Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Impact of Structured Kangaroo Care Education on Premature Infants’ Weight Gain, Breastfeeding and Length of Hospitalization in Malaysia
Authors Samsudin S, Chui PL ![]() , Ahmad Kamar A, Abdullah KL
, Ahmad Kamar A, Abdullah KL ![]() , Yu CW, Mohamed Z
, Yu CW, Mohamed Z
Received 30 December 2022
Accepted for publication 21 March 2023
Published 12 April 2023 Volume 2023:16 Pages 1023—1035
DOI https://doi.org/10.2147/JMDH.S403206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sharmiza Samsudin,1,2 Ping Lei Chui,1 Azanna Ahmad Kamar,3 Khatijah Lim Abdullah,4,5 Chye Wah Yu,2 Zainah Mohamed5
1Department of Nursing Science, Faculty of Medicine, Universiti Malaya, Kuala Lumpur, Malaysia; 2Faculty of Allied Health Professions, AIMST University, Bedong, Malaysia; 3Department of Paediatrics, Faculty of Medicine, Universiti Malaya, Kuala Lumpur, Malaysia; 4Department of Nursing, School of Medical and Life Sciences, Sunway University, Subang Jaya, Malaysia; 5Department of Nursing, Faculty of Medicine, Universiti Kebangsaan Malaysia, Bangi, Malaysia
Correspondence: Ping Lei Chui, Department of Nursing Science, Faculty of Medicine, University Malaya, Kuala Lumpur, Federal Territory of Kuala Lumpur, 50603, Malaysia, Tel +60127128893, Email [email protected]
Purpose: Kangaroo care is a complementary humanistic intervention based on a family-centered care model. This study investigated the effects of a locally contextualized, structured kangaroo care education program on weight gain, breastfeeding rate and length of hospitalization for premature infants.
Patients and Methods: This longitudinal quasi-experimental study with pre- and post-intervention design involved 96 infants born between 28 and 37 weeks of gestation for three months, and was carried out at a neonatal intensive care unit in Malaysia. The experimental group received a structured education program and careful monitoring of their kangaroo care practices, while the control group received routine care without a structured education program. The institutional review board approved the study design and registered at ClinicalTrials.gov (NCT04926402).
Results: The kangaroo care hours performed by mothers at baseline in the experimental and control group was 4.12 and 0.55 hours per week, respectively. At three months post-discharge, the experimental group had significantly higher weight gain, higher breastfeeding rates and shorter lengths of hospitalization than the control group.
Conclusion: A locally contextualized and structured kangaroo care education program is effective in the performance of kangaroo care. One hour per day of kangaroo care is positively associated with an extended period of breastfeeding, improved weight gain and shorter hospitalization of premature infants.
Keywords: premature infant, structured program, kangaroo mother care, length of hospital stay, body weight, breastfeeding
Introduction
Kangaroo care (KC), a humanistic technique, was developed in the late 1970s in Bogota, Colombia, as a solution to the neonatal intensive care unit (NICU) inability to maintain premature baby’s body temperatures when incubators were insufficient.1 This skin-to-skin contact allows the continuation of the parent’s warmth and love for the child, which is essential for the child’s growth.2 Due to the enormous advantages of KC in creating a balance of physiological indices and enhancing psychological status, its uniqueness has gained global acceptance.3 During KC, the infants are placed in an upright position against a parent’s bare chest to enable direct skin contact of the baby’s umbilicus to the sternum. The infants are covered during the care to keep warm and the maternal body heat helps control their body temperature.3 Since the introduction of KC, it has been proven that the level of care using this technique is comparable to incubator care.4 The KC method provides a biological environment to fulfill the infant’s needs for warmth and nutrition. It is based on a family-centered care model which promotes the mother’s role in the neonatal intensive care unit (NICU).5 This method fosters health and weight gain, promotes effective thermal control, increases breastfeeding rates, prevents infection and enhances bonding between mothers and infants.6,7
In premature infants, initiation of KC is vital during the critical period in which central nervous system development occurs, as this results in significant and long-lasting effects on brain function.8,9 It is observed that KC regulates body temperature, promotes daily weight gain, increases sleeping hours, balances physiological indexes, improves oxygen saturation levels and psychological status, reduces apnea and shortens hospital stays.10,11 A premature infant and mother’s bond is strengthened via KC, which boosts the mother’s self-esteem and increases milk production for breastfeeding. This reduces the premature infant’s pain reaction and associated behavioral issues.12–14 Its implementation significantly relieves NICU overcrowding and reduces the burden brought on by limited and costly resources like incubators. Furthermore, it also reduces neonatal infection and infant mortality rate.15 Previous studies have reported that KC also decreases the length of hospitalization.16–20
The survival of premature infants has improved due to the application of KC as a cost-effective and high-quality treatment.21 It was initially considered an accepted practice appropriate for resource-limited settings rather than a global standard of care.14 Nevertheless, some staffs and parents were resistant to integrating and sustaining KC into NICU practice despite knowing its benefits.22,23 The approach has not been wholly adopted as a routine practice in Malaysia and is still relatively new.23,24 The published data about the effects of conducting a KC education program on the outcomes of premature infants are lacking.22–26 Therefore, this study aims to evaluate the impact of a locally contextualized and structured kangaroo care education program on mothers’ breastfeeding rates, premature infants’ weight gain and the length of hospitalization of infants admitted to the NICU of a tertiary referral hospital in Malaysia. The findings of this study may enlighten mothers on the benefits of KC performance for premature infants.
Materials and Methods
This study was conducted between February 2018 and April 2019 at the NICU of a major tertiary teaching hospital in Kuala Lumpur, Malaysia. A longitudinal quasi-experimental research design was used with pre- and post-intervention. PS-Power software version 327 was used to calculate the sample size, which included a two-sample independent t-test of 0.05, an effect size of 0.22, and a power level of 0.80.28,29 The minimum required sample size for this study was 35 pairs per arm. After accounting for a 30% error rate, the final sample size for the control and experimental groups was 50 pairs. Furthermore, this study’s inclusion and exclusion criteria were considered for both premature infants and their mothers. Firstly, the premature infants’ mothers who gave birth between 28 and 37 weeks of gestation. The mothers must be at least 18 years old, literate and understand either basic Malay or English language. Besides that, infants’ mothers who gave birth at less than 28 weeks of gestation or older than 37 weeks were included in the exclusion criteria. Mothers with a history of medical or surgical conditions and under the influence of medications were excluded because it may interfere with breastfeeding. Moreover, mothers who had previously given birth to premature infants were also excluded from this study. Most importantly, this survey was conducted based on the mothers’ willingness.
In addition, the inclusion criteria for premature infants included babies with an Apgar score greater than 5, being admitted to NICU, isolated, clinically stable, having no congenital abnormality (could affect growth), non-vulnerable and free from the use of mechanical ventilation. Infants with surgical conditions, such as cleft lip, cleft palate, spina bifida, exomphalos (tummy wall defect) and omphalocele (belly wall defect) were excluded from this study. Ill Infants who have medical conditions with congenital abnormalities, umbilical artery catheter (UAC), umbilical vein catheter (UVC) were listed as exclusion criteria. These infants require prolonged phototherapy treatment and mechanical ventilator supports, which could interfere with KC performance.
The decision to perform KC relied on the degree of neurodevelopment and stability of the infants. The KC was initiated at 28 weeks of a premature infant.22,23 The researchers prospectively extracted data from the charts during clinical care in Level III NICUs, associated Level II units, and routine post-discharge care. Neonatal information includes Apgar score, sex, race, delivery type, birth weight, weekly weight, gestational age (weeks), respiratory supports (days), and KC performance at T1 while in the hospital. The measurements were taken based on 1 month (T2) and 3 months (T3) post-discharge breastfeeding, weight gain and KC performance.
One hundred infant-mother pairs who fulfilled the criteria were invited and consented to participate in the study. The control group (n = 50) were infant-mother pairs recruited between February 2018 and July 2018, while the experimental group (n = 50) were the pairs who were recruited between October 2018 and April 2019. The infant-mother pairs in the control group who provided consent were subjected to standard care according to the routine practice of the hospital during that period. The premature infants were managed in an incubator or under a radiant heater, naked except for a cap and diaper, or wrapped in a cloth. The mothers were allowed to touch, hold, and feed their premature infants. KC was performed at the convenience of nursing staff and parents in an unstructured manner (standard care). Information regarding KC was provided if the parent or nurse had initiated the discussion.
The experimental group also received standard routine care but underwent a structured maternal kangaroo care educational program (MKC-EP). The structured program consists of an hour of theoretical lecture (flipchart and video presentation) and a live mannequin demonstration of KC practice. Then, followed by practical sessions to provide knowledge and information on the necessary skills to perform KC and the provision of educational materials. There were also learning materials, such as a pamphlet containing KC performance and booklets for keeping track of the weight and feeding of the infants. The teaching contents were created based on existing guidelines and literature14,22,30 which were contextualized according to specific cultural norms. For instance, ensuring good modesty of the mothers and strict infection control were among the followed practices. Seven experts reviewed the provided materials and the adequacy of the KC steps. Two neonatologists with three nurses from the Neonatal Unit of the University Malaya Medical Center and two faculty members from the Nursing Department of the University of Malaya participated in the review to reach a final consensus on the appropriateness of the practice for the application in this study.
KC is best to provide an hour a day and seven days a week until discharge to obtain the desired physiological effects, brain development and maturation.22 A complete sleep cycle was defined as one hour per session (active, quiet and return to active sleep).22,23 The mothers in the experimental group were advised to perform the KC for at least 1 hour per day which total practice would be 4 to 5 hours per week23 beginning from NICU and continuing at home until the infant reached three months post-discharge. The suggested hours were based on a pilot study on 20 infant-mother pairs to confirm the proposed KC hours are applicable and feasible. KC was performed in response to the mother’s request, convenience and willingness as long as they can devote at least one hour per day anytime.23 The nurses checked the clinical conditions of the infants’ which included oxygen saturation, heart rate, bowel movements, urine output and feeding tolerance 10 minutes before the procedure to ensure the stability of infants to undergo KC.
The premature infants were naked except for wearing a diaper and a skullcap during the KC. A customized seamless tube top was provided that requires no buttons, buckles, zippers, velcro or ties to provide mothers a convenient way to feed their babies. This KC tube is simple to put on and take off, as it is breathable and lightweight. The KC tube is available in various sizes (S-3XL) and two colors (blue for boys and pink for girls), has no stress or pressure points, and allows for hands-free breastfeeding when in the KC position. The KC tube was secured, while the infant was placed in a prone, frog-leg position with the head turned sideways on the mother’s bare chest.22,23 Mothers can safely walk and move around with their baby supported in the KC tube, and also maximize skin contact between the infant and mother’s bare chest.22,23 Mothers were advised to wear a buttoned shirt ready to cover their arms and shoulders, followed by a light blanket over the infant. The dominant hand of the mother would support the infant at the buttocks while the non-dominant hand at the back of the head and between the scapulae to ensure comfort and security while maintaining proximity.23 The procedure can be conducted, while the infant receives other treatments such as oxygen supply via nasal prongs, intravenous fluids via peripheral venous cannula, gastric tube feeding, and intravenous medications. The infants were placed in an incubator or within a bassinet with an overhead radiant heater to ensure normothermia during other periods.
During this study, vital signs were examined 10 minutes before KC, 20 to 30 minutes during KC and 10 minutes after the completion of KC. A complete clinical examination was performed to prevent hypothermia and cold stress.31 Booklets about post-discharge were provided to assist in outcome documentation. The control group was required to document the number of times and type of feedings provided per day; the number of times and duration of KC if performed; and the baby’s growth parameters upon discharge from NICU at one month (44 weeks) and three months (52 weeks) from post-discharge. Besides, the experimental group was required to document the same with additional information on weight and temperature differences before, during and after the KC.
The discharge weights were measured using standardized weighing scales according to NICU, University Malaya Medical Centre discharge protocol. The infant’s weight was measured three times, which is on the day of discharge from NICU (T1), at 44 weeks (T2), and at 52 weeks (T3). The body weights of the preterm infants were documented after removing their clothes using a similar electronic weighing scale. The measurement was taken with an accuracy of 5g at least 2 hours after the last feed and twice a week on Tuesdays and Saturdays, according to the hospital protocol for weighing babies. The body weight was measured using a T-scale machine and recorded in grams (g). Upon discharge, the mothers were reminded to perform KC for a minimum of 1 hour per day and at least 4 to 5 hours weekly via a gentle short messaging system or WhatsApp reminders. The infant’s body weight was compared at various ages up to 52 weeks between the control and experimental groups using z-scores. Researchers determined the growth restriction portion as less weight based on indications between the 10th and 3rd percentiles.
As a result, the outcome variables measured included breastfeeding rates. Nutritional support data included the following: age at initiation of parenteral and enteral nutrition (minimal enteral feedings (≤20 mL/kg/day) as well as enteral nutrition feedings (>20 mL/kg/day), enteral nutrition weekly feedings (>140 mL/kg/day)). Furthermore, types of feeding in the hospital and after discharge (breast milk or formula), human milk fortification (as a fortifier, powder, or preterm formula), total fluid intakes and feeding interruptions (defined) due to discontinuation of enteral/oral feeds with the advancement of meals were also taken into consideration.27 The breastfeeding rate was determined based on infants’ ability to breastfeed or drink expressed breast milk starting from week 29th of gestation22 and the duration of follow-up over the 1-month and 3-months post-discharge of the premature infants.
The participants were assured of the confidentiality and safety of the premature infants. Written consent was obtained from them before their involvement in this study. The study was reviewed and approved by the Institutional Research Ethics Committee (MRECID no. 201765–5310) which was registered at ClinicalTrials.gov (NCT04926402). The KC was performed following the ethical standards outlined in the 2008 Declaration of Helsinki.
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 23.0 (IBM Corp., Armonk, NY, USA). Categorical data were analyzed using a general linear model and the model was fitted via ordinary least squares. Continuous data were analyzed using a repeated measure analysis of variance (ANOVA) followed by Bonferroni’s test for comparing means of the experimental and control groups upon discharge home for one month and three months post-discharge. Multiple comparisons were performed for outcomes (repeated measures) after ANOVA if there is an increased type I error which was necessary to adjust the p-value accordingly. The Dunn–Bonferroni method was designed to control the familywise error rate by calculating a new pairwise alpha to keep the familywise alpha value at 0.05. As a post-doc test, it uses thresholds based on the t-distribution.32 A p-value less than 0.05 indicated statistical significance. The assumptions for the general linear model and repeated measures ANOVA were tested and reported no clear violation.
Results
Ninety-six infant-mother pairs completed the study of 100, of which 48 were from the experimental and control groups, respectively. The reasons for non-completion include poor physical health (n = 2) and non-adherence (n = 2). Preterm infants in the NICU had similar average birth weights and gestational ages (Table 1). The mean age of the premature infants during recruitment was 32.00 weeks (SD = 0.42 weeks) of gestation. Both groups did not differ significantly in terms of their baseline demographics, with a mean gestational age of 32.05 weeks (SD = 1.20 weeks) in the experimental group and 32.04 weeks (SD = 1.09 weeks) in the control group (p > 0.05) Table 1. These babies were started with early parenteral nutrition and were often fed with their mother’s breast milk. The overall mean number of KC hours performed by mothers during NICU in the experimental and control group was 4.12 (SD = 0.26) and 0.55 (SD = 0.26) hours/week, respectively. The researchers compared the premature infants’ weight gain during recruitment until discharge to home, at one month, and three months post-discharge were evaluated. Weight gain velocity along the median weight curves for preterm infants using the G-Power calculation.33
 |
Table 1 Demographic Characteristics of Premature Infants in the Control Group (n = 48) and Experimental Group (n = 48) at Baseline |
An independent samples t-test was used to compare the mean body weight (g/day) reported by premature infants in the experimental group (n = 48) to the control group (n = 48) at three different interval periods of T1 (until discharge), T2 (1-month from post-discharge) and T3 (3-months from post-discharge) Table 2. The t-test was statistically significant with T1 experimental group (M = 10.07, SD = 5.53) than its control group (M = 9.27, SD = 4.71), t (df) = 1.54, p < 0.05. For an interval period of 1-month from post-discharge, the mean body weight scores between experimental and control group were M = 5.51, SD = 2.48 and M = 4.57, SD = 3.72, respectively, t (df) = 0.63, p<0.05. Furthermore, the mean body weight for premature infants after three months of post-discharge (T3) for the experimental group was M = 11.27, SD = 8.17; meanwhile, control group was M = 10.99, SD = 8.01, t (df) = 0.5, p<0.05.
 |
Table 2 Average Incremental Weight Gain of Infants (Gram per Day) in the Control Group (n = 48) and Experimental Group (n = 48) at T1, T2, and T3 Interval Periods |
The median body weight of premature infants during recruitment was 1449 g (IQR=343.50 g) and 1.442 g (IQR= 416.75 g) in the experimental and control groups, respectively, Table 3. In the experimental group, the median body weights were 1831 g (IQR=99.75 g) until discharge, 2140 g (IQR=80.75 g) at one month and 2522 g (IQR=1116.50 g) at three months post-discharge (p <0.05) Table 3. Besides that, the median body weights in the control group were 1831 g (IQR=102.25 g) until discharge, 2068 g (IQR=62.00 g) at one month, and 2468 g (IQR=1045.75 g) at three months post-discharge (p <0.05). The median body weight of premature infants in the experimental and control groups increased gradually from T1 to T3 interval periods. It is noted that the median body weight value of premature infants in the experimental group was significantly higher than the control group at three months post-discharge (z =−2.419, p <0.05). The predominance of growth restriction was compared at various time points using two sample groups proportional between control and experimental groups. The z-score tests were used to assess the median preterm weight gain velocity rates at T1, T2 and T3. The premature infants who received KC experienced statistically significant (p<0.05) weight gain at T1, T2 and T3.
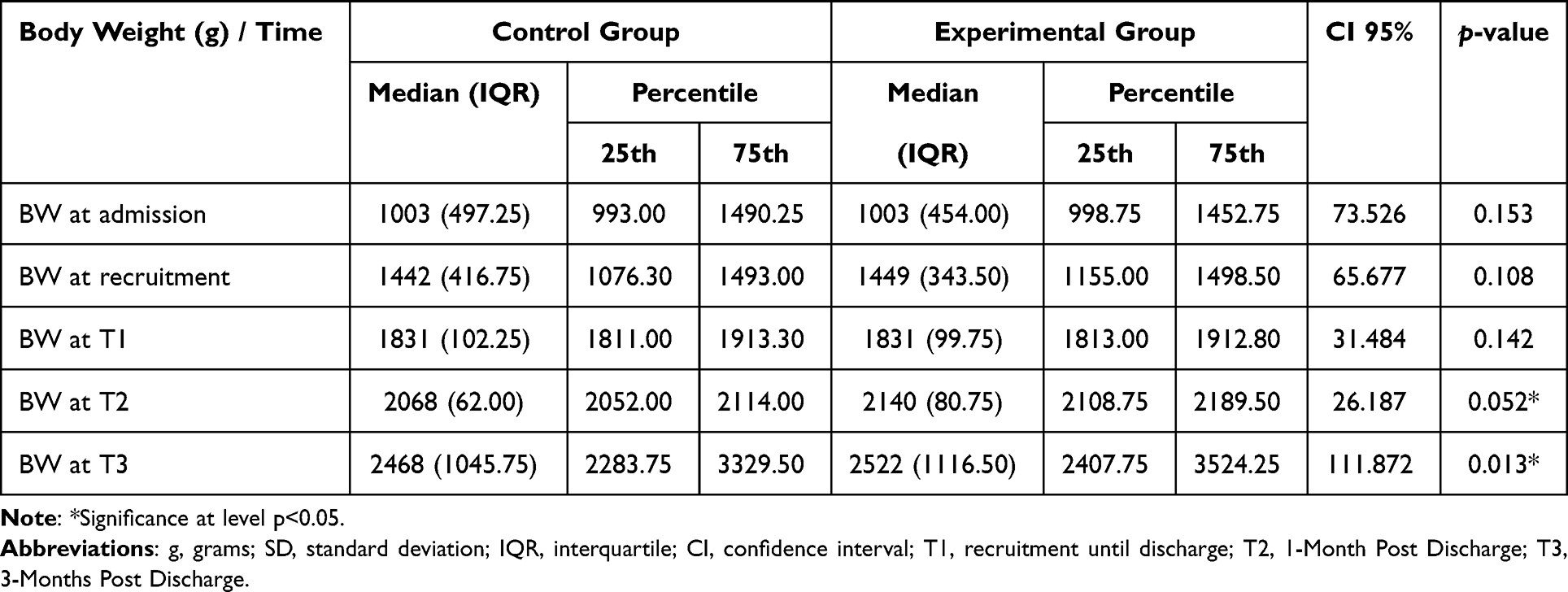 |
Table 3 Comparison of Median Body Weight (g) of Premature Infants in the Control Group (n = 48) and Experimental Group (n = 48) at T1, T2, and T3 |
The mean length of hospitalization for premature infants until discharge at 36 weeks of gestational age was 20.36 days (SD = 16.43 days) in the experimental group and 32.68 days (SD = 21.03 days) in the control group Table 4. Providing MKC-EP resulted in a slight significant decrease in the length of hospitalization for the experimental group proven by 95% confidence interval at 28.25–37.23 days than for the control group at 13.38–21.27 (t = 2.90, p <0.05). 95.8% of premature infants in the experimental group were discharged from the NICU between 36 and 39.6 weeks of postmenstrual age (PMA) compared to the control group at 91.7%. However, only 2.1% of premature infants in the experimental group and 4.2% in the control group were discharged from the NICU after 39 weeks of PMA Table 1.
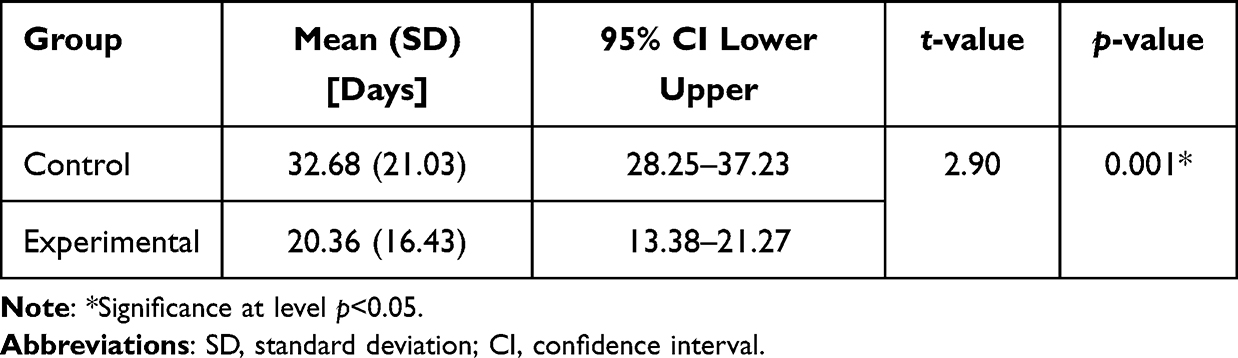 |
Table 4 Comparison Mean Length of Hospitalization of Premature Infants in the Control Group (n = 48) and Experimental Group (n = 48) Upon Discharge at 36 Weeks of Gestational Age |
Furthermore, premature infants in the experimental group were initiating direct breastfeeding on average at 32.20 weeks (SD = 0.40 weeks) (t = 2.80, p <0.05) earlier than the control group at 35.28 weeks (SD = 0.45 weeks) of PMA Table 5. In addition, the infants in the experimental group (M = 52.58, SD = 0.51 weeks) were able to continue breastfeeding at a longer age than those in the control group (M = 40.00, SD = 0.50 weeks), (df) = 3.09, p <0.05. 91.7% of premature infants in the experimental group had achieved successful breastfeeding at three months of age (45–52 weeks of gestation) compared to 20.8% in the control group.
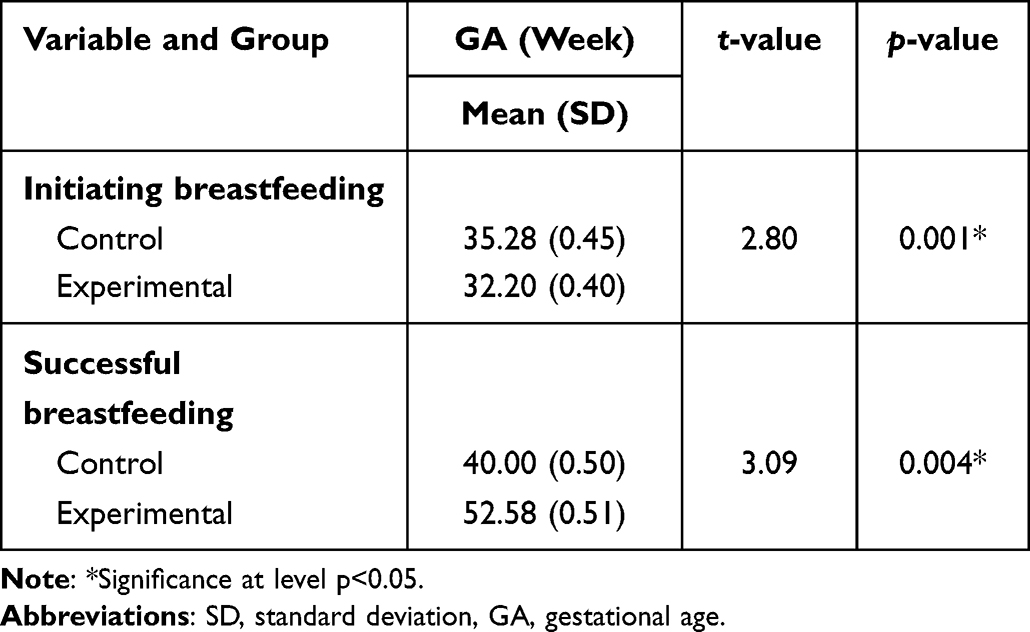 |
Table 5 Comparison Mean of Breastfeeding Rates Between the Control (n = 48) and Experimental Group (n = 48) |
Moreover, the rate of KC recommended to mothers for one hour per session in the experimental group was 91.7% (4 to 5 days in a week) higher than the control group at only 10.4% (1 to 2 days in a week). A total of 91.7% of premature infants in the experimental group initiated breastfeeding at 32 weeks of gestational age. However, 75.0% of premature infants from the control group had initiated breastfeeding at an average of 35.28 weeks. These findings showed that using KC as a complementary intervention improved breastfeeding rates among premature infants.
Discussion
This study shows that the MKC-EP session resulted in remarkable outcomes for mothers–premature infant pairs on weight gain patterns, length of hospitalization and breastfeeding rates. The findings show a significant difference in the KC performance (hours/week) between the experimental and control groups at T1, T2 and T3 interval periods. Premature infants’ outcomes with daily weight gain patterns were represented by the body weight velocity of those admitted to the NICU until three months from post-discharge. Our findings revealed a close fit between the experimental and control group infants’ weight gain velocity. This is consistent with the revised Fenton chart that stated the growth velocity of premature infants for the gestational age of 40 to 50 weeks in each gestational age group is estimated between 4 to 5g/kg/day.34
In this study, the weight gain velocity shows a statistically significant difference between both groups at T1 (32 to 39 weeks of gestation) (p<0.05) at the 50th percentile. This indicates that after KC’s performance, there is a slight improvement between both groups at T1 (after 32 weeks of recruitment). The weight gain velocity increased continuously from the recruitment period until the post-term of 52 weeks, even below the 3rd percentile at T2 and T3 Table 2. It shows that 95.8% of the infants from the experimental group were discharged at 1.81 kg to 2.10 kg, compared to the control group at only 91.7% between 36 and 39 weeks of gestation. This revealed that the consistent KC performance between 4 and 5 hours a week, helped to accelerate the weight gain of the premature infants during hospitalization in the NICU. The weight gain velocity in both groups inclines from the recruitment period until after the post-term of 52 weeks. Although there was an increase in both groups, the babies in the MKCEP group had a greater increment.
Even though the weight is fluctuating lower than the 3rd percentile and 10th percentile of Fenton’s growth chart,34 the amount of increase in the experimental group is greater than in the control group. This result indicates that the infants’ weight gain does not align with the Fenton growth chart at 44 and 52 weeks from post-discharge. Furthermore, there is a statistically significant difference (p<0.05) in the median body weight at T2 and T3 between the experimental and control group after the MKC-EP. The results show no significant difference in the average weight between the two groups before the experiment but vice versa in the second, third and fourth weeks. The findings were consistent in the previous study in which the weight gain slightly increased after 1 to 3 months post-discharge between the experimental and control groups.35 A possible explanation for the increase in premature infants’ weight gain could be related to KC performance which has improved milk production (rise of hormones and maternal sense of stimulus) and reduced infants’ motion, increase three phases of sleep in an hour, and reduce arousal in premature infants.36
The infants in the experimental group reached their birth weight earlier than those in the control group at T2 and T3. The weight gain velocity of premature infants between 44 and 52 weeks of gestation is consistent even if it was below the 3rd percentile and thus validates the smoothening assumptions made between preterm growth references. Even though the weight gain in the experimental group is a little increased equated to the control group. Hence, it made a statistically significant difference (p<0.05) in body weight between both groups at 1 to 3 months from the post-discharge weight of premature infants. Therefore, if an infant is born too early and very small, the weight gain could be as little as around 5 g per day, while the weight gain could be as high as 20 gm per day for larger infants and those born closer to their due date.37 In a recent study, the effect of KC on premature infants’ weight gain shows the experimental group infants gained 10gm more weight than the control group.38 This study showed a significant increase in the mean weight gain among the experimental group of premature infants from T1, T2 and T3. However, weight gain became slower at T2 and T3 after the discharge of premature infants from the NICU.
When the KC performance increases, the average sleep duration for premature infants also increases. This results in more calories saved, stimulation of pressure receptors, stimulation of parasympathetic nerves, increased bowel movements, the release of additional insulin hormone and increased milk intake.39 In order to increase mother–infant interaction and premature infant weight gain, it is recommended that particularly mothers receive the necessary KC training to confront and communicate with the infant and to empower mothers to care for premature neonates.39
Our findings concurred with previous studies indicating that systematic implementation of KC is associated with better weight gain in preterm infants.12,40 Infants in the control and experimental groups gained significant weight from baseline to 1 month of PMA and from baseline to 3 months post-discharge. It is worth noting that the mean weight gain of premature infants in the experimental group was significantly higher than that of premature infants in the control group at 3 months. This is congruent with meta-analysis, which showed that KC significantly reduces premature death, improves emotional attachment experienced by mothers, infants’ weight gain, and protection of babies from infections and sepsis compared to conventional neonatal care.14 Therefore, KC has been demonstrated to be a successful method for preventing mortality in preterm and low birth weight (LBW) babies in low-, middle-, and high-income countries.41
The total duration of KC during seven days in the experimental group was at T1 (M=4.12, SD= 0.26), T2 (M=2.73, SD= 0.12), and T3 (M=3.18, SD= 0.12) hours per week after engaging in the MKC-EP intervention program. The current study reported a significantly shorter (p< 0.05) KC duration than previous studies. A study previously conducted in Andhra Pradesh, India on 46 premature infant-mother pairs trained for KC at a facility indicated that 6.5% of mothers believed it was feasible to provide KC for 12 hours or more per day, while 52% of mothers thought that only 1 hour per day was realistic.42 Similarly, a KC trial on 1565 infant-mother pairs showed only 23.8% practiced KC for more than 7 hours per day within the first 48 hours of life. The total duration of KC from day 3 to 7 was M = 2.7, (SD= 3.40) hours per day.43 In this study, a significant decrease in KC duration was noted in the experimental group with a mean difference between 2 and 4 hours per week. The average duration of KC is estimated to be 1 hour per day44 and 4 to 5 hours per week.10 This is shorter than the anticipated reduction in duration and the reductions of KC performance reported by previous studies, which might be due to the length of intervention present in this study. However, the mothers who performed KC for 4 to 5 hours in the NICU intend to bring their babies back home quickly. This follows the NICU discharge weight protocol in which the baby needs to gain weight of at least 1.8 kg. However, the KC performance decreased at T2 and T3 post-discharge from NICU. Therefore, public health nurse should encourage mothers to perform KC as a routine practice during their home visits. This is an excellent strategy for developing connections between mothers and their premature infants. Studies showed KC performance has increased the impact on infants’ weight gain.23,45 Preparing parents for a proper parental role, especially mothers after their premature infants’ birth, is recommended in effective communication via KC as a foundation of family-centered services. The mothers should encourage to perform KC consistently.
Breastfeeding rate refers to the rate at which premature infants have started taking expressed breast milk (EBM), partially or successfully starting from 29 weeks. This comes with continued breastfeeding along with suitable preterm formula milk for the first three months and beyond or is weaned at a specific gestational week. In this study, the findings showed that premature infants were observed to start breastfeeding in the control group at a mean gestational age of (M = 35.28, SD = 0.45) compared to the experimental group (M = 32.20, SD = 0.40). Mothers may be determined to breastfeed and express milk for their premature infants but may not be able to do so because they are separated from their infants and unable to feed them during inconvenience that arises after hospitalization. Premature infants cannot obtain enough nutrition or immunity factors from the placenta during the last trimester, so their organs and systems are not fully mature. Therefore, the infants require special care and more breast milk.46 As such, it is evident that KC performance increases mothers’ confidence to start breastfeeding early with their premature infants. Breastfeeding should also be prioritized for its nutritional, immunological, and psychological benefits.46
Breast milk is the primary nutrient that increases the growth rate of premature infants.47 During hospitalization, breastfeeding is provided according to the hospital’s routine and protocol. Breastfeeding was given on a scheduled basis once every 3 hours or eight feedings in 24 hours, depending on the infant’s condition and the amount and calories required by them or based on demand for expressed breast milk by the mother18 Nevertheless, the infant’s breastfeeding schedule may become inconsistent after their discharge from NICU between 1 and 3 months of PMA. Furthermore, some mothers have returned to work at this time and may send their babies to childcare centers that could not adhere to the feeding schedule due to many foster babies.23 As a result, the requirement for breast milk every 3 hours could not be fully met. This could be related to the average KC performance hours spent per week being significantly lower at T2 (M = 2.73, SD = 0.12) and T3 (M = 3.18, SD = 0.12) interval periods compared to T0 (M = 4.12, SD = 0.26), p<0.05. A previous study indicated that KC has a significant positive impact on physiological functions and improved infant-mother bonding, which likely contributes to infants’ weight gain.48
In this study, the average age (week) at the time of initiation of maternal breastfeeding in the experimental group is earlier. It occurred as early as the gestational age of 32 weeks in the experimental group and the gestational age of 35 weeks in the control group. Therefore, a systematic KC performance via an education program is necessary to build breastfeeding confidence among mothers. An observational study reported that KC successfully encourages breastfeeding and increases mothers’ confidence when handling small infants fed with orogastric tubes.38 Studies have shown that premature infants whose mothers performed KC had a higher frequency of breastfeeding than those infants with mothers who practiced standard care.49–54 The literature has indicated that KC allows mothers to start breastfeeding earlier and encourages the development of their maternal instincts.48,55,56 While decreasing maternal distress.46 In addition, prematurity is a condition that can hinder or postpone mother-infant bonding by preventing mothers from seeing and holding their infants.46 The KC position has encouraged babies to nibble on their mothers’ nipples, which helps in milk production. Various studies have shown that premature infants whose mothers have used KC have higher breastfeeding rates than those who used standard care.12,20,49–54,56
Mothers who were in the control group could only maintain successful breastfeeding until the baby was 40 weeks old. Meanwhile, the experimental group continued breastfeeding until the baby was 52 weeks old during the study period. The lack of KC performance among mothers in the control group may have inhibited mother-infant bonding and slowly decreased the quantity of milk. Therefore, it will affect insufficient breast milk production and slowly reduce milk consumption.23 A previous study found a progressive reduction in the quantity of milk produced by mothers who did not practice KC,46 resulting in early weaning which may explain this observation. Practicing KC for an uninterrupted 60 minutes during the first 12 weeks and consistently for the first at least three months old would allow the mother not to cease breastfeeding.57 Therefore, this study was conducted on premature infants to evaluate the effectiveness of KC until they reached three months of PMA. It was found that the average differences in the control group mothers’ milk production using standard care were not statistically significant and the quantity of milk produced decreased gradually. These findings were similar to a study, which found that the average differences in intragroup milk production in the standard care group were not statistically significant and the volume of milk produced reduced progressively.46 The inadequacy of KC between standard care group mothers and their infants may have interfered with their bonding, decreasing the mother’s milk production. The performance of KC has helped to promote breastfeeding successfully until the baby is three months old. This is in line with the Baby-Friendly Hospital Initiative 2010 entails initiating breastfeeding within the first hours of life, encouraging breastfeeding solely for the first six months. During the data collection, several mothers in the experimental group revealed that they were still breastfeeding their infants after the completion of this study. In Malaysia, women employees are not protected by law to breastfeed or express milk at work.58 In a recent study in the Kuala Muda district area, Malaysia reported that childcare workers may also be another potential resource for maintaining exclusive breastfeeding at registered nurseries.59 Hence, every single person caring for a baby has a significant role in partially or exclusively facilitating breastfeeding.
The present study reported KC performance help with the duration of NICU stays. There is a significant reduction in the mean length of hospital stays for premature infants in the experimental group (M= 20.36, SD = 16.43 days) compared to the control group (M = 32.68, SD = 21.03 days). A similar observation was reported earlier that infants who received KC were discharged from NICU earlier (M = 11.46, SD = 4.32 days) than those without KC (M = 17.68, SD = 8.64 days), p < 0.0512 The longer length of hospital stays in our study is attributed to the earlier gestational ages of the infants recruited, ie, at 28 weeks and 36.6 weeks compared to previous research, which assessed premature infants between the ages of 32 weeks and 36 weeks. The premature infants in this study were discharged from the NICU when they could feed well and were clinically healthy. These were set according to the Hospital Preterm Baby Discharge Guidelines for having a good sucking reflex with breast or bottle feeding, weight gain of more than 15 to 20 g/day for at least three successive days and achieving a predetermined weight of 1.8kg.60
The present study revealed only 4.2% of the experimental group had been discharged at 40 to 43 weeks of age, compared to the control group at 8.3%. However, 95.8% of premature infants in the experimental group were discharged at 36 to 39 weeks, while the control group was at 91.7%, p > 0.05. Furthermore, premature infants who did not receive or were provided less than 1 hour per day and less than 3 to 4 hours per week of KC were staying longer in the hospital for both groups. The findings demonstrated the length of hospitalization between the control and the experimental groups varied significantly. Our findings agree with previous studies that the performance of a KC significantly reduces the length of stay in NICU among premature infants.30,40,45 Further study is needed to explore the relationship between characteristics, gender, premature severity, non-operative cases and mechanically ventilated premature infants. Thus, KC practice is essential to both mothers and infants.
It is challenging to perform KC in a busy NICU without empowering the mother.22,23 Implementing a locally contextualized MKC-EP can allow a better understanding of the importance of KC as an intervention, hence, allowing its practice to be strengthened and adopted beyond hospital stays. This can lead to better infant weight gain and more extended periods of breastfeeding. The main limitation of this study is that it was conducted within a single NICU and involved only singleton births. Besides, this study only included infant-mother pairs and the role of fathers was not evaluated. Further exploratory studies on parental perception are recommended. Other confounding factors influencing breastfeeding rates such as multiple pregnancies or infant co-morbidities were not studied. Thus, it is suggested that the effect of KC among these factors should be explored further.
Conclusion
The findings of this study revealed that a locally contextualized and structured kangaroo care education program is more effective than standard routine care in encouraging mothers in KC performance. One hour of KC daily is associated with an extended breastfeeding period, improved weight gain, and a shorter hospital stay for premature infants. This study backs up KC practices for premature infants, which can be used with standard health care in the NICU setting.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board University Malaya Medical Centre Medical Research Ethics Committee (UMMC MRECID no. 201765-5310), registered at ClinicalTrials.gov (NCT04926402).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors are incredibly grateful to the mothers and babies involved in this study. We also thank our University Malaya Medical Centre Malaysia colleagues who have provided insight and expertise that greatly assisted this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nieder-Heitmann E. The Impact Of A Sensory Developmental Care Programme for Very Low Birth Weight Preterm Infants in The Neonatal Intensive Care Unit [Doctoral dissertation]. University of Stellenbosch; 2010.
2. Nyqvist KH, Anderson GC, Bergman N, et al. Towards universal kangaroo mother care: recommendations and report from the first European conference and seventh international workshop on Kangaroo Mother Care. Acta Paediatr. 2010;99(6):820–826. doi:10.1111/j.1651-2227.2010.01787.x
3. Ludington-Hoe S, Morgan K, Abouelfettoh AM. A clinical guideline for implementation of kangaroo care with premature infants of 30 or more weeks’ postmenstrual age. Adv Neonatal Care. 2008;8:3–23. doi:10.1097/01.ANC.0000324330.25734.b6
4. Bauer K, Uhrig C, Sperling P, Pasel K, Wieland C, Versmold HT. Body temperature and oxygen consumption during skin-to-skin (kangaroo) care in stable preterm infants when less than 1500 grams. J Pediatr. 1997;130:240–244. doi:10.1016/S0022-3476(97)70349-4
5. Davy K, Bergh A, Van Rooyen E. The neonatal nurse’s role in kangaroo mother care: mother and child health. Prof Nurs Today. 2011;15(3):32–37.
6. Charpak N, Ruiz-Peláez JG, Charpak Y. Rey-Martinez. Kangaroo mother program: an alternative way of caring for low birth weight infants? One year mortality in a two cohort study. Pediatrics. 1994;94:804–810. doi:10.1542/peds.94.6.804
7. Ludington-Hoe SM, Nguyen N, Swinth JY, Satyshur RD. Kangaroo care compared to incubators in maintaining body warmth in preterm infants. Biol Res Nurs. 2006;2:60–73. doi:10.1177/109980040000200107
8. Kaffashi F, Scher MS, Ludington-Hoe SM, Loparo KA. An analysis of the kangaroo care intervention using neonatal EEG complexity: a preliminary study. Clin Neurophysiol. 2013;124:238–246. doi:10.1016/j.clinph.2012.06.021
9. Kieviet JF, De Zoetebier L, Elburg RM, Van Vermeulen RJ, Oosterlaan J. Brain development of very preterm and very low-birthweight children in childhood and adolescence: a meta-analysis. Dev Med Child Neurol. 2012;54:313–323. doi:10.1111/j.1469-8749.2011.04216.x
10. Ludington-Hoe SM, Morgan KL. Kangaroo Care in the NICU, Part 1: Understanding the Impact of Kangaroo Care on 23 Neonatal Vital Signs. Baltimore, MD: March of Dimes Foundation; 2013.
11. Biswas M, Malpani P, Ekka AS. To study the short-term outcome of kangaroo mother care in newborn with birth weight less than 1.5 kg. Indian J Child Health. 2016;3:171–173. doi:10.32677/IJCH.2016.v03.i02.020
12. Boundy EO, Dastjerdi R, Spiegelman D, et al. Kangaroo mother care and neonatal outcomes: a meta-analysis. Pediatrics. 2016;137:2015–2238. doi:10.1542/peds.2015-2238
13. Verklan T, Walden M. Pain Assessment and Management: Core Curriculum for Neonatal Intensive Care Nursing.
14. Conde-Agudelo A, Diaz-Rossello JL, Belizan JM. Kangaroo mother care to reduce morbidity and mortality in low 25 birthweight infants. Cochrane Database System Rev. 2000;4:CD002771. doi:10.1002/14651858.CD00277126
15. Zaidi AKM, Huskins C, Thaver D, Bhutta AZ, Abbas Z, Goldmann DA. Hospital-acquired neonatal infections in developing countries. Lancet. 2005;365:1175–1188. doi:10.1016/S0140-6736(05)71881-X
16. Shaikh TH, Sangi R, Raza MS, et al. Efficacy of Kangaroo Mother care among low birth weight newborns at a tertiary care hospital: a cross-sectional study. J Pharm Res Int. 2022;34(41B):1–6.
17. Narciso LM, Beleza LO, Imoto AM. The effectiveness of Kangaroo Mother Care in hospitalization period of preterm and low birth weight infants: systematic review and meta-analysis. J Pediatr. 2022;98:117–125. doi:10.1016/j.jped.2021.06.004
18. Kim SY, Kim AR. Attachment-and relationship-based interventions during NICU hospitalization for families with preterm/low-birth-weight infants: a systematic review of RCT data. Int J Environ Res Public Health. 2022;19(3):1126. doi:10.3390/ijerph19031126
19. McCall EM, Alderdice F, Halliday HL, Vohra S, Johnston L. Interventions to prevent hypothermia at birth in preterm and/or low birth weight infants. Cochrane Database Syst Rev. 2018;2(2):CD004210. doi:10.1002/14651858.CD004210.pub5
20. Conde‐Agudelo A, Belizán JM, Diaz‐Rossello J. Cochrane review: kangaroo mother care to reduce morbidity and mortality in low birthweight infants. Evid Based Child Health. 2012;7(2):760–876. doi:10.1002/ebch.1837
21. Bhutta ZA, Das JK, Bahl R, et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet. 2014;384:347–370. doi:10.1016/S0140-6736(14)60792-3
22. United States Institute for Kangaroo Care (USIKC) KC BIB. Promoting Skin-to skin Care; 2013. Available from: https://kangaroocareusa.org/.
23. Samsudin S, Chui PL, Kamar ABA, Abdullah KL. Maternal Kangaroo care education program in the neonatal intensive care unit improved mothers’ perceptions, knowledge, perceived barriers and stress relates to premature infant. Nurs Open. 2022;00:1–9.
24. Ong SL, Abdullah KL, Danee M, Soh KL, Lee DSK, Hussin EOD. The Effectiveness of a structured nursing intervention on maternal stress and ability among mother of premature infants in a neonatal intensive care unit. J Clin Nurs. 2019;28(3–4):641–649. doi:10.1111/jocn.14659
25. Agustina AN, Rustina YR, Triwaluyanti FT. Upaya meningkatkan berat badan bblr melalui intervensi comfort food for the soul kolcaba (Perawatan Metode Kanguru). J Ilmu Keperawatan. 2018;2(2):1–9.
26. Seidman G, Unnikrishnan S, Kenny E, et al. Barriers and enablers of kangaroo mother care practice: a systematic review. PLoS One. 2015;10(5):e0125643. doi:10.1371/journal.pone.0125643
27. Dupont WD, Plummer WD. Power and sample size calculations: a review and computer program controlled. Clin Trials. 1990;11:116–128. doi:10.1016/0197-2456(90)90005-M
28. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation 49 and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
29. Suman RP, Udani R, Nanavati R. Kangaroo mother care for low birth weight infants: a randomized control trial. Indian Peadiatr. 2008;45:17–23.
30. World Health Organization, Reproductive Health, UNAIDS. Kangaroo Mother Care: A Practical Guide. Geneva, Switzerland: World Health Organization; 2003.
31. Ludington-Hoe SM, Morgan KL. Kangaroo Care in the NICU, Part 1: Understanding the Impact of Kangaroo Care on Neonatal Vital Signs. Baltimore, MD: March of Dimes Foundation; 2018.
32. Senterre T, Rigo J. Reduction in postnatal cumulative nutritional deficit and improvement of growth in extremely preterm infants. Acta Paediatr. 2012;101:61–70. doi:10.1111/j.1651-2227.2011.02443.x
33. Moniem II, Morsy MA. The effectiveness of kangaroo technique on preterm infant’s weight gain. J Am Sci. 2011;7(1):697–702.
34. Fenton TR, Nasser R, Eliasziw M, Kim JH, Bilan D, Sauve R. Validating the weight gain of preterm infants between the reference growth curve of the fetus and the term infant. BMC Pediatr. 2013;13(1):1–10. doi:10.1186/1471-2431-13-92
35. Kashaninia Z, Dehghan M. The effect of kangaroo care on weight gain of premature neonates in hospitalized in neonatal intensive care units. Biosci Biotechnol Res Asia. 2015;12(2):1405–1410. doi:10.13005/bbra/1799
36. Davidson M, London M, Ladewig P. Postpartum Family Adaptation and Nursing Assessment. Old’s Maternal Newborn Nursing & Women’s Health Across the Lifespan.
37. Peck K, Russo F, Campos JL, Keshavarz B. Examining potential effects of arousal, valence, and likability of music on visually induced motion sickness. Exp Brain Res. 2020;238(10):2347–2358. doi:10.1007/s00221-020-05871-2
38. Field T, Diego M, Hernandez-Reif M. Potential underlying mechanisms for weight gain in massaged preterm infants. Infant Behav Dev. 2011;34:383–389. doi:10.1016/j.infbeh.2010.12.001
39. Borimnejad L, Mehrnoush N, SeyyedFatemi N, Haghani H. The effect of empowerment program on infant-mother interaction and weight gain in preterm infants. Zahedan J Res Med Sci. 2012;14(9):12–17.
40. World Health Organization. Global Strategy for Infant and Young Child Feeding. Geneva: World Health Organization; 2003.
41. Muddu GK, Boju SL, Chodavarapu R. Knowledge and awareness about benefits of Kangaroo mother care. Indian J Pediatr. 2013;80:799–803. doi:10.1007/s12098-013-1073-0
42. Sloan NL, Ahmed S, Mitra SN, et al. Community-based kangaroo mother care to prevent neonatal and infant mortality: a randomized, controlled cluster trial. Pediatrics. 2008;121:1047–1059. doi:10.1542/peds.2007-0076
43. Almutairi WM, Ludington-Hoe SM. Kangaroo care education effects on nurses’ knowledge and skills confidence. J Contin Educ Nurs. 2016;47(11):518–524. doi:10.3928/00220124-20161017-11
44. Bilal SM, Tadele H, Abebo TA, et al. Barriers for kangaroo mother care (KMC) acceptance, and practices in southern Ethiopia: a model for scaling up uptake and adherence using qualitative study. BMC Pregnancy Childbirth. 2021;21(1):1–12. doi:10.1186/s12884-020-03409-6
45. Coşkun D, Günay U. The effects of kangaroo care applied by Turkish mothers who have premature babies and cannot breastfeed on their stress levels and amount of milk production. J Pediatr Nurs. 2020;50:26–32. doi:10.1016/j.pedn.2019.09.028
46. Brown A, Raynor P, Lee M. Maternal control of child-feeding during breast and formula feeding in the first 6 months post-partum. J Hum Nutr Diet. 2011;24(2):176–186. doi:10.1111/j.1365-277X.2010.01145.x
47. Monk SJ, Champagne FA. Linking prenatal maternal adversity to developmental outcomes in infants: the role of epigenetic pathways. Dev Psychopathol. 2012;24(4):1361–1376. doi:10.1017/S0954579412000764
48. Cunningham EM, Doyle EI, Bowden RG. Maternity nurses’ perceptions of implementation of the ten steps to successful breastfeeding. Child Nurs. 2018;43:38–43. doi:10.1097/NMC.0000000000000392
49. Tully KP, Holditch-Davis D, White-Traut RC, David R, O’Shea MT, Geraldo V. A test of kangaroo care on preterm infant breastfeeding. J Obstet Gynecol Neonatal Nurs. 2016;45:45–61. doi:10.1016/j.jogn.2015.10.004
50. Moore ER, Bergman N, Anderson GC, Medley N. Early skin‐to‐skin contact for mothers and their healthy newborn infants. Cochrane Database Syst Rev. 2016;1CD003519. doi:10.1002/14651858.CD003519
51. Moore T, Hennessy EM, Myles J, et al. Neurological and developmental outcome in extremely preterm children born in England in 1995 and 2006: the EPICure studies. Br Med J. 2012;345:e7961. doi:10.1136/bmj.e7961
52. Bigelow A, Power M, MacLellan-Peters J, Alex M, McDonald C. Effect of mother/infant skin-to-skin contact on postpartum depressive symptoms and maternal physiological stress. J Obstet Gynecol Neonatal Nurs. 2012;41:369–382. doi:10.1111/j.1552-6909.2012.01350.x
53. Gouchon S, Gregori D, Picotto A, Patrucco G, Nangeroni M, Di Giulio P. Skin-to-skin contact after cesarean delivery. Nurs Res. 2010;59:78–84. doi:10.1097/NNR.0b013e3181d1a8bc
54. Sibel K, Fatma YK, Ozdemir AA, Ozcan Z. The effect of kangaroo care on breastfeeding and development in preterm neonates. J Pediatr Nurs. 2021;60:31–38. doi:10.1016/j.pedn.2021.02.019
55. Fatma Y, Sibel K, Aynur AÖ, Tanju O, Nesrin A. The effect of kangaroo mother care, provided in the early postpartum period, on the breastfeeding self-efficacy level of mothers and the perceived insufficient milk supply. J Perinat Neonatal Nurs. 2020;34:80–87. doi:10.1097/JPN.0000000000000434
56. Blomqvist YT, Frölund L, Rubertsson C, Nyqvist KH. Provision of Kangaroo Mother Care: supportive factors 82 and barriers perceived by parents. Scand J Caring Sci. 2013;27:345–353. doi:10.1111/j.1471-6712.2012.01040.x
57. Lillehoj CJ, Dobson BL. Implementation of the baby‐friendly hospital initiative steps in Iowa hospitals. J Obstet Gynecol Neonatal Nurs. 2012;41(6):717–727. doi:10.1111/j.1552-6909.2012.01411.x
58. Musa TH, Musa HH, Ali EA, Musa NE. Prevalence of malnutrition among children under five years old in Khartoum State, Sudan. Pol Ann Med. 2014;21(1):1–7. doi:10.1016/j.poamed.2014.01.001
59. Mohd Suan MA, Ayob A, Rodzali M. Childcare workers’ experiences of supporting exclusive breastfeeding in Kuala Muda District, Malaysia: a qualitative study. Int Breastfeed J. 2016;12(1):1–8. doi:10.1186/s13006-016-0095-4
60. Lian YC, Ying SH, Peng CC, Yann TY. Early discharge study for premature infants: Singapore general hospital. Perm J. 2008;12(4):15–18. PMID: 21339916; PMCID: PMC3037135. doi:10.7812/TPP/08-040
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.