Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
The Impact of Age and Disease Entity on Small Airway Dysfunction in Obstructive Airway Diseases
Authors Li Y, Su KC, Hsiao YH ![]() , Chou KT, Li YJ, Jeng TH, Ko HK, Perng DW
, Chou KT, Li YJ, Jeng TH, Ko HK, Perng DW
Received 19 November 2024
Accepted for publication 9 March 2025
Published 27 March 2025 Volume 2025:20 Pages 821—830
DOI https://doi.org/10.2147/COPD.S505855
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Yang Li,1 Kang-Cheng Su,1,2 Yi-Han Hsiao,1,2 Kun-Ta Chou,1,2 Yen-Jung Li,1 Tien-Hsin Jeng,1,3 Hsin-Kuo Ko,1,2 Diahn-Warng Perng1,2
1Department of Chest Medicine, Taipei Veterans General Hospital, Taipei, 11217, Taiwan, Republic of China; 2School of Medicine, College of Medicine, National Yang Ming Chiao Tung University, Taipei, 11221, Taiwan, Republic of China; 3Division of Pulmonary Medicine, Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chia-Yi, 60002, Taiwan, Republic of China
Correspondence: Diahn-Warng Perng, Department of Chest Medicine, Taipei Veterans General Hospital, No. 201, Sec. 2, Shih-Pai Road, Taipei, 11217, Taiwan, Republic of China, Tel +886 2 28712121, ext., 27034, Fax +886 2 28752380, Email [email protected]
Purpose: Small airway dysfunction (SAD) is prevalent in asthma and chronic obstructive pulmonary disease (COPD). Aging is acknowledged to be associated with the loss of small airway structures. However, the impact of aging and pathophysiological changes on SAD in asthma and COPD remains unclear. We aimed to investigate the impact of aging and disease entity on pathophysiological change-related SAD in asthma and COPD assessed by spirometry and impulse oscillometry (IOS).
Patients and Methods: We retrospectively reviewed adult patients diagnosed with asthma or COPD between May 2017 and August 2021 in Taipei Veterans General Hospital. Treatment-naïve COPD patients aged ≥ 60 years were enrolled, along with age- and gender-matched elderly asthmatics (EA), and younger asthmatics aged < 60 years (YA) for comparison. All participants underwent spirometry and IOS with a bronchodilator test. Blood eosinophil counts (BECs) and immunoglobulin E(IgE) levels were documented if blood tests were conducted at the time of diagnosis.
Results: The mean age of YA, EA, and COPD were 44, 73, and 73 years, respectively. The FEV1, FEV1/FVC and FEF25-75% were higher in the YA followed by EA and COPD groups. The spirometric values were significantly correlated with IOS parameters in both asthmatic and COPD groups. No significant differences were observed in baseline IOS parameters among the three groups for participants with FEV1 ≥ 80% predicted. However, in patients with FEV1< 80% predicted, COPD patients exhibited significantly worse spirometric values and most IOS parameters (except R5-R20) compared to asthmatics. Additionally, asthmatics with AX reduction ≥ 35% exhibited significantly higher levels of blood eosinophil counts and IgE.
Conclusion: Aging process contributes to more impact on small airway reactance in asthma, while disease entity in COPD exhibits worse spirometric and IOS parameters compared to the age- and gender-matched EA.
Keywords: aging, elderly asthma, chronic obstructive pulmonary disease, COPD, impulse oscillometry, IOS, small airway dysfunction, SAD
Introduction
Small airways are critical sites of inflammation and obstruction in asthma and chronic obstructive pulmonary disease (COPD).1,2 In asthma, small airway dysfunction (SAD), assessed by the forced expiratory flow between 25% and 75% of vital capacity percent predicted (FEF25-75%), is linked to asthma symptoms and healthcare utilization.3 SAD is present across all asthma severities but is particularly prevalent in severe cases.4 In COPD, SAD, characterized by abnormal small airway resistance and reactance, correlates with disease severity5 and is associated with poor spirometric outcomes, severe lung hyperinflation, and reduced quality of life.6 Despite growing evidence on the impact of SAD in obstructive lung diseases,5,7–10 factors influencing its development and severity remain unclear.
Aging-related lung function decline, including loss of small airways, has been reported in healthy non-smokers.11 Aging is also linked to functional small airway abnormalities, as observed through computed tomography in never- and ever-smokers.12 Asthma, which often begins in childhood, is also prevalent in adults aged 65 years or older, with elderly asthma rates ranging from 1.3% to 15.3% in Asian populations.13 As life expectancy rises, it is crucial to explore whether there are differences in the prevalence and severity of SAD between younger and older adult asthmatics, and thereby to explore the impact of aging on the development of SAD in obstructive lung diseases. Conversely, COPD is commonly diagnosed after age 60. While asthma and COPD differ in origin, they share physiological features, such as airflow limitation, bronchoreversibility, and type 2 (T2) inflammation.14 The factor of disease entity may be related to various degrees of physiological impairment and SAD in obstructive lung diseases, and the impact of disease entity on SAD can be studied by analyzing the patient population of age-matched asthma and COPD.
Spirometry, the standard for lung function assessment, poses challenges in elderly people (more than 65 years old).15 Interpreting airway obstruction and SAD and differentiating asthma from COPD in elderly patients using spirometry alone is difficult. Impulse oscillometry (IOS), a patient-friendly method, can measure lung mechanics in an effort-independent manner, assessing respiratory resistance and reactance during tidal breathing.16,17 Patients with respiratory symptoms and preserved pulmonary function may still have SAD, which can be identified with the aid of IOS in addition to spirometry.18,19 IOS is more sensitive than spirometry-based FEF25-75% in detecting SAD in both asthma and COPD.20,21 Moreover, bronchodilator response (BDR) assessed via IOS, particularly changes in respiratory reactance, identifies more cases of poor asthma control compared to spirometry,22 highlighting the advantages of IOS to evaluate SAD in COPD and asthma.
This study aims to evaluate the impact of aging and disease entity on SAD in age-specific asthma and COPD patients, with additional analysis of BDR on IOS and its relationship to T2 inflammatory biomarkers.
Materials and Methods
Study Subjects
This retrospective cross-sectional study analyzed the medical records of individuals aged 20 years or older who were newly diagnosed and treatment-naïve for asthma and COPD. The study population underwent spirometry and IOS testing with bronchodilator administration during a single visit at Taipei Veterans General Hospital between May 2017 and August 2021. The diagnosis of COPD was based on a clinical history, including progressive exertional dyspnea, and pulmonary function characterized by not fully reversible airflow obstruction, which was defined as forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) <70% after bronchodilator (BD) administration, in accordance with the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines.23 Asthma diagnosis was based on GINA guideline and a clinical history of variable respiratory symptoms, including wheezing, shortness of breath, chest tightness, and cough.24 COPD patients with prior asthma diagnosis or recurrent wheezing before adolescence were excluded. All COPD patients had a smoking history of >10 pack-years, while asthmatic patients were non-smokers.
Study Design
This study included a total of 77 COPD patients and 323 asthmatic patients, and those aged ≥60 years were classified into the elderly groups. After age- and gender-matching, 73 COPD patients and 73 elderly asthmatic patients were selected and categorized as COPD and EA groups, respectively. The remaining asthmatic patients under 60 years old were categorized into the younger asthma (YA) group (n = 132). The first pulmonary function tests obtained when patients were treatment-naïve were analyzed. Additionally, baseline demographic variables were collected through chart review, including sex, age, body mass index, and laboratory data.
Measurement of Spirometry and IOS with Bronchodilator Test
Herein, patients were advised to avoid inhaled bronchodilators 12 hours before spirometry and reversibility testing. The two tests were conducted using combined spirometry and IOS equipment (MS-IOS Jaeger, Würzburg, Germany, and Vmax 22 Sensor Medics, Yorba Linda, Calif) following the protocols of the European Respiratory Society.25,26 Considering that forced expiration can affect resistance and reactance, IOS measurement was performed before each spirometry assessment. The pulmonary function test and IOS were repeated 15 minutes after inhalation of 400 mg of Salbutamol from a metered-dose inhaler with a valve-bearing spacer device. Then, from the forced expiratory volume-time curve, the values of FEF25-75%, FVC, and FEV1 were collected. The percentage of predicted indices was obtained. The Bronchodilator Reversibility (BDR) was positive if FEV1 both improved by 12% and 200 mL when compared with baseline values.27 The predicted values were based on our previous study.28
For IOS measurement, nasal clips and manual compression of the cheeks were used to reduce the confounding factors of cheek vibration and escape of air through the nostrils. Herein, patients breathed quietly, through a loudspeaker-activated mouthpiece for 30–45 seconds without contraction of the glottis or interposition of the tongue. The loudspeaker emitted 120–150 pulses varying from 5 to 35 hz in frequency and overlapping normal breathing sounds (0.2–2 hz). Thus, the resulting pressure and flow rates allow the calculation of respiratory impedance (Z). Airway impedance includes total resistance of the respiratory system (Rrs) and reactance (X), which is resistance to inertia and elasticity of the tissues of the respiratory tract. Although Rrs at different frequencies reflects total resistance (resistance at 5 hz [R5]) or central airway resistance (resistance at 20 hz [R20]), the difference between R5 and R20 (R5 – R20) reflects the resistance of small or peripheral airways.16 Resonant frequency (Fres) represents the frequency at which reactance is 0, thereby indicating that the elastic and inert properties are equal and opposite. The area under the reactance curve between 5 hz and the resonant frequency is AX, known as the “Goldman Triangle”, thus indicating an index related to respiratory compliance and small airways patency.29,30 We evaluated the following IOS parameters: R5–R20, reactance at 5 hz (X5), Fres, and AX. Changes with Salbutamol inhalation in FEV1 and IOS measurements (ΔFEV1, ΔR5- R20, ΔX5, ΔFres, and ΔAX) were defined as (post-BD value – pre-BD value)/pre-BD value. Notably, the majority of ΔIOS values exhibited a negative trend. To enhance comprehension of the relationship between the relative changes in IOS and other variables, we employed the percentage reduction of IOS from baseline, instead of ΔIOS, when investigating correlation associations. The SAD was defined as FEF 25–75% less than 65% predicted and AX > 0.44.18,31 We considered AX rather than R5- R20 for the several reasons. First, while R5- R20 reflects resistance in the small airways, AX captures the elastic properties of the entire peripheral airway network, offering a more comprehensive assessment.32 Second, AX is highly sensitive to changes in airway function, particularly small airway dysfunction, and correlates with asthma severity and patient-reported outcomes.33,34 Furthermore, AX was better association with diagnosis of adult asthma compared to R5- R20, and AX combined with FEV1 enhances diagnostic accuracy for adult asthma.32 Third, a study also shows that AX responds more markedly to bronchodilator treatment compared to R5- R20 in patients with COPD.35 As for FEF25–75%, while no universal guideline exists, arbitrary cutoffs typically range between 60–75% predicted,7 with studies indicating the 95th percentile for normal is closer to 56%.36 We use an FEF25–75% <65% predicted to define SAD because it aligns with evidence suggesting this cutoff is sensitive for detecting peripheral airway impairment. A study demonstrated its abnormality and clinical relevance in a real-world study.31 Additionally, our previous work confirmed its correlation with IOS parameters, reinforcing its validity.18 Thus, <65% provides a practical, evidence-based threshold.
Statistical Analysis
The distribution of variables was evaluated by Kolmogorov–Smirnov goodness-of-fit test. The variables are presented as either mean ± standard deviation or median (interquartile range (IQR)) based on their distribution. One-way analysis of variance (ANOVA) with the Scheffe post hoc test and the Kruskal–Wallis test were used for continuous variables, while χ2 tests was employed for categorical variables. Meanwhile, coefficients of correlation and regression analysis were used to identify the correlations between percentage changes after bronchodilator administration in spirometry measurements and IOS parameters. The logistic regression was used to investigate the relationship between age, disease entity and SAD. Statistical significance was defined as a p value <0.05. All scientistic analyses were conducted using SPSS (IBM Corp. Released 2017.IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.) and MedCalc Statistical Software version 23.1.1 (MedCalc Software bv, Ostend, Belgium).
Results
Demographic and Clinical Characteristics Related with Small Airway Dysfunction in the Study Subjects
The demographic and baseline characteristics of the study subjects are shown in Table 1. Male was predominant in the COPD and EA groups as well as female was predominant in the YA group. The mean age of YA, EA, and COPD were 44, 73, and 73 years, respectively. There was no significant difference observed in BMI, blood eosinophil counts, and total IgE levels among these three groups. The prevalence of patients with bronchodilator reversibility is 31.1%, 37.0%, and 13.7% in the YA, EA, and COPD groups, respectively (p=0.004). In comparison to YA, EA group had significantly lower values of FEV1, FEV1/FVC, FEF25-75% and worse IOS parameters of X5, Fres, and AX except R5- R20. The prevalence of SAD defined as FEF 25–75% ≤ 65% predicted and AX ≥0.44 was higher in EA as compared to YA group (65.8% versus, 45.5%; 82.2% versus 62.9%).
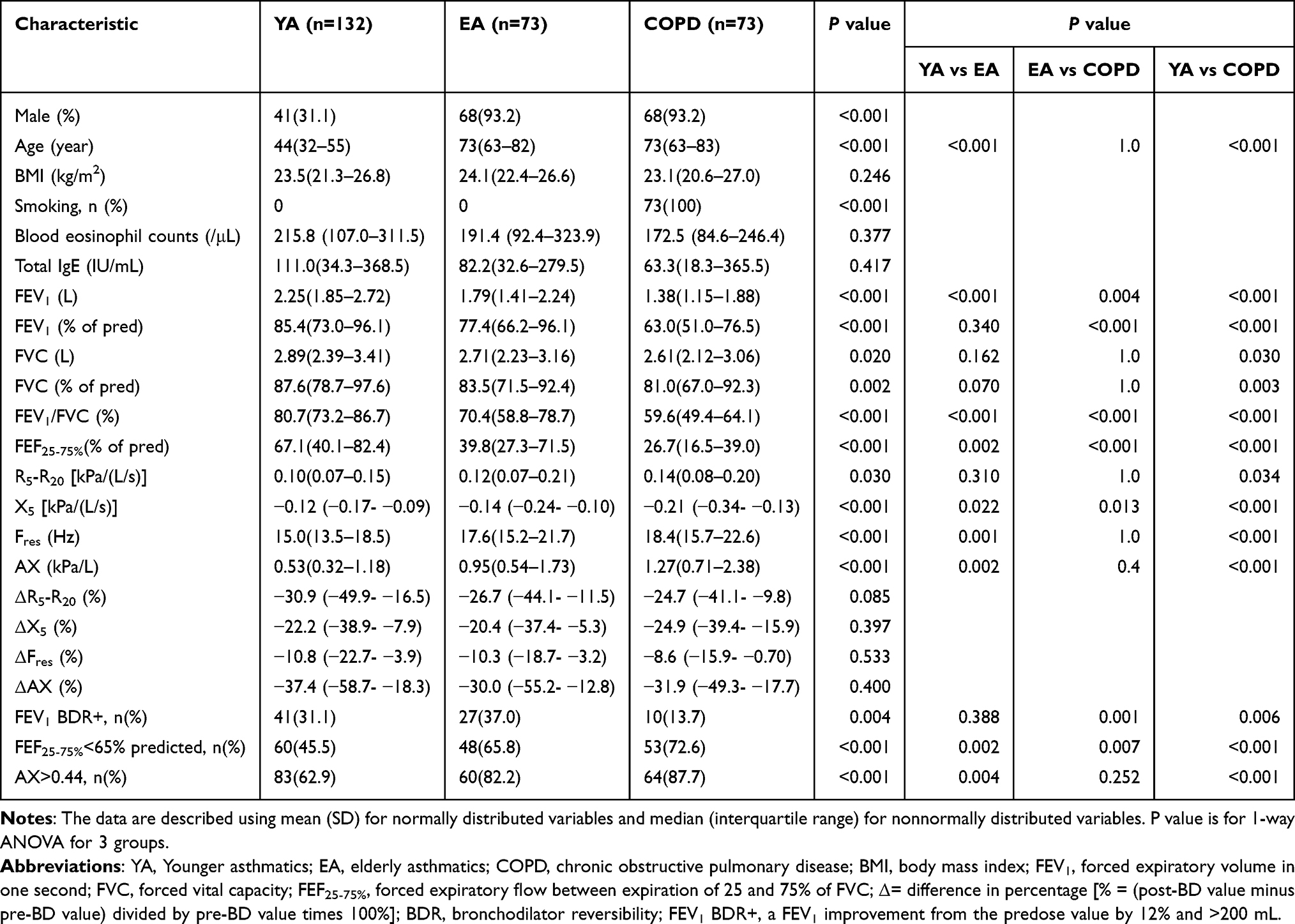 |
Table 1 Demographic and Clinical Characteristics Related with Small Airway Dysfunction in the Study Subjects |
In the COPD group, as compared to asthmatics, we found: (1) the values of FEV1, FEV1%, and FEV1/FVC were significantly lower, (2) the airway reactance X5 and FEF25-75% indicating small airway function were significantly worse, (3) the prevalence of small airway dysfunction defined as FEF 25–75% ≤65% was higher. Notably, the COPD group as compared to age-matched EA group presented with significantly lower values of FEV1, FEV1%, FEV1/FVC, FEF25-75% and worse X5. This result may indicate that disease entity plays a role determining the lung function impairment and SAD in obstructive lung disease. Smoking is the only different baseline characteristic between COPD and age-matched EA (p < 0.001), aside from differences in lung function parameters. This highlighted that smoking-related pathogenesis in COPD may have a greater impact on SAD compared to age-matched EA. Although, the prevalence of bronchial reversibility defined as the change of FEV1 between pre and post-bronchodilator administration was higher in the EA as compared to COPD patients (37.0% vs 13.7%, p = 0.001). The small airway reversibility calculated by ΔR5- R20, ΔX5, ΔFres, or ΔAX was not statistically different among three groups.
Correlation Between Spirometric and IOS Parameters at the Baseline and After Bronchodilator Testing
The spirometric parameters of FEV1, FVC, FEV1/FVC, and FEF25-75% were significantly correlated with IOS parameters of R5- R20, X5, Fres, and AX at baseline in the asthmatics and COPD groups, respectively (Table 2). Particularly, FEF25-75% indicating small airway function by spirometry was significantly correlated with IOS parameters of R5- R20, X5, Fres and AX for both asthma and COPD. After the bronchodilator test, the reduction of R5- R20 and AX were significantly associated with the increase of FEV1 in both COPD and asthma (Table 3).
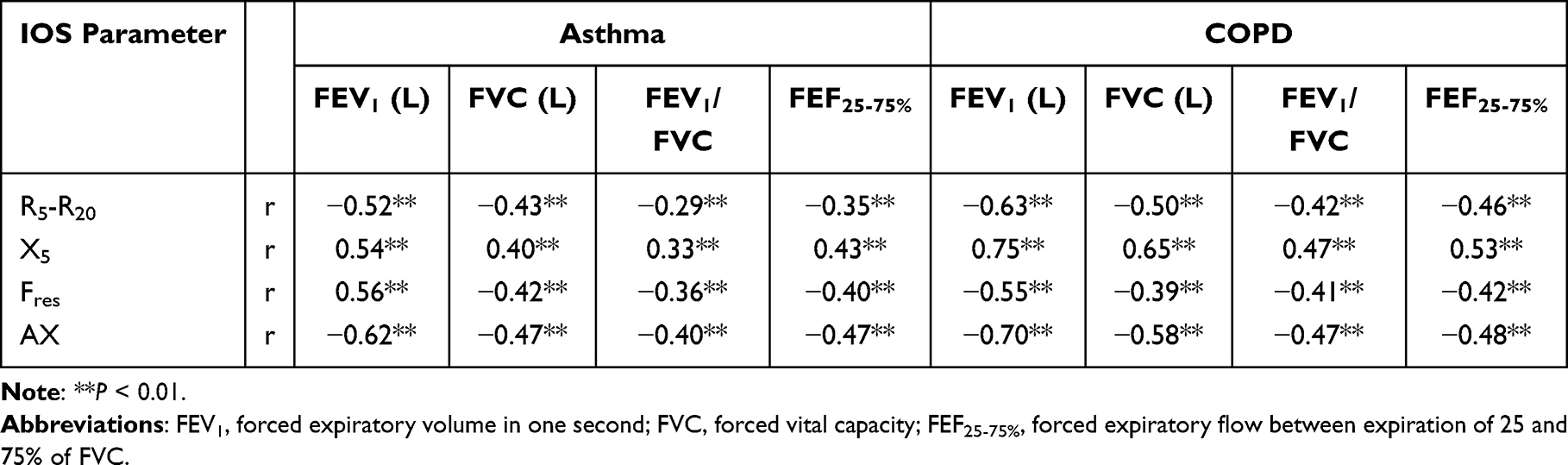 |
Table 2 Correlation Between Spirometry and IOS Parameters at the Baseline |
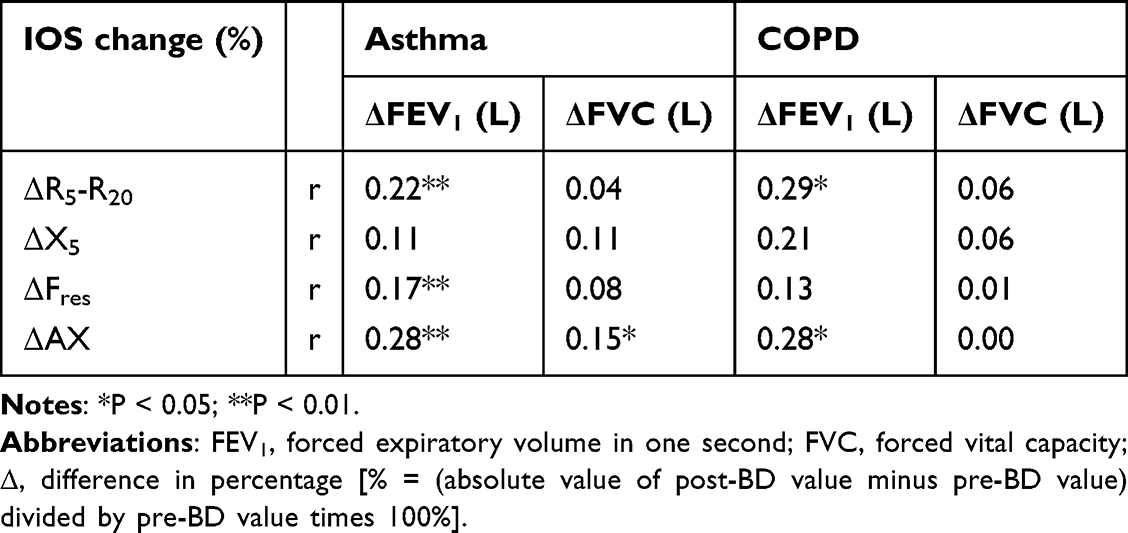 |
Table 3 Correlation Between Spirometry and IOS Parameters After Bronchodilator Test |
Burden and Severity of SAD in the Study Subjects Stratified by Forced Expiratory Volume in One second
The study subjects were divided into two categories based on their FEV1 (≥ or <80% predicted) to further compare SAD and airflow obstruction across the three groups (Table 4). There were no significant differences of IOS parameters at baseline or in their relative changes following bronchodilator inhalation among the three groups with FEV1 ≥80% predicted. The airflow obstruction (FEV1/FVC) was more severe in COPD patients compared to the asthmatics regardless of the categories of FEV1% with statistical significance. In the study subjects with lung function impairment of FEV1 < 80% predicted, the spirometric values and IOS parameters (X5, Fres, and AX except R5- R20) were significantly worse in COPD patients compared to the asthmatics. In addition, there was a significant difference in reactance parameters between the COPD and YA groups, but no significant difference was observed between the EA and YA groups, or between the EA and COPD groups.
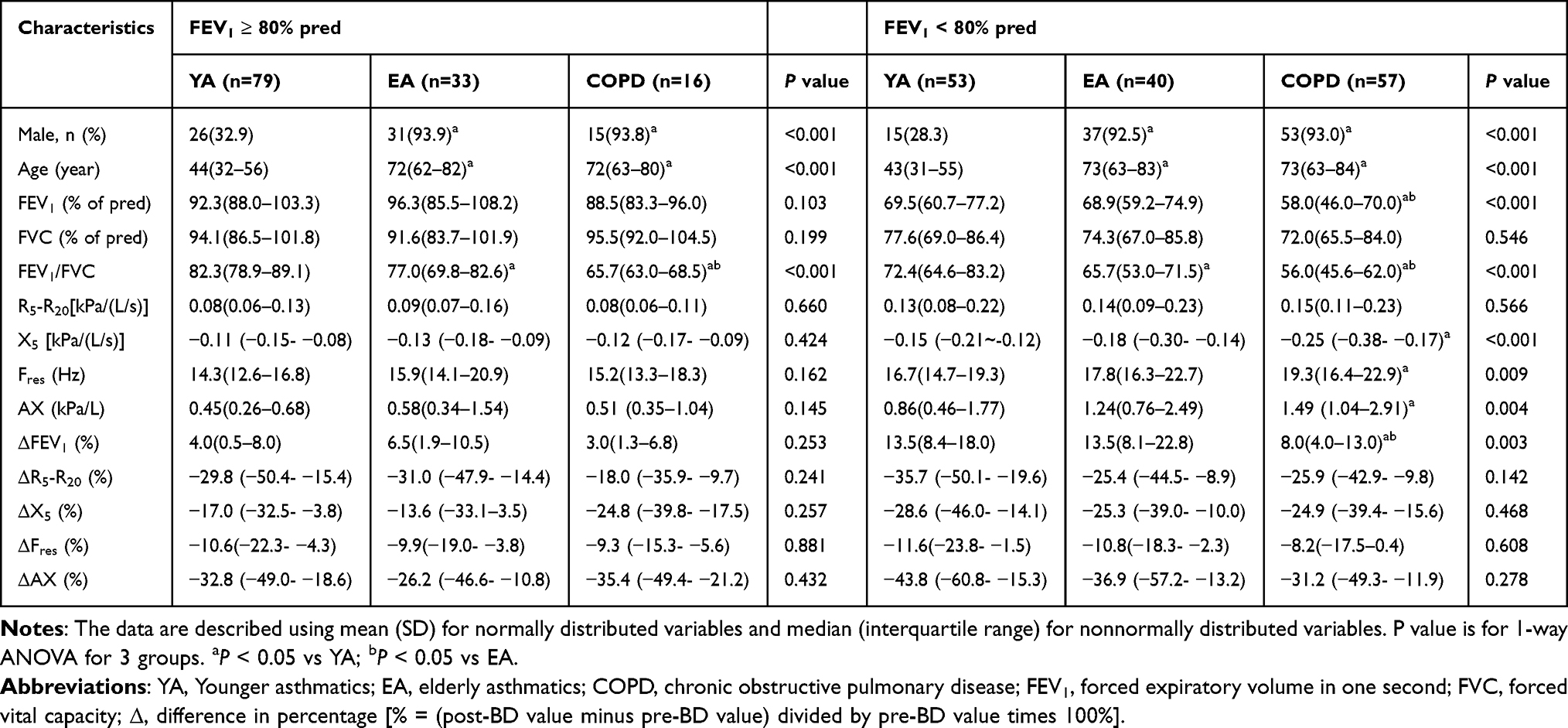 |
Table 4 Burden and Severity of SAD in the Study Subjects Stratified by Forced Expiratory Volume in One second |
The Relationship Between Type 2 Biomarkers and Small Airway Reversibility
The blood eosinophil counts (BECs) and total IgE levels were significantly correlated with the reduction of R5- R20, Fres, and AX after bronchodilator test in all asthmatics. The correlation did not exist in COPD groups (Table 5). Furthermore, asthmatic patients with a ≥ 35% reduction in AX exhibited significantly higher BECs and total IgE level compared to those with a relative change of AX less than 35% (Table 6).
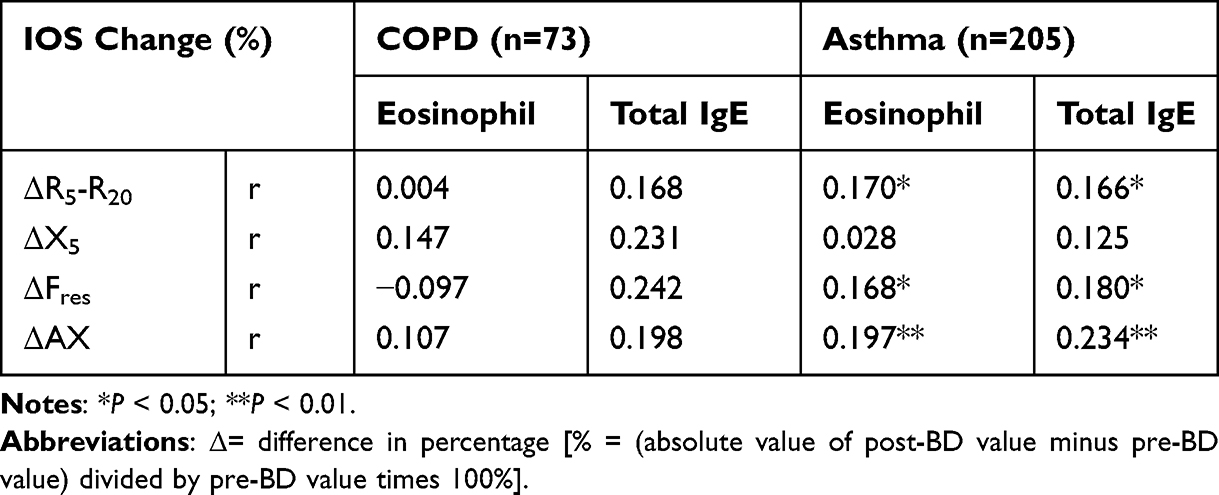 |
Table 5 Correlation Between Type 2 Inflammatory Markers and IOS Reversibility in COPD and Asthma |
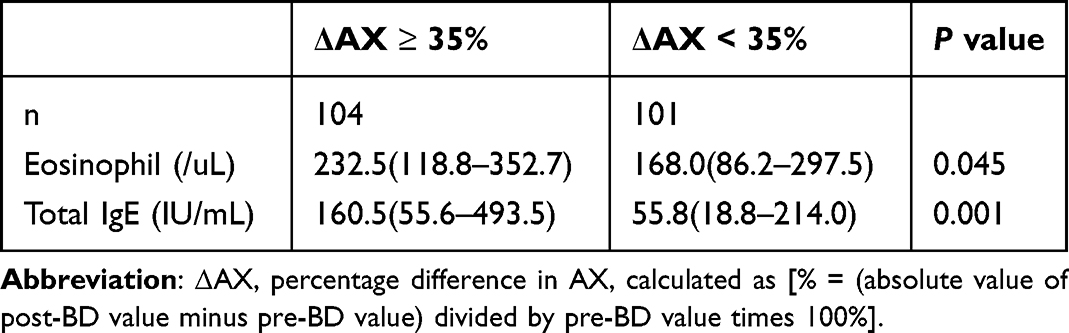 |
Table 6 Relationship Between Type 2 Inflammatory Markers and Ax Reversibility with Cut-off Value of 35% in Asthma Patients |
The Factors Associated with SAD in Patients with Obstructive Airway Diseases
The supplementary tables demonstrated the factors that were associated with SAD as defined by AX (Table S1) or FEF25-75% (Table S2). The results indicated that age and disease entity (YA, EA, or COPD) were independent risk factors associated with SAD in both univariate and multivariate logistic regression analyses.
Discussion
We have demonstrated the functional parameters of small airways assessed by IOS and their association with age and spirometric values in younger and elderly asthmatics versus COPD patients in this study. In comparison to YA, EA group had significantly lower FEV1, FEV1/FVC, FEF25-75% and worse IOS parameters except R5- R20. The age- and gender-matched EA exhibited higher values of FEV1, FEV1/FVC, FEF25-75% and X5 in comparison to the COPD patients. The values of FEV1 and FEV1/FVC were significantly lower in the COPD group compared to the asthmatics. In addition, the airway reactance X5 and FEF25-75% indicating small airway function were significantly worse in COPD compared to the asthmatics. Age and disease entity (YA, EA, or COPD) were independent risk factors associated with SAD. The results may indicate that aging and disease entity simultaneously contribute to the development of SAD in obstructive lung disease. We also demonstrated that COPD significantly possessed a higher burden and severity of SAD than EA and YA while the occurrence of lung function impairment with FEV1 <80% predicted. Our study elucidated the impact of age and disease entity on SAD in obstructive lung disease and provided the critical information on the disease management.
The age is one of the critical factors to determine the normal values of lung function in healthy subjects.28 Meanwhile, aging has been reported to be associated with computed tomography-defined functional small airway abnormality in never- and ever smokers without airflow obstruction.12 The development, prevalence and severity of SAD increased over aging had been confirmed by computed tomography, IOS and spirometry.37 In this study, we selected a cohort of age- and gender-matched elderly asthmatics in comparison to COPD patients to eliminate this confounding factor. EA had higher FEV1, FEV1/FVC, FEF25-75%, and less negative X5, suggesting the difference in pathophysiological change with the variable severity of peripheral airway and lung parenchymal damage between asthma and COPD. By contrast, we enrolled the treatment-naïve asthmatics and reported the EA presented with more serious severity of lung function impairment and SAD assessed by spirometry and IOS than YA. These results suggest that the aging process significantly influences lung function.
FEV1/FVC <0.7 or < lower limit of normal, usually defined as fixed airway obstruction (FAO), is mainly attributed to the airway and parenchymal remodeling.38 FAO appears to be more severe in COPD compared with YA and EA groups or even in asthma patients with FEV1 ≥ 80% predicted observed in this study. Airway remodeling including thickening of the basement membrane, smooth muscle, and mucus gland has been demonstrated in fatal and non-fatal asthma.39 The parenchyma remodeling includes loss of alveolar attachment, parenchymal destruction, and reduction in elastic fibers which are pathological characteristics of COPD.40 Structural parenchymal abnormalities were also observed in post-mortem lungs of non-smoker patients with chronic severe asthma.41 Aging is an additional contributing factor to FAO, including the changes of the airway wall, remodeling, stiffness, and loss of terminal bronchioles and elastic recoil.11 Airway resistance and reactance measured by IOS as well as FEV1 were significantly correlated with intraluminal area, particularly in distal bronchi confirmed by three-dimensional computed tomography in patients with COPD.42 The inverse relationship between reactance X5 and expiratory residual volume was found in COPD, indicating the role of reactance on airway narrowing associated with communicated lung volume.43 We have found that the small airway reactance and resistance determined by IOS show a significant correlation with the spirometric values of FEV1, FVC, FEV1/FVC and FEF25-75% in both asthma and COPD. These physiological parameters may be surrogate markers to evaluate the severity of small airway remodeling in asthma and COPD. Notably, the results of our study indicated that the severity of small airway remodeling assessed by spirometry and IOS was higher in COPD than EA and YA. The phenomenon of small airway remodeling may be associated with the impaction of age and disease entity in obstructive lung diseases.
Blood eosinophil counts and IgE level serve as crucial biomarkers of type 2 inflammation in individuals diagnosed with asthma. The presence of positive bronchodilator reversibility indicates a higher blood eosinophil count and IgE level and is a physiologic indicator of lower lung function in asthma.44,45 On the other hand, type 2 airway inflammation is acknowledged as a specific phenotype in COPD and is associated with a favorable response to inhaled corticosteroid.46–48 In a longitudinal cohort for COPD, a significant inverse correlation was observed between total serum IgE and FEV1/FVC, independent of smoking and asthma status.49 However, when evaluating airway reversibility by using IOS, a weak but significant correlation was observed between ΔAX and blood eosinophils or total IgE levels in individuals asthma, whereas no such correlation was evident in the COPD group, as depicted in Table 5. This observation aligns with our previous study and provides further support for the potential utility of IOS in accessing small airway reversibility in adult asthma.44 Individuals with a ΔAX value of ≥35% exhibited significantly elevated blood eosinophil counts and total IgE levels as compared to those with a ΔAX value of <35%. This finding provides additional evidence supporting the involvement of eosinophilic airway inflammation in obstructive airway diseases and contributing to small airway reversibility.
There are several limitations that should be addressed in this study. First, disease severity cannot be classified in asthma and COPD groups for comparison because of limited patient numbers. The effect of disease severity on SAD in asthma and COPD could not be determined in this study. However, there are significant correlations between spirometric and IOS parameters in both asthma and COPD patients. Second, in the age- and gender-matched EA group versus COPD, the effect of smoking on SAD in asthma and COPD cannot be determined. Third, this study had a lack of type 2 biomarkers from the airways such as sputum eosinophils or exhaled nitric oxide, which could be more reliable to reflect airway inflammation in COPD. Finally, a prospective study with a large cohort of healthy subject, asthmatics, and COPD is needed to examine the difference in small airway function and exclude confounding factors such as age, sex, and smoking.
Conclusion
The airflow obstruction and SAD assessed by spirometry and IOS are more severe in the COPD group compared with asthmatics. The age- and disease entity-related pathophysiological change may be involved in the airway remodeling and contribute to the severity of SAD in obstructive lung disease.
Abbreviations
COPD, Chronic obstructive pulmonary disease; EA, Elderly asthmatics; YA, Younger asthmatics; SAD, Small airway dysfunction; IOS, Impulse oscillometry; FVC, Forced vital capacity; FEV1, Forced expiratory volume in one second; FEV1%, FEV1% of predicted value; FEF25-75%, Forced expiratory flow between 25% and 75% of FVC; BDR, Bronchodilator reversibility; R5, Resistance at 5 hz; R20, Resistance at 20 hz; R5- R20, Difference between R5 and R20; X5, Reactance at 5 hz; Fres, Resonant frequency; AX, Area under reactance curve between 5 hz and resonant frequency; BEC, Blood eosinophil counts; FAO, Fixed airway obstruction.
Data Sharing Statement
The data that supports the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Ethical Review Board (IRB) of Taipei Veterans General Hospital (IRB-TPEVGH No.: 2022-07-001CC). Informed consent was obtained from all participants, and the study adhered to the guidelines of the Declaration of Helsinki.
Acknowledgment
This paper has been uploaded to SSRN as a preprint: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4624918. We are grateful to all participants in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The article publishing charge is funded by the National Science and Technology Council, R.O.C. NSTC 113-2314-B-075-065-MY3 to D.W.P.
Disclosure
The authors declare that they have no conflict of interest related to this subject matter or materials discussed in this article.
References
1. Hogg JC, Chu F, Utokaparch S, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(26):2645–2653. doi:10.1056/NEJMoa032158
2. Mauad T, Bel EH, Sterk PJ. Asthma therapy and airway remodeling. J Allergy Clin Immunol. 2007;120(5):997–1009. doi:10.1016/j.jaci.2007.06.031
3. Riley CM, Wenzel SE, Castro M, et al. Clinical implications of having reduced mid forced expiratory flow rates (FEF25-75, independently of FEV1, in adult patients with asthma. PloS One. 2015;10(12):e0145476.
4. Postma DS, Brightling C, Baldi S, et al. Exploring the relevance and extent of small airways dysfunction in asthma (ATLANTIS): baseline data from a prospective cohort study. Lancet Respir Med. 2019;7(5):402–416. doi:10.1016/S2213-2600(19)30049-9
5. Crisafulli E, Pisi R, Aiello M, et al. Prevalence of small-airway dysfunction among COPD patients with different GOLD stages and its role in the impact of disease. Respiration. 2017;93(1):32–41. doi:10.1159/000452479
6. Usmani OS, Dhand R, Lavorini F, et al. Why we should target small airways disease in our management of chronic obstructive pulmonary disease. Mayo Clin Proc. 2021;96(9):2448–2463. doi:10.1016/j.mayocp.2021.03.016
7. Liwsrisakun C, Chaiwong W, Pothirat C. Comparative assessment of small airway dysfunction by impulse oscillometry and spirometry in chronic obstructive pulmonary disease and asthma with and without fixed airflow obstruction. Front Med Lausanne. 2023;10:1181188. doi:10.3389/fmed.2023.1181188
8. Pornsuriyasak P, Khiawwan S, Rattanasiri S, Unwanatham N, Petnak T. Prevalence of small airways dysfunction in asthma with- and without-fixed airflow obstruction and chronic obstructive pulmonary disease. Asian Pac J Allergy Immunol. 2021;39(4):296–303. doi:10.12932/AP-310119-0485
9. Jarenbäck L, Ankerst J, Bjermer L, Tufvesson E. Flow-volume parameters in COPD related to extended measurements of lung volume, diffusion, and resistance. Pulm Med. 2013;2013:782052. doi:10.1155/2013/782052
10. Chetta A, Facciolongo N, Franco C, Franzini L, Piraino A, Rossi C. Impulse oscillometry, small airways disease, and extra-fine formulations in asthma and chronic obstructive pulmonary disease: windows for new opportunities. Ther Clin Risk Manag. 2022;18:965–979. doi:10.2147/TCRM.S369876
11. Verleden SE, Kirby M, Everaerts S, et al. Small airway loss in the physiologically ageing lung: a cross-sectional study in unused donor lungs. Lancet Respir Med. 2021;9(2):167–174. doi:10.1016/S2213-2600(20)30324-6
12. Martinez CH, Diaz AA, Meldrum C, et al. Age and small airway imaging abnormalities in subjects with and without airflow obstruction in SPIROMICS. Am J Respir Crit Care Med. 2017;195(4):464–472. doi:10.1164/rccm.201604-0871OC
13. Song WJ, Kang MG, Chang YS, et al. Epidemiology of adult asthma in Asia: toward a better understanding. Asia Pac Allergy. 2014;4(2):75–85.
14. Postma DS, Rabe KF. The asthma-COPD overlap syndrome. N Engl J Med. 2015;373(13):1241–1249. doi:10.1056/NEJMra1411863
15. Czajkowska-Malinowska M, Tomalak W, Radliński J. Quality of spirometry in the elderly. Pneumonol Alergol Pol. 2013;81(6):511–517.
16. King GG, Bates J, Berger KI, et al. Technical standards for respiratory oscillometry. Eur Respir J. 2020;55(2):1900753. doi:10.1183/13993003.00753-2019
17. Bickel S, Popler J, Lesnick B, et al. Impulse oscillometry: interpretation and practical applications. Chest. 2014;146(3):841–847. doi:10.1378/chest.13-1875
18. Chiu HY, Hsiao YH, Su KC, et al. Small airway dysfunction by impulse oscillometry in symptomatic patients with preserved pulmonary function. J Allergy Clin Immunol Pract. 2020;8(1):229–235.e3. doi:10.1016/j.jaip.2019.06.035
19. Li LY, Yan TS, Yang J, et al. Impulse oscillometry for detection of small airway dysfunction in subjects with chronic respiratory symptoms and preserved pulmonary function. Respir Res. 2021;22(1):68. doi:10.1186/s12931-021-01662-7
20. Cottini M, Licini A, Lombardi C, et al. Prevalence and features of IOS-defined small airway disease across asthma severities. Respir Med. 2021;176:106243. doi:10.1016/j.rmed.2020.106243
21. Su ZQ, Guan WJ, Li SY, et al. Significances of spirometry and impulse oscillometry for detecting small airway disorders assessed with endobronchial optical coherence tomography in COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:3031–3044. doi:10.2147/COPD.S172639
22. Cottee AM, Seccombe LM, Thamrin C, et al. Bronchodilator response assessed by the forced oscillation technique identifies poor asthma control with greater sensitivity than spirometry. Chest. 2020;157(6):1435–1441. doi:10.1016/j.chest.2019.12.035
23. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease 2024.
24. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. Available from: https://www.ginasthma.org.
25. Oostveen E, MacLeod D, Lorino H, et al. The forced oscillation technique in clinical practice: methodology, recommendations and future developments. Eur Respir J. 2003;22(6):1026–1041. doi:10.1183/09031936.03.00089403
26. Beydon N, Davis SD, Lombardi E, et al. An official American thoracic society/European respiratory society statement: pulmonary function testing in preschool children. Am J Respir Crit Care Med. 2007;175(12):1304–1345. doi:10.1164/rccm.200605-642ST
27. Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005;26(5):948–968. doi:10.1183/09031936.05.00035205
28. Wang WT, Ko HK, Lin CC, et al. Spirometric reference values in healthy Chinese adults in Taiwan: the secular changes and comparison with other Asian populations. J Formos Med Assoc. 2020;119(1 Pt 2):290–299. doi:10.1016/j.jfma.2019.05.015
29. Meraz EG, Nazeran H, Ramos CD, et al. Analysis of impulse oscillometric measures of lung function and respiratory system model parameters in small airway-impaired and healthy children over a 2-year period. Biomed Eng Online. 2011;10(1):21. doi:10.1186/1475-925X-10-21
30. Brashier B, Salvi S. Measuring lung function using sound waves: role of the forced oscillation technique and impulse oscillometry system. Breathe. 2015;11(1):57–65. doi:10.1183/20734735.020514
31. Ciprandi G, Capasso M, Tosca M, et al. A forced expiratory flow at 25-75% value <65% of predicted should be considered abnormal: a real-world, cross-sectional study. Allergy Asthma Proc. 2012;33(1):e5–8. doi:10.2500/aap.2012.33.3524
32. Kim SR, Park KH, Son NH, et al. Application of impulse oscillometry in adult asthmatic patients with preserved lung function. Allergy Asthma Immunol Res. 2020;12(5):832–843. doi:10.4168/aair.2020.12.5.832
33. Kuo CR, Lipworth B. Airwave oscillometry and patient-reported outcomes in persistent asthma. Ann Allergy Asthma Immunol. 2020;124(3):289–290. doi:10.1016/j.anai.2019.12.017
34. Chan R, Lipworth B. Real-life effects of dupilumab on airway oscillometry in severe uncontrolled asthma. Ann Allergy Asthma Immunol. 2023;131(5):664–666. doi:10.1016/j.anai.2023.07.021
35. Lipworth BJ, Jabbal S. What can we learn about COPD from impulse oscillometry? Respir Med. 2018;139:106–109. doi:10.1016/j.rmed.2018.05.004
36. Knox-Brown B, Mulhern O, Feary J, Amaral AFS. Spirometry parameters used to define small airways obstruction in population-based studies: systematic review. Respir Res. 2022;23:67. doi:10.1186/s12931-022-01990-2
37. Dai C, Wu F, Wang Z, et al. The association between small airway dysfunction and aging: a cross-sectional analysis from the ECOPD cohort. Respir Res. 2022;23(1):229. doi:10.1186/s12931-022-02148-w
38. Rutting S, Thamrin C, Cross TJ, et al. Fixed airflow obstruction in asthma: a problem of the whole lung not of just the airways. Front Physiol. 2022;13:898208. doi:10.3389/fphys.2022.898208
39. Carroll N, Elliot J, Morton A, et al. The structure of large and small airways in nonfatal and fatal asthma. Am Rev Respir Dis. 1993;147(2):405–410. doi:10.1164/ajrccm/147.2.405
40. Jeffery PK. Structural and inflammatory changes in COPD: a comparison with asthma. Thorax. 1998;53(2):129–136. doi:10.1136/thx.53.2.129
41. Mauad T, Silva LF, Santos MA, et al. Abnormal alveolar attachments with decreased elastic fiber content in distal lung in fatal asthma. Am J Respir Crit Care Med. 2004;170(8):857–862. doi:10.1164/rccm.200403-305OC
42. Karayama M, Inui N, Mori K, et al. Respiratory impedance is correlated with morphological changes in the lungs on three-dimensional CT in patients with COPD. Sci Rep. 2017;7:41709. doi:10.1038/srep41709
43. Milne S, Jetmalani K, Chapman DG, et al. Respiratory system reactance reflects communicating lung volume in chronic obstructive pulmonary disease. J Appl Physiol. 2019;126(5):1223–1231. doi:10.1152/japplphysiol.00503.2018
44. Hsiao YH, Lin YJ, Jeng TH, et al. Potentiality of impulse oscillometry to evaluate bronchodilator reversibility in untreated adult patients with newly diagnosed asthma. J Chin Med Assoc. 2022;85(8):859–865. doi:10.1097/JCMA.0000000000000757
45. Wei J, Ma L, Wang J, et al. Airway reversibility in asthma and phenotypes of Th2-biomarkers, lung function and disease control. Allergy Asthma Clin Immunol. 2018;14:89. doi:10.1186/s13223-018-0315-0
46. Su KC, Ko HK, Hsiao YH, et al. Fractional exhaled nitric oxide guided-therapy in chronic obstructive pulmonary disease: a stratified, randomized, controlled trial. Arch Bronconeumol. 2022;58(8):601–610. doi:10.1016/j.arbres.2021.11.013
47. Perng DW, Tao CW, Su KC, et al. Anti-inflammatory effects of salmeterol/fluticasone, tiotropium/fluticasone or tiotropium in COPD. Eur Respir J. 2009;33(4):778–784. doi:10.1183/09031936.00115308
48. Kitaguchi Y, Komatsu Y, Fujimoto K, et al. Sputum eosinophilia can predict responsiveness to inhaled corticosteroid treatment in patients with overlap syndrome of COPD and asthma. Int J Chron Obstruct Pulmon Dis. 2012;7:283–289. doi:10.2147/COPD.S30651
49. Sherrill DL, Lebowitz MD, Halonen M, et al. Longitudinal evaluation of the association between pulmonary function and total serum IgE. Am J Respir Crit Care Med. 1995;152(1):98–102. doi:10.1164/ajrccm.152.1.7599870
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.