Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Experiences of Nursing Managers in Implementing Palliative Care in Long-Term Care Facilities
Authors Chiang SW ![]() , Lu SF
, Lu SF ![]() , Wu SC
, Wu SC ![]() , Peng TC
, Peng TC ![]()
Received 28 September 2023
Accepted for publication 4 December 2023
Published 15 December 2023 Volume 2023:16 Pages 4053—4070
DOI https://doi.org/10.2147/JMDH.S442467
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Shu-Wan Chiang, Shiou-Fang Lu, Shu-Chen Wu, Tai-Chu Peng
Department of Nursing, Tzu Chi University, Hualien, Taiwan
Correspondence: Tai-Chu Peng, Department of Nursing, Tzu Chi University, Hualien, Taiwan, Email [email protected]
Purpose: The purpose of this study was to explore the experiences of nursing managers in implementing palliative care in long-term care facilities and to provide recommendations for managers who plan to introduce palliative care into their facilities.
Methods: This study used semi-structured interviews and grounded theory methodology, with purposive sampling. A total of 11 long-term care facilities in eastern Taiwan that had implemented palliative care were selected, and 11 facility nursing managers participated in in-depth, face-to-face interviews.
Results: The introduction of palliative care in long-term care facilities can be divided into four stages: (1) the opportunity for change, (2) playing a supportive role, (3) a new collaboration model, and (4) facility transformation. The core category shared by the participants may be summed up as “the palliative care captain in the facility”. It reflects the spirit of the successful implementation of palliative care by managers in long-term care facilities.
Conclusion: The study reveals that during the initial phases of implementing palliative care, the palliative care teams assume a crucial leadership role, while the facilities play a supportive role. At this stage, managers should focus on personnel training and addressing internal issues within the facilities to facilitate successful collaboration with the palliative care teams. In the later stages, the facilities transition from a supportive role to one of independence, marking a critical juncture for the facilities’ potential stable development. During this period, managers are tasked not only with establishing the facilities’ own palliative care team but also with facilitating the transformation of staff from learners to instructors. Finally, even after successful implementation, managers must contemplate how to innovate and set more ambitious goals.
Keywords: nursing managers, long-term care, palliative care, hospice, grounded theory
Introduction
In Taiwan, as in other countries, the issue of an aging population is prevalent. This phenomenon has led to long-term care facilities often becoming the places where elderly individuals with chronic illnesses and dementia spend their final stages of life.1–4 Residents in these long-term care facilities typically suffer from various life-threatening diseases, leading to diverse palliative care needs. Palliative care, distinct from general medical treatment, considers death as a normal process. The goal of such care is not to hasten or prolong life but to enhance the quality of life by providing relief from residents’ suffering until death occurs.5 In Taiwan, palliative care primarily operates under two main models: the “Hospital Care Model” and the “Community Care Model”. The former involves specialized palliative care teams operating within hospital environments, with a focus on hospice care wards or collaboration with general medical teams to provide integrated care for patients in regular wards. In contrast, the latter is carried out by hospital and clinic-based palliative care teams, delivering care services to long-term care facilities or residents’ homes.6 The division of service responsibilities entails hospital teams covering urban areas, while clinic teams handle rural regions.7
In recent years, the government has actively promoted the development of community palliative care to reduce the excessive concentration of palliative care services in hospitals.8 Despite these efforts, the current distribution remains skewed, with the “Hospital Care Model” dominating at 83%, leaving the “Community Care Model” at only 17%.9 This imbalance in resource allocation results in a scarcity of beds in hospital hospice wards. The overwhelming workload for palliative care teams leads to challenges when residents in facilities require such services, as the teams may be understaffed. Additionally, restrictions imposed by national health insurance on service frequency and payment amounts further complicate the delivery of palliative care to institutional residents. Consequently, when residents in facilities face acute issues such as respiratory distress or low blood pressure, and palliative care teams cannot respond promptly, facility nursing staff tend to transport residents to hospitals for emergency treatment.10 This results in the excessive use of aggressive medical interventions (such as defibrillators and vasoactive drugs) and life-sustaining treatments (such as mechanical ventilation, intubation, and extracorporeal membrane oxygenation). Not only are these treatments typically ineffective from a medical perspective, leading to increased medical burdens and wasteful resource expenditure, but they also signify lower medical quality and happiness indices for residents nearing the end of life.11
Consequently, the government has started placing more emphasis on the collaborative mechanisms between hospital palliative care teams and long-term care facilities. This is because, under the “Community Care Model”, elderly individuals residing at home are typically only sent to long-term care facilities when family members can no longer provide care due to deteriorating health. Residents in facilities require palliative care services when suffering from multiple chronic diseases and a significant decline in health.12 If nursing staff within facilities can assist palliative care teams in providing fundamental and routine palliative care services and managing urgent issues before the team arrives, it would significantly enhance the quality of palliative care services, reduce shortages, and decrease the frequency of residents being sent to hospitals for emergency treatment.13 Therefore, when palliative care teams are willing to offer educational courses and clinical guidance on palliative care to facility staff to enhance their caregiving skills, the government provides financial subsidies to support these efforts.14
Despite the continuous and proactive efforts by the Taiwanese government to promote and strengthen the “community care model”, the actual effectiveness has been quite limited. This situation mirrors challenges faced by other countries in promoting palliative care, where obstacles include insufficient managerial capabilities, lack of professional competence among healthcare personnel, and inadequate support from medical organizations.15–18 Among these factors, managers play a crucial role, as their leadership directly influences external collaborations and the quality of nursing care within the facility.19–22 Therefore, to encourage more long-term care facility managers to adopt palliative care, practical recommendations must be provided regarding the various difficulties faced at each stage of implementation and how to overcome them. Hence, it is essential to explore the processes and successful experiences of current long-term care facility managers in implementing palliative care, which is the purpose of this study.
Materials and Methods
Design and Setting
The research followed the grounded theory approach outlined by Corbin and Strauss (2015).23 Grounded theory proves valuable in situations where a phenomenon is novel or insufficiently explored, and the researcher aims to construct a framework elucidating social processes, structures, and/or interactions.23 Based on the information received from the certification of the hospital palliative care team, this study involved 11 long-term care facilities in eastern Taiwan. According to government evaluation, among them, three received an A rating (good), and six received an A- rating (qualified). Seven of the nine facilities have a capacity of 38–49 beds, while the other two have capacities of 90 and 180 beds, respectively. All nine facilities serve a role in supporting the hospital palliative care team, with a palliative care experience ranging from 2 to 5 years. The primary source of palliative care cases for these facilities is their own residents, accounting for 3–11% of all residents.
In contrast to the previously mentioned nine facilities, the remaining two facilities were rated A+ (excellent) by the government, with capacities of 36 and 49 beds, respectively. These two facilities have progressed from supporting the hospital palliative care team to assuming a collaborative role and establishing their own palliative care teams. They have accumulated 5 years of palliative care experience and source their cases not only from their own residents but also from home care and hospital hospice wards, comprising 55% and 50% of all residents, respectively.
Recruitment and Participants
In accordance with the purpose of this study and the particularity of the sample, purposive sampling was employed to select samples that meet the criteria. To enhance the richness and comprehensiveness of the sample, this study included all long-term care facilities in the entire county (Hualien County and City) that were assessed by the government as qualified or above and provided palliative care. In total, 11 facilities were included. The inclusion criteria for the managers were (1) occupying the role of a manager within the facility, responsible for the overall decision-making and operational direction of the facility, as well as overseeing the introduction and implementation of palliative care-related matters, (2) experience in directing caregivers in palliative care, and (3) the ability to communicate in Chinese or Taiwanese. Exclusion criteria included (1) not agreeing to join the study and (2) withdrawing from the study.
Finally, with the referral and assistance of the hospital palliative care teams, a total of 11 managers (A1-A9, B1-B2) agreed to participate and granted informed written consent. Group A represents facilities in a supporting role, while Group B represents facilities in a cooperative role. The participants were numbered in order of their recruitment. The participant demographics consisted of 9 people in Group A: 6 women and 3 men, aged 39 to 70 years, with 1 master’s degree, 6 university degrees, and 2 junior college degrees. Group B consisted of 2 women, aged 38 and 53 years, both with master’s degrees. All participants remained involved until the end. All recruitment was conducted by author S.W.C.
Data Collection
Data collection was conducted simultaneously across the 11 facilities using the following methods: (1) semi-structured in-depth interviews guide, and (2) a basic information sheet. The first data collection period spanned from September 1, 2019, to August 31, 2020. This period corresponds to the preliminary interview stage, during which interviews were conducted, and data were organized and analyzed. The second data collection period extended from September 1, 2020, to February 28, 2021. This phase constituted additional interviews aimed at clarifying any conceptual ambiguity, contradictions, or incomplete aspects identified in the preceding stage’s information. Research tools utilized in this study included an interview participation consent form (included publication of anonymized responses), a basic information sheet, a reflection diary, a voice recorder, and the qualitative analysis software NVivo-8. Face-to-face interviews were held in a quiet and private room within the long-term care facility by the author, S.W.C., who is qualified in qualitative research. Each participant was interviewed once or twice, with each interview lasting between 45 and 90 minutes. In the event that a relevant concept in the paper requires further explanation, or the conclusions are inconsistent with the interviews, researchers will conduct additional interviews and collect data until any conceptual gaps are addressed.
Data Analysis and Rigor
The research followed the grounded theory approach outlined by Corbin and Strauss (2015).23 The researcher initially transcribed the voice-recorded files into verbatim transcripts and also filled in the reflection log. The transcripts were then verified for consistency by listening to the recordings once again while simultaneously scrutinizing the written narrative. The analysis procedures were as follows: Open coding: In the initial stage, researchers perform open coding, breaking down the data into words or small segments and assigning descriptive labels to each of them. For example, B1 said that
Every day, people call to ask if there are any available beds, but now all the beds are full, and there are many people on the waiting list. There’s no need to worry about insufficient income.
As the researchers regarded this as “meaningful”, it was underlined and coded as “facility often at full capacity so the revenue generated is relatively stable”. A second example is taken from comments by B1 who mentioned that
Employees have been with us for a long time, and very few left. They feel they can learn a lot here, and the work environment is harmonious. In the past, there were few applicants when we advertised job openings for caregivers, but now, when we post one job opening, there are more than 20 applicants. Caregivers take pride in being able to work in our facility.
This comment was underlined and coded as “caregiver workforce has become more stable”. Since “facility often at full capacity so the revenue generated is relatively stable” and “caregiver workforce has become more stable” are a result of the implementation of palliative care, the researchers condensed these two into the concept of “steadily operate the institution”. Axial coding: The researchers then advanced to axial coding, a strategy for aggregating similar concepts. For example, “steadily operate the institution” and “families of the deceased are very appreciative of the facilities’ efforts” are both the transformation after the facilities performing palliative care, so these are classified as “facility transformation”. Selective coding: From the aggregation of similar concepts completed during the axial coding process, we identified four distinct categories into which the majority of caregiver issues could be classified. The analysis procedures can be accessed in Table 1 and Table 2. Data analysis was conducted by the author S.W.C. To enhance the rigor and coherence of the research process, the second and third authors were responsible for reviewing the first author’s analysis of the data, and the corresponding author was responsible for monitoring the research process and offering advice and consultation. After the research report was written, the author S.W.C. asked the participants to read the content, and all the participants said that the content was the same as what they described.
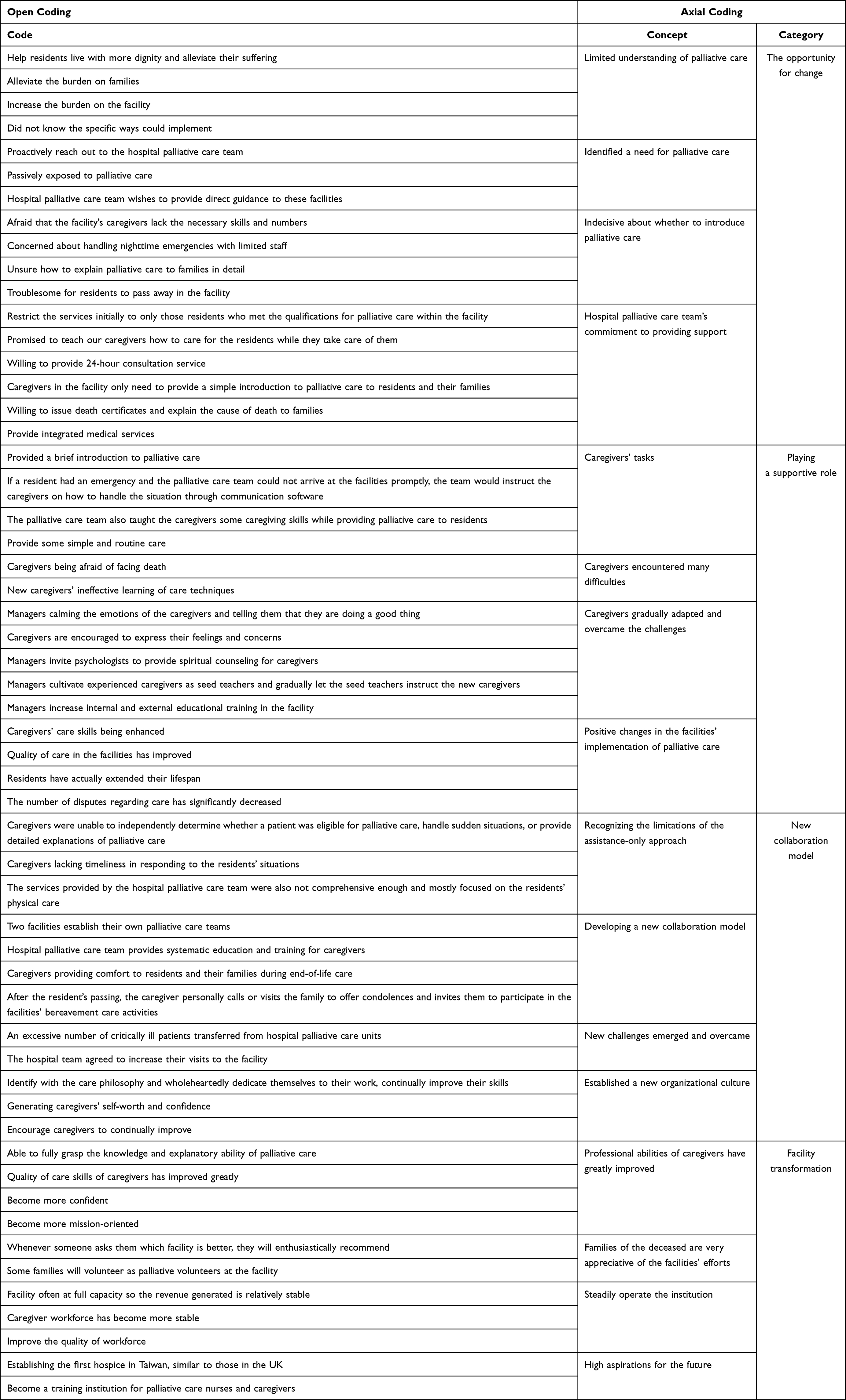 |
Table 1 Table with Codes, Concepts, and Categories |
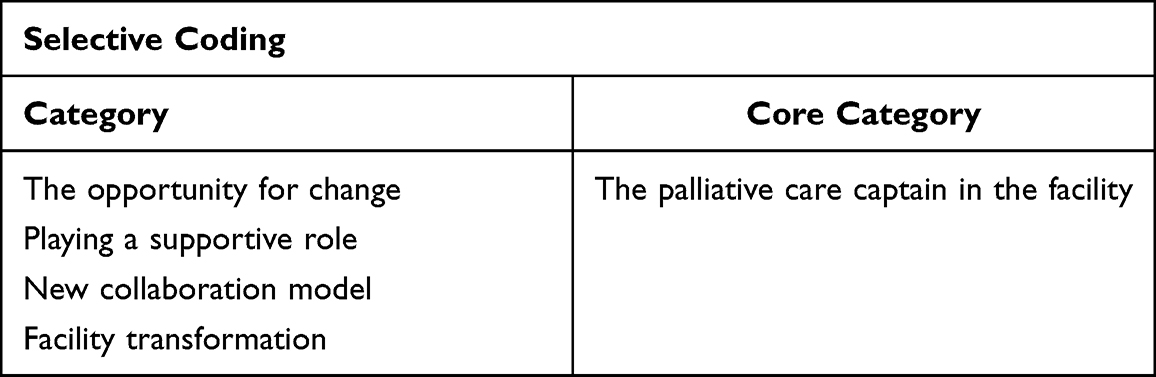 |
Table 2 Table with Categories and Core Category |
Results
Four major stages of implementing palliative care were identified in the interviews with the managers: (1) the opportunity for Change, (2) playing a supportive role, (3) a new collaboration model, and (4) facility transformation. The core category shared by the participants may be summed up as “the palliative care captain in the facility”. It reflects the spirit of the successful implementation of palliative care by managers in long-term care institutions (see Figure 1).
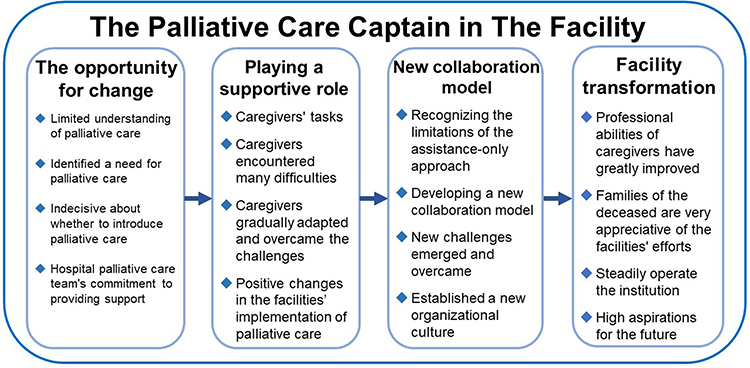 |
Figure 1 The model of implemented palliative care by the nursing managers in long term care facility. |
The Opportunity for Change
Initially, the managers of the long-term care facilities had only a limited understanding of palliative care before its implementation. However, after engaging with the hospital palliative care team and receiving explanations on how to implement it, the managers gained a clearer understanding of palliative care. Despite this, managers remained indecisive about whether to introduce palliative care into the facilities. Ultimately, with the hospital palliative care team’s commitment to providing support and practical assistance, the managers agreed to introduce it and implement it together with the hospital team.
The managers of the long-term care facilities had limited knowledge and understanding of palliative care prior to its implementation. However, some of the managers believed that introducing palliative care could enhance the end-of-life experience for residents by promoting dignity and reducing suffering.
I think it’s important for residents to live with dignity in the facility during their final stage, instead of constantly being sent to the hospital for emergency care. It can reduce a lot of their suffering [A3].
While others thought that implementing palliative care could alleviate the burden on families.
I know that the hospital palliative care team will come to the facility to provide services, so residents don’t have to be frequently sent to the hospital. Family members don’t have to go to the hospital to take care of the residents or hire caregivers [B1].
However, some managers believed that implementing palliative care would increase the burden on the facility.
Palliative care requires a lot of manpower and high-level skills, which can increase personnel costs [A8].
The majority of managers were not familiar with the specific methods of implementing palliative care in long-term care facilities.
To be honest, I only know that palliative care is good, but I really don’t know how to implement it in the facility [A2].
The managers identified a need for palliative care in the facility due to the varying conditions of the residents. For instance, a manager was moved to take action after witnessing a resident undergoing futile treatment and experiencing unnecessary suffering, prompting the manager to proactively reach out to the hospital palliative care team.
I sent a resident with terminal cancer to the hospital for emergency treatment before, and his body was full of tubes and even electric shocks, but he still passed away. After returning to the facility, I searched which hospitals have palliative care teams and contacted them [B1].
Another manager was passively exposed to palliative care due to the admission of a new resident.
There was a new resident at that time, who was already receiving home-based palliative care before coming to the facility. Afterward, the hospital palliative care team came to the facility to continue giving services [A7].
In addition, a resident received palliative care during hospitalization for an illness based on the physician’s recommendation and continued to receive it upon returning to the facility.
When an elderly person was hospitalized, the doctor suggested that he receive palliative care, and after he was discharged and returned to the facility, the hospital palliative care team came to the facility to serve him [A3].
Since there is a growing need for palliative care in various facilities, the hospital palliative care team wishes to provide direct guidance to these facilities on how to implement it.
The hospital palliative care team called and asked if they could come here to explain how to do it, and I agreed [A5].
Nonetheless, even after the hospital palliative care team provided guidance on how to implement it, the managers still hesitated about introducing palliative care. Some expressed concerns about the lack of necessary skills and number of caregivers required to provide effective palliative care.
Palliative care requires higher levels of technical proficiency, and we need to hire more talented personnel. However, it is difficult to find suitable caregivers at present [A8].
Others are concerned about handling night time emergencies with limited staff.
In fact, there are more incidents at night, and we have inadequate personnel to handle them. It is challenging to deal with residents who have emergencies and cannot be sent to hospitals [A5].
Another manager is unsure how to explain palliative care to families in detail.
We lack the ability to provide a comprehensive explanation of palliative care, and that is too difficult [A7].
Moreover, some managers believe that it is troublesome for residents to pass away in the facility, as residents’ deaths may lead to challenges in obtaining death certificates, and families may easily blame the facility.
If a resident dies in the facility or en route to the hospital, it is challenging to issue a death certificate, and it requires administrative verification. Prosecutors or designated doctors determine whether the death was accidental or due to illness. If residents pass away in the facility, some families may also perceive that the facility did not provide adequate care for the resident [A9].
Upon receiving the managers’ concerns, the palliative care team agreed to restrict the services initially to only those residents who met the qualifications for palliative care within the facility.
I told them that I can only accept my own facility’s original residents for palliative care. The number is small, and they agreed [A8].
The palliative care team also agreed to provide bedside teaching.
They promised to teach our caregivers how to care for the residents while they take care of them [A3].
Additionally, the palliative care team is willing to provide 24-hour consultation service.
They promised that we could contact them through Line at any time. They can guide us online for medication or technical aspects [A4].
Moreover, the caregivers in the facility only need to provide a simple introduction to palliative care to residents and their families.
They said that we only need to do a simple introduction. If some families still have questions after listening, they are willing to help us explain [A7].
Lastly, the palliative care team is willing to issue death certificates and explain the cause of death to families.
They are willing to issue death certificates. If families have questions about the cause of death, they are also willing to help explain [A4].
In addition to the aforementioned commitments, the palliative care team has expressed a willingness to provide integrated medical services. Specifically, when residents receiving palliative care require medical treatment, the team assumes responsibility for evaluating their condition and facilitating registration for outpatient and emergency services, as well as hospitalization if necessary.
They are willing to be the primary care team for the residents. They will evaluate the residents’ condition first, and if necessary, they will directly arrange registration for outpatient visits or hospitalization for the residents [B2].
Playing a Supportive Role
After reaching a consensus with the palliative care team in the first phase, the caregivers in the facilities, including nurses and caregivers, played a supportive role, while the palliative care team acted as the main implementer of palliative care. Despite this, caregivers still encountered many difficulties during the implementation process. However, with the guidance of the management, the caregivers gradually adapted and overcame the challenges, leading to positive changes in the facilities’ implementation of palliative care.
In agreement with the palliative care team, the facilities assumed a supportive role. Caregivers screened residents who met the criteria for palliative care and provided a brief introduction to palliative care to residents and their families. The palliative care team evaluated the residents’ eligibility for admission.
We observe the residents’ conditions and actively explain to their families if we think they are suitable for palliative care. If the family is interested, we will invite the palliative care team to evaluate them [A3].
If the residents met the admission criteria, the palliative care team provided a detailed explanation of palliative care to the residents and their families.
Whether or not the residents meet the admission criteria for palliative care is determined by the palliative care team. If they do, the team will come to the institution to provide a detailed explanation [A7].
If a resident had an emergency and the palliative care team could not arrive at the facilities promptly, the team would instruct the caregivers on how to handle the situation through communication software.
If there is an emergency with a resident and the palliative care team cannot come right away, they will use Line to tell us how to handle it, and then deal with it further when they arrive [A5].
The palliative care team also taught the caregivers some caregiving skills while providing palliative care to residents.
Sometimes the palliative care team will ask us to assist them in caring for residents and teach us some skills in the process [A6].
Caregivers could also provide some simple and routine care on their own.
The palliative care team does not come every day, so we can do some simple care on our own, such as comfort care and aromatherapy massage [A7].
Caregivers encounter some difficulties in assisting in palliative care, such as caregivers being afraid of facing death.
Caregivers do not want residents to die in the facility, and they will be afraid when they face death [A1].
Managers address this issue by first calming the emotions of the caregivers and telling them that they are doing a good thing.
Tell the caregivers that when they face the death of residents, helping them is accumulating some good karma [A1].
In addition, caregivers are encouraged to express their feelings and concerns, which can help relieve emotional stress.
Guide the caregivers to slowly express their feelings and points of fear. When everyone speaks out, the emotions will be much relieved [A2].
Managers also invite psychologists to provide spiritual counseling for caregivers.
We will invite the psychologists from the hospital’s palliative care team to provide spiritual counseling, and both staff and family members can participate [A6].
In addition to attending to the emotional well-being of caregivers, managers cultivate experienced caregivers as seed teachers to address the issue of new caregivers’ ineffective learning of care techniques and gradually let the seed teachers instruct the new caregivers.
Senior caregivers and I will first serve as seed teachers. We have more experience and can learn faster. When the palliative care team cares for residents, we will take the initiative to learn, and then slowly teach the other caregivers in our facility [A6].
Managers also increase internal and external educational training in the facility.
We will make good use of the usual handover time. When caregivers find some situations or questions in their care, they can discuss them together and clarify the issues [A4].
If there are palliative care courses outside the facility, we will send someone from our facility to attend [B2].
After the long-term care facilities assisted the hospital palliative care team in implementing palliative care, the facilities underwent positive changes, with the caregivers’ care skills being enhanced.
Now the caregivers’ skills are more proficient than before, and their movements are faster than before [A8].
In addition, the overall quality of care in the facilities has improved.
The number of outpatient, inpatient, or emergency department visits has significantly decreased [A2].
Moreover, residents have actually extended their lifespan due to receiving palliative care.
Some residents were judged by doctors to not survive for more than six months after receiving palliative care, but after our care, they have lived well for the past two years [B1].
The number of disputes regarding care in the facilities has also significantly decreased.
Before, residents with physical conditions were frequently sent to the hospital, and their families would blame us for not taking care of them properly, but now residents are rarely sent to the hospital, and their families rarely complain [A3].
New Collaboration Model
After recognizing the limitations of the assistance-only approach, two managers from long-term care facilities collaborated with the hospital palliative care team to develop a new model. However, during the implementation of this approach, new challenges emerged. With continuous adjustment and experimentation, the managers overcame these challenges and established a new organizational culture.
Originally, long-term care facilities faced many problems with the assistance-only approach, primarily due to the caregivers’ lack of advanced professional skills. As a result, they were unable to independently determine whether a resident was eligible for palliative care, handle sudden situations, or provide detailed explanations of palliative care.
It is difficult for us to judge whether the residents meet the admission criteria. Usually, we think they can, but the hospital palliative care team says no. Sometimes, when residents have sudden situations, we don’t know what to do, and we still have to wait for instructions from the palliative care team. Sometimes, we can’t answer the questions that the family members ask, and we have to ask the palliative care team to answer them [B1].
These issues would result in caregivers lacking timeliness in responding to the residents’ situations.
The hospital palliative care team cannot come immediately when we call them. If our caregivers have the ability, they can handle the situation quickly [B1].
The services provided by the hospital palliative care team were also not comprehensive enough and mostly focused on the residents’ physical care.
The hospital palliative care team has limited time to visit our facility, and they prioritize addressing the residents’ physical problems. They lack long-term care for family members, so our facility can try to provide family support on our own [B1].
To address the limitations of the assistance model, two managers of the facilities and the hospital palliative care team discussed developing a new collaboration model. With the assistance of the hospital palliative care team, the two facilities establish their own palliative care teams. One of the managers mentioned that.
The hospital palliative care team suggested referring patients discharged from the hospital’s palliative care ward to us, but I explained our facility was not capable of accepting them. Later, they offered to help train our nurses and caregivers so that our facility could form its own palliative care team, and many problems could be solved on our own [B1].
The facility’s palliative care team includes physicians, nurses, caregivers, social workers, psychologists, and religious leaders.
In terms of physicians, we work with the hospital’s palliative care team. As for nurses, caregivers, and social workers, we already have them in our facility. In addition, we work with professors from the psychology and religious departments of a university, who have expertise and background in palliative care. We invite them to our facility to engage in research, teaching, and internships. They are also willing to help us carry out palliative care [B2].
At the same time, the hospital palliative care team provides systematic education and training for caregivers.
In the past, the hospital’s palliative care team taught us based on individual cases, and what we learned was very one-sided. The current education and training are more comprehensive [B2].
In addition, the facilities also offer spiritual palliative care services, such as caregivers providing comfort to residents and their families during end-of-life care.
When a resident is dying, we will notify the family to come and accompany the resident. The family can express gratitude, love, apologies, and goodbyes to the resident so that the resident can leave peacefully and the family can have no regrets [B1].
After the resident’s passing, the caregiver personally calls or visits the family to offer condolences and invites them to participate in the facilities’ bereavement care activities.
In the first three months after the resident’s passing, we will call the family once a month to offer condolences, visit the family once every six months, and invite the family to participate in the facility’s annual bereavement care symposium [B1].
After the establishment of palliative care teams in the facilities, many challenges arose during the implementation of palliative care. Both teams were overwhelmed with an excessive number of critically ill patients transferred from hospital palliative care units, which created an unsustainable caregiving burden.
Our caregiving techniques were not yet proficient, and we were unable to care for so many palliative residents all at once. Moreover, these residents were all critically ill and could die at any time, requiring constant monitoring of their condition. The physician’s orders were numerous and frequently changed, and caregivers complained that they could not cope [B1].
The managers coordinated with the hospital palliative care team to provide additional support to address this issue, and the hospital team agreed to increase their visits to the facilities.
I told the hospital palliative care that in the beginning, you can come to our facility more frequently to help us. When our caregivers become more capable, you don’t have to come as often. They agreed to this [B1].
In addition to a new collaborative model with the hospital palliative care team, internally, the managers aim to establish a new organizational culture to facilitate smoother operations within the facilities. The managers also hope that caregivers can genuinely identify with the care philosophy and wholeheartedly dedicate themselves to their work, continually improve their skills. Therefore, the managers personally care for residents as a demonstration, allowing caregivers to observe the sincere dedication and warm care provided by the managers to the residents.
I usually demonstrate how to care for residents personally. Caregivers can feel that my dedication to the residents is sincere from my interactions with the residents and their families, and the feedback given by residents and their families can make caregivers feel that my care is warm [B1].
Furthermore, to boost caregivers’ confidence, the managers provide training on how to express themselves effectively, allowing residents and their families to give praise and thus generating caregivers’ self-worth and confidence.
I train caregivers on how to communicate with residents and their families, how to explain what to do, why to do it, the benefits of doing so, and the consequences of not doing so. After hearing the caregivers’ explanation, residents and their families feel that they are very professional and not just servants who take care of people. Caregivers also have more confidence and feel capable [B1].
Lastly, to encourage caregivers to continually improve, the managers applied to the government to convert the facilities into a qualified training and examination venue for certified caregivers. By having caregivers act as teachers, they are less likely to neglect their technical skills.
Since the facility started becoming a training organization for certified nursing assistants, caregivers have to teach new students. To avoid losing face, they spontaneously learn. The students admire the caregivers and think they are amazing. Caregivers are full of confidence [B1].
Facility Transformation
After several stages of effort, the facilities have transformed, and the professional abilities of caregivers have greatly improved. Families of the deceased are also very appreciative of the facilities’ efforts, but the management teams are not complacent and continue to steadily operate the facilities while facing many prospects for the future.
By adopting a cooperative model to implement palliative care, two long-term care facilities have significantly improved the professional abilities of their caregivers. Caregivers are now able to fully grasp the knowledge and explanatory ability of palliative care.
Now our caregivers can give detailed introductions to palliative care and answer family members’ questions [B2].
In addition, the quality of care skills of caregivers has improved greatly.
Before, our caregivers found it difficult to care for several palliative residents, but now they can easily complete the work even when caring for more residents [B2].
Caregivers have also become more confident.
Before, caregivers only knew how to do but not how to speak. Some families looked down on caregivers, thinking that they were no different from maids, but now, after listening to the professional explanation of caregivers, they think that caregiving is actually a very professional job and have begun to respect caregivers [B1].
At the same time, caregivers have also become more mission-oriented.
Our caregivers feel that the stronger their abilities, the greater their responsibilities, and they are determined to learn more caregiving knowledge and skills in order to better care for the residents [B1].
The families of the deceased are very appreciative of the two facilities’ efforts, and whenever someone asks them which facilities are better, they will enthusiastically recommend them.
Family members tell me that when their friends or relatives need palliative or long-term care, they will proactively introduce them to this facility and tell them how good it is [B2].
Some families will also volunteer as palliative volunteers at the facilities after their loved ones have passed away.
Some families feel that their loved ones received a lot of care at the facility and think that they should give something back. They will tell those grieving families about their experiences, support and accompany them [B1].
In addition, the facilities hold an annual meeting for the families of the deceased.
Many families come to attend the meeting, and they think this event is great because they can commemorate their loved ones together and get to know others who have had similar experiences. They can share their stories with each other, find comfort in their shared experiences, and potentially reduce feelings of sadness [B1].
As caregivers’ professional capabilities grow and their efforts are recognized by family members, the facilities are able to operate steadily and often at full capacity. Consequently, the revenue generated by the facilities is relatively stable.
Every day, people call to ask if there are any available beds, but now all the beds are full, and there are many people on the waiting list. There’s no need to worry about insufficient income [B1].
Additionally, the caregivers’ workforce has become more stable with low turnover rates and numerous job applicants.
Employees have been with us for a long time, and very few left. They feel they can learn a lot here, and the work environment is harmonious. In the past, there were few applicants when we advertised job openings for caregivers, but now, when we post one job opening, there are more than 20 applicants. Caregivers take pride in being able to work in our facility [B1].
Furthermore, the facilities encourage employees to pursue further education and training to improve the quality of their workforce.
Our employees also go to universities for further education. The educational background of our employees is higher than before [B1].
Although the facilities have successfully transformed, the managers still have high aspirations for the future, such as establishing the first hospice in Taiwan, similar to those in the UK.
There is no hospice in Taiwan like those in the UK. We hope that through our continuous efforts, we can one day establish a hospice that belongs to Taiwan [B1].
The managers also hope the facility to become a training institution for palliative care nurses and caregivers.
Currently, the training for palliative care in long-term care facilities is provided by hospital palliative care teams. If this training can be provided by our facility, hospital palliative care teams can have more time to care for more patients [B1].
Discussion
This study has identified four stages that managers experience when implementing palliative care in their facilities. The first stage was the opportunity for change, the second stage was playing a supportive role, the third stage was a new collaborative model, and the fourth stage was the facility transformation. All 11 long-term care facilities involved in the study achieved the second stage, but only two managed to reach the third and fourth stages. The reasons for this are discussed below.
During the first stage of implementing palliative care in the facilities, most managers lacked a complete understanding of the concept but still showed positive affirmation. Maintaining a positive attitude was crucial for managers before executing a plan, as it could affect the success or failure of subsequent steps.24 In addition, the managers had to have the ability to perceive the future development direction of the long-term care field.25 In this study, managers were able to recognize the demand for palliative care brought about by the aging society and medical advancements. It was imperative to introduce palliative care, whether as an active demand from original residents or passively brought into the facility by new residents.26 Managers also had to understand the situation of their own facilities, including sufficient manpower and potential obstacles in executing related regulations and procedures. By identifying exact problems, they could request support and find solutions.27 Lastly, managers needed good communication and coordination skills to inform the hospital palliative care team of the current shortcomings and obtain the most appropriate assistance. In this stage, it was evident that during the initial implementation of palliative care, the palliative care team played a crucial role, complementing the insufficient capabilities of personnel in early long-term care facilities. The task for institutional managers at this stage was to gain a comprehensive understanding of the content and implementation methods of palliative care. Simultaneously, managers needed to identify existing problems within the facility, eliminating uncertainties to smoothly progress to the next stage.
In the second stage, facilities started to collaborate with external units to implement palliative care. At this point, managers must have a clear understanding of the roles and tasks that the facilities need to perform when working with the hospital palliative care team to provide the most effective assistance and learn from it.28 Internally, it is necessary to address issues caused by the implementation of palliative care, such as caregivers’ concerns, negative emotions, and the challenges faced by new caregivers when learning the necessary skills. Once facilities can effectively cooperate with external units and solve internal staff problems, positive feedback starts to emerge at this stage, including improved caregiver skills, higher quality care, fewer medical visits by residents, and fewer complaints from family members.13 These feedback indicators are essential and represent a turning point in determining whether facilities can move on to the next stage. During this stage, the palliative care team continues to play a significant role, but the facilities shift from passive reliance to a supporting role. At this point, the manager’s task is to enhance staff technical training while being attentive to potential adaptation issues and emotional problems resulting from increased task burdens. If this stage involved effective collaboration with the palliative care team, the implementation could be considered on track, with positive feedback starting to emerge.
In the third stage, two facilities completed the indicators of the previous stage and entered this new phase. At this point, it was discovered that the existing collaborative model had some shortcomings that needed to be addressed. For instance, caregivers lacked the advanced abilities necessary to independently assess eligibility for palliative care, handle emergencies, and provide detailed explanations of palliative care, all of which require the assistance of the hospital palliative care team. Therefore, managers needed to have independent and immediate decision-making abilities and identify the need to cultivate their own palliative care teams to solve the problem of over-reliance.29 To establish facilities’ own palliative care teams, managers had to first examine and integrate the facilities’ existing resources, such as personnel staffing and job composition, while also identifying and addressing any gaps or deficiencies. Once managers integrated their own palliative care teams, they could begin to create an organizational culture and standard operating procedures unique to the facilities. For example, managers personally demonstrate care for residents, to allow caregivers to empathize with the managers’ thinking and understand the true meaning of palliative care, which can ignite their work passion.30 Furthermore, managers used training courses to improve caregivers’ communication skills and cultivate self-confidence through the praise of family members.31 Lastly, by transforming the facilities into ones that also train caregivers, with internal caregivers acting as instructors, caregivers achieved the goal of self-monitoring and continuous learning through the responsibility and honor derived from teaching. This way, caregivers can continuously improve their skills, and the facilities can maintain a high standard of care.32 This stage marks a crucial transformation where the facilities shift from a supporting role to independence, with the capability to independently train palliative care professionals. The ability to achieve independence serves as a watershed for entering the third stage. In this stage, the managers’ tasks extend beyond organizing and forming the facilities’ own palliative care team to motivating employees to transition from learners to instructors.
In the fourth stage, facilities managers achieved success and experienced multiple benefits, such as increased caregiver confidence and professional abilities, recognition, and strong recommendations from residents’ families, stable operating revenue, and a decrease in caregiver turnover rate. These benefits were also the new indicators of success for this stage. Nevertheless, successful managers did not stop at this stage. The managers continued to explore new and effective operational methods, such as allowing the families of the deceased to serve as volunteers and interact with new residents’ families. This provided a place for the families of the deceased to express their thoughts and feelings while also comforting the families of new residents.33 Moreover, successful managers did not become complacent but instead maintained stability and looked to the future, setting even more ambitious goals. In this stage, the facilities had successfully implemented the palliative care model, and the managers’ tasks shifted to contemplating innovation and maintaining employee enthusiasm to enhance palliative care further.
Application of Findings
Based on the study findings, this research provides a guide for long-term care facilities intending to implement palliative care. The guide includes potential issues and corresponding solutions at each stage, aiming to offer practical references for facilities during the implementation of palliative care. See Table 3 below:
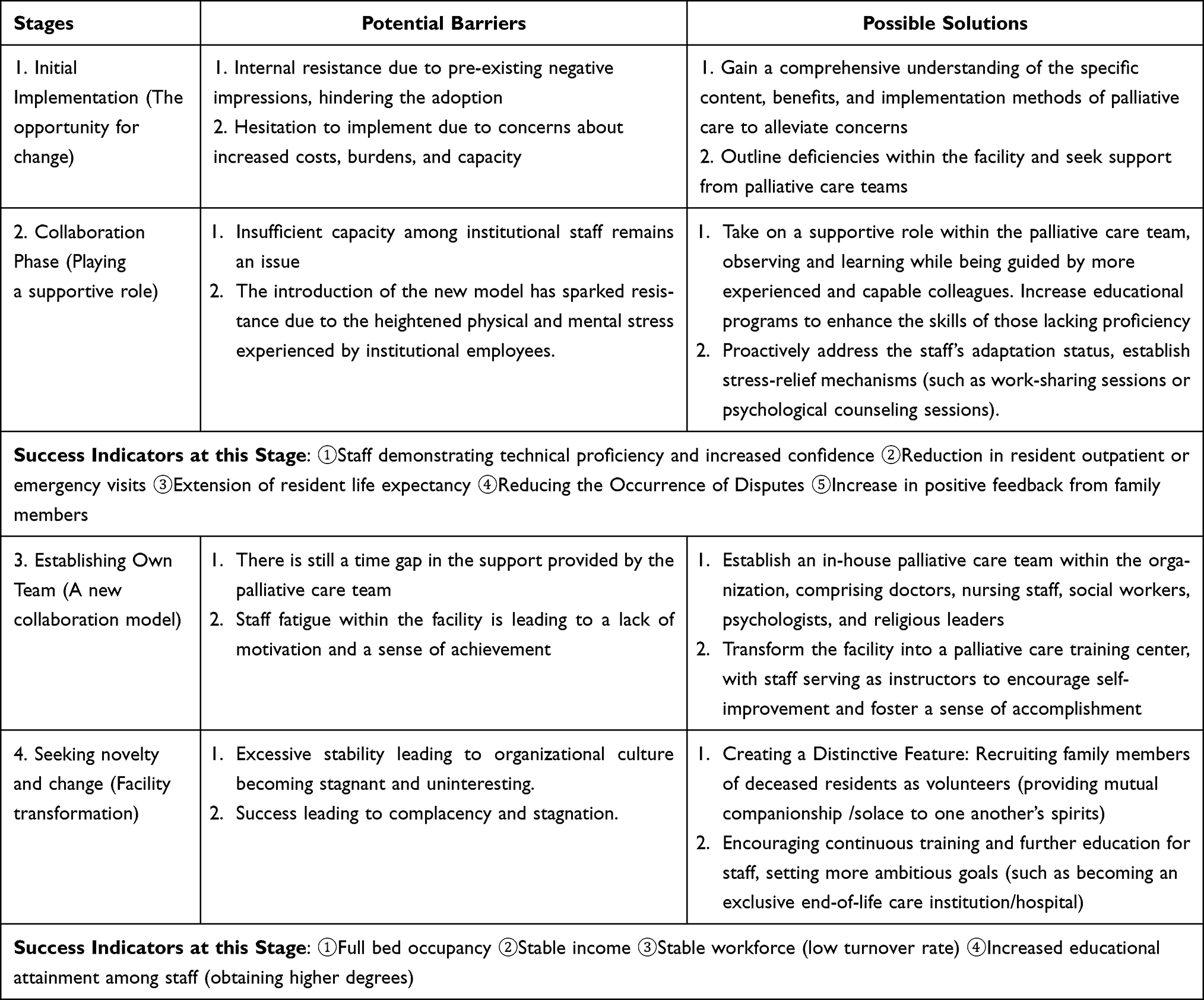 |
Table 3 Guidelines for the Implementation of Palliative Care at Various Stages by Long-Term Care Facility Managers |
Limitations and Future Research Recommendations
Firstly, due to the fact that such management experiences involve business interests, the majority of managers declined interviews to safeguard their operational advantages. Consequently, a nationwide sample could not be obtained, marking the first limitation of this study. Secondly, although the sampling in this study covered all qualified facilities (from A-Qualified to A+Excellent) in the county and city, and these facilities underwent consistent government assessments nationwide, indicating a representative operational capacity, it is noteworthy that the results of this study revealed a crucial role played by hospital and clinic palliative care teams in assisting facilities during the first two stages of implementing palliative care. Therefore, we cannot ascertain whether palliative care teams in other counties and cities provide the same service quality and whether such variations impact the study results, constituting the second limitation of this research. Despite these limitations, this study contributes to exploring the experiences and processes of long-term care facility managers in implementing palliative care and offers relevant guidance. Lastly, for future research opportunities, exploring the experiences of collaboration and implementation from the perspective of hospital or clinic palliative care teams, combined with the managerial perspective for mutual verification analysis, could reveal different problem perspectives from a clinical standpoint.
Conclusion
The study reveals that during the initial phases of implementing palliative care, the palliative care teams assume a crucial leadership role, while the facilities play a supportive role. At this stage, managers should focus on personnel training and addressing internal issues within the facilities to facilitate successful collaboration with the palliative care teams. In the later stages, the facilities transition from a supportive role to one of independence, marking a critical juncture for the facilities’ potential stable development. During this period, managers are tasked not only with establishing the facilities’ own palliative care team but also with facilitating the transformation of staff from learners to instructors. Finally, even after successful implementation, managers should contemplate strategies for innovation and set more ambitious goals.
Data Sharing Statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available because of privacy and ethical restrictions.
Ethical Approval
The study was approved by the Research Ethics Committee of Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taiwan (Approval no. IRB108-104-B) on June 6, 2019.
Acknowledgments
We would like to thank all the participants in this study for their time and willingness to share their experiences and feelings with us.
Funding
The authors receive no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Jakobsson E, Bergh I, Öhlén J, Odén A, Gaston-Johansson F. Utilization of health-care services at the end-of-life. Health Policy. 2007;82(3):276–287.
2. Hall S, Kolliakou A, Petkova H, Froggatt K, Higginson IJ. Interventions for improving palliative care for older people living in nursing care homes. Cochrane Database Syst Rev. 2011;2011(3):CD007132. doi:10.1002/14651858.CD007132.pub2
3. Antonsson H, Korjonen SE, Rosengren K. First-line managers’ experiences of alternative modes of funding in elderly care in Sweden. J Nurs Manag. 2012;20(6):737–747. doi:10.1111/j.1365-2834.2012.01464.x
4. Vilapakkam Nagarajan S, Poulos CJ, Clayton JM, Atee M, Morris T, Lovell MR. Australian residential aged care home staff experiences of implementing an intervention to improve palliative and end-of-life care for residents: a qualitative study. Health Soc Care Commu. 2022;30(6):e5588–e5601. doi:10.1111/hsc.13984
5. World Health Organization. Palliative care for older people: better practices. WHO Regional Office for Europe 2011. Available from: http://www.euro.who.int/en/publications/abstracts/palliative-care-for-older-people-better-practices.
6. Ministry of Health and Welfare [homepage on the Internet]. Taipei: National Health Insurance Administration; 2017. Available from: https://www.nhi.gov.tw/Content_List.aspx?n=46505DE49DF0AA0B&topn=0B69A546F5DF84DC.
7. Tsay MS, Chang YH, Wang CY, et al. Effectiveness of the establishment and operation of the integrated care network for community hospice care. Taiwan J Hosp Palliat Care. 2021;25(3):253–268. Chinese. doi:10.6537/TJHPC.202107_25(3).04
8. Lu SY, Lin PC. The future development of community palliative care. New Taipei J Nurs. 2017;19(1):1–5. Chinese. doi:10.6540/NTJN.2017.2.001
9. Taiwan healthcare reform foundation [homepage on the Internet]. Taipei: Taiwan Healthcare Reform Foundation; 2020. Available from: https://www.thrf.org.tw/archive/2350.
10. Chang JH. Why is it so difficult to good death in long term care facility? Common Health Mag. 2015;204:158–164. Chinese.
11. Tsai HH, Tsai YF, Huang HL. Nursing home nurses’ experiences of resident transfers to the emergency department: no empathy for our work environment difficulties. J Clin Nurs. 2016;25(5–6):610–618. doi:10.1111/jocn.13084
12. Mertens F, Sercu M, Derycke A, et al. Patients’ experiences of transfers between care settings in palliative care: an interview study. Ann Palliat Med. 2022;11(9):2830–2843. doi:10.21037/apm-22-146
13. Chiang SW, Wu SC, Peng TC. The experience to implement palliative care in long-term care facilities: a grounded theory study of caregivers. Asian Nurs Res. 2021;15(1):15–22. doi:10.1016/j.anr.2020.10.006
14. Liu ML, Chan TT, Hsieh IC, Lin MY, Kuo YH, Chen SJ. Network development of a localized community-based palliative home care service. Taiwan J Hosp Palliat Care. 2021;25(2):97–109. Chinese. doi:10.6537/TJHPC.202103_25(2).01
15. Harasym P, Brisbin S, Afzaal M, et al. Barriers and facilitators to optimal supportive end-of-life palliative care in long-term care facilities: a qualitative descriptive study of community-based and specialist palliative care physicians’ experiences, perceptions and perspectives. BMJ Open. 2020;10(8):e037466. doi:10.1136/bmjopen-2020-037466
16. Handley M, Goodman C, Froggatt K, et al. Living and dying: responsibility for end-of-life care in care homes without on-site nursing provision - A prospective study. Health Soc Care Commu. 2014;22(1):22–29. doi:10.1111/hsc.12055
17. Lo RS, Kwan BH, Lau KP, Kwan CW, Lam LM, Woo J. The needs, current knowledge, and attitudes of care staff toward the implementation of palliative care in old age homes. Am J Hosp Palliat Care. 2010;27(4):266–271. doi:10.1177/1049909109354993
18. Dwyer D. Experiences of registered nurses as managers and leaders in residential aged care facilities: a systematic review. Int J Evid Based Health. 2011;9(4):388–402. doi:10.1111/j.1744-1609.2011.00239.x
19. Norton SA, Ladwig S, Caprio TV, Quill TE, Temkin-Greener H. Staff experiences forming and sustaining palliative care teams in nursing homes. Gerontologist. 2018;58(4):e218–e225. doi:10.1093/geront/gnx201
20. Thorpe K, Loo R. Balancing professional and personal satisfaction of nurse managers: current and future perspectives in a changing health care system. J Nurs Manag. 2003;11(5):321–330. doi:10.1046/j.1365-2834.2003.00397.x
21. Johansson G, Pörn I, Theorell T, Gustafsson B. A first-line nurse manager’s goal-profile. J Clin Nurs. 2007;16(1):149–159. doi:10.1111/j.1365-2702.2006.01446.x
22. Håkanson C, Cronfalk BS, Henriksen E, Norberg A, Ternestedt BM, Sandberg J. First-line nursing home managers in Sweden and their views on leadership and palliative care. Open Nurs J. 2015;8:71–78. doi:10.2174/1874434601408010071
23. Corbin JM, Strauss AL. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory.
24. Åvik Persson H, Ahlström G, Ekwall A. Professionals’ expectations and preparedness to implement knowledge-based palliative care at nursing homes before an educational intervention: a focus group interview study. Int J Environ Res Public Health. 2021;18(17):8977. doi:10.3390/ijerph18178977
25. Dever KH. Through the eyes of nurse managers in long-term care: identifying perceived competencies and skills. J Gerontol Nurs. 2018;44(5):32–38. doi:10.3928/00989134-20180322-01
26. Persson HÅ, Ahlström G, Ekwall A. Professionals´ readiness for change to knowledge-based palliative care at nursing homes: a qualitative follow-up study after an educational intervention. BMC Palliat Care. 2022;21(1):132. doi:10.1186/s12904-022-01018-y
27. Nilsen P, Wallerstedt B, Behm L, Ahlström G. Towards evidence-based palliative care in nursing homes in Sweden: a qualitative study informed by the organizational readiness to change theory. Implement Sci. 2018;13(1):1. doi:10.1186/s13012-017-0699-0
28. Ersek M, Unroe KT, Carpenter JG, Cagle JG, Stephens CE, Stevenson DG. High-quality nursing home and palliative care-one and the same. J Am Med Dir Assoc. 2022;23(2):247–252. doi:10.1016/j.jamda.2021.11.027
29. Dahlin C, Sanders J, Calton B, et al. The cambia sojourns scholars leadership program: projects and reflections on leadership in palliative care. J Palliat Med. 2019;22(7):823–829. doi:10.1089/jpm.2018.0523
30. Griffith S, Gelling L. How do hospice nurses prepare to give end-of-life care? A grounded theory study of nurses in one UK hospice. Int J Palliat Nurs. 2021;27(7):334–350. doi:10.12968/ijpn.2021.27.7.334
31. Reitinger E, Schuchter P, Heimerl K, Wegleitner K. Palliative care culture in nursing homes: the relatives’ perspective. J Res Nurs. 2018;23(2–3):239–251. doi:10.1177/1744987117753275
32. Zhao Y, Liao L, Feng H, Chen H, Ning H. Enablers and barriers to implementing care quality improvement program in nursing homes in China. BMC Geriatr. 2021;21(1):532. doi:10.1186/s12877-021-02488-0
33. Coleman H, Sanderson-Thomas A, Walshe C. The impact on emotional well-being of being a palliative care volunteer: an interpretative phenomenological analysis. Palliat Med. 2022;36(4):671–679. doi:10.1177/02692163211064770
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.