")
Back to Journals » Infection and Drug Resistance » Volume 16
The Impact of ESBLs-Positive Escherichia coli’s Resistance to Cefepime and Its Guidance for Clinical Treatment
Authors Wu Q, Shi J, Huang J, Gan D, Zhang L, Li P
Received 27 June 2023
Accepted for publication 15 September 2023
Published 27 September 2023 Volume 2023:16 Pages 6395—6404
DOI https://doi.org/10.2147/IDR.S427836
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Qian Wu,1 Jing Shi,2 Juan Huang,3 Delu Gan,1 Lijun Zhang,1 Pu Li1
1Department of Laboratory Medicine, The Second Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Clinical Laboratory, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 3Department of Information Center, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Pu Li, Department of Clinical Laboratory, The Second Affiliated Hospital, Chongqing Medical University, Chongqing, People’s Republic of China, Fax +86-23-63693195, Email [email protected]
Background: Escherichia coli (E. coli) is a common pathogen in bloodstream infections (BSI), and the production of extended-spectrum beta-lactamases (ESBLs) is its main mechanism of resistance. However, the impact of different ESBL genotypes of E. coli on the resistance to Cefepime (FEP) remains unclear.
Methods: A total of 2356 cases of BSI patients were collected. The experimental group included 188 ESBL-positive E. coli strains that were resistant to FEP but sensitive to ceftazidime (CAZ). Antibiotic usage and resistance rates were evaluated through antimicrobial susceptibility testing and antibiotic usage records. The ESBL genotypes were identified, and the minimum inhibitory concentration (MIC) and mutant prevention concentration (MPC) of FEP were determined.
Results: In ESBL-positive E. coli, three ESBL genotypes were identified: 188 strains of CTX-M, 130 strains of TEM-1, and 26 strains of OXA-10. Among them, 124 strains carried both CTX-M-9 and TEM-1 genotypes, 22 strains carried two CTX-M genotypes (CTX-M-1 and CTX-M-2), 20 strains carried both CTX-M-9 and OXA-10, and 6 strains carried three genotypes (CTX-M-9, CTX-TEM-1, and OXA-10). The MIC50, MIC90, MPC50, and MPC90 of the 188 ESBL-positive E. coli were 64, 256, 128, and 528, respectively. The MIC values ranged from 32 to 256, while the MPC values ranged from 64 to 528. The MIC50, MIC90, MPC50, and MPC90 of the 40 ESBL-negative E. coli were 0.5, 1, 64, and 128, respectively; the MIC values ranged from 0.25 to 4, while the MPC values ranged from 32 to 256, respectively.
Conclusion: ESBL-positive E. coli induces an increase in the MIC value of FEP, leading to an increase in FEP resistance. The inoculation effect also causes a significant increase in the MPC value of FEP, especially the increase in selection index value, indicating selective enrichment and amplification of drug-resistant mutants, resulting in clinical treatment failure.
Keywords: Escherichia coli, cefepime, ESBLs, mutant prevention concentration
Introduction
With the continuous improvement of clinical recognition and prevention and treatment levels of bacterial infectious diseases, the emergence of Gram-negative multidrug-resistant bacteria and the infectious disease problems it causes have become one of the important challenges facing global public health.1 However, the enhancement of drug resistance and the ineffectiveness of commonly used antibiotics have made it increasingly difficult for clinical doctors to treat infectious diseases. Escherichia coli (E. coli), as one of the most common pathogenic bacteria, produces extended-spectrum β-lactamases (ESBLs), which makes the treatment of infectious diseases caused by it increasingly challenging. ESBLS-positive bacteria show a highly resistant state to conventional antibacterial drugs, and this resistance is increasing.2 Therefore, how to effectively delay and control the further rise of bacterial resistance has become an urgent problem to be solved in the current treatment of bacterial infectious diseases.
In antibiotic therapy, cephalosporin antibiotics are widely used. However, due to the significant resistance of ESBLS-positive bacteria to many conventional cephalosporin antibiotics, the treatment of E. coli infections has become increasingly difficult.3 In addition, the traditional minimum inhibitory concentration theory has not accurately reflected the drug’s ability to prevent resistance mutations,4 therefore, the introduction of Mutant Prevention Concentration (MPC) has become a new drug evaluation index. The latest research shows that only when the drug concentration reaches or exceeds MPC, can it effectively suppress the further rise of bacterial resistance.5 Therefore, in clinical treatment, appropriate antibiotics should be selected based on the pathogen’s sensitivity results, and the drug concentration should be monitored to achieve the best therapeutic effect. These measures can effectively delay and suppress the further rise of bacterial resistance, providing better protection for the treatment of bacterial infectious diseases.
Prior to 2010, according to the breakpoint interpretation standards of CLSI, multiple cephalosporins including FEP, as well as penicillins and aztreonam, were directly modified to resistance in ESBL-positive Gram-negative bacteria. However, the M100-S20 version of the “Antimicrobial Susceptibility Testing Standards” released after 2010 no longer modified resistance based on ESBL-positive results.6 Instead, laboratories determined antimicrobial susceptibility directly based on cephalosporin breakpoints. MIC values are particularly important for the treatment of ESBLS-producing strains.7 Therefore, this study aims to explore the clinical efficacy and related mechanisms of FEP in the treatment of ESBLs with different genotypes of E. coli infections, providing guidance for clinical antibiotic treatment and reliable reference for rational use of antibiotics. We believe that the results of this study will provide new ideas and methods for solving the treatment difficulties caused by ESBLs-positive E. coli bloodstream infections, and provide more accurate antibiotic treatment plans for clinicians in the future.
Study Subjects and Methods
Study subjects: A total of 2356 patients with bloodstream infections (BSI) caused by E. coli were selected from the Second Affiliated Hospital of Chongqing Medical University from 2016 to 2022. The patients’ age, gender, antibiotic use, Source of infection, underlying diseases, infection sites, and prognosis were recorded. A total of 188 ESBLs-positive E. coli strains resistant to FEP but sensitive to ceftazidime were screened from blood specimens of hospitalized patients at the Second Affiliated Hospital of Chongqing Medical University from 2016 to 2022 using the VITEK-2 identification and susceptibility testing system (bioMérieux, France), and the results were confirmed by broth microdilution method. The microbroth dilution method is the standard method recommended by CLSI for antimicrobial susceptibility testing. The susceptibility results obtained by VITEK2 are ultimately determined by an expert system programmed into the instrument and clinical microbiology laboratory staff.
This study was performed according to the principles of the Declaration of Helsinki and was approved by the Medical Ethics Committee of the Second Affiliated Hospital of Chongqing Medical University.
Methods
The Kirby-Bauer paper disk diffusion method was used for confirmation testing. A total of 188 ESBLs-positive E. coli strains that were resistant to FEP but sensitive to ceftazidime (CAZ) (experimental group) and 40 ESBLs-negative E. coli strains (control group) were tested. The minimum inhibitory concentration (MIC) and mutant prevention concentration (MPC) of both groups of strains against FEP were determined separately. The genotypes of all 188 ESBLs-positive E. coli strains were determined, and the effect of resistance genes on the MPC of FEP was observed.
The confirmation test for ESBLs was performed by using cefotaxime and CAZ in combination with a compound containing clavulanic acid for separate and combined testing. One of the two drugs in the Kirby-Bauer paper disk diffusion method was compared with the diameter of the inhibition zone without clavulanic acid added when the diameter of the inhibition zone increased by 5 mm or more, it was judged as ESBLs-producing E. coli.
Identification of ESBLS-Positive Genotypes
The DNA of the 188 ESBLS-positive E. coli strains selected above was extracted, and PCR was used to amplify possible ESBLS-resistant genotypes (CTXM-1, CTXM-2, CTXM-8, CTXM-9, OXA-2, OXA-10, TEM-1, SHV). The PCR amplification products were analyzed by agarose gel electrophoresis. The ESBLS screening primer sequences are shown in Table 1. The strains corresponding to the PCR products with specific bands in the electrophoresis results were selected for further sequencing to detect the ESBLS genotype.
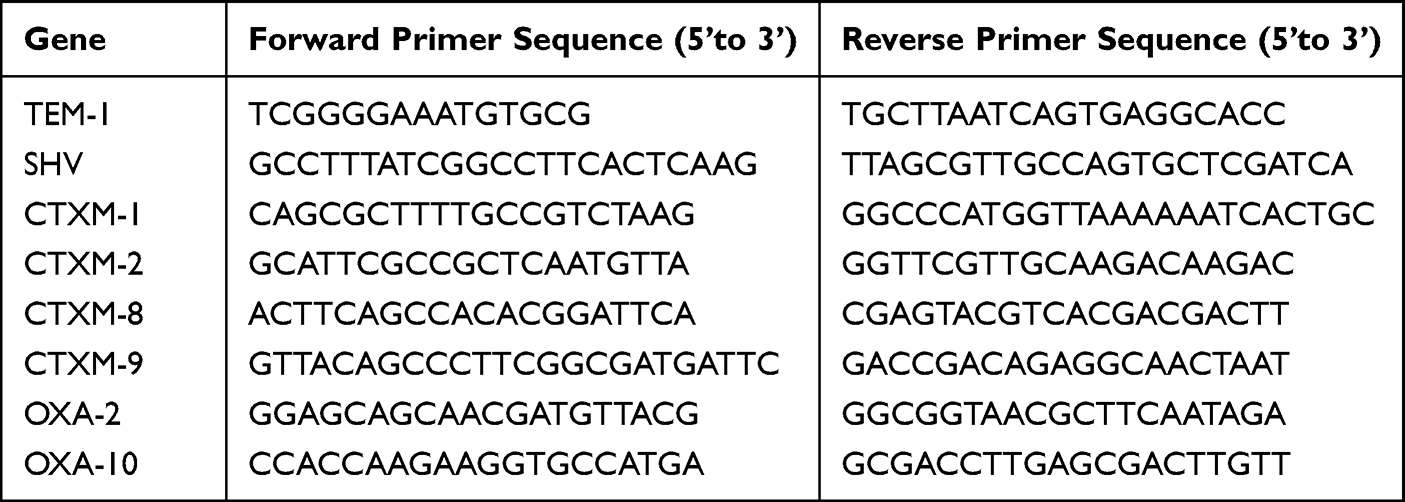 |
Table 1 Primer Sequences for Extended-Spectrum β-Lactamase (ESBLs) Genes |
Determination of Minimum Inhibitory Concentration (MPC) for Drug-Resistant Mutations
The MPC was determined using the agar plate double dilution method.8 Single colonies were picked and inoculated into LB broth, cultured for 18–24 hours, and then centrifuged at 3000r/min to discard the supernatant. The bacteria were then suspended in 10 times the volume of LB broth and cultured for 6 hours, centrifuged again, and the bacterial suspension was diluted 100 times to a concentration of 0.5 McFarland units, indicating that the concentration of the original bacterial suspension was 1~3x1010 CFU/mL. 100 μL of bacterial suspension was taken and evenly spread on MH plates containing FEP (10 concentrations, 516, 256, 128, 64, 32, 16, 8, 4, 2, and 1 μg/mL), with 4 plates prepared for each concentration. The plates were incubated at 37°C for 72 hours, and the lowest drug concentration at which no bacteria grew on all 4 plates was determined as the MPCpr (provisional MPC). Then, this was used as the reference to conduct repeat experiments, with the concentration of antimicrobial agents decreased by 20% successively to determine the final MPC value.
Determination of Minimum Inhibitory Concentration (MIC)
The MIC testing method refers to the implementation of the 2018 version of CLSI M100.6 Antibiotic sensitivity is determined by the breakpoints established by CLSI for interpretation of drug susceptibility results.
Statistical Analysis
Data were analyzed using GraphPad Prism 8 and SPSS 16.0. Differences were considered statistically significant when P<0.05.
Results
Clinical Characteristics of Patients
We conducted a statistical analysis of the clinical characteristics of patients with BSI caused by E. coli (Table 2); a total of 2356 cases were reported from 2016 to 2022. Among them, there were 374 cases in the Infectious Diseases Department (15.8%), 352 cases in the Intensive Care Unit (14.9%), 262 cases in the Hematology Department (11.1%), 222 cases in the Emergency Department (9.4%), 249 cases in the Hepatobiliary Surgery Department (10.5%), 154 cases in the Respiratory Medicine Department (6.5%), 132 cases in the Endocrinology Department (5.6%), 131 cases in the Nephrology Department (5.5%), and 96 cases in the Oncology Department (4.0%). Other departments included 64 cases in the Neurology Department (2.7%), 88 cases in the Cardiology Department (3.7%), 66 cases in the Gastrointestinal Surgery Department (2.8%), 44 cases in the Orthopedics Department (1.8%), 44 cases in the Gastroenterology Department (1.8%), 39 cases in the Geriatrics Department (1.6%), 20 cases in the Urology Department (0.8%), and 20 cases in the Thyroid and Breast Surgery Department (0.8%).
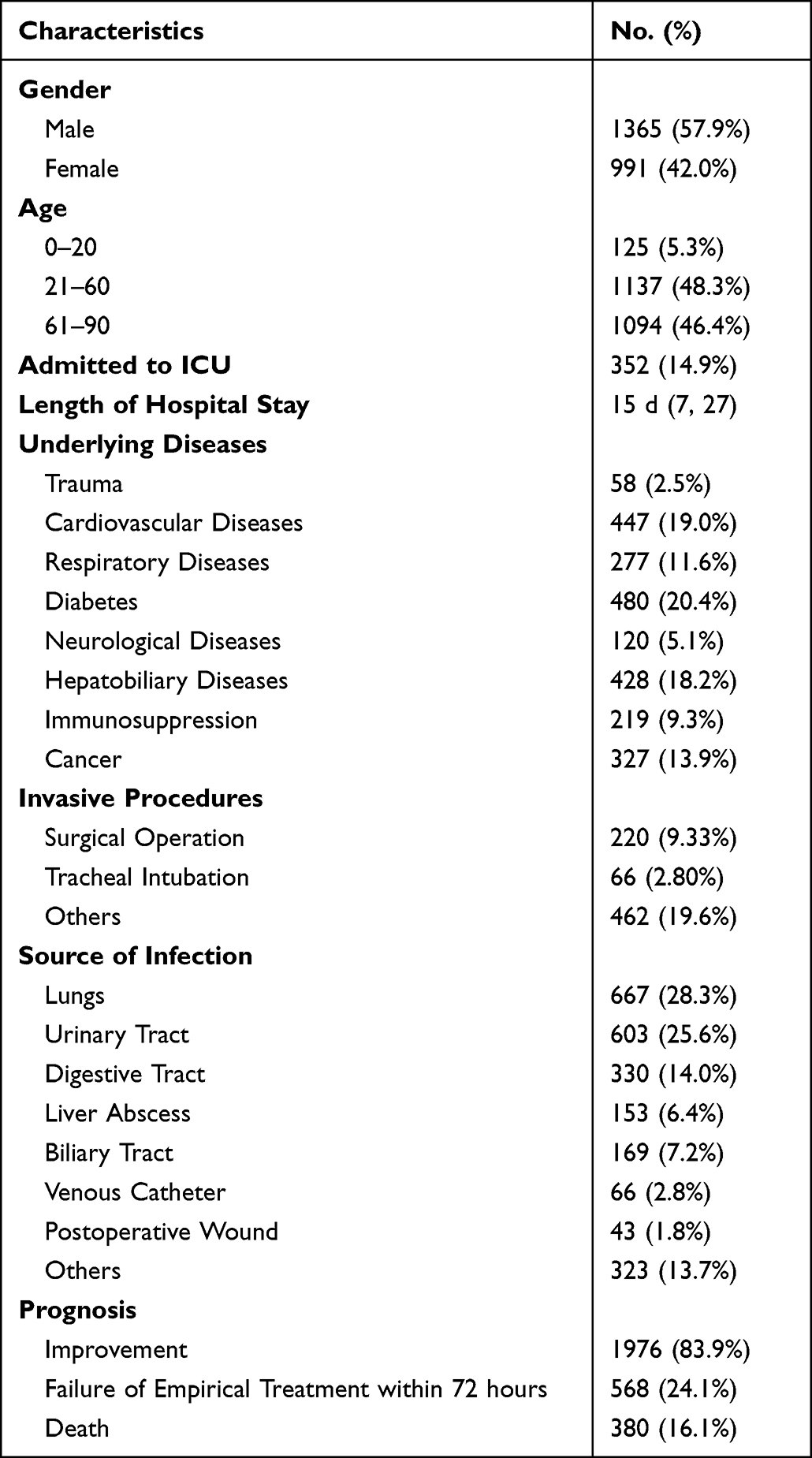 |
Table 2 Patient Characteristics |
In a total of 2356 clinical cases, we conducted a statistical analysis of the clinical efficacy and changes in serum inflammatory markers before and after treatment of three commonly used antibiotics (Table 3 and Table 4). The criteria for clinical efficacy evaluation were: 1) clinical cure, referring to the disappearance or improvement of infection-related symptoms and signs in patients after treatment, with non-microbiological indicators such as imaging and laboratory tests returning to normal or showing significant improvement; 2) clinical inefficiency, referring to the situation where patients’ symptoms and signs remain unchanged or continue to progress or worsen after treatment, or other antibacterial treatment measures need to be used; and 3) clinical efficacy rate, calculated based on the number of clinically cured cases.
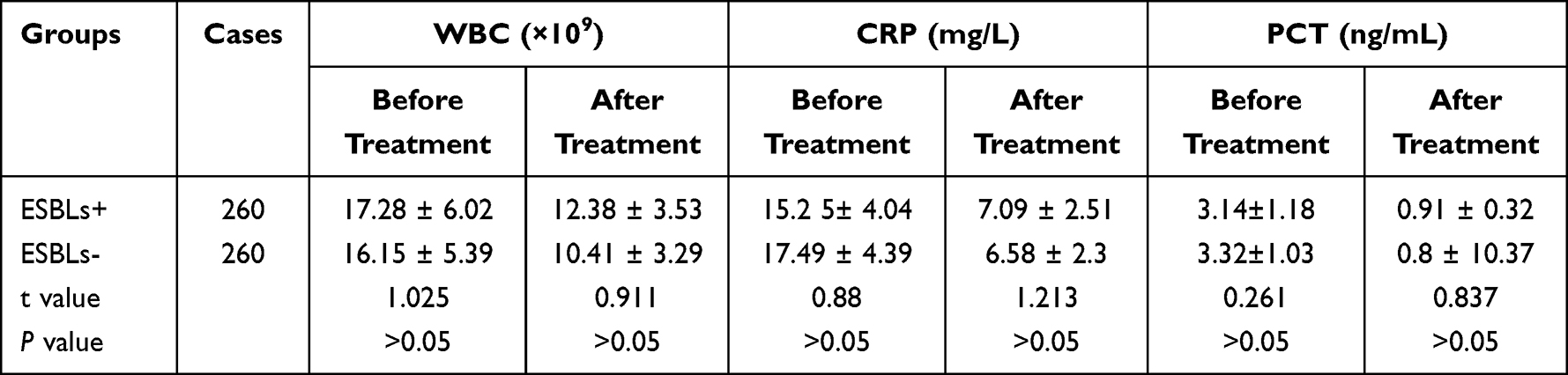 |
Table 3 Serum Inflammatory Marker Changes in Two Groups of Patients with Bloodstream Infection Caused by Escherichia coli Before and After Treatment (X±s) |
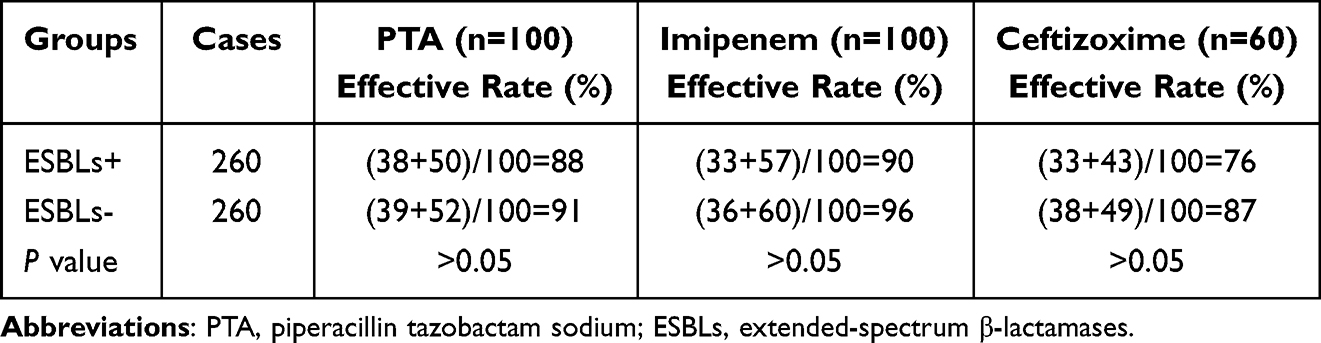 |
Table 4 Comparison of the Therapeutic Effects of Three Antibiotics: PAT, Imipenem, and Ceftizoxime |
The changes in serum inflammatory markers in 520 patients with bloodstream infections due to E. coli before and after antibiotic treatment are shown in Table 3. The blood WBC count, CRP, and PCT levels of both groups were significantly lower compared to before treatment, and the differences were statistically significant (P<0.05). However, there were no significant differences in the WBC count, CRP, and PCT levels between the two groups after antibiotic treatment (P>0.05).
Among the 2356 patients with bloodstream infections due to E. coli, 568 patients who experienced treatment failure were excluded. The remaining patients were divided into two groups: 260 patients with ESBL-positive E. coli and 260 patients with ESBL-negative E. coli. Among the 260 patients, 100 were treated with piperacillin/tazobactam, 100 were treated with imipenem, and 60 were treated with ceftizoxime (CZ). The effective rate of clinical efficacy (%) was calculated as the sum of the remarkable effect and effect divided by the total number of cases. There were no significant differences in the clinical efficacy of PTA, IMP, and CZ between the two groups (P>0.05), as shown in Table 4.
Subsequently, we further divided the cases into two groups: ESBLs-positive and ESBLs-negative. The clinical medication information of patients in both groups was analyzed. The three most frequently used antibiotics were: third-generation cephalosporins: CZ; Carbapenems: imipenem (IMP); Penicillin/beta-lactamase inhibitor: piperacillin sodium and tazobactam sodium for injection (PTZ). Among them, IMP was the most commonly used antibiotic in the treatment of ESBLs-positive E. coli, while PTZ and CZ were more commonly used in ESBLs-negative cases (Figure 1A). The antimicrobial susceptibility test results of both groups were analyzed, and the resistance rates of various antibiotics were calculated. The resistance rates of ESBLs-positive E. coli to second- and third-generation cephalosporins were as follows (Figure 1B): cefuroxime sodium (CXM) 100%, cefazolin (CZO) 100%, cefotaxime (CTX) 100%, ceftazidime (CAZ) 41.3%; fourth-generation cephalosporin: FEP 35.4%; penicillin/beta-lactamase inhibitor: piperacillin sodium and tazobactam sodium (TZP) 10.4%; the resistance rates to meropenem (MEM), tigecycline (TGC), and IMP were 0% (Figure 1C).
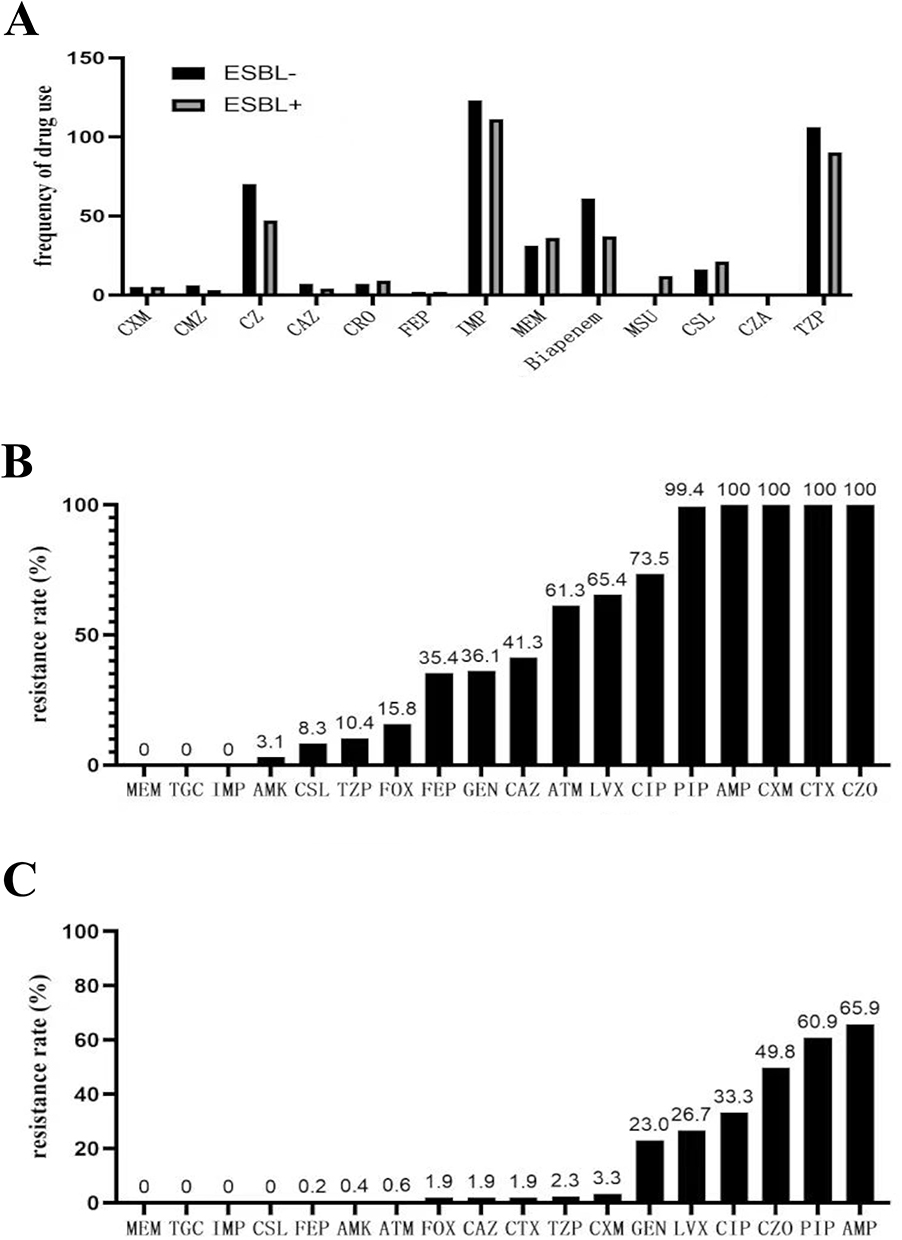 |
Figure 1 Clinical characteristics of the patient. (A) Drug use frequency of bloodstream infection positive ESBLs− group and ESBLs+ group; (B) Drug resistance rate of ESBLs+ Escherichia coli with positive bloodstream infection; (C) Drug resistance rate of ESBLs− Escherichia coli with positive bloodstream infection. Abbreviations: FEP, Cefepime; CAZ, Ceftazidime; CXM, Cefuroxime Sodium; CMZ, Cefmetazole; CZ, Ceftizoxime; CRO, Ceftriaxone; FOX, Cefoxitin; CTX, Cefotaxime; CZO, Cefazolin; CSL, Cefoperazone Sodium and Sulbactam Sodium for Injection; TZP, Piperacillin Sodium and Tazobactam Sodium for Injection; ATM, Aztreonam; LVF, Levofloxacin hydrochloride; CIP, Ciprofloxacin; PIP, Piperacillin Sodium; GEN, Gentamicin; MEM, Meropenem; IMP, Imipenem; TGC, Tigecycline; AMP, Ampicillin; CZA, Ceftazidime and Avibactam Sodium for Injection; MSU, Mezlocillin/Sulbactam. |
Identification of ESBLs-Positive Genotypes
Using PCR method, a total of 188 ESBLs-positive E. coli genotypes were detected, among which 124 strains carried both CTX-M-9 and TEM-1 genotypes, 22 strains carried two types of CTX-M genotypes (CTX-M-1 and CTX-M-2), 20 strains carried both CTX-M-9 and OXA-10, and 6 strains carried three genotypes simultaneously (CTX-M-9, TEM-1, and OXA-10) (Table 5).
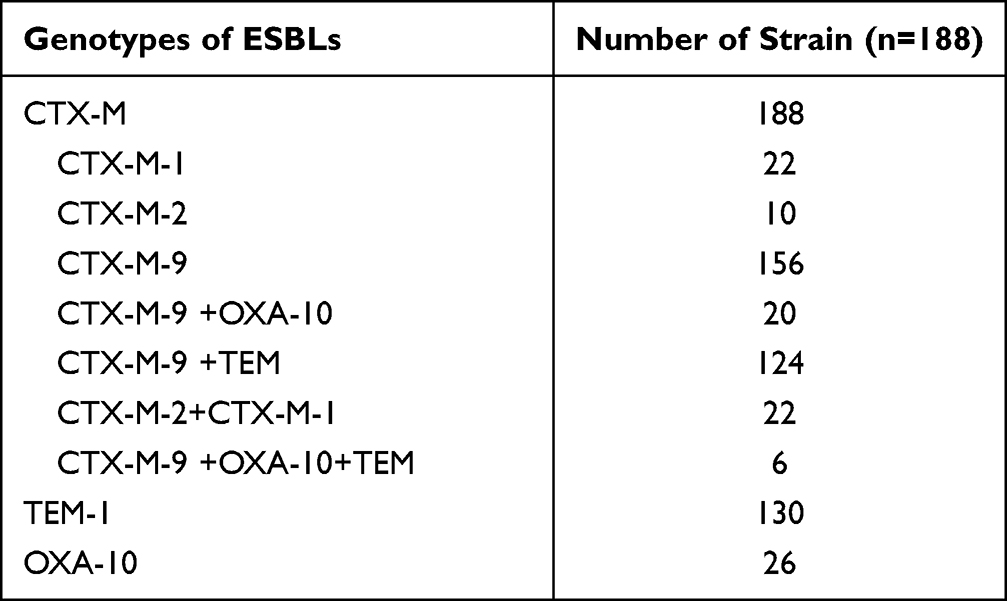 |
Table 5 Genotyping of 188 ESBLs-Positive E. coli Strains |
Agarose gel electrophoresis results showed that the ESBLS-positive gene fragments amplified by PCR were between 800–1073bp: CTX-M-9 (Figure 2A), TME-1 (Figure 2B), CTX-M-1 and CTX-M-2 (Figure 2C), OXA-10 (Figure 2D).
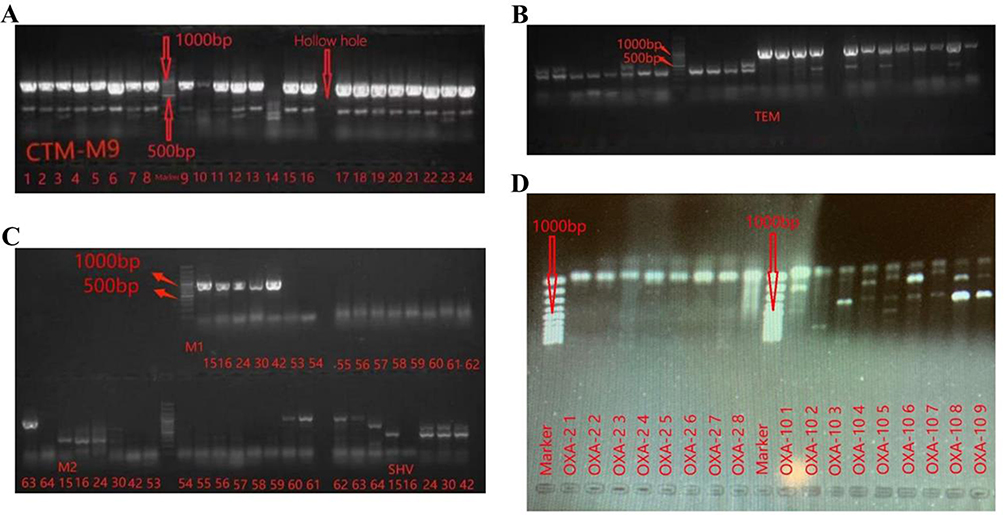 |
Figure 2 Electrophoresis results. (A) The electrophoresis results of CTXM-9 showed that the amplified gene fragments were 876 bp; (B) The electrophoresis results of TME-1 showed that the amplified gene fragments were 1073 bp; (C) The electrophoresis results of CTXM-1 and CTXM-2 showed that the amplified gene fragments were 827 bp and 876 bp, respectively; (D) The electrophoresis results of OXA-10 showed that the amplified gene fragments were 801 bp. |
Mutant Prevention Concentration (MPC)
When using antibiotics, in order to prevent bacteria from developing resistance mutations, it is necessary to use concentrations higher than the minimum inhibitory concentration to treat infections. This can effectively reduce the risk of bacteria developing resistance. Therefore, we further validated the MPC of ESBLs-positive E. coli. Results showed that the MIC90 of ESBLs-positive E. coli group was 256, while the MIC90 of the ESBLs-negative group was 1, with a significant difference between the two groups (P<0.01). The MPC ranges of E. coli with and without ESBLs genes were 64–528 and 32–256, respectively (P>0.05), indicating no significant difference (Table 6). The selection index (IS, the ratio of MPC to MIC) values of ESBL-positive and ESBL-negative E. coli were 2 and 128, respectively, and the difference between the two groups was statistically significant (P<0.01).
 |
Table 6 MIC and MPC Results of Cefepime in E. coli with or without ESBLs Genes |
Discussion
Escherichia coli (E. coli) is the most common bacteria causing bloodstream infections, and the increasing prevalence of ESBLs-positive E. coli has led to a gradual decline in treatment efficacy and even treatment failure. Fourth-generation cephalosporin-FEP has been widely used to treat severe infections caused by ESBLs-positive gram-negative and gram-positive bacteria.9 However, it is currently unclear how ESBLs-positive E. coli affects FEP resistance in patients with bloodstream infections (BSI).
We retrospectively analyzed the resistance rates of 2356 ESBLs-positive E. coli strains to different cephalosporins from 2016 to 2022. The results showed that only FEP and ceftazidime maintained a certain sensitivity, with rates of 35.4% and 41.3%, respectively, while the resistance rates of cefuroxime Sodium, cefotaxime, and cefazolin were 100%. Among other antibiotics, the resistance rates of piperacillin tazobactam (PTA), meropenem, and imipenem were 10.4%, 0%, and 0%, respectively. Imipenem is one of the most commonly used drugs for the clinical treatment of ESBLs-positive bacterial infections, but its long-term use can easily lead to resistance due to the induction of AmpC Beta-Lactamases in E. coli,10 which limits its clinical application. We found that FEP is often used to treat leukemia patients with combined infections. Compared with other cephalosporins, FEP not only has good stability against β-lactamase produced by bacteria and is less likely to induce resistance,11 but also has good clinical application prospects in the treatment of ESBLs-positive E. coli infections. At the same time, giving a higher dose of FEP to Gram-negative rods can also achieve ideal therapeutic effects.12 The above results have guiding significance for clinical doctors in the selection and use of drugs for the treatment of ESBLs-positive bacterial infections.
We further identified the genotypes of ESBLs-positive E. coli that were resistant to FEP and sensitive to CAZ in this study, and found that the main genotypes were CTX-M and TEM-1 (Table 5). Among them, 124 strains carried both CTX-M-9 and TEM-1 types, which was consistent with previous reports.13 The presence of the TEM-1 gene in E. coli represents resistance to ampicillin and penicillin,14 while the presence of the CTX-M gene confers resistance to cefotaxime and ceftriaxone. The main genotypes of ESBLs-positive E. coli in this study were CTX-M-9 and TEM-1, which also explains why cefotaxime is ineffective in treating these bacteria. In addition, we found that through statistical analysis of the drug sensitivity test results of 2356 E. coli strains, all cefotaxime-sensitive E. coli were ESBLs-negative, which verified the conclusion that the high resistance rate of cefotaxime is related to the CTX-M-9 and TEM-1 genotypes. This indicates that the drug resistance of E. coli is closely related to its genotype, and suggests that clinicians should choose drugs accurately based on different genotypes and resistance situations to avoid further exacerbation of drug resistance.
We performed genotyping on ESBLs-positive E. coli strains that were resistant to FEP and sensitive to CAZ. The results showed that 26 strains had the OXA-10 genotype. It has been reported that the expression of OXA-2 or OXA-10 genotypes can increase the MIC value of FEP or cefpirome in Enterobacteriaceae,15 but does not affect the MIC value of CAZ, especially when the expression of outer membrane protein OMP is reduced or inactivated. These resistant genes are spread through plasmids and should be avoided from causing outbreaks in clinical settings.8,12 We found that the ESBLs-positive E. coli strains resistant to FEP and sensitive to CAZ may be due to the presence of the OXA-10 gene.
Traditional antimicrobial therapy for bacterial infections is based on the MIC theory. However, because the MIC strategy only aims to inhibit or kill most sensitive bacteria, resistant mutants can selectively enrich and multiply, leading to treatment failure. The MPC is the lowest concentration that prevents the enrichment and amplification of drug-resistant mutants. When the concentration of an antimicrobial agent reaches or exceeds the MPC, it can inhibit the enrichment and amplification of drug-resistant mutants. When the concentration range is between the MPC and MIC, drug-resistant mutants are more prone to selective enrichment. This is often indicated by the selection index (SI), which is the ratio of MPC to MIC. A higher SI indicates a greater tendency to select for drug-resistant mutants, leading to treatment failure. We observed that the MIC values of ESBL-positive E. coli were higher than those of ESBL-negative strains, indicating that E. coli carrying ESBL genes, especially OXA-10, may have higher MIC values. For ESBL-negative E. coli, the MPC value of FEP increased abruptly, which may be due to inoculum effect. Inoculum effect refers to the phenomenon of disproportionate increases in MIC values with increasing bacterial inoculum. In severe infections caused by E. coli, the blood concentration of bacteria in patients can rise rapidly, far exceeding the inoculum concentration of MIC and resulting in a high SI of cefepime, enrichment of drug-resistant mutants, and clinical treatment failure.16,17
Conclusion
ESBLs-positive E. coli has an increased resistance to FEP; the inoculation effect will cause an increase in MPC, In particular, an increase in the IS value indicates that drug-resistant mutants can selectively enrich and multiply, leading to clinical failure of antibiotic therapy. For patients with bloodstream infections caused by ESBLs-positive E. coli, caution should be exercised when using FEP in the treatment of bloodstream infections. Based on the results of drug sensitivity tests, penicillin with enzyme inhibitors such as piperacillin/tazobactam (PTA) should be the first choice, and when PTA treatment fails, further use of carbapenem antibiotics (such as IMP and MER) is warranted. These recommendations have important guiding significance for clinical doctors in the selection and use of drugs in the treatment of ESBLs-positive E. coli infections.
Abbreviations
BSI, bloodstream infections; CAZ, ceftazidime; CZO, cefazolin; CXM, cefuroxime sodium; CTX, cefotaxime; CZ ceftizoxime; E. coli, Escherichia coli; ESBLs, extended-spectrum β-lactamases; FEP, Cefepime; IMP, imipenem; IS, selection index; MEM, meropenem; MIC, Minimum inhibitory concentration; MPC, Mutant prevention concentration; PTA, piperacillin/tazobactam; TZP, piperacillin sodium and tazobactam sodium; TGC, tigecycline.
Ethics Approval
This study was approved by the ethics committee of The Second Affiliated Hospital of Chongqing Medical University (No. 202308V1). The study completely followed the guiding principles in the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Joint general project of the Chongqing Science and Technology Bureau and the Chongqing Municipal Health Commission (2023MSXM117).
Disclosure
The authors declare that they have no competing interests.
References
1. Kaye KS, Pogue JM. Infections caused by resistant gram-negative bacteria: epidemiology and management. Pharmacotherapy. 2015;35(10):949–962. doi:10.1002/phar.1636
2. Minghua Z, Teng W, Wang T, et al. Long term characteristics of clinical distribution and resistance trends of carbapenem-resistant and extended-spectrum β-lactamase Klebsiella pneumoniae infections: 2014–2022. Infect Drug Resist. 2023;16:1.
3. Lu T, Quan JJ, Wang YF, et al. Prevalence of extended-spectrum beta-lactamases-producing Escherichia coli and Klebsiella pneumoniae in community-onset bloodstream infections from county hospitals of Zhejiang Province. Chin J Infect Dis. 2017;35(4):198–202.
4. Emel M-K, Mesut Y, Berna Ö-Ç. In vitro synergistic effect and mutant prevention concentrations of cefepime alone or in combination with sulbactam against OXA-48-positive Klebsiella pneumoniae isolates. Curr Microbiol. 2020;77(9):1.
5. Mataracı-Kara E, Özbek-çelik B, Yılmaz M, et al. In vitro synergistic effect and mutant prevention concentrations of cefepime alone or in combination with sulbactam against OXA-48-positiveKlebsiellapneumoniaeIsolates. Curr Microbiol. 2020;77(9):2137–2142. doi:10.1007/s00284-020-02094-0
6. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
7. An G, Creech CB, Wu N, et al. Population pharmacokinetics and target attainment analyses to identify a rational empirical dosing strategy for cefepime in critically ill patients. J Antimicrob Chemoth. 2023;78(6):1460–1470. doi:10.1093/jac/dkad106
8. Yang F, Chen P, Wang H. Comparative minimal inhibitory and mutant prevention concentration of eight antimicrobial agents against Klebsiella pneumoniae. Microb Drug Resist. 2022;28(2):229–235. doi:10.1089/mdr.2021.0228
9. Brennan-Krohn TAS, Kenneth P, James E, Kirby JE. Improved accuracy of cefepime susceptibility testing for extended-spectrum-beta-lactamase-producing Enterobacteriaceae with an on-demand digital dispensing method. J Clin Microbiol. 2017;55(2):470–478. doi:10.1128/JCM.02128-16
10. Martinez-Martinez L, Conejo MC, Pascual A, et al. Activities of imipenem and cephalosporins against clonally related strains of Escherichia coli hyperproducing chromosomal β-lactamase and showing altered porin profiles. Antimicrob Agents Chemother. 2000;44(9):2534–2536. doi:10.1128/AAC.44.9.2534-2536.2000
11. Edelberto S. Pharmacokinetics and pharmacodynamics of cefepime in adults with hematological malignancies and febrile neutropenia after chemotherapy. Antibiotics. 2021;10(5):1.
12. Christopher M, Brian E, Kirby J, et al. Outcomes associated with empiric cefepime for bloodstream infections caused by ceftriaxone-resistant, cefepime-susceptible Escherichia coli and Klebsiella pneumoniae. Int J Antimicrob Agents. 2023;61(5):106762. doi:10.1016/j.ijantimicag.2023.106762
13. Melika M, Yasmine E. Intestinal colonization with multidrug-resistant Enterobacterales: screening, epidemiology, clinical impact, and strategies to decolonize carriers. Eur J Clin Microbiol Infect Dis. 2023;42(3):1.
14. Clasen J, Birkegård AC, Græsbøll K, Folkesson A. Evolution of TEM-type extended-spectrum β-lactamases in Escherichia coli by cephalosporins. J Glob Antimicrob Res. 2019;19:32–39. doi:10.1016/j.jgar.2019.03.010
15. Aubert D, Pairel L, Chevalier J, Leotard S, Pages J-M, Nordmann P. Oxacillinase-mediated resistance to cefepime and susceptibility to ceftazidime in Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2001;45:16151620. doi:10.1128/AAC.45.6.1615-1620.2001
16. Li Z, Feng S, Sun G, et al. Extensively drug-resistant Gram-negative bacterial bloodstream infection in hematological disease. Infect Drug Resist. 2019;12:481–491. doi:10.2147/IDR.S191462
17. Mizrahi A, Chat L, Danjean M, et al. Inoculum effect of Enterobacterales co-expressing OXA-48 and CTX-M on the susceptibility to ceftazidime/avibactam and meropenem. Eur J Clin Microbiol. 2022;41(5):853–858. doi:10.1007/s10096-022-04430-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.