys, with two-thirds of uric acid being excreted from the kidneys and one-third being excreted through the intestine.65 The intestinal excretion of uric acid is mainly achieved through the catabolism of uric acid transporters and intestinal microbiota. Accumulating studies have revealed the relationship between intestinal microbiota and GA.66–68
Dipti Karmarkar1 and Kenneth L. Rock69 found that intestinal microbiota regulated the recruitment of NE stimulated by MSU through the myeloid differentiation factor MyD88-dependent pathway. Jonas Schluter et al70 revealed that there was a correlation between intestinal bacteria and immune cell dynamics, that is, metabolites of intestinal microbiota changed the permeability of the intestinal barrier and promote NE to enter the blood. A similar study71 indicated that short-chain fatty acid (SCFA) produced by intestinal microbiota metabolism, such as acetate, propionate, and butyrate, could promote related immune responses. Acetate could induce caspase-dependent apoptosis of NE, leading to inflammation regression.72 Sodium butyrate reduced the UA levels in mice, reversed the reduction of MUC2, ZO-1, Occludin, and ABCG2 proteins in intestinal tissues, and decreased the levels of inflammatory factors73.
These studies indicate that the intestinal microbiota plays a vital role in GA inflammation caused by NE activation. Recovery and improvement of intestinal microbiota and its metabolites may be a new method for the treatment of GA, but the current limitation is that the flora is significantly different among individuals. With the development of intestinal microbiota-related detection technologies, we can determine the number and types of intestinal microbiota in patients with GA, which may provide novel insights into the treatment of GA.
Neutrophil Extracellular Traps (NETs) and GA Inflammation
As one of the most prominent research highlights in the inflammation mechanism of GA in recent years, NETs are extracellular net-like structures decorated with histones and antimicrobial proteins released by activated NE. Estrella Garcia-Gonzalez et al74 found that microcrystalline particles such as MSU can promote the generation of NETs, and the amount generated is not related to NE, but positively correlated with the number of microcrystals. One of the functions of NETs is to capture MSU in the blood, thereby blocking the onset of GA. However, the large accumulation of NETs and their encapsulation of MSU may also be the cause of gouty tophi.
Maximilien Euler and Markus H. Hoffmann75 reported two opposite effects of NETs in GA. The net-like structure of NETs can capture and degrade pro-inflammatory factors due to the presence of NE serine protease (NSPs) on the DNA backbone of NETs, and the combination of NETs and NSPs hydrolyzes and destroys the protein structure of pro-inflammatory factors, thus promoting the regression of inflammation. However, the DNA and proteins on NETs are the sources of autoantigens in a disordered immune system. The binding of antigens and antibodies forms immune complexes and in turn induces the production of NETs, forming inflammatory self-amplification.
Olga Tatsiy et al76 delved deeper into the signaling pathways of NETs and found that MAPK and Akt in NE were activated by MSU under the control of TAK1 and Syk, which then participated in the production of cytokines and the formation of NETs in GA inflammatory responses. Similarly, Tang et al77 found that the NFIL3/REDD1/mTOR signaling pathway was a key pathway leading to NE autophagy, NET formation, and gouty inflammation.
In short, NETs activate and eliminate GA inflammation at different levels, constituting an important component of inflammation regulation. The focus of future research on NETs should be on how NEs transforms into NETs at the physiological level and maintains a quantitative balance of NETs. Moreover, the quantitative detection of NETs by Western blotting and ELISA is not yet complete, and a quantitative detection method for NETs needs to be explored.
Summary and Prospect
In summary, NLR is a simple and low-cost biomarker for systemic inflammation. NLR is reliable in determining GA activity and predicting GA comorbidities and prognosis. However, some scholars believe that NLR can only serve as a clinical reference factor and does not have exact significance.
In clinical practice, GA is usually diagnosed based on clinical symptoms and serum uric acid levels, and the onset of GA can be effectively suppressed by a short course of non-steroidal anti-inflammatory drugs.1 Therefore, it is of no great significance to use NLR to diagnose or predict the onset of GA. However, inflammation remains the most crucial pathological mechanism underlying GA.6 Following physical examination and history collection, an objective test index is still required to evaluate the inflammatory activity of GA. The aforementioned multiple observational studies have consistently demonstrated the reliable ability of NLR to evaluate inflammatory activity in GA.21,33–35 Similarly, comorbidities are major contributors to mortality in patients with GA, and NLR has a better significance in predicting GA comorbidities, especially cardiovascular and cerebrovascular diseases and endocrine diseases.37,40
We need to conduct more large-sample randomized control trials or cohort studies to clarify the clinical value of NLR. It is also necessary to elucidate the molecular mechanism of the relationship between NLR and related biomarkers and signaling pathways. We still have doubts about NLR as the following questions have not been answered:
- Is the normal range of NLR the same in different races? What do different NLR outliers represent?
- What biomarkers should NLR be used with to improve predictive ability?
- Can prediction ability be improved by measuring the ratio of neutrophils of a specific subtype to lymphocytes of a specific subtype?
Addressing the above issues remains a huge challenge, but exploring these issues may advance our understanding of the inflammatory mechanisms and thereby help us evaluate the immune inflammatory response status of the body, predict the activity and various complications of GA, identify different targets and signaling pathways for treating GA, and determine potential specific treatment strategies.
Acknowledgments
This work was supported by grants from Anhui Key Laboratory of Application and Development of Internal medicine of Modern Chinese medicine (2016080503B041), High-level key discipline of Traditional Chinese Medicine by the State Administration of Traditional Chinese Medicine (Teaching Letter of Traditional Chinese Medicine [2023] NO.85), Anhui Province Traditional Chinese Medicine Leading Talent Project (Traditional Chinese Medicine Development Secret [2018] No. 23).
Disclosure
The authors declare that they have no conflicts of interest regarding the publication of this paper.
References
1. Dalbeth N, Gosling AL, Gaffo A, et al. Gout. Lancet. 2021;397(10287):1843–1855. doi:10.1016/S0140-6736(21)00569-9
2. Murdoch R, Barry MJ, Choi HK, et al. Gout, Hyperuricaemia and Crystal-Associated Disease Network (G-CAN) common language definition of gout. RMD Open. 2021;7(2):e1623. doi:10.1136/rmdopen-2021-001623
3. James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–1858.
4. Safiri S, Kolahi AA, Cross M, et al. Prevalence, incidence, and years lived with disability due to gout and its attributable risk factors for 195 countries and territories 1990–2017: a systematic analysis of the Global Burden of Disease Study 2017. Arthritis Rheumatol. 2020;72(11):1916–1927. doi:10.1002/art.41404
5. Xia Y, Wu Q, Wang H, et al. Global, regional and national burden of gout, 1990–2017: a systematic analysis of the Global Burden of Disease Study. Rheumatology. 2020;59(7):1529–1538. doi:10.1093/rheumatology/kez476
6. Ragab G, Elshahaly M, Bardin T. Gout: an old disease in new perspective – a review. J Adv Res. 2017;8(5):495–511. doi:10.1016/j.jare.2017.04.008
7. Zhang B, Yang M, Wang H. Diagnostic value of ultrasound versus dual-energy computed tomography in patients with different stages of acute gouty arthritis. Clin Rheumatol. 2020;39(5):1649–1653. doi:10.1007/s10067-020-05014-6
8. Sudol-Szopinska I, Afonso PD, Jacobson JA, et al. Imaging of gout: findings and pitfalls. A pictorial review. Acta Reumatol Port. 2020;45(1):20–25.
9. Franco Trepat E, Alonso Pérez A, Guillán Fresco M, et al. Amitriptyline blocks innate immune responses mediated by toll‐like receptor 4 and IL‐1 receptor: preclinical and clinical evidence in osteoarthritis and gout. Br J Pharmacol. 2022;179(2):270–286. doi:10.1111/bph.15707
10. Lenski M, Scherer MA. Analysis of synovial inflammatory markers to differ infectious from gouty arthritis. Clin Biochem. 2014;47(1–2):49–55. doi:10.1016/j.clinbiochem.2013.10.019
11. Singh JA, Gaffo A. Gout epidemiology and comorbidities. Semin Arthritis Rheum. 2020;50(3):S11–S16. doi:10.1016/j.semarthrit.2020.04.008
12. Zhang X, Liu J, Sun Y, et al. Chinese herbal compound Huangqin Qingrechubi capsule reduces lipid metabolism disorder and inflammatory response in gouty arthritis via the LncRNA H19/APN/PI3K/AKT cascade. Pharm Biol. 2023;61(1):541–555. doi:10.1080/13880209.2023.2191641
13. Wang Z, Zhao Y, Phipps Green A, et al. Differential DNA methylation of networked signaling, transcriptional, innate and adaptive immunity, and osteoclastogenesis genes and pathways in gout. Arthritis Rheumatol. 2020;72(5):802–814. doi:10.1002/art.41173
14. Song S, Lou Y, Mao Y, et al. Alteration of gut microbiome and correlated amino acid metabolism contribute to hyperuricemia and Th17-driven inflammation in Uox-KO mice. Front Immunol. 2022;13:804306.
15. Klück V, Liu R, Joosten LAB. The role of interleukin-1 family members in hyperuricemia and gout. Joint Bone Spine. 2021;88(2):105092. doi:10.1016/j.jbspin.2020.105092
16. Cheng Y, Wang Y, Wang X, et al. Neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and monocyte-to-lymphocyte ratio in depression: an updated systematic review and meta-analysis. Front Psychiatry. 2022;13:893097. doi:10.3389/fpsyt.2022.893097
17. Kim A, Kim Y, Kim G, et al. Platelet-to-lymphocyte ratio and neutrophil-to-lymphocyte ratio as potential makers for digital ulcers and interstitial lung disease in patients with systemic sclerosis: cross-sectional analysis of data from a prospective cohort study. Rheumatol Int. 2020;40(7):1071–1079. doi:10.1007/s00296-020-04604-6
18. Enginar AU, Kacar C. Neutrophil-lymphocyte and platelet-lymphocyte rate and their seasonal differences in ankylosing spondylitis and rheumatoid arthritis patients using anti-TNF medication. Bratislava Med J. 2019;120(08):586–592. doi:10.4149/BLL_2019_096
19. Daghor Abbaci K, Ait Hamadouche N, Otmani F, et al. Validation of the neutrophil-to-lymphocyte ratio as a new simple biomarker of adult onset Still’s disease: a STROBE-Compliant prospective observational study. Medicine. 2022;101(32):e29970. doi:10.1097/MD.0000000000029970
20. Cho J, Liang S, Lim S, et al. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio reflect disease activity and flares in patients with systemic lupus erythematosus - A prospective study. Joint Bone Spine. 2022;89(4):105342. doi:10.1016/j.jbspin.2022.105342
21. Kadiyoran C, Zengin O, Cizmecioglu HA, et al. Monocyte to lymphocyte ratio, neutrophil to lymphocyte ratio, and red cell distribution width are the associates with gouty arthritis. Acta Medica. 2019;62(3):99–104. doi:10.14712/18059694.2019.132
22. Qiu X, Shi Z, Tong F, et al. Biomarkers for predicting tumor response to PD-1 inhibitors in patients with advanced pancreatic cancer. Hum Vaccin Immunother. 2023;19(1). doi:10.1080/21645515.2023.2178791
23. Kissling M, Fritschi N, Baumann P, et al. Monocyte, lymphocyte and neutrophil ratios – easy-to-use biomarkers for the diagnosis of pediatric tuberculosis. Pediatr Infect Dis J. 2023;42(6):520–527. doi:10.1097/INF.0000000000003901
24. Forget P, Khalifa C, Defour J, et al. What is the normal value of the neutrophil-to-lymphocyte ratio? BMC Res Notes. 2017;10(1). doi:10.1186/s13104-016-2335-5
25. Simonaggio A, Elaidi R, Fournier L, et al. Variation in neutrophil to lymphocyte ratio (NLR) as predictor of outcomes in metastatic renal cell carcinoma (mRCC) and non-small cell lung cancer (mNSCLC) patients treated with nivolumab. Cancer Immunol Immunother. 2020;69(12):2513–2522. doi:10.1007/s00262-020-02637-1
26. Balin ŞÖ, Tartar AS, Akbulut A. The predictive role of haematological parameters in the diagnosis of osteoarticular brucellosis. Afr Health Sci. 2018;18(4):988–994. doi:10.4314/ahs.v18i4.19
27. Kc SR, Shrestha S, Kc G, et al. Complete blood count parameters in arthritis. Nepal Med College J. 2020;22(3):99–105. doi:10.3126/nmcj.v22i3.32621
28. Toya K, Tomimaru Y, Kobayashi S, et al. Preoperative neutrophil‐to‐lymphocyte ratio predicts healing time for postoperative pancreatic fistula after distal pancreatectomy. AnnGastroenterol Surg. 2022;6(1):169–175. doi:10.1002/ags3.12510
29. Dowlati E, Mualem W, Carpenter A, et al. Early fevers and elevated neutrophil-to-lymphocyte ratio are associated with repeat endovascular interventions for cerebral vasospasm in patients with aneurysmal subarachnoid hemorrhage. Neurocrit Care. 2022;36(3):916–926. doi:10.1007/s12028-021-01399-7
30. Li L, Zhang H, Feng G. Neutrophil-to-lymphocyte ratio predicts in-hospital mortality in intracerebral hemorrhage. J Stroke Cerebrovasc Dis. 2022;31(8):106611. doi:10.1016/j.jstrokecerebrovasdis.2022.106611
31. Jiao J, Huang J, Chen X, et al. Albumin to Globulin ratio, Neutrophil to Lymphocyte ratio, and Globulin levels do not outperform ESR or CRP when diagnosing periprosthetic joint infection. BMC Musculoskelet Disord. 2022;23(1). doi:10.1186/s12891-022-05357-y
32. Korkmaz M, Korkmaz H, Küçüker F, et al. Evaluation of the association of sleep apnea-related systemic inflammation with CRP, ESR, and Neutrophil-to-Lymphocyte Ratio. Med Sci Monit. 2015;21:477–481. doi:10.12659/MSM.893175
33. Balkarli A, Dogru A, Ugan Y, et al. Neutrophil: lymphocyte ratio and mean platelet volume in patients with gout. Ann Clin Anal Med. 2017;8(2):138–141.
34. Şahin A, Uslu AU, Seven D, et al. Evaluation of neutrophil to lymphocyte ratio and monocyte to lymphocyte ratio in gouty arthritis attacks. West Indian Med J. 2015. doi:10.7727/wimj.2015.345
35. Wu H, Zhou H, Chen P. Correlation of neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), and mean platelet volume (MPV) with gout activity: a monocentric and retrospective study. Medicine. 2022;101(35):e30242. doi:10.1097/MD.0000000000030242
36. Zhu K, Deng G, Zhang L, et al. Association of neutrophil-to-lymphocyte ratio with renal impairment among patients with acute gouty arthritis. Int Urol Nephrol. 2022;54(11):2995–3000. doi:10.1007/s11255-022-03239-9
37. Maden M. Development of atherosclerotic cardiovascular mortality in gouty arthritis and rheumatoid arthritis patients: are they associated with mean platelet volume and neutrophil-lymphocyte ratio? A Comparative Study. Archiv Rheumatol. 2017;32(1):39–45. doi:10.5606/ArchRheumatol.2017.6033
38. Desai R, Parekh T, Goyal H, et al. Impact of gout on in-hospital outcomes of acute coronary syndrome-related hospitalizations and revascularizations: insights from the national inpatient sample. World J Cardiol. 2019;11(5):137–148. doi:10.4330/wjc.v11.i5.137
39. Vedder D, Gerritsen M, Nurmohamed MT, et al. A neutrophil signature is strongly associated with increased cardiovascular risk in gout. Rheumatology. 2021;60(6):2783–2790. doi:10.1093/rheumatology/keaa712
40. Zhao R, Wang Y, Fu T, et al. Gout and risk of diabetes mellitus: meta-analysis of observational studies. Psychol Health Med. 2020;25(8):917–930. doi:10.1080/13548506.2019.1707241
41. Mei Y, Dong B, Geng Z, et al. Excess uric acid induces gouty nephropathy through crystal formation: a review of recent insights. Front Endocrinol. 2022;13:911968. doi:10.3389/fendo.2022.911968
42. Sansone A, Reisman Y, Jannini EA. Relationship between hyperuricemia with deposition and sexual dysfunction in males and females. J Endocrinol Invest. 2022;45(4):691–703. doi:10.1007/s40618-021-01719-w
43. Ao J, Goldblatt F, Casson RJ. Review of the ophthalmic manifestations of gout and uric acid crystal deposition. Clin Experiment Ophthalmol. 2017;45(1):73–80. doi:10.1111/ceo.12749
44. Swierczak A, Mouchemore KA, Hamilton JA, et al. Neutrophils: important contributors to tumor progression and metastasis. Cancer Metastasis Rev. 2015;34(4):735–751. doi:10.1007/s10555-015-9594-9
45. Lin B, Du L, Li H, et al. Tumor-infiltrating lymphocytes: warriors fight against tumors powerfully. Biomed Pharmacother. 2020;132:110873. doi:10.1016/j.biopha.2020.110873
46. Cecchi I, Arias De La Rosa I, Menegatti E, et al. Neutrophils: novel key players in rheumatoid arthritis. Current and future therapeutic targets. Autoimmun Rev. 2018;17(11):1138–1149. doi:10.1016/j.autrev.2018.06.006
47. Wu X. Innate Lymphocytes in Inflammatory Arthritis. Front Immunol. 2020;11. doi:10.3389/fimmu.2020.565275
48. Buonacera A, Stancanelli B, Colaci M, et al. Neutrophil to lymphocyte ratio: an emerging marker of the relationships between the immune system and diseases. Int J Mol Sci. 2022;23(7):3636. doi:10.3390/ijms23073636
49. Jameson J, Ugarte K, Chen N, et al. A role for skin γδ T cells in wound repair. Science. 2002;296(5568):747–749. doi:10.1126/science.1069639
50. Carnevale S, Di Ceglie I, Grieco G, et al. Neutrophil diversity in inflammation and cancer. Front Immunol. 2023;14. doi:10.3389/fimmu.2023.1180810
51. Martinon F, Pétrilli V, Mayor A, et al. Gout-associated uric acid crystals activate the NALP3 inflammasome. Nature. 2006;440(7081):237–241. doi:10.1038/nature04516
52. So AK, Martinon F. Inflammation in gout: mechanisms and therapeutic targets. Nat Rev Rheumatol. 2017;13(11):639–647. doi:10.1038/nrrheum.2017.155
53. Wu M, Tian Y, Wang Q, et al. Gout: a disease involved with complicated immunoinflammatory responses: a narrative review. Clin Rheumatol. 2020;39(10):2849–2859. doi:10.1007/s10067-020-05090-8
54. Mitroulis I, Kambas K, Ritis K. Neutrophils, IL-1β, and gout: is there a link? Semin Immunopathol. 2013;35(4):501–512. doi:10.1007/s00281-013-0361-0
55. Martin WJ, Harper JL. Innate inflammation and resolution in acute gout. Immunol Cell Biol. 2010;88(1):15–19. doi:10.1038/icb.2009.89
56. Chhana A, Pool B, Wei Y, et al. Human cartilage homogenates influence the crystallization of monosodium urate and inflammatory response to monosodium urate crystals: a potential link between osteoarthritis and gout. Arthritis Rheumatol. 2019;71(12):2090–2099. doi:10.1002/art.41038
57. Renaudin F, Sarda S, Campillo-Gimenez L, et al. Adsorption of proteins on m-CPPD and urate crystals inhibits crystal-induced cell responses: study on albumin-crystal interaction. J Funct Biomater. 2019;10(2):18. doi:10.3390/jfb10020018
58. Terkeltaub R, Tenner AJ, Kozin F, et al. Plasma protein binding by monosodium urate crystals. Analysis by two-dimensional gel electrophoresis. Arthritis Rheum. 1983;26(6):775–783. doi:10.1002/art.1780260612
59. Xu H, Zhang B, Chen Y, et al. Type II collagen facilitates gouty arthritis by regulating MSU crystallisation and inflammatory cell recruitment. Ann Rheum Dis. 2023;82(3):416–427. doi:10.1136/ard-2022-222764
60. Terkeltaub R, Curtiss LK, Tenner AJ, et al. Lipoproteins containing apoprotein B are a major regulator of neutrophil responses to monosodium urate crystals. J Clin Invest. 1984;73(6):1719–1730. doi:10.1172/JCI111380
61. Alberts A, Klingberg A, Hoffmeister L, et al. Binding of macrophage receptor MARCO, LDL, and LDLR to disease-associated crystalline structures. Front Immunol. 2020;11. doi:10.3389/fimmu.2020.596103
62. Nature. The integrative human microbiome project. Nature. 2019;569(7758):641–648. doi:10.1038/s41586-019-1238-8
63. Pickard JM, Zeng MY, Caruso R, et al. Gut microbiota: role in pathogen colonization, immune responses, and inflammatory disease. Immunol Rev. 2017;279(1):70–89. doi:10.1111/imr.12567
64. Thriene K, Michels KB. Human gut microbiota plasticity throughout the life course. Int J Environ Res Public Health. 2023;20(2):1463. doi:10.3390/ijerph20021463
65. Wang J, Chen Y, Zhong H, et al. The gut microbiota as a target to control hyperuricemia pathogenesis: potential mechanisms and therapeutic strategies. Crit Rev Food Sci Nutr. 2022;62(14):3979–3989. doi:10.1080/10408398.2021.1874287
66. Chu Y, Sun S, Huang Y, et al. Metagenomic analysis revealed the potential role of gut microbiome in gout. NPJ Biofilms Microbiomes. 2021;7(1):66. doi:10.1038/s41522-021-00235-2
67. Wang Z, Li Y, Liao W, et al. Gut microbiota remodeling: a promising therapeutic strategy to confront hyperuricemia and gout. Front Cell Infect Microbiol. 2022;12:935723.
68. Chen Y, Pei C, Chen Y, et al. Kidney tea ameliorates hyperuricemia in mice via altering gut microbiota and restoring metabolic profile. Chem Biol Interact. 2023;376:110449. doi:10.1016/j.cbi.2023.110449
69. Karmarkar D, Rock KL. Microbiota signalling through MyD88 is necessary for a systemic neutrophilic inflammatory response. Immunology. 2013;140(4):483–492. doi:10.1111/imm.12159
70. Schluter J, Peled JU, Taylor BP, et al. The gut microbiota is associated with immune cell dynamics in humans. Nature. 2020;588(7837):303–307. doi:10.1038/s41586-020-2971-8
71. Kim M, Qie Y, Park J, et al. Gut microbial metabolites fuel host antibody responses. Cell Host Microbe. 2016;20(2):202–214. doi:10.1016/j.chom.2016.07.001
72. Vieira AT, Galvão I, Macia LM, et al. Dietary fiber and the short-chain fatty acid acetate promote resolution of neutrophilic inflammation in a model of gout in mice. J Leukoc Biol. 2017;101(1):275–284. doi:10.1189/jlb.3A1015-453RRR
73. Li Y, Li H, Wang R, et al. Protective effect of sodium butyrate on intestinal barrier damage and uric acid reduction in hyperuricemia mice. Biomed Pharmacother. 2023;161:114568. doi:10.1016/j.biopha.2023.114568
74. Garcia-Gonzalez E, Gamberucci A, Lucherini O, et al. Neutrophil extracellular traps release in gout and pseudogout depends on the number of crystals regardless of leukocyte count. Rheumatology. 2021;60(10):4920–4928. doi:10.1093/rheumatology/keab087
75. Euler M, Hoffmann MH. The double-edged role of neutrophil extracellular traps in inflammation. Biochem Soc Trans. 2019;47(6):1921–1930. doi:10.1042/BST20190629
76. Tatsiy O, Mayer TZ, de Carvalho Oliveira V, et al. Cytokine production and NET formation by monosodium urate-activated human neutrophils involves early and late events, and requires upstream TAK1 and Syk. Front Immunol. 2020;10. doi:10.3389/fimmu.2019.02996
77. Tang H, Tan C, Cao X, et al. NFIL3 facilitates neutrophil autophagy, neutrophil extracellular trap formation and inflammation during gout via REDD1-dependent mTOR inactivation. Front Med. 2021;8. doi:10.3389/fmed.2021.692781
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.