")
Back to Journals » Infection and Drug Resistance » Volume 16
The in vitro Activity of Echinocandins Against Clinical Trichophyton rubrum Isolates and Review of the Susceptibility of T. rubrum to Echinocandins Worldwide
Authors Su H , Jiang W, Verweij PE, Li L, Zhu J, Han J, Zhu M, Deng S
Received 29 June 2023
Accepted for publication 12 August 2023
Published 18 August 2023 Volume 2023:16 Pages 5395—5403
DOI https://doi.org/10.2147/IDR.S423735
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Huilin Su,1– 3,* Weiwei Jiang,4,* Paul E Verweij,3,5 Li Li,2 Junhao Zhu,2 Jiande Han,1 Min Zhu,2 Shuwen Deng6
1Department of Dermatology, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China; 2Department of Dermatology, Huashan Hospital, Fudan University, Shanghai, People’s Republic of China; 3Department of Medical Microbiology and Center of Expertise in Mycology, Radboud University Medical Center, Nijmegen, the Netherlands; 4Department of Dermatology, Hospital affiliated to the 72nd Army of Chinese PLA, Huzhou, People’s Republic of China; 5Department of Medical Microbiology and Center of Expertise in Mycology, CWZ Hospital, Nijmegen, the Netherlands; 6Department of Medical Microbiology, The People’s Hospital of SND, Suzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuwen Deng, Department of Medical Microbiology, The People’s Hospital of SND, Suzhou, People’s Republic of China, Email [email protected] Min Zhu, Department of Dermatology, Huashan Hospital, Fudan University, Shanghai, People’s Republic of China, Email [email protected]
Introduction: The emergence of resistance in Trichophyton rubrum to azoles and terbinafine has become increasingly evident in recent years, necessitating the development of novel antifungal drugs and the exploration of new indications for existing agents.
Methods: In this study, we retrospectively evaluated the in vitro antifungal activity of 3 echinocandins (anidulafungin, caspofungin, and micafungin) against 73 clinical isolates of T. rubrum collected from a teaching hospital in Shanghai, China, using EUCAST E.DEF 9.3.1 with minor modification. We also reviewed the susceptibility of T. rubrum to echinocandins globally by literature searching.
Results: Our findings revealed that micafungin exhibited the lowest modal minimum effective concentration (MEC) value (0.08 mg/L, n = 28) and the lowest geometric mean (GM) MEC value (0.014 mg/L) among the 73 isolates of T. rubrum tested, followed by anidulafungin with a modal MEC value of 0.016 mg/L (n = 67) and a GM of 0.018 mg/L. Caspofungin displayed a higher modal MEC value of 0.5 mg/L (n = 35) and a GM of 0.308 mg/L. Despite variations in methodologies, similar results were obtained from the review of five relevant studies included in our analysis.
Discussion: Echinocandins exhibited excellent in vitro activity against T. rubrum isolates, with micafungin and anidulafungin demonstrating greater potency than caspofungin. These findings suggest that echinocandins could be considered as potential treatment options for managing recalcitrant dermatophytoses resulting from the emergence of resistance. However, it is important to note that the clinical efficacy of these in vitro findings has yet to be established and warrants further investigation.
Keywords: echinocandins, Trichophyton rubrum, antifungal activity, review
Introduction
Dermatomycosis is a prevalent superficial fungal infection primarily affecting keratinized tissues, including the skin, hair, and nails, with a remarkably high incidence rate of 20–25%.1 Dermatophyte species are the most common causative agents of dermatomycosis. Of the more than 40 dermatophyte species infecting humans, Trichophyton rubrum is the most common species,2 although there has been a rise in infections caused by the Trichophyton indotineae in Trichophyton mentagrophytes/Trichophyton interdigitale complex in India.3,4 Generally, dermatophytosis is easily cured with a wide range of topical and oral antifungal drugs. Azoles and allylamines are the primary recommended topical and systemic agents for treating T. rubrum infections. Terbinafine, renowned for its clinical efficacy, is the most commonly prescribed drug against Trichophyton species due to its fungicidal properties.5 However, since the first reported case of T. rubrum resistance to terbinafine in 2003,6 reports of T. rubrum resistance to antifungal agents have been increasing in the Americas, Europe, and Asia.7–9 Several studies have demonstrated that T. rubrum can develop resistance to terbinafine, azoles, and amorolfine after prolonged exposure to sub-inhibitory concentrations of these drugs.6–12 An epidemiological study conducted in India reported a remarkably high frequency of terbinafine-resistant T. rubrum strains, reaching 44% (8 out of 18 isolates).13 A review encompassing 26 global studies on T. rubrum susceptibility revealed that 15 studies (57.69%) exhibited a terbinafine geometric mean above 0.03 mg/L (the epidemiological cut-off value), indicating the presence of non-wildtype T. rubrum strains with potential pandemic characteristics.14 In India, T. indotineae in T. mentagrophytes/T. interdigitale complex replaces T. rubrum as the most common skin infection in the last decade.15 Notably, the highest resistance rates of the T. indotineae have been observed in northern India, with a terbinafine resistance rate of 76% (MIC ≥0.5 mg/L).13 T. indotineae appears to be spreading towards Europe and other Asian countries.15 Therefore, the development of new antifungal drug classes is crucial in overcoming the existing and future challenges in managing dermatophyte infections.
Echinocandins are lipopeptides derived from the fermentation broths of various fungi, which have been synthetically modified. These compounds act by inhibiting the synthesis of cell wall β-1,3-glucan.16 Echinocandins have been approved for invasive aspergillosis and candidiasis. Echinocandins generally exhibit fungistatic and fungicidal activities against Aspergillus and Candida species, respectively.17,18 Echinocandins have also shown in vitro activity against dermatophytes but reports on clinical use are lacking;19 however, the data on the antifungal efficacy of echinocandins to dermatophytes in vitro are limited.19–23 In this study, we aimed to evaluate the potency of echinocandins (anidulafungin, caspofungin and micafungin) against a large set of clinical T. rubrum isolates collected from China and review the existing literature on in vitro susceptibility of echinocandins against clinical isolates of T. rubrum worldwide.
Materials and Methods
T. rubrum Isolates and Identification
A total of 73 clinical isolates of Trichophyton rubrum were collected from patients diagnosed with dermatophytosis between 2014 and 2018 at Huashan Hospital, Fudan University in Shanghai, China. The diagnosis of dermatophytosis was established through a combination of clinical presentation and mycological examination:24 (a) the presence of skin lesions indicative of dermatophytosis; (b) positive direct microscopy demonstrating the presence of hyphae in the specimen; and (c) positive culture of dermatophytes.
The 73 clinical T. rubrum isolates were identified using morphological features and subsequently confirmed by sequencing the ITS gene as described previously.25 Isolates information and GenBank accession numbers for the generated ITS sequences of the 73 T. rubrum isolates are listed in Table S1.
Antifungal Susceptibility Testing
In vitro antifungal susceptibility testing of the 73 isolates of T. rubrum was performed according to the EUCAST E.DEF 9.3.1 (https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/AFST/Files/EUCAST_E_Def_9_3_1_Mould_testing__definitive.pdf) and adjusted part of the parameters for dermatophytes. The isolates were subcultured on potato dextrose agar and incubated at 28°C for 7 days or longer to sporulate sufficiently. Cover colonies with sterile water supplemented with 0.1% Tween-20. Then, the culture was gently swabbed with a cotton tip and the conidia are transferred with a pipette to a sterile tube. After vortexed, the suspension was counted with a haemocytometer chamber and checked the no presence of hyphae. If a significant number of hyphae is detected, transfer the suspension to the filter to remove hyphae and yield a suspension composed of conidia. The suspension is then diluted with sterile distilled water to obtain a final working inoculum of 2–5 × 105 CFU/mL. Anidulafungin and caspofungin were purchased from Sigma-Aldrich (MO, USA). Micafungin was bought from Toronto Research Chemicals (Toronto, Canada). The testing range for micafungin was 0.002 to 2 mg/L; for anidulafungin and caspofungin were both 0.016 to 16 mg/L. Vortex the inoculum suspension and inoculate each well of a microdilution plate with 100μL of the conidial suspension. Panels were incubated at 28°C for 4–5 days. MECs were first read at 4 days incubation. The final results were determined when the control well got sufficient growth. The MEC denotes the lowest echinocandin concentration at which the fungus displayed growth retardation and/or microscopic morphological changes in contrast to the control well. There are no clinical breakpoints available for all these drugs yet. Candida parapsilosis ATCC 22019 and C. krusei ATCC 6258 were used as the quality control strains. The original antifungal susceptibility testing data are listed in Table S1.
Literature Review
Literature searching was carried out in databases including PubMed, Scopus, and Web of Science. We retrieved the papers using the terms “(Trichophyton rubrum) AND (echinocandins OR anidulafungin OR caspofungin OR micafungin)” in the title and abstract.
Results
Table 1 lists the MEC ranges, geometric mean (GM), modal MEC, and MEC distribution of three echinocandins against 73 clinical T. rubrum isolates tested in this study. Figure 1 shows the modal MEC and MEC distribution of three echinocandins against 73 clinical T. rubrum isolates tested in this study. The MEC ranges of micafungin, anidulafungin and caspofungin were 0.002–0.063 mg/L, 0.016–0.063 mg/L and 0.031–1 mg/L, respectively. Micafungin had the lowest modal MEC (0.008mg/L, n = 28) and MECs geometric mean (GM) (0.014 mg/L), followed by anidulafungin (modal MEC 0.016mg/L, n = 67, GM 0.018 mg/L) and caspofungin (modal MEC 0.5mg/L, n = 35, GM 0.308 mg/L) against all T. rubrum isolates tested.
 |
Table 1 MEC Ranges, GM, Modal MEC, and MEC Distribution of 3 Echinocandins Against 73 Clinical T. rubrum Isolates from China |
 |
Figure 1 MEC distribution of 3 echinocandins against 73 clinical T. rubrum isolates from China. |
The literature review resulted in 5 publications reporting the susceptibility of T. rubrum to echinocandins worldwide from 2013 to 202219–23 (Table 2, Figure 2). Table 2 summarizes the susceptibility data of T. rubrum isolates to echinocandins based on the 5 publications and the results of our study. Of all 6 studies, our study included the largest set of T. rubrum isolates (73 isolates) and 3 echinocandins (micafungin, anidulafungin, caspofungin), the rest of the studies tested sample sets varying from 7 to 43 isolates of T. rubrum, and 4 literatures involved only two echinocandins. The methods used in all 6 studies included Clinical and Laboratory Standards Institute (CLSI) M38-A2, European Committee on Antimicrobial Susceptibility Testing (EUCAST), modified EUCAST, and E-Test. The culture mediums for T. rubrum were mainly potato dextrose agar (PDA) and oatmeal agar (OA). Only the modified method in Rissleger’s study used Sabouraud −2% glucose agar (SAB) to get fragmented mycelium for inoculum preparation. The incubation temperature was 28°C in Aktas’s study using the E-test method.20 Similarly, in our study, we utilized the modified EUCAST method and maintained the incubation temperature at 28°C. Rissleger’s study adopted a slightly higher temperature of 30°C while using the modified EUCAST method.22 In the remaining studies, the incubation temperature was set at 35°C. The incubation period varied from 2 to 9 days.
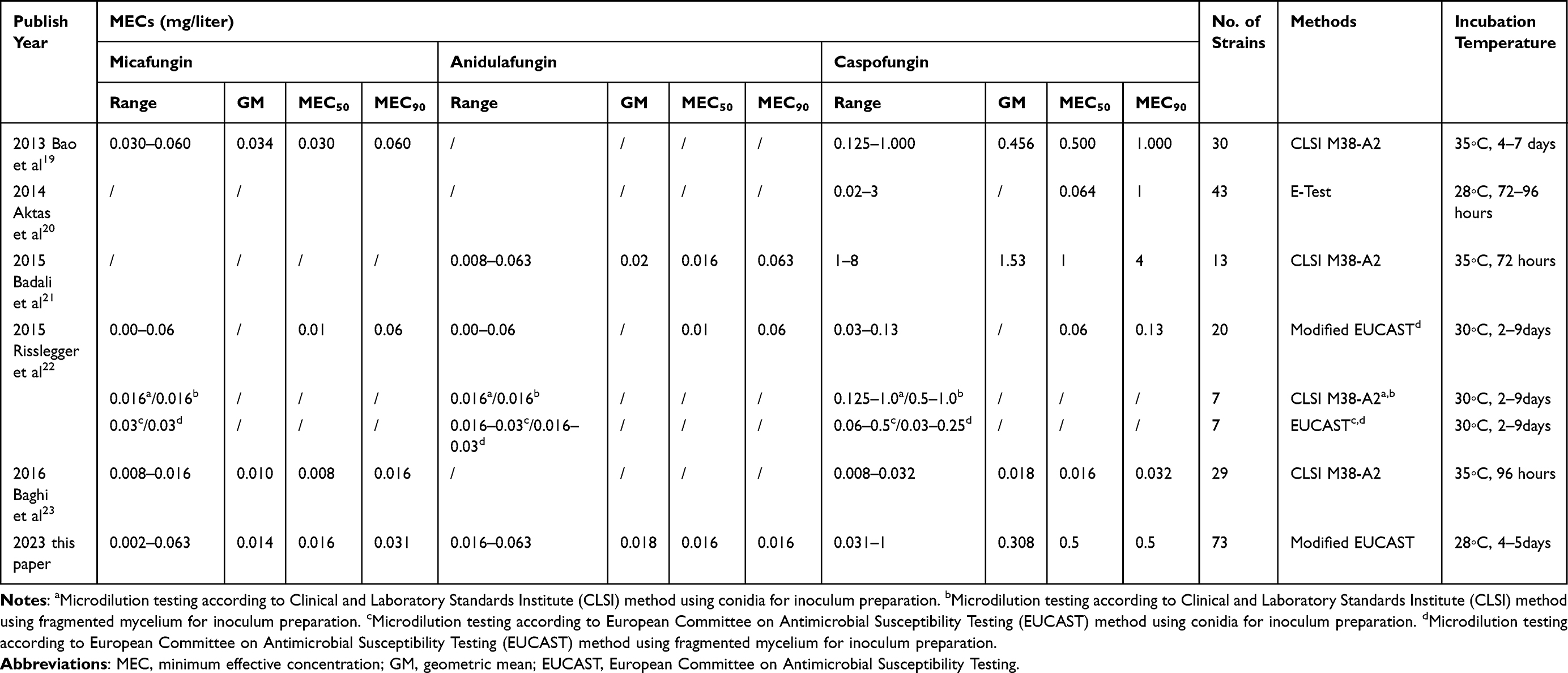 |
Table 2 Summarized Data of the 6 Studies on Susceptibility of T. rubrum to Echinocandins |
 |
Figure 2 Summarized data of 6 studies on antifungal susceptibility of T. rubrum to echinocandins. |
Caspofungin is the most common echinocandin tested for the activity against T. rubrum in all 6 studies. MEC ranges and GM, MEC90 values are variable in different studies, with the highest MEC range (1–8mg/L) in Badali et al’s study and the lowest MEC range (0.008–0.032mg/L) in Baghi et al’s study (Table 2, Figure 2).21,23
Micafungin exhibited the lowest MEC value with MIC value relatively consistent (GM varying from 0.010 to 0.034 mg/L, MIC90 from 0.016 to 0.06mg/L) among 4 studies in which Micafungin was included (Table 2, Figure 2).
Only 3 studies reported the activity of anidulafungin against T. rubrum. Generally, anidulafungin exhibited a similar MEC range (0.008–0.063mg/L) among 3 studies although small samples were tested in studies by Badali et al and Rissleger et al.21,22 However, there are two diluted steps difference for MIC90 value (0.016mg/L) of anidulafungin against T. rubrum in our results compared to those in the other two studies (MIC90, 0.063mg/L) (Table 2, Figure 2).
Discussion
Echinocandins are a class of antifungal drugs with milder side effects compared to polyenes and azoles, since these agents only inhibit the fungal-specific metabolic pathway—β-(1,3)-glucan biosynthesis.26 Caspofungin acetate was the first synthesized echinocandin and then approved for clinical use by the US Food and Drug Administration (FDA) in 2001, followed by micafungin in 2005 and anidulafungin in 2006. Because of the good drug safety, echinocandins were even approved for the treatment of children over 3 months of age and there is no need to adjust the dose in renal or hepatic insufficient patients.27 The FDA has approved the indications of echinocandins in the empirical treatment of febrile neutropenia, Candida infections, invasive aspergillosis in refractory patients, or intolerant to other therapies.
However, the antifungal susceptibility profile of dermatophytes to echinocandins remains poorly examined. Among 5 literatures reviewed and our results (Table 2, Figure 2) in this study,19–23 the activity of caspofungin against T. rubrum was tested in all 6 studies, whereas micafungin was tested in 4 studies, and anidulafungin only in 3 studies. Most studies are with a limited sample set of T. rubrum isolates (7–43 isolates) except our study with 73 isolates of T. rubrum.
Though there are no reference breakpoints of echinocandins to T. rubrum available at the moment, in our study, three echinocandins tested showed good activity against the 73 clinical T. rubrum isolates in this collection, while micafungin and anidulafungin showed a lowest modal MEC of 0.008 mg/L (n = 28) and 0.016 mg/L (n = 67), respectively, followed by caspofungin with modal MEC of 0.5 mg/L (n = 35) (Table 1, Figure 1). Micafungin and anidulafungin appeared more potent than caspofungin against T. rubrum, and similar results have been achieved in other studies.19–23
Baghi et al23 tested in vitro activity of caspofungin and anidulafungin against clinical dermatophyte isolates using CLSI M38A2, both echinocandins demonstrated potent activities against dermatophyte isolates, the MEC50, MEC90, and GM values of caspofungin and anidulafungin against 29 isolates of T. rubrum tested in the study by Baghi et al were similar to those reported in our study (Table 2, Figure 2). Badali et al21 presented in vitro susceptibility patterns of clinically important Trichophyton and Epidermophyton species against nine antifungal drugs including caspofungin and anidulafungin using CLSI M38A2, caspofungin exhibited higher MEC value (GM 1.67mg/L, MEC90 4mg/L) against Trichophyton and Epidermophyton species, the GM, MEC90 of caspofungin against 13 T. rubrum isolates tested in the study were 1.53mg/L and 4 mg/L, respectively. Nevertheless, anidulafungin exhibited potent in vitro antifungal activity against all dermatophyte isolates (GM, 0.06mg/L) and excellent activity for T. rubrum as well (GM, 0.02mg/L). Bao et al19 tested the potency of micafungin and caspofungin against dermatophyte isolates from China using CLSI M38-A2. Both caspofungin and micafungin exhibit good in vitro antifungal activity in most dermatophytes compared with the traditional antifungal agents (terbinafine). The GM, MEC90 values of micafungin and caspofungin to 30 isolates of T. rubrum tested are similar to those in our study. In addition, the E-test method was used to investigate the in vitro activity of caspofungin against 43 isolates of T. rubrum in Aktas’s study20 and caspofungin exhibited as an active agent with a MEC range of 0.02–3mg/L for T. rubrum. Rissleger et al22 evaluated the modified EUCAST fragmented-mycelium inoculum method for in vitro susceptibility testing of dermatophytes and the activity of novel antifungal agents including 3 echinocandins. Consistency between the mycelial inoculum method and the CLSI broth microdilution method was high (93% to 100%). Echinocandins showed good activity against all tested dermatophytes and worked as the most effective agents against dermatophytes compared with other drugs like voriconazole, posaconazole, fluconazole, and amphotericin B. All the MEC values of caspofungin, micafungin and anidulafungin for T. rubrum isolates tested in the study are comparable to those in other studies (Table 2, Figure 2).
There are certain limitations in this study. As this work had been done before EUAST method for the susceptibility testing of dermatophytes was launched.28 We followed the EUCAST E.DEF 9.3.1 edition with minor modification on incubation temperature and time for dermatophytes. Of note, the EUCAST method for dermatophytes28 was mainly validated for terbinafine, voriconazole, itraconazole and amorolfine against T. rubrum and T. interdigitale, however, the susceptibility testing of dermatophytes to echinocandins is observed with MEC which is not included in the EUCAST method for dermatophytes yet.28 The standard protocol on the susceptibility testing of dermatophytes to echinocandins is needed urgently.
Overall, micafungin and anidulafungin exhibited a low MEC range (both 0.008–0.063 mg/L) to T. rubrum which are similar among those studies,19,21–23 relatively higher MEC values for caspofungin to T. rubrum isolates were observed in 5 studies despite different methods and culture mediums when compared with those for anidulafungin and micafungin (Table 2, Figure 2), which indicated that micafungin and anidulafungin have better activity than caspofungin against T. rubrum. Micafungin has stronger in vitro antifungal activity than caspofungin in our study and also other research19 (Table 2, Figure 2). Echinocandins generally exhibit fungistatic and fungicidal activities against Aspergillus and Candida species, respectively.29 Comparing the in vitro potency of echinocandins to Aspergillus fumigatus, anidulafungin and micafungin were also the most active drugs against A. fumigatus in vitro with the lowest modal MICs/MECs (0.016mg/L, n = 61 and 0.031mg/L, n = 64, respectively), followed by caspofungin (0.25mg/L, n = 119) when compared with azoles and AmB in our previous study,30 and similar results reported by our previous study.31
Conclusion
Our study provided evidence of the good potency of micafungin, anidulafungin and caspofungin against T. rubrum in vitro based on our results and review of the data published on the susceptibility of T. rubrum to echinocandins worldwide. These findings suggest that echinocandins could be considered as potential treatment options for recalcitrant dermatophytoses infected by resistant dermatophytes. However, further clinical investigations must be conducted for the in vivo efficacy of echinocandins for the treatment of dermatophytosis caused by T. rubrum.
Ethics Approval
The study was approved by the Ethics Committee of Fudan University School of Medicine (20151010A330). All methods were performed in accordance with the relevant guidelines and regulations. Written informed consent was obtained from individual or guardian participants.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, interpretation, or all these areas, took part in drafting, revising, or critically reviewing the article, gave final approval to the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This study was funded by the National Natural Science Foundation of China (82102417, 82273544), and Grants from the Science and Technology Commission of Shanghai Municipality (22Y11905600), Suzhou Bureau of Science and Technology (SKY2022037) and the People’s Hospital of SND (SGY2019D02).
Disclosure
Huilin Su and Weiwei Jiang are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Havlickova B, Czaika VA, Friedrich M. Epidemiological trends in skin mycoses worldwide. Mycoses. 2008;51(Suppl 4):2–15. doi:10.1111/j.1439-0507.2008.01606.x
2. White TC, Findley K, Dawson TL
3. Singh A, Masih A, Khurana A, et al. High terbinafine resistance in Trichophyton interdigitale isolates in Delhi, India harbouring mutations in the squalene epoxidase gene. Mycoses. 2018;61(7):477–484. doi:10.1111/myc.12772
4. Tang C, Kong X, Ahmed SA, et al. Taxonomy of the Trichophyton mentagrophytes/T. interdigitale species complex harboring the highly virulent, multiresistant genotype T. indotineae. Mycopathologia. 2021;186(3):315–326. doi:10.1007/s11046-021-00544-2
5. Gupta AK, Foley KA, Versteeg SG. New antifungal agents and new formulations against dermatophytes. Mycopathologia. 2017;182(1–2):127–141. doi:10.1007/s11046-016-0045-0
6. Mukherjee PK, Leidich SD, Isham N, Leitner I, Ryder NS, Ghannoum MA. Clinical Trichophyton rubrum strain exhibiting primary resistance to terbinafine. Antimicrob Agents Chemother. 2003;47(1):82–86. doi:10.1128/aac.47.1.82-86.2003
7. Schøsler L, Andersen LK, Arendrup MC, Sommerlund M. Recurrent terbinafine resistant Trichophyton rubrum infection in a child with congenital ichthyosis. Pediatr Dermatol. 2018;35(2):259–260. doi:10.1111/pde.13411
8. Suzuki S, Mano Y, Furuya N, Fujitani K. Discovery of terbinafine low susceptibility Trichophyton rubrum strain in Japan. Biocontrol Sci. 2018;23(3):151–154. doi:10.4265/bio.23.151
9. Salehi Z, Shams-Ghahfarokhi M, Razzaghi-Abyaneh M. Antifungal drug susceptibility profile of clinically important dermatophytes and determination of point mutations in terbinafine-resistant isolates. Eur J Clin Microbiol Infect Dis. 2018;37(10):1841–1846. doi:10.1007/s10096-018-3317-4
10. Osborne CS, Hofbauer B, Favre B, Ryder NS. In vitro analysis of the ability of Trichophyton rubrum to become resistant to terbinafine. Antimicrob Agents Chemother. 2003;47(11):3634–3636. doi:10.1128/aac.47.11.3634-3636.2003
11. Hryncewicz-Gwóźdź A, Kalinowska K, Plomer-Niezgoda E, Bielecki J, Jagielski T. Increase in resistance to fluconazole and itraconazole in Trichophyton rubrum clinical isolates by sequential passages in vitro under drug pressure. Mycopathologia. 2013;176(1–2):49–55. doi:10.1007/s11046-013-9655-y
12. Ghelardi E, Celandroni F, Gueye SA, et al. Potential of Ergosterol synthesis inhibitors to cause resistance or cross-resistance in Trichophyton rubrum. Antimicrob Agents Chemother. 2014;58(5):2825–2829. doi:10.1128/aac.02382-13
13. Ebert A, Monod M, Salamin K, et al. Alarming India-wide phenomenon of antifungal resistance in dermatophytes: a multicentre study. Mycoses. 2020;63(7):717–728. doi:10.1111/myc.13091
14. Jiang Y, Luo W, Verweij PE, et al. Regional differences in antifungal susceptibility of the prevalent dermatophyte Trichophyton rubrum. Mycopathologia. 2021;186(1):53–70. doi:10.1007/s11046-020-00515-z
15. Uhrlaß S, Verma SB, Gräser Y, et al. Trichophyton indotineae-an emerging pathogen causing recalcitrant dermatophytoses in India and worldwide-a multidimensional perspective. J Fungi. 2022;8(7). doi:10.3390/jof8070757
16. Cappelletty D, Eiselstein-McKitrick K. The echinocandins. Pharmacotherapy. 2007;27(3):369–388. doi:10.1592/phco.27.3.369
17. Pappas PG, Kauffman CA, Andes DR, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the infectious diseases society of America. Clin Infect Dis. 2016;62(4):e1–e50. doi:10.1093/cid/civ933
18. Patterson TF, Thompson GR 3rd, Denning DW, et al. Practice guidelines for the diagnosis and management of Aspergillosis: 2016 update by the infectious diseases society of America. Clin Infect Dis. 2016;63(4):e1–e60. doi:10.1093/cid/ciw326
19. Bao YQ, Wan Z, Li RY. In vitro antifungal activity of micafungin and caspofungin against dermatophytes isolated from China. Mycopathologia. 2013;175(1–2):141–145. doi:10.1007/s11046-012-9571-6
20. Aktas AE, Yigit N, Aktas A, Gozubuyuk SG. Investigation of in vitro activity of five antifungal drugs against dermatophytes species isolated from clinical samples using the E-Test Method. Eurasian J Med. 2014;46(1):26–31. doi:10.5152/eajm.2014.05
21. Badali H, Mohammadi R, Mashedi O, de Hoog GS, Meis JF, de Hoog GS. In vitro susceptibility patterns of clinically important Trichophyton and Epidermophyton species against nine antifungal drugs. Mycoses. 2015;58(5):303–307. doi:10.1111/myc.12315
22. Risslegger B, Lass-Flörl C, Blum G, Lackner M. Evaluation of a modified EUCAST fragmented-mycelium inoculum method for in vitro susceptibility testing of dermatophytes and the activity of novel antifungal agents. Antimicrob Agents Chemother. 2015;59(6):3675–3682. doi:10.1128/aac.04381-14
23. Baghi N, Shokohi T, Badali H, et al. In vitro activity of new azoles luliconazole and lanoconazole compared with ten other antifungal drugs against clinical dermatophyte isolates. Med Mycol. 2016;54(7):757–763. doi:10.1093/mmy/myw016
24. Moriarty B, Hay R, Morris-Jones R. The diagnosis and management of tinea. BMJ. 2012;345(jul10 1):e4380. doi:10.1136/bmj.e4380
25. Su H, Packeu A, Ahmed SA, et al. Species distinction in the Trichophyton rubrum complex. J Clin Microbiol. 2019;57(9). doi:10.1128/JCM.00352-19
26. Szymański M, Chmielewska S, Czyżewska U, Malinowska M, Tylicki A. Echinocandins - structure, mechanism of action and use in antifungal therapy. J Enzyme Inhib Med Chem. 2022;37(1):876–894. doi:10.1080/14756366.2022.2050224
27. Chen SC, Slavin MA, Sorrell TC. Echinocandin antifungal drugs in fungal infections: a comparison. Drugs. 2011;71(1):11–41. doi:10.2165/11585270-000000000-00000
28. Arendrup MC, Kahlmeter G, Guinea J, Meletiadis J. How to: perform antifungal susceptibility testing of microconidia-forming dermatophytes following the new reference EUCAST method E.Def 11.0, exemplified by Trichophyton. Clin Microbiol Infect. 2021;27(1):55–60. doi:10.1016/j.cmi.2020.08.042
29. Cantón E, Pemán J, Hervás D, Espinel-Ingroff A. Examination of the in vitro fungicidal activity of echinocandins against Candida lusitaniae by time-killing methods. J Antimicrob Chemother. 2013;68(4):864–868. doi:10.1093/jac/dks489
30. Deng S, Ansari S, Ilkit M, et al. In vitro antifungal susceptibility profiles of 12 antifungal drugs against 55 Trichophyton schoenleinii isolates from Tinea Capitis Favosa Patients in Iran, Turkey, and China. Antimicrob Agents Chemother. 2017;61(2). doi:10.1128/AAC.01753-16
31. Su H, Zhu M, Tsui CK, et al. Potency of olorofim (F901318) compared to contemporary antifungal agents against clinical Aspergillus fumigatus isolates, and review of azole resistance phenotype and genotype epidemiology in China. Antimicrob Agents Chemother. 2021;65(5). doi:10.1128/AAC.02546-20
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.