")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
The Incidence of Metabolic Syndrome in People Over 40 Years Old with Normal Fasting Plasma Glucose and the Predictive Cutoff Value of Effective Fasting Plasma Glucose for Metabolic Syndrome in Guiyang
Authors Liu Y , Zhuang H, Han N, Yang Y, Zhang Q, Peng N , Hu Y, Shi L, Li H
Received 11 June 2023
Accepted for publication 7 September 2023
Published 25 September 2023 Volume 2023:16 Pages 2979—2989
DOI https://doi.org/10.2147/DMSO.S425412
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Yue Liu,1,* Huijun Zhuang,1,* Na Han,1 Yuxing Yang,1 Qiao Zhang,1 Nianchun Peng,1 Ying Hu,1 Lixin Shi,1 Hong Li1,2 On behalf of REACTION Study Group. REACTION Study Group of author information is available at the end of the article
1Department of Endocrinology and Metabolism, Affiliated Hospital of Guizhou Medical University, Guiyang, Guizhou, 550004, People’s Republic of China; 2School Hospital, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hong Li, Department of Endocrinology and Metabolism, Affiliated Hospital of Guizhou Medical University, No. 28 Guiyi Road, Guiyang, Guizhou, 550001, People’s Republic of China, Tel +8618685136016, Fax +86-851-86770523, Email [email protected]
Purpose: This study aimed to investigate the incidence of metabolic syndrome (MS) in people over 40 years of age with normal blood glucose levels in Guiyang’s urban areas and determine the effective glycemic cutoff value for predicting MS.
Methods: The analysis was based on anthropometric and biochemical indicators of residents aged 40 years or older in urban areas of Guiyang City who participated in the “Epidemiological Study of Tumor Risk in Chinese Patients with Type 2 Diabetes” in 2011. This study included 3509 patients (2567 females and 942 males) with normal fasting plasma glucose (FPG) and no MS. Multivariate logistic regression was used to analyze the correlation between FPG and MS ROC was used to analyze the effective cutoff value of FPG for the incidence of MS.
Results: After 3-year follow-up, 675 patients had MS (567 females and 108 males). MS incidence in the total population was 19.24%, 11.46% in males, and 22.09% in females, and it increased with FPG. After multivariate logistic regression analysis, the risk of MS corresponding to FPG in females and males was OR=4.607,95% CI (3.477– 6.105) and OR=2.944, 95% CI (1.785– 4.855), respectively. ROC results demonstrated that FPG could predict the onset of MS (AUC: 0.720 in males and 0.666 in females).
Conclusion: Increased FPG correlated with the incidence of metabolic syndrome. Subjects with FPG in the normal range still had a high incidence of MS. The population cutoff value for predicting effective FPG for metabolic syndrome was 5.545 mmol/L in men and 5.605 mmol/L in women. Epidemiological investigations are needed to determine whether a lower FPG cutoff value is required to diagnose MS. FPG not only diagnoses diabetes but also serves as a cost-effective and convenient screening method for developing of MS in the general Chinese population.
Keywords: metabolic syndrome, incidence, fasting plasma glucose, cutoff value
Introduction
According to the International Diabetes Federation (IDF) analysis, approximately 25% of the world’s population will suffer from MS.1 MS is characterized by central obesity, abnormal glucose metabolism, dyslipidemia, and other metabolic disorders such as hypertension.2,3 With a growing economy, MS has also grown worldwide.4 Therefore, this is a global public health issue that must be addressed.
Previous studies on residents aged 40 years or older in urban areas of Guiyang City showed that the crude incidence of metabolic syndrome in the total population was 21.86%.5 In addition, a study explored MS incidence in American adults from 1999 to 2014.6 This study included 14,171 NHANES participants with an average age of 46.8±19.3 years, 7354 (51.9%) of whom were female. Later, 4789 participants were diagnosed with MS using the NCEP ATP III diagnostic criteria. From 1999 to 2014, the incidence of MS increased from 27.6% to 32.3%. Studies have also shown that MS incidence in Spain,7 Japan,8 and Taiwan9 is 3.1, 21.0, and 22.9 per 1000 person-years. This indicates that the high prevalence of MS must be taken seriously.
Not only the International Diabetes Federation (IDF), the US National Cholesterol Education Program Adult Treatment Panel III (ATP III), the Chinese Diabetes Society (CDS), and the joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention (JIS) will be involved in the diagnostic criteria of metabolic syndrome, all of these will involve FPG issues. Xing et al10 one study suggested removing the 2h-PPG blood test used to diagnose hyperglycemia from CDS-MS criteria. Instead, it proposes a lower diagnostic threshold of 5.6 mmol/L for FPG. This study was conducted on the 2007–2008 Chinese study population with diabetes and metabolic diseases. This study included 46,239 participants with a mean age of 44.95 years. Conclusions were drawn by comparing the different diagnostic criteria for metabolic syndrome. However, there are no global reports on the overall MS incidence in the general population within the normal FPG range.
Currently, China adopts the diagnostic and classification criteria for diabetes proposed by the International WHO Expert Committee on Diabetes (1999). FPG 3.9–6.0 mmol/L was considered normal. However, it is currently unclear what FPG cutoff value should be used for MS diagnosis. Based on a clinical and epidemiological study of urban residents over 40 years of age in Guiyang, Guizhou Province, China, we conducted a follow-up study of MS incidence among subjects in the normal FPG range to determine an effective FPG threshold for predicting MS and establish a theoretical basis for clinical prevention and early treatment of MS.
Methods
Study Participants
The population was drawn from a Chinese epidemiological study on tumor risk in type 2 diabetes patients. The study was conducted on residents over 40 in the urban area of Guiyang City using a cluster sampling method. The completed survey included 10,140 participants, excluding 3980 patients with baseline MS, 1392 with FPG<3.9mmol/L or FPG>6.1mmol/L, and 123 with incomplete data. A total of 4645 subjects were included in the follow-up. The follow-up period was May 2011 to July 2014. A total of 1136 subjects who were lost to follow-up, had incomplete data, and died were excluded. Finally, 3509 subjects (2567 females and 942 males) were included in the analysis. The data from these subjects were used to conduct a cohort follow-up study with a follow-up rate of 76%. Informed consent was obtained from each participant during data collection. The study was approved by the Guizhou Medical University Ethics Committee.
Data Collection and Measurements
Because our previous study and this one used the same survey, the data collection and measurement procedures were fully documented.5,11 Data were collected by trained physicians through a standardized questionnaire. The data mainly consisted of demographic characteristics, anthropometric parameters, personal medical history, family history, medication use, and lifestyle risk factors such as age, sex, ethnicity, history of diabetes, history of hypertension, smoking, alcohol, and exercise status. Ethnicity was categorized as Han Chinese or other. Smoking was defined as smoking > 100 cigarettes in one’s lifetime. At least 30 g of alcohol were consumed monthly throughout the year. At least 30 minutes of walking activity was required weekly. In addition, the education level was collected and divided into lower and higher education levels.
Professionals measured anthropometric data such as height, weight, body mass index (BMI), and waist circumference (WC). Participants were asked to wear light clothing and no shoes. A calibrated digital scale was used to quantify the standard weights to the nearest 0.1 kg. For height measurements, subjects were asked to maintain a standing position and use a calibrated sight distance scale to quantify the reading to the nearest 0.1 cm. Waist circumference measurement was conducted 1 cm above the umbilicus of the line connecting the anterior superior iliac spine and the umbilicus. When the subject was standing upright and breathing deeply with a relaxed abdomen and calm breathing, a measuring tape was used to measure the lower edge of the 12th rib. The body mass index was calculated as weight/height squared. Blood pressure was measured by a medical professional using an OMRON mercury sphygmomanometer. The participants were allowed to rest for 5 minutes before the measurement. Blood pressure was measured with the patient seated in the right upper arm. The mean systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured three times and calculated in mmHg.
Participants were asked to fast for at least 8 hours. On the day before the study, the participants fasted and stopped taking hypoglycemic drugs for 10 hours after 20:00. Subsequently, 10 mL of fasting venous blood was collected in the morning in a negative-pressure vacuum tube. Except for patients with diabetes, 75 g of anhydrous glucose was administered orally, and blood glucose levels were monitored every 2 hours. Liver and kidney functions and fasting blood glucose levels were tested at the Shanghai Institute of Endocrine Metabolic Diseases. Total cholesterol was measured by glycerol phosphate oxidase, low-density lipoprotein cholesterol (LDL-C) by the direct homogeneous enzymatic method, and high-density lipoprotein cholesterol (HDL-C) was measured using an accelerator selective detergent. In addition, FPG and 2h blood glucose of the oral glucose tolerance test were determined using the hexokinase method.
MS Diagnostic Criteria
We have been studying MS in community populations since 2009 using IDF criteria, and this series of studies followed the 2005 International Diabetes Federation (IDF) criteria.3 Any two of the four indices listed below were combined in patients who met the central obesity standard (WC: male≥90 cm, female≥80 cm);1) triglyceride (TG) ≥ 1.7 mmol/l or undergoing current treatment; 2) HDL-C < 1.03 mmol/l (male) or < 1.29 mmol/l (female) or undergoing current treatment; 3) blood pressure rise: SBP ≥ 130 mmHg or DBP ≥ 85 mmHg or undergoing current treatment or having hypertension; and 4) FPG ≥ 5.6 mmol/l or undergoing current treatment or having type 2 diabetes (T2D).
Statistical Analyses
SPSS 25.0 statistical software was used for data analysis. Each gender was analyzed separately. When continuous variables were not normally distributed, a nonparametric test of two independent samples was chosen for the one-way study. The results were expressed as the median, upper, and lower quartiles. The qualitative variables were statistically described using rates. The qualitative information is expressed as the total number of cases (n) and percentages (%). The chi-square test (χ2) was used for statistical analysis. Multivariate logistic regression analysis was performed after 3 years of follow-up to explore the independent association between FPG and MS occurrence. The OR value and 95% CI of FPG were calculated. The Receiver Operating characteristic (ROC) curve was used to determine the optimal cutoff point for FPG diagnosis. The optimal diagnostic cutoff point was obtained when the Yoden index was at its maximum. P< 0.05 was considered statistically significant.
Results
Comparison of Basic Characteristics of Female and Male Subjects After Follow-Up
A total of 3509 participants (males 26.85% and females 73.15%) were included in the analysis. After 3-year follow-up, 108 men and 567 women without MS at baseline developed MS. The incidence was 11.46% and 22.09% for men and women, respectively. There was a significant difference in the incidence of metabolic syndrome between males and females (χ2=50.056, P<0.001). The incidence of metabolic syndrome was significantly higher in women than in men. Among females, MS group were older than non-MS group. Female MS patients had a lower level of education, and there was no difference in men’s education level between the MS morbidity and non-morbidity groups. In women, all indicators except race, walking activity, smoking, alcohol consumption, and LDL-C were statistically significant in both the onset and non-onset groups of MS. In addition to height and HDL-C, cholesterol (CHOL), body weight, BMI, WC, SBP, DBP, CHOL, TG, and FPG in the disease group were higher than in the non-disease group. Among men, other factors were statistically significant, except for race, education level, walking activity, smoking, alcohol consumption, and LDL. Except for age and HDL-C, height, body weight, BMI, WC, SBP, DBP, CHOL, TG, and FPG were all higher in the morbidity group than in the non-morbidity group (Table 1).
 |
Table 1 Incidence of MS Stratified by Sex in the Follow-Up Population with Baseline Normal FPG Range |
Comparison of MS Incidence Among FPG Quartile Arrays FPG
The incidence of MS was compared between the quartiles of FPG for different sexes (Figure 1). The incidence of MS was significantly higher in the highest FPG quartile group in both men and women than in the other lower quartiles. In women, the incidence of MS displayed a continuous increase with increasing FPG quartile. Men with MS syndrome showed a slight decrease, followed by a significant increase as the FPG quartiles increased. There was a significant correlation between FPG and MS incidence in men and women, with a 4.83-fold increase in MS incidence in women and only a 3.75-fold increase in men in the comparison between the lower and upper quartiles (P<0.001). Based on the results of both groups, MS incidence and FPG are strongly correlated.
 |
Figure 1 The Incidence of MS by quartiles of FPG. |
Incidence of MS Within the Baseline Normal FPG Range in Subjects of Different Age Groups
Table 2 compares MS incidence in men and women of different ages after 3- year follow-up in subjects with a normal baseline FPG. MS incidence in males aged from 40 to 49 years, 50 to 59 years, 60 to 69 years, and over 70 years was 5.56%, 33.33%, 51.85%, and 9.26%, respectively. MS incidence in females was 8.11%, 37.92%, 41.98%, and 11.99%, respectively. The incidence of MS in males and females significantly differed between the different age groups. MS incidence increased significantly with age in women aged 40–69 years (P<0.001), and it also increased significantly in men aged 40–69 years (P=0.015).
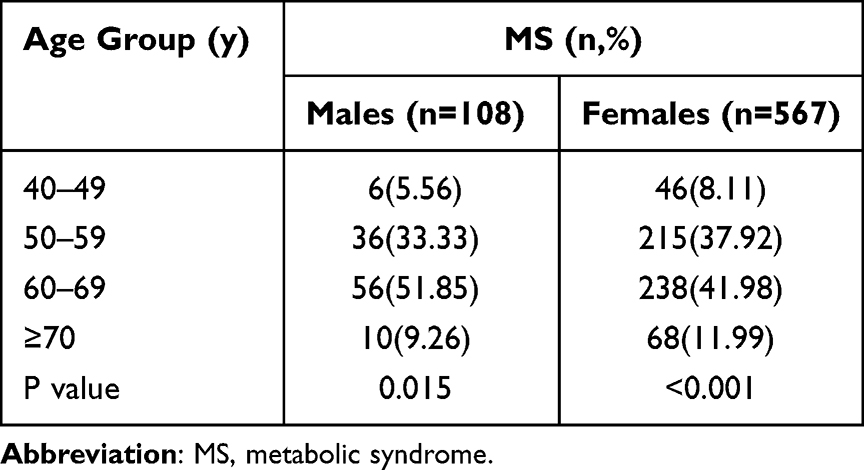 |
Table 2 Incidence of MS with Baseline Normal FPG Range in Subjects of Different Age Groups |
Binary Logistic Regression Analysis of the Relationship Between the Incidence of FPG and MS
Logistic regression analysis further evaluated the correlation between FPG and MS incidence (Table 3). FPG and the incidence of MS were strongly correlated. Gender was an independent risk factor for MS. The risk in females was higher than in males. In the crude model, the odds ratios(ORs) of males and females with a one-unit increase in FPG were 2.944 (1.785~4.855) and 4.610 (3.479~6.109), respectively. After adjusting for age, the association changed but remained strong, with a one-unit increase in FPG associated with a 2.835-fold increase in the risk of MS in men. After adjusting for height and age, the correlation between FPG and MS incidence was weakened but not obvious. When FPG increased by one value, the risk of MS incidence in males still increased by 2.769 times. In women, the correlation was stronger after adjusting for age, the risk of MS increased by 4.615 times for each unit value increase of FPG. After adjusting for height and age, the correlation between FPG and MS incidence was still enhanced. When FPG increased by one value, the risk of MS incidence in women was still increased by 4.631 times. The OR value for FPG in women was higher than in men, and the correlation between FPG and MS incidence was stronger in women.
 |
Table 3 Multivariate Logistic Regression of FPG for MS |
ROC Analysis of FPG in Subjects with MS and Prediction of Effective FPG Threshold for MS
Figure 2 depicts FPG ROC curves that predict the overall male and female MS incidence. Except for the female FPG cutoff points, the cutoff points are more specific than sensitive. The AUC of the ROC analysis compared the predictive ability of MS onset in the population, in women and men (Table 4). In the area under the curve (AUC) of relevant biochemical indicators for MS patients, the AUC value of FPG of MS patients was highly correlated with MS incidence, and the AUC value of the overall FPG was 0.702 (P<0.001). The incidence was considered when the FPG level exceeded 5.595 mmol/L. values less than this were considered disease-free. The sensitivity and specificity were 0.492 and 0.827, respectively, which were critical points. The sensitivity and specificity of this point were very high. The AUC value of FPG in males was 0.720 (P<0.001). When FPG was >5.545 mmol/L, the sensitivity was 0.515, and the specificity was 0.833, indicating the onset of MS. The AUC value of female FPG was 0.666 (p<0.001). When FPG was >5.605 mmol/L, the sensitivity and specificity were 0.537 and 0.463, respectively, indicating the onset of MS. FPG has a high degree of accuracy in predicting MS incidence.
 |
Table 4 ROC Analysis of MS in the Follow-Up Population with Baseline Normal FPG Range |
 |
Figure 2 ROC curves for FPG to predict MS in subjects with baseline normal FPG range. |
Discussion
Cardiovascular disease is the leading cause of death in developed and developing countries.12 It is widely accepted that metabolic syndrome increases the risk of diabetes, cardiovascular disease (CVD), and all-cause death.13,14 Therefore, the incidence of MS cannot be disregarded. Early prevention and treatment of MS will significantly reduce the occurrence of chronic diseases such as diabetes and CVD. This prospective cohort study of the general Chinese population found a strong positive association between FPG and MS incidence. Our results also support the accuracy of FPG in predicting the incidence of MS in individuals with normal FPG without any additional examination or cost and finding the effective FPG threshold for predicting metabolic syndrome. Therefore, our study provides an economical route for the early control of diabetes and the subsequent primary prevention of cardiovascular outcomes.
We have been studying MS in the community population since 2009, and this study is one of a series of studies. Previous studies on people over 40 years in Guiyang urban area showed that the incidence of metabolic syndrome in the total population was 21.86%.5 After 3-year follow-up, subjects with baseline FPG>3.9mmol/L or <6.1mmol/L were excluded. This study demonstrated that the incidence rate of metabolic syndrome among people over 40 years in the normal blood glucose range in the Guiyang urban area was 19.24%. Our research group previously surveyed the incidence rate of MS among subjects over 40 years in the normal blood pressure range in the Guiyang urban area, excluding subjects with blood pressure ≥140/90 mmHg or ≤90/60 mmHg. The incidence of MS was 19.83%,11 similar to this study. Yang et al15 studied the incidence of metabolic syndrome among adults in rural communities of islands in Zhejiang Province. A follow-up survey was conducted in Yuhuan City, Zhejiang Province in 2018. There were 522 cases of metabolic syndrome among 3162 follow-up subjects in the baseline survey in 2012, with a cumulative incidence of 16.5% in 6 years. The incidence of metabolic syndrome was higher among unemployed, smoking, and drinking subjects. Carnethon et al16 studied Coronary Artery Risk Development in Young Adults (CARDIA). A total of 4192 Americans aged 18–30 (49% black) were followed from 1985 to 2001 based on the National Cholesterol Education Program Adult Treatment Panel III diagnostic criteria. The incidence of MS was 13.72%. The incidence of MS among subjects in Guiyang was significantly higher, possibly because of the different influences of race, economic development level, and diagnostic criteria. However, it is necessary to detect and prevent higher incidence in advance.
In Guiyang, the incidence of MS in people over 40 with normal blood glucose levels showed a higher trend in females than males. The incidence of MS in males and females was 11.46% and 22.09%, respectively. In this study, there was a significant positive correlation between FPG and MS incidence. The incidence of MS in the highest quartile array of FPG in women was higher than in men. Since 2003, 762 subjects (332 males and 430 females) aged over 20 years in rural areas of South Korea have been followed up for 5 years.17 MS incidence in males and females was 13.9% and 20.8%. Cohort studies, including those on US military personnel18 and Thailand19 have reported a higher incidence of MS in women than men. The inclusion criteria for these studies differed from those of our study. Our study focused on the difference in MS incidence in people with normal FPG, consistent with previous research findings. There are few studies on the relationship between normal FPG levels and MS incidence at home and abroad, which is one of the innovations of this study. This study divided the men and women into different age groups. When the FPG level was within the normal range, the incidence of MS increased with age in both men and women aged 40–69 years, except for subjects aged 70 years and older, where the incidence decreased. Hwang et al17 showed in a cohort study in South Korea that MS incidence was the highest in men aged < 50 years. Before age 50, the incidence of MS in women was lower than that in men. However, our study found that the disease incidence was significantly higher in women than in men after the age of 50 years. Men and women had the most cases between 60 and 69. This condition may be linked to changes in the hormone levels in woman after menopause. One population condition in our study was related to normal FPG. A study on the relationship between menopausal hormone changes and MS incidence based on bioinformatics20 showed that MS prevalence in postmenopausal women was significantly higher than that in premenopausal women, and the risk of high fasting blood glucose in postmenopausal women increased with an increase in menopause years. Numerous cross-sectional studies have displayed that postmenopausal women are more likely to develop CVD and T2D than premenopausal women by affecting central fat redistribution, arterial pressure, and insulin function.21 This high risk of CVD and T2D in postmenopausal women is associated with an increased risk of MS during menopausal transition.22 Therefore, the incidence of MS and other chronic diseases in postmenopausal women in Guiyang should be considered.
This study depicts that education level is negatively correlated with the risk of MS among females, while there is no significant difference among males. In a longitudinal prospective cohort study of the Iranian population,23 it was also found that MS incidence decreased with an increase in education level among females, while there was no difference among males. In the study by Wilsgaard and Jacobsen,24 the longest follow-up period was 22 years from 1979–1980 to 2001, and a correlation between several lifestyle factors and metabolic syndrome events in both men and women was observed. It was also found that education level was negatively correlated with the incidence of MS in women but not significantly correlated with that in men. Therefore, in areas with underdeveloped education, we should increase the popularization of the science of healthy lifestyles to improve the preventive role of education in reducing the risk of MS.
Several studies have shown increased FPG to be a key feature that increases the risk of developing MS. A prospective study of predictors of metabolic syndrome in non-diabetic adults included 714 white, black, and Hispanic IRAS study participants who were MS-free at baseline and 139 who developed MS after 5-year follow-up.25 FPG was a significant predictor in this univariate model, and FPG was associated with a significantly increased risk of MS. Santos et al26 also reached a similar conclusion in their study on the incidence of MS in southern European urban populations. They established that higher FPG is associated with an increased risk of MS. A study comparing the ability to FPG and HBA1c to predict the onset of MS in normoglycemic Ghanaian adults27 found that FPG was the best predictor of MS and its components. These results are consistent with those of our study and highlight the importance of impaired blood glucose levels in MS progression.
The commonly used diagnostic criteria for MS are CDS, IDF and NEPA TPIII, and the critical values of FPG are 6.1, 5.6, and 5.6mmol/L, respectively. CDS has poor consistency with international traditional diagnostic criteria among these diagnostic criteria. At present, there are few studies on the critical FPG for the diagnosis of MS. This study was a 3-year cohort follow-up study based on FPG threshold for MS. When the FPG of the subjects was within the normal range, the critical value for male subjects was 5.545mmol/L, and the critical value for female subjects was 5.605mmol/L, which has diagnostic significance for the onset of MS. In a large cross-sectional study that revised the CDS criteria and determined the optimal FPG cutoff value for diagnosing hyperglycemia in the Chinese population,10 the selected subjects were the Chinese diabetes and metabolic disease study population from 2007 to 2008. In total, 46,239 participants with an average age of 44.95 years old were included in the study. According to the 2013 CDS-MS hyperglycemia diagnostic criteria, the optimal diagnostic threshold of FPG was determined to be 5.62 mmol/L according to the ROC curve of the subjects. The sensitivity and specificity of the optimal FPG cutoff point were 66.92% and 89.09%. Finally, it was concluded that reducing the FPG diagnostic threshold to 5.6 mmol/L in the CDS-MS standard is more suitable for diagnosing MS in the Chinese population. In our study, the FPG critical value of subjects in the whole population was slightly lower than that of Xing et al.10 Based on the diagnostic criteria of IDF, the optimal FPG critical value suitable for diagnosing MS in the Chinese population was determined using the ROC curve to be 5.595 mmol/L. Although based on different diagnostic criteria, similar conclusions have been reached regarding the optimal diagnostic threshold for FPG.
In the ROC curve analysis in this study, the AUC value of FPG was also highly correlated with MS incidence. After gender stratification, the AUC value of male FPG was higher than that of female FPG. The optimal cutoff point for the AUC value of male FPG was 5.545, sensitivity was 0.515, and specificity was 0.833. For female FPG, the optimal tangent point of the AUC value was 5.605, the sensitivity was 0.537, and the specificity was 0.463. Therefore, when the FPG was within the normal range, the cutoff value of FPG was 5.5mmol/L for men and 5.6mmol/L for women, which were effective predictive cutoff values for MS. This study’s FPG cutoff value was lower than the FPG cutoff value defined by CDS, a commonly used MS diagnostic standard in China. However, more regional and extensive epidemiological investigations are needed to determine whether the cut-off for optimal FPG diagnosis of MS can be reduced.
This study had some limitations. First, our analysis did not adjust for dietary habits, family history, etc., which may have influenced the incidence of FPG and MS. Second, our sample selected Guiyang, a relatively backward city in southwest China, and the results may not apply to people and races in other regions. Third, other indicators related to the presence of MS were not collected in our study design owing to epidemiological feasibility, and other potential confounding factors may have interfered with the results.
This is the first IDF criteria-based study in China to determine the optimal FPG threshold for the diagnosis of MS in the Chinese population. The sample size of this study was large, the age range of the participants was wide, and the data control was strict. In addition, we also verified the stability of the results using a sensitivity analysis.
Conclusions
Our study confirmed a significant independent association between FPG and MS in a general Chinese population with normal blood glucose levels. The critical effective FPG values for predicting MS were determined to be 5.545mmol/L for males and 5.605mmol/L for females. Our findings have improved the application value of FPG in the clinical diagnosis of MS using simple methods to screen high-risk diabetes and cardiovascular disease populations. In addition, the utilization of FPG in routine health examinations holds potential for the early identification of individuals at high risk for MS, especially for people over 40. It should also be noted that additional research in multiracial populations is needed to validate our optimal FPG cutoff values.
Data Sharing Statement
Data for the current study can be obtained from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of the Affiliated Hospital of Guizhou Medical University and was in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent had already been given by all the subjects.
Acknowledgments
We thank the participants for participating in the study. We appreciate the REACTION Study Group’s and the Steering Committee of the REACTION Study Group’s help in this study.
REACTION Study Group: Weiqing Wang, Yufang Bi, Jieli Lu, National Clinical Research Center for Metabolic Diseases, Rui Jin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China; Yiming Mu, Chinese People’s Liberation Army General Hospital, Beijing, China; Jiajun Zhao, Shandong Provincial Hospital affiliated with Shandong University, Jinan, China; Chao Liu, Jiangsu Province Hospital on the Integration of Chinese and Western Medicine, Nanjing, China; Lulu Chen, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China; Lixin Shi, Affiliated Hospital of Guiyang Medical College, Guiyang, China; Qiang Li, The Second Affiliated Hospital of Harbin Medical University, Harbin, China; Tao Yang, The First Affiliated Hospital of Nanjing Medical University, Jiangsu Province Hospital, Nanjing, China; Li Yan, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, China; Qin Wan, The Affiliated Hospital of Luzhou Medical College, Luzhou, China; Shengli Wu, Karamay Municipal People’s Hospital, Xinjiang, China; Guixia Wang, The First Hospital of Jilin University, Changchun, China; Zuojie Luo, The First Affiliated Hospital of Guangxi Medical University, Nanning, China; Xulei Tang, The First Hospital of Lanzhou University, Lanzhou, China; Gang Chen, Fujian Provincial Hospital, Fujian Medical University, Fuzhou, China; Yanan Huo, Jiangxi People’s Hospital, Nanchang, China; Zhengnan Gao, Dalian Municipal Central Hospital, Dalian, China; Qing Su, Xinhua Hospital Affiliated with Shanghai Jiaotong University School of Medicine, Shanghai, China; Zhen Ye, Zhejiang Provincial Center for Disease Control and Prevention, China; Youmin Wang, The First Affiliated Hospital of Anhui Medical University, Hefei, China; Guijun Qin, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China; Huacong Deng, The First Affiliated Hospital of Chongqing Medical University, Chongqing, China; Xuefeng Y u, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China; Feixia Shen, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China; and Li Chen, Qilu Hospital of Shandong University, Jinan, China.
Steering Committee of the REACTION Study Group: Guang Ning (Principal Investigator), National Clinical Research Center for Metabolic Diseases, Rui Jin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China. Yiming Mu, Chinese People’s Liberation Army General Hospital, Beijing, China. Jiajun Zhao, Shandong Provincial Hospital affiliated with Shandong University, Jinan, China. Weiqing Wang, National Clinical Research Center for Metabolic Diseases, Rui Jin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China. Chao Liu, Jiangsu Province Hospital on the Integration of Chinese and Western Medicine, Nanjing, China. Y ufang Bi, National Clinical Research Center for Metabolic Diseases, Rui Jin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China. Donghui Li, Department of Gastrointestinal Medical Oncology, the University of Texas MD Anderson Cancer Center, Houston, Texas, USA. Shenghan Lai, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA. Zachary T. Bloomgarden, Mount Sinai School of Medicine, New York, USA.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the National Key R&D Program of China (2017YFC1310704).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Poh S, Mohamed Abdul RB, Lamoureux EL, et al. Metabolic syndrome and eye diseases. Diabetes Res Clin Pract. 2016;113:86–100. doi:10.1016/j.diabres.2016.01.016
2. Dobrowolski P, Prejbisz A, Kurylowicz A, et al. Metabolic syndrome - a new definition and management guidelines: a joint position paper by the Polish Society of Hypertension, Polish Society for the Treatment of Obesity, Polish Lipid Association, Polish Association for Study of Liver, Polish Society of Family Medicine, Polish Society of Lifestyle Medicine, Division of Prevention and Epidemiology Polish Cardiac Society, “club 30” Polish Cardiac Society, and Division of Metabolic and Bariatric Surgery Society of Polish Surgeons. Arch Med Sci. 2022;18(5):1133–1156. doi:10.5114/aoms/152921
3. Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2005;365(9468):1415–1428. doi:10.1016/S0140-6736(05)66378-7
4. Alberti KG, Zimmet P, Shaw J. Metabolic syndrome—a new world-wide definition. A Consensus Statement from the International. Diabetes Federation Diabet Med. 2006;23(5):469–480. doi:10.1111/j.1464-5491.2006.01858.x
5. Yue L, Huijun Z, Hong L, et al. Cardiometabolic index and metabolic syndrome in the Population over 40 years old in Guiyang city: a prospective cohort study. Chin J Endocrinol. doi:10.3760/cma.j.cn311282-20220114-00024
6. Li W, Qiu X, Ma H, et al. Incidence and long-term specific mortality trends of metabolic syndrome in the United States. Front Endocrinol. 2022;13:1029736. doi:10.3389/fendo.2022.1029736
7. Pimenta AM, Toledo E, Rodriguez-Diez MC, et al. Dietary indexes, food patterns and incidence of metabolic syndrome in a Mediterranean cohort: the SUN project. Clin Nutr. 2015;34(3):508–514. doi:10.1016/j.clnu.2014.06.002
8. Haruyama Y, Nakagawa A, Kato K, et al. Incidence of metabolic syndrome in young japanese adults in a 6-year cohort study: the Uguisudani Preventive Health Large-Scale Cohort Study (UPHLS). J Epidemiol. 2020;30(5):219–226. doi:10.2188/jea.JE20180246
9. Shang P, Shu Z, Wang Y, et al. Veganism does not reduce the risk of the metabolic syndrome in a Taiwanese cohort. Asia Pacific J Clin Nutr. 2011;20:404–410.
10. Xing Y, Xu, S, Jia, A, Cai, J, Zhao, M, Guo, J, Ji, Q, Ming, J. Recommendations for revision of Chinese diagnostic criteria for metabolic syndrome: a nationwide study. J Diabetes. 2018;10(3):232–239. doi:10.1111/1753-0407.12578
11. Ma L, Li H, Zhuang H, et al. The incidence of metabolic syndrome and the valid blood pressure cutoff value for predicting metabolic syndrome within the normal blood pressure range in the population over 40 years old in Guiyang, China. Diabetes Metab Syndr Obes. 2021;14:2973–2983. doi:10.2147/DMSO.S308923
12. Virani SS, Alonso A, Aparicio HJ, et al. Heart disease and stroke statistics-2021 update: a report from the American Heart Association. Circulation. 2021;143(8):e254–e743. doi:10.1161/CIR.0000000000000950
13. Tang X, Wu M, Wu S, et al. Continuous metabolic syndrome severity score and the risk of CVD and all-cause mortality. Eur J Clin Invest. 2022;52(9):e13817. doi:10.1111/eci.13817
14. Grundy SM. Metabolic syndrome pandemic. Arterioscler Thromb Vasc Biol. 2008;28(4):629–636. doi:10.1161/ATVBAHA.107.151092
15. Yang SY, Li ST, Ying XH, et al. [Incidence and risk factors of metabolic syndrome in rural community population on islands in Zhejiang province]. Zhonghua liuxingbingxue zazhi. 2022;43(3):387–391. Chinese. doi:10.3760/cma.j.cn112338-20210305-00175
16. Carnethon MR, Loria CM, Hill JO, Sidney S, Savage PJ, Liu K. Coronary artery risk development in young adults study. Risk factors for the metabolic syndrome: the Coronary Artery Risk Development in Young Adults (CARDIA) study, 1985-2001. Diabetes Care. 2004;27(11):2707–2715. doi:10.2337/diacare.27.11.2707
17. Hwang JH, Kam S, Shin JY, et al. Incidence of metabolic syndrome and relative importance of five components as a predictor of metabolic syndrome: 5-year follow-up study in Korea. J Korean Med Sci. 2013;28(12):1768–1773. doi:10.3346/jkms.2013.28.12.1768
18. Williams VF, Oh GT, Stahlman S. Incidence and prevalence of the metabolic syndrome using ICD-9 and ICD-10 diagnostic codes, active component, U.S. Armed Forces. 2018;25(12):20–25.
19. Pietroiusti A, Neri A, Somma G, et al. Incidence of metabolic syndrome among night-shift healthcare workers. Occup Environ Med. 2009;67(1):54–57. doi:10.1136/oem.2009.046797
20. Jaballah A, Soltani I, Bahia W, et al. The relationship between menopause and metabolic syndrome: experimental and bioinformatics analysis. Biochem Genet. 2021;59(6):1558–1581. doi:10.1007/s10528-021-10066-7
21. Zhou H, Zhang C, Ni J, et al. Prevalence of cardiovascular risk factors in non-menopausal and postmenopausal inpatients with type 2 diabetes mellitus in China. BMC Endocr Disord. 2019;19(1):98. doi:10.1186/s12902-019-0427-7
22. Carr MC. The emergence of the metabolic syndrome with menopause. J Clin Endocrinol Metab. 2003;88(6):2404–2411. doi:10.1210/jc.2003-030242
23. Hosseini N, Talaei M, Dianatkhah M, et al. Determinants of incident metabolic syndrome in a middle eastern population: isfahan cohort study. Metab Syndr Relat Disord. 2017;15(7):354–362. doi:10.1089/met.2016.0156
24. Wilsgaard T, Jacobsen BK. Lifestyle factors and incident metabolic syndrome. The tromso study 1979–2001. Diabetes Res Clin Pract. 2007;78(2):217–224. doi:10.1016/j.diabres.2007.03.006
25. Palaniappan L, Carnethon MR, Wang Y, et al. Predictors of the incident metabolic syndrome in adults: the insulin resistance atherosclerosis study. Diabetes Care. 2004;27(3):788–793. doi:10.2337/diacare.27.3.788
26. Santos AC, Severo M, Barros H. Incidence and risk factors for the metabolic syndrome in an urban South European population. Prev Med. 2010;50(3):99–105. doi:10.1016/j.ypmed.2009.11.011
27. Amidu N, Owiredu W, Quaye L, et al. Comparative abilities of fasting plasma glucose and haemoglobin A1c in predicting metabolic syndrome among apparently healthy normoglycemic Ghanaian adults. Int J Chronic Dis. 2019;2019:2578171. doi:10.1155/2019/2578171
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.