Back to Journals » Journal of Pain Research » Volume 15
The Focus and New Progress of Percutaneous Balloon Compression for the Treatment of Trigeminal Neuralgia
Authors Xia Y ![]() , Yu G, Min F
, Yu G, Min F ![]() , Xiang H, Huang J, Leng J
, Xiang H, Huang J, Leng J
Received 14 May 2022
Accepted for publication 2 September 2022
Published 29 September 2022 Volume 2022:15 Pages 3059—3068
DOI https://doi.org/10.2147/JPR.S374433
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Krishnan Chakravarthy
Yinghua Xia,1,2 Gui Yu,2,3 Feixiang Min,1,2 Hui Xiang,2 Jinqing Huang,4,5 Jingxing Leng2
1Medical College of Nanchang University, Nanchang, People’s Republic of China; 2Department of Neurosurgery, Jiangxi Provincial People’s Hospital, Nanchang, People’s Republic of China; 3The First Clinical Medical College of Gannan Medical University, Ganzhou, People’s Republic of China; 4Department of Neurosurgery, Ganzhou People’s Hospital, Ganzhou, People’s Republic of China; 5Department of Neurosurgery, the Affiliated Ganzhou Hospital of Nanchang University, Ganzhou, People’s Republic of China
Correspondence: Hui Xiang, Jiangxi Provincial People’s Hospital, No. 266, Fenghe North Avenue, Honggutan District, Nanchang City, People’s Republic of China, Tel +86-13803514563, Email [email protected] Jinqing Huang, Ganzhou People’s Hospital, No. 16, Meiguan Avenue, Zhanggong District, Ganzhou City, People’s Republic of China, Tel +86-18160779765, Email [email protected]
Abstract: Trigeminal neuralgia is a condition confined to the trigeminal nerve, causing one or more branches of facial nerve pain. Surgical treatment options for trigeminal neuralgia include microvascular decompression(MVD), percutaneous balloon compression (PBC), radiofrequency thermocoagulation(RF), percutaneous retrogasserian glycerol rhizotomy(PRGR), gamma knife, etc. Of these treatments, PBC is increasingly being used by clinicians for trigeminal neuralgia. PBC is a simple surgical operation performed to treat trigeminal neuralgia. Owing to its advantages, PBC is favored by many clinicians. In this study, we aimed to emphasize the need to analyze the shape of the balloon, position, compression time, and pressure, as these factors can affect the efficacy of PBC. The relief of pain by balloon compression is related to the shape of the balloon on X-ray, which is the key to the operation. Owing to continued progress and advances in current imaging technologies, clinicians revealed that the precise positioning of the foramen ovale is no longer an intraoperative problem. Instead, the anatomy of Meckel’s cave and the shape of the balloon must be the focus to achieve the best treatment effect. For clinicians, PBC is simple and is associated with a short operation time. PBC also has other advantages, such as low cost and immediate postoperative pain relief. The recurrence rate of pain post-PBC is low, despite the occurrence of facial numbness post-op. However, this side effect is reversible and does not affect daily life of the patient. In fact, the patient can be discharged 1– 2 days after surgery. Overall, PBC can be considered as one of the preferred surgical methods for the treatment of primary trigeminal neuralgia. In this paper, we explain the main points of PBC operation in detail in terms of Meckel’s cave, surgical procedure, complications, discussion of the focus and new progress, etc.
Keywords: trigeminal neuralgia, balloon compression, Meckel’s cave, trigeminocardiac reflex
Introduction
Trigeminal neuralgia is a common neuropathic pain experienced in neurosurgery that is mainly manifested as pain in the unilateral distribution area of facial trigeminal nerve branches. The pain is mainly in the distribution of second and third branches, and bilateral is relatively rare. Trigeminal neuralgia can often be triggered by minor actions in the face, which have characteristic trigger points. These actions cause electric shock or shooting-like pain. In the early stages of the disease, the pain can last from a few seconds to 2 min and can gradually develop into persistent facial pain as the disease progresses.1,2
At present, trigeminal neuralgia is first treated with drugs, mainly carbamazepine. If patients exhibit drug tolerance and the treatment effect is not obvious, surgery is employed for treatment. According to the classification of IASP, trigeminal neuralgia is currently divided into three types: classic, secondary, and idiopathic. Classical trigeminal neuralgia causes pain due to focal demyelination induced by compression of the trigeminal nerve root by the responsible blood vessel, especially in the central myelin-peripheral myelin transitional zone.3–8 Microvascular decompression (MVD) is currently the first-line surgical therapy for trigeminal neuralgia. However, not all patients with trigeminal neuralgia have neurovascular conflict. In fact, approximately 12% of patients do not have a neurovascular conflict.2,9 Based on continuous research and attempts to discover trigeminal neuralgia treatment methods, other surgical methods have emerged. Of these methods, PBC is favored by a growing number of clinicians owing to its simple operation and evident efficacy.
Percutaneous balloon compression (PBC) was first proposed by Mullan and Lichtor10 in 1983 for the treatment of trigeminal neuralgia. By using a puncture needle, placing the balloon in the Meckel’s cave, and filling the balloon to form a “pear” shape, the shape can be maintained and the trigeminal ganglia in the Meckel’s cave can be compressed for a short time, thereby immediately relieving facial pain after surgery. The postoperative pain relief effect of PBC is significant and is associated with a long pain relief period. Compared to many minimally invasive or non-invasive therapies, the overall surgical procedure of PBC is simple, the operation time is short, the surgical wound is small, and the operation can be repeated. Further, the postoperative complications of PBC will not affect the daily life of the patient. Therefore, PBC has been increasingly used by clinicians in recent years. With the continuous development of auxiliary technologies, the surgical focus of PBC is increasingly on the morphological changes of the balloon. As a result, the surgical details of PBC must be carefully analyzed.
Anatomy of Meckel’s Cave
As the dural space containing the trigeminal ganglion, the anatomy of the Meckel’s cave determines the intraoperative shape of the balloon in the Meckel’s cave. In fact, Meckel’s cave is the dural concave protruding from the postcranial fossa. Based on the sagittal image from MRI, the shape of Meckel’s cave can be divided into three different types: bulbous, oval, and flat, with the oval as the most common shape, accounting for 60% of cases. Few trigeminal neuralgia patients do not have Meckel’s cave.11,12 Meckel’s cave is divided into upper, lower, anterior, posterior walls, inner and lateral walls. The anterior and upper walls are adjacent to the posterior venous space of the posterior cavernous sinus; the lateral wall is adjacent to the dura of the medial fossa, and the front of the inner wall is adjacent to the posterior cavernous sinus segment of the internal carotid artery. As the internal carotid artery enters the cavernous sinus below the Meckel’s cave, special attention must be paid to avoid damage to the internal carotid artery, as the resulting bleeding will lead to delayed surgery to enable emergency treatment. The arachnoid and meningeal layers of the dura mater are closely connected to the trigeminal ganglia, which reverse on the nerve surface to form a dural sheath. Further, the three branches of the trigeminal ganglia penetrate the dura. The cavernous sinus is adjacent to the trigeminal ganglion, where V1 and V2 exit through the cavernous sinus. In contrast, V3 does not penetrate the cavernous sinus.13 Intraoperative puncture or balloon injury can cause a cavernous fistula. Fiber masses in the trigeminal ganglion occupy most of the ganglia. The three branches originating from the trigeminal ganglion each correspond to the respective fibrous nerve masses.14 Brown et al found that balloon compression relieves the pain of trigeminal neuralgia by damaging myelinated axons in rabbits, and that large fibers are more affected than smaller fibers, because they undergo greater mechanical deformation than smaller fibers at a given pressure. Surgery can be used to relieve pain as the balloon selectively damages the larger myelinated nerve fibers associated with the conduction of nociception, while the smaller unmyelinated nerve fibers are not damaged. As a result, the conduction in corneal reflex fibers is preserved, which is a unique advantage in the treatment of pain in the branch I distribution area.15,16
Operative Procedure
Patients subjected to PBC are treated under general anesthesia in the supine position. The Hartel approach method is used. The point of the needle entering the skin is 2.5 cm lateral to the corners of the mouth, and the other two reference points are located 3 cm anterior to the ipsilateral external auditory canal and 1 cm below the pupil. The relative position of the needle and the foramen ovale is constantly determined using the C-arm. During the puncture process, the puncture needle should not pierce the oral mucosa, which would cause contamination. The author suggests that the front end of the puncture needle should be at the outer mouth of the foramen ovale on the lateral X-ray film (Figure 1). After importing the balloon, it is most appropriate that the mark of the end of the balloon catheter exceeds the clivus line by 0.5 cm (Figure 2), enabling the “pear” shaped balloon to be obtained smoothly (Figure 3). If the puncture is too deep, the balloon may slip away from the Meckel’s cave and form an ovale balloon shape. If the puncture is too shallow, the balloon may leave part of the bone pipe in the foramen ovale and eventually form an inverted “pear” shape with a small protuberance oblique. After the balloon is inserted into the Meckel’s cave, approximately 0.4–0.8 mL of contrast media is slowly injected into the balloon to fill the balloon; the position and shape of the balloon are then verified. If the balloon does not possess a good shape, the angle and position of the needle will be adjusted, and the balloon will be readjusted to obtain the ideal “pear” shape. After the balloon is compressed for approximately 3 min, the contrast media is removed, the catheter is removed, and the skin is pressed on the puncture site for 5–10 min. Pear shaped is not always radiologically obtained, in fact we can use the presence of conjunctival hyperemia as evidence of successful compression. After surgery, only a small facial puncture would be visible, and the pain would be relieved immediately. If there are no side effects after the operation, patients can be discharged 1–2 days later.
 |
Figure 1 (A) The needle penetrated the foramen ovale; (B) the puncture needle. |
 |
Figure 2 (A) The clivus line; (B) the mark of the end of the balloon catheter. |
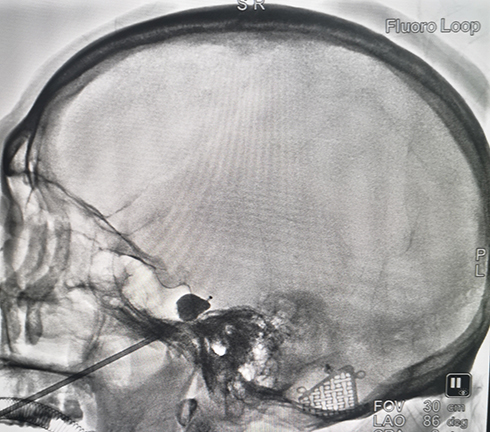 |
Figure 3 Contrast media is injected into the balloon to fill the balloon and obtain the “pear” shape. |
Common Intraoperative Phenomenon: Trigeminocardiac Reflex
During PBC, when the needle in the foramen ovale causes mechanical compression of the mandibular nerve or the enlarged balloon compresses the trigeminal ganglion, the heart rate and blood pressure of patients are found to decline. Further, balloon compression of the trigeminal ganglion is more obvious. This phenomenon is called the trigeminocardiac reflex (TCR), and it is often observed during the operation. The incidence of TCR is approximately 97.3%.17
The TCR is essentially a brainstem reflex. Owing to this physiological response, systemic and cerebral circulation are adjusted, blood is transferred to the brain, or blood flow increases in the brain. The potential mechanism of the TCR is still not clear. However, when the trigeminal ganglion nerve branch is compressed, trigeminal nerve sensory endings via the trigeminal ganglion to trigeminal nerve sensory nucleus are thought to form the afferent pathway of the reflex and connect with the efferent pathway in the vagus nerve motor nucleus, causing parasympathetic activation and sympathetic inhibition, eventually leading to reduced heart rate and blood pressure.18,19
When the TCR occurs during the operation, the reflex can be automatically relieved quickly after halting the operation, and the normal heart rate and blood pressure can be restored. At this time, the operation can continue. Notably, the TCR is often particularly severe for some patients and can cause cardiac arrest. In this case, the operation must be immediately stopped and atropine must be injected to inhibit the vagus pathway.20,21 Generally, the heart rate and blood pressure will return to normal even if the reflex recurs, as the reflex strength will be weaker than before.22 Some surgeons administer atropine at the beginning of surgery to prevent the occurrence of the TCR. For patients with TCR that cannot be controlled with atropine and lidocaine, a continuous infusion of isoproterenol can be used to ensure that the heart rate is maintained above 90 bpm.23 TCR is very common in surgery. Generally, proper prevention and treatment measures will not affect the completion of the treatment process. Further, the emergence of this reflex shows that the balloon does compress the trigeminal ganglion located in the Meckel’s cave, which is a common phenomenon to ensure the success of surgery.
Surgical Effect After Surgical Operation
When PBC is used as a surgical method for trigeminal neuralgia, the initial postoperative pain relief rate is approximately 82–97.1%, the pain relief time is approximately 18–20 months.22,24–27 The time of symptom recurrence after PBC is related to the degree of balloon compression on the trigeminal ganglion, the length of compression, and the recovery after nerve injury. For patients with recurrent pain after PBC, repeated PBC can be performed. The immediate pain relief rate of postoperative pain after repeated PBC is approximately 93.8%. The recurrence rate of repeated PBC is slightly higher than that after the first operation. In another study, the mean pain relief time to recurrence was 11.8 months for PBC versus 9.0 months for MVD.28,29
Complications
As with any destructive surgery, the most common postoperative complication is the loss of facial sensation. Facial numbness is directly related to the success of the operation and is an important indicator of sufficient compression. Complications include facial hypesthesia, masseter weakness, herpes labialis, meningitis, arterial hemorrhage, etc.30–32 For corneal sensation, the effect of PBC was not significant Table 1.
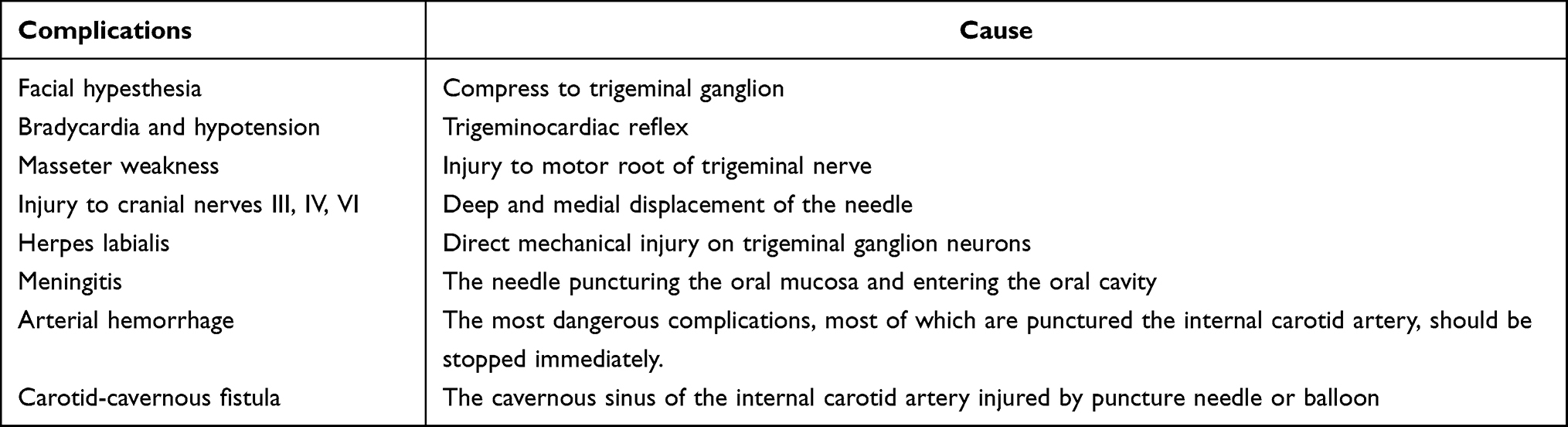 |
Table 1 Possible Complications in the Operation |
Other Operative Treatments Compared with PBC
Drugs or surgery can be used to treat trigeminal neuralgia. For patients that are unresponsive to drugs, several surgical methods are available, such as MVD, RF, PRGR, Gamma Knife, etc Table 2.15,24,26,31,33
 |
Table 2 Surgical Treatment of Other Trigeminal Neuralgia |
Compared with other surgical methods for trigeminal neuralgia, PBC, as a minimally invasive and simple surgical treatment, has a short operation time. Furthermore, compared with other surgical methods, the postoperative complications of PBC are less and the most reversible. The most common postoperative facial numbness can gradually recover within 3–6 months. In terms of pain relief effect and recurrence rate, the cost of PBC is less than other treatments, which markedly reduces the cost incurred by patients. Further, most patients can be treated with PBC. Owing to more advanced imaging technologies, the overall performance of PBC is not difficult, and the patient can experience relief from pain immediately after surgery. Further, the postoperative recurrence rate is low. Most importantly, PBC selectively damages large, myelinated nerve fibers that conduct pain, without impacting small fibers that maintain corneal reflex.
Discussion
PBC consists of two main steps: correct needle insertion at the foramen ovale and correct balloon insertion in the Meckel’s cave. Using imaging technology, we can determine whether the needle has accurately reached the foramen ovale and is in the correct position. The shape of the balloon can also be observed via imaging. If the balloon shape is round, funnel-shaped, or assumes other shapes, the contrast media should be withdrawn in time, and the position of the puncture needle should be adjusted, until the balloon presents a typical “pear” shape; this is an important imaging indication to ensure the efficacy of PBC. In addition to the effect of balloon shape on efficacy, the balloon pressure and compression time are important factors affecting postoperative efficacy. However, there is no unified standard for these indicators, which still needs to be explored.
Positioning of the Foramen Ovale is No Longer the Main Intraoperative Step
In the past, clinicians emphasized the importance of foramen ovale positioning during PBC and even considered it as the most critical step in PBC. Indeed, the precision of the foramen ovale puncture is an indispensable step in PBC; however, owing to continuous development of imaging technology, except for approximately 2–4% of patients were found to have a foramen ovale with obvious anatomical variation, it is not difficult for most patients to accurately locate the foramen ovale.34 For most patients, the position of the foramen ovale is under the C-arm. With intraoperative imaging, the operator can clearly see the location of the foramen ovale and the puncture needle.
In addition to the most commonly used C-arm, for foramen ovale puncture, a 3D-CT guide can also be selected. A CT scan of the patient and a 3D reconstruction of the acquired CT images on the post processing workstation can reveal the exact position of the needle and the ovale to enable adjustments of the position of the needle to achieve fast and accurate identification of the foramen ovale. Robot-assisted operations have also been performed in recent years, although this technology requires a long preoperative preparation time. However, for foramen ovale positioning, the use of this technology can enable high accuracy and safety. Further, positioning error can be controlled at 0.14 mm, the operation time can be remarkably reduced, and the incidence of serious complications caused by multiple punctures can be decreased. Moreover, the neuronavigation technique may be an alternative for specific patients with significant anatomical variants that cause unsuccessful foramen ovale puncture.34–38
Previously, clinicians emphasized the importance of the foramen ovale puncture. If the imaging technology is in its infancy and the operator is not skilled, the time taken to find the foramen ovale is often long. Further, due to individual differences, accurate punctures are needed to locate the foramen ovale position. Multiple punctures often lead to more muscle, blood vessel, and nerve damage; increase the incidence of postoperative complications; and affect the operation time and success rate. However, under the current technical conditions and other auxiliary conditions, precise positioning of the foramen ovale is no longer difficult. In particular, with the availability of different imaging techniques, the location of the foramen ovale can be identified and reached with the naked eye. Accordingly, the surgeon should mainly focus on the location and morphological changes of the balloon.
The Key Point—Shape and Morphological Changes of the Balloon
The crucial point of PBC, which is also a sign of surgical success, is the “pear” shape of the C-arm presented by the balloon located in the Meckel’s cave. Owing to intraoperative emphasis on the appearance of the shape and the anatomy of the Meckel’s cave itself, when the balloon is in the Meckel’s cave, it naturally assumes the shape of the Meckel’s cave. Accordingly, the balloon leads to sufficient compression to achieve pain relief in a limited compression time.
Morphological Changes of the Balloon
Based on the anatomy of the Meckel’s cave, when the balloon is in the correct position and the contrast medium is injected, the balloon assumes the anatomical shape of the Meckel’s cave and appears similar to a “pear.” Balloon filling pressure can cause enough compression of the trigeminal ganglia and trigeminal nerve root to enable the best compression effect. Since the establishment of PBC, the intraoperative “pear” shaped balloon has been regarded as a necessary condition for successful operation. The final efficacy of surgery is mainly related to intraoperative balloon morphology, compression time, and balloon pressure. Among them, the shape of the balloon is the most important influencing factor, and the pain relief rate is markedly better in patients with an obvious pear shape than in those without this pear shape.22,39 After the balloon enters the Meckel’s cave, the contrast medium is injected into the balloon, leading to a large abdomen and the tip of a small bulge consisting of a “pear-shaped”. Dissection of the carcass revealed several small openings in the dura bordering the upper and lower walls of the Meckel’s cave. Li et al40 called these openings the “cribriform district.” Cribriform district separates the Meckel’s cave from the peripheral sheath. Only the motor roots of the trigeminal nerve fibers do not pass through the cribriform region. Instead, a separate sheath enters the wall of the Meckel’s cave. Due to the anatomy of the Meckel’s cave, when the balloon is located in the Meckel’s cave, it can eventually present a “pear-shaped” consisting of a large abdomen and a tip. The oblique upward protrusion is very important. Due to the narrow porus trigeminus, the balloon will form a small protrusion around the narrow porus trigeminus, causing compression on the trigeminal nerve root and axon damage. In the absence of such a small protrusion formation, the pain relief effect is often worse. When the balloon is not placed correctly and the needle is too shallow, the balloon may leave a part of the bony pipe of the foramen ovale to form a small inverted protrusion. When the balloon presents an inverted “pear” shape, the small protrusion will cause more obvious compression on the mandibular nerve, which will be too backward to form the “dumbbell” shape. If the balloon completely slides out of the cavity, only an original oval shape can form outside the cavity.39,41 Whether “dumbbell” shaped, oval shaped, or inverted “pear” shaped balloon, the pain relief is worse than that of the “pear” shaped balloon. Some balloon shapes, such as “dumbbell” shaped balloons, can also cause some degree of postoperative pain relief, as well as effective compression on the trigeminal ganglion. However, only an ideal “pear shape” can achieve the best surgical results.42
The Current Balloon Compression Time and Pressure
In addition to the position of the balloon relative to Meckel’s cave, the time and pressure of filling the balloon also affect the shape and compression effect of the balloon. At present, there is no unified standard for the intraoperative balloon compression time and balloon pressure during compression. However, the span of balloon compression and compressive pressure are related to postoperative pain relief of the patients, the severity of complications, and the recurrence rate of pain. At present, the main sign of the ideal “pear” shape is the success of the operation; however, increasing number of scholars are focusing on the impact of compression time and pressure on the surgical effect.
Time
The time of balloon compression will affect the postoperative recurrence rate and the degree of facial sensory loss. The appropriate compression time can control the surgical procedure more reasonably, reduce the incidence of postoperative facial numbness and other complications, and reduce the recurrence rate of pain. Most studies have shown that the compression time of 1–3 minutes can effectively relieve the pain of patients, and for recurrent trigeminal neuralgia, the compression time can be extended to 5 min or even more.15,42,43 In animal experiments for rabbits, a compression time of 2 min could effectively inhibit pain conduction. Further, using an electron microscope, large-diameter myelin nerve axon swelling, rupture, and demyelination changes could be observed. When the compression time was extended to 5 min, these phenomena were more obvious, indicating that a long compression time is more effective for pain recurrence or refractory trigeminal neuralgia.44 In recent years, the time of balloon compression has been controversial. To obtain a perfect “pear” shaped balloon, some surgeons believe that full compression for 60s can achieve effective pain relief. Of note, more than 5 min of compression has not been found to result in a better pain relief effect. However, a longer compression time is closely related to the incidence of complications, especially postoperative facial feeling.45,46
Pressure and Volume
The pressure of balloon compression and the volume of contrast injection have not been unified. Full compression in the correct position is crucial for the relief of trigeminal neuralgia using PBC. The balloon pressure determines the extent of damage to the trigeminal ganglion. If intraoperative balloon pressure monitoring is found when the balloon presents a typical “pear” shape, the injection of contrast media should be halted, and over time, the balloon pressure will reduce.47 This occurrence may be related to slight tissue deformation caused by balloon compression surrounding the tissue. Pressure reduction may also lead to insufficient trigeminal ganglion compression, ultimately affecting the efficacy of the operation. Brown et al43 suggested that the balloon pressure can be approximately 1160 ± 62 mmHg; within this pressure range, the balloon can present a typical “pear” shape and achieve good compression effect. The pressure of the balloon can be quantitatively analyzed by the volume of the contrast media injection. Based on practical surgical experience, contrast media injection volume is 0.4–0.8 mL; 0.7 mL can often achieve better compression effect.25,48 The size of the foramen ovale is also correlated with the balloon pressure, and a narrow foramen ovale is often associated with lower balloon pressure.41,49 Balloon pressure and volume can be used as an auxiliary reference index. Of note, the intraoperative pressure can be recorded to build the pressure model.
The Potential of Personalizing the Operation
Based on a postoperative analysis of the sensory sensitivity of PBC, the decreased sensitivity for perception and pain is most remarkable in the maxillary branch, rather than the mandibular branch.39 For the first trigeminal nerve, eye branch, the postoperative sensory loss is very minor and is also related to the selective compression damage by PBC. This study raises important questions regarding whether the efficacy of surgery is different for trigeminal neuralgia mainly in a certain branch, or whether personalized treatments for pain can be provided in a certain branch. As PBC is a minimally invasive operation using a puncture needle, to avoid excessive intraoperative damage to the abundant craniofacial blood vessels and nerves, the surgical path of PBC adopts the Hartel anterior approach, with the foramen ovale as the intraoperative puncture target, and the mandibular nerve passing through the foramen ovale. According to the therapeutic effect of simple third branch pain by Lu et al,50 the third branch of the trigeminal ganglion has been shown to achieve better pain relief than conventional compression. For patients with simple mandibular nerve symptoms, after a short compression time, the balloon catheter at the mouth of the foramen ovale was filled with 0.1–0.2 mL of contrast media. When the compression ranges from 1–2 minutes, the balloon can present a “dumbbell” or “cylindrical” shape, achieve better pain relief effect, reduce the recurrence rate of pain, and considerably reduce the impact of the first and second branches. First and second branch pain cannot be targeted owing to the anatomical position of the first and second branches in Meckel’s cave. This is because the aforementioned trigeminal ganglion from the three branches of the nerve fiber group gathers separately, thereby corresponding to different nerve fiber groups. The subtle shape difference of the intraoperative balloon does have an impact on the surgical effect; however, there is no relevant research to enable further discussions. Further, if the first balloon compression is not satisfied, the balloon compression can be performed again for these patients.
Future
Owing to the current surgical conditions, the actual performance of PBC is not difficult. However, ensuring that the balloon can perfectly present the “pear” shape in Meckel’s cave is very critical. The shape of the balloon mainly depends on the location of the balloon. A “pear” shaped balloon is standard for patients without anatomical variation. Although the balloon shape is the main indicator of the postoperative effect, the balloon compression time and balloon pressure must also be considered. At present, compression time and balloon pressure mainly rely on the experience of the clinicians, which is not conducive to the scientific management of patients with trigeminal neuralgia. A markedly long compression time will lead to more facial numbness, while a markedly short compression time will easily cause pain relapse. The currently used compression time is 1–3 min. Owing to a lack of standardized compression time for balloon, further studies are required to standardize the compression time and achieve the best compression effect with fewer complications.
Conclusions
PBC has been employed for almost 40 years as a treatment for trigeminal neuralgia. Although PBC has a similar treatment effect to other surgical methods, it is a simple operation, its surgical process can be shortened to 30 minutes, and postoperative pain relief can be estimated based on the shape of the balloon via an X-ray. Although almost all patients have other symptoms, such as facial numbness post-operation, these symptoms do not affect their daily lives. In fact, most patients gradually recover after months. Of note, patients can be discharged 1–2 days after PBC. Accordingly, PBC markedly shortens hospital stay and cost. Further, owing to DSA, CT, and neuronavigation technology, the success rate of PBC is improved and the emergence of complications is reduced. MVD should be considered in forms where vascular conflict is evident or where there is a secondary cause (such as a tumor) visible on MRI. But for elderly patients who are unwilling to undergo craniotomy or relapse after MVD,27,51,52 PBC can be considered as one of the preferred methods used by clinicians for the treatment of primary trigeminal neuralgia.
Disclosure
The authors declare no conflicts of interest.
References
1. Cruccu G, Di Stefano G, Truini A. Trigeminal neuralgia. N Engl J Med. 2020;383(8):754–762. doi:10.1056/NEJMra1914484
2. Maarbjerg S, Di Stefano G, Bendtsen L, Cruccu G. Trigeminal neuralgia - diagnosis and treatment. Cephalalgia. 2017;37(7):648–657. doi:10.1177/0333102416687280
3. Scholz J, Finnerup NB, Attal N, et al. The IASP classification of chronic pain for ICD-11: chronic neuropathic pain. Pain. 2019;160(1):53–59. doi:10.1097/j.pain.0000000000001365
4. Bendtsen L, Zakrzewska JM, Heinskou TB, et al. Advances in diagnosis, classification, pathophysiology, and management of trigeminal neuralgia. Lancet Neurol. 2020;19(9):784–796. doi:10.1016/s1474-4422(20)30233-7
5. Matsushima T, Huynh-Le P, Miyazono M. Trigeminal neuralgia caused by venous compression. Neurosurgery. 2004;55(2):334–7;discussion 338–9. doi:10.1227/01.neu.0000129552.87291.87
6. Maarbjerg S, Wolfram F, Gozalov A, Olesen J, Bendtsen L. Significance of neurovascular contact in classical trigeminal neuralgia. Brain. 2015;138(Pt 2):311–319. doi:10.1093/brain/awu349
7. Devor M, Amir R, Rappaport ZH. Pathophysiology of trigeminal neuralgia: the ignition hypothesis. Clin J Pain. 2002;18(1):4–13. doi:10.1097/00002508-200201000-00002
8. Peker S, Kurtkaya O, Uzün I, Pamir MN. Microanatomy of the central myelin-peripheral myelin transition zone of the trigeminal nerve. Neurosurgery. 2006;59(2):354–9;discussion 354–9. doi:10.1227/01.Neu.0000223501.27220.69
9. Desouza DD, Moayedi M, Chen DQ, Davis KD, Hodaie M. Sensorimotor and pain modulation brain abnormalities in trigeminal neuralgia: a paroxysmal, sensory-triggered neuropathic pain. PLoS One. 2013;8(6):e66340. doi:10.1371/journal.pone.0066340
10. Mullan S, Lichtor T. Percutaneous microcompression of the trigeminal ganglion for trigeminal neuralgia. J Neurosurg. 1983;59(6):1007–1012. doi:10.3171/jns.1983.59.6.1007
11. Jain A, Muneer MS, Okromelidze L, et al. Absence of Meckel cave: a rare cause of trigeminal neuralgia. Am J Neuroradiol. 2021;42(9):1610–1614. doi:10.3174/ajnr.A7205
12. Tsutsumi S, Ono H, Ishii H. Meckel cave: an anatomical study using magnetic resonance imaging. J Comput Assist Tomogr. 2021;45(5):743–748. doi:10.1097/rct.0000000000001185
13. Bathla G, Hegde AN. The trigeminal nerve: an illustrated review of its imaging anatomy and pathology. Clin Radiol. 2013;68(2):203–213. doi:10.1016/j.crad.2012.05.019
14. Messlinger K, Russo AF. Current understanding of trigeminal ganglion structure and function in headache. Cephalalgia. 2019;39(13):1661–1674. doi:10.1177/0333102418786261
15. De Córdoba JL, García Bach M, Isach N, Piles S. Percutaneous balloon compression for trigeminal neuralgia: imaging and technical aspects. Reg Anesth Pain Med. 2015;40(5):616–622. doi:10.1097/aap.0000000000000292
16. Brown JA, Hoeflinger B, Long PB, et al. Axon and ganglion cell injury in rabbits after percutaneous trigeminal balloon compression. Neurosurgery. 1996;38(5):993–1003;discussion 1003–4. doi:10.1097/00006123-199605000-00028
17. Lv W, Hu W, Chi L, Zhang L. Factors that may affect recurrence of trigeminal neuralgia after percutaneous balloon compression. J Clin Neurosci. 2022;99:248–252. doi:10.1016/j.jocn.2022.03.022
18. Buchholz B, Kelly J, Bernatene EA, Méndez Diodati N, Gelpi RJ. Antagonistic and synergistic activation of cardiovascular vagal and sympathetic motor outflows in trigeminal reflexes. Front Neurol. 2017;8:52. doi:10.3389/fneur.2017.00052
19. Schaller B. Trigeminocardiac reflex. A clinical phenomenon or a new physiological entity? J Neurol. 2004;251(6):658–665. doi:10.1007/s00415-004-0458-4
20. Chigurupati K, Vemuri NN, Velivela SR, Mastan SS, Thotakura AK. Topical lidocaine to suppress trigemino-cardiac reflex. Br J Anaesth. 2013;110(1):145. doi:10.1093/bja/aes450
21. Tibano AT, de Siqueira SR, da Nóbrega JC, Teixeira MJ. Cardiovascular response during trigeminal ganglion compression for trigeminal neuralgia according to the use of local anesthetics. Acta Neurochir. 2010;152(8):1347–1351. doi:10.1007/s00701-010-0664-z
22. Li MW, Jiang XF, Niu CS. Efficacy of and risk factors for percutaneous balloon compression for trigeminal neuralgia in elderly patients. Br J Neurosurg. 2021;35(3):280–284. doi:10.1080/02688697.2020.1787341
23. Qin Q, Wang Y. Recurrent trigeminocardiac reflex in percutaneous balloon compression for trigeminal neuralgia: a case report. Medicine. 2020;99(44):e22467. doi:10.1097/md.0000000000022467
24. Asplund P, Blomstedt P, Bergenheim AT. Percutaneous balloon compression vs percutaneous retrogasserian glycerol rhizotomy for the primary treatment of trigeminal neuralgia. Neurosurgery. 2016;78(3):421–8; discussion 428. doi:10.1227/neu.0000000000001059
25. Bergenheim AT, Asplund P, Linderoth B. Percutaneous retrogasserian balloon compression for trigeminal neuralgia: review of critical technical details and outcomes. World Neurosurg. 2013;79(2):359–368. doi:10.1016/j.wneu.2012.03.014
26. Bick SKB, Eskandar EN. Surgical treatment of trigeminal neuralgia. Neurosurg Clin N Am. 2017;28(3):429–438. doi:10.1016/j.nec.2017.02.009
27. Fan X, Xu F, Ren H, et al. The analysis of percutaneous balloon compression on efficacy and negative emotion in the treatment of recurrent trigeminal neuralgia after surgical procedures. Pain Physician. 2021;24(8):E1255–E1262.
28. Chaves JPG, Francisco AN, Trintinalha MO, Carvalho NVP. Trigeminal neuralgia recurrence: a comparison of microvascular decompression and percutaneous balloon compression: a five years follow-up study. Arq Neuropsiquiatr. 2021;79(1):51–55. doi:10.1590/0004-282X-anp-2020-0115
29. Chen JF, Tu PH, Lee ST. Repeated percutaneous balloon compression for recurrent trigeminal neuralgia: a long-term study. World Neurosurg. 2012;77(2):352–356. doi:10.1016/j.wneu.2011.06.013
30. Peris-Celda M, Graziano F, Russo V, Mericle RA, Ulm AJ. Foramen ovale puncture, lesioning accuracy, and avoiding complications: microsurgical anatomy study with clinical implications. J Neurosurg. 2013;119(5):1176–1193. doi:10.3171/2013.1.Jns12743
31. Cheng JS, Lim DA, Chang EF, Barbaro NM. A review of percutaneous treatments for trigeminal neuralgia. Neurosurgery. 2014;10(Suppl 1):25–33; discussion 33. doi:10.1227/neu.00000000000001687
32. Berra LV, Armocida D, Pesce A, Di Rita A, Santoro A. Herpes simplex reactivation after surgical treatment of trigeminal neuralgia: a retrospective cohort study. World Neurosurg. 2019;127:e16–e21. doi:10.1016/j.wneu.2019.01.226
33. Martínez Moreno NE, Gutiérrez-Sárraga J, Rey-Portolés G, Jiménez-Huete A, Martínez Álvarez R. Long-term outcomes in the treatment of classical trigeminal neuralgia by gamma knife radiosurgery: a retrospective study in patients with minimum 2-year follow-up. Neurosurgery. 2016;79(6):879–888. doi:10.1227/neu.0000000000001404
34. Xiao X, Wei Z, Ren H, Sun H, Luo F. Comparison of effectiveness and safety between intraoperative 3D-CT-guided and C-arm-guided percutaneous balloon compression for idiopathic trigeminal neuralgia: a multi-center retrospective study. Pain Res Manag. 2021;2021:9306532. doi:10.1155/2021/9306532
35. Liu Q, Wang J, Wang C, et al. Robot-assisted percutaneous balloon compression for trigeminal neuralgia: technique description and short-term clinical results. Front Surg. 2022;9:869223. doi:10.3389/fsurg.2022.869223
36. Aydoseli A, Akcakaya MO, Aras Y, et al. Neuronavigation-assisted percutaneous balloon compression for the treatment of trigeminal neuralgia: the technique and short-term clinical results. Br J Neurosurg. 2015;29(4):552–558. doi:10.3109/02688697.2015.1019418
37. Huo X, Sun X, Zhang Z, Guo W, Guan N, Luo J. Dyna-CT-assisted percutaneous microballoon compression for trigeminal neuralgia. J Neurointerv Surg. 2014;6(7):521–526. doi:10.1136/neurintsurg-2013-010676
38. Wiggins A, Lonie M, Pimentil I, Newall N, Bodkin P, Venkatesh A. Electromagnetic neuronavigation for the percutaneous treatment of trigeminal neuralgia with balloon compression: technical note and cadaveric validation study. Acta Neurochir. 2018;160(7):1337–1341. doi:10.1007/s00701-018-3548-2
39. Asplund P, Linderoth B, Bergenheim AT. The predictive power of balloon shape and change of sensory functions on outcome of percutaneous balloon compression for trigeminal neuralgia. J Neurosurg. 2010;113(3):498–507. doi:10.3171/2010.2.Jns091466
40. Li Y, Zhang XA, Qi S. Anatomic characteristics of the dural sheath of the trigeminal nerve. Head Neck. 2016;38(Suppl 1):E185–8. doi:10.1002/hed.23968
41. Sun C, Zheng W, Zhu Q, Du Q, Yu W. The transformation of the balloon shape in percutaneous balloon compression for trigeminal neuralgia. J Pain Res. 2021;14:3805–3814. doi:10.2147/jpr.S343783
42. Urculo E, Alfaro R, Arrazola M, Astudillo E, Rejas G. Trochlear nerve palsy after repeated percutaneous balloon compression for recurrent trigeminal neuralgia: case report and pathogenic considerations. Neurosurgery. 2004;54(2):505–8;discussion 508–9. doi:10.1227/01.neu.0000103675.32713.a9
43. Brown JA, Pilitsis JG. Percutaneous balloon compression for the treatment of trigeminal neuralgia: results in 56 patients based on balloon compression pressure monitoring. Neurosurg Focus. 2005;18(5):E10. doi:10.3171/foc.2005.18.5.11
44. Li F, Han S, Ma Y, Yi F, Xu X, Liu Y. Optimal duration of percutaneous microballoon compression for treatment of trigeminal nerve injury. Neural Regen Res. 2014;9(2):179–189. doi:10.4103/1673-5374.125347
45. Kouzounias K, Schechtmann G, Lind G, Winter J, Linderoth B. Factors that influence outcome of percutaneous balloon compression in the treatment of trigeminal neuralgia. Neurosurgery. 2010;67(4):925–34; discussion 934. doi:10.1227/NEU.0b013e3181eb5230
46. Xu W, Jiang C, Yu C, Liang W. Percutaneous balloon compression for persistent or recurrent trigeminal neuralgia after microvascular decompression: personal experience of 28 patients. Acta Neurol Belg. 2018;118(4):561–566. doi:10.1007/s13760-017-0858-8
47. Wilkinson HA. Percutaneous trigeminal ganglion balloon compression for treatment of trigeminal neuralgia–part I: pressure recordings. Surg Neurol. 2003;60(5):470. doi:10.1016/s0090-3019(03)00514-7
48. Wang H, Chen C, Chen D, et al. Clinical analysis of the treatment of primary trigeminal neuralgia by percutaneous balloon compression. Front Surg. 2022;9:843982. doi:10.3389/fsurg.2022.843982
49. Wang Q, Chen C, Guo G, Li Z, Huang D, Zhou H. A prospective study to examine the association of the foramen ovale size with intraluminal pressure of pear-shaped balloon in percutaneous balloon compression for trigeminal neuralgia. Pain Ther. 2021;10(2):1439–1450. doi:10.1007/s40122-021-00311-7
50. Lu Z, Wang J, Cao Y, et al. Treatment of third branch trigeminal neuralgia with a balloon inflated in the foramen ovale. Front Neurol. 2022;13:826653. doi:10.3389/fneur.2022.826653
51. Ni H, Wang Y, Chen X, Gu W. Outcomes of treatment for elderly patients with trigeminal neuralgia: percutaneous balloon compression versus microvascular decompression. J Craniofac Surg. 2020;31(7):e685–e688. doi:10.1097/scs.0000000000006544
52. Berra LV, Armocida D, Mastino L, et al. Trigeminal neuralgia secondary to intracranial neoplastic lesions: a case series and comprehensive review. J Neurol Surg A Cent Eur Neurosurg. 2021;82(2):118–124. doi:10.1055/s-0040-1718708
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Consistency Between the Preoperative 3D-Reconstructed Meckel’s Cave and the Intraoperative Balloon Results in Percutaneous Balloon Compression
Cheng R, Wang T, Cai Y, Chai S, Shen L, Xu D, Yang J, Yue C, Pu J, Xiong N
Journal of Pain Research 2023, 16:2929-2937
Published Date: 28 August 2023