")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
The Implications of the Pandemic with Covid-19 in the Glycemic Control of People with Type 2 Diabetes
Authors Gherbon A , Frandes M , Nicula-Neagu M , Timar R , Timar B
Received 14 September 2023
Accepted for publication 7 December 2023
Published 15 December 2023 Volume 2023:16 Pages 4109—4118
DOI https://doi.org/10.2147/DMSO.S434990
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Adriana Gherbon,1– 3 Mirela Frandes,4 Marioara Nicula-Neagu,5 Romulus Timar,1– 3 Bogdan Timar1– 3
1Department VII Internal Medicine - Diabetes, Nutrition, Metabolic Diseases and Systemic Rheumatology, “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania; 2Centre of Molecular Research in Nephrology and Vascular Disease, “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania; 3Department of Diabetes, Nutrition, and Metabolic Diseases, “Pius Brinzeu” Emergency Hospital, Timisoara, Romania; 4Department of Functional Sciences - Biostatistics and Medical Informatics, “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania; 5Banat’s University of Agricultural Sciences and Veterinary Medicine “King Michael I of Romania”, Timisoara, Romania
Correspondence: Mirela Frandes, Department of Functional Sciences - Biostatistics and Medical Informatics, “Victor Babes” University of Medicine and Pharmacy, 2 Eftimie Murgu Sq, Timisoara, 300041, Romania, Email [email protected]
Introduction: The COVID-19 lockdown influenced the glycemic control and other metabolic parameters in people with type 1 and 2 diabetes mellitus.
Objective: To study the effects of COVID-19 lockdown on glycemic control in people with type 2 diabetes mellitus (T2DM).
Material and Methods: Our study group included 120 Romanian people with T2DM from both urban and rural areas. We employed a structured questionnaire with multiple-choice to collect data about DM management during lockdown, the interaction with their diabetologist, the access to treatment, and what other factors influenced their DM management during the lockdown.
Results: We did not observe an increase of numbers of hyper or hypoglycemia during the restriction period in people with T2DM. The number of glycemic imbalances was higher in people treated with insulin than those with oral antidiabetics (OAD) (p=0.003, X2=8.91). Regarding the causes of imbalances, we did not obtain a significant difference during the restriction period, neither between patients following treatment with insulin nor with OAD. On the contrary, we observed that only 26.7% of people with T2DM managed to maintain their weight or lost weight vs 73.3% patients who gained several extra kg (p< 0.001, X2=52.26).
Conclusion: The findings of this study have demonstrated that in people with T2DM, the COVID-19 lockdown determines better glycemic control among patients treated with OAD compared to those treated with insulin therapy. Anxiety, stress, and emotions were the main reasons that led to the increase in glycemic values of these patients. Also, most patients have gained weight either due to lack of physical activity or due to stress.
Keywords: type 2 diabetes, COVID-19, lockdown, diabetes management, body mass index
A Letter to the Editor has been published for this article.
Introduction
Type 2 diabetes mellitus (T2DM) is the most common type of diabetes, accounting for over 90% of all diabetes worldwide. Its prevalence is rising from an estimated 537 million adults aged 20–79 years worldwide (10.5% of all adults in this age group) in 2030, 643 million, and in 2045, 783 million adults aged 20–79 years are projected to have type 2 diabetes. Thus, while the world’s population is estimated to grow by 20% over this period, the number of DM is estimated to increase by 46%.1
T2DM is partly caused, maintained, and worsened by preventable risk factors such as physical inactivity, unhealthy diet, obesity, and smoking. For many patients, lifestyle modification may be the most effective intervention. In addition, lifestyle changes after a diagnosis of T2DM reduce the risk of cardiovascular and other adverse events.2
COVID-19 (Coronavirus disease 2019) is a pathology of a viral nature caused by a coronavirus associated with severe acute respiratory syndrome (SARS), appearing for the first time in December 2019 in Wuhan, China.3 The disease is highly contagious, spreading rapidly throughout the world, and the virus responsible for it is part of the coronavirus family, which causes a variety of diseases, some even more severe but rare, such as SARS and Middle East Respiratory Syndrome (MERS).4 Also, different studies that use large cohorts highlighted that SARS-CoV-2 infection is linked to a substantially increased risk of developing a diverse spectrum of new-onset autoimmune diseases.5
In general, people with DM have a higher risk of developing complications from infections, especially viral ones. In addition, a series of aggressive factors act on the human body, such as chemicals, pollution, infections, etc.6 DM is one of the most important risk factors in COVID-19 infection.7,8 However, compliance with the treatment determines better control, decreases the risk of complications, and a longer survival.
In Romania, various restrictions were imposed during the pandemic to limit the spread of COVID-19 infections. These had consequences on people with T2DM, such as limited access to the healthcare system, interaction with their diabetologist, access to treatment, and physical exercise. In the literature, previous studies have shown different results regarding the impact of the COVID-19 lockdown on glycemic control and medication adherence in people with T2DM.9,10 In some studies, the lockdown period was associated with worsening glycemic control,9 while in other studies, there was no difference in medication fills or glycemic control pre-pandemic and during the pandemic period.10 In other studies, physical inactivity is associated with a relatively higher risk of hospitalization for COVID-19, suggesting that physical inactivity may also increase hospitalizations due to COVID-19.11
This paper aims to observe how the COVID-19 pandemic influenced the glycemic control of people diagnosed with T2DM and how they were affected by the pandemic and the restrictions in the health field.
Materials and Methods
Study Design and Patients
The study was carried out between January and February 2022; 120 people took part in it: patients with T2DM, volunteers, female (95) and male (25), from all over the country, aged between 24 and 85 years old, users of basal-bolus regimen or oral antidiabetics.
Our study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the “Pius Brinzeu” Emergency Hospital Ethics Committee, Timisoara. All patients included in the study signed an informed consent.
The inclusion criteria in the study were
- people with T2DM in treatment with different types of oral antidiabetics drugs or with insulin therapy.
The exclusion criteria from the study were
- people with type 1 diabetes;
- pregnant or lactating T2DM people;
- the presence of mental illness.
For this non-interventional, retrospective observational study (case-control), a questionnaire with grid-type questions and several answer options was used. We chose this method since, given the restrictions imposed, we considered it a much more accessible way to contact T2DM people.
Compliance with medication was measured as the proportion of days covered (PDC) by medication one year before and after the index date. PDC was calculated as number of days people have access to treatment in the specified time interval divided by number of days in a specified time interval (one year pre- and post-index date).12 A compliance threshold of ≥0.8 was set to classify individuals as compliant, while those with a value <0.8 were categorized as non-compliant.
Questionnaire
The questionnaire was published online using the Google Forms program. It consisted of questions regarding blood glucose values, hypoglycemia, hyperglycemia episodes, glycosylated hemoglobin value, ways of accessing medical services, and how people with T2DM contacted the diabetologist. The questionnaire was anonymous, and the answers were strictly confidential.
The questionnaire includes questions related to HbA1c and glycemic values measured by people with T2DM during the pandemic to analyze their glycemic control objectively. The questionnaire also included questions about hypoglycemic episodes and the HbA1c value to see if the pandemic affected how patients maintained their glycemic values within normal limits. The obtained values were then compared with the criteria corresponding to hypoglycemia and diabetic ketoacidosis, in accordance with the DM Management Guide developed by the National Society of Diabetes, Nutrition and Metabolic Diseases in Romania13 and American Diabetes Association (ADA).14
Other parameters used were demographic data (gender, origin, age), type of medication, and meal patterns. We considered a meal irregular when food was eaten in varying amounts throughout the day and at different times from one day to the next. We also included in questions about communication methods with the diabetologist, how they benefited from health services during the pandemic, how they were able to manage episodes of hyperglycemia and hypoglycemia, physical activity performed and weight maintenance.
The Timisoara County Emergency Hospital Research Committee approved the questionnaire for use with the Romanian population (see Appendix).
Statistical Analysis
We used the Excel program was used to export the obtained data from the questionnaire, for which we created two tables (people with T2DM treated only with oral antidiabetics and people with T2DM with basal bolus insulin therapy). These data were then statistically analyzed (the percentage calculation of the variables was performed and then compared with the x2 test) using the EpiInfoTM software (v 7.2 CDC).
The value of p was calculated for each individual parameter, and the following rules were applied: if p>0.05, there were no significant differences between the groups, if p<0.05, than it meant that there were significant differences between the groups, if p<0.01 we considered that there were very large differences between patient groups, and if p<0.001 it resulted that there were extremely large differences between the 2 groups of T2DM people.
The odds ratio (OR) was also calculated, and the following were found:
- OR > 1 it is considered that the lockdown affected the level of glycemic control in people with T2DM;
- OR = 1, it is considered that the pandemic did not influence the glycemic control of people with T2DM;
- OR < 1 it is considered that the risk factor had a protective level.
To compare the differences, we used the x2 tests, and its value was calculated with the Epi InfoTM software (v 7.2 CDC).
Results
The study included 120 people with T2DM, 95 women (79.2%) and 25 men (20.8%) (p<0.001, X2=81.66), both from the urban environment (n=85, 70.8%) and from the rural (n=35, 29.2%) (p<0.001, X2=41.66), from the entire territory of the country.
The baseline characteristics of the studied group are listed in Table 1.
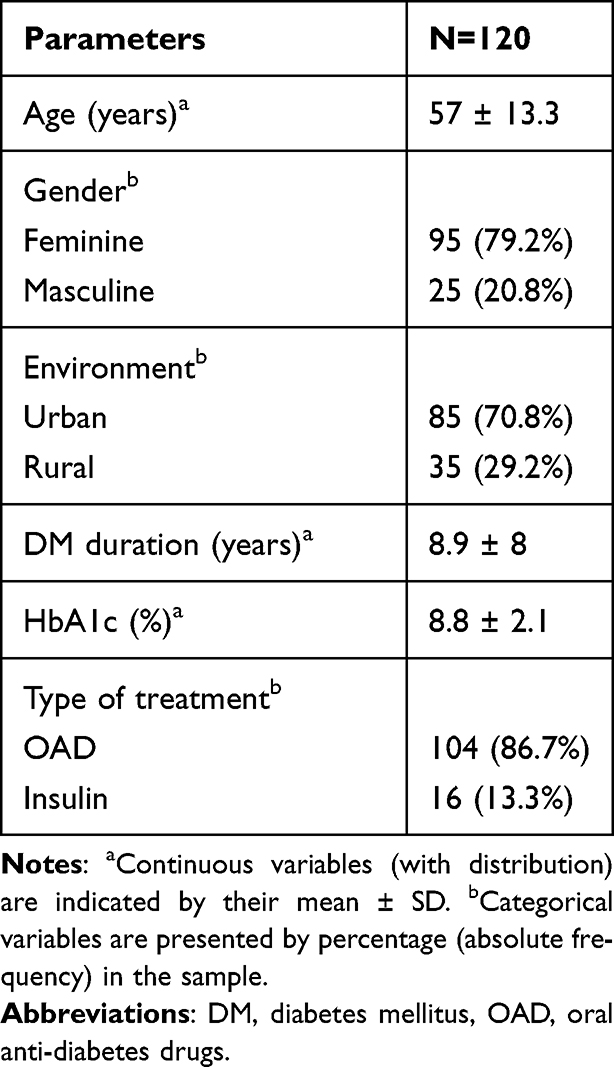 |
Table 1 Characteristics of the Studied Samp |
To analyze whether the people with T2DM had optimal control of their blood glucose values, they were asked if they noticed an increase in the number of episodes of hyperglycemia and if they recorded increases in blood glucose compared to the periods before the pandemic, as well as how they managed the episodes of hyperglycemia.
We observed that 89 T2DM people (74.2%) did not have more frequent episodes of hyperglycemia during the restriction period, and 31 (25.8%) claimed that they had more frequent episodes of hyperglycemia (p<0.001, X2=56.06).
Table 2 illustrates the responses of T2DM people in connection with the causes of episodes of hyperglycemia. Of these, the majority (n=70, 58.3%) believed that anxiety and stress due to the pandemic led to the occurrence of hyperglycemia episodes. In comparison, 15 (12.5%) claimed that they did not have access to the necessary treatment, 15 (12.5%) did not comply with the treatment, and 20 (16.7%) did not comply with the diet.
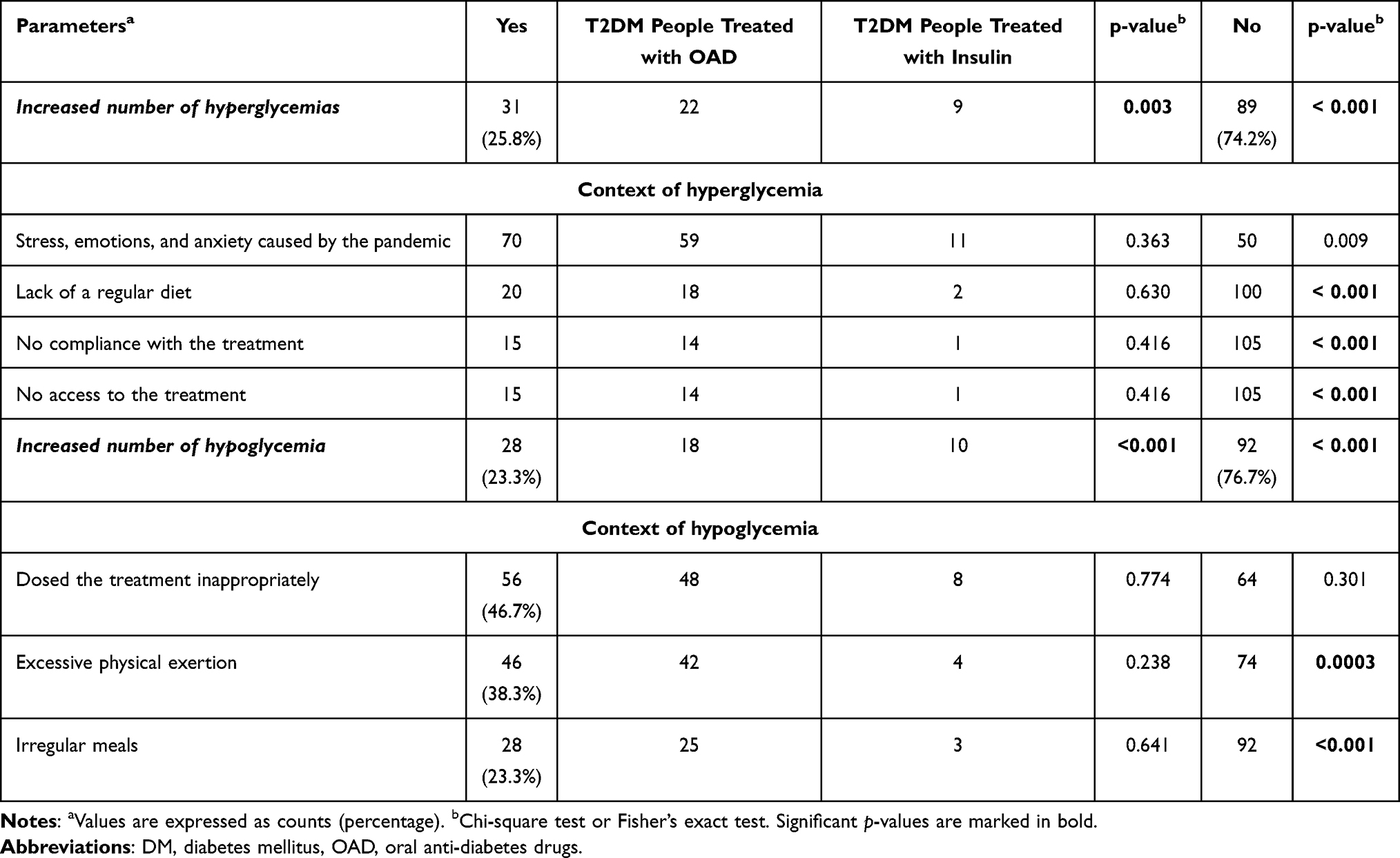 |
Table 2 Description of Hyperglycemic and Hypoglycemic Episodes Between Studied Groups of People Receiving OAD or Insulin Treatment |
To observe whether there was adequate control of the glycemic level of the T2DM people, we added questions regarding the glycosylated hemoglobin and the daily glycemic level to the questionnaire.
HbA1c values higher than 8% show inadequate glycemic control and require adjustment of the treatment dose. Of the T2DM people who responded to the questionnaire, 72 (60%) of them (65 with oral antidiabetic treatment and 7 with insulin therapy) maintained their blood glucose value within the limit of 126–250 mg/dl, 41 (34.2%) (35 with oral antidiabetic treatment and 6 with insulin therapy) within 250–300 mg/dl, respectively 7 (5.8%) (5 with oral antidiabetic treatment and 2 with insulin therapy) at values over 300 mg/dl (p<0.001, X2=106.96).
Regarding HbA1c, 26 T2DM people (21.5%) declared a value lower than 6.5, of which 3 required insulin therapy, 59 (49%) declared values of HbA1c between 6.5 and 8, 12 patients (10%) over 8, respectively 23 T2DM people (19.5%) did not measure their HbA1c during the pandemic (Table 3).
 |
Table 3 Glycemic Control in the Study Sample of People Receiving OAD or Insulin Treatment |
Good glycemic control is considered both in patients treated with oral antidiabetics and in patients treated with insulin.
Regarding episodes of hypoglycemia, 28 T2DM people (23.3%) confirmed that they had observed increases in episodes of hypoglycemia (of which 18 were treated with oral antidiabetics and 10 with insulin), compared to 92 of T2DM people (76.7%) who claim that the number of episodes of glycemia did not increase during the pandemic (p=0.003, X2=6.88).
We observed that 56 (46.7%) people with t2DM followed the treatment inappropriately, while for 46 (38.3%) people, the exaggerated physical effort led to a drop in blood sugar, and in 28 cases the schedule was not respected snacks and meals (23.3%). From this, it can be deduced that the inadequate dosage of the treatment was the main problem that led to the occurrence of hypoglycemic episodes among people with T2DM.
Due to travel restrictions and limited access to gyms, 19 (15.8%) people stated that they did not do sports during the pandemic, 16 (13.3%) people said that the imposed restrictions prevented them from perform physical exercises as before, 55 (45.8%) people continued to exercise at home in order to manage to maintain their glycemic values within normal limits and not to have to increase their treatment dose, respectively 30 (25%) of people stated that they did not report significant differences in terms of sports (35 T2DM people considered that their access to exercise was restricted vs 85 who continued to do sports) (p<0.001, X2=41.66).
Regarding the diet, 88 (73.3%) T2DM people stated that during the pandemic, they consumed a larger amount of food, and 21 (17.5%) did not notice a significant difference in diet. In comparison, 11 (9.2%) of them stated that the stress caused by the pandemic caused them to consume a smaller amount of food. Despite the recommendations to maintain a balanced lifestyle and keep glycemic values within normal limits, especially among T2DM people with comorbidities who could suffer complications following infection with COVID-19, only 32 T2DM people managed to maintain their weight or lose weight vs 88 T2DM people who gained several extra kg (the weight gain was between 4.25± 7.99 kg). In the studied T2DM people, during the pandemic, depending on the BMI value, the percentage of patients with degree III obesity increased from 7% to 10% of those with degree II obesity from 12% to 19% of those with degree I obesity from 35% to 37%, and overweight from 24% to 31%. We concluded that there is an extremely significant difference between the groups (p<0.001, X2=52.26).
Following the restrictions established during the pandemic, both trips to the medical office and the relationship with the diabetologist were made difficult, with doctors using the means of telephone or online communication to keep in touch with T2DM people.
We observed that 87 (72.5%) T2DM people stated that they had access to the health system, compared to 10 (8.3%) who considered that they did not have access to the health system, and 23 (19.2%) had a neutral opinion. A major disagreement can be observed (n=87, 72.5%) of T2DM people who considered that they had access to the health system, compared to another 10 (8.3%) who stated that they did not have access to the system of health (p<0.001, X2=122.24).
Significant disagreement can also be seen regarding access to treatment, with 75 (62.5%) disagreeing with the sentence “I did not have access to treatment as before the pandemic” compared to 24 (20%) who agreed with this statement (p<0.001, X2=52.54). We also find a major disagreement regarding communication with the diabetologist during the pandemic; 72 T2DM people (60%) say that they managed to communicate with the doctor, compared to 25 (20.8%) who did not keep in touch with him (p<0.001, X2=45.54). We can conclude that access to the health system, treatment, and communication with the diabetologist were not strongly influenced during the pandemic.
The T2DM people were also asked how they kept in touch with the diabetologist and how the control went during the pandemic. We observed that 32 (26.7%) T2DM people went to the office, 10 (8.3%) of them used online communication networks (WhatsApp, e-mail), and 78 (65%) talked with the diabetologist by phone. Regarding how the control proceeded, only 25 (20.8%) patients physically went to the consultation (in a private clinic, diabetes center or polyclinic), compared to them, 32 (26.7%) contacted the doctor only in case of emergency, when they failed to maintain their glycemic values within normal limits, 21 (17.5%) talked to the doctor by phone and 36 of them kept in touch with the doctor online to communicate glycemic values. Out of the total of 120 T2DM people, only 25 (20.83%) patients went to the physical consultation, the rest of the patients opting for the telephone or online consultation.
An essential factor in glycemic control is treatment compliance. Patients must be informed about the importance of following the treatment plan, especially since they did not have as regular check-ups as before during the pandemic. Of the 120 patients, 72 (60%) stated that they only sometimes complied with the treatment, unlike 48 (40%) who indicated that they followed exactly the treatment recommended by the diabetologist (p=0.001, X2=9.6).
Patients were also asked about their disease management during the pandemic and whether they felt it was more difficult to keep their blood glucose levels within normal limits throughout the restrictions. We observed that 20 (19.1%) of the 105 patients treated with oral antidiabetics believe that it was more difficult for them to manage their disease during the pandemic. In comparison, 85 (81%) of them believe that the pandemic did not it changed their disease management (p<0.001, X2=80.47).
Discussions
In our study, more episodes of hyperglycemia occurred during the pandemic compared to the pre-pandemic period. Stress and anxiety were the leading cause of hyperglycemia among patients with T2DM. This was expected since hyperglycemia is caused by reduced glucose in muscle and increased glucose production in the liver, which are generated by the action of stress hormones such as glucagon and epinephrine during glycogenolysis and gluconeogenesis.
Reports on glycemic control in people with T2DM during the COVID-19 pandemic were mixed. Studies from India,15 China,16 Korea17 and by another group in India18 showed worsening glycemic control due to psychological stress and difficulty in obtaining medication and medical advice under lockdown. In contrast, a separate study from India19 and one from Greece20 reported that glycemic control improved; nevertheless, it was reported as unchanged in studies from Italy21,22 and Turkey.23 Overall, these findings suggest that the impact of the COVID-19 pandemic on glycemic control differs depending on the type of diabetes mellitus and the region of the world.
A cross-sectional study suggests a positive association between COVID-19 anxiety and hyperglycemia, while the degree of anxiety is associated with an increased risk of hyperglycemia.24 Also, studies perform in Romania about glycemic control in patients with type 1 diabetes, respectively with type 1 diabetes and Graves-Basedow disease during the pandemic showed that stress, emotions, and anxiety were among the main reasons that led to increases in blood sugar levels, suggesting that the psychological impact may have long-term complications.25,26
People with COVID-19 treated with Metformin were reported to have better outcomes, including reduced mortality and lower levels of inflammation, in studies using univariate analyses27 and adjusted multivariable analyses.28 This was consistent with previous findings of Metformin’s anti-inflammatory properties, although improved outcomes related to COVID-19 were not found in every study. However, Metformin carries a known risk of lactic acidosis in critically ill patients, including patients with COVID-19.29
Some studies have reported that insulin use in patients with diabetes was associated with higher morbidity and mortality related to COVID-19.30 Patients on insulin therapy are more likely to have more severe diabetes and more extended hospital stays.31 In addition, glucose dysregulation and increasing insulin use are associated with a more severe form of COVID-19.32 Indeed, better glycemic control is associated with better outcomes related to COVID-19. In one study, insulin treatment was associated with reaching glycemic targets and improving outcomes related to COVID-19 in hospitalized patients with the disease.33 Another study from India showed a 0.51% increase in patients’ average HbA1c levels from an average of 7.92% pre-pandemic HbA1c to an average of 8.43% post-pandemic.15
According to the results obtained from the questionnaire, we observed in T2DM people an increase in weight during the quarantine period. This weight gain can be explained by the fact that the T2DM people did not have access to gyms and outdoor walks, but also by the fact that they were more anxious and consumed a larger amount of food. Weight gain is harmful for people with T2DM since it generally generates the presence of some comorbidities such as hypertension, ventilatory dysfunction, arthrosis, venous and lymphatic circulation diseases, depression, and others, which have a negative impact on health and increase morbidity and mortality.34 Moreover, the glucose level is influenced by the lack of exercise, which can cause muscle cells to lose their sensitivity to insulin.
A study conducted in India in 2020 showed that in people with T2DM, a trend toward weight gain was observed in 40% of the cohort, with 16% of the population experiencing a weight gain of 2.1–5 kg.35 When all risk parameters were analyzed together using the ADA risk engine, there was an increase in the ADA diabetes risk score in 7% of the population, with 6.7% in the high-risk group. There was further weight gain among the 3% of the people who were already obese at baseline.36
A study from Spain investigating the eating habits of T2DM patients during isolation reported that patients made efforts to improve their nutritional habits, with increased consumption of vegetables and reduced consumption of fast food, for example. However, that study also noted increased high carb snacking due to boredom, stress, and decreased physical activity.37
Another question in the questionnaire was related to managing the disease during the period of restrictions. It can be concluded that T2DM people treated with insulin therapy had more significant disease management problems compared to T2DM people treated with oral antidiabetics. Regarding access to treatment, during the restrictions, most T2DM people believed that they had no issues obtaining treatment and that the restrictions did not prevent them from maintaining adequate glycemic values.
In the world, patient adherence to medication is done through teleconsultation, and healthcare providers make sure that all diabetes patients have sufficient medication stocks and are prescribed enough medication because of limited access to clinics during the pandemic.38 The communication with the diabetologist occurred during the physical check-up (at the private clinic, outpatient clinic, or hospital), through online communication (WhatsApp, e-mail), and by phone. From the study data, the primary way T2DM people contacted the diabetologist was by telephone. Although electronic consultation has been widely advocated, other non-medical barriers, such as administrative support, must be overcome before this method can become a part of routine care. Online consultations and self-monitoring were mainly used. The experience of virtual care due to the pandemic can be transformed into an innovative solution for optimizing diabetes care and education after the disappearance of COVID-19 infection.39
Technologies are also likely less widely available or practical in many countries, such as Romania, which has a large population of people with DM.40 Governments need to invest in infrastructures to support telemedicine and alternative models of care.41 Access to the health system was satisfactory for most interviewed people. Even though video consultation confers an advantage over a telephone consultation, many people with DM prefer face-to-face attendance. People with DM are more interested in establishing relationships with clinicians, seeing who they are talking to, and having a better opportunity to ask questions.42,43
A limitation of this study is the small sample size; however, all the patients with T2DM were volunteers, and their computer literacy and internet competence conditioned their participation in the study. The strengths of our study include the novelty of the study design, being the first study that compares people with COVID-19 and T2DM treated with insulin or oral antidiabetic drugs.
Conclusions
Even if the restrictions of the pandemic limited the movement of T2DM people to the doctor’s office, they still benefited from access to treatment and health services. People with T2DM could communicate with the diabetologist via telemedicine, thus avoiding hospitals congestion and shortening the waiting time allocated to each patient.
Better glycemic control was observed among T2DM people treated with oral antidiabetics compared to those treated with insulin therapy. Anxiety, stress, and emotions were the main reasons that led to the increase in glycemic values of the T2DM people. Most of them have gained weight, either due to lack of physical activity or due to stress.
It was not necessary to increase the dose of oral antidiabetics and insulin; the leading causes that determined the appearance of hyperglycemia were a sedentary lifestyle, an unbalanced diet, and non-compliance with treatment. Inadequate treatment dosing was the main cause of most hypoglycemia, which was more common in people with T2DM treated with insulin compared to people treated with oral antidiabetics.
Acknowledgments
The authors would like to kindly thank to Dr. Denisa Balea for their help in data collection.
Consent for Publication
All participants signed a document of informed consent.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Magliano DJ, Boyko EJ. IDF Diabetes Atlas, 10th edition scientific committee . IDF DIABETES ATLAS [Internet]. 10th edition. Brussels: International Diabetes Federation; 2021. ISBN-13: 978-2-930229-98-0; 2021. Avaliable from: https://www.ncbi.nlm.nih.gov/books/NBK581934/.
2. Chong S, Ding D, Byun R, Comino E, Bauman A, Jalaludin B. Lifestyle changes after a diagnosis of type 2 diabetes. Diabetes Spectr. 2017;30(1):43–50. doi:10.2337/ds15-0044
3. Ciotti M, Ciccozzi M, Terrinoni A, Jiang WC, Wang CB, Bernardini S. The COVID-19 pandemic. Crit Rev Clin Lab Sci. 2020;57(6):365–388. doi:10.1080/10408363.2020.1783198
4. Stein SR, Ramelli SC, Grazioli A, et al. SARS-CoV-2 infection and persistence in the human body and brain at autopsy. Nature. 2022;612(7941):758–763. doi:10.1038/s41586-022-05542-y
5. Popoviciu MS, Kaka N, Sethi Y, Patel N, Chopra H, Cavalu S. Type 1 diabetes mellitus and autoimmune diseases: a critical review of the association and the application of personalized medicine. J Pers Med. 2023;13(3):422. doi:10.3390/jpm13030422
6. Nicula M, Pacala N, Stef L, et al. In vivo experiments of natural products protection of antagonistic effects of lead on iron. Rev Chim. 2017;68:12.
7. Gęca T, Wojtowicz K, Guzik P, Góra T. Increased risk of COVID-19 in patients with diabetes mellitus-current challenges in pathophysiology, treatment and prevention. Int J Environ Res Public Health. 2022;19(11):6555. PMID: 35682137; PMCID: PMC9180541. doi:10.3390/ijerph19116555
8. Sen S, Chakraborty R, Kalita P, Pathak MP. Diabetes mellitus and COVID-19: understanding the association in light of current evidence. World J Clin Cases. 2021;9(28):8327–8339. PMID: 34754842; PMCID: PMC8554438. doi:10.12998/wjcc.v9.i28.8327
9. Eberle C, Stichling S. Impact of COVID-19 lockdown on glycemic control in patients with type 1 and type 2 diabetes mellitus: a systematic review. Diabetol Metab Syndr. 2021;13(1):95. doi:10.1186/s13098-021-00705-9
10. Patel SY, McCoy RG, Barnett ML, Shah ND, Mehrotra A. Diabetes care and glycemic control during the COVID-19 pandemic in the United States. JAMA Intern Med. 2021;181(10):1412–1414. doi:10.1001/jamainternmed.2021.3047
11. Young DR, Sallis JF, Baecker A, et al. Associations of physical inactivity and COVID-19 outcomes among subgroups. Am J Prev Med. 2023;64(4):492–502. doi:10.1016/j.amepre.2022.10.007
12. Canfield SL, Zuckerman A, Anguiano RH, et al. Navigating the wild west of medication adherence reporting in specialty pharmacy. J Manag Care Spec Pharm. 2019;25(10):1073–1077. doi:10.18553/jmcp.2019.25.10.1073
13. Timar R, Roman G Ghid de management al diabetului zaharat elaborat de către societatea română de diabet, nutriție și boli metabolice și federația română de diabet, nutriție și boli metabolice [diabetes management guide developed by the Romanian society of diabetes, nutrition and metabolic diseases and the Romanian federation of diabetes, nutrition and metabolic diseases]; 2020.
14. American Diabetes Association. Standards of medical care in diabetes-2019. Diabetes Care. 2019;42:1.
15. Khare J, Jindal S. Observational study on effect of lock down due to COVID 19 on HBA1c levels in patients with diabetes: experience from Central India. Primary Care Diabetes. 2022;16(6):775–779. doi:10.1016/j.pcd.2020.12.003
16. Xue T, Li Q, Zhang Q, et al. Blood glucose levels in elderly subjects with type 2 diabetes during COVID-19 outbreak: a retrospective study in a single center. medRxiv. 2020;3:20048579.
17. Park SD, Kim SW, Moon JS, et al. on the changes in glycosylated hemoglobin level in people with type 2 diabetes mellitus. Diabet Metabol J. 2019;2020:1.
18. Khader MA, Jabeen T, Namoju R. A cross sectional study reveals severe disruption in glycemic control in people with diabetes during and after lockdown in India. Diabetes Metabol Synd. 2020;14(6):1579–1584. doi:10.1016/j.dsx.2020.08.011
19. Rastogi A, Hiteshi P, Bhansali A. Improved glycemic control amongst people with long-standing diabetes during COVID-19 lockdown: a prospective, observational, nested cohort study. Int J Diabetes Dev Count. 2020;40(4):476–481. doi:10.1007/s13410-020-00880-x
20. Psoma O, Papachristoforou E, Kountouri A, et al. Effect of COVID-19-associated lockdown on the metabolic control of patients with type 2 diabetes. J Diabetes Compl. 2020;34(12):107756. doi:10.1016/j.jdiacomp.2020.107756
21. Biancalana E, Parolini F, Mengozzi A, Solini A. Short-term impact of COVID-19 lockdown on metabolic control of patients with well-controlled type 2 diabetes: a single-centre observational study. Acta Diabetol. 2020;58(4):431–436. doi:10.1007/s00592-020-01637-y
22. Bonora BM, Morieri ML, Avogaro A, Fadini GP. The toll of lockdown against COVID-19 on diabetes outpatient care: analysis from an outbreak area in Northeast Italy. Diabetes Care. 2020;44(1):e18–e21. doi:10.2337/dc20-1872
23. Önmez A, Gamsızkan Z, Özdemir Ş, et al. The effect of COVID-19 lockdown on glycemic control in patients with type 2 diabetes mellitus in Turkey. Diabetes Metabol Synd. 2020;14(6):1963–1966. doi:10.1016/j.dsx.2020.10.007
24. Hikmah K, Helda H, Killeen C. Coronavirus-related anxiety with hyperglycemia in type 2 diabetes patients. Period Epidemiol J. 2022;10(2):111–120. doi:10.20473/jbe.V10I22022.111-120
25. Gherbon A, Frandes M, Timar R, Timar B. The impact of COVID-19 Lockdown on glycemic balance in Romanian patients with type 1 diabetes mellitus. Diabetes Metab Syndr Obes. 2022;Volume 15:3403–3413. doi:10.2147/DMSO.S386614
26. Gherbon A, Frandes M, Timar R. 637-P: the impact of the lockdown on Romanian patients with type 1 diabetes and Basedow-Graves’ disease. Diabetes. 2022;71(Supplement_1). doi:10.2337/db22-637-P
27. Chen Y, Yang D, Cheng B, et al. Clinical characteristics and outcomes of patients with diabetes and COVID-19 in association with glucose-lowering medication. Diabetes Care. 2020;43(7):1399–1407.
28. Cameron AR, Morrison VL, Levin D, et al. Anti-inflammatory effects of metformin irrespective of diabetes Status. CircRes. 2016;119(5):652–665.
29. Cheng X, Liu YM, Li H, et al. Metformin is associated with higher incidence of acidosis, but not mortality, in individuals with COVID-19 and Pre-existing type 2 diabetes. Cell Metab. 2020;32(4):537–547.e3. doi:10.1016/j.cmet.2020.08.013
30. Assaad M, Hekmat-Joo N, Hosry J, et al. Insulin use in type II diabetic patients: a predictive of mortality in covid-19 infection. Diabetol Metab Syndr. 2022;14(1):85. Erratum in: Diabetol Metab Syndr. 2022;14(1):98. doi:10.1186/s13098-022-00857-2
31. Dhatariya K, Corsino L, Umpierrez GE. Management of diabetes and hyperglycemia in hospitalized patients. In: Feingold KR, Anawalt B, Blackman MR, editors. Endotext. South Dartmouth (MA): MDText.com, Inc; 2000.
32. Mirabella S, Gomez-Paz S, Lam E, Gonzalez-Mosquera L, Fogel J, Rubinstein S. Glucose dysregulation and its association with COVID-19 mortality and hospital length of stay. Diabetes Metab Syndr. 2022;16(3):102439. doi:10.1016/j.dsx.2022.102439
33. Sardu C, D’Onofrio N, Balestrieri ML, et al. Outcomes in patients with hyperglycemia affected by COVID-19: can we do more on glycemic control? Diabetes Care. 2020;43(7):1408–1415. doi:10.2337/dc20-0723
34. Popoviciu M-S, Păduraru L, Yahya G, Metwally K, Cavalu S. Emerging role of GLP-1 agonists in obesity: a comprehensive review of randomised controlled trials. Int J Mol Sci. 2023;24(13):10449. doi:10.3390/ijms241310449
35. Zhang Y, Geng X, Tan Y, Li Q, Xu C, Xu J. New understanding of the damage of SARS-CoV-2 infection outside the respiratory system. Biomed Pharmacol. 2020;127. doi:10.1016/j.biopha.2020.110195
36. Ghosal S, Arora B, Dutta K, Ghosh A, Sinha B, Misra A. Increase in the risk of type 2 diabetes during lockdown for the COVID19 pandemic in India: a cohort analysis. Diabetes Metabol Synd. 2020;14(5):949–952. doi:10.1016/j.dsx.2020.06.020
37. Ruiz-Roso MB, Knott-Torcal C, Matilla-Escalante DC, Garcimartín A, Sampedro- Nuñez MA, Dávalos A. COVID-19 lockdown and changes of the dietary pattern and physical activity habits in a cohort of patients with type 2 diabetes mellitus. Nutrients. 2020;12(8):2327. doi:10.3390/nu12082327
38. Banerjee M, Chakraborty S, Pal R. Diabetes self-management amid COVID-19 pandemic. Diabetes Metab Syndr Clin Res Rev. 2020;14(4):351–354. doi:10.1016/j.dsx.2020.04.013
39. Khunti K, Aroda VR, Aschner P, et al. The impact of the COVID-19 pandemic on diabetes services: planning for a global recovery. Lancet Diabetes Endocrinol. 2022;10(12):890–900. PMID: 36356612; PMCID: PMC9640202. doi:10.1016/S2213-8587(22)00278-9
40. Chudasama YV, Gillies CL, Zaccardi F, et al. Impact of COVID-19 on routine care for chronic diseases: a global survey of views from healthcare professionals. Diabetes Metab Syndr. 2020;14(5):965–967. doi:10.1016/j.dsx.2020.06.042
41. Bullen C, McCormack J, Calder A, et al. The impact of COVID-19 on the care of people living with noncommunicable diseases in low- and middle-income countries: an online survey of physicians and pharmacists in nine countries. Prim Health Care Res Dev. 2021;22:e30.
42. Kilvert A, Wilmot EG, Davies M, Fox C. Virtual consultations: are we missing anything? Pract Diabetes. 2020;37(4):143–146. doi:10.1002/pdi.2288
43. Kilvert A, Fox C, Calladine L. What do people with diabetes really think about remote consultations. Pract Diabetes. 2020;38(4):51–56. doi:10.1002/pdi.2353
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.