")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
The Incidence of Adult Obesity is Associated with Parental and Adolescent Histories of Obesity in North Sumatra, Indonesia: A Cross-Sectional Study
Authors Sari DK , Ichwan M, Masyithah D, Dharmajaya R, Khatib A
Received 14 June 2021
Accepted for publication 26 August 2021
Published 3 September 2021 Volume 2021:14 Pages 2437—2444
DOI https://doi.org/10.2147/JMDH.S324774
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Dina Keumala Sari.
Views: 116
Dina Keumala Sari,1 M Ichwan,2 Dewi Masyithah,3 Ridha Dharmajaya,4 Alfi Khatib5
1Department of Nutrition, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia; 2Department of Pharmacology, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia; 3Department of Parasitology, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia; 4Department of Neurosurgery, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia; 5Kulliyah of Pharmacy, International Islamic University Malaysia, Kuala Lumpur, Malaysia
Correspondence: Dina Keumala Sari
Department of Nutrition, Faculty of Medicine, Universitas Sumatera Utara, Jl. Dr. Mansyur No. 5, Padang Bulan, Kec. Medan Baru, Kota Medan, Sumatera Utara, Medan, 20155, Indonesia
Tel +62 81397177693
Email [email protected]
Purpose: Obesity that occurs in adulthood is influenced by various factors, not only energy balance, especially concerning the amount of energy consumed, but also heredity. The hereditary factors of obese parents on childhood obesity have been studied, but what about adulthood? This study examines the relationship between a history of obesity in adolescence, and maternal and paternal incidences of adult obesity.
Patients and Methods: This study was a cross-sectional study that included adult men and women aged 20– 60 years old. The subjects had no chronic or metabolic disease. This research was conducted from April to November, 2020, in North Sumatra Province, Indonesia. The parameters studied were demographics, daily food intake, anthropometry and a history of obesity in adolescence, and for the participants’ fathers and mothers. The statistical test used was the chi-squared test/Fisher test.
Results: This study included 136 research subjects, 60 male and 76 female; based on the results of the study, 47.8% were found to be obese, but food intake showed a low intake (96.2%). There was a significant relationship between a history of obesity in adolescence and incidences of obesity (≥ 30 kg/m2) in the mother and father, with significance values of p=0.01, p=0.004, and p=0.001, respectively.
Conclusion: This study found that there was a significant relationship between a history of obesity in adolescence and incidences of adult obesity (≥ 30kg/m2) in parents, but not with the level of food intake per day. The risk of obesity will increase further with a history of obesity in parents and obesity in adolescence, and this can be used to understand and prevent obesity.
Keywords: adolescent, energy, food, heredity, anthropometry
Introduction
The overall increase in obesity worldwide has not only occurred in developed countries; this increase has also been experienced by developing countries such as those in Asia.1 It is estimated that there will be an increase in obesity cases every year.1,2 Weight gain during growth, especially adolescence, can lead to obesity in adulthood.3,4 However, previous studies that have examined obesity in adolescence were influenced by diet and by a history of obesity in parents.3 This is controlled by the obesity gene that parents pass down.5
The prevalence of obesity in children globally, especially in Asia, is increasing.1 The increase is estimated to be more than 30%, especially in developing countries compared to developed countries.1,6,7 Cases of obesity are also more common in urban areas than in rural areas.1,8 Overweight and obesity are defined as excess fat accumulation that poses a dangerous health risk.6,9 A body mass index of more than 25 kg/m2 is expressed as overweight, and more than 30 kg/m2 is declared as obese.1 However, in Asia–Pacific countries, the criteria for obesity are set as the body mass index being more than 25 kg/m2.10 The rate at which obesity is increasing has more than quadrupled, from 4% to 18% since 1975, not only in high-income countries, but also in low- and middle-income countries.1,8 The prevalence of obesity is increasing in major cities in Indonesia, including in North Sumatra, where the prevalence rate of obesity has reached 30%.11
Obesity is closely related to the accumulation of fat in the abdomen, namely, abdominal visceral fat, which causes the dysregulation of fatty acid metabolism, which later becomes key for type 2 diabetes mellitus.6,12,13 Therefore, obesity studies are vital in order to develop understandings of health and prevent obesity in the future. The increase in body weight during adolescence will determine obesity in adulthood; this is a determining factor because obese adolescents tend to become obese adults.3 Furthermore, if obesity occurs in adulthood, it will be easier for non-communicable diseases such as diabetes, cardiovascular disease, and complications of other metabolic disorders to occur.3–5
Previous research has shown that there is a relationship between obesity in adolescence and obesity in adulthood.4,14–16 In addition to a history of obesity in adolescence, the obesity gene inherited by parents is closely related to the likelihood of a person being obese compared with adolescents who have parents with a history of being a normal weight.17–20 Previous research reported that there is an influence of maternal obesity on dietary fat intake in children, suggesting that mothers may contribute to the development of obesity in children by influencing their dietary fat intake.4 This research also explored how dietary fat intakes contribute to obesity in boys, independent of physical activity energy expenditure.4 There were also associations between a family history of diabetes (FHD) in children and adolescents, which remained strong for girls and boys.15,16 However, other research has reported that parents’ own obesity-related behaviors are factors that may affect their confidence to support their child’s behavioral changes.14 Therefore, actors seeking to prevent childhood obesity should address parent/family behaviors as part of their obesity prevention strategies.14
The development of obesity prevention techniques needs to be emphasized. The role of genes, especially obesity genes inherited from parents, can be a target for preventing obesity in adulthood.5 In addition, the role of parents in preventing obesity is needed, especially in forming children’s habits.14,21,22 Based on various studies, it can be seen that there is a role of genes inherited by the father or mother in the occurrence of obesity in children, in addition to obesity which occurs in adolescence also determining the occurrence of obesity in adulthood. These factors can be studied and observed along with the increasing prevalence of obesity in Asian countries; thus, this study aimed to find the relationship between a history of obesity in adolescence and parents with a history of adult obesity. The results of this study are expected to provide an understanding of preventing obesity through socialization, communicating the importance of maintaining a normal body weight during adolescence.
Methods
Study Design
This study included a cross-sectional design that took sociodemographic data (ie, age, sex, occupation, adolescent history, history obesity of father and mother), anthropometric examinations (ie, body mass index and abdominal circumference), and examinations of daily food intake (ie, energy, fat, protein, and carbohydrate intakes per day) in the study subjects. This study included the incidence of adult obesity as a dependent variable, with parental and adolescent histories of obesity as independent variables.
All research subjects were recruited from the same region, in rural areas in North Sumatera and Medan City, Sumatra Island, Indonesia. This research was conducted from April to July, 2020, after the COVID-19 pandemic had spread across the globe; the data collection was carried out with the implementation of strict health protocols.
Participants
The included research subjects were healthy men and women aged 20–60 years old; the exclusion criteria included pregnant women, nursing mothers, impaired kidney and liver functions, chronic disease, or other metabolic disorders. Research subjects were sampled randomly at existing public health centers. The dissemination of information was performed through counseling about the importance of maintaining health by maintaining a normal weight to prevent obesity. The research subjects volunteered willingly, with the number of subjects gathered being 153 subjects, although after applying the exclusion criteria, 136 subjects were included in the criteria and data analysis.
Statistical Analysis
Data were analyzed using version 11.5 of the IBM-SPSS statistical program (IBM Corp., Chicago, IL). Categorical variables were expressed as percentages. Normally distributed continuous variables were expressed as the mean ± SD, whereas non-normally distributed continuous variables were expressed as medians (minimum–maximum). The tests were performed to identify whether there was a relationship between a history of obesity in adolescence and parents with a history of obesity, using the chi-squared test; however, if this did not meet the requirements, Fisher’s test was used.
Sample Size and Power Calculation
This study aimed to prove the research hypothesis that there is a relationship between a history of obesity in adolescence, as well as parents with a history of obesity. To determine the minimum sample size in each two-tailed hypothesis test, this study had a significance level of 0.05 (α-value) and 80% power (β-value). This study calculated all hypotheses and took the largest sample size. This study used a purposive sampling method, which is a sampling technique based on the researcher’s considerations regarding which samples are the most appropriate, useful and considered to be representative of a population.
Parental and Adolescent’s History
This study used a questionnaire completed by the participants, which collected data pertaining to age, gender, ethnicity, a history of obesity in parents, and a history of obesity in adolescence. This research used a retrospective approach, where effects were identified at this time; then, risk factors are identified as existing or having occurred in the past.
Anthropometric Examination
Anthropometry included height (to the nearest 0.5 cm), weight (to the nearest 0.1 kg), and body mass index (calculated as kg/m2). The categorized body mass index (BMI) was based on the World Health Organization (WHO) guidelines for the general population, which are <18.5 kg/m2 classified as underweight; 18.5–24.9 kg/m2 classified as normal weight; 25–29.9 kg/m2 classified as overweight/at risk; and >30 kg/m2 classified as obese.10 The assessment of obesity based on the World Health Organization criteria is applied globally, namely, ≥30 kg/m2; the criteria for the association analysis were obese and not obese.1 We examined waist circumference using a standardized measuring tape, in centimeters. The category of abdominal circumference was different between men and women. For men, less than 90 cm was classified as normal, and more than 90 cm was classified as central obesity. For women, an abdominal circumference of less than 80 cm was classified as normal, and that more than or equal to 80 cm was classified as central obesity.10
Nutrient Intake Assessment
Assessments of nutrient intakes were based on food recall for two days (one weekday and one day), including energy, protein, fat, and carbohydrate intakes, and the percentage of fulfilment according to the Indonesian Recommended Dietary Allowances (RDA) 2019.23 The questionnaire was conducted using the Nutrisurvey application (2005), which included Indonesian foods.24
The following categorizations were determined: for calorie intake, <2500 calories per day was low and ≥2500 calories per day was average; for protein intake, <60 grams per day was low and ≥60 grams per day was average; for carbohydrate intake, <400 grams per day was low and ≥400 grams per day was average; for fat intake, <65 grams per day was low and ≥65 grams per day was average; for fiber intake, <25 grams per day was low and ≥25 grams per day was average; and for vitamin D intake, <15 micrograms per day was low and 15 micrograms per day was average.23,24
Ethics Approval and Consent to Participate
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all methods/procedures involving research study participants were registered with ClinicalTrials.gov (NCT04650308) with a registration date of November 18, 2020. This study was also approved by the Universitas Sumatera Utara Ethical Committee. This research procedure and protocol were approved by the Research Ethics Committee of the University of North Sumatra, Indonesia, with the certificate number: No. 61/KEP/USU/2020. All participants knowingly consented to participate in this study; the research subjects read the explanation about the research and indicated their willingness to take part by signing an informed consent form.
Results
This study included 136 research subjects, with primary data collected including the characteristics of the research subjects and data on the history of obesity in parents and adolescence. Anthropometric data were used for direct anthropometric measurements and assessments for food intake data were performed by interviewing the research subjects. In addition, an assessment of food intake was carried out with the help of food models and pictures of food ingredients to help research subjects remember the amount of food consumed.
Table 1 shows the basic characteristics of the research subjects, with the highest percentage for age being those in the 41–50 years group (32.4%). The youngest participant in this study was 20 years old, and the oldest was 58 years old. The distribution of sex was almost evenly distributed between men and women, although the percentage of women was slightly higher than that of men. The distribution of those working as housewives was found to be higher than other occupations, and the lowest percentage was working as a teacher. Most of the research subjects had a Senior High School education; only a small proportion had achieved a master’s degree (Table 1).
 |
Table 1 Socio-Demographic Data of All Subjects |
Table 2 shows the distribution of the research subjects with the global WHO obesity body mass index criterion of 30 kg/m2, according to which as many as 11% were obese. Table 2 shows that based on the abdominal circumference criteria, the female group was included in the category with an abdominal circumference of more than 80 cm (50%). In contrast, a low percentage was found for an abdominal circumference of less than 90 cm in the male group. Abdominal circumference was moderately correlated with body mass index (p=0.001, r: 0.419) through Pearson’s analysis.
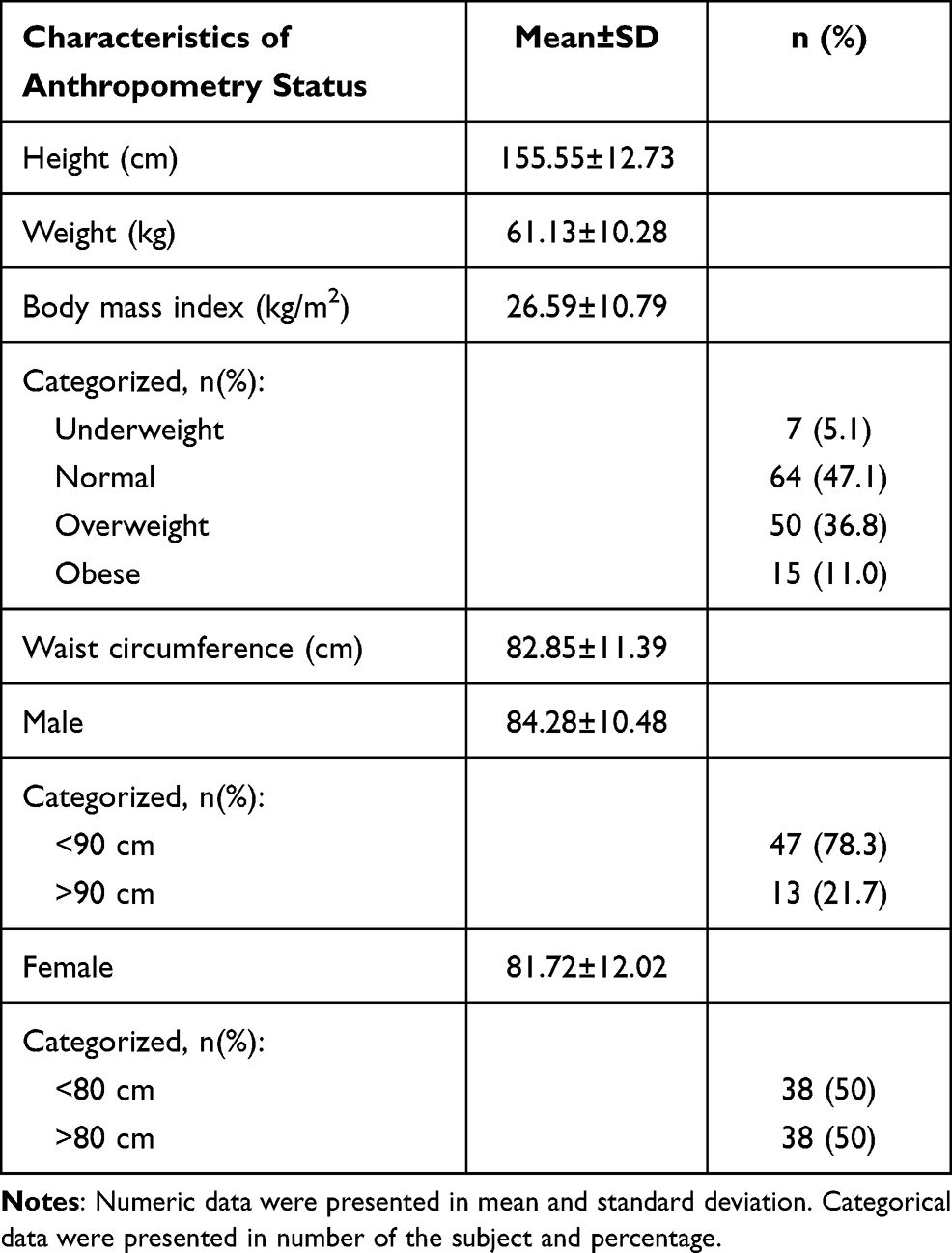 |
Table 2 Characteristic Data of the Subjects Based on Anthropometry Status |
The daily food intakes are shown in Table 3. This information indicates that the intakes of energy, fat, protein, carbohydrates, and fiber are not correlated with the recommended nutritional adequacy rate. Regarding vitamin D intake, most of the study subjects reported a more than healthy intake per day (51.5%). All study subjects reported a carbohydrate intake of fewer than 400 grams per day, which was very low. There was no correlation between whole food intake and body mass index.
 |
Table 3 Characteristic Data of the Subjects Based on Nutrient Intake |
Table 4 reports significant relationships between a history of obesity in adolescence and a history of obesity in parents, with the criteria for obesity of weighing over 30 kg/m2. This study indicates that there is a significant relationship between obesity in adolescence and parents with an incidence of adult obesity. The high body mass indexes (obesity criterion of more than 30 kg/m2) indicate that the probability factor had no relationship between a history of obesity in adolescence and parents with incidences of adult obesity was less than 5%, and the result is significant. This significance showed more value in maternal and paternal obesity history compared to the history of obesity in adolescence.
 |
Table 4 Association Between Parental and Adolescent’s History of Obesity and Adulthood Obesity |
Female research subjects exhibited significant relationships with a history of maternal, paternal and adolescent obesity (p=0.001, p=0.001, and p=0.027, respectively); the association with maternal obesity was highly significant. At the same time, male research subjects showed a significant relationship with a history of paternal obesity (p=0.03), whereas a history of maternal obesity and adolescence did not reveal significant relationships (p=0.631 and p= 0.247, respectively).
Discussion
This study explored the relationships between a history of obesity in adolescence, as well as mothers and fathers with a history of adult obesity. Based on the results of this study, the main findings were: (1) there is a significant relationship between a history of obesity in adolescence, a history of obesity in the father, and a history of obesity in the mother and an incidence of adult obesity in the subject; and (2) histories of obesity in the mother, father, and in adolescence revealed a significant relationship in female subjects, but only father’s obesity history revealed an association in male subjects.
Previous research has shown that parental obesity is a predictor of childhood overweight.20,25–27 The family risk ratio contributing to childhood obesity is when one parent reaches >2.5.5,17 Birth weight is characterized by 30% genetic heritability; this effect is significant, based on the genetic influences of the mother and father.4,5,17,28,29 However, obesity genes, or so-called obesogenic genes, that mothers and fathers inherit are predictors of obesogenic behavior in an obesogenic environment.5 This study also presents a relationship between a history of obesity in parents and obesity in adulthood, although it was found that food intake was no more than the recommended daily nutritional adequacy rate.
Calorie intake for participants in this study revealed an intake of fewer than 2500 calories per day. The percentage of obesity in adulthood was still found; a history of obesity in parents and obesity in adolescence may influence this. This study found that a person is born carrying the obesity gene from his parents, from the father, the mother, or both. The magnitude of the influence of one parent being obese is 40%, and 80% if both are obese.4
This study shows that the influence of a history of maternal obesity in women is more significant than that of father obesity or adolescent obesity. Meanwhile, in males, it is the history of father obesity which is relevant. There is no effect on the history of maternal obesity and childhood obesity. These findings are necessary as factors that must be understood and addressed, especially when dealing with cases of obesity in women and men. Previous research only assigned a relationship between the likelihood of a person being obese based on a history of obesity in parents but did not differentiate between men and women.19,20,25,30
Furthermore, the obesity gene is influenced by an obesogenic environment; however, most critical is the parents’ role in passing on the obesity gene and raising the child in an obesogenic environment until they enter adolescence. If obesity develops in adolescence, the likelihood of becoming obese in adulthood will be greater. For this reason, understanding the relationship between these factors must be properly considered so that obesity prevention programs can be successful.
Previous research has stated that mothers play a role in obesity in adolescence through the intake of fast foods, and fat intake plays a role in obesity in boys independent of physical activity.2,4,5,12 Furthermore, discussions on this matter have been developed by other researchers, who stated that there was a close relationship between childhood obesity and adult obesity.3 This risk factor can be prevented through behavior modifications and clinical therapy. A healthy lifestyle needs to be maintained in the family and community; this needs to be applied to reduce the prevalence of childhood obesity and its effects in adulthood.
Another important effect is the occurrence of cardiovascular disease, which increases morbidity and mortality.6,7,9,20 Obese children may have risk factors detrimental to cardiovascular health with cardiovascular comorbidities such as dyslipidemia, which manifests as an increase in low-density lipoprotein (LDL) levels.2,3,6 Previous studies have also reported a direct relationship between body mass index and cardiovascular disease.18,28,31 Abdominal circumference (central obesity) is not only related to body mass index; it also influences the occurrence of metabolic disorders, which are related to the occurrence of type 2 diabetes mellitus.6,12 The epidemic of childhood obesity has been linked with an increase in the prevalence of coronary artery disease in young and middle-aged adults.3,6,31 It is estimated that the prevalence of coronary artery disease could increase by 5–16% by 2035.3,31
This study had some bias, which was interview bias in nutrient assessment analyses, although food models were used and a nutritionist interviews the study subjects. This could have reduced the bias in this study. This study also had limitations, namely, not performing obesity gene examinations, which would have provided a more meaningful insight. In addition, this study did not examine excess fat mass. Therefore, this study could only identify significant relationships and could not establish a relationship with deeper discussions of the factors involved.
Conclusions
This study found a significant relationship between a parent’s history of obesity, adolescent obesity, and the incidence of adult obesity (≥30 kg/m2). In women, the factors related to the incidence of adult obesity were a history of maternal obesity and adolescence. However, in men, the factor associated with an incidence of adult obesity was a history of paternal obesity. Therefore, obesity risk factors can be used to understand the prevention of obesity in order to reduce the overall incidence of the condition.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Acknowledgments
We would like to thank the local government of North Sumatera and Universitas Sumatera Utara for the grants.
Author Contributions
All authors made a significant contribution to this study, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; the drafting, revising or critically reviewing of the article; giving final approval of the version to be published; agreeing on the journal to which the article has been submitted; and agreeing to be accountable for all aspects of the work.
Funding
This project was funded, in part, by the Lembaga Penelitian Universitas Sumatera Utara according to TALENTA Universitas Sumatera Utara, year 2020, no. 4142/UN5.1.R/PPM/2020, date: 27 April 2020.
Disclosure
The authors report no conflicts of interest or financial interest in this work.
References
1. WHO. Obesity; 2021, Available from: https://www.who.int/health-topics/obesity#tab=tab_1.
2. Meyer JF, Larsen SB, Blond K, et al. Associations between body mass index and height during childhood and adolescence and the risk of coronary heart disease in adulthood: a systematic review and meta-analysis. Obes Rev. 2021:e13276. doi:10.1111/obr.13276
3. Raghuveer G. Lifetime cardiovascular risk of childhood obesity. Am J Clin Nutr. 2010;91(5):1514S–1519S. doi:10.3945/ajcn.2010.28701D
4. Nguyen V, Enette Larson D, Rachel K, et al. Fat intake and adiposity in children of lean and obese parents. Am J Clin Nutr. 1995;63:507–513. doi:10.1093/ajcn/63.4.507
5. Bouchard C. Childhood obesity: are genetic differences involved? Am J Clin Nutr. 2009;89(5):1494S–1501S. doi:10.3945/ajcn.2009.27113C
6. Yayun L, Yang H, Zhiyue X, et al. Association Between Different Obesity Patterns and the Risk of Developing Type 2 Diabetes Mellitus Among Adults in Eastern China: a Cross-Sectional Study. Diabetes Metab Syndrome Obesity. 2021;14:2631–2639. doi:10.2147/DMSO.S309400
7. Ziser K, Decker S, Stuber F, et al. Barriers to Behavior Change in Parents With Overweight or Obese Children: a Qualitative Interview Study. Front Psychol. 2021;12:631678. doi:10.3389/fpsyg.2021.631678
8. Shen C, Zhou Z, Lai S, et al. Urban-rural-specific trend in prevalence of general and central obesity, and association with hypertension in Chinese adults, aged 18–65 years. BMC Public Health. 2019;19:661. doi:10.1186/s12889-019-7018-4
9. Hou X, Liu Y, Huijuan L, et al. Ten-year changes in the prevalence of overweight, obesity and central obesity among the Chinese adults in urban Shanghai, 1998–2007 — comparison of two cross-sectional surveys. BMC Public Health. 2013;13:1064–1072. doi:10.1186/1471-2458-13-1064
10. WHO. The Asia-Pacific perspective: redefining obesity and its intervention. Health Communications Australia Pte Limited. Australia; 2000. Available from: http://wwwdiabetes.com.au/pdf/obesity_report.pdf.
11. RI K. RISKESDAS 2018: Laporan Provinsi Sumatera Utara. Medan, North Sumatra: Lembaga Penerbit Balitbangkes; 2019.
12. Niu J, Seo DC. Central obesity and hypertension in Chinese adults: a 12-year longitudinal examination. Prev Med. 2014;62:113–118. doi:10.1016/j.ypmed.2014.02.012
13. Du T, Sun X, Yin P, et al. Increasing trends in central obesity among Chinese adults with normal body mass index, 1993–2009. Pediatr Diabetes. 2013;13:327–335. doi:10.1186/1471-2458-13-327
14. Arsenault LN, Xu K, Taveras EM, et al. Parents’ obesity-related behavior and confidence to support behavioral change in their obese child: data from the STAR study. Acad Pediatr. 2014;14(5):456–462. doi:10.1016/j.acap.2014.03.001
15. Rodriguez-Moran M, Guerrero-Romero F, Aradillas-Garcia C, et al. Obesity and family history of diabetes as risk factors of impaired fasting glucose: implications for the early detection of prediabetes. Pediatr Diabetes. 2010;11:331–336. doi:10.1111/j.1399-5448.2009.00590.x
16. Romero-Ibarguengoitia ME, Vadillo-Ortega F, Caballero AE, et al. Family history and obesity in youth, their effect on acylcarnitine/aminoacids metabolomics and non-alcoholic fatty liver disease (NAFLD). Structural equation modeling approach. PLoS One. 2018;13:e0193138. doi:10.1371/journal.pone.0193138
17. Lee JH, Reed DR, Price RA. Familial risk ratios for extreme obesity: implications for mapping human obesity genes. Int J Obes Relat Metab Disord. 1997;21(10):935–940. doi:10.1038/sj.ijo.0800498
18. Gunnell DJ, Frankel SJ, Nanchahal K, et al. Childhood obesity and adult cardiovascular mortality: a 57-y follow-up study based on the Boyd Orr cohort. Am J Clin Nutr. 1998;67(6):1111–1118. doi:10.1093/ajcn/67.6.1111
19. Corica D, Aversa T, Valenzise M, et al. Does Family History of Obesity, Cardiovascular, and Metabolic Diseases Influence Onset and Severity of Childhood Obesity? Front Endocrinol (Lausanne). 2018;9:187. doi:10.3389/fendo.2018.00187
20. Sull JW, Kim S, Jee SH. Effects of Obesity and Family History of Diabetes on the Association of CETP rs6499861 with HDL-C Level in Korean Populations. J Lipid Atheroscler. 2019;8:252–257. doi:10.12997/jla.2019.8.2.252
21. Chung CJ, Huang YG. Predictive factors for accuracy of perception of parents regarding their overweight or obese children in Taiwan. Asia Pac J Clin Nutr. 2016;25:571–577. doi:10.6133/apjcn.092015.18
22. Davidson K, Vidgen H. Why do parents enrol in a childhood obesity management program?: a qualitative study with parents of overweight and obese children. BMC Public Health. 2017;17(1):159. doi:10.1186/s12889-017-4085-2
23. RI PMK. Angka Kecukupan Gizi bagi Bangsa Indonesia. Indonesia KKR, editor. Jakarta: Kementerian Kesehatan RI; 2019. 33.
24. Erhardt DJ. Nutrition Surveys and Calculation. Gross, Dr. Rainer; 2010.
25. Cederberg H, Stancakova A, Kuusisto J, et al. Family history of type 2 diabetes increases the risk of both obesity and its complications: is type 2 diabetes a disease of inappropriate lipid storage? J Intern Med. 2015;277(5):540–551. doi:10.1111/joim.12289
26. Reuter CP, Burgos MS, Bernhard JC, et al. Association between overweight and obesity in schoolchildren with rs9939609 polymorphism (FTO) and family history for obesity. J Pediatr (Rio J). 2016;92(5):493–498. doi:10.1016/j.jped.2015.11.005
27. Manios Y, Moschonis G, Karatzi K, et al. Large proportions of overweight and obese children, as well as their parents, underestimate children’s weight status across Europe. The ENERGY (EuropeaN Energy balance Research to prevent excessive weight Gain among Youth) project. Public Health Nutr. 2015;18(12):2183–2190. doi:10.1017/S136898001400305X
28. Baker JL, Olsen LW, Sorensen TI. Childhood body-mass index and the risk of coronary heart disease in adulthood. N Engl J Med. 2007;357:2329–2337. doi:10.1056/NEJMoa072515
29. Must A, Jacques PF, Dallal GE, et al. Long-term morbidity and mortality of overweight adolescents. A follow-up of the Harvard Growth Study of 1922 to 1935. N Engl J Med. 1992;327(19):1350–1355. doi:10.1056/NEJM199211053271904
30. Saunders TJ, Tremblay MS, Mathieu ME, et al. Associations of sedentary behavior, sedentary bouts and breaks in sedentary time with cardiometabolic risk in children with a family history of obesity. PLoS One. 2013;8:e79143. doi:10.1371/journal.pone.0079143
31. Bibbins-Domingo K, Coxson P, Pletcher MJ, et al. Adolescent overweight and future adult coronary heart disease. N Engl J Med. 2007;357(23):2371–2379. doi:10.1056/NEJMsa073166
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.