Back to Journals » Journal of Inflammation Research » Volume 17
The Impact of Laparoscopic Appendectomy and Open Appendectomy on B7-H3-Mediated Intrinsic Immune Response in Children with Acute Suppurative Appendicitis
Authors Duan C, Li Y, Ma J, Song Y, Zhou L
Received 23 October 2023
Accepted for publication 1 February 2024
Published 11 March 2024 Volume 2024:17 Pages 1577—1587
DOI https://doi.org/10.2147/JIR.S446199
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Chunsheng Duan, Yuan Li, Jiansu Ma, Yanglin Song, Lixia Zhou
Department of Pediatric Surgery, Xingtai People’s Hospital, Xingtai, Hebei, 054000, People’s Republic of China
Correspondence: Lixia Zhou, Department of Pediatric Surgery, Xingtai People’s Hospital, 16 Hongxing Street, Xingtai, Hebei, 054000, People’s Republic of China, Tel/Fax +86-0319-3286096, Email [email protected]
Purpose: Surgery impairs immune function and increases postoperative complications. B7H3, a co-stimulatory molecule, plays a crucial role in immune regulation. The present study examined the impact of B7H3 on the postoperative immune response in children with acute suppurative appendicitis (ASA) by comparing preoperative and postoperative B7H3 levels in laparoscopic surgery (LA) and open appendectomy (OA).
Patients and Methods: 198 pediatric ASA patients were enrolled. The researcher group performed LA, while the control group performed OA. Perioperative time, recovery time of gastrointestinal function, time to pass gas, length of incision, and length of hospitalization were compared in the perioperative period. Additionally, an ELISA assay was conducted to examine the levels of inflammatory factors and B7H3 and CD28. Short-term postoperative complications were also evaluated.
Results: Compared with the control group, the research group had a short operative time, gastrointestinal function recovery time, gas time, and hospitalization time. The short-term complication rate was significantly lower in the research group. More importantly, B7H3 and CD28 were insignificantly different preoperatively, but they were all reduced postoperatively. Moreover, the reduction was more pronounced in the research group. The same results were noted in inflammatory factors and immune markers, which were non-significant different preoperatively and were typically reduced postoperatively, particularly in the research group. Finally, postoperative B7H3 was positively correlated with both inflammatory factors and immune cell levels.
Conclusion: B7H3 was reduced in both postoperative periods, and the reduction was more pronounced in the LA group. B7H3 may be involved in postoperative recovery by modulating postoperative inflammation and immune responses.
Keywords: ASA, laparoscopic surgery, open appendectomy, B7H3, CD298
Introduction
Acute appendicitis is the most predominant cause of acute abdominal infections in children, with a prevalence of 1–8% in children with acute abdominal pain, characterized by severe disease, rapid progression, and atypical physical signs.1,2 Due to the lower inflammatory response capacity of the pediatric organism and the thin wall of the appendix, it is often found to be in acute suppurative appendicitis (ASA). If left untreated 24.68% of pediatric ASA can progress to appendiceal perforation, posing a serious threat to the life.3 Surgery is currently the main treatment for ASA; however, traditional open appendectomy (OA) is more traumatic, and children recover more slowly.4 With the continuous development of minimally invasive techniques, laparoscopic appendectomy (LA) has gradually become a common surgical procedure for pediatric ASA, which is less invasive and facilitates patient recovery.5 However, surgical procedures including appendectomy, can lead to an imbalance in the immune system, creating an inflammatory response that affects the patient’s condition.6
Immune imbalances and disorders are critical in infectious diseases. Co-stimulatory molecules and their networks play an important regulatory role in the efficient initiation, moderate effect, and timely abortion of immune responses. B7 homolog 3 (B7H3), also known as CD276 or B7RP-2, was first identified as a member of the B7 family in 2000 years and was first isolated from a human dendritic cell cDNA library.7 Previous studies have found that B7H3 is aberrantly expressed in tumors and infectious diseases and participates in immune-associated inflammatory responses. For example, B7H3 is abnormally reduced in patients with systemic lupus erythematosus.7 Circulating B7H3 assesses the intensity of infectious inflammatory processes in the central nervous system of children and can differentiate between bacterial and aseptic meningitis. B7H3 ameliorates LPS-induced acute lung injury by inhibiting neutrophil migration and infiltration.8 Furthermore, targeting B7-H3/CD28 has been proposed as a new biological and clinical therapeutic strategy.9 More importantly, Du et al research in 2020 found that B7H3 was on the rise in pediatric AA patients but was not diagnostically effective in differentiating pediatric ASA from noma appendicitis.10 However, the levels of B7-H3 are unknown in pediatric ASA patients treated with LA and OA.
This study compared the changes in B7H3 levels between LA and OA in the treatment of ASA in an attempt to analyze whether the difference in treatment outcomes between the two surgical modalities was related to the immune dysregulation caused by B7H3 levels.
Materials and Methods
Participants in This Research
One hundred and ninety-eight pediatric ASA patients who were seen at Xingtai People’s Hospital from January 2017 to June 2021 and underwent appendectomy were included. Inclusion criteria were: 1) age less than 14 years; 2) meeting the diagnostic criteria for ASA; 3) patients with fixed pressure points in the right lower abdomen and elevated white blood cell count; 4) imaging studies show edema of the appendix, which is confirmed by routine blood tests, ultrasound, abdominal CT, and laparoscopy; 5) first time of illness; 6) undergoes preoperative cardiopulmonary function tests, and is refractory to the surgery. Exclusion criteria: 1) Combined hepatic, renal, and other organ pathologies; 2) Combined coagulation disorders or autoimmune system disorders; 4) Recent administration of anti-inflammatory or anti-immune drugs. Patients are predominantly OA until 2019 and LA from 2019 onwards. 95 patients with OA (51 males, and 7.9±2.8 years old) served as the control group, and 103 patients with LA (56 males, and 7.5±2.3 years old) served as the Research group.
The study was conducted after approval by the Medical Ethics Committee of Xingtai People’s Hospital and the experiments were by the guidelines of the Declaration of Helsinki. The guardians of the children signed an informed consent form.
Surgical Procedures
The research group used LA methods. Tracheal intubation was performed under general anesthesia, and the child was placed in the supine position. A 1 cm curved incision was made next to the umbilicus, and the Trocar was inserted, and CO2 pneumoperitoneum was established. Pressure was maintained at 8–12 mm Hg and Trocar puncture points (0.5 cm each) were placed above the symphysis pubis in the left lower abdomen and at McBurney’s point. After suctioning the purulent cavity fluid and separating the tissue, the appendix mesentery was exposed. The mesentery of the appendix was managed in the avascular area and ligated with a 2–0 silk suture. It was ligated and transected 0.5 cm from the base of the appendix, with electrocoagulation of the residual mucosa. The appendix was removed using a 10 mm trocar, the purulent fluid was cleaned out, and the abdominal cavity was irrigated until the irrigation fluid became clear. The accumulated fluid in each space was absorbed by a negative pressure aspirator, the incision was sutured, and finally, antibiotics were given for treatment.
The control group underwent OA surgery. General anesthesia for tracheal intubation, with the child in the supine position. An oblique or transverse incision of approximately 5 cm in length is made in the right lower abdomen through the point of McBurney according to the previous studies.11 Subcutaneous tissue was incised in layers, avoiding large blood vessels, fully exposing the appendix, which was lighted and excised, and wet gauze was used to wipe the right lower abdominal and pelvic cavities. The decision to place an abdominal drain is based on the volume and nature of the abdominal pus and abdominal washout. The incision was sutured.
Postoperative Management
After routine postoperative, two groups of pediatric patients are given combined antibiotics for anti-infection treatment, with cefuroxime and metronidazole being administered. Unless the patient is allergic to cefuroxime, quinolone antibiotics and metronidazole should be used. Semi-recumbent position is maintained for 6 h after surgery, and appropriate movement is advised after gas discharge. Antibiotics should be discontinued when clinical symptoms disappear, body temperature remains normal for 24–48 h, and white blood cell and neutrophil ratio return to normal.
Clinical Baseline and Perioperative Indicators
Preoperative clinical baseline characteristics including age, gender, disease duration, admission temperature, and systolic and diastolic blood pressure were recorded for both groups of children. Perioperative data such as operation time, recovery time of gastrointestinal function, time of defecation, time of incision, length of incision, and hospitalization time were also recorded. A visual analog scale (VAS) score was used to assess the level of pain in the children preoperatively and 3 days postoperatively. The score of which was 0–10, with higher scores indicating more severe pain. The total intraoperative blood loss is measured by subtracting the total weight of gauze from the combined weight of gauze with blood and adding the volume of blood in the suction bottle.
Inflammatory and Immune Indicators
Preoperative and 7 days postoperatively, 3 mL of fasting venous blood was collected from both groups and centrifuged at 2500 rpm/min for 10 min. The serum of the upper part of the blood was taken and the concentrations of interleukin (IL)-8 (#ab214030, Abcam), IL-6 (#ab178013, Abcam), tumor necrosis factor (TNF)-α (#ab181421, Abcam), C-reactive protein (CRP, #ab260058, Abcam), B7H3 (#ab221831, Abcam) and CD28 (#BMS290, Invitrogen) were measured by enzyme-linked immunosorbent assay (ELISA) commercial kit. Lymphocytes, neutrophils, and leukocytes were detected by blood smear method.
Postoperative Complication
Complications, including incision infections, mesenteric adhesions, and early inflammatory bowel obstruction, were recorded in the short-term postoperative period in both groups. Children with incision infection should be cleaned and disinfected with povidone-iodine, and in severe cases, debridement surgery should be performed to remove pus and necrotic tissue from the wound and change the dressing regularly. In contrast, children with mesenteric adhesions were treated with abdominal massage, breathing exercises, and infrared electrotherapy. The patient’s diagnosis of mesenteric adhesions is determined by the presence of symptoms such as abdominal pain, bloating, nausea, vomiting, cessation of gas, and stool passage. Children with intestinal obstruction were treated with strict fasting and water fasting, parenteral nutritional support, indwelling gastric tube for gastrointestinal decompression, growth hormone inhibitors, and antimicrobial drugs. There were no reoperations for patients with intestinal obstruction.
Statistical Analysis
SPSS 23.0 and GraphPad Prism 9.0 software for statistical analysis and visualization of data. Measurements were expressed as mean ± SD, and differences between groups were tested using the T-test. Count data were presented as n (%), and differences between groups were tested using the chi-square test. P < 0.05 was considered a statistically significant difference.
Results
Clinical Baseline and Perioperative Indicators in Two Groups of Pediatric ASA Patients
The surgery procedures were completed in both groups, and none of the pediatric patients in the research group who underwent LA were converted to OA. Moreover, as presented in Table 1, the two groups of pediatric ASA patients had non-statistically different clinical baseline characteristics in terms of age, gender, disease duration, admission temperature, and admission systolic and diastolic blood pressure (P > 0.05). However, compared to the control group, the research group had shorter operation time, gastrointestinal function recovery time, exhaust time, incision time, and incision length as well as hospital stay (P < 0.05, Table 1).
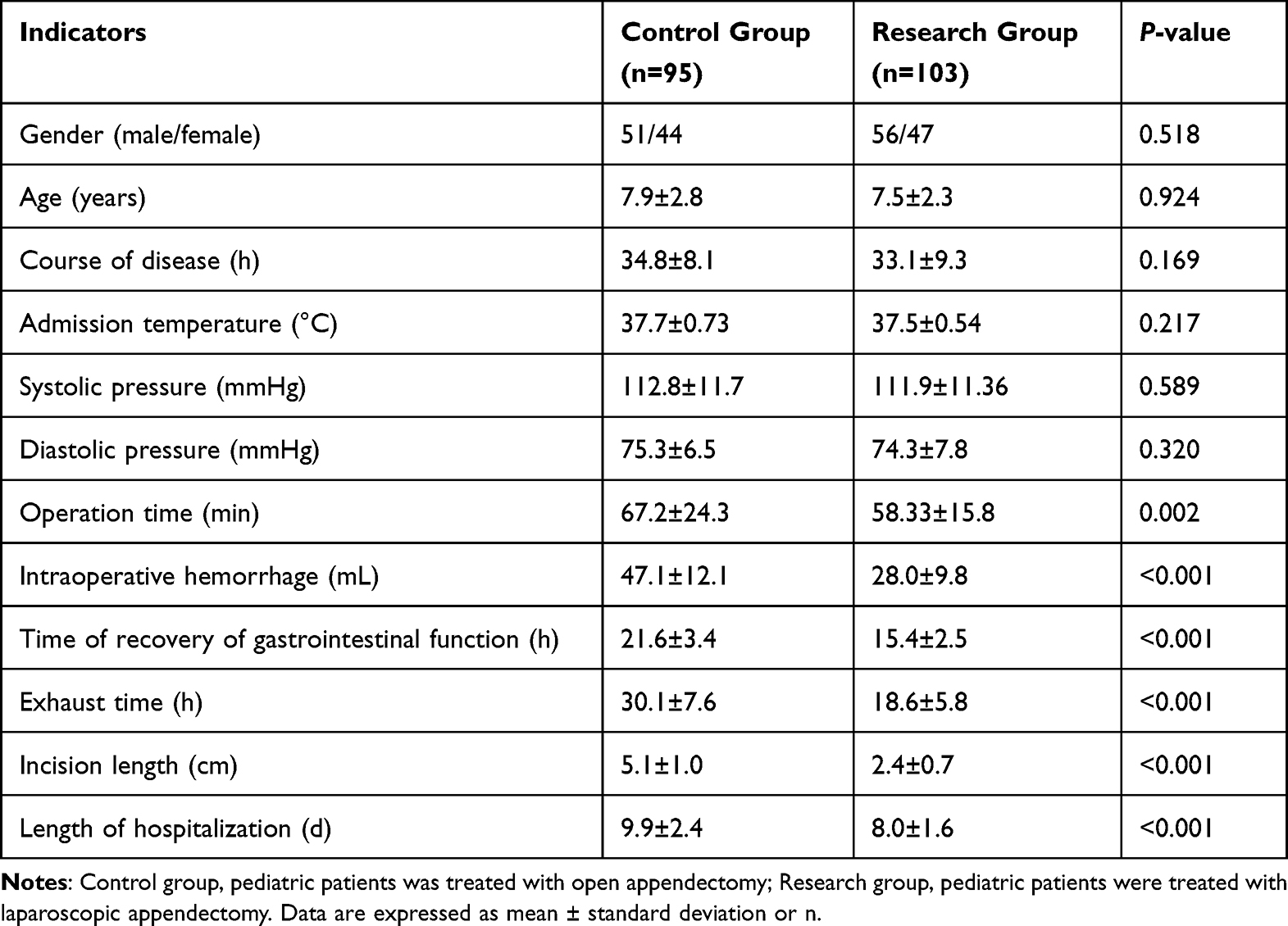 |
Table 1 Clinical Data of the Study Subjects |
VAS scores, a pain indicator, were not significantly different between the two groups preoperatively but were sharply decreased in both groups postoperatively. Notably, the research group exhibited a more pronounced reduction compared to the control group (P < 0.05, Figure 1A and B).
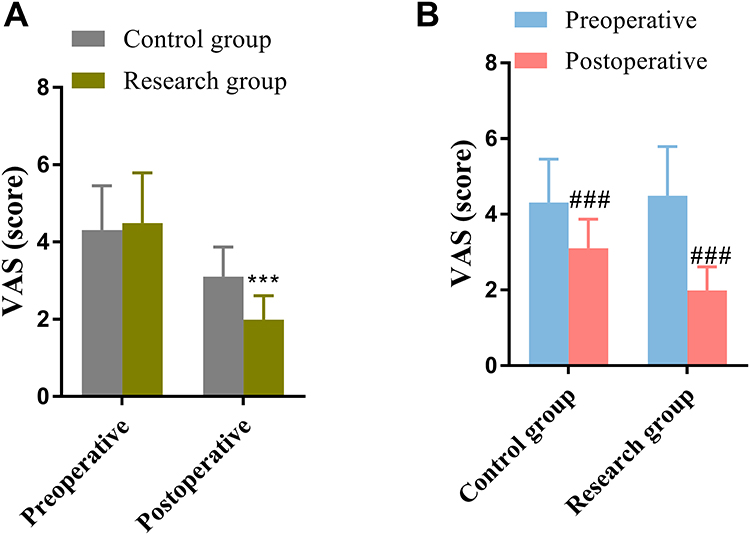 |
Figure 1 Changes in VAS score of patients in both groups preoperatively and postoperatively. (A) Inter-group comparison of preoperative and postoperative VAS score changes in the two groups of patients, respectively. (B) Within-group comparisons were made to analyze the difference between preoperative and postoperative VAS scores. ***P < 0.001, vs postoperative control group; ###P < 0.001 vs Preoperative control group or preoperative research group. |
Preoperative and Postoperative Inflammatory Factor Levels in Both Groups of Pediatric
Subsequently, inflammatory indicators were analyzed. No significant differences were found in CRP, IL-8, IL-6, and TNF-α between the two groups preoperatively, but they were all significantly reduced at 1 week postoperatively compared with preoperatively (P < 0.05, Figure 2A–H, Supplemental Table 1). Importantly, serum CRP, IL-8, IL-6, and TNF-α of the research group were significantly lower than those in the control group (P < 0.05, Figure 2A–H, Supplemental Table 1).
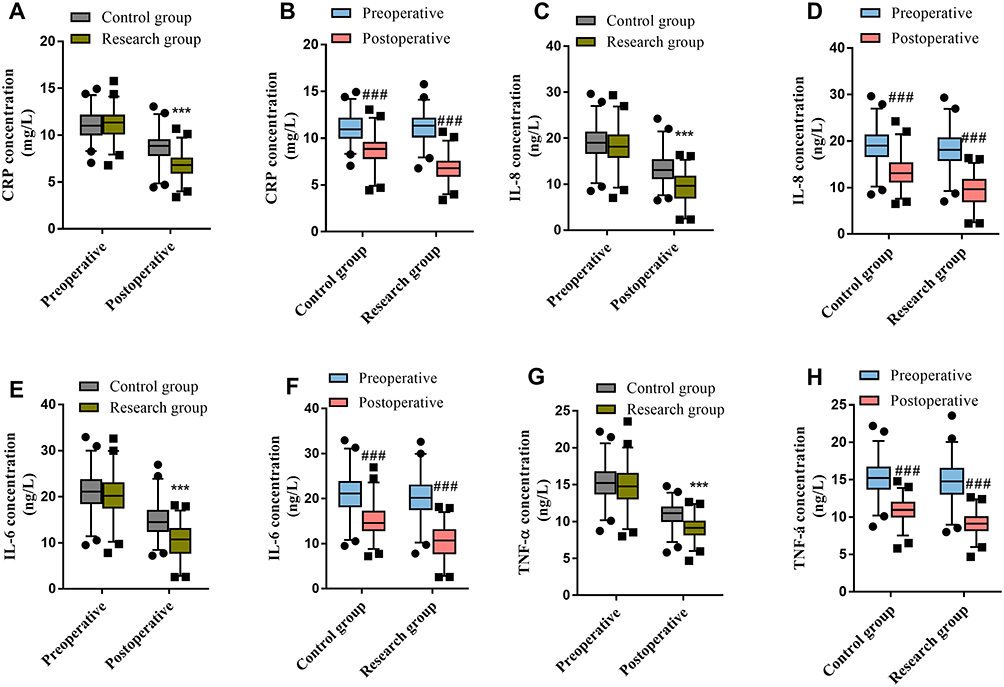 |
Figure 2 Comparison of preoperative and postoperative inflammatory indicators in two groups of children. (A and B) preoperative and postoperative CRP levels in both groups. (C and D) preoperative and postoperative IL-8 levels in both groups. (E and F) preoperative and postoperative IL-6 levels in both groups. (G and H) preoperative and postoperative TNF-α levels in both groups. ***P < 0.001 vs postoperative control group; ###P < 0.001 vs Preoperative control group or preoperative research group. |
Comparison of Preoperative and Postoperative Immune Markers
Lymphocytes, neutrophils, and leukocytes were not statistically different between the two groups preoperatively, but they were all significantly more reduced one week postoperatively compared to preoperatively (P < 0.05, Figure 3A–F, Supplemental Table 1). Additionally, lymphocytes, neutrophils, and leukocytes were significantly lower in the research group than in the control group postoperatively (P < 0.05, Figure 3A–F, Supplemental Table 1).
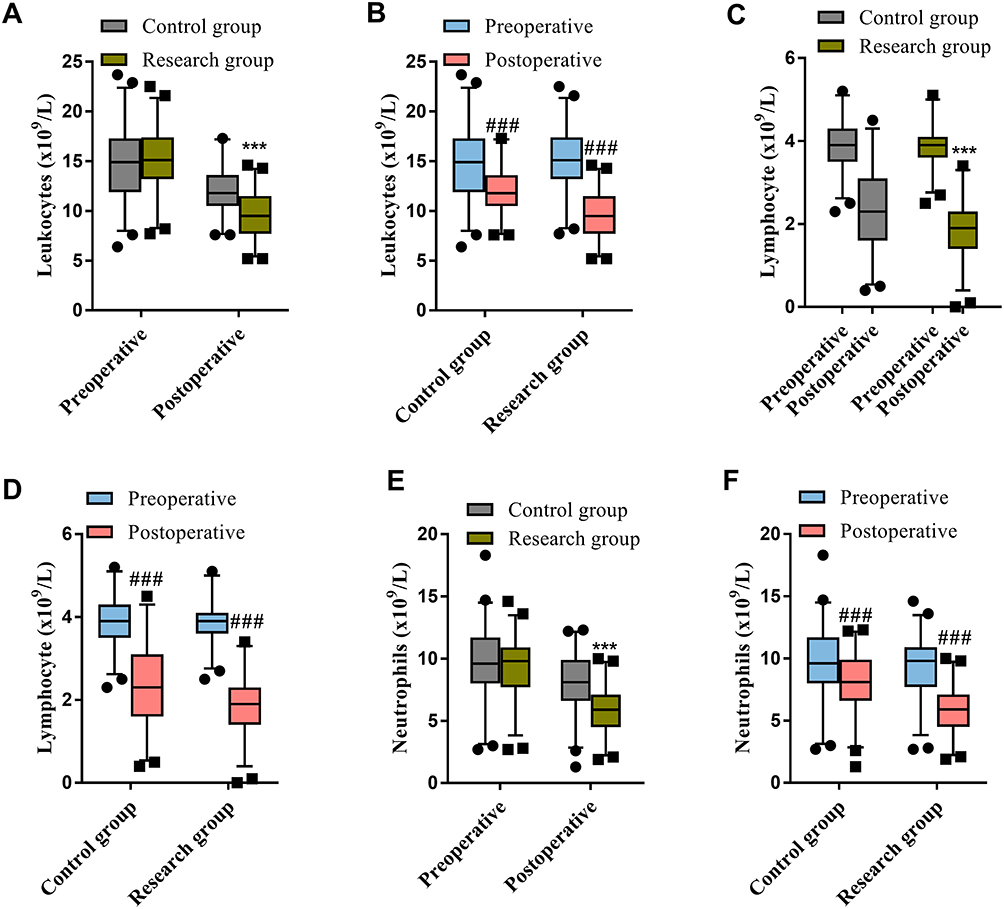 |
Figure 3 Comparison of leukocytes (A and B), lymphocytes (C and D), and neutrophils (E and F) between the two groups of patients preoperatively and postoperatively. ***P < 0.001 vs postoperative control group; ###P < 0.001 vs Preoperative control group or preoperative research group. |
B7H3 and CD28 Expression in the Preoperative and Postoperative Period
CD28/B7H3 signaling is strongly recommended with adaptive immunity and reflects the degree of immune dysfunction. B7H3 and CD28 were not statistically different between the two groups of children preoperatively, but they were both significantly lower postoperatively (P < 0.05, Figure 4A–D). In addition, B7H3 levels were notably lower in the research group than in the control group (P < 0.05, Figure 4A–D). Pearson’s correlation coefficients showed a significant positivity correlation between B7H3 and lymphocytes, neutrophils, and leukocytes, which are postoperative immune indicators, as well as CRP, IL-6, IL-8, and TNF-α, which are inflammatory indicators (P < 0.05, Table 2).
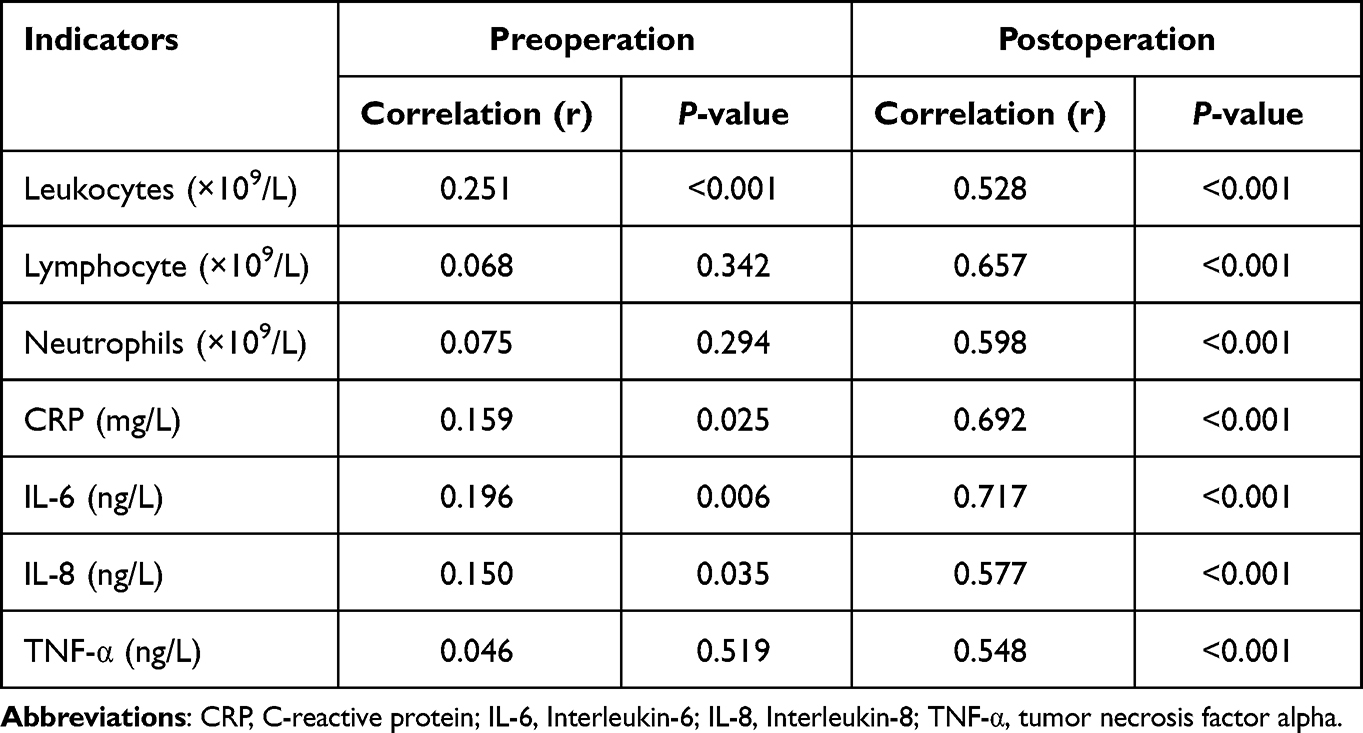 |
Table 2 Correlation Between B7H3 and Various Inflammatory Markers in the Subjects |
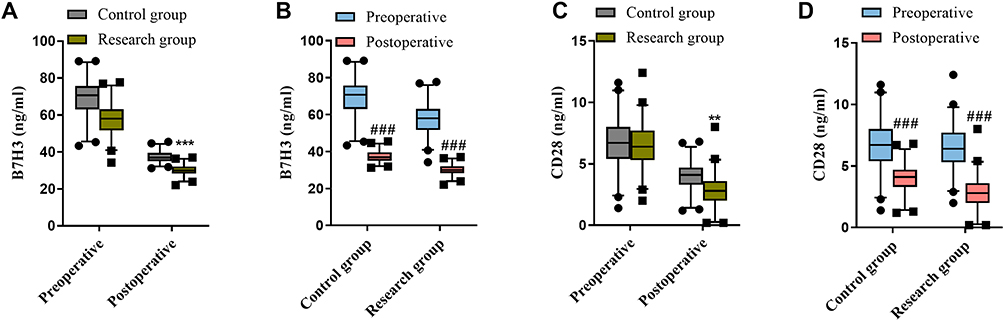 |
Figure 4 Comparison of B7H3 (A and B) and CD28 (C and D) between the two groups of patients preoperatively and postoperatively. **P < 0.01, ***P < 0.001 vs postoperative control group; ###P < 0.001 vs Preoperative control group or preoperative research group. |
Comparison of Short-Term Postoperative Complications
Ten complications occurred in the short-term postoperative period in both groups, and there were no children with two or more complications. 2 incision infections, 3 mesenteric adhesions, and 3 postoperative intestinal obstruction were found in the control group, and 1 incision infection and 1 intestinal obstruction were found in the research group. The overall rate of postoperative complications was significantly lower in the research group (1.94%) than in the control group (8.42%, P < 0.05, Table 3).
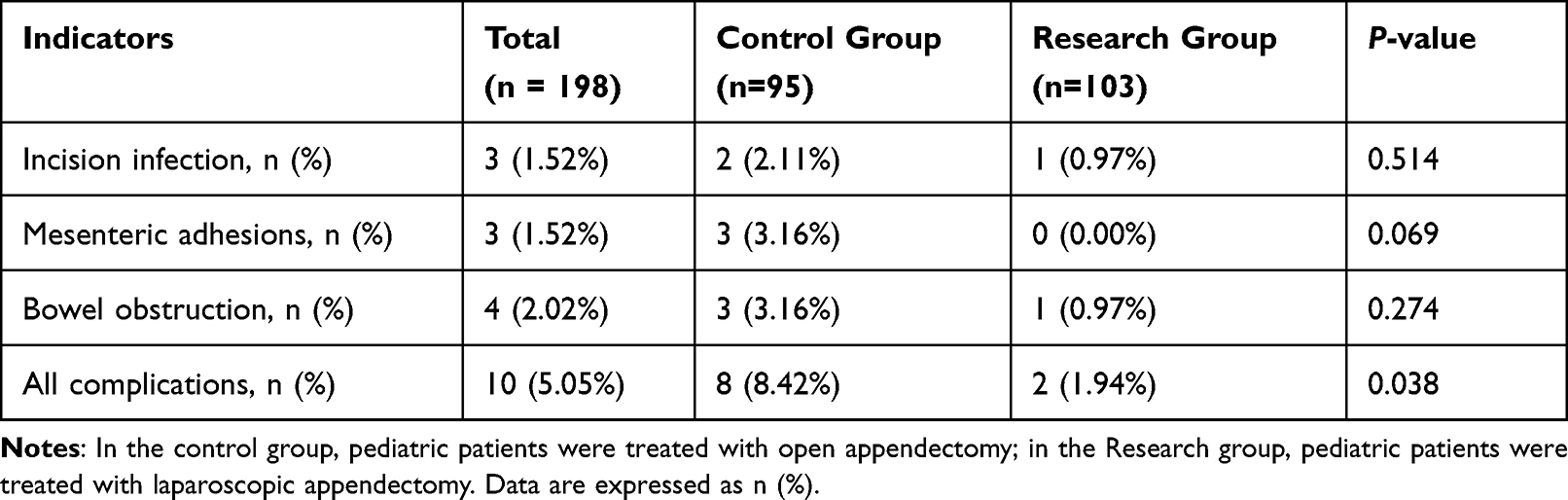 |
Table 3 Complications Occur After Resection in Pediatric Patients with Acute Suppurative Appendicitis |
Discussion
ASA is a condition in which the lesion has invaded the entire appendiceal wall, with marked swelling of the appendix and elevation of the outer appendiceal plasma membrane.12 Due to the small size of the appendix in early childhood, the appendix wall is weak, with little basal tissue, and when circulatory disorders of appendiceal blood flow occur, the appendix is locally ischemic and necrotic, which is conducive to the propagation and growth of pathogens. Therefore, ASA was previously reported to be the dominant cause of acute abdominal infections in children.13 Surgery is the usual treatment for ASA, with approximately 370,000 patients undergoing appendectomy each year in the United States,14 70,000 of which are pediatric surgeries, and the average cost is $9000.15
Certain variability exists between OA and LA in the treatment of patients with ASA.16 OA, as a traditional and mature surgical procedure, is associated with high trauma, and severe damage to the body. Also, in children with abdominal abscesses and diffuse inflammation, a small incision open abdomen has a relatively small field of view, and it is impossible to determine the amount of pus and abdominal inflammation, so OA has some limitations. LA, as a minimally invasive procedure combining modern surgical techniques with endoscopic techniques and a wide surgical field, is now widely used in pediatric ASA patients. However, due to the specificity of ASA and its complications, LA as the first treatment modality for septic appendicitis is still somewhat controversial.17 In the present study, we first compared the effects of the two procedures on perioperative indicators of pediatric ASA. Children with LA have shorter operative time, gastrointestinal recovery time, venting time, incision length, and length of hospitalization than patients with OA, and this is consistent with previously reported outcomes.18 In addition, we found a significantly lower incidence of short-term complications in children who underwent LA than in children with OA, this is consistent with previous research.19 In conclusion, we verified that LA was more effective than OA in terms of perioperative and postoperative complications.
The surgical procedure can result in compromised immune function, rendering the body more vulnerable to microorganisms, and impacting both systemic system and tissue cells, thereby increasing the likelihood of postoperative complication.20 The levels of several cytokines are significantly altered postoperatively and are mainly involved in the inflammatory response and the regulation of the immune response to maintain homeostasis in the body.21 Chawla LS’s analysis in 2016 found that immune cells in ASA patients were not directly activated by pathogens but were triggered by diffusion factors in the infected microenvironment, which involved immune mechanisms.22 Therefore, we first analyzed the changes in different inflammatory factors between the two surgeries in children preoperatively and postoperatively. IL-6 has been identified as a disease-related biomarker of appendicitis. In a recent study on specific metabolomics and mass spectra of inflammatory mediators in pediatric acute appendicitis, IL-6 and CRP were the most unique inflammatory biomarkers.23,24 In addition, studies have confirmed that high IL-8 levels are observed in the appendix, peritoneal fluid, and serum during acute appendicitis.25 The mRNA levels of TNF-α were also strongly elevated in ASA.26 In our study, we found that there was no significant difference in CRP, IL-6, IL-8, and TNF-α between the two groups of patients preoperatively, but the levels of secretion were significantly reduced postoperatively, suggesting that both surgeries achieved the therapeutic effect of alleviating ASA by suppressing inflammatory secretion. In contrast, LA suppressed inflammation more significantly than OA, suggesting that OA may require more inflammatory factors to maintain homeostatic balance. Previous studies have documented that the secretion of inflammatory factors triggers an in vivo immune response, while foreign antigens may be introduced during surgical procedures.27 These antigens interact with specific T cells, leading to adaptive immune responses involving antigen presentation and T-cell activation, which necessitate the involvement of co-stimulatory signaling molecules. We further analyzed the immunity indexes and found that the number of leukocytes, neutrophils, and lymphocytes did not differ significantly between the two groups before the operation, but decreased significantly after the operation, suggesting that appendectomy not only affects the inflammatory response but also leads to the impairment of the body’s immune function. In addition, the immune indexes of LA were reduced more significantly than OA, suggesting that LA is more conducive to the protection of the patient’s immune function.
ASA is the predominant cause of acute abdominal infections in children, and immune dysfunction and disorders are critical in ASA. The significance of co-stimulatory molecules and their networks in the effective initiation, moderate effect, and timely abortion of immune responses. B7H3 belongs to the B7-CD28 pathway and is thought to be an immune checkpoint molecule regulating T cell and NK cell viability in infectious diseases.28 Recent studies have shown that B7H3 is also involved in innate immune-related inflammatory response. In intrinsic immunity, B7H3 can act as a co-stimulatory molecule to enhance the release of inflammatory factors. B7H3 is significantly elevated in plasma and cerebrospinal fluid, which can be diagnosed in patients with sepsis and bacterial meningitis.29,30 Furthermore, B7H3 ameliorated LPS-induced acute lung injury by attenuating neutrophil migration and infiltration.8 B7H3-deficient mice develop more severe airway inflammation and earlier onset of experimental autoimmune allergic encephalomyelitis.31 B7H3 is associated with the pathogenesis of asthma, arthritis, and allergic conjunctivitis.32,33 Surgery can also affect B7H3 expression. For example, a study by Li et al in 2016 found that the plasma B7H6 was significantly lower on postoperative day 7 in both children undergoing pediatric general and cardiac general and was significantly lower in cardiac surgery than general surgery.21 In our study, we found that the expression of B7H3 and CD28 was insignificant difference in the preoperative period in the two groups, but were greatly reduced in the postoperative period, which is consistent with the findings of Li et al. This suggested that the changes in B7H3/CD28 signaling were all caused by surgical stress. Meanwhile, we also found a significant positive correlation between B7H3 and both inflammatory indicators and immune factor levels. This suggests that the therapeutic effect of surgery on ASA may be because the reduction of B7H7 levels inhibits its mediated inflammatory and adaptive immune response and thus alleviates the condition. In addition, we found that B7H3 was more significantly reduced in LA than OA. Suggesting that fewer complications and faster recovery in LA may also be related to the immune co-regulation of B7H3. In conclusion, the significant difference in outcome between the two surgical treatments may be related to B7H3-mediated immunomodulation, and LA may have a more positive correspondence of B7H3-mediated immune response than OA. This provides the possibility for clinical practice, perhaps through in vitro anti-B7H3 antibodies that can reduce the immune response in laparoscopic surgery and serve to alleviate postoperative complications and increase the therapeutic effect.
In addition, this study also has certain limitations. As this study serves as an initial exploration of the relationship between B7H3 and appendectomy methods and complications, it involves various aspects including clinical, postoperative, and postoperative comparisons to ensure the clinical outcomes are associated with B7H3, which may lead to relatively scattered data. However, we will focus on exploring B7H3, inflammation, and specific molecular mechanisms in the later stage. Furthermore, the duration of antibiotic treatment in both groups was not collected for all patients in this study as it was based on the patients’ postoperative recovery. Finally, it is essential to further expand the clinical samples and explore potential mechanisms.
Conclusion
LA is more effective than OA in blocking the excessive production of inflammatory factors and intrinsic immune imbalance by reducing B7H3, which is more beneficial to the postoperative recovery of patients.
Abbreviations
ASA, acute suppurative appendicitis; B7H3, B7 homolog 3; CRP, C-reactive protein; ELISA, enzyme-linked immunosorbent assay; IL, interleukin; LA, laparoscopic appendectomy; OA, open appendectomy; TNF, tumor necrosis factor; VAS, visual analog scale.
Funding
This study was funded by the Medical Science Research Project of Hebei Province (20201585).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kono J, Yoshimaru K, Matsuura T, et al. COVID19 detection in appendix of acute appendicitis in a child: a case report and review of literature. Surg Case Rep. 2023;9(1):37. doi:10.1186/s40792-023-01618-7
2. Nishimura K, Terui K, Mise N, et al. Larger physique as a risk factor for infantile appendicitis: a Retrospective Study. Pediatr Rep. 2022;14(1):20–25. doi:10.3390/pediatric14010004
3. Wu J, Lu AD, Zhang LP, Zuo YX, Jia YP. 儿童核心结合因子相关性急性髓系白血病疗效及预后因素分析 [Study of clinical outcome and prognosis in pediatric core binding factor-acute myeloid leukemia]. Zhonghua Xue Ye Xue Za Zhi. 2019;40(1):52–57. Chinese. doi:10.3760/cma.j.issn.0253-2727.2019.01.010
4. Cherif M, Mesbahi M, Zaafouri H, et al. Laparoscopic appendicectomy: risk factors for conversion to laparotomy. Arq Bras Cir Dig. 2023;36:e1737. doi:10.1590/0102-672020230019e1737
5. Wang B, Shi L, Fu W, Liu T. Effects of sequence of irrigation, suction, and extraction in cases of acute purulent appendicitis or gangrenous perforated appendicitis after laparoscopic appendectomy. J Laparoendosc Adv Surg Tech A. 2021;31(7):751–755. doi:10.1089/lap.2020.0610
6. Cury DB, Oliveira R, Cury MS. Inflammatory bowel diseases: time of diagnosis, environmental factors, clinical course, and management - a follow-up study in a private inflammatory bowel disease center (2003–2017). J Inflamm Res. 2019;12:127–135. doi:10.2147/JIR.S190929
7. Sun J, Lai H, Shen D, et al. Reduced sB7-H3 expression in the peripheral blood of systemic lupus erythematosus patients. J Immunol Res. 2017;2017:5728512. doi:10.1155/2017/5728512
8. Li Y, Huang J, Foley NM, et al. B7H3 ameliorates LPS-induced acute lung injury via attenuation of neutrophil migration and infiltration. Sci Rep. 2016;6:31284. doi:10.1038/srep31284
9. Pulanco MC, Madsen AT, Tanwar A, Corrigan DT, Zang X. Recent advancements in the B7/CD28 immune checkpoint families: new biology and clinical therapeutic strategies. Cell Mol Immunol. 2023;20(7):694–713. doi:10.1038/s41423-023-01019-8
10. Du X, Chen Y, Zhu J, et al. sB7H3 in children with acute appendicitis: its diagnostic value and association with histological findings. J Immunol Res. 2020;2020:2670527. doi:10.1155/2020/2670527
11. Yingchu H, Gelin Z, Guanxuan L, Surgery PC. Postoperative immune and inflammatory responses after laparoscopic surgery in children with acute suppurative appendicitis. Journal of New Medicine. 2018;49:757–761.
12. Zhang N, Li Y, Zhou R, Teekaraman Y. Comparison of single-person laparoscopic appendectomy using a novel brace-assisted camera holding system and conventional laparoscopic appendectomy: a neural network algorithm analysis. Contrast Media Mol Imaging. 2022;2022:5915670. doi:10.1155/2022/5915670
13. Shen Z, Sun P, Jiang M, et al. Endoscopic retrograde appendicitis therapy versus laparoscopic appendectomy versus open appendectomy for acute appendicitis: a pilot study. BMC Gastroenterol. 2022;22(1):63. doi:10.1186/s12876-022-02139-7
14. Hayes D, Tan M, Wang M, Weinsheimer R. A multi-institutional approach for decreasing narcotic prescriptions after laparoscopic appendectomy. Surg Endosc. 2022;36(8):6250–6254. doi:10.1007/s00464-022-09107-y
15. Mosuka EM, Thilakarathne KN, Mansuri NM, et al. A systematic review comparing nonoperative management to appendectomy for uncomplicated appendicitis in children. Cureus. 2021;13(10):e18901. doi:10.7759/cureus.18901
16. Zachos K, Kolonitsiou F, Panagidis A, et al. Association of the bacteria of the vermiform appendix and the peritoneal cavity with complicated acute appendicitis in children. Diagnostics. 2023;13(11). doi:10.3390/diagnostics13111839
17. Shiihara M, Sudo Y, Matsushita N, et al. Therapeutic strategy for acute appendicitis based on laparoscopic surgery. BMC Surg. 2023;23(1):161. doi:10.1186/s12893-023-02070-y
18. Liu T, Jiang K, Bi Y. Endoscopic retrograde appendicitis therapy in a pregnant patient with acute septic appendicitis. Asian J Surg. 2022;45(10):2070–2071. doi:10.1016/j.asjsur.2022.04.098
19. Zhang G, Wu B. Meta-analysis of the clinical efficacy of laparoscopic appendectomy in the treatment of acute appendicitis. World J Emerg Surg. 2022;17(1):26. doi:10.1186/s13017-022-00431-1
20. Furak J, Paroczai D, Burian K, Szabo Z, Zombori T. Oncological advantage of nonintubated thoracic surgery: better compliance of adjuvant treatment after lung lobectomy. Thorac Cancer. 2020;11(11):3309–3316. doi:10.1111/1759-7714.13672
21. Li Y, Yuan Q, Huang J, et al. Assessment of plasma B7-H3 levels in pediatric patients with different degrees of surgical stress. BMC Pediatr. 2016;16:110. doi:10.1186/s12887-016-0655-1
22. Chawla LS, Toma I, Davison D, et al. Acute appendicitis: transcript profiling of blood identifies promising biomarkers and potential underlying processes. BMC Med Genomics. 2016;9(1):40. doi:10.1186/s12920-016-0200-y
23. Shommu NS, Jenne CN, Blackwood J, et al. Metabolomic and inflammatory mediator based biomarker profiling as a potential novel method to aid pediatric appendicitis identification. PLoS One. 2018;13(3):e0193563. doi:10.1371/journal.pone.0193563
24. Chen P, Huang Z, Chen L, et al. The relationships between LncRNA NNT-AS1, CRP, PCT and their interactions and the refractory mycoplasma pneumoniae pneumonia in children. Sci Rep. 2021;11(1):2059. doi:10.1038/s41598-021-81853-w
25. Shommu NS, Blackwood J, Jenne CN, et al. Metabolomics and inflammatory mediator profiling for the differentiation of life-threatening and non-severe appendicitis in the pediatric population. Metabolites. 2021;11(10):664. doi:10.3390/metabo11100664
26. Psaltis E, Zaitoun AM, Neal KR, Lobo DN. Immunohistochemical inflammation in histologically normal appendices in patients with right iliac fossa pain. World J Surg. 2021;45(12):3592–3602. doi:10.1007/s00268-021-06288-w
27. Reiff DD, Zhang M, Cron RQ. DOCK2 mutation and recurrent hemophagocytic lymphohistiocytosis. Life. 2023;13(2). doi:10.3390/life13020434
28. Vuletic A, Mirjacic Martinovic K, Tisma Miletic N, Zoidakis J, Castellvi-Bel S, Cavic M. Cross-talk between tumor cells undergoing epithelial to mesenchymal transition and natural killer cells in tumor microenvironment in colorectal cancer. Front Cell Dev Biol. 2021;9:750022. doi:10.3389/fcell.2021.750022
29. Zhang G, Wang J, Kelly J, et al. B7-H3 augments the inflammatory response and is associated with human sepsis. J Immunol. 2010;185(6):3677–3684. doi:10.4049/jimmunol.0904020
30. Chen X, Zhang G, Li Y, et al. Circulating B7-H3(CD276) elevations in cerebrospinal fluid and plasma of children with bacterial meningitis. J Mol Neurosci. 2009;37(1):86–94. doi:10.1007/s12031-008-9133-z
31. Huang Y, Zhang HL, Li ZL, et al. FUT8-mediated aberrant N-glycosylation of B7H3 suppresses the immune response in triple-negative breast cancer. Nat Commun. 2021;12(1):2672. doi:10.1038/s41467-021-22618-x
32. Luo L, Zhu G, Xu H, et al. B7-H3 promotes pathogenesis of autoimmune disease and inflammation by regulating the activity of different T cell subsets. PLoS One. 2015;10(6):e0130126. doi:10.1371/journal.pone.0130126
33. Gu W, Zhang X, Yan Y, et al. B7-H3 participates in the development of asthma by augmentation of the inflammatory response independent of TLR2 pathway. Sci Rep. 2017;7:40398. doi:10.1038/srep40398
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.