")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Impact of Prehospital Point of Care Ultrasounds on Emergency Patients Length of Stay in Thailand
Authors Ienghong K , Cheung LW , Tiamkao S , Bhudhisawasdi V, Apiratwarakul K
Received 10 November 2022
Accepted for publication 17 January 2023
Published 24 January 2023 Volume 2023:16 Pages 219—226
DOI https://doi.org/10.2147/JMDH.S396986
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kamonwon Ienghong,1 Lap Woon Cheung,2,3 Somsak Tiamkao,4 Vajarabhongsa Bhudhisawasdi,1 Korakot Apiratwarakul1
1Department of Emergency Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 2Accident & Emergency Department, Princess Margaret Hospital, Kowloon, Hong Kong; 3Emergency Medicine Unit, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Pokfulam, Hong Kong; 4Department of Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
Correspondence: Korakot Apiratwarakul, Department of Emergency Medicine, Faculty of Medicine, Khon Kaen University, 123 Mittraphap Road, Mueang Khon Kaen District, Khon Kaen, 40002, Thailand, Tel +66 89 416 3663, Fax +66 43 366 870, Email [email protected]
Purpose: Globally, emergency departments (ED) are faced with an overcrowding problem. This issue is further compounded due to the multitude of contributing factors. Point of Care ultrasound (POCUS), especially when performed in prehospital care, that is before the patient is admitted to the ED has a high potential to reduce time of diagnosis and time of investigation which leads to shorter ED length of stay (LOS). The primary focus was on variances in ED LOS between the prehospital POCUS group and the standard care group.
Patients and Methods: A cross-sectional study was conducted on prehospital patients who were admitted to the ED at Srinagarind Hospital, Thailand, from January to December 2021. We divided patients into two groups including patients who obtained prehospital POCUS (the prehospital POCUS group) and patients who received standard care treatment in which there was no prehospital POCUS performed (the standard care group). POCUS and ED medical records were documented and submitted for analysis.
Results: Of 1348 prehospital patients, 840 were enrolled in this study: 169 with prehospital POCUS and 671 with standard care. Median LOS in the prehospital POCUS group was 159 min (IQR 89,289) versus 165 (IQR 102,330) in the standard care group (p = 0.125). Further imaging diagnostic test which affected ED LOS more than four hours was lower in the prehospital POCUS group (adjusted odds ratio [OR], 0.92; 95% confidence intervals [CI], 0.729– 1.666) than in the standard care group. The factor associated with increased odds of ED LOS more than four hour in the prehospital POCUS group was admission to hospital (adjusted OR 1.88; 95% CI, 1.230-2.239).
Conclusion: Patients evaluated with prehospital POCUS had a shorter LOS than the only standard care treatment without statistical significance.
Keywords: ultrasonography, prehospital emergency care, length of stay, emergency departments, crowding
Introduction
Emergency department length of stay (ED LOS) is one of the main contributing factors when determining patient outcomes. Previous studies1,2 demonstrated wide variances in the cut-offs used to define extended ED LOS among settings and appear to be picked at random between lengths of between four and forty-eight hours. However, longer ED LOS resulted in emergency department crowding and lower patient-centered outcomes.3,4
Point of Care Ultrasound (POCUS) is one of the effective bedside diagnostic tools and is currently mostly performed in the emergency department (ED).5 As it has a range of applications, including as soft tissue, appendix, pelvic, biliary, and renal ultrasounds, POCUS has been linked to a reduced ED LOS, particularly in adults.6–10 Significant progress in the medical technology,11,12 particularly for handheld ultrasound, has been rapidly developing. The prehospital POCUS is currently used as an adjunct tool for clinical assessments in trauma patients, cardiac arrest, hemodynamic instability, respiratory failure, vascular access, and various other types of applications.13–18 Most studies in prehospital POCUS center on the feasibility of prehospital POCUS, prehospital POCUS programs assessment, and the accuracy of diagnosis.19–21 However, the influence on prehospital patient outcomes has a very limited number of studies.13,22–24 Moreover, the association between prehospital POCUS and ED LOS has not yet been seriously studied.
In Thailand, the prehospital POCUS is a novice tool in emergency medical services (EMS). The prehospital POCUS is performed only in medical training centers. From the past reviews, there are only two studies of prehospital POCUS in the aspects of prehospital POCUS training25 and the diagnostic accuracy of POCUS used in a prehospital setting.26 Due to this lack of investigation, the specific research question addressed was: Does the employing of prehospital POCUS reduce the ED LOS for emergency patients?
Materials and Methods
This was a cross-sectional, observational study obtained from patients admitted to the EMS unit and the ED at Srinagarind hospital located in Khon Kaen province, Thailand. This hospital is the central medical training center and home to the most advanced tertiary care facilities and personnel in northeastern Thailand, with an annual average of approximately two thousand EMS operations and seventy thousand emergency department visits.
ED LOS in this study was defined as the time from when patients from the EMS unit signed up at the triage unit at the ED to when the discharge order from the ED was placed in the electronic medical record (EMR).
Long ED LOS in this study was defined as total boarding time of patients in the ED exceeding four hours according to our hospital policy.
Data Collection
The study was conducted in patients who received EMS and visited the emergency department between January 2021 and December 2021. Patients with missing data were excluded.
EMS physicians were emergency medicine residents, who had completed 1 month POCUS training in the 2019–2020 Academic year and had routinely assessed patients at the scene. The decision to perform POCUS was dependent on EMS physicians at that time. POCUS was performed either at the emergency site (on scene) or during patient transport.
This study defined two study groups. Patients in the first group received prehospital POCUS and standard treatment at EMS (the prehospital POCUS group; the study group) and patients in the second group received only standard treatment without performing POCUS (the standard care group; the control group).
The data collected from both patient groups consisted demographic information about the patients including gender, age, type of illness, triage level following the emergency severity index, chief complaint, area of POCUS examination, POCUS findings, ED process, and ED LOS. Prehospital POCUS was obtained using a Butterfly IQ handheld ultrasound machine (Butterfly Network, Inc, Guilford, Connecticut USA). These data were retrieved from EMR and the database from the Butterfly IQ. After that, these data were documented in standard format by two independent investigators who were blind to the treatment team. The duplicate data entry was completed. If the data did not match, the senior emergency physician was consulted, and the correct data were acquired.
Sample Size
The sample size was determined using the following formula.27 P was estimated using data from a previously published study,28 and a sample size of 169 was judged to be necessary in the POCUS group.
Statistical Analysis
A descriptive analysis was conducted on the demographics and characteristics of the participants. ED LOS between two groups was compared using the Student’s t-test and Wilcoxon rank-sum test for each group. Odds ratios (ORs) and 95% confidence intervals (CIs) were also calculated. We demonstrated frequencies for categorical variables, and medians and interquartile ranges for continuous variables. The data was input into Microsoft Excel and analyzed with IBM SPSS for Windows version 27.0, which is licensed to Khon Kaen University (SPSS Inc., Chicago, IL, USA).
Results
1348 EMS operations were assessed by EMS physicians between January 2021 and December 2021. Of these, 840 patients were admitted to our ED and 169 patients received prehospital POCUS. The patient demographic information for both groups is demonstrated in Table 1. All patients in the prehospital group were medical patients. The prehospital POCUS group had patients triaged at levels 1 and 2 as an equal percentage to the standard care group. The prehospital POCUS group demonstrated a higher percentage of laboratory tests, consultation to specialists, and admission to hospital compared to the standard care group. The further imaging diagnostic test was lower than the standard care group (P = 0.050). The ED LOS in the prehospital POCUS group was shorter than the control group (P = 0.125).
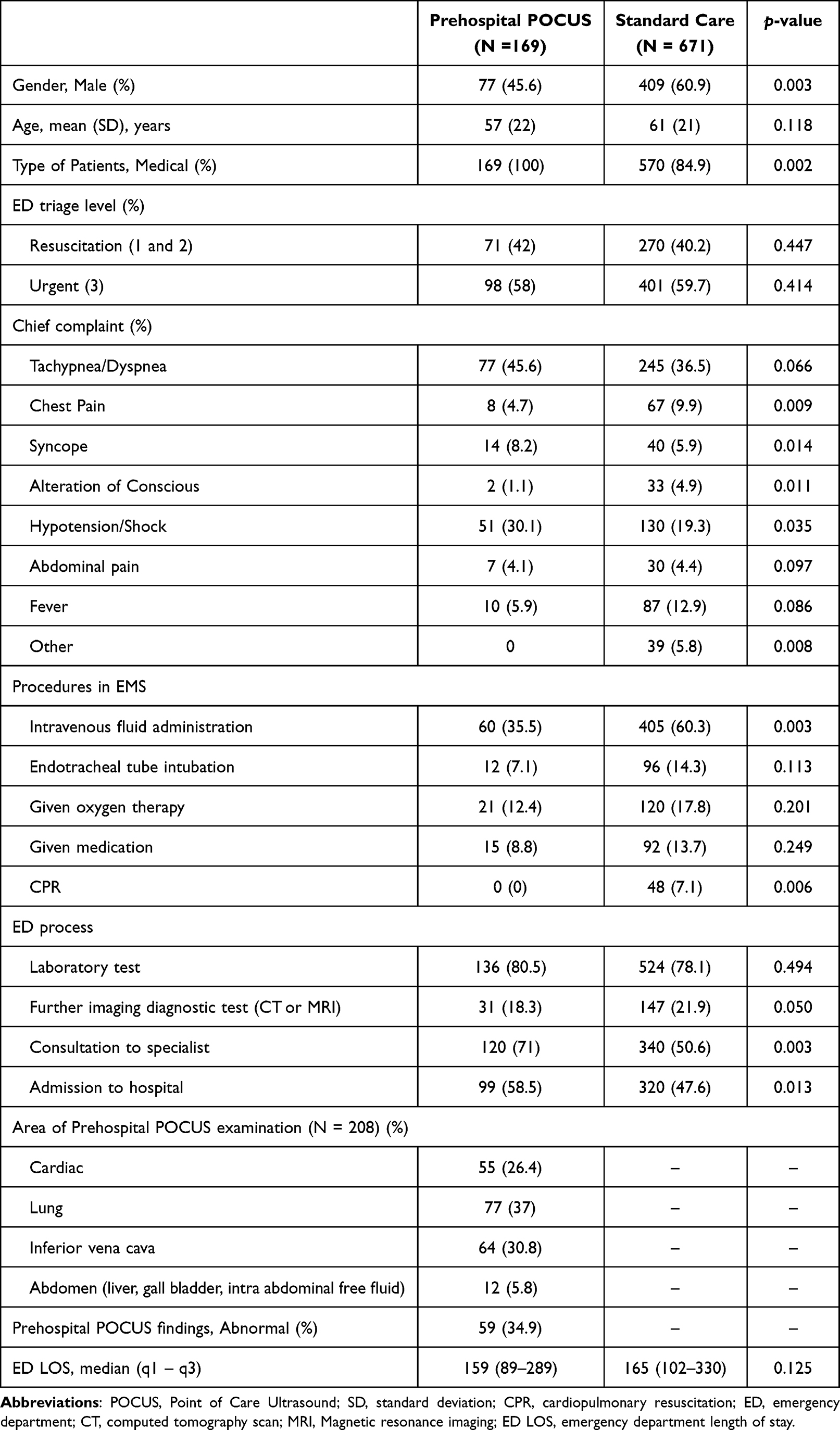 |
Table 1 Demographics of the Study Population |
After adjusting for confounding factors, the factors associated with ED LOS of more than 4 hours are demonstrated in Table 2. Factors associated with decreased odds of ED LOS of more than four hours in the prehospital POCUS group were further imaging diagnostic tests (adjusted odds ratio [OR] 0.92, 95% CI: 0.729–1.666, P = 0.499). The factor associated with increased odds of ED LOS of more than four hours in the prehospital POCUS group was admission to hospital (adjusted OR 1.88, 95% CI: 1.230-2.239, P < 0.001), laboratory test, and consultation with a specialist, respectively.
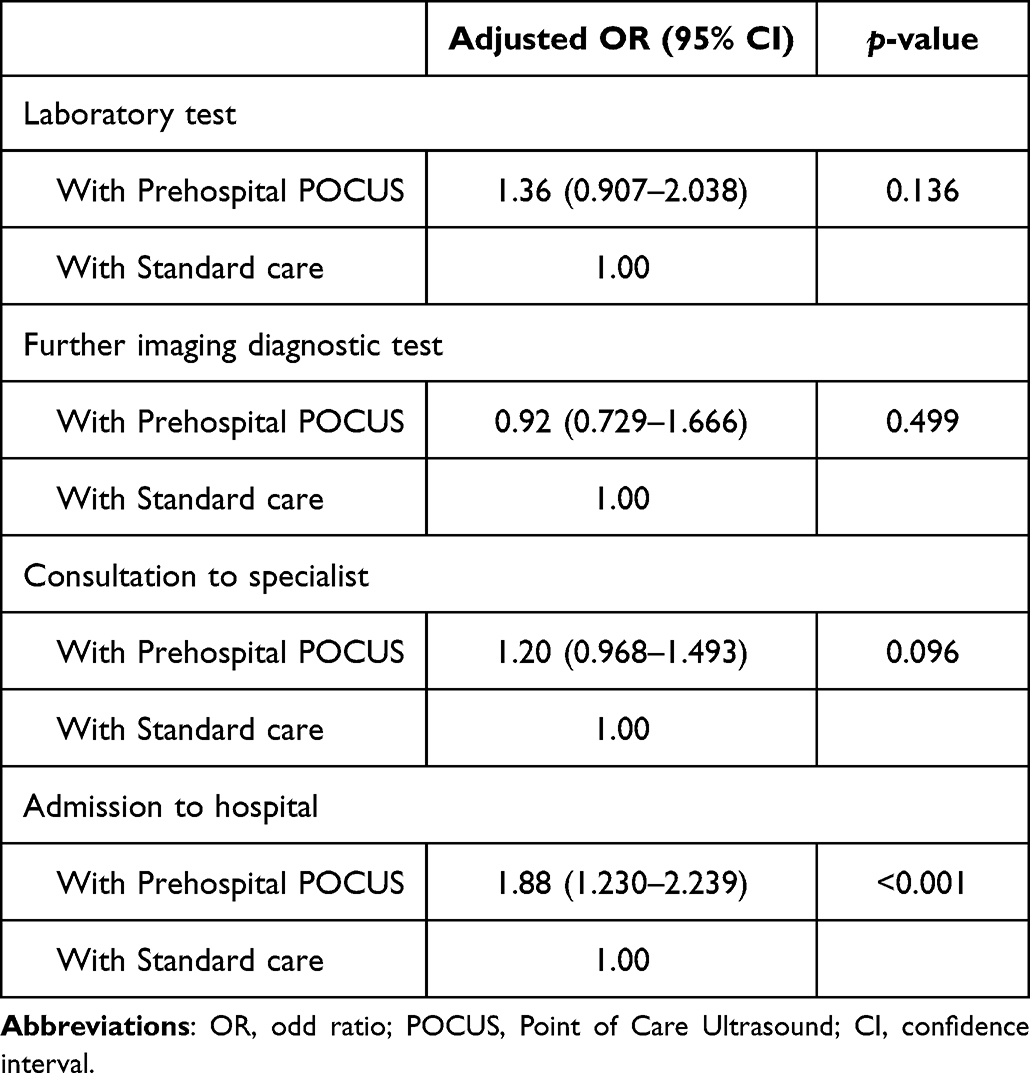 |
Table 2 Multivariable Analysis According to Prehospital POCUS on ED LOS of More Than 4 Hours |
Discussion
Crowding in the emergency department is a complex problem compounded by a wide variety of causes and has significant implications for the worldwide health-care system. Manpower, the number of patients, rate of arrival to the ED, inpatient bed availability, and delays in collecting diagnostic testing findings all influence LOS in the ED.29,30 One of the most promising solutions with real potential to reduce ED LOS is the bedside investigation such as point of care blood tests or bedside imaging tests including POCUS.31–33 However, these solutions remain controversial and are limited by the small number of studies, especially in terms of the contributions of the POCUS examination.32
This study was carried out on 169 patients who received prehospital POCUS and clearly demonstrated a shorter ED LOS (159 minutes) than the standard care group (165 minutes). Nevertheless, no statistically significant difference was observed for ED LOS between two groups. Our findings were consistent with the previous studies that showed a decrease in LOS in patients who had POCUS for various reasons.6,34–37 However, these studies performed POCUS in ED which differed from our study which focused on pre-ED scenarios.
The current study in Denmark38 demonstrates prehospital emergency medical technicians (EMTs) who performed POCUS and blood analysis in patients with chronic obstructive pulmonary disease indicated that roughly half of patients (49%) were treated and released at the scene. This study noticed 1) the prehospital POCUS can be performed by the different levels of emergency medical services personnel, 2) patients can be evaluated by using prehospital POCUS at the scene, and 3) some patients did not need to be admitted to the ED which could be significantly reduce ED overcrowding. However, this study had a small sample population (41/771). Moreover, the difference of our study from this study was the experience of individuals who performed POCUS and undertook the evaluation of patients. Another study39 reported prehospital POCUS in trauma patients for detection of free fluid in the abdomen could significantly hasten door-to-CT scan or door-to-operating theater time in abdominal trauma patients. However, this study demonstrated only the reduction of time to treatment.
Our results indicated that the prehospital POCUS group has a smaller number of EMS procedures than the control group. Moreover, all patients who obtained POCUS were medical patients and there were no cardiac patients in the study group. This may be due to 1) prehospital patients who need to perform a lot of EMS procedures such as trauma patients and cardiac arrest patients, EMS physician might have less time to perform the POCUS, which was an adjunction tool, and 2) the transportation time of our ambulance was approximately 10–15 minutes which was a short duration time.
Our study illustrated the prehospital POCUS group had a higher percentage of laboratory tests, consultation with a specialist, and admission to hospital compared to the standard care group. This implied that the nature of prehospital patients who receive POCUS in this study were complex patients which was likely why our EMS physician decided to perform prehospital POCUS to aid them in getting a rapid diagnosis. Thus, these patients need more investigation at the hospital and must consult a specialist for in hospital admission. Nevertheless, our study illustrated the percentage of further imaging investigation in the prehospital POCUS group was lower than the other group. Likewise, when adjusted for confounding factors, our study found the further imaging diagnostic tests in the prehospital POCUS group were lower adjusted OR (0.92) than the control group. This was consistent with several studies which have found that POCUS minimizes possible diagnoses and improves diagnostic effectiveness.40 The prehospital POCUS group had a higher percentage of admission to hospital than the standard care group. According to the input-throughput-output model, admission to hospital was the main output factor. Our previous study41 about ED overcrowding demonstrated requiring admission acquired highest OR (4.171) among other factors. Likewise, the prehospital POCUS group with admission to hospital was the critical factor which made ED LOS longer (adjusted OR 1.88). However, it was not statistically significant when compared to the other group.
The study’s limitations were 1) Our institution was a teaching hospital, which meant that the comorbidity and illness patterns were more severe and convoluted. According to the findings of this study, a significant number of patients who require investigation, consultation, and admission may be transferred to other institutions and have a longer LOS., 2) there were no set of guidelines for when to utilize POCUS in prehospital patients. It was dependent on physicians’ clinical judgment, which might lead to selection bias. 3) Although we had corrected the specified variables in the regression model, the factors impacting the LOS were multifactorial which were difficult to completely investigate, and 4) the data of this study presented is statistically insignificant; therefore, this study did not demonstrated the clinical outcome between these patients.
Conclusion
Prehospital POCUS obtained for EMS patients demonstrated shorter ED LOS than with the standard care without being statistically significant. This study suggested the availability of bedside investigation including POCUS may improve ED LOS for prehospital patients. We advocate all levels of EMS providers to expand the number of credentialed POCUS providers available for improving the prehospital and emergency care.
Abbreviations
ED, emergency department; POCUS, Point of Care Ultrasound; LOS, length of stay; OR, odds ratio; ED LOS, Emergency department length of stay; EMS, emergency medical services; EMR, electronic medical record; CIs, confidence intervals; EMTs, emergency medical technicians.
Data Sharing Statement
On reasonable request, the corresponding author will provide the data sets used and/or analyzed during the current work.
Ethics Approval and Informed Consent
This study was authorized by the the Khon Kaen University Ethics Committee for Human Research based on the Declaration of Helsinki and the ICH Good Clinical Practice Guidelines (HE651469). Because patient privacy was maintained by employing a unique research number, informed consent was waived.
Acknowledgment
The authors would like to express our sincere gratitude to Josh Macknick for acting as an English consultant.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Fundamental Fund of Khon Kaen University which has received funding support from the National Science, Research and Innovation Fund (NSRF).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Moskop JC, Geiderman JM, Marshall KD, et al. Another look at the persistent moral problem of emergency department crowding. Ann Emerg Med. 2019;74(3):357–364. doi:10.1016/j.annemergmed.2018.11.029
2. Andersson J, Nordgren L, Cheng I, Nilsson U, Kurland L. Long emergency department length of stay: a concept analysis. Int Emerg Nurs. 2020;53:100930. doi:10.1016/j.ienj.2020.100930
3. Boulain T, Malet A, Maitre O. Association between long boarding time in the emergency department and hospital mortality: a single-center propensity score-based analysis. Intern Emerg Med. 2020;15(3):479–489. doi:10.1007/s11739-019-02231-z
4. Ouyang H, Wang J, Sun Z, Lang E. The impact of emergency department crowding on admission decisions and patient outcomes. Am J Emerg Med. 2022;51:163–168. doi:10.1016/j.ajem.2021.10.049
5. Hashim A, Tahir MJ, Ullah I, Asghar MS, Siddiqi H, Yousaf Z. The utility of point of care ultrasonography (POCUS). Ann Med Surg. 2021;71:102982. doi:10.1016/j.amsu.2021.102982
6. Beals T, Naraghi L, Grossestreuer A, Schafer J, Balk D, Hoffmann B. Point of care ultrasound is associated with decreased ED length of stay for symptomatic early pregnancy. Am J Emerg Med. 2019;37(6):1165–1168. doi:10.1016/j.ajem.2019.03.025
7. Morgan BB, Kao A, Trent SA, et al. Effect of emergency physician-performed point-of-care ultrasound and radiology department-performed ultrasound examinations on the emergency department length of stay among pregnant women at less than 20 weeks’ gestation. J Ultrasound Med. 2018;37(11):2497–2505. doi:10.1002/jum.14607
8. Elikashvili I, Tay ET, Tsung JW, Costantino T. The effect of point-of-care ultrasonography on emergency department length of stay and computed tomography utilization in children with suspected appendicitis. Acad Emerg Med. 2014;21(2):163–170. doi:10.1111/acem.12319
9. Wilson SP, Connolly K, Lahham S, et al. Point-of-care ultrasound versus radiology department pelvic ultrasound on emergency department length of stay. World J Emerg Med. 2016;7(3):178–182. doi:10.5847/wjem.j.1920-8642.2016.03.003
10. Ienghong K, Cheung LW, Tiamkao S, Bhudhisawasdi V, Apiratwarakul K. The diagnostic capabilities of the combined cardiac and lung point of care ultrasound in shocked patients at the emergency department - resourced limited country. Eur J Radiol Open. 2022;9:100446. doi:10.1016/j.ejro.2022.100446
11. Apiratwarakul K, Cheung LW, Tiamkao S, et al. Smart glasses: a new tool for assessing the number of patients in mass-casualty incidents. Prehosp Disaster Med. 2022;37(4):480–484. doi:10.1017/S1049023X22000929
12. Yoon H, Kim SK, Lee Y, Choi J. Google glass-supported cooperative training for health professionals: a case study based on using remote desktop virtual support. J Multidiscip Healthc. 2021;14:1451–1462. doi:10.2147/JMDH.S311766
13. Shaddock L, Smith T. Potential for use of portable ultrasound devices in rural and remote settings in Australia and other developed countries: a systematic review. J Multidiscip Healthc. 2022;15:605–625. doi:10.2147/JMDH.S359084
14. Donovan JK, Burton SO, Jones SL, Meadley BN. Use of point-of-care ultrasound by non-physicians to assess respiratory distress in the out-of-hospital environment: a scoping review. Prehosp Disaster Med. 2022;37(4):520–528. doi:10.1017/S1049023X22000711
15. Burton SO, Donovan JK, Jones SL, Meadley BN. Can non-physician providers use ultrasound to aid in establishing peripheral IV access in patients who are difficult to cannulate? A scoping review. Prehosp Disaster Med. 2022;37(4):535–546. doi:10.1017/S1049023X22000796
16. Mercer CB, Ball M, Cash RE, Rivard MK, Chrzan K, Panchal AR. Ultrasound use in the prehospital setting for trauma: a systematic review. Prehosp Emerg Care. 2021;25(4):566–582. doi:10.1080/10903127.2020.1811815
17. Fitzgibbon JB, Lovallo E, Escajeda J, Radomski MA, Martin-Gill C. Feasibility of out-of-hospital cardiac arrest ultrasound by EMS physicians. Prehosp Emerg Care. 2019;23(3):297–303. doi:10.1080/10903127.2018.1518505
18. von Foerster N, Radomski MA, Martin-Gill C. Prehospital ultrasound: a narrative review [published online ahead of print, 2022 Oct 24]. Prehosp Emerg Care. 2022;1–13. doi:10.1080/10903127.2022.2132332
19. McCallum J, Vu E, Sweet D, Kanji HD. Assessment of paramedic ultrasound curricula: a systematic review. Air Med J. 2015;34(6):360–368. doi:10.1016/j.amj.2015.07.002
20. Hermann M, Hafner C, Scharner V, et al. Remote real-time supervision of prehospital point-of-care ultrasound: a feasibility study. Scand J Trauma Resusc Emerg Med. 2022;30(1):23. doi:10.1186/s13049-021-00985-0
21. Chen J, Dobron A, Esterson A, et al. A randomized, controlled, blinded evaluation of augmenting point-of-care ultrasound and remote telementored ultrasound in inexperienced operators. Isr Med Assoc J. 2022;24(9):596–601.
22. Rudolph SS, Sørensen MK, Svane C, Hesselfeldt R, Steinmetz J. Effect of prehospital ultrasound on clinical outcomes of non-trauma patients--a systematic review. Resuscitation. 2014;85(1):21–30. doi:10.1016/j.resuscitation.2013.09.012
23. Lucas B, Hempel D, Otto R, et al. Prehospital FAST reduces time to admission and operative treatment: a prospective, randomized, multicenter trial. Eur J Trauma Emerg Surg. 2022;48(4):2701–2708. doi:10.1007/s00068-021-01806-w
24. Bøtker MT, Jacobsen L, Rudolph SS, Knudsen L. The role of point of care ultrasound in prehospital critical care: a systematic review. Scand J Trauma Resusc Emerg Med. 2018;26(1):51. doi:10.1186/s13049-018-0518-x
25. Buaprasert P, Sri-On J, Sukhuntee J, et al. Diagnostic accuracy of extended focused assessment with sonography for trauma performed by paramedic students: a simulation-based pilot Study. Open Access Emerg Med. 2021;13:249–256. doi:10.2147/OAEM.S311376
26. Ienghong K, Cheung LW, Tiamkao S, Bhudhisawasdi V, Apiratwarakul K. The utilization of handheld ultrasound devices in a prehospital setting. Prehosp Disaster Med. 2022;37(3):355–359. doi:10.1017/S1049023X22000644
27. Šimundić AM. Measures of diagnostic accuracy: basic definitions. EJIFCC. 2009;19(4):203–211.
28. Scharonow M, Weilbach C. Prehospital point-of-care emergency ultrasound: a cohort study. Scand J Trauma Resusc Emerg Med. 2018;26(1):49. doi:10.1186/s13049-018-0519-9
29. Austin EE, Blakely B, Tufanaru C, Selwood A, Braithwaite J, Clay-Williams R. Strategies to measure and improve emergency department performance: a scoping review. Scand J Trauma Resusc Emerg Med. 2020;28(1):55. doi:10.1186/s13049-020-00749-2
30. Kenny JF, Chang BC, Hemmert KC. Factors affecting emergency department crowding. Emerg Med Clin North Am. 2020;38(3):573–587. doi:10.1016/j.emc.2020.04.001
31. Di Somma S, Zampini G, Vetrone F, et al. Opinion paper on utility of point-of-care biomarkers in the emergency department pathways decision making. Clin Chem Lab Med. 2014;52(10):1401–1407. doi:10.1515/cclm-2014-0267
32. Hausfater P, Hajage D, Bulsei J, et al. Impact of point-of-care testing on length of stay of patients in the emergency department: a cluster-randomized controlled study. Acad Emerg Med. 2020;27(10):974–983. doi:10.1111/acem.14072
33. Chaisirin W, Wongkrajang P, Thoesam T, et al. Role of point-of-care testing in reducing time to treatment decision-making in urgency patients: a randomized controlled trial. West J Emerg Med. 2020;21(2):404–410. doi:10.5811/westjem.2019.10.43655
34. Choi YA, Jung JY, Park JW, et al. Association between focused cardiac ultrasound and time to furosemide administration in acute heart failure. Am J Emerg Med. 2022;59:156–161. doi:10.1016/j.ajem.2022.07.020
35. Wang PH, Chen JY, Ling DA, et al. Earlier point-of-care ultrasound, shorter length of stay in patients with acute flank pain. Scand J Trauma Resusc Emerg Med. 2022;30(1):29. doi:10.1186/s13049-022-01017-1
36. Claiborne MK, Ng C, Breslin KA, Chamberlain J, Thomas-Mohtat R. The effect of point-of-care ultrasound on length of stay in the emergency department in children with neck swelling. Am J Emerg Med. 2021;48:295–300. doi:10.1016/j.ajem.2021.05.009
37. Lin MJ, Neuman M, Rempell R, Monuteaux M, Levy J. Point-of-care ultrasound is associated with decreased length of stay in children presenting to the emergency department with soft tissue infection. J Emerg Med. 2018;54(1):96–101. doi:10.1016/j.jemermed.2017.09.017
38. Nadim G, Laursen CB, Pietersen PI, et al. Prehospital emergency medical technicians can perform ultrasonography and blood analysis in prehospital evaluation of patients with chronic obstructive pulmonary disease: a feasibility study. BMC Health Serv Res. 2021;21(1):290. doi:10.1186/s12913-021-06305-7
39. Gamberini L, Tartaglione M, Giugni A, et al. The role of prehospital ultrasound in reducing time to definitive care in abdominal trauma patients with moderate to severe liver and spleen injuries. Injury. 2022;53(5):1587–1595. doi:10.1016/j.injury.2021.12.008
40. Weile J, Frederiksen CA, Laursen CB, Graumann O, Sloth E, Kirkegaard H. Point-of-care ultrasound induced changes in management of unselected patients in the emergency department - a prospective single-blinded observational trial. Scand J Trauma Resusc Emerg Med. 2020;28(1):47. doi:10.1186/s13049-020-00740-x
41. Ienghong K. Factors affecting length of stay more than 4 hours in the emergency department of Srinagarind hospital. SRIMEDJ. 2014;29(1):7–13.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.