Back to Journals » Infection and Drug Resistance » Volume 15
The First Case Report of Community-Acquired Infective Endocarditis Due to Sequence Type 1223 Staphylococcus argenteus Complicated with Convexity Subarachnoid Hemorrhage
Authors Hirai J ![]() , Suzuki H, Sakanashi D, Kuge Y, Kishino T, Asai N, Hagihara M, Mikamo H
, Suzuki H, Sakanashi D, Kuge Y, Kishino T, Asai N, Hagihara M, Mikamo H
Received 9 May 2022
Accepted for publication 15 August 2022
Published 29 August 2022 Volume 2022:15 Pages 4963—4970
DOI https://doi.org/10.2147/IDR.S373352
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Jun Hirai,1,2 Hiroyuki Suzuki,3 Daisuke Sakanashi,2 Yuji Kuge,4 Takaaki Kishino,4 Nobuhiro Asai,1,2 Mao Hagihara,5 Hiroshige Mikamo1,2
1Department of Clinical Infectious Diseases, Aichi Medical University Hospital, Nagakute, Aichi, Japan; 2Department of Infection Control and Prevention, Aichi Medical University Hospital, Nagakute, Aichi, Japan; 3Department of Neurology, Aichi Medical University, Nagakute, Aichi, Japan; 4Department of Emergency and Critical Care Medicine, Aichi Medical University Hospital, Nagakute, Aichi, Japan; 5Department of Molecular Epidemiology and Biomedical Sciences, Aichi Medical University, Nagakute, Aichi, Japan
Correspondence: Jun Hirai, Department of Clinical Infectious Diseases, Aichi Medical University Hospital, 1-1, Yazako-karimata, Nagakute, Aichi, 480-1195, Japan, Tel +81-561-62-3311, Fax +81-561-76-2673, Email [email protected]
Abstract: Staphylococcus argenteus is a new species classified as part of the Staphylococcus aureus-related complex in 2015 and has been recognized to be as pathogenic as S. aureus. We describe the first case of endocarditis caused by S. argenteus. A 51-year-old man presented with chief complaints of fever and headaches. On admission, he showed a slight decrease in consciousness level (Glasgow Coma Scale, E4V4M6). Careful physical examination and imaging revealed a systolic heart murmur, Janeway lesions, and complicating convexity subarachnoid hemorrhage (cSAH) of the left frontal lobe. Ceftriaxone 4 g/day was administered immediately after blood cultures were obtained. The next day, all blood cultures grew Gram-positive cocci, identified as Staphylococcus aureus or Staphylococcus argenteus by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS). However, the version of MALDI-TOF MS used could not distinguish these bacteria. Although we could not find valvular vegetation, he was clinically diagnosed with infective endocarditis according to the modified Duke’s criteria. Meropenem 6 g/day and linezolid 1.2 g/day were started to cover S. aureus and methicillin-resistant S. aureus. Finally, ampicillin was selected based on drug susceptibility, and the patient was treated for 8 weeks and recovered without permanent damage. The isolated strain formed white colonies on blood agar plates, characteristic of S. argenteus, and differs from golden colony-forming S. aureus. Genetic analysis revealed the isolated strain as S. argenteus (sequence type 1223). Although distinguishing S. argenteus from S. aureus using routine conventional laboratory tests is difficult, the updated library version of MALDI-TOF MS is useful in identifying S. argenteus. Interestingly, all published cases of infection caused by ST1223 have been reported in Japan. Therefore, the trend of infections from the ST1223 strain should be carefully monitored, particularly in Japan. Further investigation is needed to clarify the epidemiology and clinical characteristics of S. argenteus infection, as there are few studies regarding this pathogen.
Keywords: Staphylococcus argenteus, sequence type 1223, infective endocarditis, convexity subarachnoid hemorrhage, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry, Japan
Introduction
Staphylococcus argenteus, formerly known as Staphylococcus aureus clonal complex 75, is a novel coagulase-positive staphylococcal species that belongs to S. aureus-related complex, which also includes Staphylococcus schweitzeri.1 Although previous studies reported that the detection rate of S. argenteus was very low among S. aureus strains isolated from clinical specimens (Thailand 4–5%, Japan 1%, Europe <1%),2–5 reports of invasive infections caused by S. argenteus have been increasing worldwide, including Japan, since the bacterium was identified as a new species within the S. aureus-related complex in 2015.5–9
One of the problems regarding this species is that it is very closely related to S. aureus; therefore, it is difficult to distinguish S. argenteus from S. aureus by conventional diagnostic microbiology identification methods in most common clinical laboratories.10 Recently, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) has become a useful tool for microbial identification in clinical diagnostic microbiology.11 A recent study evaluated the utility of MALDI-TOF MS for accurate identification of this novel bacterium and revealed that MALDI-TOF MS can reliably distinguish S. argenteus from S. aureus if available in an updated version.12
Notably, a prospective multicenter observational study (including 58 patients with S. argenteus and 253 with S. aureus sepsis, respectively) revealed that S. argenteus caused a similar rate of shock (6.9% vs 12.3%, p = 0.18) and 28-day mortality (6.9% vs 8.7%, p = 0.72) compared to S. aureus.13 The European Society of Clinical Microbiology and Infectious Disease recommends that a clinical laboratory technician should inform the attending physicians that this new pathogen is highly pathogenic, similar to S. aureus.1
Here, we describe the first case of infective endocarditis (IE) caused by S. argenteus in a previously healthy Japanese man. In this case, analysis by polymerase chain reaction (PCR) amplification of the non-ribosomal peptide synthetase (NRPS) gene was required to correctly identify the causative pathogen, in addition to MALDI-TOS MS analysis. Written informed consent was obtained from the patient described here for the publication of this case report and accompanying images. S. argenteus was confirmed by nrps gene PCR.
Case Report
A 51-year-old, right-handed man presented to the emergency room complaining of headache, difficulty speaking clearly, and a mild decrease in consciousness level that developed 2 h before admission. He also had a 2-day history of fever. He had no comorbidities and was not taking any medication. He also underwent regular annual checkups and never showed abnormalities in heart sounds or urine tests. Further, he had no history of heart disease or dermatological diseases, such as atopic dermatitis, recent head or body trauma, drug user, or acupuncture. Upon admission, a slight decrease in consciousness level was observed (Glasgow Coma Scale, E4V4M6). His body temperature was 38.0 °C, and physical examination revealed drooping left corner of the mouth and abduction of the eye. Neck rigidity and jolt accentuation were not present. Blood tests showed an elevated neutrophil cell count (7900 cells/μL; neutrophil 85.1%) and C-reactive protein (23.0 mg/dL). Urine tests revealed occult blood of 5–9 RBCs/HPF and urinary protein level of 30 mg/dL. Although he had no risk factors for stroke, contrast-enhanced computed tomography (CT) revealed cortical convexity subarachnoid hemorrhages (cSAH) of the left frontal lobe, in addition to multiple subcortical hemorrhages in the right frontal lobe and left occipital lobe (Figure 1A and B). Magnetic resonance imaging (MRI) on T2 fluid-attenuated inversion recovery (FLAIR) revealed hemorrhage in the left frontal lobe gyrus (Figure 1C). Diffusion MRI also revealed acute brain infarction in the right cerebellar hemisphere (Figure 1D). Magnetic resonance angiography revealed no evidence of cerebrovascular malformations, such as aneurysm or obstruction. In the search of the etiology of multiple hemorrhages and infarction in the brain, repeated thorough physical examinations revealed a heart murmur in the mitral valve area and non-tender erythematous macules on the palms, fingers, toes, and soles recognized as Janeway lesions (Figure 2). Based on these findings, the patient was strongly suspected to have acute IE. Immediately, an attending physician ordered three sets of blood cultures and started intravenous ceftriaxone (CRO) 4 g/day.
 |
Figure 1 Contrast-enhanced CT and MRI of the head on admission. Black arrow indicates cortical convexity subarachnoid hemorrhages of the left frontal lobe (A), multiple subcortical hemorrhages are also observed (B), MRI on T2 FLAIR reveals a hemorrhage (white arrow) in the left frontal lobe gyrus (C), and diffusion-weighted MRI also reveals acute brain infarction (white arrowhead) in the right cerebellar hemisphere (D). |
 |
Figure 2 Black arrowheads indicated Janeway lesions in the present case. |
The next day, all aerobic and anaerobic samples showed Gram-positive bacterial growth, which appeared as grape-like clusters under a microscope. MALDI-TOF MS (MALDI Biotyper ver. 9.0.0.0; Bruker Daltonics, Billerica, MA, USA) confirmed this microorganism to be S. aureus or S. argenteus with spectral scores of 1.999 and 1.987, respectively (this version of MALDI-TOF MS could not distinguish between S. aureus and S. argenteus). The antimicrobial stewardship team commented that the patient might have had a central nervous system infection based on his slightly decreased consciousness level in addition to fever and headache, although a lumbar puncture for identifying complicating meningitis could not be performed due to cerebral hemorrhage. Usually, cerebrospinal fluid has poor drug transferability, and higher doses are considered desirable. Therefore, the administration of meropenem (MEM) 6 g/day was recommended instead of CRO because the usual dose of MEM for cerebral infection is higher than that of CRO (although oxacillin and nafcillin are the standard therapeutic antibiotics used globally against methicillin-susceptible S. aureus infections, including meningitis, as anti-staphylococcal penicillin, these drugs are not approved in Japan). Linezolid (LZD) 1.2 g/day was also added considering the possible involvement of methicillin-resistant S. aureus meningitis. Additionally, the nasal swab specimen was cultured to detect Staphylococcus spp., and the result was negative (we did not screen the sample for throat carriage). Transthoracic echocardiography (TTE) revealed only mitral valve regurgitation. Although both TTE and transesophageal echocardiography could not detect valvular vegetations, the condition was diagnosed as IE based on the modified Duke’s criteria.14 The patient had met two major criteria (persistently positive blood cultures, defined as the first and last sample drawn 1 h apart, and emergence of cardiac murmur) in addition to three minor criteria (fever >38°C, evidence of vascular phenomena; Janeway lesions and intracranial hemorrhage, and findings suggestive of glomerulonephritis, hematuria, and proteinuria). Additional imaging tests, such as CT and MRI, revealed that metastatic infections, such as vertebral osteomyelitis, liver abscess, and iliopsoas abscess, were not complicated. An ophthalmologist also revealed that the patient did not have endophthalmitis.
The patient’s consciousness level was restored on the 2nd day of hospitalization. Headache and speaking difficulty also disappeared on day 4 after starting treatment. Blood cultures obtained on day 5 after hospitalization were sterile. He became afebrile from the 6th day of hospitalization, and MEM and LZD were switched to ampicillin (AMP) 12 g/day based on the drug susceptibility of the isolated strain (Table 1). Antimicrobial susceptibility testing was performed using VITEK-2 antibiotic susceptibility cards for Gram-positive microbes (AST P625 TEST KIT) on the VITEK-2 system (bio-Mérieux, Marcy-l’Étoile, France). He received 4 weeks of intravenous AMP, recovered without sequelae, and was discharged from our hospital on day 35 with oral ampicillin for two more weeks. We did not conduct follow-up imaging tests, such as brain CT, because his headache and neurological symptoms had clearly improved promptly after administrating antibiotics. The patient had no fever, nor was elevation of white blood cells or C-reactive protein observed for 2 months after therapy during his regular clinical visit.
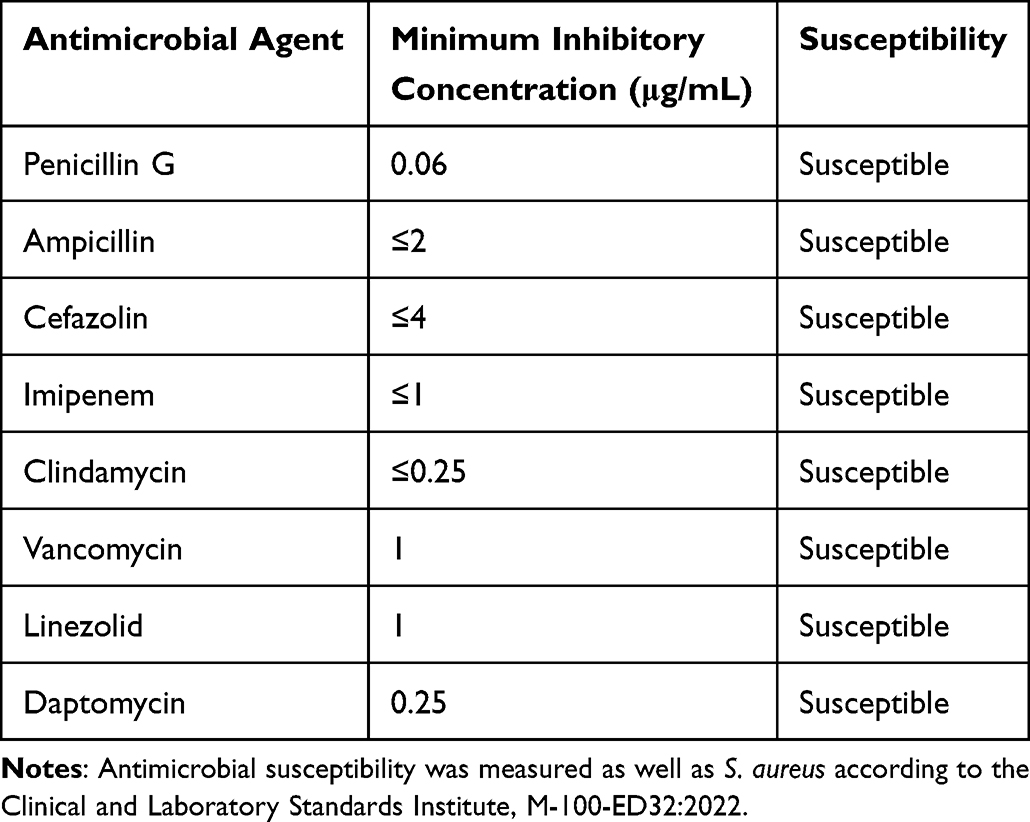 |
Table 1 Antimicrobial Susceptibility of S. argenteus Isolated in the Present Case |
We conducted an additional microbiological examination to identify the isolated strain. Finally, the isolated strain from the blood cultures was confirmed as S. argenteus by NRPS gene PCR; the used primers were nrps-F (TTGARWCGACATTACCAGT) and nrps-R (ATWRCRTACATYTCRTTATC), as reported by Zhang et al.15 In addition, the isolated strain formed white (non-pigmented) colonies on mannitol salt agar (Becton, Dickinson and Company) incubated at 35°C in ambient air for 48 h (Figure 3A), which is characteristic of S. argenteus, as S. aureus forms gold-colored colonies (Figure 3B). To identify the sequence type (ST) of the isolated strain, we used the following primer sets: aroE-5F (AATTGCAGTTATMGGWARTCCW), aroE-742R (TCCAWATTTTAAARCTTTCMGCACC), glp-34F (GCAATCTTAATCCTTTTTGGTGG), and glp-743R (GCAATTGCACAACCAATATTAAA) based on previous research.16 Ultimately, the causative pathogen was classified as belonging to ST1223 of S. argenteus.
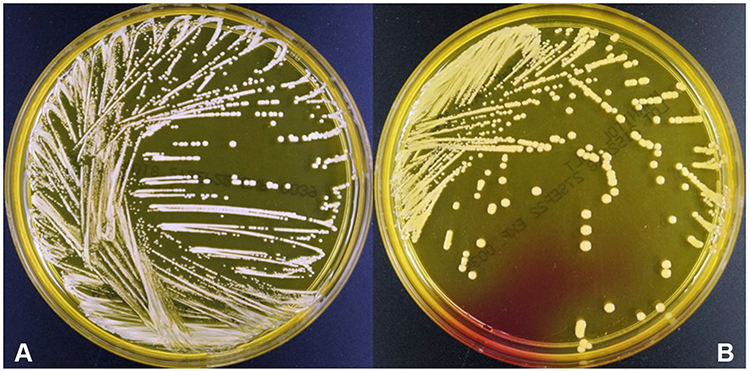 |
Figure 3 Colonies of S. argenteus (A) and S. aureus (B) on Mannitol Salt Agar (Becton, Dickinson and Company). |
Discussion
We encountered a case of severe IE caused by S. argenteus that was complicated by cSAH and multiple brain infarctions. We screened whether the patient had colonization of S. argenteus in the nasal cavity, since the carriage of S. aureus is a risk factor for S. aureus infection.17 However, S. argenteus was not cultured from the nasal swab specimen in the present patient. Besides, we should have screened the throat for S. argenteus based on a previous study, which clarified that S. aureus was more likely to be found in the throat than in the nose.18 In addition, the patient had no history of atopic dermatitis, skin or soft tissue infection, or recent trauma. In the present case, we were unable to detect the site of bacterial entry.
Previously, S. argenteus was considered less virulent than S. aureus because of a lack of staphyloxanthin that works as an antioxidant agent against reactive oxygen species produced by the infected host immune mechanism, inducing evasion from the protective system.19 However, including the present case, many fatal infectious cases caused by S. argenteus have been reported in both community and hospital-acquired situations worldwide.2–5 Chen et al reported that the mortality related to bacteremia due to S. argenteus was higher than that due to S. aureus using multivariate analysis [adjusted hazard ratio = 1.845, 95% confidence interval 1.033–3.294].20 Therefore, when encountering a patient with S. argenteus infection, clinicians should follow the clinical course carefully, considering this pathogen causes invasive infection similar to S. aureus.
Notably, the condition of the patient in the present case was complicated by cSAH. Although the specific mechanism by which IE causes cSAH is not well understood, several previous studies have revealed that cSAH is associated with IE.21–23 In a retrospective study including 240 IE patients, Boukobza et al reported 31 IE cases (13%) with complicated cSAH that frequently occurred in middle-aged patients. They also reported that the majority of causative pathogens were Streptococcus spp. and Staphylococcus spp. (48.4% and 35.5%, respectively), indicating that IE due to Staphylococcus spp. is a risk factor for cSAH. Similar to our case, cSAH occurred mainly in the frontal, parietal, and temporal lobes, mostly in the unilateral sulcus, and more than half of the patients had complicated microinfarcts in addition to cSAH. The prognosis for IE patients with cSAH is relatively favorable, and recurrence of cSAH was not experienced in a previous retrospective study.22 As shown in the present case, physicians should suspect IE when complicated by cSAH, particularly multifocal ischemic lesions in non-traumatic patients with fever.
As mentioned earlier, it is difficult to distinguish S. argenteus from S. aureus using conventional methods, such as automated biochemical tests. The typical color of S. argenteus colonies is creamy white (Figure 3A), but S. aureus sometimes has a similar colony appearance.24 Even 16S rRNA gene sequencing, which provides species-specific signatures for useful identification of bacteria, fails to identify S. argenteus.25,26 Recently, MALDI-TOF MS was shown to be useful in clearly differentiating S. argenteus from S. aureus using the updated MALDI database, which contains additional spectral profiles of S. argenteus.12,24 Therefore, it is recommended to use the latest MALDI-TOF MS whenever possible to identify S. argenteus.
ST2250 of S. argenteus is the most frequently isolated clone worldwide,1 and many invasive clinical cases, such as aortic mycotic aneurysm, purulent lymphadenitis, infection of the prosthetic joint, bacteremia, and catheter-related bloodstream infection, caused by ST2250 have been reported.5,8,9,27,28 Although ST1223 is also one of the major clinically isolated strains, infectious cases due to S. argenteus ST1223 are scarce. Our search of PubMed revealed that ST1223 has been reported as the causative agent of keratoconjunctivitis and food poisoning outbreaks, and all studies were reported in Japan.29–31 Aung et al also reported that 24% of the genotype of ST1223 among 82 S.argenteus clinical specimens were mainly isolated from sputum, pharynx, stool, and urine samples in Japan.26 Therefore, compared to other countries, Japan may have a unique molecular epidemiology in that ST1223 is the major strain causing invasive infection among S. argenteus strains.
This case report has some limitations. First, we could not identify the primary source of S. argenteus infection based on clinical history and physical examinations. Second, although this is the first report of IE caused by S. argenteus, we could not explain why S. argenteus caused IE in this case. To date, few studies regarding risk factors for invasive infections due to S. argenteus have been reported. Further investigation is needed to elucidate the epidemiology and clinical features, including what kinds of infections are more likely, and the ST of invasive infections due to S. argenteus.
Conclusion
We report a case of IE caused by S. argenteus. Physicians should be aware of this new strain that causes severe infections and has higher mortality than S. aureus, although it is difficult to identify S. argenteus by routine conventional tests and the old version of MALDI-TOF MS. Additionally, clinicians need to consider the possibility of IE when encountering cSAH in a febrile patient, as described in this case. More cumulative cases are required to clarify the clinical features of S. argenteus infection.
Abbreviations
MALDI-TOF MS, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry; IE, infective endocarditis; CT, computed tomography; cSAH, convexity subarachnoid hemorrhage; MRI, magnetic resonance image; FLAIR, fluid-attenuated inversion recovery; DWI, diffusion-weighted imaging; CRO, ceftriaxone; MEM, meropenem; LZD, linezolid; TTE, transesophageal echocardiography; AMP, ampicillin; NRPS, non-ribosomal peptide synthetase; ST, sequence type.
Data Sharing Statement
The data is available upon reasonable request to the corresponding author.
Ethics and Consent
The patient was informed of the publication of this case report and signed a letter of consent. The ethics committee of our institution approved the waiver in this case report, based on the Japanese ethical guidelines for clinical research to publish the case details.
Acknowledgments
We appreciate Editage (www.editage.com) for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors and co-workers did not receive any specific funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Becker K, Schaumburg F, Kearns A, et al. Implications of identifying the recently defined members of the Staphylococcus aureus complex S. argenteus and S. schweitzeri: a position paper of members of the ESCMID Study Group for Staphylococci and Staphylococcal Diseases (ESGS). Clin Microbiol Infect. 2019;25(9):1064–1070. doi:10.1016/j.cmi.2019.02.028
2. Thaipadungpanit J, Amornchai P, Nickerson EK, et al. Clinical and molecular epidemiology of Staphylococcus argenteus infections in Thailand. J Clin Microbiol. 2015;53(3):1005–1008. doi:10.1128/JCM.03049-14
3. Argudín MA, Dodémont M, Vandendriessche S, et al. Low occurrence of the new species Staphylococcus argenteus in a Staphylococcus aureus collection of human isolates from Belgium. Eur J Clin Microbiol Infect Dis. 2016;35(6):1017–1022. doi:10.1007/s10096-016-2632-x
4. Tång Hallbäck E, Karami N, Adlerberth I, et al. Methicillin-resistant Staphylococcus argenteus misidentified as methicillin-resistant Staphylococcus aureus emerging in western Sweden. J Med Microbiol. 2018;67(7):968–971. doi:10.1099/jmm.0.000760
5. Kitagawa H, Ohge H, Hisatsune J, et al. Low incidence of Staphylococcus argenteus bacteremia in Hiroshima, Japan. J Infect Chemother. 2020;26(1):140–143. doi:10.1016/j.jiac.2019.07.011
6. Jiang B, You B, Tan L, et al. Clinical Staphylococcus argenteus develops to small colony variants to promote persistent infection. Front Microbiol. 2018;9:1347. doi:10.3389/fmicb.2018.01347
7. Bogut A, Niedźwiadek J, Kozioł-Montewka M, et al. Characterization of Staphylococcus epidermidis and Staphylococcus warneri small-colony variants associated with prosthetic-joint infections. J Med Microbiol. 2014;63(Pt 2):176–185. doi:10.1099/jmm.0.066068-0
8. Diot A, Dyon-Tafani V, Bergot M, et al. Investigation of a Staphylococcus argenteus strain involved in a chronic prosthetic-joint infection. Int J Mol Sci. 2020;21(17):6245. doi:10.3390/ijms21176245
9. Mitsutake K, Watanabe N, Karaushi H, et al. Thoracic aortic mycotic aneurysm due to Staphylococcus argenteus: a case report. J Infect Chemother. 2020;26(11):1213–1215. doi:10.1016/j.jiac.2020.05.003
10. Kaden R, Engstrand L, Rautelin H, Johansson C. Which methods are appropriate for the detection of Staphylococcus argenteus and is it worthwhile to distinguish S. argenteus from S. aureus? Infect Drug Resist. 2018;11:2335–2344. doi:10.2147/IDR.S179390
11. Tsuchida S, Umemura H, Nakayama T. Current status of matrix-assisted laser desorption/ionization-time-of-flight mass spectrometry (MALDI-TOF MS) in clinical diagnostic microbiology. Molecules. 2020;25(20):4775. doi:10.3390/molecules25204775
12. Chen SY, Lee H, Teng SH, et al. Accurate differentiation of novel Staphylococcus argenteus from Staphylococcus aureus using MALDI-TOF MS. Future Microbiol. 2018;13:997–1006. doi:10.2217/fmb-2018-0015
13. Chantratita N, Wikraiphat C, Tandhavanant S, et al. Comparison of community-onset Staphylococcus argenteus and Staphylococcus aureus sepsis in Thailand: a prospective multicentre observational study. Clin Microbiol Infect. 2016;22(5):
14. Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. 2000;30(4):633–638. doi:10.1086/313753
15. Zhang DF, Xu X, Song Q, et al. Identification of Staphylococcus argenteus in Eastern China based on a nonribosomal peptide synthetase (NRPS) gene. Future Microbiol. 2016;11:1113–1121. doi:10.2217/fmb-2016-0017
16. Moradigaravand D, Jamrozy D, Mostowy R, et al. Evolution of the Staphylococcus argenteus ST2250 clone in Northeastern Thailand is linked with the acquisition of livestock-associated Staphylococcal genes. mBio. 2017;8(4):e00802–17. doi:10.1128/mBio.00802-17
17. Safdar N, Bradley EA. The risk of infection after nasal colonization with Staphylococcus aureus. Am J Med. 2008;121(4):310–315. doi:10.1016/j.amjmed.2007.07.034
18. Hamdan-Partida A, Sainz-Espuñes T, Bustos-Martínez J. Characterization and persistence of Staphylococcus aureus strains isolated from the anterior nares and throats of healthy carriers in a Mexican community. J Clin Microbiol. 2010;48(5):1701–1705. doi:10.1128/JCM.01929-09
19. Tong SY, Sharma-Kuinkel BK, Thaden JT, et al. Virulence of endemic nonpigmented northern Australian Staphylococcus aureus clone (clonal complex 75, S. argenteus) is not augmented by staphyloxanthin. J Infect Dis. 2013;208(3):520–527. doi:10.1093/infdis/jit173
20. Chen SY, Lee H, Wang XM, et al. High mortality impact of Staphylococcus argenteus on patients with community-onset staphylococcal bacteraemia. Int J Antimicrob Agents. 2018;52(6):747–753. doi:10.1016/j.ijantimicag.2018.08.017
21. Khan F, Sharma N, Ud Din M, Shirke S, Abbas S. Convexal subarachnoid hemorrhage caused by infective endocarditis in a patient with advanced human immunodeficiency virus (HIV): the culprits and bystanders. Am J Case Rep. 2021;22:e931376. doi:10.12659/AJCR.931376
22. Boukobza M, Ilic-Habensus E, Duval X, Laissy JP. Acute convexity subarachnoid hemorrhage (cSAH) in infectious endocarditis (IE): imaging features and follow-up. J Neurol. 2020;267(10):2971–2982. doi:10.1007/s00415-020-09953-7
23. Dakay K, Mahta A, Rao S, et al. Yield of diagnostic imaging in atraumatic convexity subarachnoid hemorrhage. J Neurointerv Surg. 2019;11(12):1222–1226. doi:10.1136/neurintsurg-2019-014781
24. Schuster D, Rickmeyer J, Gajdiss M, et al. Differentiation of Staphylococcus argenteus (formerly: staphylococcus aureus clonal complex 75) by mass spectrometry from S. aureus using the first strain isolated from a wild African great ape. Int J Med Microbiol. 2017;307(1):57–63. doi:10.1016/j.ijmm.2016.11.003
25. Eshaghi A, Bommersbach C, Zittermann S, et al. Phenotypic and genomic profiling of Staphylococcus argenteus in Canada and the United States and recommendations for clinical result reporting. J Clin Microbiol. 2021;59(6):e02470–20. doi:10.1128/JCM.02470-20
26. Aung MS, Urushibara N, Kawaguchiya M, et al. Molecular epidemiological characterization of Staphylococcus argenteus clinical isolates in Japan: identification of three clones (ST1223, ST2198, and ST2550) and a novel Staphylocoagulase genotype XV. Microorganisms. 2019;7(10):389. doi:10.3390/microorganisms7100389
27. Ohnishi T, Shinjoh M, Ohara H, et al. Purulent lymphadenitis caused by Staphylococcus argenteus, representing the first Japanese case of Staphylococcus argenteus (multilocus sequence type 2250) infection in a 12-year-old boy. J Infect Chemother. 2018;24(11):925–927. doi:10.1016/j.jiac.2018.03.018
28. Söderquist B, Wildeman P, Stenmark B, Stegger M. Staphylococcus argenteus as an etiological agent of prosthetic Hip joint infection: a case presentation. J Bone Jt Infect. 2020;5(4):172–175. doi:10.7150/jbji.44848
29. Yamada K, Sasaki M, Imai W, et al. Bacterial keratoconjunctivitis caused by Staphylococcus argenteus belonging to sequence type 1223 isolated in Japan. J Infect Chemother. 2020;26(9):1002–1004. doi:10.1016/j.jiac.2020.04.026
30. Suzuki Y, Kubota H, Ono HK, et al. Food poisoning outbreak in Tokyo, Japan caused by Staphylococcus argenteus. Int J Food Microbiol. 2017;262:31–37. doi:10.1016/j.ijfoodmicro.2017.09.005
31. Wakabayashi Y, Umeda K, Yonogi S, et al. Staphylococcal food poisoning caused by Staphylococcus argenteus harboring staphylococcal enterotoxin genes. Int J Food Microbiol. 2018;265:23–29. doi:10.1016/j.ijfoodmicro.2017.10.022
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.