")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
The Impact of Insulin Staging in the Context of Pharmaceutical Care on Patients with Type 2 Diabetes Mellitus
Authors Obeid KA , Hamasaeed AG
Received 13 November 2022
Accepted for publication 28 December 2022
Published 11 January 2023 Volume 2023:16 Pages 71—83
DOI https://doi.org/10.2147/DMSO.S388750
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Kawa Ahmad Obeid, Ahmed Ghafour Hamasaeed
Department of Clinical Pharmacy/ College of Pharmacy, University of Sulaimani, Sulaimani, Kurdistan Region, Iraq
Correspondence: Kawa Ahmad Obeid, College of Pharmacy, University of Sulaimani, Old Campus, Sulaimaniyah, Kurdistan Region, 46001, Iraq, Tel +9647501112412, College of Pharmacy, University of Sulaimani, Email [email protected]
Purpose: The problem of polypharmacy and the nature of the disease make patients with type 2 diabetes mellitus highly vulnerable to drug therapy problems, especially those who are on insulin therapy. Despite this challenge, reaching the desired clinical outcome and using an appropriate insulin regimen are also considered a controversial issue among clinicians. The current study is designed to explore the impact of insulin staging regimens in the context of pharmaceutical care on patients with type 2 diabetes mellitus.
Patients and Methods: This study is a randomized interventional comparative study of a few groups. It was conducted at the Diabetes and Endocrine Centre in Sulaymaniyah City in Iraq from January to August 2022. Patients with T2DM who were on insulin therapy were enrolled in this trial. The participants were divided into two groups, the interventional and non-interventional groups. The insulin regimen was modified, and pharmaceutical care process was performed for the intervention group. Drug therapy problems (DTPs) and clinical parameters were monitored both groups over the course of six months.
Results: A total of 67 patients with T2DM on insulin were included in this study, and of them, 73% were females, with a mean age of 57.34 ± 7.825 years. The groups were randomly divided into intervention and non-intervention groups. After six months of applying insulin staging in the context of pharmaceutical care, FPG (Mean Diff.= 72.25, 95% CI of diff.= 20.44 to 124.1), HbA1c (Mean Diff.= 2.087, 95% CI of diff.= 1.151 to 3.023) and DTP were significantly improved in the intervention group.
Conclusion: Implementing the insulin staging approach within the context of the pharmaceutical care process showed a significant impact on controlling plasma glucose levels.
Keywords: drug therapy problem, clinical pharmacy, insulin staging, adherence, insulin regimen
Introduction
Currently, diabetes mellitus (DM) poses a challenge to world health. Due to diabetes, one person dies every five seconds. Nearly half a billion (537 million) individuals (20–79 years) have diabetes mellitus. This number is expected to reach 783 million by 2050.1 In 2021, only in Iraq, more than 10.7% of adults are living with diabetes.2 Approximately (~95%) of the diabetic case were type 2 diabetes (T2DM).3 The problem of polypharmacy and the nature of the disease make patients with T2DM highly vulnerable to drug therapy problems (DTP), especially those who are on insulin therapy. Despite this challenge, achieving the desired clinical outcome and using an appropriate insulin regimen are also considered controversial issue among clinicians.
At some points of their life, a significant number of patients with type 2 diabetes will require to take insulin therapy as their beta-cell activity falls over time. Using insulin always associated with challenges, such as hypoglycemia and weight gain,4 psychological barriers,5 patients feeling of failure to control of their glucose level,6 Patients’ misperceptions about insulin being not effective, toxic or lead to more complications and injection pain,7 lack of awareness,8 dose titration and adjustment,7 physicians lack of sufficient time for patients training and education.9
Tackling all the above-mentioned problems by physicians alone is not an easy task. Many studies pointed out that clinical pharmacists can play a key role in this regard.10–13 Adding pharmaceutical care to the health care system creates an opportunity for clinical pharmacists to manifest their roles, especially in Iraq where most of their jobs are constrained in the dispensary pharmacies.14 Pharmaceutical care “is the responsible provision of drug therapy for the purpose of achieving definite outcomes that improve a patient’s quality of life”.15 (Pharmaceutical care process steps are shown in Figure 1.)
 |
Figure 1 Pharmaceutical care process. |
After 100 years of insulin discovery, clinicians are still struggling to reach into an agreement on a unified insulin regimen to use for patients with T2DM.16 A unified approach in terms of insulin regimen is a significant milestone for the management of patients with T2DM. This approach enables both clinicians and other healthcare providers to closely monitor the insulin therapy and its drug-related problems. In this study, we have tried to apply insulin staging that suggested by American Diabetic Association as a systematic and unified approach of insulin regimen.17 Insulin staging consist of four hierarchical stages from the stage one to the stage four. Each stage has its own insulin type, frequency and ratio (as shown in Figure 2). In the current study, this systematic approach of insulin regimen was applied to the patients with T2DM in the context of pharmaceutical care process.
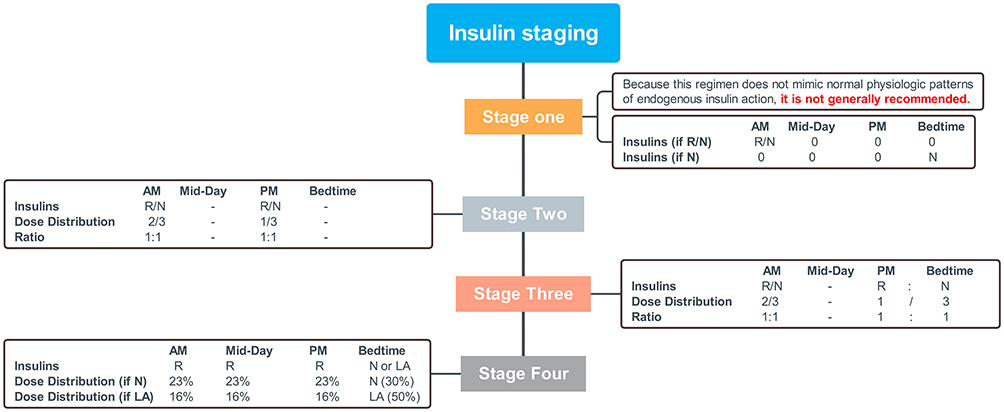 |
Figure 2 Insulin staging. Abbreviations: R, short acting; RA, rapid Acting; N, intermediate acting; LA, long acting. |
Materials and Methods
The Setting
The study design is a randomized interventional comparative study of few groups that is carried out from January 2022 to August 2022 in the Diabetes and Endocrine Centre in Sulaymaniyah City in Iraq. There is one lab, a pharmacy, and a special section for data entry, weight, and blood pressure checking. Those patients willing to attend this study has referred by one of the physicians to the researcher.
Ethical Considerations
- The study was approved by Ethical Committee of the College of Pharmacy – University of Sulaimani (approval number: PH 29–21).
- This study complies with the Declaration of Helsinki.
- All subjects participated voluntarily.
- All participants provided informed consent before starting the study.
- Data sharing statement: no further data will be shared because researchers had not received informed consent or ethics approval to share data (upon journal’s request, we can share the data with the editor privately).
Trial Registration
The study was registered at clinicaltrials.gov database (ClinicalTrials.gov Identifier: NCT05244200).
Patient Selection
Seventy-three patients were enrolled to this study. All of them were previously diagnosed with T2DM and they were on insulin therapy. From the total number of patients enrolled at the beginning, only sixty-seven patients completed the study, while six patients lost in the follow-up period.
Patients were assigned into two groups, intervention group and non-intervention group. Thirty-three patients were enrolled in the intervention group. These patients were receiving insulin staging and pharmaceutical care process. Evaluation and follow-up were performed at baseline for fasting plasma glucose (FPG), glycated hemoglobin (HbA1c), serum level of total cholesterol (TC), low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglyceride (TG). Later on, these parameters were measured every three months. In terms of pharmaceutical care, intervention was performed in four main categories of DTPs, i.e. indication, effectiveness, safety and compliance. These four main categories were further divided into thirty-four subcategories as indicated in Appendix 1. These problems were monitored on monthly basis. Researchers had a cumbersome work around to detect, prevent and resolve DTPs.
While, in the non-intervention group, thirty-six patients were enrolled. Patients in this group were receiving a non-unified approach of insulin regimen. They were receiving conventional medical care. DTPs were followed up without intervention. The following parameters were also monitored at the beginning and every three months intervals: FPG, HbA1c, serum level of TC, LDL, HDL, TG.
Data Collection
Information regarding the demographic characteristics, disease record, and past medication history were gathered from patients. Laboratory data (FPG, HbA1c, cholesterol, TG, LDL and HDL) were gathered from Diabetes and Endocrine Centre database program and then, six months pharmacist intervention were performed and DTPs were identified in both groups using UpToDate system (The UpToDate system is an evidence-based clinical resource), ADA (American Diabetes clinical guideline for the treatment of DM. Robust DTPs performed for the intervention group via implementing pharmaceutical care described by Cipolle et al to show the impact of DTP resolution on the above-mentioned parameters. The patient information sheet includes all the details recorded for those who were clinically diagnosed to have type 2 diabetes.
Inclusion and Exclusion Criteria
Inclusion Criteria
- Patients with T2DM.
- Patients must be on insulin therapy.
- Willing to participate in the study.
Exclusion Criteria
- Patients with type 1 diabetes.
- Type 2 diabetes patients who are not on insulin therapy.
- Patients that have disabilities that interfere with compliances towards medications.
Sample Collection
Venous blood about (5–8 mL) was obtained by vein puncture of each individual (intervention and non-intervention) in the same daily hours (between 8:00 and 10:30. a.m.) after overnight fasting (8–12 hours). Blood samples were transferred into gel and clot activator tube and after coagulation, they were centrifuged at 4000 rpm and the separated serum samples was then inserted into plain tubes and stored at −35°C until time for laboratory analysis.
Measurement of Body Mass Index (BMI) and Waist Circumference
The international categorization of weight depending on BMI was used to evaluate the degree of obesity. By dividing weight of each patient by patient’s squared height in meters, BMI was calculated:
- Underweight (BMI < 18.5 kg/m2).
- Normal weight (BMI 18.5–24.9 kg/m2).
- Overweight (BMI 25–29.9 kg/m2).
- Obese (BMI 30 kg/m2).
Statistical Analysis
The data collection was completed, and the questions of the study were coded. Then data entry and analysis were performed. Data entry was carried out by using an Excel spreadsheet and then the statistical analysis was performed by GraphPad Prism, version 8.
Different types of bar charts (component bar charts) and line graphs were used to describe the variables of the study diagrammatically. Any p-value < 0.05 considered to be significant statistically.
Results
Patient Characteristics
Seventy-three patients were enrolled in the study at the Diabetes and Endocrine Centre in Sulaymaniyah City in Iraq. Out of this number, only 67 patients were remained until the end of the study. Characteristics of the patients, including medication allergies and adverse reactions to medications, are presented in Table 1.
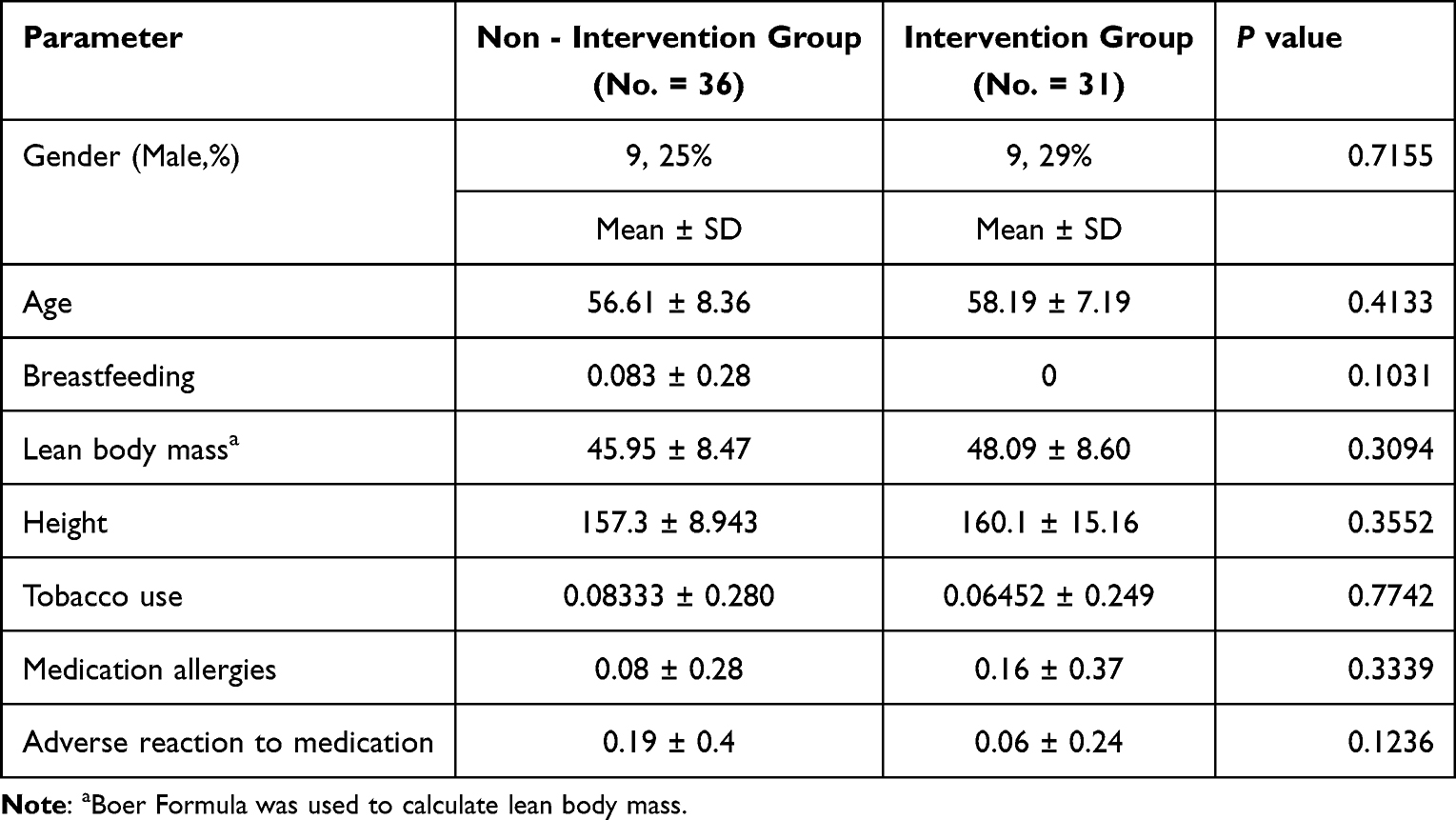 |
Table 1 Characteristics of Study Population |
Drug Therapy Problems Among Both Groups at Different Intervals
The total drug therapy problems for the intervention group per three consequent visit, i.e. 1st, 2nd and 3rd visits are showed in Figures 3–5, respectively. Upon comparison of these results with their pair ones in the non-intervention group, as showed in Figures 6–8, it is evident that most of the DTPs were located in the effectiveness and indication categories followed by compliance and safety one. At the same time, the problems related to the category of effectiveness showed to be tackled significantly in the intervention group (decreased from 61 DTPs in the 1st visit to 11 DTPs in the 3rd visit).
 |
Figure 3 DTPs among intervention group 1st visit. Abbreviation: DTP, drug therapy problem. |
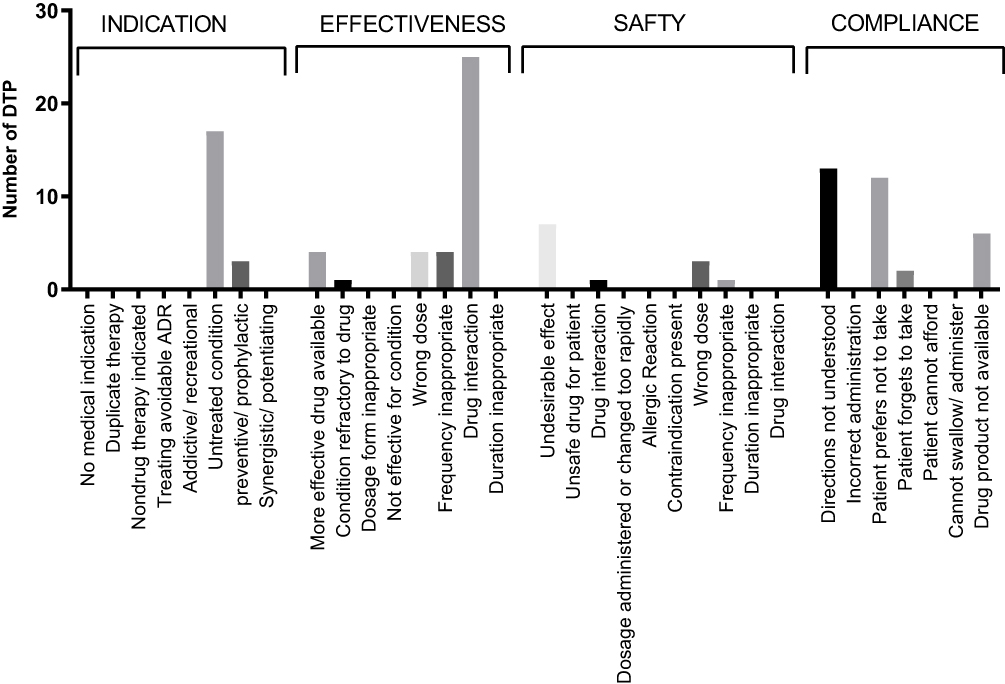 |
Figure 4 DTPs among intervention group 2nd visit. Abbreviation: DTP, drug therapy problem. |
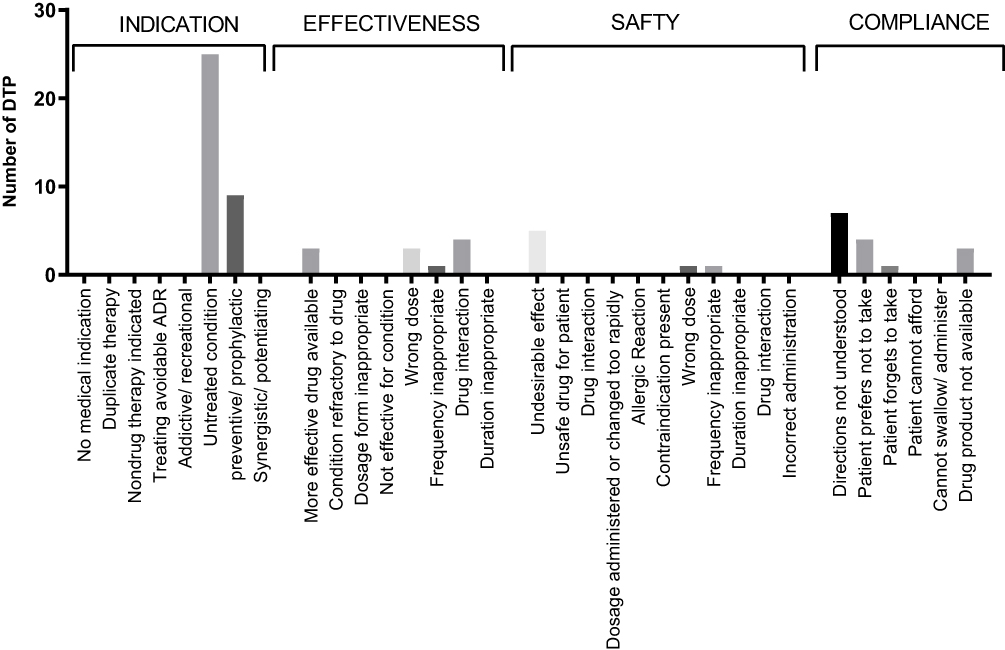 |
Figure 5 DTPs among intervention group 3rd visit. Abbreviation: DTP, drug therapy problem. |
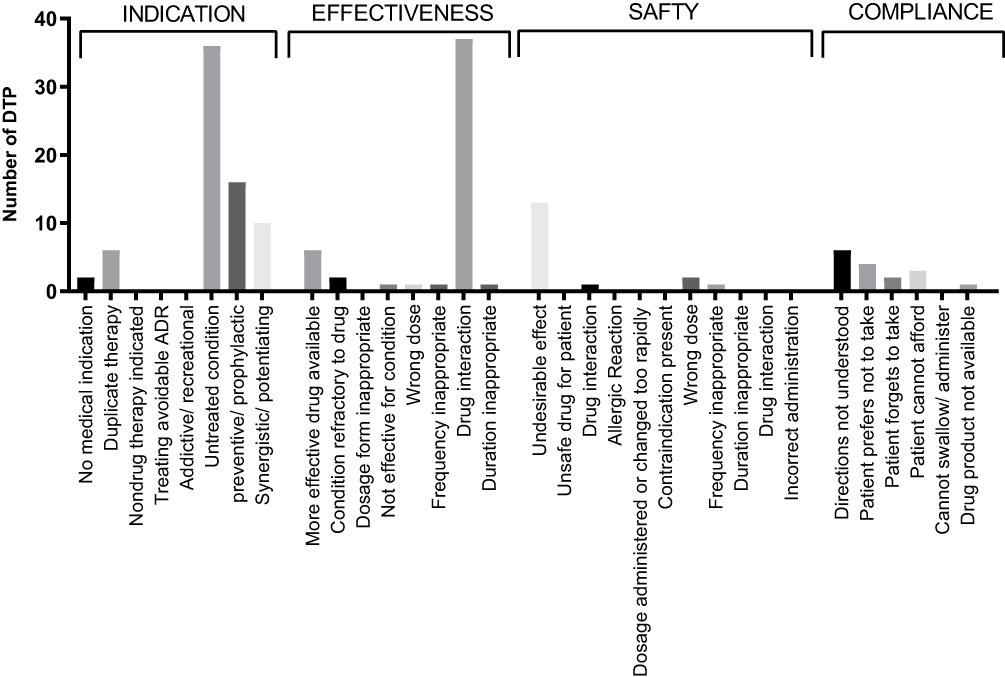 |
Figure 6 DTPs among non-intervention group 1st visit. Abbreviation: DTP, drug therapy problem. |
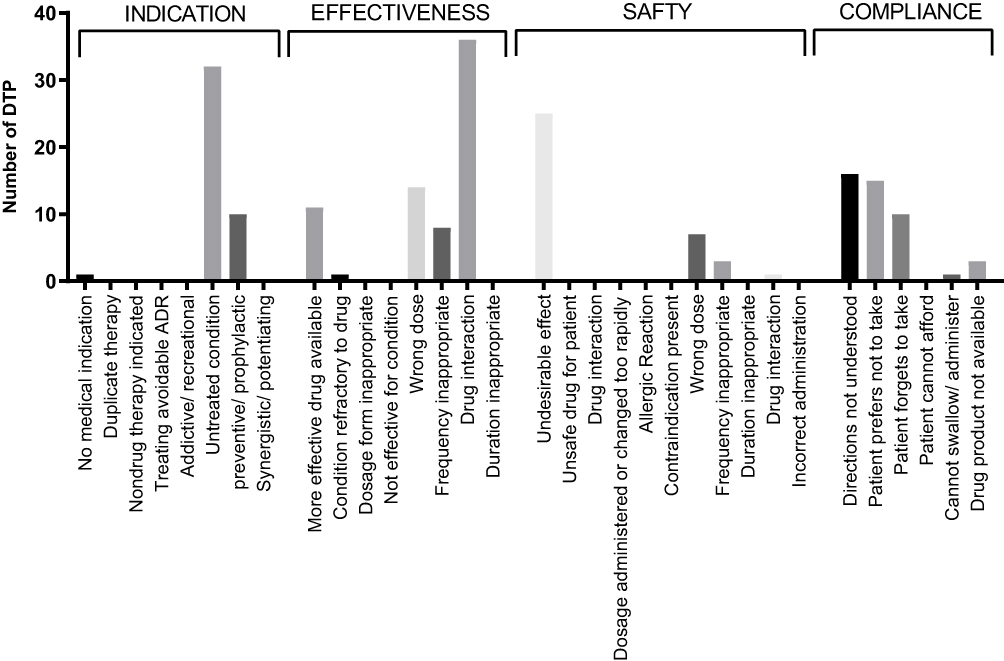 |
Figure 7 DTPs among non-intervention group 2nd visit. |
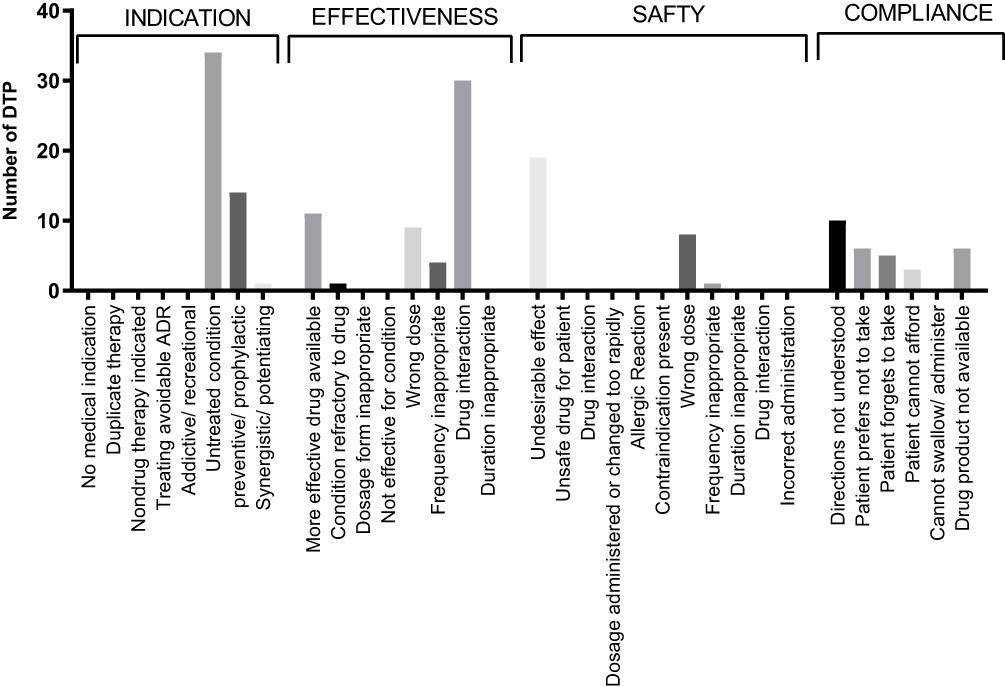 |
Figure 8 DTPs among non-intervention group 3rd visit. Abbreviation: DTP, drug therapy problem. |
As presented in Figure 9, after 6 months of intervention, there was a significant reduction in the DTPs of the intervention group (P-value < 0.0001****).
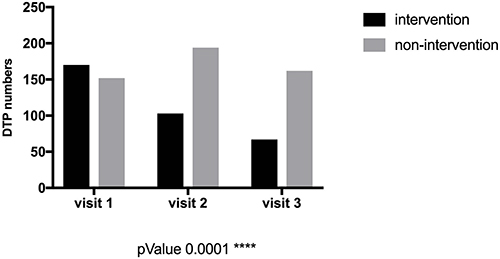 |
Figure 9 DTP change in intervention and non-intervention group. Abbreviation: DTP, drug therapy problem. |
The Impact of Insulin Staging and Pharmaceutical Care on Plasma Glucose Level, Body Weight, and Lipid Profile
After the implementation of our unified insulin approach plus the pharmaceutical care process, HbA1c (Figure 10) and FPG (Figure 11) were significantly improved in the intervention group (P-value < 0.05). While the same parameters in the non-intervention group showed no significant changes as shown in Figures 12 and 13 respectively. Changes in BMI (Table 2) were insignificant in both groups. Throughout our study, the lipid parameters in both groups showed non-significant changes as well (as shown in Figure 14).
 |
Table 2 Change in Body Mass Index (BMI) Over 6 Months |
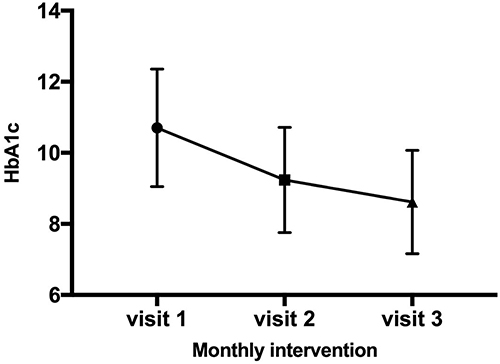 |
Figure 10 Changes in HbA1c among the intervention group. Abbreviation: HbA1c, glycated hemoglobin. |
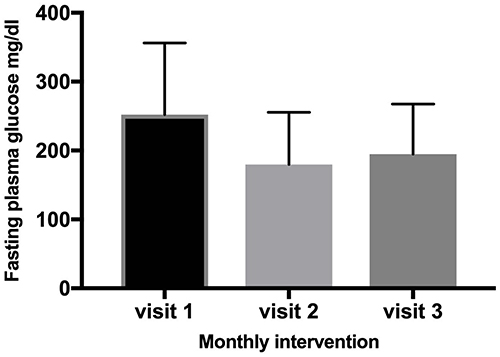 |
Figure 11 FPG changes among the intervention group. Abbreviation: FPG, fasting plasma glucose. |
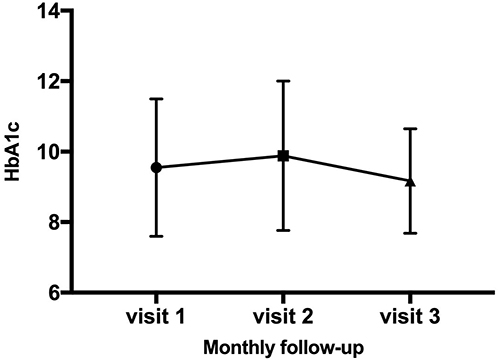 |
Figure 12 Changes in HbA1c among the non-intervention group. Abbreviation: HbA1c, glycated hemoglobin. |
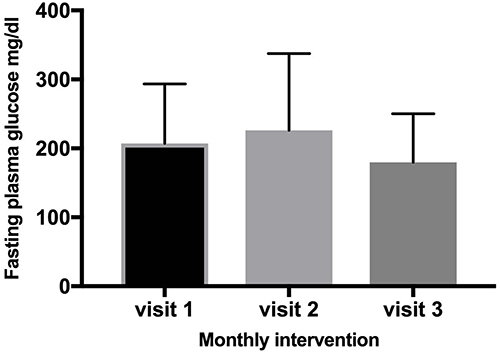 |
Figure 13 FPG changes among the non-intervention group. Abbreviation: FPG, fasting plasma glucose. |
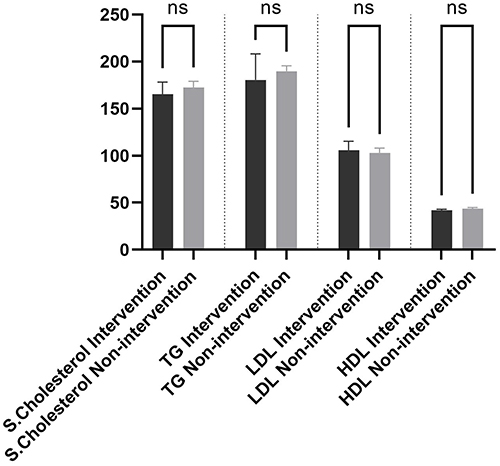 |
Figure 14 Lipid profile in intervention and non-intervention group. Abbreviations: s.cholesterol, serum cholesterol; TG, triglyceride; LDL, low-density lipoprotein; HDL, high-density lipoprotein; ns, non-significance. |
Discussion
In this study, we report the experience of applying insulin staging on patients with T2DM in the context of pharmaceutical care in Iraq. To the best of our knowledge, this is the first research of its type to be applied in the Middle East. The participants, who were insulin-treated patients with T2DM, were divided into non-intervention (36 patients) and intervention (31 patients) groups. We ought to explore the impact of insulin staging in the contest of pharmaceutical care on clinical outcomes. The division process was random and there was no significant difference between groups in terms of demographic characteristics as demonstrated in Table 1. Our study revealed that applying pharmaceutical care and insulin staging approach by clinical pharmacists in collaboration with physicians have a significant positive impact on reducing drug therapy problems and improving therapeutic outcomes. These results suggested that clinical pharmacists can play a key role in solving DTPs. Similar findings have been reported in other studies.18–20 Pharmaceutical care work has three main steps (as shown in Figure 1) including assessment, care plan and evaluation. To apply these steps in our study, first the assessment form, called pharmacotherapy workup table (Appendix 2), which is described by Cipolle et al,21 was filled out by the pharmacist for every patient in both groups. In line with other studies, our assessments showed that patients with T2DM are at high risk for DTPs22,23 and pharmacists are capable of helping patients to overcome the challenges of medication use with chronic diseases.24
The data revealed that, out of 322 DTPs on the first visit, the categories of drug therapy problems were sharing inequal numbers. For example, problems related to the indication were taking 38% of total DTPs. While effectiveness, compliance, and safety shares were 34%, 18%, and 7%, respectively. These results are in contrast with previous studies in which most of the DTPs were ascribed to patients’ non-compliance towards medications.25 Two points are emerging here, firstly, the lack of a unified insulin regimen, and secondly, underrating the problems related to indication and effectiveness categories hurdle the patients to achieving a desired therapeutic outcome.
Based on our results, the rate of DTPs is higher (4.67± 1.78 DTPs/patient as mentioned in Table 3) in comparison with other published studies performed by Ogbonna et al, and Koyra et al22,23 Arguably, this might be amounted to the fact that all of our patients were on insulin, while the number of insulin users were much lower in the above-mentioned articles (17.1% and 27.8% respectively). Despite a high rate of DTPs/patients in both Groups (4.10 ± 1.6 for non-intervention Group and 5.31 ± 1.8 for the intervention Group), a significant reduction (P value< 0.0001****) of DTPs can be seen in the intervention group (from 170 DTPs to 67 DTPs), while the change was insignificant in the non-intervention group (the mean of DTPs/patients were 4.10 ±1.6, 5.1±2, and 4.5 ±1.8, during the 1st, 2nd and 3rd, consequently as shown in Figure 9).
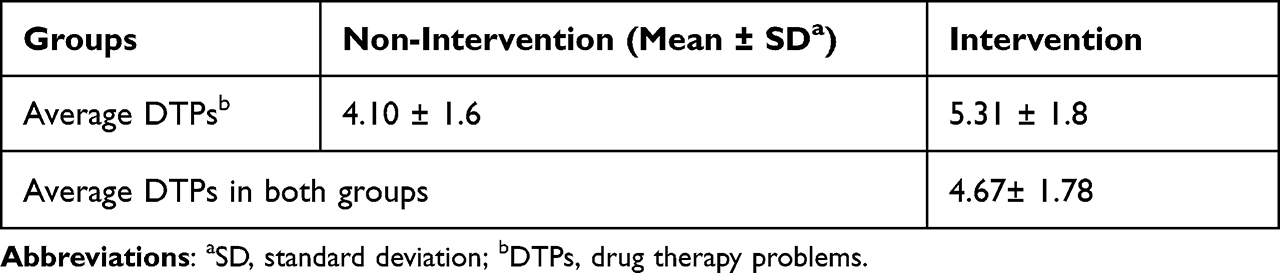 |
Table 3 Number of DTPs at First Visit |
Our data indicated that during the first visit, the most frequently encountered DTP in the intervention group was located in the category of effectiveness with 61 DTPs (36%) followed by Indication with 53 DTPs (31%), compliance with 42 DTPs (25%) and safety with 14 DTPs (8%) as shown in Figure 3. Meanwhile, the most frequently encountered DTP in the non-intervention group was ascribed to the category of indication with 70 DTPs (46%) followed by effectiveness with 49 DTPs (32%), safety with 17 DTPs (11%), and compliance with 16 DTPs (11%) as shown in Figure 6. After 6 months of pharmacist’s intervention, the number of DTPs were significantly reduced among patients in the intervention group, the mean DTPs/patients were 5.3 ±1.8, 3.6±1.9 and 2.2 ±1.8 during the 1st, 2nd and 3rd, respectively. The maximum reduction was noticed in the category of effectiveness where 61 problems were reduced into 11 DTPs towards the end of the study. This was followed by compliance in which out of 42 DTPs in first visit only 15 DTPs were remained at the end of our study, as shown in Figures 3 and 5.
As a consequence of DTP resolution and insulin staging application and providing appropriate pharmaceutical service, we have observed a significant changes in the glycemic picture of patients in both glycated hemoglobin (p=0.0001***) (as shown in Figure 10) and fasting plasma glucose (p=0.0032**) (as shown in Figure 11). Meanwhile, our data revealed a non-significant change in the same parameters among patients in the non-intervention group (p > 0.05) as presented in Figures 12 and 13. The rate of glycated hemoglobin reduction in our study (>2%) is significantly higher than those studies applying staged diabetes management program alone without pharmaceutical care process. For instance, a prospective, randomized controlled study, of one years’ duration performed by general practitioners in France resulted in glycated hemoglobin reduction only by 0.31% in the intervention group.26
It is worth to mention that the same clinical outcomes have not been observed in terms of lipid profile (as shown in Figure 14). The issue standing here is that the lipid profile was not high at the baseline for both groups and eighty one percent of the patients were on lipid lowering agents. Despite significant reduction in HbA1c level, there is no significant changes in BW and BMI as presented Table 2. This is in line with the results of a study conducted by Kim et al, in which intensive insulin regimen led to HbA1c reduction significantly without a significant change in BW and BMI.27
Conclusion
Our findings highlight that using of insulin staging therapy in the context of pharmaceutical care process is a promising approach. Detection, prevention, and resolution of DTPs alongside with applying a unified insulin regimen will lead to a significant reduction of plasma glucose levels in patients with T2DM. We have also concluded that clinical pharmacists, as health care providers, can play a pivotal role in applying this unified approach of insulin therapy which in turn leads to a substantial achievement in terms of therapeutic outcomes.
Abbreviations
T2DM, type two diabetes mellitus; DTP, drug therapy problems; DM, diabetes mellitus; FPG, fasting plasma glucose; HbA1c, glycated hemoglobin; TC, total cholesterol; LDL, low-density lipoprotein; HDL-c, high-density lipoprotein; VLDL, very low-density lipoprotein; TG, triglyceride; BMI, body mass index.
Acknowledgments
We thank the participants of the study, the Diabetes and Endocrine Centre in Sulaymaniyah, nursing services, and the clinic staff for their support in this study. Finally, we would like to express our heartfelt gratitude to Dr Taha O. Mahwi for referring participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Home, Resources, diabetes L. IDF diabetes atlas | tenth edition. Available from: https://diabetesatlas.org/.
2. Diabetes prevalence (% of population ages 20 to 79) - Iraq | data. Available from: https://data.worldbank.org/indicator/SH.STA.DIAB.ZS?end=2021&locations=IQ&start=2011.
3. Diabetes. Available from: https://www.who.int/news-room/fact-sheets/detail/diabetes.
4. Insulin adherence behaviours and barriers in the multinational global attitudes of patients and physicians in insulin therapy study - peyrot - 2012 - diabetic medicine - Wiley online library. Available from: https://onlinelibrary.wiley.com/doi/10.1111/j.1464-5491.2012.03605.x. Accessed September 6, 2022.
5. Polonsky WH, Fisher L, Guzman S, Villa-Caballero L, Edelman SV. Psychological insulin resistance in patients with type 2 diabetes: the scope of the problem. Diabetes Care. 2005;28(10):2543–2545. doi:10.2337/diacare.28.10.2543
6. Polonsky WH, Jackson RA. What’s so tough about taking insulin? Addressing the problem of psychological insulin resistance in type 2 diabetes. Clin Diabetes. 2004;22(3):147–150. doi:10.2337/diaclin.22.3.147
7. Perreault L, Vincent L, Neumiller JJ, Santos-Cavaiola T. Initiation and titration of basal insulin in primary care: barriers and practical solutions. J Am Board Fam Med. 2019;32(3):431–447. doi:10.3122/jabfm.2019.03.180162
8. Gyawali B, Ferrario A, van Teijlingen E, Kallestrup P. Challenges in diabetes mellitus type 2 management in Nepal: a literature review. Glob Health Action. 2016;9(1):31704. doi:10.3402/gha.v9.31704
9. Insights into optimal basal insulin titration in type 2 diabetes: results of a quantitative survey - Berard - 2018 - diabetes, obesity and metabolism - Wiley online library. Available from: https://dom-pubs.onlinelibrary.wiley.com/doi/full/10.1111/dom.13064.
10. Dhandapani C, Sony S. Role of clinical pharmacist in the management of type ii diabetes mellitus and its outcomes. Int J. 2014;5(3):7.
11. Chua SS, Kok LC, Yusof FAM, et al. Pharmaceutical care issues identified by pharmacists in patients with diabetes, hypertension or hyperlipidaemia in primary care settings. BMC Health Serv Res. 2012;12(1):388. doi:10.1186/1472-6963-12-388
12. Sanii Y, Torkamandi H, Gholami K, Hadavand N, Javadi M. Role of pharmacist counseling in pharmacotherapy quality improvement. J Res Pharm Pract. 2016;5(2):132–137. doi:10.4103/2279-042X.179580
13. Farsaei S, Sabzghabaee AM, Zargarzadeh AH, Amini M. Effect of pharmacist-led patient education on glycemic control of type 2 diabetics: a randomized controlled trial. J Res Med Sci. 2011;16(1):43–49.
14. Martin-Calero MJ, Machuca M, Murillo MD, Cansino J, Gastelurrutia MA, Faus MJ. Structural process and implementation programs of pharmaceutical care in different countries. Curr Pharm Des. 2004;10(31):3969–3985. doi:10.2174/1381612043382549
15. Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;47(3):533–543.
16. Selecting insulin regimens for the management of non-ICU patients with type 2 diabetes | journal of the endocrine society | Oxford Academic. Available from: https://academic.oup.com/jes/article/5/10/bvab134/6354345.
17. Mazze R, Strock ES, Simonson GD, Bergenstal RM. Staged Diabetes Management: A Systematic Approach. John Wiley & Sons; 2007.
18. Elhabil MK, Yousif MA, Ahmed KO, Abunada MI, Almghari KI, Eldalo AS. Impact of clinical pharmacist-led interventions on drug-related problems among pediatric cardiology patients: first Palestinian experience. IPRP. 2022;11:127–137. doi:10.2147/IPRP.S374256
19. Contreras-Vergara A, Sifuentes-Franco S, Haack S, et al. Impact of pharmaceutical education on medication adherence and its clinical efficacy in patients with type 2 diabetes and systemic arterial hypertension. PPA. 2022;16:1999–2007. doi:10.2147/PPA.S370323
20. Dong PTX, Pham VTT, Dinh CT, et al. Implementation and evaluation of clinical pharmacy services on improving quality of prescribing in geriatric inpatients in Vietnam: an example in a low–resources setting. CIA. 2022;17:1127–1138. doi:10.2147/CIA.S368871
21. Cipolle RJ, Strand LM, Morley PC. Pharmaceutical Care Practice: The Patient-Centered Approach to Medication Management. McGraw Hill Professional; 2012.
22. Ogbonna B, Ezenduka C, Opara C, Ahara L. Drug therapy problems in patients with Type-2 Diabetes in a tertiary hospital in Nigeria. Int J Innov Res Dev. 2014;3(1):494–502.
23. Argaw A, Hiwet T, Derse B. Drug therapy problems and determinants among ambulatory type 2 diabetes mellitus patients: pharmacists’ intervention in south-east Ethiopia. Endocrinol Metab Syndr. 2019;8:1. doi:10.35248/2161-1017.19.8.303
24. Rahayu SA, Widianto S, Defi IR, Abdulah R. Role of pharmacists in the interprofessional care team for patients with chronic diseases. JMDH. 2021;14:1701–1710. doi:10.2147/JMDH.S309938
25. Kefale B, Tegegne GT, Kefale Y, Molla M, Ewunetei A, Degu A. Magnitude and determinants of drug therapy problems among type 2 diabetes mellitus patients with hypertension in Ethiopia. SAGE Open Med. 2020;8:2050312120954695. doi:10.1177/2050312120954695
26. Varroud-Vial M, Simon D, Attali J, et al. Improving glycaemic control of patients with type 2 diabetes in a primary care setting: a French application of the staged diabetes management programme. Diabet Med. 2004;21(6):592–598. doi:10.1111/j.1464-5491.2004.01207.x
27. Kim HS, Yu JM, Jang HC, et al. Real-world analysis of rapid-acting insulin analog use and its blood glucose lowering effect in patients with type 2 diabetes mellitus: results from PASSION disease registry in Korea. Diabetes Metab Syndr Obes. 2022;15:1495–1503. doi:10.2147/DMSO.S334944
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.