")
Back to Journals » Journal of Pain Research » Volume 16
The High Burden of Acute and Chronic Pain in General Practice in French-Speaking Belgium
Authors Steyaert A , Bischoff R, Feron JM, Berquin A
Received 24 November 2022
Accepted for publication 23 April 2023
Published 1 May 2023 Volume 2023:16 Pages 1441—1451
DOI https://doi.org/10.2147/JPR.S399037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Robert Twillman
Arnaud Steyaert,1,2 Romain Bischoff,3 Jean-Marc Feron,4 Anne Berquin2,5
1Department of Anesthesiology, Cliniques universitaires Saint-Luc, Brussels, Belgium; 2Institute of Neuroscience, Université Catholique de Louvain, Brussels, Belgium; 3General Practice Medecine Internship, Université Catholique de Louvain, Brussels, Belgium; 4Centre Académique de médecine générale, Université Catholique de Louvain, Brussels, Belgium; 5Department of Physical and Rehabilitation Medicine, Cliniques universitaires Saint-Luc, Brussels, Belgium
Correspondence: Anne Berquin, Department of Physical and Rehabilitation Medicine, Cliniques universitaires Saint-Luc, Avenue Hippocrate 10, Brussels, 1200, Belgium, Email [email protected]
Background: Chronic pain prevalence is very high in the general population, much higher than can be managed by chronic pain centers. Therefore, most pain patients are cared for by first-line professionals. However, general practitioners often feel ill at ease with these patients, and only a few studies assess the burden of chronic pain in general practice. To better estimate the resources needed to support these professionals, a good knowledge of (sub)acute and chronic pain prevalence and prognosis in general practices is needed.
Methods: We report cross-sectional data from a larger longitudinal study performed in French-speaking general practices in Belgium in November 2018. Fifth-year medical students performing a one-month internship collected data for every third patient they saw each day: demographic information, pain characteristics, lifestyle, general health perception and the short Örebro Musculoskeletal Pain Screening Questionnaire in the French language.
Results: 3882 patients (participation rate 66%) accepted to take part in the study. 22 and 50% of these suffered from (sub)acute and chronic pain, respectively. Pain was more often the motive of the consultation for (sub)acute than for chronic pain patients. Pain intensity and functional impact were moderate, irrespective of pain duration. 70% of (sub)acute and 31% of chronic pain patients were at low risk of chronicity.
Conclusion: In our sample, chronic pain patients constituted 33– 50% of patient contacts in general practice, indicating the high importance of providing adequate support to general practitioners and other first-line professionals, ie, by reinforcing collaboration with chronic pain centers.
Keywords: Acute pain, chronic pain, general practice
Plain Language Summary
This report describes a sub-study aimed at increasing our knowledge of the epidemiology of acute and chronic pain in general practice in French-speaking Belgium. Its results confirm that chronic pain patients account for a very high percentage (between 33 and 50%) of GP patient contacts and that most of these patients have been suffering for more than one year. Furthermore, pain was the primary motive of the consultation for a majority of both acute and chronic pain patients. Overall, their pain had a moderate impact on their daily functioning. Encouragingly, a significant proportion of patients were at low risk of persistent disabling pain in the future. Finally, lifestyle (as evaluated by weight, smoking status, sleep quality and exercise level) and social determinants (professional status, work heaviness) correlated with pain duration. The high prevalence of patients with acute or chronic pain in general practice suggests that a radical shift is needed in the missions of chronic pain centers: rather than devoting themselves mainly to treating pain patients, they should put more efforts into supporting first-line professionals, ie, by taking part in local networks.
Introduction
Chronic pain prevalence in the general population is as high as 20% in Europe, with significant geographical variations.1 Extrapolating Belgian data from the Pain in Europe survey to the Belgian population, it was estimated in 2011 that approximately 940 000 adults (11% of adults) suffered from mild to severe chronic pain.1,2 If all these patients were to be managed in specialized facilities, each of the 35 Belgian chronic pain centers should be able to provide care for nearly 27,000 patients. However, the yearly activity reports of these centers show an annual median number of new patients of 235 (2015 data, source: Health Federal Public Service). Thus, most chronic pain patients seek help in primary care, which stresses the pivotal role of general practitioners (GPs) and other first-line caregivers such as physiotherapists in the management of chronic pain patients.1,3 Although there is little literature about the prevalence, impact, and severity of chronic pain in general practice (GP) patients, the available studies show that up to 40% of GP contacts concern chronic pain patients.4–7 Indeed, the effective burden of chronic pain in GP might not be proportional to population prevalence data, as these patients may consult more often than others.8 Moreover, GPs often feel ill at ease managing chronic pain patients.9,10 Several small studies have reported positive outcomes after the implementation in primary care practices of multimodal pain rehabilitation, provided by multidisciplinary teams that collaborate to assess and manage chronic pain patients according to the bio-psycho-social model.11–15 These reports suggest that multidisciplinary care is possible at the GP level, but emphasize the need for training and education of primary care healthcare professionals.
Another issue relating to chronic pain is secondary prevention, ie, developing strategies to help avoid or reduce the transition from acute to chronic pain. Stratified approaches specifically targeting patients at high risk of developing persistent pain —as assessed by screening tools such as the STarT Back Screening Tool or the Örebro Musculoskeletal Pain Screening Questionnaire (ÖMPSQ)— have been shown to improve outcomes.16 Two recent trials evaluating stratified care (for sciatica17 and musculoskeletal pain)18 in primary care delivered disappointing results but have reported difficulties in implementing the stratified care approaches, eg, ensuring that patients received the treatment matching their risk level and that the treatments themselves were correctly executed.19 This emphasizes that these approaches require specific skills, notably to manage psychosocial issues.20
To estimate the resources necessary to improve the care of pain patients in GP in Belgium (eg, through the implementation in primary practice of stratified care for subacute pain and multidisciplinary rehabilitation programs for chronic pain patients), more information is needed on this population. Therefore, the aims of this study were (1) to estimate the proportion of (sub)acute and chronic pain patients in routine consultations of GPs in French-speaking Belgium (Brussels and Wallonia) and (2) to assess the long-term prognosis of patients with (sub)acute or chronic pain in this population.
Methods
Procedures
We report cross-sectional data from a larger longitudinal study performed in the general practice setting. Fifth-year medical students performing their one-month general practice internship (November 2018) and their supervisors were invited to collaborate. Detailed written instructions were provided, and the investigators were available for any questions. The study was approved by an independent ethic committee (2018/19JUI/258, Commission d’Éthique Biomédicale Hospitalo-Facultaire, Université Catholique de Louvain) and was run in compliance with the Declaration of Helsinki.
As we wanted to limit the impact of study participation at the beginning of the working day, we instructed the students to ask the third patient scheduled every day to take part in the study. If this patient refused, the student could ask the fourth, and so on. Patients received information on the purpose and procedures of the study. They filled in an informed consent form and the questionnaire. Students encoded the data anonymously and sent it to one of the investigators (AS), together with the original paper questionnaires. Participating students received extra credits for their algology exam. Students who did not wish to participate received a similar number of credits upon completing an alternative assignment. No gratification was offered to the supervisors.
Inclusion and Exclusion Criteria
All patients scheduled for an appointment with participating GPs could potentially be included in the study. Every working day, the third patient was eligible for the study, whatever the reason for the consultation. If he or she declined to participate, the fourth patient was invited to participate, and so on. Exclusion criteria were age under 18 and inability to answer questionnaires in French.
Questionnaires
Demographic questions included age, gender, weight, height, professional status (employed, student, retired, invalidity, unemployed), and postal code (allowing us to assess the geographical distribution of participants).
Lifestyle was assessed by (1) inquiring if the patient currently smoked (yes/no), (2) asking about any sleep problems (“During the last month, have you had any problems falling asleep or sleep problems?” with responses to be chosen from “never, sometimes, often, almost every night”) and (3) the Exercise Vital Sign (EVS, “On average, how many days per week do you engage in moderate to strenuous exercise (like a brisk walk)?” × “On average, how many minutes per day do you engage in exercise at this level?”).21,22
General health perception was assessed using the first item of the SF-36 questionnaire (“In general, would you say your health is…”, with categorical responses including “excellent, very good, good, fair, poor”).23 The eighth question from the original (long) Örebro Musculoskeletal Pain Screening Questionnaire (ÖMPSQ) assessed work perception (“Is your work heavy or monotonous?” with answers from 0 = not at all to 10 = extremely); answers < 4 were considered to indicate light work, between 4 and 6 moderately heavy and 7–10 heavy work.24
Patients who suffered from pain at the time of recruitment were asked additional questions to assess whether their pain was the reason for the consultation and whether it was related to active cancer. Moreover, we recorded pain localization using axis I of the IASP taxonomy of chronic pain syndromes, as well as the number of painful sites.25
Finally, we used the French version of the short ÖMPSQ as a prognostic tool.26,27 The short-form 10-item ÖMSPQ is derived from the original 25-item ÖMSPQ, a validated tool that assists clinicians in assessing the risk of persistent pain in people with musculoskeletal injury. It focuses mainly on “yellow flags”, which have been shown to be good predictors of the risk of persistent pain in the future, both in acute and chronic pain patients.28 The short version was developed to improve clinical utility, by being shorter and easier to administer and score than the original. It was found to be nearly as accurate as the original extended version.
Data Analysis
We used descriptive statistics to present the participant’s demographics, clinical characteristics and OMPSQ scores, which are reported as percentages or median (with interquartile range - IQR). We contrasted the results from patients without pain and those with pain. In the latter group, after excluding patients whose pain was attributed to active cancer, we differentiated between patients suffering from acute or subacute pain (pain duration less than three months) and patients with chronic pain. We compared the results between patient groups using Kruskal–Wallis’ tests for numerical or Fisher’s exact tests for categorical variables. For patients with pain, we computed the short ÖMPSQ score as described previously. We used cutoff scores of 45 and 55 to distinguish three groups of patients with a low, moderate, and high risk of chronicity.27 We analyzed missing values in the dataset in accordance with recently published recommendations.29 The percentage of missing values across the reported variables in Table 1 varied between 0 and 7.8%. Only the exercise vital sign (n = 223, 5.8% of the total) and the Örebro score (n = 211, 7.6% of patients in pain) had over 5% missing values. Logistic regression showed that the missingness of the EVS was not associated with any of the other variables, while that of the Örebro score was associated only with increasing age and tobacco use. Statistical analysis was performed with Microsoft Excel and SAS JMP Pro 15.2.
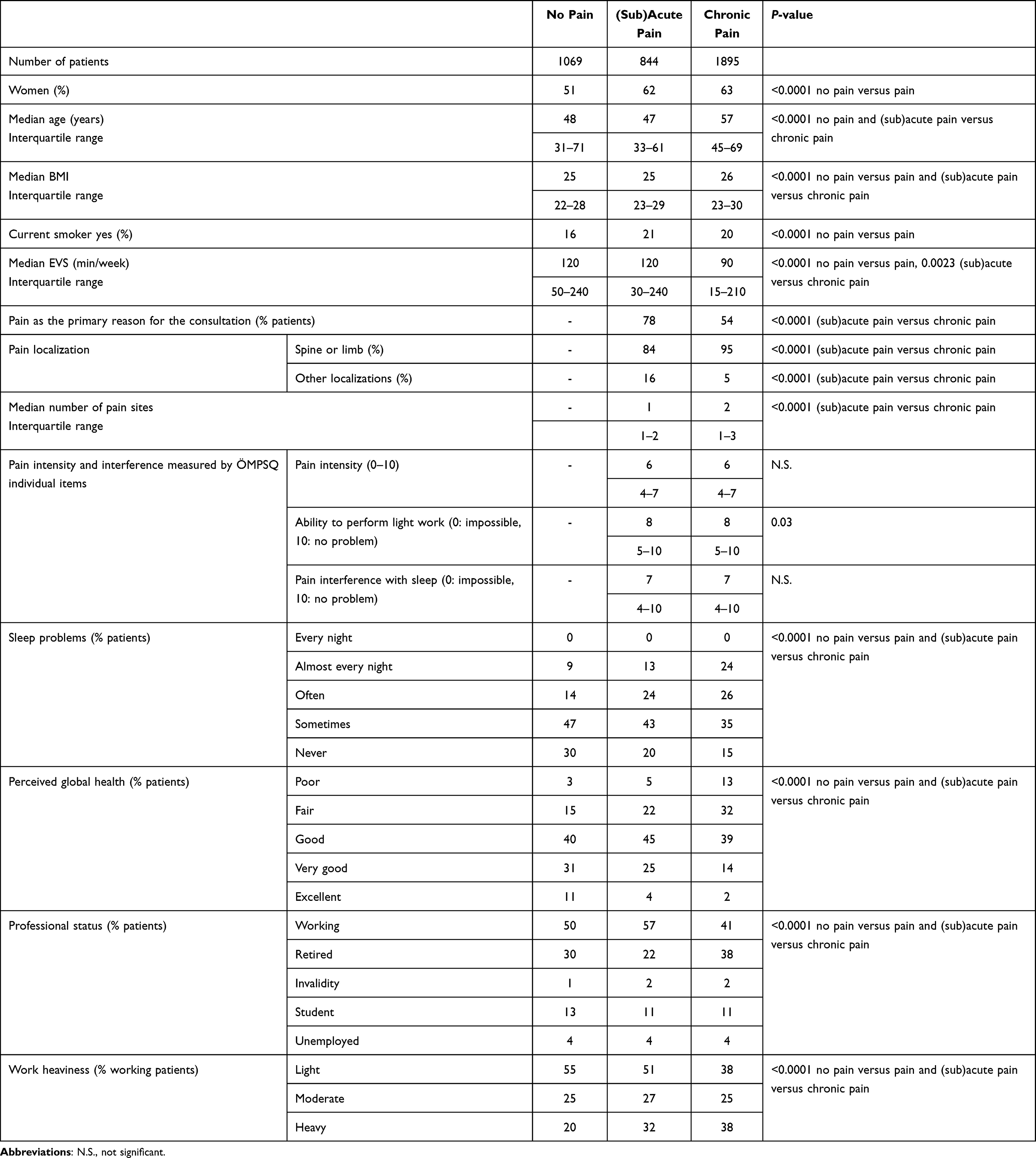 |
Table 1 Demographic and Clinical Data |
Results
Demographic and Clinical Characteristics
Out of 433 medical students, 289 took part in the study. They approached 5815 patients, of which 3882 agreed to fill in the questionnaires. Among those, and after excluding patients with cancer pain or missing data about pain duration, 28% reported no pain, 22% suffered from acute or subacute pain, and 49% had chronic pain (see Figure 1 for the study flowchart). These numbers suggest that, in this patient cohort, between 33% and 49% of patient contacts involved chronic pain patients, assuming respectively that all non-responding patients were pain-free and that the proportion of pain patients was the same in both groups. The geographical distribution of participating patients reflected the network of general practitioners affiliated with our university: nearly all patients live in French-speaking areas, and the provinces of Liège and Hainaut were under-represented.
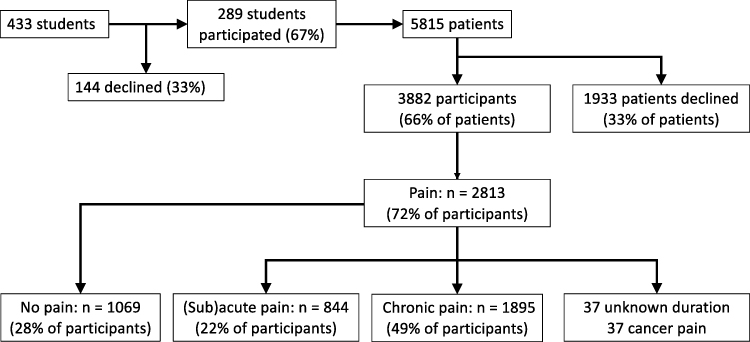 |
Figure 1 Flow chart of the study. “% of patients” refers to the percentage of screened patients, while “% of participants” refers to the percentage of patients who accepted to answer the study questionnaires. |
Demographic and clinical data are reported in Table 1. Patients with pain were more often women, had a higher Body Mass Index (BMI), were more likely to smoke and exercised less than patients with no pain. Chronic pain patients were older than other patients. Pain was more often the motive of the consultation for (sub)acute than for chronic pain patients. The median number of pain sites was 1 for (sub)acute patients and 2 for chronic patients. Most patients reported back or limb pain: 84% for patients with (sub)acute and 95% for patients with chronic pain. The median pain intensity, ability to do light work, and pain interference with sleep, as measured by individual items of the ÖMPSQ questionnaire, were not significantly different between (sub)acute and chronic pain patients and showed a moderate impact of pain. A gradient of decreased physical activity, increased sleep problems, and decreased perceived global health was observed, with pain-free patients reporting the best outcomes, followed by (sub)acute pain patients and, finally, by patients with chronic pain. Chronic pain patients were less often gainfully employed, considered their work heavier, and were more often retired than other patients.
The distribution of pain duration (Figure 2) showed that most (sub)acute pain patients had been suffering from pain for less than five weeks, while the vast majority (81%) of chronic pain patients had been experiencing pain for over a year.
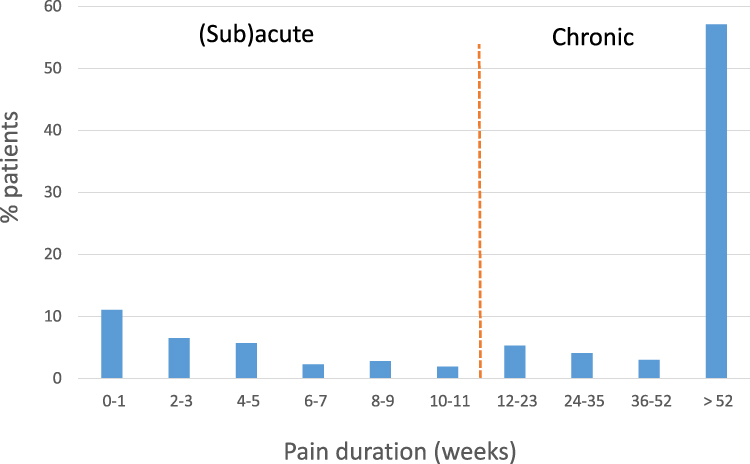 |
Figure 2 Distribution of pain duration in participating patients. |
Evaluation of Prognosis
Among painful patients, the proportion of patients in the different prognostic groups – evaluated by the short ÖMPSQ total score – was 43, 27 and 30%, in the low-, medium- and high-risk groups, respectively. The long-term prognosis was worse in chronic than in (sub)acute pain patients. The mean (SD) ÖMPSQ scores were 40 (2) and 52 (10) in (sub)acute and chronic pain patients, respectively (p<0.0001). Most (sub)acute pain patients were at low risk of persistent disabling pain in the future, while most chronic pain patients were at medium- or high risk. Still, about a third of chronic pain patients were at low risk of persistent disabling pain in the future (Figure 3).
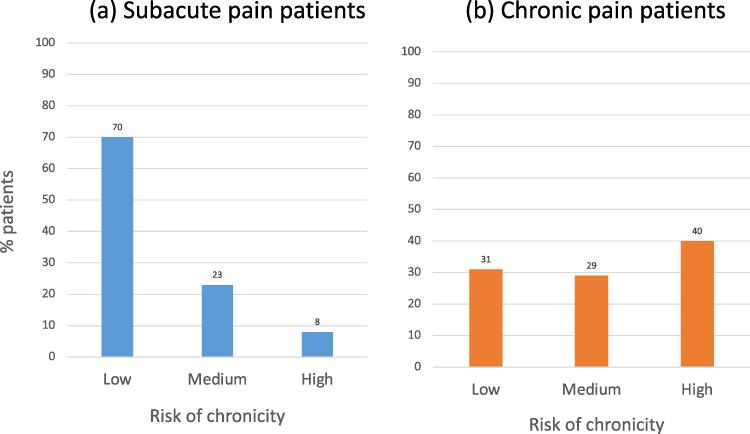 |
Figure 3 Proportion of participating patients suffering from subacute (a) or chronic (b) pain in the different categories of risk for persistent pain, as determined by the short Örebro Musculoskeletal Pain Screening Questionnaire (ÖMPSQ) scores. A majority of (sub)acute pain patients are at low risk of persistent pain. |
It should be noted, however, that the choice of cutoff scores in prognostic studies depends on several parameters: the chosen outcome variable (ie, work absence versus pain intensity versus functional limitations), and the objectives of the work (lowering the cutoff will increase sensitivity but decrease specificity). For example, Figure 4 shows that for scores in the 40–60 range, a threshold shift of 5 units can change the group assessment for more than 10% of the patients.
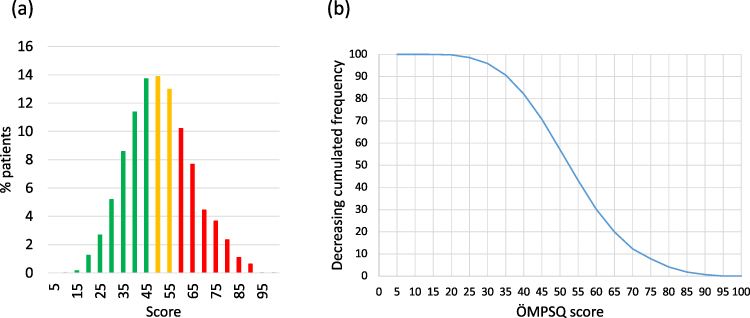 |
Figure 4 Distribution (a) of short Örebro Musculoskeletal Pain Screening Questionnaire (ÖMPSQ) score (green = low risk, yellow = medium risk, red = high risk of persistent pain) and cumulative distribution of the score (b) in participating patients. Panel b demonstrates that in the middle of the curve, a threshold shift of 5 units can change the group assessment for more than 10% of the patients. |
Discussion and Conclusion
The main finding of this study is that chronic pain patients account for a very high percentage (between 33 and 49%) of GP patient contacts and that most of these patients have been suffering for more than one year. Pain was the primary motive of the consultation for 78% of (sub)acute and 54% of chronic pain patients. Analysis of individual ÖMPSQ items suggests that pain has a moderate impact on the daily functioning of the patients. The total ÖMPSQ score indicates that a significant proportion of (sub)acute but, more surprisingly, of chronic pain patients as well, are at low risk of persistent disabling pain in the future. Finally, lifestyle (as evaluated by BMI, smoking status, sleep quality, and exercise level) and social determinants (professional status, work heaviness) are correlated with pain duration.
The point prevalence of chronic pain observed in our study is higher than that observed in most of the few similar studies in the general practice setting. For example, in a Danish study assessing pain as the primary motive for the consultation, 22% of patient contacts were motivated by pain, and 39% of those concerned chronic pain. However, this study did not record the number of pain patients consulting for other reasons than pain, thus underestimating the total number of pain patients.5 In Finland, pain was the main reason for the consultation in 40% of patients, while 21% (whatever the reason for the consultation) suffered from pain lasting more than six months.30 In a large German study assessing several GP practices (stratified by gender of the participating GP and by rural/semi-urban versus urban sites), the point prevalence of chronic pain in GP was 18% of patient contacts.6 In Italy, 32% of the contacts were pain patients, 53% of these being chronic.7 To our knowledge, only one study (in Bochum, Germany) reported a point prevalence comparable to our findings: in their population, 43% of patient contacts were primarily motivated by pain, but 62% of all patient contacts concerned patients suffering from pain, ⅔ of them (40% of the total) for over three months.4 In contrast, sex ratio, pain localization, and putative causes (mainly musculoskeletal) were comparable across studies and in good agreement with the Survey of Chronic Pain in Europe.1 The large variability between these studies is surprising. Breivik et al also observed significant differences between countries.1 However, their estimates of chronic pain prevalence in several countries (16% in Denmark, 17% in Germany, 19% in Finland, 23% in Belgium, 27% in Italy) do not parallel the differences between the above studies. Several factors may explain these discrepancies: regional differences in pain prevalence or severity, patients care-seeking behavior, availability of healthcare practices (for studies realized in healthcare settings), and differences in recruitment procedures, as well as in inclusion and exclusion criteria. For instance, all the studies mentioned above recruited consecutive patients, which is a significant difference that could explain the higher prevalence we found. The present study offered participation to the third scheduled patient every working day, whatever the reason for the consultation. If they declined, the fourth patient was invited to participate, and so on. This could have led to a selection bias, as patients suffering from pain were perhaps more likely to accept participation. This may have led to an overestimation of the proportion of painful patients.
Beyond prevalence, is essential to also consider the prognosis of patients in pain. In this work, we used the classical duration of 3 months to distinguish (sub)acute pain from chronic pain.31 However, it has been suggested that the term “chronic” can be both a description of pain history and a prognostic statement.32 Consequently, chronic pain is not a fixed state and should instead be viewed dynamically as “clinically significant pain likely to be present one or more years in the future”.32 While the ÖMPSQ has originally been validated with (sub) acute patients24,26 it has since then been shown to correlate with the outcome of patients with chronic low back33 or mixed pain.27 Our results show that 31% of the patients suffering from pain lasting for more than three months may be considered at low risk of persistent pain-related disability and may therefore still have a relatively good prognosis.
Regarding the prevention of the development of chronic pain through adequate management of acute pain patients, several studies have shown that a stratified model of care gives better results than a “one size fits all” treatment, notably in the treatment of subacute low back pain.34,35 In these stratified approaches, questionnaires such as the ÖMPSQ are helpful in adapting treatment to the patients’ needs and, therefore, calculating the resources needed for adequate management. For example, in an important study of stratified care for low-back pain patients medium risk patients received up to 6 physiotherapy sessions of 30 minutes, and high-risk patients had up to 6 sessions of 45 minutes delivered over approximately three months.16 In our study, the proportion of painful patients in the different prognostic groups is 43, 27 and 30%, in the low-, medium- and high-risk groups, respectively. Considering that a GP meets about 20 patients per day, every working day, a GP would meet an average of 3.8 patients at medium risk and 4.3 patients at high risk, generating approximately 36 hours of work for a physiotherapist (to be distributed during the three following months). Thus, the physiotherapy needs could be very high. However, this estimation relies on the following questionable assumptions: patients consult their GP only once, physiotherapy is the treatment of choice for high-risk patients, every high-risk patient will be ready to adopt such an approach, and stratified care validated using the Start Back Tool can be extrapolated to a stratified approach using the ÖMPSQ. Moreover, Figure 4 shows that small changes in cutoff scores can cause significant changes in patient group assessment. Therefore, the extrapolation given above must be considered with caution. It should also be noted that several recent studies which evaluated stratified approaches in GP settings have yielded less positive results.17,36,37 While their methodologies were different, all have reported difficulties in implementing the stratified care approaches, eg, ensuring that patients received the matched treatment for their risk level and that the treatments themselves were correctly executed. This emphasizes that these approaches require that providers master specific skills, notably to manage psychosocial issues.20
Finally, another interesting finding of this study is that it shows a correlation between pain and several lifestyle factors. Unfortunately, this transversal study does not allow for the assessment of causality: sedentary lifestyle, high BMI, bad sleep, or smoking could be either a cause or a consequence of chronic pain, stress, and disability. However, our recent systematic review does suggest that high body weight, smoking, and low physical activity are associated with a higher risk of persistent chronic neck and low-back pain.38 This question will be further assessed in a subsequent paper analyzing one-year follow-up data from the present cohort.
This study has several strengths and limitations. Strengths include the large geographical distribution (within French-speaking Belgium) of participating GPs, the large number of patients, and the assessment of pain impact on daily life. Limitations include the fact that we did not characterize the pain beyond duration and localization, and that the variability of cutoff scores can lead to uncertainty in prognosis assessment. In addition, the estimates of physiotherapy resources are very tentative and subject to criticism, as small changes in the initial assumptions may result in significant changes in the results. Finally, we used the ÖMSPQ to evaluate prognosis in all patients, even though it has initially been validated in acute low-back pain patients.24,26 However, recent reviews have suggested that prognostic factors are comparable across several pain conditions. In particular, psychosocial factors are associated with poor outcomes not only for musculoskeletal pain39 but also for post-surgical neuropathic pain,40 and for neuroplastic pain conditions such as irritable bowel disease41 and temporomandibular disorder.42 As the short form ÖMPSQ addresses most of these factors and does not refer specifically to musculoskeletal pain in its wording, it might be a good starting point in the search for a generic screening tool. In support of this view, we refer to Korogod et al, where we present longitudinal data confirming the usefulness of the ÖMSPQ for the prediction of patients with (sub)acute and chronic pain.27
In conclusion, chronic pain patients account for 33–50% of patient contacts in the GP setting in this sample of patients from French-speaking Belgium. Regarding secondary prevention strategies, and therefore improvement in public health, particularly important target populations might be the 31% of (sub)acute pain patients at medium and high risk of chronicity and the 31% of chronic pain patients at low risk of chronicity. These patient populations could represent between 15 and 22% of patient contacts in general practice. In light of this large population, it is unfortunate that GPs often feel ill at ease when meeting these patients, which stresses the importance of providing adequate support to GPs and other first-line professionals.9,10 Strengthened collaboration between these professionals and chronic pain centers is needed to provide better education to pain patients, giving them accurate and practical tools, helping them become less dependent on specialized care and more confident in their resources to prevent and manage pain.
Data Sharing Statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Acknowledgments
The study was approved by an independent ethic committee (2018/19JUI/258, Commission d’Éthique Biomédicale Hospitalo-Facultaire, Université Catholique de Louvain). We are very grateful to the medical students and their supervisors who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Arnaud Steyaert is supported by a research grant from the Fonds de Recherche Clinique of the Cliniques Universitaires Saint-Luc.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287–333. doi:10.1016/j.ejpain.2005.06.009
2. Berquin A, Faymonville M, Deseure K et al. Prise en charge de la douleur chronique en Belgique: passé, present et futur [Management of chronic pain in Belgium: past, present and future]. Available from: https://www.health.belgium.be/sites/default/files/uploads/fields/fpshealth_theme_file/douleurrapportetude.pdf.
3. Smith BH, Hopton JL, Chambers WA. Chronic pain in primary care. Fam Pract. 1999;16(5):475–482. doi:10.1093/fampra/16.5.475
4. Friessem CH, Willweber-Strumpf A, Zenz MW. Chronic pain in primary care. German figures from 1991 and 2006. BMC Public Health. 2009;9:299. doi:10.1186/1471-2458-9-299
5. Frolund F, Frolund C. Pain in general practice. Pain as a cause of patient-doctor contact. Scand J Prim Health Care. 1986;4(2):97–100. doi:10.3109/02813438609014810
6. Hensler S, Heinemann D, Becker MT, et al. Chronic pain in German general practice. Pain Med. 2009;10(8):1408–1415. doi:10.1111/j.1526-4637.2009.00735.x
7. Koleva D, Krulichova I, Bertolini G, Caimi V, Garattini L. Pain in primary care: an Italian survey. Eur J Public Health. 2005;15(5):475–479. doi:10.1093/eurpub/cki033
8. Gonzalez-Chica DA, Vanlint S, Hoon E, Stocks N. Epidemiology of arthritis, chronic back pain, gout, osteoporosis, spondyloarthropathies and rheumatoid arthritis among 1.5 million patients in Australian general practice: NPS MedicineWise MedicineInsight dataset. BMC Musculoskelet Disord. 2018;19(1):20. doi:10.1186/s12891-018-1941-x
9. Elder N, Ricer R, Tobias B. How respected family physicians manage difficult patient encounters. J Am Board Fam Med. 2006;19(6):533–541. doi:10.3122/jabfm.19.6.533
10. Kristiansson MH, Brorsson A, Wachtler C, Troein M. Pain, power and patience--a narrative study of general practitioners’ relations with chronic pain patients. BMC Fam Pract. 2011;12:31. doi:10.1186/1471-2296-12-31
11. Eklund K, Stalnacke BM, Stenberg G, Enthoven P, Gerdle B, Sahlen KG. A cost-utility analysis of multimodal pain rehabilitation in primary healthcare. Scand J Pain. 2021;21(1):48–58. doi:10.1515/sjpain-2020-0050
12. Eklund K, Stalnacke BM, Sundberg A, Eklund F, Eklund M. Introduction of a multimodal pain rehabilitation intervention in primary care: a pilot study. J Rehabil Med Clin Commun. 2023;6:3712. doi:10.2340/jrmcc.v6.3712
13. Falkhamn LM, Stenberg G, Enthoven P, Stalnacke BM. Interdisciplinary multimodal pain rehabilitation in patients with chronic musculoskeletal pain in primary care-a cohort study from the Swedish Quality Registry for Pain Rehabilitation (SQRP). Int J Environ Res Public Health. 2023;20(6):5051. doi:10.3390/ijerph20065051
14. Pietila-Holmner E, Enthoven P, Gerdle B, Molander P, Stalnacke BM. Long-term outcomes of multimodal rehabilitation in primary care for patients with chronic pain. J Rehabil Med. 2020;52(2):jrm00023. doi:10.2340/16501977-2649
15. Westman A, Linton SJ, Ohrvik J, Wahlen P, Theorell T, Leppert J. Controlled 3-year follow-up of a multidisciplinary pain rehabilitation program in primary health care. Disabil Rehabil. 2010;32(4):307–316. doi:10.3109/09638280903095924
16. Hill JC, Whitehurst DG, Lewis M, et al. Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a randomised controlled trial. Lancet. 2011;378(9802):1560–1571. doi:10.1016/S0140-6736(11)60937-9
17. Konstantinou K, Lewis M, Dunn KM, et al. Stratified care versus usual care for management of patients presenting with sciatica in primary care (SCOPiC): a randomised controlled trial. Lancet Rheumatol. 2020;2(7):e401–e411. doi:10.1016/S2665-9913(20)30099-0
18. Hill JC, Garvin S, Bromley K, et al. Risk-based stratified primary care for common musculoskeletal pain presentations (STarT MSK): a cluster-randomised, controlled trial. Lancet Rheumatol. 2022;4(9):e591–e602. doi:10.1016/S2665-9913(22)00159-X
19. Saunders B, Chudyk A, Protheroe J, et al. Risk-based stratified primary care for common musculoskeletal pain presentations: qualitative findings from the STarT MSK cluster randomised controlled trial. BMC Prim Care. 2022;23(1):326. doi:10.1186/s12875-022-01924-3
20. Foster NE, Delitto A. Embedding psychosocial perspectives within clinical management of low back pain: integration of psychosocially informed management principles into physical therapist practice--challenges and opportunities. Phys Ther. 2011;91(5):790–803. doi:10.2522/ptj.20100326
21. Coleman KJ, Ngor E, Reynolds K, et al. Initial validation of an exercise “vital sign” in electronic medical records. Med Sci Sports Exerc. 2012;44(11):2071–2076. doi:10.1249/MSS.0b013e3182630ec1
22. Mork PJ, Vik KL, Moe B, Lier R, Bardal EM, Nilsen TI. Sleep problems, exercise and obesity and risk of chronic musculoskeletal pain: the Norwegian HUNT study. Eur J Public Health. 2014;24(6):924–929. doi:10.1093/eurpub/ckt198
23. Ware JE, Gandek B. Overview of the SF-36 health survey and the International Quality of Life Assessment (IQOLA) project. J Clin Epidemiol. 1998;51(11):903–912. doi:10.1016/s0895-4356(98)00081-x
24. Linton SJ, Boersma K. Early identification of patients at risk of developing a persistent back problem: the predictive validity of the Orebro Musculoskeletal Pain Questionnaire. Clin J Pain. 2003;19(2):80–86. doi:10.1097/00002508-200303000-00002
25. Turk DC, Rudy TE. IASP taxonomy of chronic pain syndromes: preliminary assessment of reliability. Pain. 1987;30(2):177–189. doi:10.1016/0304-3959(87)91073-6
26. Linton SJ, Nicholas M, MacDonald S. Development of a short form of the orebro musculoskeletal pain screening questionnaire. Spine. 2011;36(22):1891–1895. doi:10.1097/BRS.0b013e3181f8f775
27. Korogod N, Steyaert A, Nonclercq O, Opsommer E, Berquin A. Can the French version of the short Orebro Musculoskeletal Pain Screening Questionnaire or its subsets predict the evolution of patients with acute, (sub) acute and chronic pain? BMC Musculoskelet Disord. 2022;23(1):311. doi:10.1186/s12891-021-04944-9
28. Nicholas MK, Linton SJ, Watson PJ, Main CJ; Decade of the Flags Working Group. Early identification and management of psychological risk factors (“yellow flags”) in patients with low back pain: a reappraisal. Phys Ther. 2011;91(5):737–753. doi:10.2522/ptj.20100224
29. Lee KJ, Tilling KM, Cornish RP, et al. Framework for the treatment and reporting of missing data in observational studies: the Treatment And Reporting of Missing data in Observational Studies framework. J Clin Epidemiol. 2021;134:79–88. doi:10.1016/j.jclinepi.2021.01.008
30. Mantyselka P, Kumpusalo E, Ahonen R, et al. Pain as a reason to visit the doctor: a study in Finnish primary health care. Pain. 2001;89(2–3):175–180. doi:10.1016/s0304-3959(00)00361-4
31. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
32. Von Korff M, Miglioretti DL. A prognostic approach to defining chronic pain. Pain. 2005;117(3):304–313. doi:10.1016/j.pain.2005.06.017
33. Hilfiker R, Knutti IA, Raval-Roland B, Rivier G, Crombez G, Opsommer E. Validity and responsiveness of the French version of the Orebro Musculoskeletal Pain Screening Questionnaire in chronic low back pain. Eur Spine J. 2016;25(9):2741–2749. doi:10.1007/s00586-016-4635-9
34. Meyer C, Denis CM, Berquin AD. Secondary prevention of chronic musculoskeletal pain: a systematic review of clinical trials. Ann Phys Rehabil Med. 2018;61(5):323–338. doi:10.1016/j.rehab.2018.03.002
35. Ogbeivor C, Elsabbagh L. Management approach combining prognostic screening and targeted treatment for patients with low back pain compared with standard physiotherapy: a systematic review & meta-analysis. Musculoskeletal Care. 2021;19(4):436–456. doi:10.1002/msc.1541
36. Delitto A, Patterson CG, Stevans JM, et al. Stratified care to prevent chronic low back pain in high-risk patients: the TARGET trial. A multi-site pragmatic cluster randomized trial. EClinicalMedicine. 2021;34:100795. doi:10.1016/j.eclinm.2021.100795
37. Morso L, Olsen Rose K, Schiottz-Christensen B, Sowden G, Sondergaard J, Christiansen DH. Effectiveness of stratified treatment for back pain in Danish primary care: a randomized controlled trial. Eur J Pain. 2021;25(9):2020–2038. doi:10.1002/ejp.1818
38. Manderlier A, de Fooz M, Patris S, Berquin A. Modifiable lifestyle-related prognostic factors for the onset of chronic spinal pain: a systematic review of longitudinal studies. Ann Phys Rehabil Med. 2022;65(6):101660. doi:10.1016/j.rehab.2022.101660
39. Artus M, Campbell P, Mallen CD, Dunn KM, van der Windt DA. Generic prognostic factors for musculoskeletal pain in primary care: a systematic review. BMJ Open. 2017;7(1):e012901. doi:10.1136/bmjopen-2016-012901
40. Heinzel JC, Dadun LF, Prahm C, et al. Beyond the knife-reviewing the interplay of psychosocial factors and peripheral nerve lesions. J Pers Med. 2021;11(11):1200. doi:10.3390/jpm11111200
41. Klem F, Wadhwa A, Prokop LJ, et al. Prevalence, risk factors, and outcomes of irritable bowel syndrome after infectious enteritis: a systematic review and meta-analysis. Gastroenterology. 2017;152(5):1042–1054 e1. doi:10.1053/j.gastro.2016.12.039
42. Jung W, Lee KE, Suh BJ. Influence of psychological factors on the prognosis of temporomandibular disorders pain. J Dent Sci. 2021;16(1):349–355. doi:10.1016/j.jds.2020.02.007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.