Back to Journals » International Journal of General Medicine » Volume 18
The Impact of Echogenicity Grading on the Diagnostic Performance of C-TIRADS
Authors Huang GL, Su JY, Liang RQ, Yang XY ![]() , Xu LF
, Xu LF
Received 20 May 2025
Accepted for publication 30 August 2025
Published 15 September 2025 Volume 2025:18 Pages 5509—5517
DOI https://doi.org/10.2147/IJGM.S541530
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Ge-Lang Huang,1,* Jing-Yan Su,2,* Rui-Qiao Liang,3 Xi-Yue Yang,3 Li-Fang Xu4
1Department of Rehabilitation, Guigang Peoples’s Hospital, Guigang, Guangxi Zhuang Autonomous Region, People’s Republic of China; 2Department of Radiology, Guangxi Zhuang Autonomous Region Corps Hospital of Chinese People’s Armed Police Force, Nanning, Guangxi Zhuang Autonomous Region, People’s Republic of China; 3Department of Diagnostic Ultrasound, Guigang Peoples’s Hospital, Guigang, Guangxi Zhuang Autonomous Region, People’s Republic of China; 4Department of Diagnostic Ultrasound, The Second Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi Zhuang Autonomous Region, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li-Fang Xu, Department of Diagnostic Ultrasound, The Second Affiliated Hospital of Guangxi Medical University, No. 166, Daxuedong Road East, Nanning, Guangxi Zhuang Autonomous Region, 530007, People’s Republic of China, Email [email protected]
Purpose: To investigate whether echogenicity grading can improve the diagnostic performance of the Chinese Thyroid Imaging Reporting and Data System (C-TIRADS).
Patients and methods: Ultrasonic (US) images of 646 thyroid nodules (TNs) were retrospectively reviewed. The sonographic features of each nodule were analyzed and noted, including the orientation, margin, composition, echogenicity, echogenic foci, and extrathyroidal extension. Hypoechoic was further graded as mildly, moderately and markedly hypoechoic, and the malignancy risk at different echogenicity levels was compared. Each nodule was categorized according to C-TIRADS using markedly hypoechoic, modified markedly hypoechoic, and hypoechoic as malignant indicators, and the classification results were recorded as TI-RADS 1, 2, and 3, respectively. The diagnostic sensitivity, specificity, and area under the curve (AUC) of the different echogenicity and TIRADS were compared using chi-square analysis and Receiver Operating Characteristic curves (ROC). Binary logistic regression analysis was used to calculate cancer risk for different echogenicity. The interobserver agreement in the grading of echogenic of the nodules was also assessed.
Results: Most malignant nodules were hypoechoic (85.2%), and the malignancy risk of hypoechoic nodules was significantly higher than that of iso-hyperechoic nodules (34.4% vs 9.8%). The malignancy risk gradually increased as nodule echogenicity decreased (odd ratios (ORs) of 2.132, 10.009, and 15.006, respectively). There was no significant difference in the malignancy risk between moderately and markedly hypoechoic nodules (P=0.203). The modified markedly hypoechoic region showed the highest AUC and the most balanced sensitivity and specificity for the diagnosis of thyroid cancer. The diagnostic performance of TI-RADS 2 was significantly higher than that of TI-RADS 1 and 3 (AUC of 0.715, 0.608, and 0.656, respectively). Substantial agreement was obtained between the two observers in grading markedly hypoechoic and modified markedly hypoechoic (κ = 0.79 and 0.75; 95% CI: 0.75,0.83 and 0.64,0.86).
Conclusion: Stratifying hypoechogenic to three degrees enhances confidence in evaluating malignancy risk. Compared to markedly hypoechoic, the modified markedly hypoechoic significantly boosted the ability of C-TIRADS to differentiate benign TNs from malignant ones.
Keywords: ultrasound, thyroid nodule, echogenicity, thyroid imaging reporting and data system, diagnostic performance
Introduction
Recently, there has been a global increase in the incidence of thyroid nodules (TNs), with prevalence rates reaching 65% in the general population.1 However, only 7–15% of TNs cases are diagnosed as malignant, underscoring the importance of excluding carcinomas.2 Ultrasound (US) is frequently employed in the evaluation of thyroid disorders because of its simplicity, non-invasiveness, repeatability, and efficacy in differentiating malignant nodules from benign nodules.3–7 In general, US characteristics such as vertical orientation, solid composition, markedly hypoechogenic, microcalcifications, irregular margins, or extrathyroidal extension are predominantly associated with malignant thyroid nodules.3–7 Conversely, features such as cystic composition, horizontal orientation, isoechoic or hyperechogenic, and macrocalcifications are typically indicative of benign lesions.8 However, taken individually, each of these features is poorly predictive.
Echogenicity is one of the most critical US characteristics for TNs assessment. The echogenicity of thyroid nodules is typically classified into four grades: hyperechoic, isoechoic, mildly hypoechoic, and markedly hypoechoic, relative to the surrounding thyroid parenchyma or strap muscles of the neck.6,7 Previous studies have shown that the grade of nodule echogenicity is closely related to its benign and malignant nature, with markedly hypoechogenic often implying malignant and mildly hypoechoic, usually benign.9,10 This stratification is crucial in the ultrasound malignancy risk assessment of TNs, as it helps to distinguish between different levels of risk based on echogenicity. Various Thyroid Imaging Reporting and Data System (TIRADS) guidelines, such as those from the American College of Radiology (ACR), European TIRADS (EU-TIRADS), and others, incorporate this feature into their risk stratification models to help differentiate between benign and malignant TNs.3,6,7
Recently, a limited group of researchers have categorized hypoechoic lesions into three distinct degrees: mildly, moderately, and markedly.9,10 These findings indicated that nodules exhibiting moderately to markedly hypoechogenic were associated with a higher risk of malignancy than those with mildly hypoechogenic. Furthermore, the analysis revealed no statistically significant difference in malignancy risk between markedly and moderately hypoechoic nodules,9,10 emphasizing the role of hypoechogenic in the risk assessment. Few studies have indicated that using moderately hypoechoic areas as a risk indicator notably enhances the diagnostic accuracy of Chinese Thyroid Imaging Reporting and Data System (C-TIRADS).11 The C-TIRADS which proposed in 2002 is popular in China for its simplicity and convenience with counting positive and negative signs to classify TNs. Besides, several studies showed that the diagnostic performance of C-TIARS was compare favorably with the other guidelines12–14 while some did not show satisfactory results.15 This study aimed to determine whether a three-level hypoechogenic grading system would enhance the diagnostic performance of the C-TIRADS.
Methods
Study Population
This retrospective observational study was approved by the Institutional Review Board of The Guigang People’s Hospital, and informed consent was waived by the patients (No. GYYXLL-20210601-15). The study complied with the Declaration of Helsinki. All subjects were selected from among the 728 individuals who underwent thyroid surgery at our hospital between January 2021 and February 2023. Only one nodule with the most suspicious ultrasound features per patient was selected in this study to avoid possible inconsistencies. Only solid nodules with a definitive pathological diagnosis were selected. All data were collected from the hospital’s electronic archive system and de-identified. In total, 648 nodules from 648 patients were included in this study. The study group selection process is illustrated in Figure 1.
 |
Figure 1 Flowchart of selecting study group. Abbreviation: US, ultrasound. |
Image Acquisition
All US scans of the thyroid were performed using a 5–12-MHz linear array transducer (LOGIQ S8 or LOGIQ E9; GE Healthcare, Wauwatosa, WI, USA) by experienced sonologists. Thyroid ultrasound examinations were conducted in accordance with the practice guidelines established by the American Institute of Ultrasound in Medicine (AIUM) for performing thyroid US.16 At least two US images of each nodule were obtained in both the transverse and longitudinal planes, and subsequently archived in the US numerical database.
Image Analysis
Two blinded, professionally trained US physicians (X.Y.Y and R.Q.L) with more than 10 years of experience in thyroid US independently analyzed and recorded all retained US images. The most suspicious nodule was selected for patients with multiple nodules and the largest nodule was chosen if no suspicious nodules were present. The maximum diameter of the nodule and US features such as morphology, margin, structure, echogenicity, focal echogenic foci, and extrathyroidal invasion were noted. In cases of discrepancies between X. Y. Y. and R. Q. L., a third ultrasound physician (L. F. X)., with 15 years of expertise in thyroid ultrasound diagnosis, made the final decision. All nodules were categorized using L.F.X. based on the C-TIRADS.
According to C-TIRADS,7 positive indicators of US features include vertical orientation, blurred or irregular margins, extrathyroidal invasion, solid composition, markedly hypoechoic, and microcalcifications. The negative indicator is the comet tail artifact. +1 were scored for each positive indicator, and −1 points for each negative indicator. The total score was categorized as follows: 1 point is classified as TI-RADS 4A, 2 points is classified as TI-RADS 4B, 3–4 points is classified as TI-RADS 4C, and 5 is categorized as TI-RADS 5.
The nodule echogenicity was classified as iso-hyperechoic (echogenicity similar to or higher than the surrounding thyroid parenchyma), hypoechoic (echogenicity lower than the surrounding thyroid parenchyma), mildly hypoechoic (echogenicity lower than the surrounding thyroid parenchyma but higher than the strap muscles of the neck), moderately hypoechoic (echogenicity equal to the strap muscles of the neck), and markedly hypoechoic (echogenicity lower than the strap muscles of the neck) (Figure 2A–E). 10 When different echogenic presented in one nodule, dominant echogenic was noted.
 |
Figure 2 Thyroid nodules with different echogenic. Figure A to E sequentially displays isoechoic (A), hyperechoic (B), mildly hypoechoic (C), moderately hypoechoic (D), and markedly hypoechoic (E) nodules respectively, indicated by capiler “+”. The white arrows indicate the anterior strap muscles. |
All nodules were graded separately using the C-TIRADS, with markedly hypoechoic, modified markedly hypoechoic (echogenic equal to or lower than that of the strap muscles), and hypoechoic as a positive indicator. The classification results are denoted as TI-RADS 1, 2, and 3.
100 nodules were randomly selected to evaluate the interobserver variability of grading echogenic. The ultrasound images of these nodules were separately assigned to the primary observer X. Y. Y. and R. Q. L., both were blinded to the pathology results.
Data Analysis and Statistics
Statistical analysis was conducted using Medcalc15.2 and SPSS 27.0. Data normality was assessed using the Kolmogorov–Smirnov (K-S) test. Normally distributed data are presented by  , non-normally distributed data are presented as median (interquartile range), and categorical data are expressed as percentages. The comparison of normally distributed data between the two groups was performed using an independent sample t-test, whereas the Mann–Whitney U-test was employed to compare two non-normally distributed data. The composition ratios for the counted data were compared using the chi-square test. McNemar’s test was used to compare sensitivity and specificity. P < 0.05. Pairwise comparisons between groups of count data were conducted using the Chi-square segmental test with adjustment of significance level, where P < 0.008 was considered statistically significant. Binary logistic regression analysis was used to calculate the risk of thyroid carcinoma associated with the different echogenicity. Receiver operating characteristic (ROC) curves were constructed to facilitate comparison and analysis of the area under the curve (AUC) for diagnosing thyroid carcinoma across various echogenic types and classification methodologies. The interobserver agreement for the degree of echogenic was calculated using the Cohen Kappa statistic. κ ≤0.2 was interpreted as slight agreement; 0.21~0.40 as fair; 0.41~0.60 as moderate; 0.61~0.80 as substantial and 0.81~1.0 as perfect agreement.
, non-normally distributed data are presented as median (interquartile range), and categorical data are expressed as percentages. The comparison of normally distributed data between the two groups was performed using an independent sample t-test, whereas the Mann–Whitney U-test was employed to compare two non-normally distributed data. The composition ratios for the counted data were compared using the chi-square test. McNemar’s test was used to compare sensitivity and specificity. P < 0.05. Pairwise comparisons between groups of count data were conducted using the Chi-square segmental test with adjustment of significance level, where P < 0.008 was considered statistically significant. Binary logistic regression analysis was used to calculate the risk of thyroid carcinoma associated with the different echogenicity. Receiver operating characteristic (ROC) curves were constructed to facilitate comparison and analysis of the area under the curve (AUC) for diagnosing thyroid carcinoma across various echogenic types and classification methodologies. The interobserver agreement for the degree of echogenic was calculated using the Cohen Kappa statistic. κ ≤0.2 was interpreted as slight agreement; 0.21~0.40 as fair; 0.41~0.60 as moderate; 0.61~0.80 as substantial and 0.81~1.0 as perfect agreement.
Results
Demographic Characteristics
A total of 646 nodules from 646 patients (103 men, 543 women) were included in this study. The average age was 48 (35,55) years, and the maximum diameter was 26.0 (16.0,35.0) mm. Of the 646 nodules, 484 (74.9%) were benign, and 162 (25.1%) were malignant. Among the benign nodules, 456 (94.2%) were goiters, 20 (4.1%) were adenomas, 3 (0.6%) had Hashimoto’s thyroiditis, and 5 (1.0%) had subacute thyroiditis. Of the malignant tumors, 158 (97.5%) were papillary carcinomas and 4 (2.5%) were follicular carcinomas. The benign group was older than the malignant group (49y vs 41y, P=0.001), and benign nodules were larger than malignant ones (28.0 mm vs 20.5 mm, P < 0.001). Women comprised the majority of the patients in both groups. Demographic characteristics are shown in Table 1.
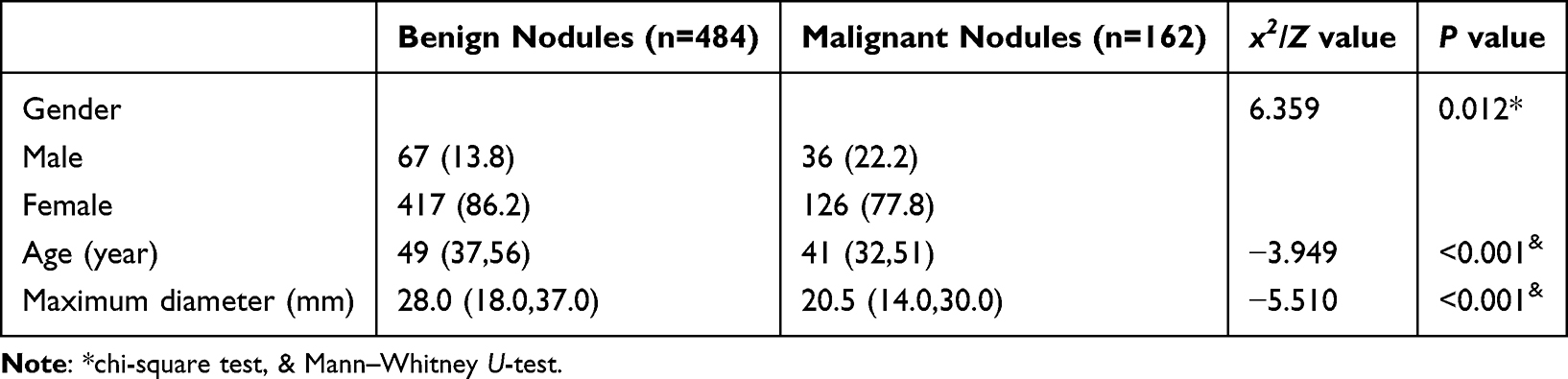 |
Table 1 Demograpic Characteristics [n (%) / M (P25, P75)] |
Relationship Between Echogenicity and Nodule Malignancy
The majority of malignant nodules were hypoechogenic, accounting for 85.2% (138/162) of cases. The malignancy rate of hypoechoic nodules was significantly higher than that of iso-hyperechogenic nodules (34.4% vs 9.8%, P < 0.001). Following tri-grading of hypoechoic nodules, significant differences in malignancy rates were observed between iso-hyperechoic nodules and various grades of hypoechoic nodules (P < 0.001, Table 2). The Chi-square segmental test showed that mildly hypoechoic nodules had a higher malignancy risk than iso-hyperechoic nodules, but a lower malignancy risk than moderately or markedly hypoechoic nodules (all P < 0.008). Moderately and markedly hypoechoic nodules had higher malignancy rates than iso-hyperechoic or mildly hypoechoic nodules (all P < 0.008), with no significant difference between moderately and markedly hypoechoic nodules (x2 = 1.622, P = 0.203). Binary logistic regression analysis showed that compared with iso-hyperechoic nodules, the malignancy risk progressively increased for mildly, moderately, and markedly hypoechogenic nodules, with odds ratios (ORs) of 2.132, 10.009, and 15.006, respectively, and 95% CI of 1.250~3.637, 5.597~17.898 and 7.929~28.402 respectively (Table 3).
 |
Table 2 Malignant Risk Regarding Different Echogenicity |
 |
Table 3 Binary Logistic Analysis Results of Hypoechogenicity Grading and Risk of Thyroid Cancer |
Comparison of Diagnostic Performance
When diagnosing thyroid carcinoma, markedly hypoechoic lesions had the highest specificity (94.4%) but the lowest sensitivity (27.7%). Hypoechoic lesions showed the lowest specificity (46.1%) and highest sensitivity (86.2%). The modified markedly hypoechoic area offered a balanced sensitivity and specificity of 58.0% and 84.9%, respectively. There were significant differences in the sensitivity and specificity across all echo levels (all P < 0.001). The modified markedly hypoechoic area achieved the highest AUC for diagnosis, significantly outperforming both markedly hypoechoic and hypoechoic areas (all P < 0.001) (Table 4).
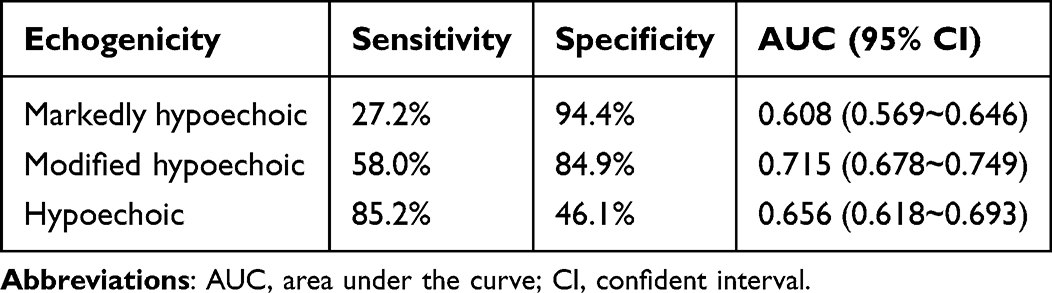 |
Table 4 Diagnosis Efficiency of Different Echogenicity in Discriminating Malignant Nodules |
As shown in Figure 3, TIRADS-2 had a significantly higher AUC of 0.858 (95% CI: 0.828–0.884) for diagnosing thyroid carcinoma than TIRADS-1 and TIRADS-3, both at 0.814 (95% CI: 0.782–0.844), with Z-values of 4.100 and 4.281, respectively, and P values <0.001. No significant difference was observed between TIRADS-1 and TIRADS-3 (Z=0.006, P=0.9952).
 |
Figure 3 The diagnostic efficacy of different TIRADS in diagnosis of thyroid carcinoma. Note: TI-RADS1, categorized results using markedly hypoechoic as positive indicator; TI-RADS2, categorized results using modified markedly hypoechoic as positive indicator; TI-RADS3, categorized results using hypoechoic as positive indicator. |
Interobserver Agreement of Grading Echogenicity
Both modified markedly hypoechogenic and markedly hypoechogenic achieved substantial agreement between the two observers (κ = 0.79 and 0.75; 95% CI: 0.75,0.83 and 0.64,0.86).
Discussion
This study found that iso-hyperechoic nodules had a significantly lower malignancy rate (9.8%) than that of hypoechoic nodules (34.4%). Mildly, moderately, and markedly hypoechoic nodules also showed higher malignancy rates than iso-hyperechoic nodules; however, no significant difference was observed between moderately and markedly hypoechoic nodules. Further regression analysis indicated that a progressive increase in cancer risk was correlated with mildly, moderately, and markedly hypoechoic characteristics, yielding ORs of 2.132, 10.009, and 15.006, respectively. When mildly, modified moderately, and markedly hypoechogenic were employed as distinct indicators for diagnosing thyroid cancer, the curve (AUC) for modified moderately hypoechogenic was the largest, exceeding those of mildly and markedly hypoechogenic. Moreover, the AUC for C-TIRADS in diagnosing thyroid cancer demonstrated significant enhancement when modified moderately hypoechogenic was utilized as a malignancy indicator. Both modified markedly hypoechoic and markedly hypoechoic achieved substantial agreement between the two observers.
Common thyroid nodules consist of four main histopathological components: (1) Follicular cells, which produce colloid in the thyroid follicles; (2) Colloid, a gel-like substance made of thyroglobulin; (3) Papillary cancer cells, linked to papillary carcinoma, featuring tall epithelial cells with “ground-glass” nuclei and often psammoma bodies; and (4) Fibrosis, seen in papillary carcinoma and as nodular goiter progress.17 Chen observed that fibrous tissues exhibited the lowest echogenicity, followed by papillary carcinoma cells, follicular cells, and colloids.18 The echo level of a nodule depends on the combination of these four components. Papillary thyroid carcinomas, with more cancer cells and widespread fibrosis, tend to be hypoechoic, and more fibrosis results in lower echogenicity.9,10,19 Follicular tumors are often iso-hyperechoic because of their high proportion of follicular cells.20,21 Nodular goiter are characterized by enlarged follicular cells filled with glial components, making them mostly iso-hyperechoic.22–24 In this study, a substantial proportion (90.2%) of hyperechoic nodules were identified as benign, whereas the majority of malignant nodules (85.2%) exhibited hypoechoic characteristics, which is consistent with findings from previous research.10,24 The observed correlation between echogenicity and histopathological outcomes highlights the critical role of echogenicity grading in clinical management of thyroid nodules.
Although hypoechogenic demonstrates high sensitivity for the diagnosis of thyroid cancer, its specificity is comparatively low.10 Current Thyroid Imaging Reporting and Data System (TI-RADS) classifications do not categorize hypoechoic features as a direct malignant index.3,4,6,7,25 Instead, they differentiate between mildly and markedly hypoechoic characteristics, with the latter being considered indicative of malignancy. In this study, hypoechoic features showed a sensitivity of 85.2%, specificity of 46.1%, and AUC of 0.656 for diagnosing thyroid cancer, whereas markedly hypoechoic features showed a sensitivity of 27.2%, specificity of 94.4%, and AUC of 0.608. Although markedly hypoechogenic has a high specificity for diagnosing thyroid cancer, its sensitivity is very low. Liu et al identified modified markedly hypoechoic nodules as markers of thyroid cancer, achieving a balanced diagnostic sensitivity and specificity. The sensitivity improved from 28.03% to 63.26%, with only a slight decrease in specificity (91.53% to 84.88%).11 The study found that while the specificity for thyroid cancer with moderately hypoechoic lesions decreased slightly (84.9% vs 94.4%), the sensitivity increased significantly (58.0% vs 27.2%), achieving a good balance between sensitivity and specificity.
Due to the high specificity (91.5%~94.3%) of markedly hypoechogenic in the diagnosis of thyroid cancer,11,26 most TIRADS listed it as an indication of malignancy, and was defined as echogenic lower than that of the strap muscles.3,6,7 Some guidelines equated it with the strap muscles or described it as ambiguous (lower than the thyroid tissue echo or the strap muscles).4,25 The study found that hypoechoic nodules had a significantly higher malignancy rate than iso-hyperechoic nodules, with malignancy increasing as echogenic decreased (ORs of 2.132, 10.009, and 15.006). However, Chi-square analysis revealed no significant difference in malignancy risk between moderately and markedly hypoechoic nodules, suggesting that moderately hypoechoic nodules also had a high malignancy risk and should not be overlooked. Delfim et al suggested that moderately hypoechoic features indicate malignancy in thyroid cancer diagnosis.10 Liu found that using modified markedly hypoechogenic as a malignancy indicator significantly improved the C-TIRADS diagnostic performance (AUC 0.878 vs 0.888, P=0.01).11 The study found that modifying markedly hypoechogenic as an indicator of malignancy significantly improved the diagnostic performance of C-TIRADS (AUC, 0.858 vs 0.814), consistent with Liu’s findings.
The agreement on grading modified markedly hypoechoic was substantial between the two observers might support the reliability of using this new definition to classify TNs. Also, it would be helpful in management of the TNs especially in nodules of C-TIRADS 4A. A solid moderate hypoechoic (echogenicity equal to the strap muscle) TNs was categorized as 4A according to C-TIRADS whereas 4B according this modified TIRADS. The new categorization implied much higher malignant risk of the nodule and more intervention such as FNA might be taken. Otherwise, conservative action should be taken on solid iso-hyperechogenic or mildly hypoechoic nodules which also categorized as 4A according to C-TIRADS for most of these nodules usually were benign.
There are certain limitations in this study: firstly, only cases with surgical pathological results were included, and cases with fine needle biopsy were not included, which may lead to a certain degree of selective bias; Secondly, the study’s retrospective nature posed another limitation. Future research should involve prospective studies with larger sample sizes should be conducted.
Conclusion
The echogenicity of TNs is closely linked to the malignancy risk, which increases as echogenicity decreases. Stratifying hypoechogenic into three degrees is of great help in differentiating between benign and malignant nodules. Using a modified hypoechoic as a malignancy index could greatly enhance the diagnostic performance of the C-TIRADS.
Abbreviation
TIRADS, Thyroid Imaging Reporting and Data System, C-TIRADS = Chinese Thyroid Imaging Reporting and Data System, US, ultrasound; TNs, thyroid nodules; AUC, area under the curve; OR, odds ratio; ROC, receiver operating characteristic, CI, confidence interval.
Funding
This study was supported by Guigang Science and Technology Projects, China (No. 2200023).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Durante C, Grani G, Lamartina L, Filetti S, Mandel SJ, Cooper DS. The diagnosis and management of thyroid nodules: a review. JAMA. 2018;319(9):914–924. doi:10.1001/jama.2018.0898
2. Gharib H, Papini E, Garber JR, et al. AACE/ACE/AME task force on thyroid nodules American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologic medical guidelines for clinical practice for the diagnosis and management of thyroid nodules – 2016 update. Endocr Pract. 2016;22(5):622–639. doi:10.4158/EP161208.GL
3. Grant EG, Tessler FN, Hoang JK, et al. Thyroid ultrasound reporting lexicon: white paper of the ACR Thyroid Imaging, Reporting and Data System (TIRADS) committee. J Am Coll Radiol. 2015;12(12):1272–1279. doi:10.1016/j.jacr.2015.07.011
4. Haugen BR, Alexander EK, Bible KC, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133. doi:10.1089/thy.2015.0020
5. Shin JH, Baek JH, Chung J, et al. Ultrasonography diagnosis and imaging-based management of thyroid nodules: revised korean society of thyroid radiology consensus statement and recommendations. Korean J Radiol. 2016;17(3):370–395. doi:10.3348/kjr.2016.17.3.370
6. Russ G, Bonnema Steen J, Erdogan Murat F, Durante C, Ngu R, Leenhardt L. European thyroid association guidelines for ultrasound malignancy risk stratification of thyroid nodules in adults: the EU-TIRADS. Eur Thyroid J. 2017;6(5):225–237. doi:10.1159/000478927
7. Zhou J, Yin L, Wei X, et al. 2020 Chinese guidelines for ultrasound malignancy risk stratification of thyroid nodules: the C-TIRADS. Endocrine. 2020;70(2):256–279. doi:10.1007/s12020-020-02441-y
8. Remonti LR, Kramer CK, Leitão CB, Pinto LC, Gross JL. Thyroid ultrasound features and risk of carcinoma: a systematic review and meta-analysis of observational studies. Thyroid. 2015;25(5):538–550. doi:10.1089/thy.2014.0353
9. Lee JY, Na DG, Yoon SJ, et al. Ultrasound malignancy risk stratification of thyroid nodules based on the degree of hypoechogenicity and echotexture. Eur Radiol. 2020;30(3):1653–1663. doi:10.1007/s00330-019-06527-8
10. Delfim RLC, Assumpção LR, Lopes F, de Fátima Dos Santos Teixeira P. Does a three-degree hypoechogenicity grading improve ultrasound thyroid nodule risk stratification and affect the TI-RADS 4 category? A retrospective observational study. Arch Endocrinol Metab. 2023;67(4):e000608. doi:10.20945/2359-3997000000608
11. Liu J, Luo T, Zhang H, et al. Markedly hypoechoic: a new definition improves the diagnostic performance of thyroid ultrasound. Eur Radiol. 2023;33(11):7857–7865. doi:10.1007/s00330-023-09828-1
12. Hu Y, Xu S, Zhan W. Diagnostic performance of C-TIRADS in malignancy risk stratification of thyroid nodules: a systematic review and meta-analysis. Front Endocrinol. 2022;13:938961. doi:10.3389/fendo.2022.938961
13. Jin Z, Pei S, Shen H, et al. Comparative study of C-TIRADS, ACR-TIRADS, and EU-TIRADS for diagnosis and management of thyroid nodules. Acad Radiol. 2023;30(10):2181–2191. doi:10.1016/j.acra.2023.04.013
14. Cai Y, Yang R, Yang S, et al. Comparison of the C-TIRADS, ACR-TIRADS, and ATA guidelines in malignancy risk stratification of thyroid nodules. Quant Imaging Med Surg. 2023;13(7):4514–4525. doi:10.21037/qims-22-826
15. Cai M, Chen L, Shui L, Lv X, Wang H. Explore the diagnostic performance of 2020 Chinese thyroid imaging reporting and data systems by comparing with the 2017 ACR-TIRADS guidelines: a single-center study. Endocrine. 2023;80(2):399–407. doi:10.1007/s12020-023-03304-y
16. American Institute of Ultrasound in M, American College of R, Society for Pediatric R, Society of Radiologists in U (2013) AIUM practice guideline for the performance. Thyroid and parathyroid ultrasound examination. J Ultrasound Med. 2013;32(7):1319–1329. doi:10.7863/ultra.32.7.1319
17. Isarangkul W. Dense fibrosis. Another diagnostic criterion for papillary thyroid carcinoma. Arch Pathol Lab Med. 1993;117(6):645–646.
18. Chen SJ, Yu SN, Tzeng JE, et al. Characterization of the major histopathological components of thyroid nodules using sonographic textural features for clinical diagnosis and management. Ultrasound Med Biol. 2009;35(2):201–208. doi:10.1016/j.ultrasmedbio.2008.08.017
19. Yang X-Y, Huang L-F, Han Y-J, Cen -X-X, Tao Z-X. Histopathological analysis of thyroid nodules with taller-than-wide shape in adults. Int J Gen Med. 2024;17:5123–5131. doi:10.2147/IJGM.S473731
20. Castellana M, Piccardo A, Virili C, et al. Can ultrasound systems for risk stratification of thyroid nodules identify follicular carcinoma? Cancer Cytopathol. 2020;128(4):250–259. doi:10.1002/cncy.22235
21. Park KW, Shin JH, Hahn SY, et al. Ultrasound-guided fine-needle aspiration or core needle biopsy for diagnosing follicular thyroid carcinoma? Clin Endocrinol. 2020;92(5):468–474. doi:10.1111/cen.14167
22. Moon WJ, Jung SL, Lee JH, et al. Benign and malignant thyroid nodules: US differentiation--multicenter retrospective study. Radiology. 2008;247(3):762–770. doi:10.1148/radiol.2473070944
23. Arpana Panta OB, Gurung G, Pradhan S, Pradhan S. Ultrasound findings in thyroid nodules: a radio-cytopathologic correlation. J Med Ultrasound. 2018;26(2):90–93. doi:10.4103/JMU.JMU_7_17
24. Kim JH, Na DG, Lee H. Ultrasonographic echogenicity and histopathologic correlation of thyroid nodules in core needle biopsy specimens. Korean J Radiol. 2018;19(4):673–681. doi:10.3348/kjr.2018.19.4.673
25. Ha EJ, Chung SR, Na DG, et al. 2021 Korean thyroid imaging reporting and data system and imaging-based management of thyroid nodules: korean society of thyroid radiology consensus statement and recommendations. Korean J Radiol. 2021;22(12):2094–2123. doi:10.3348/kjr.2021.0713
26. Prieditis P, Radzina M, Mikijanska M, et al. Non-markedly hypoechogenic nodules: multicenter study on the thyroid malignancy risk stratification and accuracy based on TIRADS systems comparison. Medicina. 2022;58(2):257. doi:10.3390/medicina58020257
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparing Diagnostic Efficacy of C-TIRADS Positive Features on Different Sizes of Thyroid Nodules

Zhou Y, Li WM, Fan XF, Huang YL, Gao Q
International Journal of General Medicine 2023, 16:3483-3490
Published Date: 14 August 2023